")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
The Collaboration Compass: A Preliminary Model for Navigating Collaborative Practice
Authors Turnbull LL , Carr SM
Received 6 April 2020
Accepted for publication 6 July 2020
Published 7 October 2020 Volume 2020:13 Pages 1107—1120
DOI https://doi.org/10.2147/JMDH.S257160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lindy L Turnbull,1 Susan M Carr2
1Faculty of Health Sciences and Wellbeing, University of Sunderland, Sunderland, UK; 2Faculty of Health & Life Sciences, Northumbria University, Newcastle upon Tyne, UK
Correspondence: Lindy L Turnbull
Faculty of Health Sciences and Wellbeing, University of Sunderland, Helen McArdle House, Chester Road, Sunderland SR1 3SD, UK
Email [email protected]
Purpose: To investigate the meaning and manifestation of collaboration in practice including the experience and outcomes for patients and professionals.
Methods: Grounded theory was used to investigate collaboration in an integrated outpatient parenteral antimicrobial therapy (OPAT) service. The sample consisted of staff and patients with experience of OPAT. Interviews and focus groups were used to generate data, and grounded theory methods were used to progress the study through constant comparative analysis and theoretical sampling to data saturation. Coding, categorizing, and techniques of situational analysis were used to analyze data and develop theory.
Results: The relationship between the influences in the situation and the interaction which takes place between individuals was found to produce four different types of collaboration: developing, maintaining, limiting, and disrupting collaboration. The collaboration compass model was developed to illustrate and aid interactive navigation of collaborative situations.
Discussion: The findings present the complexity of practice, and a model to explain the multiple influences and interaction which shape collaboration. In this model, patients are part of collaboration, and this ensures that patients’ views and experiences, as well as those of professionals, are included and represented in knowledge about collaboration. This adds a new dimension to existing interprofessional presentations of collaborative practice and examines collaboration as it is operationalized in practice and co-constructed between patients and professionals during day to day practice.
Keywords: collaboration, integrated services, service development, patient participation, co-produced care, grounded theory
Introduction
Working with others is an integral part of coordinated health and social care systems delivering individualized, person-centered, and co-produced care.1,2 The need to collaborate has been repeatedly highlighted in national and international policy.3–6 It is seen as a key part of managing care7 and central to sustaining and transforming the NHS.8 However, despite this inundation in policy directives, there are significant gaps in the knowledge base to guide implementation.
Although patient care is identified as the focus for collaborative working in health and care-related literature, there is little representation of patients in studies, and a lack of explicit patient perspectives in the literature.9 Although collaboration is seen as desirable by patients,10 there are differing perceptions and expectations of collaboration between patients and healthcare staff.11 While the benefits and challenges of collaboration between professionals are well rehearsed,12 there is limited evidence of how collaboration relates to patient outcomes13 or how it impacts on patient care.14
This paper presents doctoral research focused on patient and professional exploration of collaboration as it is experienced in the delivery of integrated care. This moves beyond looking at how patients are involved in their care, to examine the extent to which they are able to participate in collaboration and influence their care within healthcare environments. Viewing patients as part of collaboration expands existing interprofessional models by including the extent of co-construction taking place. Exploring what shapes the ability of individuals to collaborate provides insight into how situational factors influence the action and interaction of patients and professionals and how this impacts on the experience and outcomes of care.
The substantial collaboration literature base presents a diversity of interchangeable terms, definitions, and applications related to multiple disciplines. The consequence of this diversity and ambiguity is a lack of clarity about what collaboration actually means in practice. Healthcare definitions have developed to reflect the changing expectations of collaboration, and range from the simple idea of “a mechanism by which a new negotiated order emerges among a set of stakeholders”15 to far more complex definitions which involve multidisciplinary working in processes arrived at through interprofessional education.16 One more recent definition stands alone in including the client as part of collaboration, and this more inclusive view of collaboration reflects the wider aim for greater patient involvement in care:17,18
a partnership between a team of healthcare professionals and a client in a participatory, collaborative and coordinated approach to share decision making around health and social issues19
Despite the multiple definitions and policy drivers to collaborate, there is little to guide the operationalization of collaborative practice and often definitions do not represent the complexity of practice situations. This complexity has been regarded as a hidden aspect of collaborative practice,15,20 and reviews12,21 suggest that we have limited understanding of the complex relationships involved. There is a need for greater understanding of how collaboration in complex healthcare situations is achieved, and how it contributes to the experience and outcomes of care.
The research reported here was inspired by a collaborative project to deliver intravenous antibiotics in patient homes, which offered an opportunity to co-ordinate care and develop new approaches to delivering treatment. There are many different models for the structure of OPAT services ranging from the outpatient departments to community based facilities with visiting nurses and community clinics.22 Each model has advantages and disadvantages and the type of service model established in any particular area usually depends on the local needs and drivers for development of an OPAT service. OPAT models which offer both acute and community services are rare in the UK23 and highlights the barriers, which arise from cultural and organizational situations and a general lack of willingness to work across organizational boundaries. This new Outpatient Parenteral Antimicrobial Therapy (OPAT) project presented a number of challenges and barriers in establishing new ways of working between acute and community departments in an NHS Trust. This experience raised the main research question: what is the meaning of collaboration and how is it manifested in a domiciliary OPAT service? A number of sub questions were also developed to allow exploration of the factors which influence individual and collective interaction as well as the consequences of collaboration. Although a new OPAT service provided the inspiration and setting for this study, the focus of investigation was the collaborative practice involved in day-to-day care delivery, rather than the medicines management or treatment aspects of care delivery.
A detailed interpretivist situational analysis24 revealed a substantive theory called Interactive Navigation which explained the complex and dynamic relationships found in the situation. The Collaboration Compass model was developed to illustrate the theory, to aid understanding of collaboration, and to act as a tool to support collaboration in practice. This article provides a brief summary of the study and presents the Collaboration Compass Model as a way to navigate situations and direct collaborative outcomes in practice. This article therefore has the potential to benefit anyone involved in planning, implementing, or evaluating collaboration in practice.
Methods
Study Design
A social constructionist approach to grounded theory24,25 was used to investigate collaboration in the situation of OPAT care delivery. The methods used were designed to capture detailed accounts of collaboration and to join these perspectives together to develop understanding of the collective aspects of collaboration in the healthcare practice situation. The sample consisted of staff within acute and community services who deliver OPAT, and patients who have experience of receiving treatment. Interviews and focus groups were used to generate data. Grounded theory methods were used to progress the study through constant comparative analysis and theoretical sampling, until a point of data saturation, and then on to theory development.
