")
Back to Journals » Infection and Drug Resistance » Volume 14
The Clinical Characteristics of Fever-Ward Pediatric Patients with a Definite Epidemiological History During the Early COVID-19 Epidemic Period
Authors Song W , Li J, Zou N, Guan W, Pan J, Xu W
Received 24 June 2021
Accepted for publication 6 August 2021
Published 14 August 2021 Volume 2021:14 Pages 3175—3181
DOI https://doi.org/10.2147/IDR.S326279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Wenliang Song,1,* Junhua Li,2,* Ning Zou,1 Wenhe Guan,1 Jiali Pan,1 Wei Xu1
1Department of Pediatrics, Shengjing Hospital of China Medical University, Shenyang City, Liaoning Province, People’s Republic of China; 2Department of Pediatrics, Central Hospital of XiangYang City, Xiangyang City, Hubei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Xu
Department of Pediatrics, Shengjing Hospital of China Medical University, Shenyang City, Liaoning Province, People’s Republic of China
Email [email protected]
Objective: The number of children presenting with coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2 infection is increasing, and we aimed to assess the clinical characteristics of pediatric patients with a definite epidemiological history during the early COVID-19 epidemic.
Methods: Retrospective analysis was performed on the clinical data of children admitted to the fever ward of Xiangyang Central Hospital in Hubei province between January 1, 2020 and March 17, 2020. According to definite epidemiological history, patients with SARS-CoV-2 nucleic acid test (NAT) positive detection were grouped as confirmed cases, and patients with two consecutive negative NATs were grouped as suspected cases. We compared the clinical characteristics of the two groups.
Results: A total of 47 (47/127, 37%) cases had a definite epidemiological history, of which 32 (68.1%) were suspected, with a median age of 5.5 years (interquartile range [IQR]: 0.7– 10.3), and 15 (31.9%) were confirmed, with a median age of 9 years (IQR: 4– 14). Statistically significant differences in age, family cluster of infection, and numbers of patients with clinical symptoms and fever (P< 0.05) were found between the two groups, but no statistically significant differences in leucocyte and lymphocyte counts were observed (P> 0.05). Significant differences were found in the computed tomography (CT) manifestation of ground glass opacity (GGO) between the two groups (P< 0.05).
Conclusion: Children of older age and from family clusters of infection were more easily diagnosed as having COVID-19. GGO changes on chest CT was more likely in confirmed cases. Although obvious clinical manifestations increase our awareness of COVID-19, children without manifestations of fever or cough should not be ignored as they may be asymptomatic carriers.
Keywords: novel coronavirus disease, COVID-19, SARS-CoV-2, children, clinical manifestation
Introduction
Since December 2019, an outbreak of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) has spread in China and around the world.1–7 The World Health Organization has declared the COVID-19 epidemic a public health emergency of international concern8 and of pandemic status.9 Although people of all ages are susceptible to SARS-CoV-2 infection,4,10 the number of infections in children is much lower than adults, as is the severity of the disease.11,12 Evidence from increasing reports of pediatric cases13–17 suggests milder, atypical and nonspecific manifestations in children, when compared with adults. Furthermore, asymptomatic infections and low positivity rates from SARS-CoV-2 nucleic acid tests (NATs) in the early epidemic period made diagnosing pediatric COVID-19 difficult. During the epidemic, children with definite epidemiological history and obvious clinical manifestations have been considered as suspected cases of COVID-19 and finally confirmed according to NAT results. In the early stages of the epidemic, children with two consecutive negative NATs were diagnosed as suspected cases, and managed with little difference in treatment and quarantine between them and children with confirmed COVID-19. We were therefore interested in any differences in the epidemiology and clinical manifestations between these two groups, or specific clinical features that might lead us to pay closer attention to suspected patients. In this study, we retrospectively analyzed the clinical data of pediatric patients admitted to the fever ward to further assist in the diagnosis, prevention, and control of COVID-19 in children.
