")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 14
The Clinical Impact of Seropositivity on Treatment Response in Patients with Rheumatoid Arthritis Treated with Etanercept: A Real-World Iraqi Experience
Authors Ridha A, Hussein S , AlJabban A, Gunay LM , Gorial FI, Al Ani NA
Received 3 April 2022
Accepted for publication 27 May 2022
Published 14 June 2022 Volume 2022:14 Pages 113—121
DOI https://doi.org/10.2147/OARRR.S368190
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Asal Ridha,1 Saba Hussein,2 Ali AlJabban,3 Levent Mert Gunay,4 Faiq I Gorial,5 Nizar Abdulateef Al Ani5
1Rheumatology Unit, Department of Medicine, Baghdad Teaching Hospital, Medical City, Baghdad, Iraq; 2Rheumatology Unit, Department of Medicine, Al-Kindy Teaching Hospital, Baghdad, Iraq; 3Medical Department, Pfizer, Baghdad, Iraq; 4Emerging Markets Medical Affairs Department, Pfizer Turkiye, Istanbul, Turkiye; 5Rheumatology Unit, Department of Medicine, College of Medicine, University of Baghdad, Baghdad, Iraq
Correspondence: Ali AlJabban, Medical Department, Pfizer, Building 5, Street 51, Sec. 611, AlDawoodi, Baghdad, Iraq, Tel +964 7706056226, Email [email protected]
Purpose: To assess the clinical impact of rheumatoid factor (RF) and anti-cyclic citrullinated peptide antibody (ACPA)’s seropositivity on treatment response in patients with rheumatoid arthritis (RA) treated with etanercept.
Patients and Methods: A retrospective analysis of patients with RA registered in Baghdad Teaching Hospital Registry from May 2012 to August 2019 was conducted. Patients aged ≥ 18 years, meeting the ACR/EULAR 2010 criteria for RA, being treated with etanercept, and followed up at ≥ 1 year after etanercept initiation were included; patients who received any other biologics for RA were excluded. Patients were classified as seropositive (RF- and ACPA-positive), seronegative (RF- and ACPA-negative), RF-positive, RF-negative, ACPA-positive, and ACPA-negative. The primary outcomes included Clinical Disease Activity Index (CDAI) and Disease Activity Score 28 (DAS28) which were measured at one year after treatment initiation.
Results: At baseline, a total of 1318 (88.3%) patients were seropositive; 1122 (75.2%) and 1054 (70.6%) patients were RF- and ACPA-positive, respectively. Baseline mean CDAI scores were significantly (P = 0.001) higher among seropositive patients compared with seronegative patients. The baseline mean DAS28 score was also significantly higher in ACPA-positive group compared with the ACPA-negative group (P = 0.021). At baseline, the number of patients who had high CDAI scores was significantly higher among the seropositive, RF-positive, and ACPA-positive groups (P = 0.001, P = 0.001, and P = 0.002, respectively). After one year of treatment with etanercept, among seropositive versus seronegative and ACPA-positive versus ACPA-negative groups, there was a significant improvement in terms of the mean CDAI score (P = 0.004 and P = 0.017, respectively) and CDAI response (P = 0.011 and P = 0.048, respectively). At one year, the proportion of patients among the seropositive versus seronegative group who reached remission were 566 (42.9%) versus 78 (44.6%) and 642 (47.3%) versus 83 (47.4%), for CDAI and DAS28 response, respectively.
Conclusion: The results imply that seropositivity and ACPA-positivity may influence the treatment response in patients with RA, who were treated with etanercept.
Keywords: anti-cyclic citrullinated peptide antibody, Iraq, real-world, rheumatoid factor
Introduction
Rheumatoid arthritis (RA) is a chronic debilitating inflammatory disease in which the peripheral joints are the primary sites of inflammation, often leading to impairment of these joints.1 The global prevalence of RA was estimated in a recent meta-analysis as 0.46%, with a 95% prediction interval of 0.06% to 1.27%.2 The disease has also been found to be more prevalent in women.3,4
Rheumatoid factor (RF) has long been a component of the diagnostic criteria for RA. About 70% of patients with RA test positive for RF at onset, and 85% become positive during the first 2 years of the disease.5 RF and its association with a more severe disease course of RA have been extensively studied.6 Anti-cyclic citrullinated peptide antibody (ACPA) is another important serological biomarker of RA and studies have found ACPA to be positive in 60% to 80% of patients with RA.1,7,8 The ACPA serological status provides important prognostic information regarding patients with RA.1,9,10 One of the studies showed that ACPA-positive patients had more active disease during follow-up than ACPA-negative patients.11 Based on the available evidence, ACPA was included in the diagnostic criteria for RA in 2009.12
During the last two decades, there has been a paradigm shift in the treatment patterns of RA. Previously, early treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) was followed by progressive addition of disease-modifying antirheumatic drugs (DMARDs); however, the present treatment modality starts with aggressive DMARD therapy soon after the diagnosis of RA. The initiation of DMARD therapy early in the course of a symptomatic disease has been substantiated with improved prognosis and disease outcomes in several studies.13,14 Although several patients with RA respond to the conventional synthetic DMARDs (such as methotrexate), a large proportion of RA remains active despite such treatments. Immunotherapy with biological agents has significantly enhanced treatment outcomes in patients with RA.15 Tumor necrosis factor‑α (TNF‑α) antagonists, such as etanercept, infliximab, adalimumab, golimumab, and certolizumab pegol have been widely used for the treatment of RA.12 Etanercept is the first anti-TNF agent to be approved for the treatment of RA. Over the last few years, numerous clinical studies have shown the efficacy and safety of etanercept in established and early RA, as a monotherapy or in combination with methotrexate.16,17
Given the optionality of biological treatment for patients with RA, it is important to identify a predictor for treatment response, which in turn can guide early treatment decisions.18,19 RF and ACPA are well studied, and their associations with a more severe disease course have been described in western countries. However, there are limited data available from the Middle East region.20–22 The present study was conducted to determine the clinical impact of RF and ACPA seropositivity on the treatment response in patients with RA treated with etanercept in Iraq.
