")
Back to Journals » International Journal of General Medicine » Volume 15
The Concept of Pharmacy Ethics and the Examples of Ethical Dilemmas Encountered by Pharmacists in the Asir Region, Saudi Arabia: A Qualitative Study
Authors Orayj K , Alahmari K, Alasiri M
Received 27 March 2022
Accepted for publication 9 May 2022
Published 16 May 2022 Volume 2022:15 Pages 4985—4996
DOI https://doi.org/10.2147/IJGM.S368262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Khalid Orayj,1 Khalid Alahmari,2 Moath Alasiri2
1Department of Clinical Pharmacy, College of Pharmacy, King Khalid University, Abha, Saudi Arabia; 2College of Pharmacy, King Khalid University, Abha, Saudi Arabia
Correspondence: Khalid Orayj, Email [email protected]
Introduction: Pharmacists’ involvement in patient care is expanding. The inclusion of this function within a complex healthcare system populated by demanding patients may create ethical challenges. In Saudi Arabia, few studies have been conducted on pharmacy ethics, and the available data are quantitative in nature. Thus, there remains a need for a qualitative assessment of the ethical dilemmas facing pharmacists.
Methods: This exploratory study utilized a qualitative methodology that included open-ended, in-depth, semi-structured interviews, followed by content analysis. The study recruited credentialed pharmacists from community and hospital pharmacies. Themes and codes were created and classified.
Results: Eighteen pharmacists were interviewed, and their responses were categorized into eight areas of ethical dilemma: beneficence and non-maleficence, autonomy, justice, confidentiality, veracity, communication skills, sincerity and religion, and law. Taken together, it appears that most of the ethical challenges to the practice of pharmacy center on the theme of beneficence and non-maleficence. Additionally, it was found that some social and religious practices and beliefs contribute to the formation of participants’ ethical backgrounds.
Conclusion: These findings may aid in the development of national pharmacy ethics guidelines in Saudi Arabia. Additional quantitative research is necessary to confirm the study’s findings.
Keywords: pharmacy ethics, community pharmacy, hospital pharmacy, bioethics
Introduction
Given the significance of ethical issues in medical practice, it is crucial for pharmacists to consider ethical principles when practicing their profession. Medical ethics can be traced back to ancient civilizations, as seen by the Hippocratic Oath, which is still in use today.1 In recent years, there has been a significant increase in the number of ethical challenges within healthcare, particularly involving moral decision-making and the prioritization of patients.2 Ethical considerations in healthcare have become more complicated in recent years, mostly because of rising costs and technical advancements in pharmacy practice.2 Due to the commercial nature of pharmacies, the expanding role of commercial health insurance which is motivated by profit maximization, and the growing role played by clinical pharmacists in hospitals, the practice of pharmacy in hospital and community settings presents various ethical dilemmas.3
Modern healthcare ethics have been shaped by the bioethics concepts articulated in the Declaration of Geneva in 1948, following World War II.4 The principles of beneficence (doing good), non-maleficence (first, do no harm), justice (equity in distribution of potential benefits and harms, as well as equity in access) and autonomy (respect for patients’ decision-making, privacy, and their right to refuse) have become cornerstones of modern healthcare ethics standards.4 In fact, most pharmacy codes of professional ethics around the world reflect these principles.4 Pharmacy ethics standards have evolved throughout the years, based on similar principles of practice but with varying degrees of detail. In 2012, the Saudi Commission for Health Specialties (SCFHS) developed ethical guidance for Saudi health practitioners. Following an Islamic perspective, this document laid out the most significant guidelines for medical professionals.5 Though this guide was written by a group of Islamic and medical experts, it did not address certain concerns in health practice, such as ethical dilemmas and how to resolve them. Additionally, information concerning specific health specialties, such as the pharmacy profession, was omitted from this guide due to its generalist nature.5
In Saudi Arabia, the establishment of a public health department in 1925 marked the beginning of the development of the country’s healthcare system.6 The Ministry of Health was formed in 1951, and since then the healthcare system has grown tremendously, particularly between 1970 and 1980.7 In addition to distributing medications, regular pharmacists in Saudi Arabia also answer a wide range of questions from patients about a variety of medical conditions.8 Add to this the increasing role of clinical pharmacists in Saudi hospitals,8 and it is clear that pharmacists (regular or clinical) must understand not only ethical issues but also how to develop the most ethical response to critical situations.
Given that the SCFHS guide does not address pharmacy ethics, it is therefore necessary to identify the most significant ethical dilemmas confronting community and hospital pharmacists prior to developing a comprehensive ethical guide for pharmacists in Saudi Arabia. Only one study has focused on the ethical challenges facing pharmacists in Saudi Arabia, but it has been quantitative rather than qualitative studies.9 Thus, we must begin with qualitative investigations to refine our understanding of the subject before moving on to quantitative studies to confirm the findings.
This study aims to; (1) fill a knowledge gap in the field by conducting a qualitative investigation of the most pressing ethical dilemmas facing community and hospital pharmacists in the Asir region of the Kingdom of Saudi Arabia, and (2) help SCFHS to know the most prevalent ethical dilemmas among pharmacists, which facilitates the issuance of an ethical guide that helps pharmacists to overcome these dilemmas.
Methods
Research Design
This study used a qualitative research approach involving semi-structured interviews to gather pharmacists’ perspectives on ethical issues pertaining to pharmacy practice, as well as to understand the experiences that influenced their perspectives. The classification of codes was retrieved directly from the interviews in this method. The interviews were held between August 2021 and March 2022.