Materials and Methods
Patient Population
Clinical data were collected from children (aged from 1 month to 14 years) diagnosed as COVID-19 suspected cases or confirmed cases in the fever ward at Xiangyang Central Hospital in Hubei province of China between January 1, 2020 and March 17, 2020. We retrospectively analyzed the clinical features, laboratory tests, and chest computed tomography (CT) of pediatric patients with definite epidemiological history.
Diagnostic Criteria
All subjects met the diagnostic guidelines established in China, as stipulated in Diagnosis and Treatment Recommendation for Pediatric Coronavirus Disease-19 (second edition).18
The criteria for definite epidemiological history were as follows: (1) travel or residence in Wuhan area or other areas showing continuous local spread within 2 weeks of onset; (2) exposure within 2 weeks prior to fever or respiratory symptoms to Wuhan area or other areas where local spread was ongoing; (3) close contact with confirmed or suspected cases of COVID-19 within 2 weeks of onset; and (4) disease clusters, comprising patients (other than the child in question) with fever or respiratory symptoms suggesting or identified as COVID-19.
Qualifying clinical manifestations were as follows: (1) fever, fatigue, and dry cough, or fatigue and dry cough with no fever; (2) abnormal chest imaging (X-ray or CT); and (3) normal or low total leukocytes count or lymphopenia in the early phase of disease.
Pediatric patients with any of the definite epidemiological history criteria were grouped as either suspected cases: at least two related clinical provisions and two consecutive negative NATs, or as COVID-19 confirmed cases: at least two related clinical manifestations and NAT positive.
Data Collection
For the NAT, real-time quantitative polymerase chain reaction (RT-qPCR) was used, based on pharyngeal swab and performed 1 day before or on the day of CT imaging. Routine laboratory testing of blood count, C-reactive protein (CRP), biochemistry, and other factors was also completed 1–2 days prior to or on the day of CT imaging. During hospitalization, NAT was performed every other day until it showed negative.
Statistical Analysis
Continuous variables were expressed as medians and interquartile ranges or simple ranges, as appropriate. Categorical variables were described as counts and percentages. Chi-square test and Fisher’s exact test were used for categorical variables as appropriate and Mann–Whitney U-test was used for comparing median values of non-normally distributed variables. Analyses were conducted using Statistical Product and Service Solutions (SPSS 22.0) software. A two-sided α of less than 0.05 was considered statistically significant.
Results
Clinical Characteristics
A total of 47 (47/127, 37%) cases had a definite epidemiological history. Among them, 30 (63.8%) had fever, 21 (44.7%) had cough, 34 (72.3%) had abnormal chest CT, and 18 (38.3%) were from a family cluster of cases. These 47 cases were classified as either suspected or confirmed. The suspected group totaled 32 (68.1%) cases, including 16 (50%) males and 16 (50%) females, with a median age of 5.5 (0.7–10.3) years. There were 31 (96.9%) cases with obvious clinical symptoms, including 26 (81.3%) cases with fever, 17 (53.1%) cases with cough, 3 (3.1%) cases with sore throat, 1 (3.1%) case with runny nose, 1 (3.1%) case with vomiting, and 1 (3.1%) case with diarrhea. The confirmed group comprised 15 (31.9%) cases, including 9 (60%) males and 6 (40%) females, with a median age of 9 (4–14) years. Of these, 7 (46.7%) cases had obvious clinical symptoms, including 4 (26.7%) cases with fever and 4 (26.7%) with cough. There were no statistically significant differences between the two groups in terms of sex or clinical manifestations including cough, sore throat, runny nose, vomiting, and diarrhea (P>0.05); there were statistically significant differences in age, travel or residence in Wuhan, family cluster, and number of patients with clinical symptoms and fever (P<0.05). None of the children had symptoms of dyspnea, fatigue, or severe or critical symptoms. Details are shown in Table 1.