Study Population
The sample consisted of the main group of people involved in the OPAT collaboration associated with specific patients and their designated treatment. The circle of care approach26 was adapted to map collaborative activity across each patient’s circle of care associated with OPAT. Kitson et al26 found the number of people involved across the continuum of care related to medicines varies with the circumstances for each patient, but determine that the numbers of roles involved in a medicines management circle of care are between five and 11, including the patient. This was used as a guide for the number of roles which would be appropriate to be included in the sample. Ten roles were identified as being involved in the care situations and the sample contained eight roles, which was consistent with numbers identified by Kitson et al.26 The exact number of participants was determined by the patients’ care situations, theoretical sampling, and responses from potential participants. Although the sample had a large proportion of nurses, this was representative of the professionals involved in the delivery of OPAT and so the sample was representative of practice as experienced by each patient participant.
The twenty-four participants were three patients and 15 district and community nurses from two teams, one OPAT specialist nurse, one pharmacist, and one microbiologist involved in their care (Table 1). A purposive sampling strategy was used to identify the patients who were each experiencing different types and lengths of OPAT treatment. Theoretical sampling27,28 was then used as analysis of data from the first participants identified concepts for exploration and a number of professionals involved in collaboration with the patient. Theoretical sampling continued as analysis of data from each participant informed the ongoing recruitment of participants to follow collaborative interactions and explore conceptual ideas29 in the developing theory.30
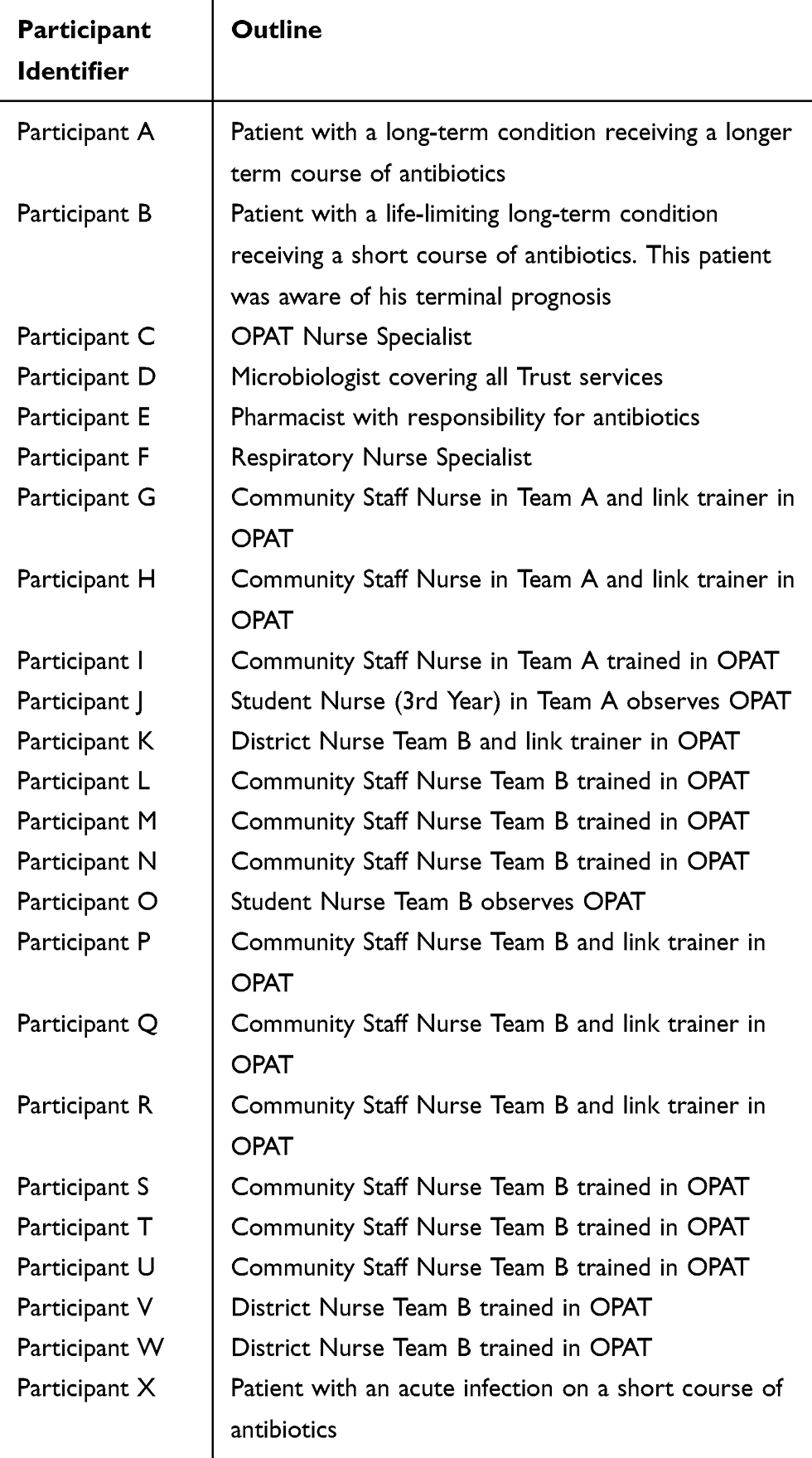 |
Table 1 Participant Details |
Data Collection
Data was generated over an 18-month period, through eight face-to-face, semi-structured interviews and two focus groups, which were all audio recorded and transcribed. An OPAT nurse acted as gatekeeper inside the NHS Trust to help identify potential participants, provide them with the appropriate participant information, and seek consent for the researcher to follow-up with telephone or email to discuss the study. Interviews were arranged at the convenience of participants. Patient participants were interviewed in their homes, while other interviews and focus groups took place in NHS property during office hours. Focus groups were used to generate data from members of two district nursing teams. Multiple interviews with individual nurses were not possible due to the workload of the team and the potential impact on patient care. Both district nursing teams chose focus groups at a time to suit the team workload. Prior to interviewing all participants were reminded of the information provided in the information sheet, given the opportunity to ask questions before reading and signing the research consent form.
The researcher conducted all interviews and focus groups according to interview protocols, which were developed to guide semi-structured conversational interviews lasting between 45 minutes to 1 hour and 10 minutes. The protocols provided sufficient flexibility within the interviews and focus groups to allow development of discussion, which explored participant experiences, perceptions, and opinions of OPAT, and also facilitated exploration of developing theoretical analysis. Participants were asked to describe their experiences of OPAT and questions explored roles and the way people worked. Participants shared positive and negative experiences openly and the researcher used more probing questions to explore the situation and aspects of collaboration.