Participants and Data Collection
Purposive sampling was used to select the study participants from pharmacists in the Asir region of Saudi Arabia. The researchers chose purposive sampling to ensure the participation of a subset of people who provide a rich source information about the issue under study. Purposive sampling is a random selection of sampling units within the population segment having the greatest information on the desired attribute.10 A bachelor’s degree in pharmacy, knowledge of the subject, and willingness to engage in the study were all required to be considered for inclusion in the study. The study included a total of 18 pharmacists, nine of whom were community pharmacists and nine of whom worked in hospitals. Due to conflicts with work, fear, or personal reasons, nine pharmacists opted not to engage in an interview with the researcher. This study used semi-structured interviews, conducted face-to-face, between an interviewer and participants who did not know one another. Depending on the researcher-participant interaction, interviews lasted anywhere from 30 to 90 minutes. The goal of the interview was described for the participant at the outset. With the help of an interview guide sheet, participants were able to respond to each question at their own pace. The researchers asked probing follow-up questions to explore respondents’ thoughts. The first interview question asked participants to define pharmacy ethics in their own words; ensuing questions presented examples of ethical dilemmas that pharmacists might face in their work. These dilemmas were developed based on prior research on this issue9 (see Box 1). Finally, the participants were asked if to describe any ethical dilemmas they had faced that did not come up in the interview. The participants’ choices were considered while determining the day, time, and location of the interviews. All interviews were recorded and fully transcribed after gaining permission from the participants. The interviews lasted until the data saturation point, at which point no new information or concepts were gained.
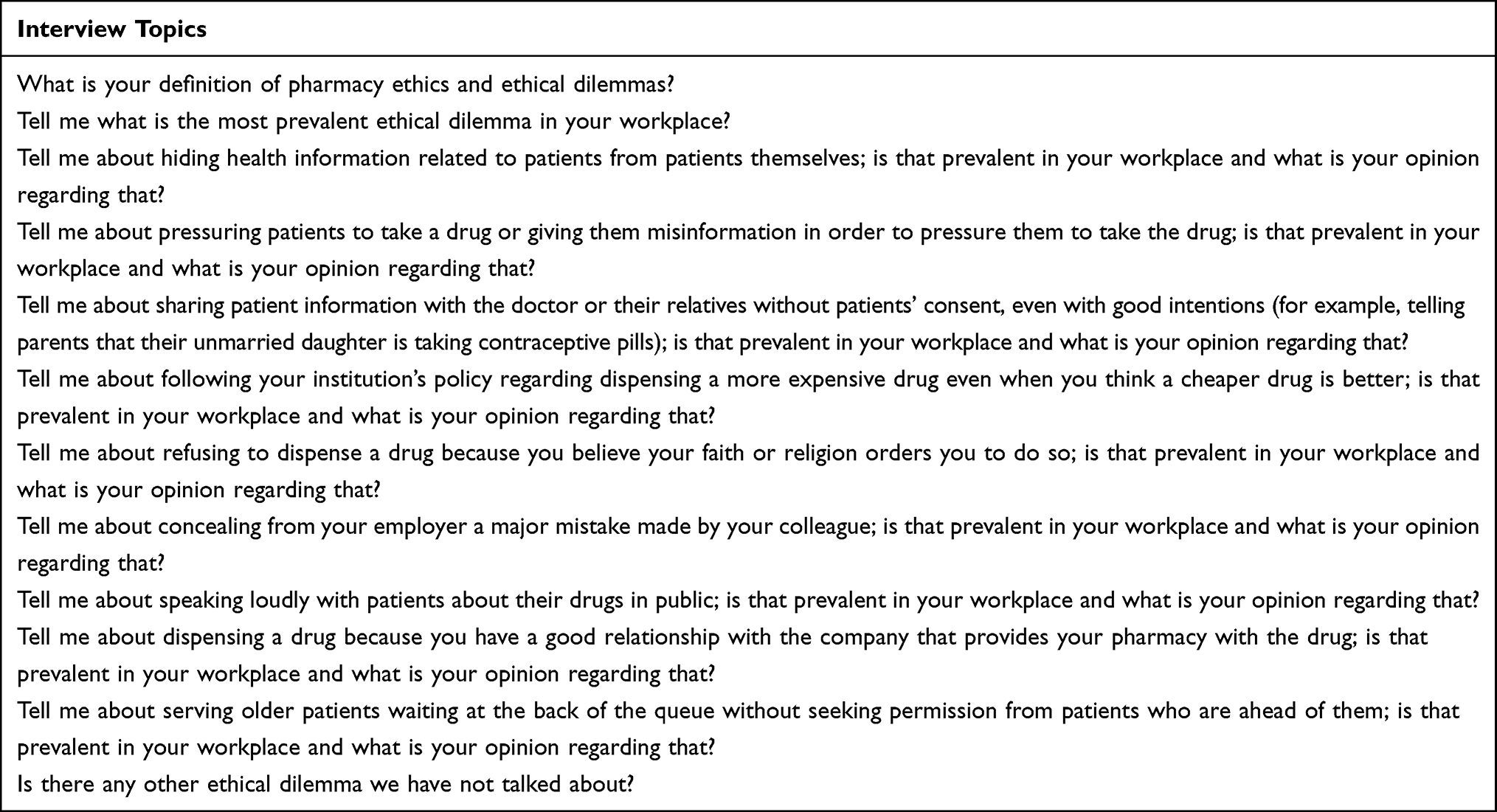 |
Box 1 Content of the Interview Questions |
Data Analysis
The interviews were translated from Arabic to English and the information was reproduced as accurately as feasible. To ensure the accuracy of our translations into English, we sent the interviews to an English specialist who verified our work. We then retranslated the interviews from English to Arabic and returned them to participants for approval. We began transcribing, translating, and analyzing the interviews as soon as they were completed. The transcripts were coded line by line by two researchers, who kept a diary of developing codes, their definitions, and examples of their use (open coding). The researchers then compared and contrasted their findings (constant comparative technique).11 This debriefing helped achieve agreement on new codes, code expansion, and code merger (axial coding). A third investigator settled disagreements. In the aftermath of each conversation, we adjusted the interview guide to allow for more investigation, clarification, or elaboration on any remaining questions.