Patients and Methods
Study Design
This is a retrospective, observational, real-world study performed on data collected from all the patients diagnosed with RA in the Baghdad Teaching Hospital registry, between May 2012 and August 2019. The rheumatology patient registry was an initiative established in 2012 to build a prospective, longitudinal, multicenter cohort. The registry captures data pertaining to all the patients treated with biologic therapies in the Rheumatology unit, Baghdad Teaching Hospital. The treatment decisions for patients with RA were guided by the American College of Rheumatology (ACR) recommendations. Data captured in the study included patient demographics (age and gender) and disease duration (in years); Disease Activity Score 28 (DAS28), Clinical Disease Activity Index (CDAI) at baseline and at one year after initiation of etanercept treatment, RF, and ACPA status. The treatment response was determined by measuring the change between baseline and one-year scores of DAS28 and CDAI. A patient with a DAS28 score of <2.6 denotes remission,23 ≥2.6 to <3.1 indicates low activity, ≥3.1 to <5.1 indicates moderate activity, and ≥5.1 indicates high activity.24,25 A CDAI score of <2.8 indicates remission, 2.9 to 10 indicates low activity, 10.1 to 22 indicates moderate activity, and 22.1 to 76 indicates high activity.26
The study was conducted in accordance with legal and regulatory requirements, scientific purpose, value and rigor; it followed generally accepted research practices described in the Guidelines for Good Pharmacoepidemiology Practices (GPP) by the International Society for Pharmacoepidemiology (ISPE), Good Epidemiological Practice (GEP) guidelines by the International Epidemiological Association (IEA), and Good Practices for Outcomes Research issued by the International Society for Pharmacoeconomics and Outcomes Research (ISPOR).
All patients had signed individual consent forms before including their data in the Baghdad Teaching Hospital Registry. The study was approved by the Ethics Committee, Baghdad Teaching Hospital. Our study is in full compliance with the Declaration of Helsinki.
Study Population
The eligibility criteria for the study included all patients aged ≥18 years with a diagnosis of RA based on the criteria defined by the ACR/The European League Against Rheumatism (EULAR) 2010, patients referred for treatment with etanercept (as monotherapy or combination therapy with any other concomitant conventional DMARDs), and those who had ≥1 year of follow-up after initiating etanercept. All patients with RA receiving any biologic therapy other than etanercept during their entire treatment period were excluded.
Outcomes and Statistical Analysis
The response variable was defined as DAS28 and CDAI response at 1 year. Clinical response to etanercept treatment was assessed by evaluating mean changes in CDAI and DAS28 scores from baseline to 1 year after initiation of treatment. A P-value of <0.05 without multiplicity adjustment is considered statistically significant for this post hoc analysis. Patients were classified as seropositive (RF- and ACPA-positive), seronegative (RF- and ACPA-negative), RF-positive, RF-negative, ACPA-positive, and ACPA-negative. Categorical covariates were described by frequency distribution, whereas continuous covariates were expressed in terms of their mean and standard deviation or median and interquartile range, as appropriate. The unadjusted comparisons between groups of the covariates and the outcomes were evaluated using Chi-square test for categorical data, while for continuous data, the Student’s t-test was used for normally distributed variables and the Kruskal–Wallis test for non-parametric data. SPSS (version 23) was used for statistical analysis.
Results
Baseline Characteristics
A total of 1493 patients with RA were included in this analysis, and the majority were female patients (1234; 82.7%) (Table 1). The mean duration of RA symptoms prior to the initiation of etanercept treatment was 9 ± 8.1 years (Table 1). At baseline, a total of 1318 (88.3%) patients were seropositive and 1122 (75.2%) and 1054 (70.6%) patients were RF- and ACPA-positive, respectively (Table 2). Significantly higher baseline mean CDAI scores were observed among seropositive patients as compared to seronegative patients (P=0.001) (Table 2). The baseline mean DAS28 score was also significantly higher in ACPA-positive group compared to ACPA-negative group (P=0.021) (Table 2). At baseline, the number of patients who had high disease activity according to CDAI (high CDAI score) was significantly higher among seropositive, RF-positive, and ACPA-positive groups (P=0.001, P=0.001, and P=0.002, respectively) (Table 2).