Data Analysis
Data analysis was undertaken using a combination of grounded theory analytical processes, which include initial and focused coding, categorizing,31,32 and the development of theoretical concepts.31 A range of situational analysis tools25 were used throughout the process to promote greater depth of analysis. The aim of analysis was to make sense of the data, to analyze individual and group perspectives, and to interpret the collective interaction within the situation of collaboration. The analytical process focussed first on the perspectives of individuals and groups and then combined these perspectives to analyze the collaborative situation they shared.
Each transcript was coded using a line-by-line approach to ascribe a concept to each segment of data. Each code was compared and relational maps24 were used to explore the relationships between them. Codes were then joined together into categories, which were mapped using MindGenius software (Version updates 3, 4, and 5) to create a map for each participant or group of participants. At the point of data saturation, when no new categories emerged, the codes and categories from each participant map were compared and combined to produce a situational map.24
The situational map framed the broader collaborative situation by merging analyzed data from individual participants within the situation. Combining each participant’s categorized data provided a detailed picture of all their different perspectives and experiences of interaction in the shared situation. Social world mapping techniques24 were then used to trace social activity and consider social action within the situation of study. This type of mapping added to consideration of individual micro perspectives and the more macro organizational issues to highlight a meso area of social interaction taking place. Positional Mapping techniques were also used to facilitate understanding of the issues within the data. These maps did not represent individuals or groups, but plotted the issues of focus. Each category was mapped against each of the others to plot the issues arising in the data and explored the interaction taking place in relation to different combinations of influences.
The third patient participant was identified following analysis of the patient role in collaboration and the gatekeeper was asked to identify a younger patient on a shorter course of treatment in order to check the developing theory with a patient in a different situation from those experienced by the first two patient participants. This was a valuable aspect of analysis to check the theory in an additional treatment situation. This also provided assurance of data saturation as no new categories emerged during analysis of this additional data.
The analytical process identified nine situational categories grouped into two theoretical categories which form the substantive theory of Interactive Navigation which interprets the complex relationships revealed during analysis of the collaborative situation. The final conceptual diagram produced during analysis demonstrates these relationships in a theoretical model called the Collaboration Compass.
Ethical Approval
The University Ethics Committee, NHS Ethics Committee, and NHS Trust Research and Development Department all approved the study and granted access to patients and staff within the situation of OPAT.
Results
Two theoretical categories emerged from data analysis (Figure 1); situational coordinates and interactive mechanisms. Participants expressed a number of interactive mechanisms (trusting, rehearsing, coordinating, and communicating) which were influenced by a range of situational co-ordinates (goals, limits, certainty, uncertainty, and power). Combination of these theoretical categories represents the mechanisms and influences found in the individual perspectives, relationships, and situation of collaboration in OPAT.
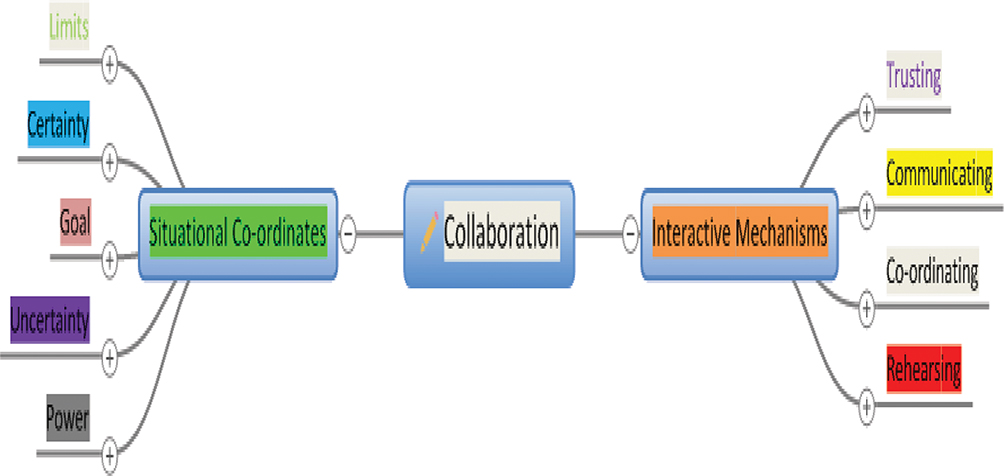 |
Figure 1 Theoretical categories and sub-categories represent the mechanisms of interaction used in collaboration and the co-ordinates within the situation which influence how interaction is used. |
The Collaboration Compass conceptual model (Figure 2) was developed as a tool to illustrate the navigation of influencing co-ordinates and the interaction used by participants to direct four types of collaboration. The model depicts collaboration as a navigational process with interactive mechanisms at the center of the compass and situational co-ordinates as cardinal points of direction in the situational landscape. The intermediate areas, between the four co-ordinates, represent the different types of collaboration found to be taking place. Interactive navigation takes place as co-ordinates orientate the situation and interactive mechanisms direct collaboration into the area which relates to the most influential co-ordinates. Power was found to be a dynamic influence within the situation with the ability to influence interactive mechanisms in each type of collaboration.
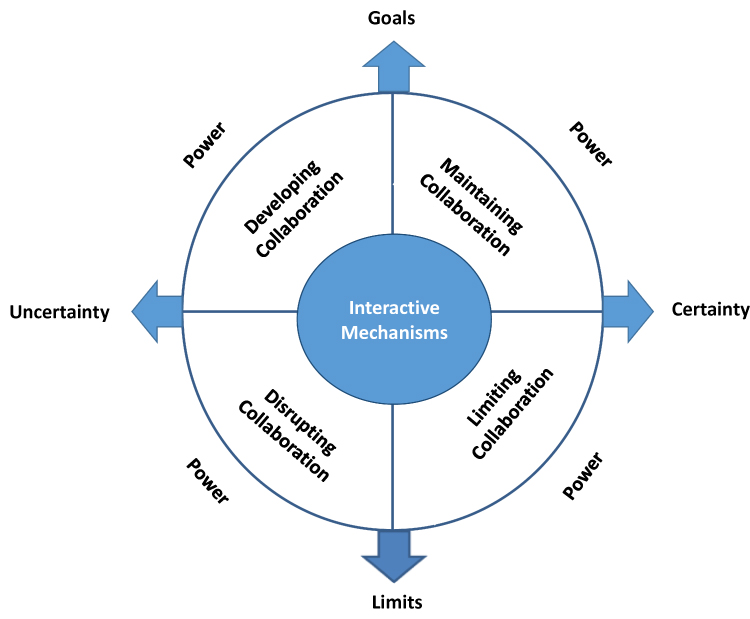 |
Figure 2 The Collaboration Compass Model depicts collaboration as a navigational process with interactive mechanisms at the center of the compass and situational co-ordinates as cardinal points of direction in the situational landscape and the different types of collaboration as areas between co-ordinates. Power is shown as a dynamic influence in each type of collaboration. |
The findings are presented below to illustrate how the Collaboration Compass was manifested in patient and professional interactions and experiences within the healthcare situation. The four areas of the Compass are presented, with the navigation of co-ordinates and interaction found to shape collaboration in each area.