Increasing Rigor
Several strategies were employed in this study to ensure the reliability of the data and to strengthen its rigor. Participants were selected through purposive sampling from both community and hospital pharmacies to improve the credibility of the data. Other techniques to improve data credibility included continuous data analysis while collecting data, data analysis following interviews, and using the findings of interviews to improve and adjust the questions asked in subsequent interviews.
Ethical Considerations
The Research Ethics Committee of King Khalid University gave their consent for this study. The interviews were performed at the interviewees’ desired time and location, with their informed consent and the ability to withdraw consent at any moment during the process. Participants did not object to publishing their data as long as it is anonymized. The confidentiality of the information was maintained during these interviews.
Results
Demographic data about participants are shown in Table 1. Eighteen pharmacists were interviewed for this study, and the results were organized into eight themes and 18 codes, which are detailed in Table 2. Eight themes of ethical dilemmas in the field of pharmacy emerged: beneficence and non-maleficence, autonomy, justice, confidentiality, veracity, communication skills, sincerity and religion, and law. It should be noted that there may be some overlap between themes and codes, making a thorough separation of them impossible (Table 2).
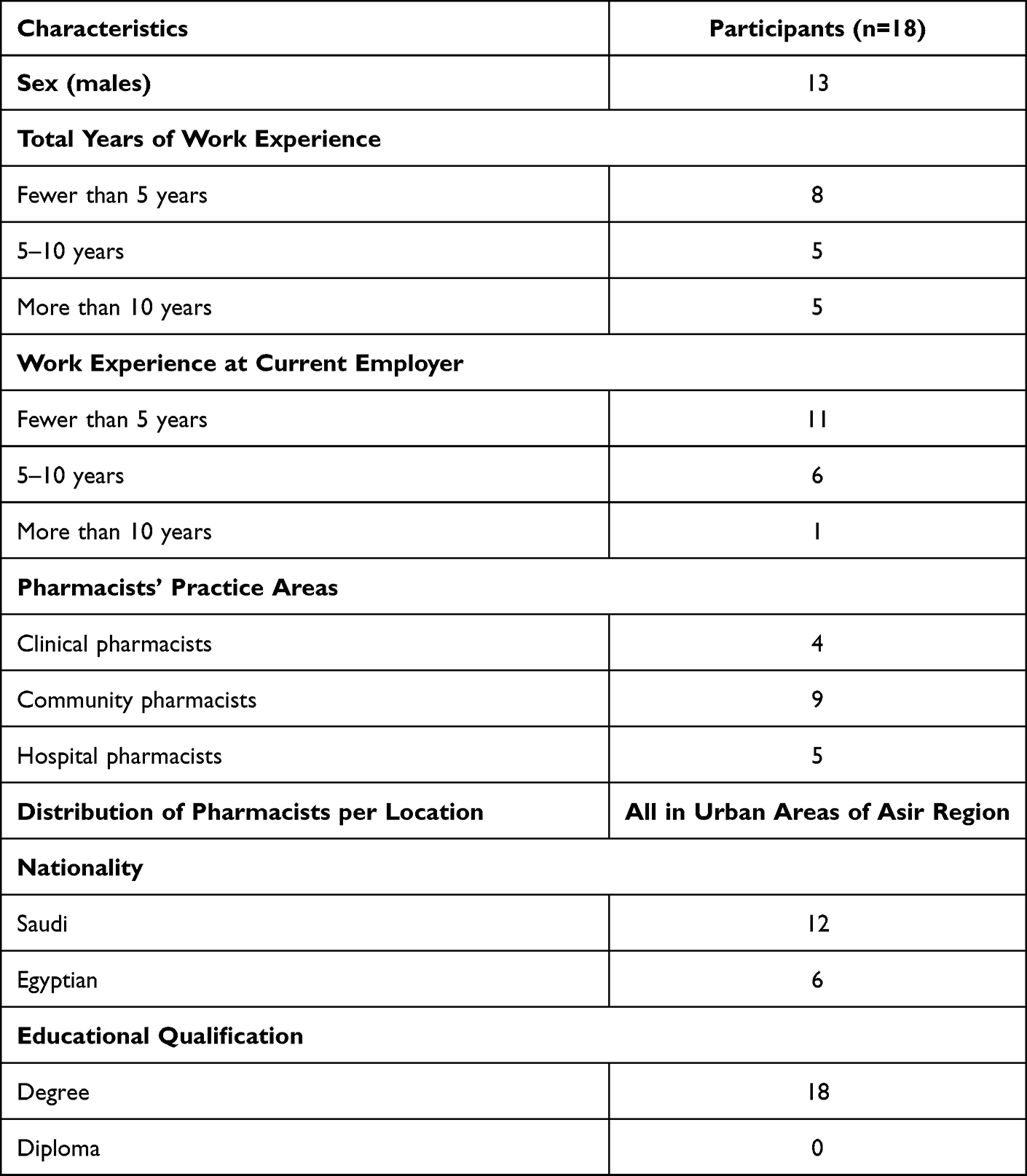 |
Table 1 Demographic Characteristic of Interviewees |
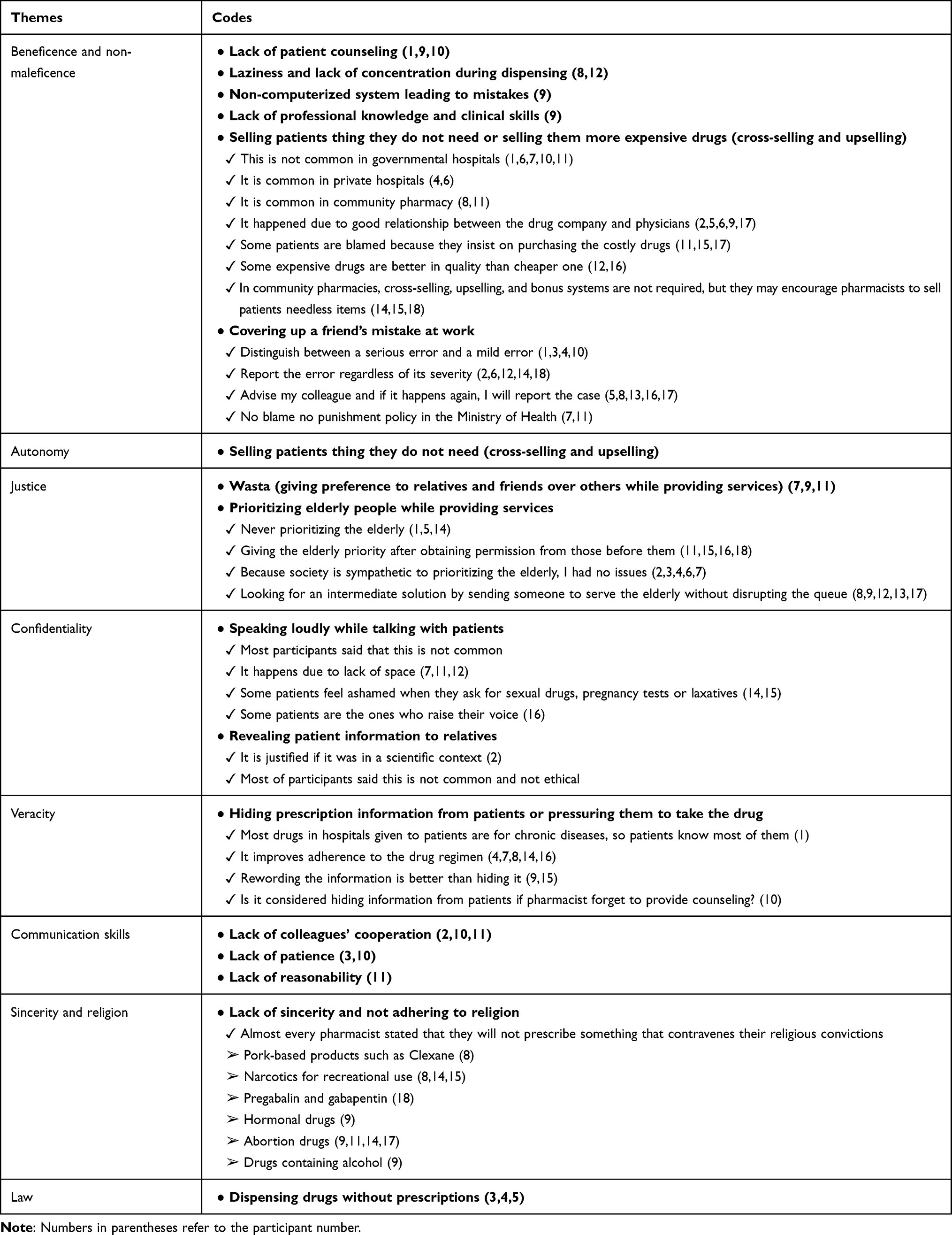 |
Table 2 Themes and Codes Generated from the Interviews |
Theme 1: Beneficence and Non-Maleficence
This theme is represented in two areas: first, in the definition of pharmacy ethics, and second, as the most prevalent ethical dilemma with which pharmacists must deal. In terms of pharmacy ethics, several participants defined it as helping the patients and satisfying their desires, which contributes to the patient’s benefit and avoids harm. Several participants made this argument in broad strokes without elaboration; as one of them stated,