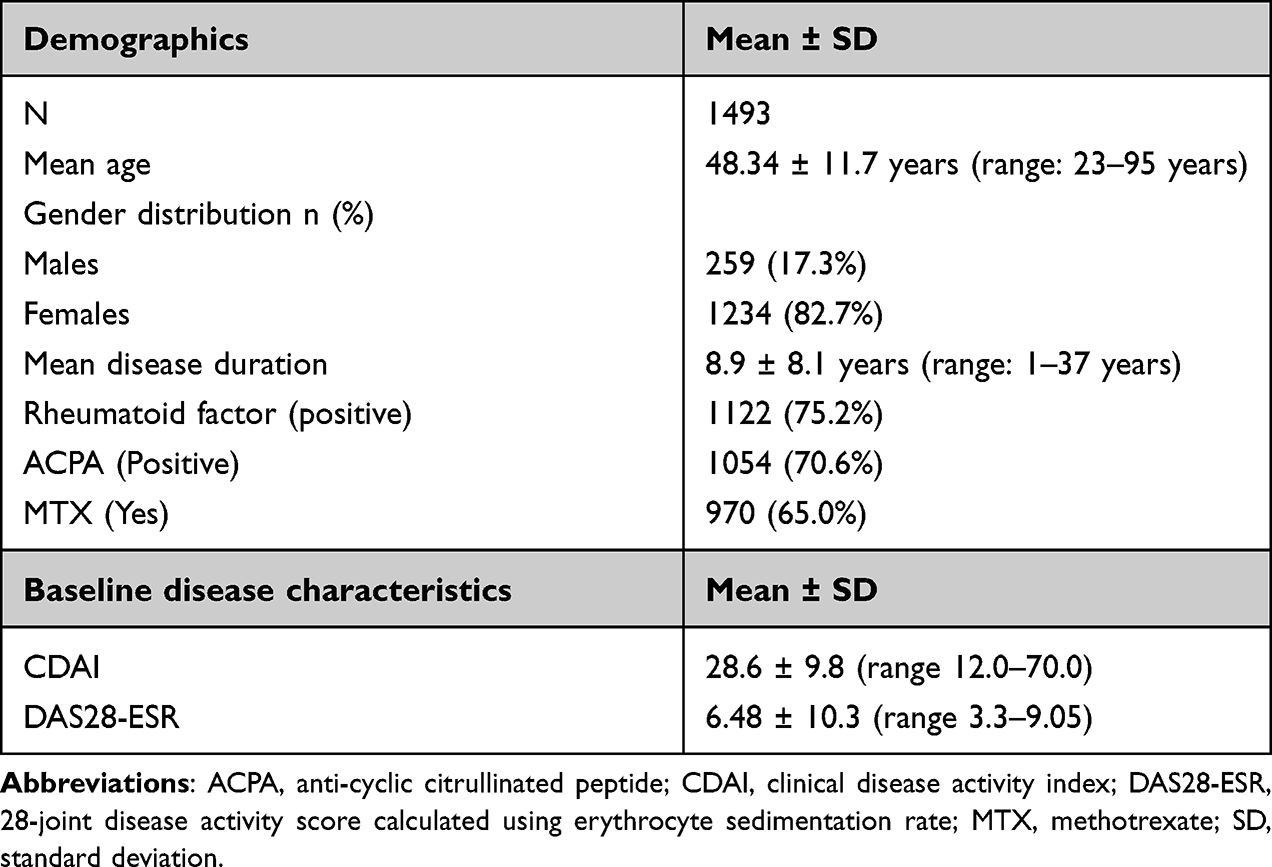 |
Table 1 Demographics and Baseline Disease Characteristics of the Study Population |
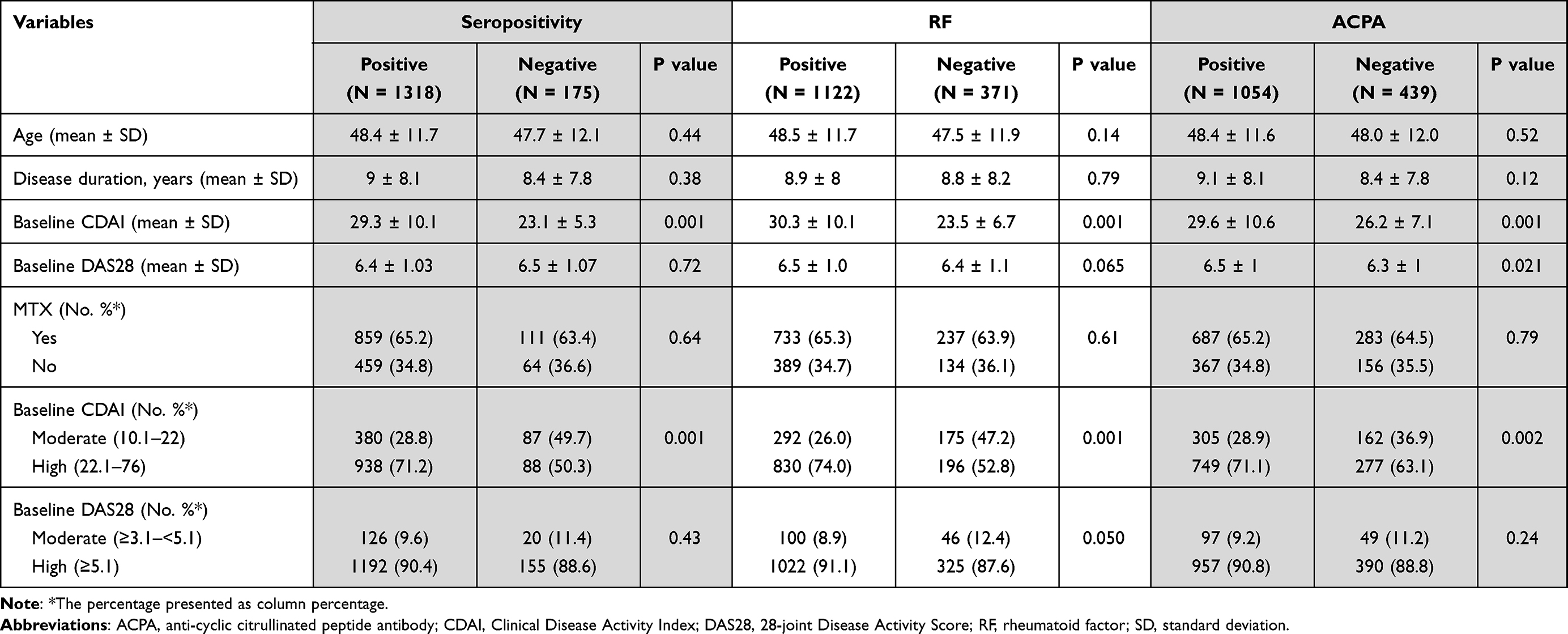 |
Table 2 Baseline Characteristics Data of Patients with Rheumatoid Arthritis |
Primary Outcomes
At one year after initiating treatment with etanercept, there was a significant improvement in terms of the mean CDAI scores among seropositive versus seronegative (P=0.004) and ACPA-positive versus ACPA-negative groups (P=0.017). Similarly, improvement of the CDAI response was observed in seropositive versus seronegative groups (P=0.011) and ACPA-positive versus ACPA-negative