Developing Collaboration
Developing collaboration was found to be orientated by the co-ordinates uncertainty and goals. Uncertainty about a new type of care or new relationship stimulated interaction to develop goals to be agreed. For patients the uncertainty was about new treatment or changes in health, and for one patient the uncertainty was about income and home life while he was in hospital. He was first to identify and communicate his goal:
X: I was in near enough 2 weeks and I needed to get back for work and we were moving (gestures to boxes in the room) so I asked if I could have it at home. They weren’t sure at first, but after a day or so the hospital put the line in and it was all good. (Participant X: transcript lines 20–23)
This intense interaction using communication, coordination, and trust was used in the development of collaborative relationships and rehearsal of working with others in new ways. Reciprocated communication of a shared goal promoted increased interaction and participants discussed rehearsal as learning from mistakes, sharing responsibility, and embedding new interaction into ways of working with shared co-ordination and trust. Rehearsal involved working together towards achieving the shared goal, and one participant discussed how communicating and learning from mistakes adapted existing systems to develop and embed new ways of working.
F: … the busier ambulatory care got the worse our patient experience was getting. So it went to a real low time when I think one patient spent 8 hours waiting for drugs … so I think at that point we realized we had to change … I worked quite closely with pharmacy to say look we have to do something different we can’t have this wait … so now I know downstairs in pharmacy there is always the equivalent of a week’s course. (Participant F: transcript lines 86–95)
The goal of delivering care and treatment in the patient’s home was easily agreed and, although patients and professionals all discuss some contribution to the coordination of people working together, it was the professionals who took on most of the coordination when collaboration was developing.
C: I guide them through the process and guide them to which information that they need to fill out and then how to fill out and then where to send that information on. I then erm contact the iv team, … then speak to the pharmacist team and the microbiology team, just to make sure that that antibiotic choice is OK for that patient and that that antibiotic choice is actually in the hospital and then I erm collaborate with the medical or surgical team. (Participant C: transcript, lines 6–12)
The extent to which the patients had power to make choices and be involved differed. One patient, who was receiving palliative treatment, was the most actively involved in developing collaboration as he and a range of professionals worked together towards the shared goal of his treatment at home. He discussed active involvement as he communicated with professionals to solve problems and build relationships in rehearsal of new procedures. He described developing trust and coordinating visits from different professionals for whom he had respect and was also comfortable to challenge. The other patients were far less involvement in developing collaboration, and their interpretation of patient and professional roles impacted on how they interacted:
X: I’m not involved. I’m here and I have the injections. Beyond asking for this I’m not involved. I’m not part of any decision-making, they do all that. I couldn’t do any of that. (Participant X: transcript lines 126–129)
Another patient acknowledged that past experiences and culture influence the way she interacts with some groups of professionals, and she associates professional roles with hierarchy, which hinders open communication:
A: I don’t know what it is, I think it’s because they’re doctors. erm and you think well they know what they‘re doing and maybe I’m being a bit cheeky. I suppose its cos I’m older and it was the way you were brought up … (Patient A: transcript 1, lines 217–219)
Collaboration was found to develop from uncertainty, and all interactive mechanisms were used as participants navigated away from uncertainty towards the goal shared by patients and professionals. Patients interpreted their role in collaboration in different ways. Two patients had minimal involvement in interaction and they drew a distinction between professionals and patients and identified themselves in a patient role. The third patient, who had a terminal diagnosis, took an active part in directing collaboration to achieve the shared goal.
Maintaining Collaboration
Collaboration could be maintained once a shared goal had been achieved and there was more certainty in the situation. This area of collaboration was orientated by the goals and certainty in the situation and interaction was based on coordination, communication, and trust. There was no rehearsal in this area as roles and responsibilities had been confirmed with clear plans in place for care delivery. There was no collaboration in this area for one patient as there was no certainty about treatment and uncertainty remained the most influential co-ordinate in her care. For the patients who were receiving a short course of antibiotics there was more certainty, but it was in the situation of the patient receiving palliative treatment where collaboration was maintained.
This patient’s palliative care involved recurring, short-term treatment which brought the certainty of routine. In addition to this, the patient was very open about the certainty of his terminal diagnosis and he communicated his deteriorating and limiting health:
B: (coughing and breathless) … every time I have a flare up I lose a little bit of lung, a bit of lung capacity. I noticed this time I’ve lost a lot, a lot of capacity. (Participant B: transcript lines 127–129)
The certainty of this patient’s condition, together with the short-term nature of his treatment and the inevitability of his deterioration, influenced the interaction which took place. Co-ordination emerged as the role of one professional (Nurse Specialist) who directed and facilitated to ensure that the goal of care at home was maintained:
F: I coordinate from here, the other guys know what to do and they will do it if I’m on holiday, but they’ll devolve it to me if I’m around which is sort of fair enough. I think it’s just you know the patient more, one, you become more confident with the patient type so erm you can sort of get a much better feel for how the patient’s going. (Participant F: transcript lines between, 77–80)
Knowledge of the patient’s condition influenced this one professional to take on co-ordination even though it involved extra work and responsibility:
I would hate to see that I hadn’t tried to do everything I could to improve my patients journey erm and if that means I work a few hours extra and if that means I put in a little bit more to coordinate care that’s what I do … You know I wouldn’t wanna be stuck in hospital for 2 weeks, and towards the end of life it’s even more important. (Participant F: transcript lines137–140 and 285–287)
By coordinating and communicating this professional maintained the goal and ensured the certainty in the situation, which also maintained trust with collaborators.
This area of collaboration is shaped by the goal and certainty in the situation. The use of coordination maintained the trust and communication required to maintain the goal. One professional was found to take on the role of coordinator, acting as a hub for communication with others, despite increased workload.
Limiting Collaboration
Collaboration was found to be limited when certainty about the situation combined with personal or professional limitations. All patients and professionals were found to have limitations in the situation. The way these limitations were communicated, and interpreted by others, influenced ongoing interaction, and had the potential to reduce communication and trust. No coordination was found in this area of collaboration. Communication and trust were found, which resulted in functional and effective treatment, but limited collaboration.