But in general, the ethics of the pharmacist’s profession, is about … securing the health needs in providing pharmaceutical care. Also, we have to assure patient’s understanding of his medication. [Participant No. 1]
It is a humanitarian profession, and our job is to help people. The pharmacist is present at any time and ready to help. The materialistic thinking has no place in our profession. [Participant No. 5]
On the other hand, several participants offered practical examples of the principles of beneficence and non-maleficence in their definitions of pharmacy ethics. For instance, one of them stated that the pharmacist must possess a high level of scientific expertise and a commitment to continual education to provide the best possible care to the patient:
You must have a good sense of pharmacotherapy knowledge. This is the first thing; you should not deal with a patient if you do not have a minimum of pharmacological knowledge. You must be licensed, and the license ensures that the pharmacist has the minimum information that is useful to deal with the patients. You do not deal with concrete and not with a program on the computer. You deal with the greatest creature, that is man. The human could be me, or your father … also, you must have continuous education, it is harmful to stop reading. If you stop reading the books, you will find yourself forgetting and many things you do not know. [Participant No. 9]
Regarding the ethical dilemmas underlying this theme, we determined six codes: lack of patient counseling, laziness and lack of concentration during dispensing, non-computerized system that leads to mistakes, lack of professional knowledge and clinical skills, selling patients things they did not need or selling them a more expensive drug (cross-selling and up-selling, respectively), and covering up a co-worker’s mistake at work.