groups (P=0.048) (Table 3). However, there was no significant difference between RF-positive and RF-negative groups in terms of CDAI scores (P=0.27) and CDAI response (P=0.23).
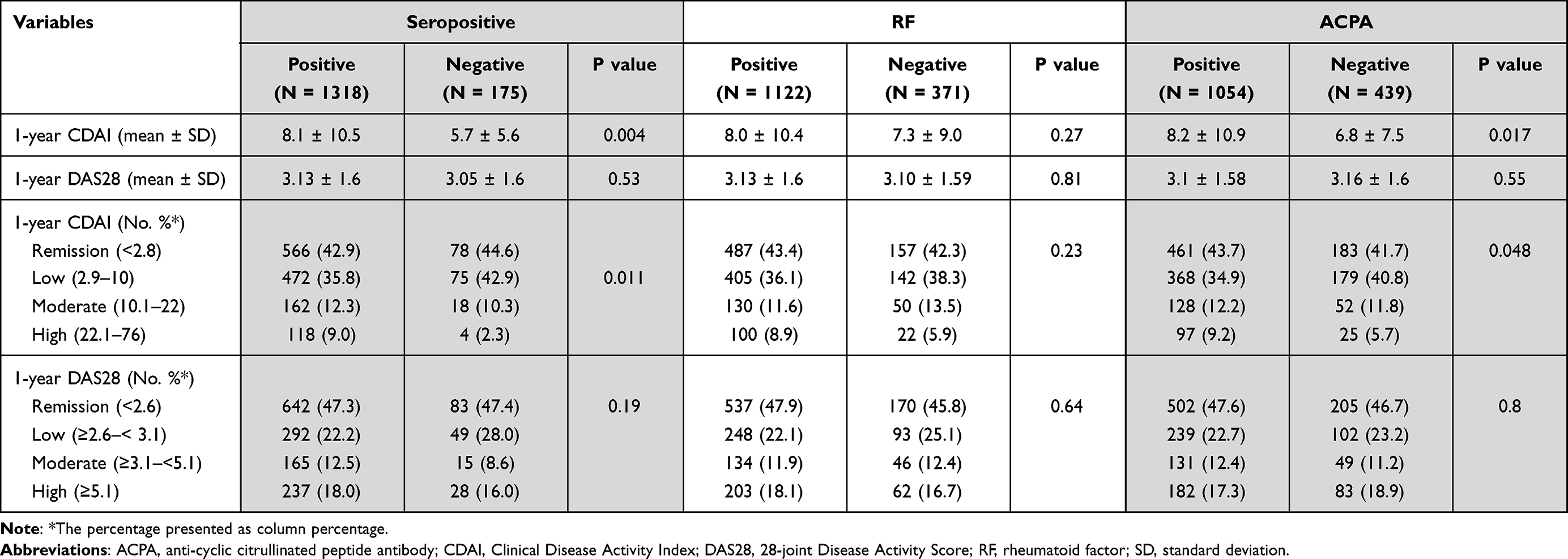 |
Table 3 Response After 1 Year of Etanercept Treatment in Patients with Rheumatoid Arthritis |
At one year, there was no observable difference in terms of DAS28 scores and DAS response (statistically insignificant, P>0.05) among all the three comparative analyses: seropositive versus seronegative (P=0.53), RF-positive versus RF-negative (P=0.81), and ACPA-positive versus ACPA-negative groups (P=0.55) (Table 3).
