")
Back to Journals » Drug Design, Development and Therapy » Volume 15
The Clinical Efficacy of Three Different Follicle-Stimulating Hormones for Follicle Growth and Development in Long-Protocol Controlled Ovarian Hyperstimulation Treatment
Authors Zhang XQ, Zhang LJ, Zhu XL, Xu H, Luo YQ, Yao L, Huang QW, Nong YQ, Liu WJ, Liu FH
Received 16 April 2021
Accepted for publication 8 July 2021
Published 16 August 2021 Volume 2021:15 Pages 3573—3580
DOI https://doi.org/10.2147/DDDT.S316189
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Tin Wui Wong
Xi-Qian Zhang,* Li-Jia Zhang,* Xiu-Lan Zhu, Hong Xu, Yan-Qun Luo, Li Yao, Qian-Wen Huang, Ying-Qi Nong, Wen-Juan Liu, Feng-Hua Liu
Reproductive Medical Center, Guangdong Women and Children Hospital, Guangzhou, 511442, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Feng-Hua Liu
Department of Reproductive Medical Center, Guangdong Women and Children Hospital, No. 521 Xingnan Road, Panyu District, Guangzhou, 511442, Guangdong Province, People’s Republic of China
Tel +86 20-3915 1861
Fax +86 20-3915 1617
Email [email protected]
Objective: To compare the use and clinical efficacy of three different follicle-stimulating hormones (FSHs) for follicle growth and development in long-protocol controlled ovarian hyperstimulation (COH).
Methods: A total of 540 gonadotropin-releasing hormone (GnRH) agonists’ long protocol treatment cycles at our hospital between January 2015 and May 2020 and met the inclusion criteria were retrospectively analyzed. The cycles were divided into three groups based on their indexes (groups A, B, and C). Each of the groups received a different type of FSH during treatment. A cross-group comparison was then undertaken to evaluate the growth and development of the three largest follicles and the patients’ pregnancy-related indexes between the normal-response and high-response populations.
Results: In the normal-response populations, the number of high-quality embryos obtained in groups A and B was significantly higher than in group C, and the FSH dosage was significantly lower than in group C (P < 0.05). There were more follicles with a diameter of 16– 18 mm found in group A than in group C on the day of hCG injection (hCG day) (P < 0.05), but there were no significant differences in the groups in other indicators. In the high-response populations, the number of oocytes retrieved and high-quality embryos obtained in group A were significantly higher than in group C (P < 0.05), and the total dosage and duration of FSH stimulation in group C were significantly higher than groups A and B (P < 0.05).
Conclusion: Three different types of FSH led to comparable growth rates of the three largest follicles and clinical pregnancy rates per fresh cycle in long-protocol COH treatment.
Keywords: follicle-stimulating hormone, follicle growth rate, high-quality embryos, Gn stimulation duration, follicle distribution on hCG day
Introduction
With the rapid development of society, lifestyle changes, increased stress, and increased environmental pollution, infertility rates are increasing. Previous studies have found that the incidence of infertility in China has reached 12.5–15%.1,2 Controlled ovarian hyperstimulation (COH) is widely used in assisted reproductive techniques (ART), such as in vitro fertilization and embryo transfer.3,4 Human follicle-stimulating hormones (hFSHs) have become the primary therapeutic agent for COH in ART.5 These hormones induce multiple follicular production and maturation within a controlled range, expecting to obtain high-quality oocytes to improve clinical pregnancy rates. Currently, the most commonly used recombinant human FSHs (rFSHs) in China include the imported rFSH Gonal-f (Merck Serono, Switzerland), the domestic rFSH Jinsaiheng (GenSci, China), and the urinary FSH (uFSH) Lishenbao (Lizhu Pharmaceuticals, China). In order to provide a theoretical basis for clinical use, the present study compared the efficacy and application of these three FSHs by retrospectively analyzing follicular growth and development—indicated by the results of vaginal ultrasound monitoring—during COH.