Some participants remarked, for example, that patient counseling is not sufficiently emphasized and at times is not offered to patients. As one of them stated,
There is the dilemma that we try to eliminate and reduce as much as possible, which is the issue of lack of patient counseling. The patient has the right to know his full medications, how to use them correctly, and the medications that conflict with them, but sometimes the work pressure did not allow us to do so. [Participant No. 1]
Several participants raised another issue that is detrimental to the patient: providing patients with medicines and items they do not require via cross-selling and upselling. Upselling is the practice of persuading customers to purchase a more expensive product that is comparable to the one requested, while cross-selling encourages customers to acquire related or complementary things.12 These two phenomena were noted by participants as being more widespread in private hospitals and community pharmacies, where employees are compensated for meeting monthly or annual sales targets. One participant said,
There is something called cross-selling. One pharmacist told me that a patient came to the pharmacy with a skin allergy. Literally, he only needed one medicine to treat the issue, but the pharmacist gave him 14 products of unnecessary shampoo, creams, oils, fingernail cutter and the pharmacist would claim that the products the patient used before he came to the pharmacy were the ones that caused him to have an allergy, so he must change them. In addition, there is a product list that one famous pharmacy has, which included products that if the pharmacist sells, he will be rewarded. [Participant No. 14]
One final issue related to the principle of non-maleficence was mentioned by most participants: not reporting a coworker for mistakes. Participants described differing attitudes depending on the kind of mistake, distinguishing between small mistakes and large mistakes. In addition, participants articulated a preference for advising a colleague before reporting a mistake. Participants who worked in governmental hospital pharmacies indicated that their institutions had flexible policies that encourage pharmacists to disclose errors. One participant said,
I work in the hospital as a medication safety officer, so we have the culture of medication errors. We give the wrongdoer a report written in bold at the top of the page, no blame no punishment, and the idea of this report is to improve the work and make sure that the error did not happen again. Of course, the report does not contain the name of the one who wrote the report. This has helped us during the past three years, as it has high transparency in any error that is documented. This culture, thank God, exists and has a high level of secrecy and transparency. [Participant No. 7]
Theme 2: Autonomy
Although this theme overlaps with others, we have chosen to focus on it separately because of its importance and its prominence in many international codes of ethics. Autonomy relates to the right of patients to make their own medical decisions without being subjected to undue influence or deception. We asked participants about coercing patients to take certain prescriptions out of a desire to help the patient; they all stated that this was not a practice at their place of employment. However, based on the participants’ statements, we discovered that some pharmacists engage in actions that violate the concept of the patient’s autonomy indirectly, such as deceiving patients by prescribing medications or products they do not require (cross-selling and upselling).
Theme 3: Justice
Justice was a recurring theme in some participants’ definitions of pharmacy ethics; as one of them said,
In general, the ethics of the pharmacist’s profession, is about treating patients with justice and equality. [Participant No. 1]
Additionally, several participants mentioned some ethical dilemmas concerning justice, which were captured by two codes: the first is “wasta,” which in Arabic means giving preference to a relative or friend over others when providing services, and the second is related—giving preference to the elderly over others when providing services. Regarding wasta, several participants said that it is a recurring issue in pharmacies, resulting in injustice to individuals who need service. According to one of the participants,
The society in which we live is a tribal society, and the biggest problem we face is the wasta, which takes many years to be resolved. [Participant No. 7]
The participants’ perspectives on prioritizing the elderly over others varied. Some did not view this issue as a problem because of cultural and societal respect for the elderly; as one participant stated,
But to be honest, respecting and appreciating the elderly people is a distinctive feature in our society, as it is most likely that they offer it. [Participant No. 15]
Some participants agreed that an intermediary action, such as getting permission from those in line ahead of the elderly or sending someone to assist them, would be more suitable One participant said,
The correct response is that I ask permission from the people who are waiting. If everyone cooperates, then I will serve the elderly people, but some waiting people say I want to preserve my right, I have my time. In this case, I will direct another pharmacist to take care of this person. It is assumed that there will be a special area to take care of these cases so that he will go directly to them, and this is the safest solution. [Participant No. 11]
One of the participants shared a story of what happened when he introduced some elderly people to one of the women in the queue, which made her complain about the pharmacist; this participant said,
Honestly, I used to put older people ahead of others until I faced an incident. One time, I prioritized an old woman in front of a young girl, so the girl got upset and created chaos in the place, and she filed a complaint against me, and said: We are in the era of equality between men and women, but praise be to God, the matter was resolved in the end. In general, after that, I repented. [Participant No. 14]
Theme 4: Confidentiality
The theme of patient confidentiality was mentioned by some participants in their definition of pharmacy ethics; one of them said about his view on pharmacy ethics,
These are many things. One of the most important things is to maintain the confidentiality of patients. [Participant No. 8]
Additionally, the issue of patient confidentiality arose when participants discussed their ethical dilemmas, and this theme is summarized in two codes: the first is that some pharmacists speak to the patient loudly enough to reveal the patient’s private information to other patients, and the second is disclosing the patient’s information to relatives without permission.
Although most participants stated that the problem of speaking to a patient loudly enough to be overheard is not widespread, some acknowledged the existence of this problem as a result of the limited space in the pharmacy. In addition, some participants noted that some patients feel embarrassed when asking for erectile dysfunction medications or pregnancy tests (see Supplementary Table 1), which puts pharmacists in a difficult position; close quarters in the pharmacy make it impossible for the pharmacist to speak privately with the patient. One participant said,
There are many patients who are ashamed to dispense some medicines to the point that they call me in the corner of the pharmacy especially when they prescribed sexual medicines or even a pregnancy test for women. [Participant No. 14]
Most participants stated that it was uncommon and unethical to disclose patients’ information to family or the rest of the medical team even when believing that such disclosure would be in the patient’s best interest, with some exceptions; for example, some participants believed it was ethical to disclose some information to the patient’s family if the discussion was scientific. This participant said about disclosing patients’ information,