The proportion of patients among the seropositive versus seronegative groups reaching remission within a year of etanercept treatment initiation based on CDAI scores was 566 (42.9%) and 78 (44.6%); it was 642 (47.3%) and 83 (47.4%) for DAS28 response (Table 2 and Figure 1).
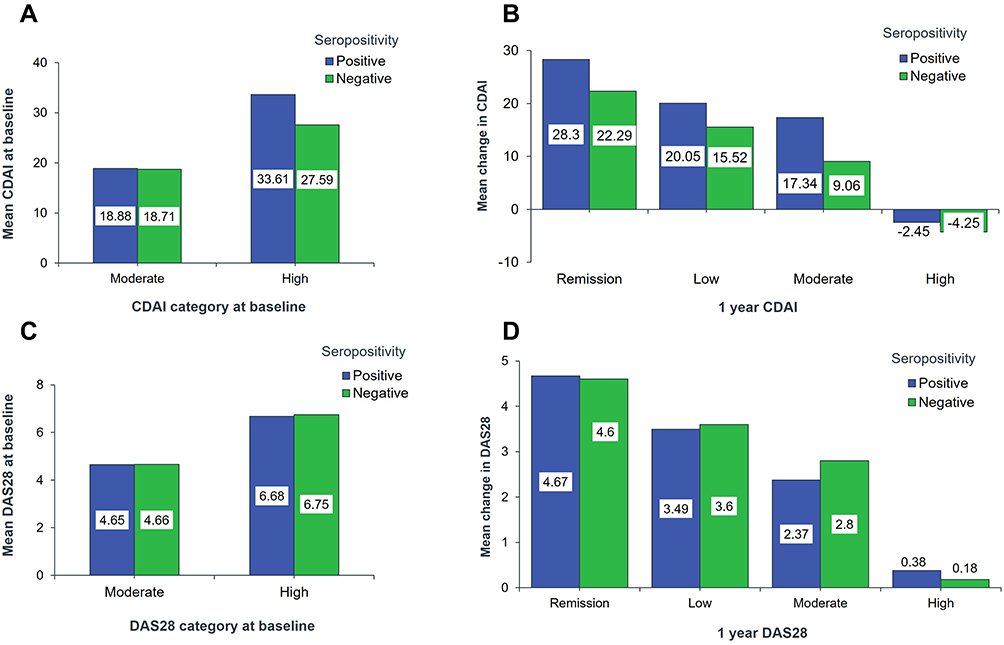 |
Figure 1 Seropositivity impact on baseline CDAI, DAS28 and one year after treatment with etanercept. (A-D) Mean change in CDAI and DAS28 scores from baseline to 1 year after initiation of treatment. Abbreviations: CDAI, Clinical Disease Activity Index; DAS28, 28-joint Disease Activity Score. |
At one year compared to baseline, both CDAI and DAS28 scores improved across the patient groups, irrespective of the baseline serological status of RF and ACPA. CDAI scores (baseline vs one year) were as follows: seropositive (29.3 vs 8.1), seronegative (23.1 vs 5.7), RF-positive (30.3 vs 8.0), RF-negative (23.5 vs 7.3), ACPA-positive (29.6 vs 8.2), and ACPA-negative (26.2 vs 6.8). DAS28 scores (baseline vs one year) were as follows: seropositive (6.4 vs 3.1), seronegative (6.5 vs 3.0), RF-positive (6.5 vs 3.1), RF-negative (6.4 vs 3.1), ACPA-positive (6.5 vs 3.1), and ACPA-negative (6.3 vs 3.1) (Tables 1 and 2).
Discussion
The introduction of anti-TNF-α biological agents has contributed significantly to the advancement in the treatment of RA. However, the possible risk of serious toxicity and substantial treatment expenses associated with biologics have emphasized the need for reliable treatment response predictors for anti-TNF-α treatments.27,28 A predictor for treatment response is essential in guiding early treatment decisions. ACPA and RF are widely used in the diagnosis and classification of RA.29 Patients with RA, who are seropositive for RF or ACPA, are considered to manifest an aggressive disease course compared with seronegative patients. However, the association between seropositivity and measures of disease severity (CDAI and DAS28) remains unclear.30 The present study investigated the clinical impact of RF and ACPA seropositivity on treatment response in patients with RA, who were treated with etanercept for at least 1 year. The results of our analysis show that patients with RA who received treatment with etanercept for 1 year had clinical improvements in CDAI and DAS28 scores, versus baseline, irrespective of baseline serological status for RF and ACPA. Further, seropositive versus seronegative and ACPA-positive group versus ACPA-seronegative groups showed a significant impact on the CDAI score and CDAI response (Table 3).