Materials and Methods
Subjects
Patients who received COH treatment at Guangdong Women and Children’s Hospital between January 2015 and May 2020 were selected, with the first follow-up on the fifth day after receiving FSH, the second follow-up on day eight, and the third follow-up on day ten. The patients were organized into groups based on age, anti-Müllerian hormone (AMH) levels, antral follicle count (AFC), body mass index (BMI), and the FSH drug they were given. Those who had received Gonal-f became group A, those who had received Jinsaiheng became group B, and those who had received Lishenbao became group C. Then, based on their AMH levels, each group was further divided into a low-response population (AMH <1.1 µg/L), a normal-response population (AMH ≤1.1–≤4.5 µg/L), and a high-response population (AMH >4.5 µg/L). As the number of patients in the low-response population was insufficient, only the normal-response and high-response populations were compared. In total, 540 cycles were retrospectively analyzed, with 360 cycles in the normal-response populations and 180 cycles in the high-response populations. This study was conducted with approval from the Ethics Committee of Guangdong Women and Children’s Hospital. This study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Methods
The standard long-protocol COH was adopted for all patients. A single injection of GnRHa was administered after ovulation was confirmed by ultrasonography. When the luteinizing hormone (LH) level was lower than 5 mIU/mL, the estradiol (E2) level was lower than 50 pg/mL, and the endometrium was less than 5 mm, the patient was examined to confirm the absence of functional ovarian cysts. Ovulation was then promoted with FSHs (Gonal-f in group A, Jinsaiheng in group B, and Lishenbao in group C). The physician determined the initial dose of Gn based on each patient’s specific condition, and the dose was increased or decreased during the treatment based on observations during monitoring. When two or more follicles were more than 18 mm in diameter, hCG was injected at night, and the eggs were retrieved 34–36 hours later for in vitro fertilization/intracytoplasmic sperm injection–embryo transfer. Seventy-two hours after egg retrieval, patients received up to two transferable embryos. Luteal support was given after egg retrieval, and hCG was measured 14 days after the embryo transfer to determine biochemical pregnancy. Ultrasonography examination of the gestational sac or fetal heart was conducted approximately 30 days after embryo transfer to determine clinical pregnancy. In vitro fertilization or intracytoplasmic sperm injection was performed 4–6 hours after oocyte retrieval. Fertilization was observed 16–20 hours later. After embryo quality evaluation, 1–2 D3 embryos or one D5 or D6 blastocyst was selected for transfer. Luteal support was routine for 14 days after egg extraction.
Ultrasonography Monitoring
The vaginal ultrasound imaging was performed with the GE Voluson S8 (United States), and the transvaginal electronic convex probe used was the 8C-RS. The frequency was 4–10 MHz. Follicle monitoring for COH was based on the vaginal ultrasonography examination records. Due to the asynchronous growth of follicles during COH, the average diameter, in mm, of the three largest follicles at each follow-up and on the hCG day was recorded. The mean of the longest and shortest diameter of the follicles was taken as the average follicle diameter, referred to as the follicle diameter.
Observation Indicators
General Characteristics
The general characteristics of the patients in each group were observed, including age, AMH, ACF, BMI, basal FSH (bFSH), basal E2, basal LH, basal prolactin (PRL), years of infertility, and reasons for infertility.
The Growth and Development of the Three Largest Follicles During the COH in the Patients in Different Groups
The three largest follicle diameters of ovaries in each group were observed on the fifth, eighth, and tenth day monitored by follicular ultrasound examination.
Indicators of Clinical Therapeutic Efficacy, Safety, and Those Relevant to Medication
The indicators of clinical therapeutic efficacy, safety, and those relevant to medication included the number of eggs obtained, the number of high-quality embryos, metaphase II egg rate, embryo implantation rate, clinical pregnancy rate, early miscarriage rate, the incidence of moderate to severe ovarian hyperstimulation syndrome (OHSS), FSH total dosage, Gn stimulation duration, and follicle distribution on hCG day.
Definition of Terms
Implantation rate = number of gestational sacs/total number of embryos transferred × 100% (the number of gestational sacs of a single embryo transfer is only one)
Clinical pregnancy rate = number of clinical pregnant patients/number of patients (transplantation cycle) × 100%
Miscarriage rate = number of cycles canceled/number of cycles of start cycle treatment ×100%
Severe and moderate OHSS = number of medium and severe OHSS cycles/total treatment cycle of fresh stimulation cycle × 100%
Statistical Analysis
The SPSS software (version 23.0; IBM Corporation, Armonk, NY, USA) was used to conduct data analysis. The skewness coefficient, kurtosis coefficient, and normal single sample Kolmogorov–Smirnov test were used to judge whether the distribution was normal. The measurement data were expressed as mean ± standard difference (x ± s). One-way analysis of variance was used for data that conformed to a normal distribution, while a non-parametric test was used for data with non-normal distribution. Categorical variables were expressed as a percentage (%), and the χ2 test was adopted. P < 0.05 was considered statistically significant.