This might happen if it was in a scientific context (like a scientific discussion with the relatives regarding their loved ones). However, I do not remember that I told any relatives inappropriate information about the patient. [Participant No. 2]
Theme 5: Veracity
Several participants noted this theme while defining pharmacy ethics, and they articulated it using the term “honesty”; one of them defined pharmacy ethics as
The instinctive qualities that pharmacists should have such as good character, honesty, and honesty with patients. [Participant No. 10]
Concerning the ethical dilemmas associated with this theme, only one code was extracted: concealing critical information about the patient while claiming that doing so is in the patient’s best interest. Some participants believed it was acceptable to withhold information from the patient, particularly about the adverse effects of a medication, so that the patient would take it without hesitation. One participant said,
There are times when we hide some information from our patients. But while he didn’t know about some things, I must give him other information so that he won’t be hurt by me not giving him this information. For example, if I told a patient to take immunosuppressive drugs, and I knew that the patient who I told this advice could leave the drug that could cause him to have second problems, I might have to hide some information and give him another piece of advice to avoid the causes of infection. [Participant No. 7]
As a compromise, several participants suggested that rather than withholding information from patients, medical information should be reworded in such a way that the patient might accept it without feeling threatened; as one participant said,
We never hide the information, but we choose a better way to deliver it. For example, instead of saying that this medicine can cause bleeding in the brain, I would say if you feel a headache, see the doctor. [Participant No. 9]
Theme 6: Communication Skills
Communication skills were a common theme for many participants when they defined pharmacy ethics. One of them defined pharmacy ethics as follows:
“ … good communication with the patient, patience, and compassion.” [Participant No. 3]
Under this thematic heading, three ethical dilemmas were identified: lack of colleagues’ cooperation, lack of patience, and patients’ lack of reasonability. One participant complained,
Negative feedback and destructive comments from some colleagues. This included unwanted competition, blameworthy competition, lack of cooperation, as well as personal problems. Also, some colleagues did not change their opinions, even if they are not right and they didn’t allow even to discuss their mistakes. [Participant No. 2]
Additionally, several participants indicated that some patients displayed a poor sense of responsibility while interacting with pharmacists. As this participant said,
“Patients may lack the sense of responsibility and appreciation; we are human beings, not machines. The pharmacy is not a grocery store.” [Participant No. 11]
Theme 7: Sincerity and Religion
Not surprisingly, religion played a significant role in several participants’ notions of pharmacy ethics, since the Islamic religion serves as the foundation for ethics and effective patient care in Saudi Arabia. One participant defined pharmacy ethics as
“Fear of God above all things, and not selling the people drugs beyond their financial capabilities.” [Participant No. 14]
Additionally, many of the ethical dilemmas described by participants include refusing to dispense medications that their religion forbids them from using, such as narcotics, medications containing alcohol or pork derivatives, hormonal drugs, or abortion-inducing medications. One participant said,
But like abortion medicines, I reject to dispense them. If there is a prescription, I will contact the doctor. For example, there are some medicines that are dissolved in alcohol. We, as Muslims, may take these medicine out of necessity, but we should inform the patient that they contain alcohol. For example, there are cough medicines that dissolved in elixir, the patient should know about it. [Participant No. 9]
Another participant said,
Here is a drug like gabapentin that young people use a lot for bad purposes. Sometimes I refuse to dispense it because I fear god. I know that the person in front of me does not use it for a legal purpose, even if he has a prescription. From time to time, the Ministry of Health sends a fake patient from them to test how you act, for example if you dispense antibiotics without a prescription or something else, and they will have fines if you do not pass the test. [Participant No. 14]
Theme 8: Law
Few participants viewed any of the illegal issues they confronted in practice, such as dispensing medications without a prescription, to be ethical challenges. One participant said the most prevalent ethical dilemma in his workplace was as follows:
“Requesting some drugs without prescriptions such as antibiotics and narcotics.” [Participant No. 4]
Discussion
Qualitative research is a branch of investigation that crosses disciplinary boundaries and topics.12 In most cases, qualitative approaches are employed to answer research questions that are discovery-oriented, descriptive, and exploratory in character, among other things. To gain a comprehensive understanding of human behavior and the factors influencing it, qualitative researchers conduct in-depth interviews. Various forms of conduct might be influenced by strongly held beliefs, personal viewpoints, life experiences, and the environment in which one operates.12 In contrast to quantitative designs, which include hypotheses stated at the outset of the investigation whose truth can be tested statistically, qualitative research is flexible; the researcher enters the world of the subject without preconceived notions.12 This research employed a qualitative approach to understand the ethical dilemmas confronting pharmacists in Saudi Arabia’s Asir area. Eight themes and eighteen codes were extracted from this study.
The existence of a centralized healthcare system in Saudi Arabia’s culturally varied population may raise a number of ethical concerns. Thus, the results of this research are critical in demonstrating that ethical problem-solving is an integral element of pharmacists’ “job descriptions”.13 However, it is already well established that ethics plays a vital role in the healthcare system.14 Our research discovered that most ethical concerns involve the connection between pharmacist and patient. This is unsurprising, given that pharmacists are accountable for helping patients achieve favorable health outcomes, which compels them to interact with patients regularly. We discovered that most ethical difficulties encountered by pharmacists are connected to the four ethical principles defined by Beauchamp and Childress, which have significantly influenced the medical field.15 These four principles are beneficence, non-maleficence, autonomy, and justice.15
Regarding the principles of beneficence and non-maleficence, this study discovered that a lack of patient counseling and a lack of sufficient clinical knowledge to deliver acceptable service to the patient are two of the most common ethical difficulties encountered by pharmacists. This phenomenon has been observed in earlier research conducted in other countries,16,17 and it results from time and job pressures that prevent the pharmacist from spending enough time counseling the patient.17,18 Additionally, because some patients may not be aware of the existence of patient counseling, it is easier for pharmacists to disregard it; patients must be educated about their rights to proper medical care.19 Previous research has shown that one of the primary reasons why patients fail to adhere to their prescribed drug regimens is that they misunderstand the value of the drugs, owing to the pharmacists’ failure to counsel them.20 Thus, it is vital to educate pharmacists on the critical nature of this patient counseling and its significant influence on the patient’s health, as well as to expand the number of pharmacists in hospitals and community pharmacies to ensure that pharmacists have sufficient time to counsel patients.21 Another solution is automatic dispensing devices, which may save the pharmacist’s time and make it available to consult patients, but the effectiveness of these devices is still questionable.22