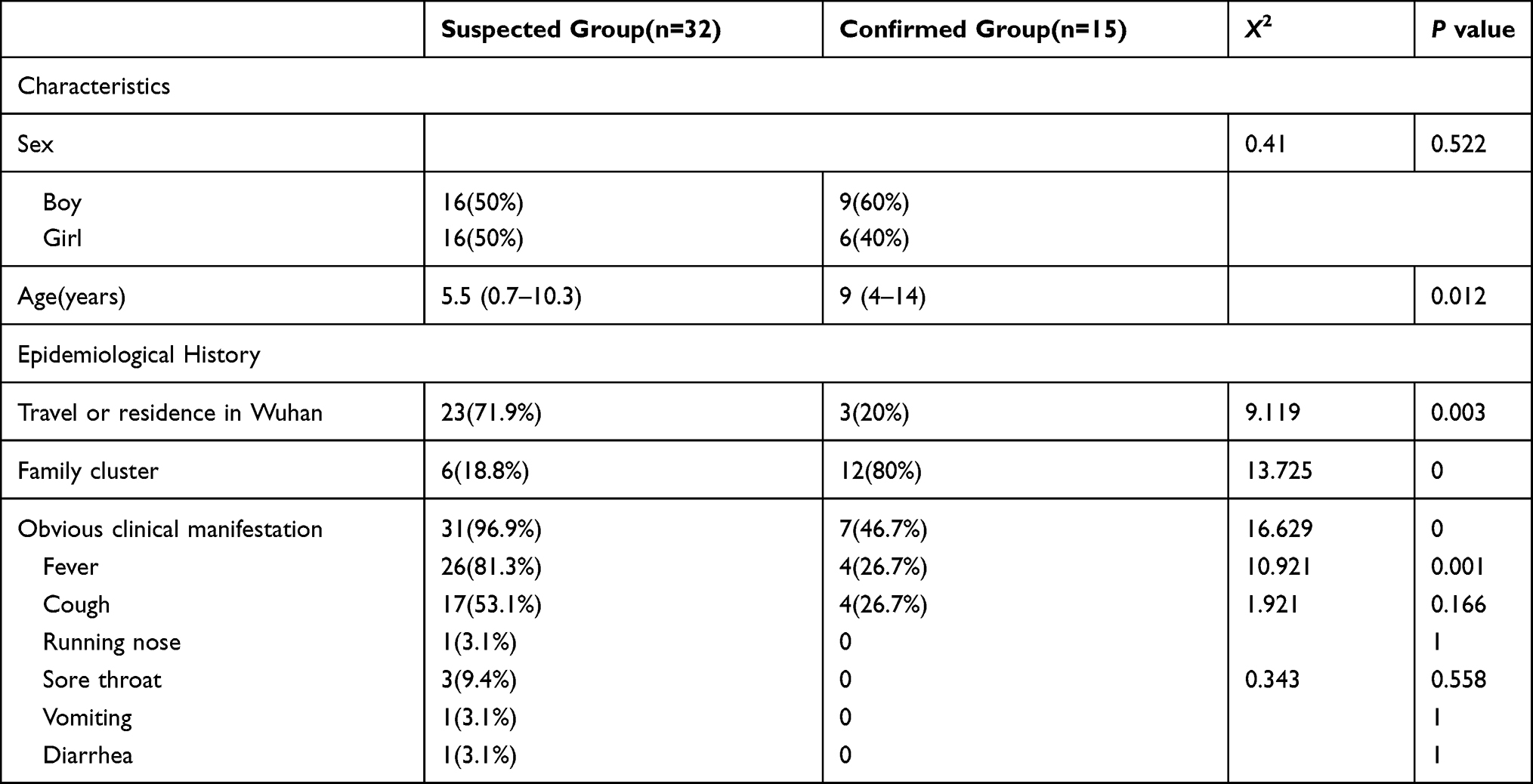 |
Table 1 General Characteristics of Suspected and Confirmed COVID-19 Patients |
Laboratory Findings
The white blood cell (WBC) counts in the suspected and confirmed groups were 8.15 × 109/L (5.76–10.54) and 6.04 × 109/L (3.36–8.72), respectively, and were not statistically significantly different between groups. Lymphocyte counts were 2.6 × 109/L (1.31–3.89) and 2.6 × 109/L (1.26–3.94) for suspected and confirmed groups, respectively; the difference between them was also not statistically significant. In addition, no statistically significant difference was observed in the proportion of patients with reduced or normal leucocytes and reduced lymphocytes between the two groups (P>0.05).