Results
The Normal-Response Populations
General Characteristics
There were no statistically significant differences in age, AMH, AFC, BMI, bFSH, and years of infertility between groups A, B, and C (Table 1).
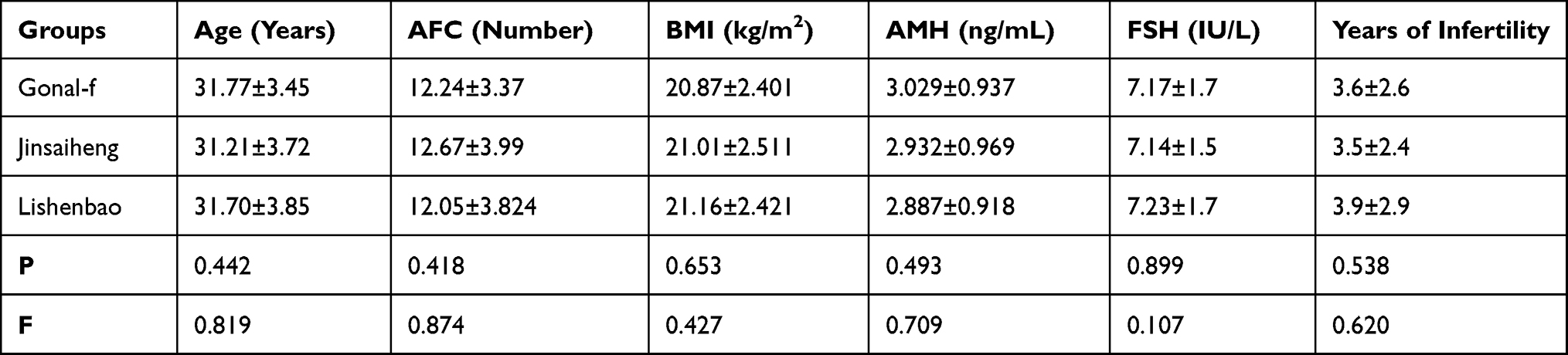 |
Table 1 The General Characteristics Among the Normal-Response Populations ( |

The Growth and Development of the Three Largest Follicles
The daily growth rates of the three largest follicles prior to the eighth day after COH were found to be fastest in group B, but the differences between the growth rates in this group, group A, and group C were not statistically significant. The average daily growth rate was also found to slow down after the eighth day. In terms of follicle size, there were no significant differences in the groups. Daily follicle growth rates and follicle sizes in each group are shown in Figure 1A–C.
 |
Figure 1 (A) The growth of the first-largest follicle in the normal-response group. (B) The growth of the second-largest follicle in the normal-response group. (C) The growth of the third-largest follicle in the normal-response group. |
Therapeutic Efficacy and Safety
The number of high-quality embryos obtained in groups B and A was significantly higher than in group C. The number of eggs obtained was highest in group A, but the difference was not statistically significant. The implantation rate and clinical pregnancy rate per fresh cycle were highest in group B, but the difference was not statistically significant. There were no significant differences in the miscarriage rate and the incidence of moderate to severe OHSS.
The Gn dosage and number of Gn days were highest in group C, but the difference was not statistically significant. The distribution of follicles on the hCG day, the number of follicles with a diameter >20 mm, and those with a diameter of 18–20 mm were higher in group B than in groups A and C, but the difference was not statistically significant. The number of follicles 16–18 mm in diameter in group A was significantly higher than in group C, but there was no difference between groups A and B. All indicators pertaining to therapeutic efficacy, safety, and drug-related indicators in the normal-response populations are shown in Table 2.