The expansion of cross-selling and upselling in community pharmacy, indicated by several participants, attracts our attention under the themes of beneficence and non-maleficence. This phenomenon has been observed in other countries,23 but our studies have established for the first time its existence in Saudi Arabia. This phenomenon in our study exists only in community pharmacies in Saudi Arabia and pharmacies in private hospitals due to its commercial nature, unlike pharmacies of government hospitals supported by the state. Cultural attitudes that treat the patient as an object to be exploited stem from the “liquid modernity” described by the Polish thinker Zygmunt Baumann.24 Because the global market currently controls many enterprises and institutions, it is hard to reconcile the desire to provide patients the service they deserve with the financial motives driving community pharmacy chains.25
From an ethical standpoint, the basic motive for morality has evolved throughout time. Throughout the Confessions of St. Augustine, for example, theological motivations provided the driving force for ethics in the European Middle Ages.26 Thomas Aquinas eventually integrated reason and logic into ethics;27 Immanuel Kant then built a new moral framework based entirely on reason.28 In today’s world, however, Jeremy Bentham’s utilitarianism is prominent, and it is used by capitalists to argue that the greatest utility is money and technological growth, without regard for ethics or moral fundamentals.29 This consumerist perspective of the patient, which undermines the whole healthcare system, highlights the need to reconsider the relationship between healthcare providers and patients to replace the consumerist vision with a human one. However, such a project would require a significant overhaul of the global cultural and economic system, which makes us less optimistic.30
The participants also discussed some ethical dilemmas related to the principle of justice, and among the most prominent of those was the phenomenon of wasta, which means preferring relatives or friends over those more deserving of service. Much prior research has shown that wasta is widespread in Saudi Arabia and the Middle East when it comes to delivering healthcare.31,32 The most obvious reason for the spread of this phenomenon appears to be the huge impact of tribal society in the Middle East, as well as strong family bonds, which make health practitioners feel obligated to serve relatives and family first, even if it means delaying service to those who need it more.33 This embedded tribalism in the Middle East has been accompanied by a loss of a pragmatic sense of serious work culture, which characterizes cultures that emphasize industrial development and elevate the role of work at the expense of family and tribal relationships.34
Additionally, the participants debated some ethical challenges involving the veracity principle. The only dilemma mentioned by the participants in this principle was hiding some health information from the patient with the intention of benefiting the patients, or to inform his/her relatives instead of the patient him/herself, in order for the patient to complete the treatment plan. In some cultures, a serious medical problem affecting an elderly woman should be discussed with the mother’s eldest adult male child rather than with the patient.35 This would not be considered ethical behavior in the United States, since such discussions without the patient’s consent are prohibited by law.35 There have been no previous studies in Saudi Arabia on this subject or on whether it is acceptable to conceal information from the patient for his benefit, yet our study discovered a contradiction in pharmacists’ comments on this subject, necessitating further research.
Finally, one of the most important moral motives of the participants in our study was the Islamic religion. Religious motives manifested in almost all participants’ refusal to engage in practices that were contrary to their religion, like dispensing medicines they believed were prohibited by Islam, such as medicines containing alcohol or narcotics. Prior studies conducted in Islamic countries have similarly demonstrated the significance of religion in forming moral frameworks in conservative nations like Saudi Arabia.36,37 This vision reminds us of the importance of religion in shaping ethics and that the materialistic globalization that is sweeping the world is one of the reasons for the detraction of religion, making the definition of ethics more complex and subject to personal whims controlled by companies and individuals.38
This research has several strengths; it is the first to use qualitative methods to examine pharmacy ethics and the most prevalent dilemmas confronting Saudi pharmacists. This study provided many ideas that may be validated in further quantitative investigations. Also, the inclusion of community pharmacists and hospital pharmacists broadens the scope of the findings, even if the qualitative method is unconcerned with generalizability.39
There are limitations to the study, however—most notably, the small number of participants. While the number of participants in this research is considered reasonable for a qualitative study,39 we aimed for a larger sample but were unable to obtain one for several reasons. The primary reason was our concern that some participants would withhold information out of fear of retribution by their employer. Although we emphasized the confidentiality of all stages of the process, a certain number of potential participants declined. The concept of qualitative research and the use of voice recorders in personal interviews is not widespread in Saudi society, especially within the health community, which may explain the reluctance of some pharmacists to participate; if qualitative research were more familiar within the culture, we suspect we would not encounter this difficulty.
Conclusion
Our findings showed the most common ethical dilemmas faced by pharmacists in Saudi Arabia facilitating the formulation of an ethical code for pharmacists that help pharmacists to overcome these dilemmas. Additionally, community and hospital pharmacists need formal training in ethics, as well as support regarding where to find and analyze ethical guidelines before making a recommendation or presenting information to their patients. Future quantitative investigations are necessary to validate and generalize from the present study’s results and to distinguish between the ethical dilemmas faced by the community pharmacist compared to those faced by the hospital pharmacist.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Scheinman SJ, Fleming P, Niotis K. Oath taking at US and Canadian medical school ceremonies: historical perspectives, current practices, and future considerations. Acad Med. 2018;93:1301–1306. doi:10.1097/ACM.0000000000002097
2. Chaar B. Ethical dilemmas: are you across the EHC guidelines? Aust Pharm. 2016;35:72.
3. Popattia A, Winch S, La Caze A. Ethical responsibilities of pharmacists when selling complementary medicines: a systematic review. Int J Pharm Pract. 2018;26:93–103. doi:10.1111/ijpp.12425
4. Parsa-Parsi R. Walter. The revised declaration of Geneva: a modern-day physician’s pledge. JAMA. 2018;318:1971–1972. doi:10.1001/jama.2017.16230
5. Ethics of Health practitioners [webpage on the Internet]. published in January 20, Riyadh, 2019. Available from: https://www.scfhs.org.sa/Media/DigitalLibrary/DocumentLibrary/OtherPublications/Documents/%D8%A3%D8%AE%D9%84%D8%A7%D9%82%D9%8A%D8%A7%D8%AA%20%D8%A7%D9%84%D9%85%D9%85%D8%A7%D8%B1%D8%B3%20%D8%A7%D9%84%D8%B5%D8%AD%D9%8A.pdf. Accessed May 2, 2022.
6. Al Yousuf M, Akerele TM, Al Mazrou YY. Organization of the Saudi health system. East Mediterr Health J. 2002;8:645–653. doi:10.26719/2002.8.4-5.645
7. Alshahrani SA, Alsadiq AJ. Economic growth and government spending in Saudi Arabia: an empirical investigation. IMF Working Papers; 2014:14.