The differences in the proportions of patients with abnormal CRP, lactate dehydrogenase (LDH), erythrocyte sedimentation rate (ESR) and D-dimer were statistically significant between the suspected group (56.3%, 62.5%, 75%, and 35.7%, respectively) and the confirmed group (6.7%, 26.7%, 0%, and 0.0%, respectively; P<0.05). No significant difference was found in the proportions of children with abnormal glutamic oxaloacetic transaminase (AST), creatine kinase isoenzyme (CKMB) and procalcitonin (PCT) between the two groups (P>0.05). Renal function and creatine kinase (CK) were normal in all children. Details are shown in Table 2.
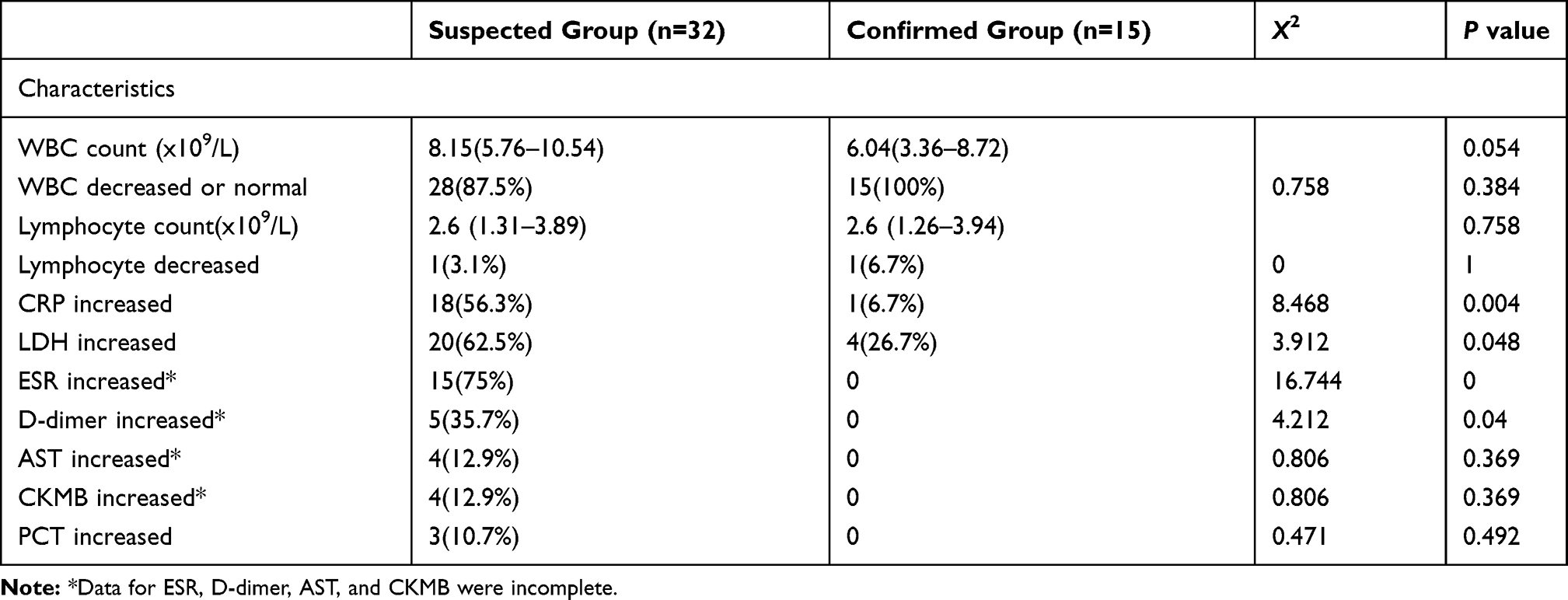 |
Table 2 Laboratory Findings of Suspected and Confirmed COVID-19 Patients |
Chest CT Findings
In the suspected group, 24 (75%) cases had chest CT abnormalities, including 16 (50%) with left lung involvement, 19 (59.4%) with right lung involvement, and 10 (31.3%) with both lungs involved. A total of 14 (43.8%) cases were patchy, 6 (18.8%) had bronchopneumonia, four (12.5%) had ground glass opacity (GGO), one (3.1%) had nodules, one (3.1%) had cord-like changes, one (3.1%) had fibrous lesion changes, and one (3.1%) had enlarged lymph nodes. In the confirmed group, there were 10 (66.7%) cases with chest CT abnormalities, including five (33.3%) with left lung involvement, seven (46.7%) with right lung involvement, and two (13.3%) with both lungs involved. Seven (46.7%) cases had GGO, six (40%) were patchy, 5 (33.3%) were nodular, and two (13.3%) had bronchopneumonia. No statistical difference was found between the two groups in the proportion of patients with CT abnormalities or the proportions with pulmonary lobe involvement or patchy changes (P>0.05); however, differences in CT manifestations of nodular shadow and GGO were statistically significant (P<0.05). Details are shown in Table 3.