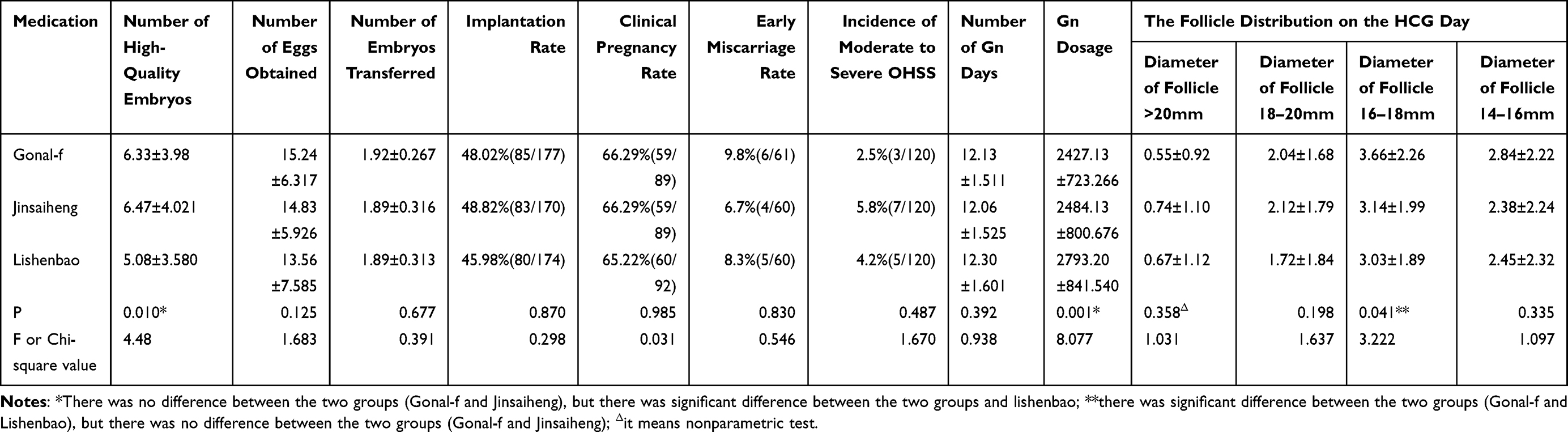 |
Table 2 The Therapeutic Efficacy and Safety Among the Normal-Response Populations |
The High-Response Populations
General Characteristics
There were no statistically significant differences in age, AMH, AFC, BMI, bFSH, and years of infertility between groups A, B, and C (as shown in Table 3).
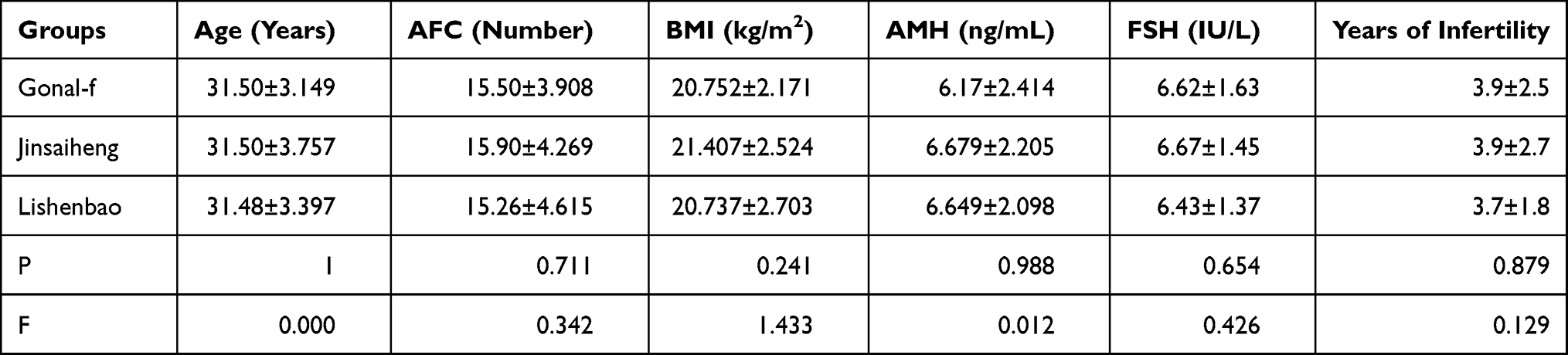 |
Table 3 The General Characteristics Between High-Response Group ( |

The Growth and Development of the Three Largest Follicles
The daily growth rates of the three largest follicles at different periods varied between the three groups, but there was no significant difference in final follicle size (see Figure 2A–C).
 |
Figure 2 (A) The growth of the first-largest follicle in the high-response group. (B) The growth of the second-largest follicle in the high-response group. (C) The growth of the third-largest follicle in the high-response group. |
Therapeutic Efficacy and Safety
The number of eggs obtained, the number of high-quality embryos, embryo implantation rate, clinical pregnancy rate, early miscarriage rate, the incidence of moderate to severe OHSS, FSH total dosage, Gn stimulation duration, and the distribution of follicles on the hCG day were analyzed in each group to compare the efficacy and safety of the three different FSHs.