8. Al-Arifi MN. Patients’ perception, views and satisfaction with pharmacists’ role as health care provider in community pharmacy setting at Riyadh, Saudi Arabia. Saudi Pharm J. 2012;20:323–330. doi:10.1016/j.jsps.2012.05.007
9. Al-Arifi MN. Community pharmacist perception and attitude toward ethical issues at community pharmacy setting in central Saudi Arabia. Saudi Pharm J. 2014;22:315–325. doi:10.1016/j.jsps.2013.08.003
10. Guarte JM, Barrios EB. Estimation under purposive sampling. Commun Stat Simul Comput 2006;35(2):277–284. doi:10.1080/03610910600591610
11. Fram SM. The constant comparative analysis method outside of grounded theory. Qual Rep. 2013;18:1.
12. Hell F, Taha Y, Hinz G, et al. Graph convolutional neural network for a pharmacy cross-selling recommender system. Eur J Educ. 2013;48:311–325.
13. Al-Ahmadi H, Roland M. Quality of primary health care in Saudi Arabia: a comprehensive review. Int J Qual Health Care. 2005;17:331–346. doi:10.1093/intqhc/mzi046
14. Alkabba AF, Hussein GA, Albar A, et al. The major medical ethical challenges facing the public and healthcare providers in Saudi Arabia. J Family Community Med. 2012;19(1):1. doi:10.4103/2230-8229.94003
15. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. New York, NY, USA: Oxford University Press; 2001.
16. Resnik DB, Ranelli PL, Resnik SP. The conflict between ethics and business in community pharmacy: what about patient counseling? J Bus Ethics. 2002;28:179–186. doi:10.1023/A:1006280300427
17. Salari P, Namazi H, Abdollahi M, et al. Code of ethics for the national pharmaceutical system: codifying and compilation. J Res Med Sci. 2013;18:442.
18. Agomo CO, Ogunleye J, Portlock J. A survey to identify barriers in the public health role of community pharmacists. J Pharm Health Serv Res. 2016;7:253–261. doi:10.1111/jphs.12153
19. Albekairy AM. Pharmacists’ perceived barriers to patient counseling. J Appl Pharm Sci. 2014;4:70.
20. Levensky ER, O’Donohue WT. Patient adherence and nonadherence to treatments. In: Levensky ER, O’Donohue WT, editors. Promoting Treatment Adherence: A Practical Handbook for Health Care Providers. New York, NY, USA: Sage Publications; 2006:3–14.
21. Svarstad BL, Bultman DC, Mount JK. Patient counseling provided in community pharmacies: effects of state regulation, pharmacist age, and busyness. J Am Pharm Assoc. 2004;44:22–29. doi:10.1331/154434504322713192
22. AlShahrani S, Al Fadhli N, ALZahrani E, et al. Role of automated dispensing machines: an emerging and efficient technology in Saudi Arabia. J Health Inform Dev Ctries. 2020;14(2):45.
23. Sävlind C. Customers’ perceptions of the re-regulated pharmacy market: a qualitative study of the views of Stockholm customers five years after the re-regulation process; 2015.
24. Bauman Z. Liquid Modernity. New York, NY, USA: John Wiley & Sons; 2013.
25. Wingfield J, Bissell P, Anderson C. The scope of pharmacy ethics—an evaluation of the international research literature, 1990–2002. Soc Sci Med. 2004;58:2383–2396. doi:10.1016/j.socscimed.2003.09.003
26. Teske RJ. Book review: Augustine the reader: meditation, self-knowledge, and the ethics of interpretation; 1996:744–746.
27. Gallagher DM. Person and ethics in Thomas Aquinas. Acta Philos. 1995;4:51–71.
28. Kant I. Kant: The Metaphysics of Morals. Cambridge, UK: Cambridge University Press; 2017.
29. Stark W. Liberty and equality or: Jeremy Bentham as an economist. Econ J. 1941;51:56–79. doi:10.2307/2225646
30. Hallaq W. Reforming Modernity: Ethics and the New Human in the Philosophy of Abdurrahman Taha. New York, US: Columbia University Press; 2019:77–118.
31. Dobia AM, Ryan KM, BaHammam AS, et al. The use of hypnotics for insomnia disorder in Saudi Arabia: a survey of patients’ experiences and perceptions. Sleep Vigilance. 2021;5:235–244. doi:10.1007/s41782-021-00151-7
32. Rubinstein RA. Breaking the bureaucracy: drug registration and neocolonial relations in Egypt. Soc Sci Med. 1998;46:1487–1494. doi:10.1016/S0277-9536(97)10147-2
33. Marktanner M, Wilson M. Wasta in the Arab world: an overview. In: Handbook on the Geographies of Corruption. Edward Elgar Publishing; 2018.
34. Koburtay T, Syed J, Haloub R. Implications of religion, culture, and legislation for gender equality at work: qualitative insights from Jordan. J Bus Ethics. 2020;164(3):421–436. doi:10.1007/s10551-018-4036-6
35. Amer AB. The ethics of veracity and it is importance in the medical ethics. Open J Nurs. 2019;9(2):194–198. doi:10.4236/ojn.2019.92019
36. Alsharif NZ, Khanfar NM, Brennan LF, et al. Cultural sensitivity and global pharmacy engagement in the Arab world. Amer J Pharm Educ. 2019;83:45.
37. Elkalmi RM, Alkoudmani RM, Elsayed TM, et al. Effect of religious beliefs on the smoking behaviour of university students: quantitative findings from Malaysia. J Relig Health. 2016;55:1869–1875. doi:10.1007/s10943-015-0136-0
38. Cahill LS. Theological Bioethics: Participation, Justice, and Change. Washington, DC, USA: Georgetown University Press; 2005.
39. Lewis S. Qualitative inquiry and research design: choosing among five approaches. Health Promot Pract. 2015;16:473–475. doi:10.1177/1524839915580941
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.