The influence of limitations was found to be dependent on the interpretation of their significance within the situation. For one patient there was certainty about the short course of treatment, but both the patient and professionals expressed limitations of time and workload. Interaction was adapted to accommodate both patient and professional limitations, and the patient traveled between professionals to communicate with them individually and one at a time, but there is no coordination role evident in this:
X: I asked for it and we arranged a time so I could still work. It has to fit in with their other patients and shifts and whatnot, but it works well. The only thing I’d change is going to hospital every couple of days to get blood results … I go to the GP’s and then get results at hospital; that could be a phone call, but I suppose he looks at me leg and hopefully it’s not for long this time. (Participant X: transcript lines 52–59)
Recognition, and communication, of a limitation was found to act as an influence on others to alter their interaction. Some professionals discussed their professional and organizational limitations, such as workload, lack of time or lack of resources, and they communicate these limits to others. They reduce their communication in the face of constraining professional demands. Community Staff Nurses discuss their workload limit:
Q: Once we had to say no to actually taking any more on didn’t we? Once we had a lot and massive staffing issues didn’t we? So we did get, I think, did we accept five, and then we kind of were like that’s our limit that we can do at the moment. (Participants Q: transcript lines 253–257)
Participants navigated the situation by interpreting the influence of limitations and considering the competing influence of other co-ordinates. This is evident in the care of the patient with the terminal condition. The limiting lack of staff was considered with the certainty of his terminal situation and short course of treatment. The certainty of terminal illness and the patient’s physical condition were interpreted as significant enough to redirect collaboration away from limiting factors. The influence of treatment at home, as the goal for a terminal patient, promoted the specialist nurse to navigate away from her professional limitations in order to maintain collaboration. She did this by taking on the co-ordination role despite her increased workload, and she discusses reducing her communication about wider OPAT service issues in order to coordinate for her patient:
F: So you know I can’t talk for anybody else and therefore my involvement with all those extra discussions, I sit back, as long as I don’t feel there’s going to be too much impact on what is delivered to my patient. (Participant F: transcript lines 234–236)
Although professionals expressed their limitations to others, patients did not always communicate their limiting factors for fear of judgment:
A: … you know, like when I had so much pain, sometimes you wondered oh did they think I’m just putting it on, and cos everybody says I look well and you know. (Patient A: transcript 1, lines 157–158)
This patient was also found to stay silent about limiting pain in order to fulfil the responsibilities of being a patient having the treatment at home:
A: … it’s not pleasant erm and it’s on me back, so it means I’m like in the car all that time erm and last time I went, getting parked was horrendous erm and then I’d have to go in and the MRI takes about 40 minutes to 50 minutes and I’m on me back all the time. Then I would have to get out, and get back in the car again, and travel home again you know erm. But if I’ve got to do that I will do it. (Patient A: transcript 2, lines 45–49)
Professionals clearly identified and communicated their own limitations within the situation. One professional described the interpretation of professional limitations:
E: There’s possibly some discussion … around erm how much they should get involved … the consultant for the patient wasn’t here, they were on holiday and the decision needed to be made as to whether to continue and there was no one to make it. So one kinda said It’s not my place, I’m not doing anything with this, and the other one said we can’t just do that and took the responsibility on … but then the other one argued that we shouldn’t be doing that and the responsibility shouldn’t lie with us, it should lie with the referring clinician if he’s not there then he should be delegating out. His team should review the patient … (Participant E: transcript lines 198–210)
Another professional discussed the impact such professional limits have on patients and other professionals as communication becomes one way and uncertainty increases:
C: … patients are left in the dark they don’t know what’s supposed to happen with them. They‘re told to report for a particular scan and they’re told to ring through erm for results and the physician at the other hospital will erm speak to them, but they never do and then they are left desperate knowing what’s, what’s meant to be happening with them. (Participant C: transcript lines 92–97)
Within this area, collaboration was found to be limited by the personal or professional limitations which exist when there is certainty about the requirements and roles within the situation. Interaction was limited and functional, with reduced communication and trust. Power within this area of collaboration related to the capability of individuals to communicate their limitations and influence others. The communication of the terminal illness had significance and influenced one professional to work beyond the limits of staff resources and contractual hours in order to direct collaboration away from limitations towards maintaining the shared goal.
Disrupting Collaboration
Collaboration was found to be disrupted when limitations and uncertainty were most influential in the situation. Uncertainty existed for many reasons, but when associated with restrictive limitations, it was found to disrupt interaction with loss of communication and trust. Some professionals were found to respond to restrictive limitations and uncertainty by ceasing to communicate. The lack of response and feedback impacted on trust and increased the uncertainty for others. Professionals reported disillusion in collaboration and patients experienced loss of confidence, anxiety, guilt, and fear as collaboration was disrupted.
Professionals responded to restrictive limitations in different ways, and while some individuals communicated their limits and continued to interact in a limited, but functional way, others reached limits and ceased to communicate, thereby increasing uncertainty and disrupting collaboration:
D: … we get a lot of feedback for any of the patients on the (names a team) ward a lot of communication whereas other conditions we don’t get anything back so it’s often they (consultants) only ever ring you back when it’s really gone wrong. (Participant E: transcript lines 172–180)
This lack of response or feedback produced uncertainty for other collaborators, which impacted on trust and, in turn, was perceived as a disrupting limiting factor by other collaborators, who may then also limit or cease interaction.