The number of eggs and high-quality embryos obtained in group A was significantly higher than in group C, whereas the differences between the number of eggs and high-quality embryos obtained in group B and those from the other two groups were not statistically significant. The embryo implantation rate was the highest in group B, but the difference was not statistically significant.
The Gn dosage and number of Gn days were significantly higher in group C than in groups A and B. There were no statistically significant differences between the groups in the number of embryos transferred, the clinical pregnancy rate per fresh cycle, early miscarriage rate, and the incidence of moderate to severe OHSS. In terms of the distribution of follicles on the hCG day, the number of follicles with a diameter of 18–20 mm in group A was significantly higher than in group C, but there was no significant difference when compared with group B. There were also no significant differences in the distribution of follicles of other sizes. All indicators pertaining to therapeutic efficacy safety and drug-related indicators in the high-response populations are shown in Table 4.
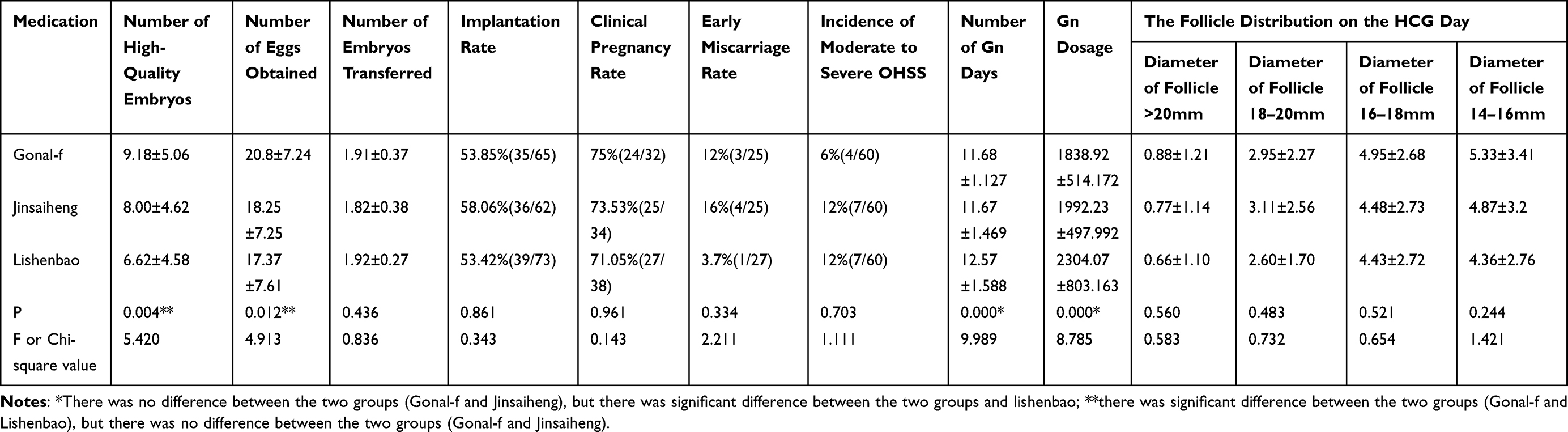 |
Table 4 Comparison of the Therapeutic Efficacy and Safety Among the High-Response Populations |
Discussion
Recombinant hFSH is the main ovulation-promoting drug used in ART. It can be categorized into two types, α and β, both of which are genetically engineered by inserting the DNA coding sequences encoding the α and β subunits of FSHs into the ovarian cells of Chinese hamsters. By preparing the FSHs with a biochemical purity of more than 99%, meaning the preparations do not contain LH activity, endogenous LH overload or early appearance of the LH peak can be avoided, and better efficacy and improved safety can be achieved.6,7 One study has shown that the new recombinant hFSH (FSH; DA-3801) is no less effective and safe than folliculin α in women treated with COH–ART.8 Jinsaiheng, administered via injection, is the first recombinant hFSH product to meet international quality standards. It is manufactured through advanced genetic engineering technology in China and has the same genes, expressed cells, molecular structure homogeneity, and uniformity of activity as Gonal-f.12,13
The application of GnRHa and human menopausal gonadotropins was first undertaken by Aboulghar et al9 in 1990 to successfully treat women with hypothalamic primary and secondary persistent amenorrhea and infertility. GnRHa stimulates the ovaries, increases FSH levels, and activates the follicular course. Recently, several comparative trials have shown that FSHs are as effective in this as human menopausal gonadotropin (hMG). In other words, the residual endogenous LH levels in GnRHa-treated cycles are usually sufficient to support FSH-induced follicular development, thus removing the co-administration of exogenous LH. In previous research, no significant differences have been found in the incidence of canceled cycles, oocyte retrieval failure rate, the average number of oocytes retrieved per person, fertilization rate, and embryo oogenesis rate between treatment with FSHs and treatment with hMG, but pregnancy rate and the incidence of miscarriage were relatively higher in women treated with hMG.10,11 However, even highly purified uFSH still contains a small amount of LH and less than 5% of urinary protein impurities.