Although the present study did not measure the ACPA and RF levels, it confirmed that a substantial proportion of patients reached remission in terms of CDAI and DAS28 response within a year of treatment with etanercept. These findings are comparable to a previous study that demonstrated a significant decrease in the ACPA and RF levels in the sera of rheumatoid patients after three months of etanercept treatment. The same study also reported a reduction in DAS28 score, indicating a decline in disease activity.31 However, in the present study, there is no significant difference at one year in terms of DAS28 scores and DAS28 response between the seropositive and seronegative groups.
Previous studies with anti-TNFα agents (infliximab, adalimumab, etanercept, and golimumab) showed that there is a differential treatment response to biological therapies based on the RF or ACPA serological status.32–34 Some studies have suggested that the seropositive status of RF or ACPA in patients with RA is associated with a clinical response to treatment,27,28,35–40 while there was no correlation between treatment response and RF and ACPA seropositivity in other studies.30,41,42
Similar to the findings of the present study, the ACTION study demonstrated clinical efficacy in biologic-naïve patients with RA, who were treated with abatacept for six months, irrespective of baseline serostatus for RF or ACPA. Additionally, a significantly superior clinical efficacy of abatacept was observed in seropositive (RF- and ACPA-positive) patients compared to those who were seronegative (RF- and ACPA-negative) at baseline.43 Harrold et al demonstrated in the patients treated with abatacept that higher ACPA concentrations at baseline were associated with numerically greater improvements in CDAI and significant improvements in patient-reported outcomes after six months. However, there was no association between baseline ACPA concentration and treatment response in patients treated with a tumor necrosis factor inhibitor (TNFi).1 Furthermore, a meta-analysis indicated that the status of RF and ACPA is not associated with the clinical response to anti-TNF-α treatment in patients with RA.34 There is no definite conclusion on the impact of RF or ACPA serological status on the treatment response. However, the determination of RF and ACPA is useful for diagnostic and prognostic implications of early RA.34,42
To the best of our knowledge, this is the first study from the Middle East region examining the predictive role of ACPA and RF on etanercept treatment response in patients with RA. As with all real-world studies, there are limitations to our study. This study does not include a control group of patients with RA not treated with etanercept, limiting the comparison of treatment response with other anti-TNF-α agents or any other DMARD treatment. Additionally, there are missing data that could lead to inherent bias in the analysis.
Conclusion
The results of the present analysis show that seropositive and ACPA-positive Iraqi patients with RA, who received treatment with etanercept for one year, had significant improvements in CDAI scores and CDAI response. However, there was no observable difference between the groups in terms of DAS28 scores and DAS28 response. These results imply that seropositivity and ACPA positivity may influence the treatment response in patients with RA treated with etanercept. Further studies are needed to corroborate the definitive predictive role of ACPA and RF seropositivity on treatment response in patients with RA treated with etanercept or any other anti-TNF-α agents.
Acknowledgments
The authors would like to thank Chandra Shaker Sriram and Smitha Sreedharan from IQVIA for providing medical writing support.
Funding
The manuscript writing support was funded by Pfizer.
Disclosure
AR, SH, FIG, and NAA declare no conflicts of interest in this work. AA and LMG are employees of Pfizer.
References
1. Harrold LR, Bryson J, Lehman T, et al. Association between baseline anti-cyclic citrullinated peptide antibodies and 6-month clinical response following Abatacept or TNF inhibitor treatment: a real-world analysis of biologic-experienced patients with RA. Rheumatol Ther. 2021;8(2):937–953. doi:10.1007/s40744-021-00310-2
2. Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int. 2021;41(5):863–877. doi:10.1007/s00296-020-04731-0
3. Gabriel SE, Michaud K. Epidemiological studies in incidence, prevalence, mortality, and comorbidity of the rheumatic diseases. Arthritis Res Ther. 2009;11(3):1–16. doi:10.1186/ar2669
4. Cross M, Smith E, Hoy D, et al. The global burden of rheumatoid arthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1316–1322. doi:10.1136/annrheumdis-2013-204627