Prolonged limited collaboration or lack of response and feedback resulted in disillusion; a limiting factor which was disruptive and potentially destructive to collaboration:
C: … we are not getting any clinical responsibility erm really no information from them. We know that sometimes they see the occasional outpatient appointment but we don’t get any information directly from them, so it’s always a chasing up. Always having to leave messages with their secretaries always finding out they’re on holiday, always. (Participant C: transcript lines 81–85)
Lack of appreciation for limitations which had been communicated to others also produced disillusion and feelings of being taken for granted, which was expressed by one nurse:
F: I really got quite disillusioned by the whole OPAT thing and I was sitting in a meeting and we were discussing hours and who needed what hours … We’ve done it several times you know this was the latest round of it and I said I think I need … nursing time and I was told I didn’t. I was told categorically I did not need nursing time and I said well how do you work that out? (Participant F: transcript lines 296–301)
Becoming disillusioned had the potential to disrupt interaction; communication, trust, and co-ordination were all affected. One professional identified a shift in power and the capability to withdraw interaction and as the influence of limits and uncertainty within the situation are navigated:
F: … time for my team was absolutely discarded and we put by far the most patients through this programme … so there the power switches and you know the base of it switches and I was ready to walk at that point … I really was absolutely furious that there was no recognition of what we’d done. (Participant F: transcript lines between 309–319)
For one patient the situation quickly moved from being orientated by the goal of treatment to become orientated by the limitations of professionals, hospitals, and the increasing uncertainty resulting from reduced communication:
A: … so when I had me first MRI done at (name) they sent it erm, faxed it or whatever you do, across to, for them to have a look at it erm but I think it was the doctor … that decided erm the antibiotic to give me, mebbe this is where it’s all going wrong because I’m between two hospitals and each doctors waiting … The carry on I had before when I went to see him erm a week ago, a week on Wednesday erm I can understand now a little bit what was going on because he is sitting there waiting for (name) to tell him what to do. (Patient A: transcript 2, lines 54–62)
As collaboration became disrupted this patient recounted numerous examples of leaving messages, traveling to hospitals, wasted journeys, waiting to see professionals, and being re-directed to other professionals. She found herself communicating without response from others and attempting to coordinate, despite her limiting pain and immobility. She tries to navigate back to her goal of being treated safely and cared for at home, but as communication reduces, uncertainty increases:
A: it’ll be three weeks on Wednesday since I was there and I haven’t heard anything and would I have? I mean I still haven’t heard anything even though I’ve phoned, but if I do hear anything is it because I’ve phoned? or would I have heard anyway or would I just be sitting here for another month just waiting to see, you know, what’s going on … I just feel a little bit as though, how can I put it erm. I’m the person that’s poorly, but I feel as though I’m the person that’s like having to, jig things up … (Patient A: transcript 2, lines 72–77)
Disrupted interaction continued, and this compounded the uncertainty in the situation. The patient began to lose sight of the goal as uncertainty became more influential. This patient expressed loss of confidence, anxiety, and fear and guilt as she blamed herself for the uncertainty in the situation:
A: I just feel as though I’m like in the middle … I’ve always slept well on a night and for the last fortnight I’ve been very restless I’ve been having nightmares erm I’m not sleeping I’m not having very good nights at all and I think it’s a little bit anxiety. My husband thinks it is, he thinks there a little bit like panic attacks and I wake up erm and I don’t know whether it’s because I just haven’t got a goal any more, there’s not a date, or a you know what I mean … My fault, I mean I didn’t ask. (Patient A: transcript 2, lines between 140−162)
Discussion
This interpretive research captured the multifaceted aspects of a collaborative situation in healthcare and the research design allowed consideration of individual perspectives, social interaction, and organizational issues within the situation. This enabled a detailed and multidimensional model of collaboration to emerge from data, which includes patients as part of collaboration with professionals. This adds a new dimension to existing interprofessional presentations of collaborative practice and provides a picture of how collaboration is differentiated and co-constructed between patients and professionals in the day-to-day experiences of care.
Collaborative practice was revealed as a complex and dynamic social process where individuals interpret the situation and navigate multiple competing influences. The way individuals navigate, interpret, and interact within the situation is key to their experience, and also to the part they play in collaboration. The four areas of collaborative practice, identified in the Collaboration Compass, differentiate collaboration into areas of practice with differing influences and distinct types of interaction. These areas also have very different outcomes for all those involved in collaboration. The findings present the complexity of practice, and a model to explain the multiple influences, which shape the ability of individuals to collaborate, and the interaction, which directs four different types of collaboration.
The findings demonstrate how patients and professionals navigate the tension between the influences of competing situational co-ordinates. In practice the tensions between goals and limits and between certainty and uncertainty occur simultaneously and underpin the complexity of the practice situation. Navigation of competing co-ordinates orientates collaboration and interaction directs it. In geographical navigation, aligning a compass with the co-ordinates on a map identifies a position and sets a direction. In collaborative practice, the competing influences in the situation orientate collaboration and interaction directs and positions collaboration in one of four areas. The Collaboration Compass model identifies four distinct areas of collaboration and these share some similarities with the types of collaboration identified in the literature, but also present some new perspectives.
Professionals navigate a position between the demands of a professional role, organizational restrictions and the requirements of a collectively agreed goal. Patients navigate the tensions between the goal of treatment at home, the limitations of their health condition, and the constraints of a healthcare system which requires them to leave home, travel, wait in clinics, and sometimes make wasted journeys. Navigation of certainty and uncertainty has a direct impact on clinical decisions with the uncertainty of new treatments only acceptable and maintained when balanced with the certainty created by good communication and trust. Certainty in care is balanced with the uncertainty produced when professionals reduce or stop communicating. The findings suggest that, for patients, the goal of treatment at home is the most influential co-ordinate in the situation, and they continually navigate towards it, despite the limits of their health condition and the limitations and uncertainty presented by professionals and the healthcare system.
Developing collaboration is found in situations where there is uncertainty, but also the need to identify and achieve a clear goal. This requires intense interaction and time in the rehearsal of new roles and ways of working. This is often the only type of collaboration presented in the literature, in healthcare definitions of collaborative practice15,16,19 and in many theoretical models,33 but the findings of this study present a more differentiated picture of collaboration, shaped by the situation and the way individuals navigate it.
Coordination, communication, and trust emerged as the interactive mechanisms which maintain collaboration within a situation where there are clear agreed goals and certainty about roles and care. Coordination has been defined as “interlocking care planning activities created with and for team members” which involves efficient and effective use of resources.34 All professionals identified coordination as part of their role, but while maintaining collaboration over a longer period of time one professional took on the role of coordinator, rather than sharing this aspect of interaction. Patients expressed undertaking some aspects of coordination activity, but were found to be far less involved in coordination than professionals. While one central co-ordinator has been found to be effective at channeling communication and having good overall understanding of the situation,35 this role can also increase workload for the coordinator, and runs the risk of reduced levels of communication, as workload becomes too great.36 This identifies a potential for patients to take on the role of coordinator to maintain collaboration in their care, or be active in decision-making about who should be co-ordinating care. While professionals take on this role, they are not always the most efficient or effective at maintaining coordination in the long-term.36
Limiting collaboration is orientated by constraining influences in situations, but also where there is some certainty. This may be about the short-term treatment or in a time limited situation. Rigid professional boundaries have been identified as the downfall of collaborative enterprise,37 but this study identifies that, although professional role and identity influence collaboration, it is navigation of the constraints of organizational systems, increasing workloads, and lack of time which cause professionals to restrict their interaction. Limited collaboration featured reduced communication and trust and no coordination of care. Face-to-face communication between the patient and each professional delivered treatment step-by-step rather than any forward planning of team activities. In other research, face-to-face communication has been found to be the most valuable type of communication,38 and this may ensure the effectiveness of this type of collaboration as the patient relays information between professionals. This involves the patient in limited collaboration, and adds both the responsibility of passing on information and the restriction of keeping multiple appointments. This form of collaboration is effective in a short-term plan of care, but findings demonstrated that, if uncertainty occurs, limited collaboration is not sustainable in the long-term, and soon becomes disrupted.