In the present study, there were no statistically significant differences in the general characteristics of the patients in the three groups in both the normal-response populations and the high-response populations, which indicates that the clinical efficacies of the three drugs are sufficiently comparable. There were also no significant differences in clinical pregnancy rates in the normal-response populations. The number of high-quality embryos obtained in groups A and B was significantly higher than in group C. The Gn dosage in group C was significantly higher than in groups A and B, suggesting that a higher dosage of Lishenbao is required to achieve a comparable level of clinical efficacy. Furthermore, the number of good-quality embryos obtained in group C was relatively low.
In the normal-response populations, the implantation rate in group B was higher than in groups A and C, indicating that the embryos obtained following treatment with Jinsaiheng were of higher quality, which could be related to the production process and purity of the drug. It was also found that the growth of follicles promoted by Jinsaiheng in the normal-response populations was initially fast but slowed after eight days. From the distribution of follicle size on the hCG day, the number of follicles above 16 mm in diameter was lowest in group C, and the number of follicles between 16 and 18 mm in diameter was significantly lower in group C than in group A.
In the high-response populations, although there were no significant differences between the three groups in pregnancy rate per fresh cycle, the number of eggs and high-quality embryos obtained was significantly higher in group A than in group C and slightly higher in group B than in group C. The Gn dosage and number of Gn days were significantly higher in group C than in groups A and B, which indicates that treatment with Lishenbao resulted in fewer high-quality embryos at the maximum dose. The average daily growth rate of the three largest follicles and the final follicular size did not differ significantly between the three groups.
The findings of the present study are consistent with previous research, which has also identified no statistically significant differences in the clinical outcomes following treatment with Gonal-f and Lishenbao.14
The present study had some limitations. The fact that it was a retrospective study with a small sample may have influenced the results, and future studies need to expand the sample size. Future prospective randomized controlled studies with large samples should also be conducted to compare the differences between clinical ovulatory drugs. In addition, the effect of ovarian stimulation is also impacted by endometriosis and polycystic ovary syndrome, which are the current challenges.15,16 To date, many efforts are spent to identify a correct algorithm that considers a woman’s age and ovarian reserve markers as a tool to optimize the rFSH starting dose in IVF procedure. Nevertheless, current evidence regarding polycystic ovary syndrome in women, particularly those with high AMH, does not seem adequate.17,18
Conclusion
Compared with Gonal-f and Lishenbao, Jinsaiheng had a comparable follicle growth rate during ovulation and clinical pregnancy rate per fresh cycle, without a significant increase in miscarriage rate and risk of moderate to severe OHSS. It was also found to have the highest embryo implantation rate and the highest number of high-quality embryos in the normal-response populations. The number of high-quality embryos obtained from treatment with Lishenbao was significantly lower, the resulting implantation rate was the lowest of all the drugs, and the maximum drug dose was required to achieve comparable results.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Guangdong Women and Children Hospital. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
All participants signed a document of informed consent.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Wu J, Dong X, Liu K, et al. Association of semenogelin (SEMG) gene variants in idiopathic male infertility in Chinese-Han population. J Toxicol Environ Health A. 2019;82(16):928–934. doi:10.1080/15287394.2019.1669304
2. Wang LJ. Current status of cognitive behaviors and stress in patients with infertility based on Maslow’s hierarchy theory and the influencing factors. Chin J Health Psychol. 2019;27:64–67.