5. Wilson D. Rheumatoid factors in patients with rheumatoid arthritis. Can Fam Physician. 2006;52(2):180.
6. Ingegnoli F, Castelli R, Gualtierotti R. Rheumatoid factors: clinical applications. Dis Markers. 2013;35(6):727–734. doi:10.1155/2013/726598
7. Kurowska W, Kuca-Warnawin EH, Radzikowska A, Maśliński W. The role of anti-citrullinated protein antibodies (ACPA) in the pathogenesis of rheumatoid arthritis. Cent Eur J Immunol. 2017;42(4):390. doi:10.5114/ceji.2017.72807
8. Vaidya B, Nakarmi S, Rajbhandari N, Bataju P. Clinical correlation between Anti-CCP antibody, rheumatoid factor and clinical parameters of patients with rheumatoid arthritis. J Univers College Med Sci. 2013;1(4):13–16. doi:10.3126/jucms.v1i4.9566
9. Kroot EJJ, De Jong BA, Van Leeuwen MA, et al. The prognostic value of anti–cyclic citrullinated peptide antibody in patients with recent‐onset rheumatoid arthritis. Arthritis Rheum. 2000;43(8):1831–1835. doi:10.1002/1529-0131(200008)43:8<1831::AID-ANR19>3.0.CO;2-6
10. Berglin E, Johansson T, Sundin U, et al. Radiological outcome in rheumatoid arthritis is predicted by presence of antibodies against cyclic citrullinated peptide before and at disease onset, and by IgA-RF at disease onset. Ann Rheum Dis. 2006;65(4):453–458. doi:10.1136/ard.2005.041376
11. Rönnelid J, Wick MC, Lampa J, et al. Longitudinal analysis of citrullinated protein/peptide antibodies (anti-CP) during 5 year follow up in early rheumatoid arthritis: anti-CP status predicts worse disease activity and greater radiological progression. Ann Rheum Dis. 2005;64(12):1744–1749. doi:10.1136/ard.2004.033571
12. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
13. Demoruelle MK, Deane KD. Treatment strategies in early rheumatoid arthritis and prevention of rheumatoid arthritis. Curr Rheumatol Rep. 2012;14(5):472–480. doi:10.1007/s11926-012-0275-1
14. Smolen JS, Landewé RB, Bijlsma JW, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
15. Ma X, Xu S. TNF inhibitor therapy for rheumatoid arthritis. Biomed Rep. 2013;1(2):177–184. doi:10.3892/br.2012.42
16. Haraoui B, Bykerk V. Etanercept in the treatment of rheumatoid arthritis. Ther Clin Risk Manag. 2007;3(1):99. doi:10.2147/tcrm.2007.3.1.99
17. Lethaby A, Lopez‐Olivo MA, Maxwell LJ, Burls A, Tugwell P, Wells GA. Etanercept for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev. 2013;(5). doi:10.1002/14651858.CD004525.pub2
18. Anderson JJ, Wells G, Verhoeven AC, Felson DT. Factors predicting response to treatment in rheumatoid arthritis: the importance of disease duration. Arthritis Rheum. 2000;43(1):22–29. doi:10.1002/1529-0131(200001)43:1<22::AID-ANR4>3.0.CO;2-9
19. Miriovsky BJ, Michaud K, Thiele GM, et al. Anti-CCP antibody and rheumatoid factor concentrations predict greater disease activity in men with rheumatoid arthritis. Ann Rheum Dis. 2010;69(7):1292–1297. doi:10.1136/ard.2009.122739
20. Jilani A, Mackworth-Young C. The role of citrullinated protein antibodies in predicting erosive disease in rheumatoid arthritis: a systematic literature review and meta-analysis. Int J Rheumatol. 2015;2015:1–8. doi:10.1155/2015/728610
21. Bugatti S, Manzo A, Montecucco C, Caporali R. The clinical value of autoantibodies in rheumatoid arthritis. Front Med. 2018;5(339):2018. doi:10.3389/fmed.2018.00339
22. Harrold LR, Litman HJ, Connolly SE, et al. Effect of anticitrullinated protein antibody status on response to Abatacept or antitumor necrosis factor-α therapy in patients with rheumatoid arthritis: a US national observational study. J Rheumatol. 2018;45(1):32–39. doi:10.3899/jrheum.170007
23. Fransen J, Creemers MC, Van Riel PL. Remission in rheumatoid arthritis: agreement of the disease activity score (DAS28) with the ARA preliminary remission criteria. Rheumatology. 2004;43(10):1252–1255. doi:10.1093/rheumatology/keh297
24. Fransen J, Stucki G, van Riel PL. Rheumatoid arthritis measures: disease activity score (DAS), Disease activity score‐28 (DAS28), Rapid assessment of disease activity in rheumatology (RADAR), and Rheumatoid arthritis disease activity index (RADAI). Arthritis Care Res. 2003;49(S5):S214–S224. doi:10.1002/art.11407
25. Kumar BS, Suneetha P, Mohan A, Kumar DP, Sarma KVS. Comparison of disease activity score in 28 joints with ESR (DAS28), Clinical Disease Activity Index (CDAI), Health Assessment Questionnaire Disability Index (HAQ-DI) & Routine Assessment of Patient Index Data with 3 measures (RAPID3) for assessing disease activity in patients with rheumatoid arthritis at initial presentation. Indian J Med Res. 2017;146(Supplement):S57–s62. doi:10.4103/ijmr.IJMR_701_15
26. Aletaha D, Smolen J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): a review of their usefulness and validity in rheumatoid arthritis. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S100–8.