Lack of communication has been found to be the most significant issue in complicating collaboration,39 and these findings demonstrate the disruptive impact a lack of communication has on collaboration when associated with limitations and uncertainty in the situation. In disrupted collaboration communication and trust are lost, thereby creating more uncertainty. This leads to feelings of frustration and disillusion amongst collaborators. In the area of disrupted collaboration there is a loss of two-way communication. Professionals were found to lose trust and become disillusioned while the patient experienced loss of confidence, anxiety, guilt, and fear.
The levels of patient involvement found in collaboration within OPAT resonates with theory which presents the use of collaboration in varying degrees of involvement.40 The Collaboration Compass presents a fluid and dynamic picture of patient involvement, which changes in response to influences in the care situation. Opportunities exist for greater patient involvement, particularly in the area of development and in the use of coordination to maintain collaboration. As others have theorized, collaboration is an important part of developing and delivering empowering outcomes for patients,12,41 and this study identifies how existing structures and the use of interaction impact on patient involvement in collaboration and the consequences this has for care. Patient involvement in collaboration is more than a simple two-way communication process42 and more complex than a relationship of decision-making.43 It is a complex relationship between patients, professionals, and the situation of care. It depends on the conflicting demands of the situation, interpretation of social and organizational structures, and the relational, discursive, and performative dimensions of power in those relationships. Differences in navigation of the same situation may explain the differing perceptions and expectations of collaboration which have been found between patients and healthcare staff in other studies.11 The Collaboration Compass offers a way of understanding the processes and consequences of collaboration and the impact this has on patient involvement and experience of care.
The Collaboration Compass model provides a way of understanding the individual, social, and organizational influences in collaboration. It offers a tool for use by patients and professionals to identify the interaction which will direct appropriate collaboration for the situation. Developing collaboration requires intense interaction and resources. All collaborators need to be part of this if co-construction of care is to be achieved and if resources are to be used effectively. Not all collaboration needs to be maintained over a long period, but, where it is, finding the right coordinator is essential to sustain certainty in the situation. In some situations, limited collaboration allows for constraints and, if it meets the needs of all involved, can deliver functional and effective care in the short-term. Limited collaboration is certainly more effective, and more positive in outcome, than disrupted collaboration. Understanding the combined impact of uncertainty and limitations will help to identify situations where collaboration is likely to disrupt so that, with appropriate interaction, it can be redirected to collaboration with more positive and productive outcomes.
The findings present the action, interaction, and influence found in the collaborative situation. The consequences of non-collaboration were found within data from the perceptions of participants and there are no findings which represent the perspective of an individual who is involved in the OPAT situation, but who is perceived by others as being uncollaborative. Doctors were identified by participants as being less collaborative, and through theoretical sampling three were invited to participate, but did not respond to the invitations. Although this representation of doctors being less involved in collaboration fits with other studies,44,45 findings from this study would also suggest that collaboration or non-collaboration is complex and part of the interactive navigation of healthcare situations. Further research is required to investigate collaboration from the perspective of doctors.
The findings represent the collaboration found in the OPAT care of three patients and, although this is a limited number of patients, the ratio of patients and professionals is representative of care in community settings. These patients also represent a limited age range and a limited range of conditions, and this may impact on the transferability of these findings. Further research would be required to test the substantive theory and conceptual model in other healthcare settings with patients of different ages and with differing conditions.
The Collaboration Compass model provides a way of understanding the individual, social, and organizational influences in collaboration. It offers a tool for use by patients and professionals to identify the interaction which will direct appropriate collaboration for the situation. Understanding the combined impact of uncertainty and limitations will help to identify situations where collaboration is likely to disrupt so that appropriate interaction can be redirected to achieve more positive and productive outcomes. Future research should seek the perspectives of doctors involved in collaborative practice and test the collaboration compass model in other care settings.
Conclusion
This study involved three patients and twenty one professionals in a sample, which was representative of patient-to-professional ratios found in this OPAT care situation. Collaborative practice was revealed as a complex and dynamic social process where individuals interpret the situation and navigate multiple competing influences. The way individuals navigate, interpret, and interact within the situation is key to their experience, and also to the part they play in directing collaboration. The Collaboration Compass model presents a differentiated picture of collaboration with four distinct areas where collaboration is developed, maintained, limited, or disrupted. Navigation of competing co-ordinates orientates collaboration, and interaction directs it. The specific uses of rehearsal and coordination add understanding of how collaborative relationships are developed and maintained. The use, or restriction, of communication and the impact this has on trust also adds to understanding about how collaboration maintains or disrupts, with direct impact on the way collaboration is experienced. The mechanism of using interaction shapes collaboration and directs different collaborative outcomes. This poses the possibility that interactive navigation can be used actively to direct collaboration in practice situations. The Collaboration Compass can aid understanding of how collaboration is shaped in a situation, and how it can be directed. This may have implications for the outcomes of collaborative projects, and for the realization of truly co-constructed care.
Disclosure
The authors report no conflicts of interest for this work.
References
1. NHS England. Five year forward view; 2014. Available from: https://www.england.nhs.uk/publication/nhs-five-year-forward-view/.
2. Seale B Patients as partners: building collaborative relationships among professionals, patients, carers and communities; 2016. Available from: https://www.kingsfund.org.uk/.
3. NHS England. Commissioning for quality and innovation. CQUIN scheme 2017/19; 2017. Available from: https://www.england.nhs.uk/nhs-standard-contract/cquin/cquin-17-19/.
4. World Health Organization. Multisectoral Collaboration; 2018. Available from: http://www.euro.who.int/en/health-topics/Health-systems/primary-health-care/publications/2018/ensuring-collaboration-between-primary-health-care-and-public-health-services-2018.
5. Van der Heide I, Snoeijs SP, Boerma WG, et al. How to strengthen patient centeredness in caring for people with multimorbidity in Europe. Policy Brief. 2017;22.
6. NHS England. NHS long term plan; January 2019. Available from: https://www.england.nhs.uk/long-term-plan/.
7. NHS England. Prime minister’s challenge fund (PMCF): improving access to general practice. Collaboration in delivery; 2015. Available from: https://www.england.nhs.uk/wp-content/uploads/2015/05/pmcf-innov-showcase-five-collaboration-delivery.pdf.
8. NHS England. Local partnership to improve health and care, Sustainability and transformation partnerships (STPs); 2017. Available from: https://www.england.nhs.uk/stps/.
9. D’Amour D, Sicotte C, Levy R. Collective action within interprofessional teams in health services. Sciences Sociales et Santé. 1999;17(3):67–94.