3. Nardo LG, Bosch E, Lambalk CB, Gelbaya TA. Controlled ovarian hyperstimulation regimens: a review of the available evidence for clinical practice. Produced on behalf of the BFS policy and practice committee. Hum Fertil (Camb). 2013;16(3):144–150. doi:10.3109/14647273.2013.795385
4. Rodgers RJ, Reid GD, Koch J, et al. The safety and efficacy of controlled ovarian hyperstimulation for fertility preservation in women with early breast cancer: a systematic review. Hum Reprod. 2017;32(5):1033–1045. doi:10.1093/humrep/dex027
5. van Wely M, Westergaard LG, Bossuyt PM, van der Veen F. Effectiveness of human menopausal gonadotropin versus recombinant follicle-stimulating hormone for controlled ovarian hyperstimulation in assisted reproductive cycles: a meta-analysis. Fertil Steril. 2003;80(5):1086–1093. doi:10.1016/S0015-0282(03)02187-3
6. Qiao J, Ma CH, Liu JY, et al. A consensus of poor ovarian response. Chin J Reprod Contracept. 2015;35:211–223.
7. Winstel R, Wieland J, Gertz B, Mueller A, Allgaier H. Manufacturing of recombinant human follicle-stimulating hormone ovaleap® (X M 1 7), comparability with G onal-f®, and performance/consistency. Drugs R D. 2017;17(2):305–312. doi:10.1007/s40268-017-0182-z
8. Moon SY, Choi YS, Ku SY, et al. Comparison of the efficacy and safety of a new recombinant human follicle-stimulating hormone (DA-3801) with follitropin-alpha (Gonal-F) in women undergoing controlled ovarian hyperstimulation for assisted reproductive technology. J Obstet Gynaecol Res. 2007;33(3):305–315. doi:10.1111/j.1447-0756.2007.00529.x
9. Aboulghar MA, Mansour RT, Serour GI, Ramzy AM. Successful treatment of infertile women with hypothalamic primary and secondary protracted amenorrhoea using gonadotrophin releasing hormone analogue and human menopausal gonadotrophin. Human Reprod. 1990;5(5):557–560. doi:10.1093/oxfordjournals.humrep.a137142
10. Yang TS, Wang BC, Chang SP, Ng HT. Comparison of human menopausal gonadotropin and follicle-stimulating hormone with gonadotropin-releasing hormone agonist desensitization for controlled ovarian hyperstimulation in in vitro fertilization. Zhonghua Yi Xue Za Zhi (Taipei). 1995;55:452–456.
11. Grøndahl ML, Borup R, Lee YB, Myrhøj V, Meinertz H, Sørensen S. Differences in gene expression of granulosa cells from women undergoing controlled ovarian hyperstimulation with either recombinant follicle-stimulating hormone or highly purified human menopausal gonadotropin. Fertil Steril. 2009;91(5):1820–1830. doi:10.1016/j.fertnstert.2008.02.137
12. Cao M, Wang JL, Wu YZ, et al. Advances in the development of recombinant human follicle-stimulating hormone. Pharm Biotechnol. 2014;21:86–90.
13. He YK, Xu W, Lu WY, et al. Clinical observation of domestic rhFSH and Gonal-f on ovulation promotion in patients with ovulation disorders. J Hainan Med Coll. 2010;16:417–420.
14. Liu XZ, Chen YW, Guo SS. A comparative study on the clinical application of two ovulation-promoting drugs. Contemp Med. 2020;26:26–27.
15. Šalamun V, Verdenik I, Laganà AS, Vrtačnik-Bokal E. Should we consider integrated approach for endometriosis-associated infertility as gold standard management? Rationale and results from a large cohort analysis. Arch Gynecol Obstet. 2018;297(3):613–621. doi:10.1007/s00404-017-4633-0
16. Facchinetti F, Espinola MSB, Dewailly D, et al. Expert group on inositols in preclinical and clinical research. Breakthroughs in the use of inositols for assisted reproductive treatment (ART). Trends Endocrinol Metab. 2020;31(8):570–579. doi:10.1016/j.tem.2020.04.003
17. Di Paola R, Garzon S, Giuliani S, et al. Are we choosing the correct FSH starting dose during controlled ovarian stimulation for intrauterine insemination cycles? Potential application of a nomogram based on woman’s age and markers of ovarian reserve. Arch Gynecol Obstet. 2018;298(5):1029–1035. doi:10.1007/s00404-018-4906-2
18. Peluso C, Oliveira R, Laporta GZ, et al. Are ovarian reserve tests reliable in predicting ovarian response? Results from a prospective, cross-sectional, single-center analysis. Gynecol Endocrinol. 2021;37(4):358–366. doi:10.1080/09513590.2020.1786509
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.