27. Potter C, Hyrich K, Tracey A, et al. Association of rheumatoid factor and anti-cyclic citrullinated peptide positivity, but not carriage of shared epitope or PTPN22 susceptibility variants, with anti-tumour necrosis factor response in rheumatoid arthritis. Ann Rheum Dis. 2009;68(1):69–74. doi:10.1136/ard.2007.084715
28. Vasilopoulos Y, Bagiatis V, Stamatopoulou D, et al. Association of anti-CCP positivity and carriage of TNFRII susceptibility variant with anti-TNF-α response in rheumatoid arthritis. Clin Exp Rheumatol. 2011;29(4):701–704.
29. Martinez-Prat L, Nissen MJ, Lamacchia C, et al. Comparison of serological biomarkers in rheumatoid arthritis and their combination to improve diagnostic performance. Front Immunol. 2018;9:1113. doi:10.3389/fimmu.2018.01113
30. Choi S-T, Lee K-H. Clinical management of seronegative and seropositive rheumatoid arthritis: a comparative study. PLoS One. 2018;13(4):e0195550. doi:10.1371/journal.pone.0195550
31. Chen H-A, Lin K-C, Chen C-H, et al. The effect of etanercept on anti-cyclic citrullinated peptide antibodies and rheumatoid factor in patients with rheumatoid arthritis. Ann Rheum Dis. 2006;65(1):35–39. doi:10.1136/ard.2005.038851
32. De Rycke L, Verhelst X, Kruithof E, et al. Rheumatoid factor, but not anti-cyclic citrullinated peptide antibodies, is modulated by infliximab treatment in rheumatoid arthritis. Ann Rheum Dis. 2005;64(2):299–302. doi:10.1136/ard.2004.023523
33. Caramaschi P, Biasi D, Tonolli E, et al. Antibodies against cyclic citrullinated peptides in patients affected by rheumatoid arthritis before and after infliximab treatment. Rheumatol Int. 2005;26(1):58–62. doi:10.1007/s00296-004-0571-9
34. Lv Q, Yin Y, Li X, et al. The status of rheumatoid factor and anti-cyclic citrullinated peptide antibody are not associated with the effect of anti-TNFα agent treatment in patients with rheumatoid arthritis: a meta-analysis. PLoS One. 2014;9(2):e89442. doi:10.1371/journal.pone.0089442
35. Klaasen R, Cantaert T, Wijbrandts CA, et al. The value of rheumatoid factor and anti-citrullinated protein antibodies as predictors of response to infliximab in rheumatoid arthritis: an exploratory study. Rheumatology. 2011;50(8):1487–1493. doi:10.1093/rheumatology/ker010
36. Canhão H, Rodrigues AM, Mourão AF, et al. Comparative effectiveness and predictors of response to tumour necrosis factor inhibitor therapies in rheumatoid arthritis. Rheumatology. 2012;51(11):2020–2026. doi:10.1093/rheumatology/kes184
37. Bobbio-Pallavicini F, Caporali R, Alpini C, et al. High IgA rheumatoid factor levels are associated with poor clinical response to tumour necrosis factor α inhibitors in rheumatoid arthritis. Ann Rheum Dis. 2007;66(3):302–307. doi:10.1136/ard.2006.060608
38. Alessandri C, Bombardieri M, Papa N, et al. Decrease of anti-cyclic citrullinated peptide antibodies and rheumatoid factor following anti-TNFα therapy (infliximab) in rheumatoid arthritis is associated with clinical improvement. Ann Rheum Dis. 2004;63(10):1218–1221. doi:10.1136/ard.2003.014647
39. Atzeni F, Sarzi-Puttini P, Dell’Acqua D, et al. Adalimumab clinical efficacy is associated with rheumatoid factor and anti-cyclic citrullinated peptide antibody titer reduction: a one-year prospective study. Arthritis Res Ther. 2005;8(1):1–8.
40. Gardette A, Ottaviani S, Tubach F, et al. High anti-CCP antibody titres predict good response to rituximab in patients with active rheumatoid arthritis. Joint Bone Spine. 2014;81(5):416–420. doi:10.1016/j.jbspin.2014.06.001
41. Soto L, Sabugo F, Catalan D, et al. The presence of anti-citrullinated protein antibodies (ACPA) does not affect the clinical response to Adalimumab in a group of RA patients with the tumor necrosis factor (TNF) α-308 G/G promoter polymorphism. Clin Rheumatol. 2011;30(3):391–395. doi:10.1007/s10067-011-1679-4
42. Katchamart W, Koolvisoot A, Aromdee E, Chiowchanwesawakit P, Muengchan C. Associations of rheumatoid factor and anti-citrullinated peptide antibody with disease progression and treatment outcomes in patients with rheumatoid arthritis. Rheumatol Int. 2015;35(10):1693–1699. doi:10.1007/s00296-015-3271-8
43. Alten R, Nüßlein HG, Mariette X, et al. Baseline autoantibodies preferentially impact Abatacept efficacy in patients with rheumatoid arthritis who are biologic naïve: 6-month results from a real-world, international, prospective study. Rmd Open. 2017;3(1):e000345. doi:10.1136/rmdopen-2016-000345
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.