10. Baars J, Markus T, Kuipers E, et al. Patients’ preferences regarding shared decision-making in the treatment of inflammatory bowel disease: results from a patient-empowerment study. Digestion. 2010;81:113–119. doi:10.1159/000253862
11. Carlsson C, Nilbert M, Nilsson K. Patients’ involvement in improving cancer care: experiences in three years of collaboration between members of patient associations and health care professionals. Patient Educ Couns. 2006;61(2006):65–71.
12. Williams P. Collaboration in Public Policy and Practice: Perspectives on Boundary Spanners. Bristol: Policy Press; 2012.
13. Dickinson H, Sullivan H. Towards a general theory of collaborative performance: the importance of efficacy and agency. Public Adm. 2014;92(1):161–177. doi:10.1111/padm.12048
14. Novikov Z, Glover WJ, Trepman C, et al. How do integrative practices influence patient-centred care?: an exploratory study comparing diabetes and mental health care. Health Care Manage Rev. 2016;41(2):113–126. doi:10.1097/HMR.0000000000000062
15. Gray B. Collaborating: Finding Common Ground for Multiparty Problems. San Francisco: Jossey-Bass Publishers; 1989.
16. Petri L. Concept analysis of interdisciplinary collaboration. Nurs Forum. 2010;45(2):73–82. doi:10.1111/j.1744-6198.2010.00167.x
17. Department of Health. The NHS Plan: A Plan for Investment, a Plan for Reform. London: HMSO; 2000.
18. Department of Health. The Health and Social Care Act 2012. London: HMSO; 2012.
19. Orchard CA, Curran V, Kabene S. Creating a culture for interdisciplinary collaborative professional practice. Med Educ Online. 2005;10(11):1–13. doi:10.3402/meo.v10i.4387
20. National Audit Office. Health and social care integration. (HC 1011 SESSION 2016-17 8 FEBRUARY 2017); 2017. Available from: https://www.nao.org.uk/wp-content/uploads/2017/02/Health-and-social-care-integration.pdf.
21. D’Amour D, Ferrada-Videla M, San Martin Rodriguez L, et al. The conceptual basis for interprofessional collaboration: core concepts and theoretical frameworks. J Interprof Care. 2005;19(S1):116–131. doi:10.1080/13561820500082529
22. Chapman AL, Seaton RA, Cooper MA, et al. Good practice recommendations for outpatient parenteral antimicrobial therapy (OPAT) in adults in the UK: a consensus statement. J Antimicrob Chemother. 2012;67(5):1053–1062. doi:10.1093/jac/dks003
23. Chapman AL. Outpatient parenteral antimicrobial therapy in a changing NHS: challenges and opportunities. Clin Med (Northfield Il). 2013;13(1):35–36. doi:10.7861/clinmedicine.13-1-35
24. Clarke AE. Situational Analysis: Grounded Theory After the Postmodern Turn. Thousand Oaks, California: Sage; 2005.
25. Charmaz K. Constructionism and the Grounded Theory Method. Handbook of Constructionist Research, 397–412. New York: Guilford Press; 2008.
26. Kitson NA, Price M, Lau FY, et al. Developing a medication communication framework across continuums of care using the circle of care modeling approach. BMC Health Serv Res. 2013;13:418. doi:10.1186/1472-6963-13-418
27. Charmaz K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. Newbury Park, CA: Pine Forge Press; 2006.
28. Glaser BG. Theoretical Sensitivity: Advances in the Methodology of Grounded Theory. Mill Valley, California: Sociology Press; 1978.
29. Charmaz K. ‘Discovering’chronic illness: using grounded theory. Soc Sci Med. 1990;30(11):1161–1172. doi:10.1016/0277-9536(90)90256-R
30. McCallin AM. Designing a grounded theory study: some practicalities. Nurs Crit Care. 2003;8(5):203–208. doi:10.1046/j.1362-1017.2003.00033.x
31. Charmaz K. Constructing Grounded Theory. London and Thousand Oaks, CA: Sage; 2005.
32. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Thousand Oaks, California: Sage; 2008.
33. Bridges D, Davidson RA, Soule Odegard P, et al. Interprofessional collaboration: three best practice models of interprofessional education. Med Educ Online. 2011;16(1):6035. doi:10.3402/meo.v16i0.6035
34. Orchard CA, King GA, Khalili H, et al. Assessment of interprofessional team collaboration scale (AITCS): development and testing of the instrument. J Contin Educ Health Prof. 2012;32(1):58–67. doi:10.1002/chp.21123
35. Hollenbeck JR, Ellis AP, Humphrey SE, et al. Asymmetry in structural adaptation: the differential impact of centralizing versus decentralizing team decision-making structures. Organ Behav Hum Decis Process. 2011;114(1):64–74. doi:10.1016/j.obhdp.2010.08.003
36. Cross RL, Parker A. The Hidden Power of Social Networks: Understanding How Work Really Gets Done in Organizations. Brighton, Massachusetts: Harvard; 2004.
37. Aein F, Alhani F, Mohammadi E, et al. Struggling to create new boundaries: A grounded theory study of collaboration between nurses and parents in the care process in Iran. J Adv Nurs. 2011;67(4):841–853. doi:10.1111/j.1365-2648.2010.05515.x
38. Pentland A. The new science of building great teams. Harv Bus Rev. 2012;90(4):60–69.
39. Jünger S, Pestinger M, Elsner F, et al. Criteria for successful multiprofessional cooperation in palliative care teams. Palliat Med. 2007;21(4):347–354. doi:10.1177/0269216307078505
40. Grantham G, McMillan V, Dunn S, Gassner L, Woodcock P. Patient self-medication – a change in hospital practice. J Clin Nurs. 2006;15:962–970. doi:10.1111/j.1365-2702.2006.01398.x
41. Leske E, Strodl X, Hou. Y. Patient–practitioner relationships desired by overweight/obese adults. Patient Educ Couns. 2012;89(2):309–315. doi:10.1016/j.pec.2012.07.002
42. Gande SW, Faber MJ, Durand M-A, Thompson R, Elwyn G. A classification model of patient engagement methods and assessment of their feasibility in real-world settings. Patient Educ Couns. 2014;95:281–287. doi:10.1016/j.pec.2014.01.016
43. Angel S, Frederiksen KR. Challenges in achieving patient participation: a review of how patient participation is addressed in empirical studies. Int J Nurs Stud. 2015;52:152 5–1538. doi:10.1016/j.ijnurstu.2015.04.008
44. Sollami A, Caricati L, Sarli L. Nurse–physician collaboration: A meta-analytical investigation of survey scores. J Interprof Care. 2015;29(3):223–229. doi:10.3109/13561820.2014.955912
45. Reeves S, Lewin S. Interprofessional collaboration in the hospital: strategies and meanings. J Health Serv Res Policy. 2004;9(4):218–225. doi:10.1258/1355819042250140
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.