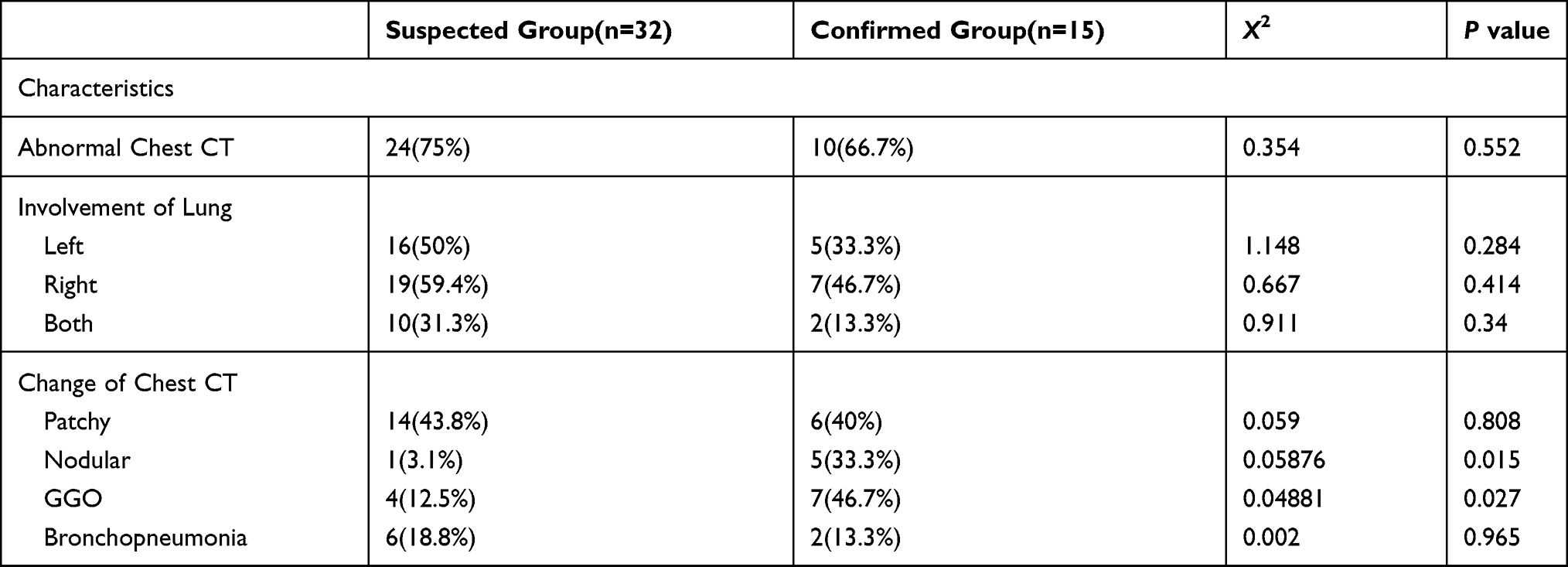 |
Table 3 Chest CT Findings of Suspected and Confirmed COVID-19 Patients |
Discussion
Positive NAT from throat and nose swabs or lower airway secretion is the gold standard for the diagnosis of COVID-19;18 however, NAT testing is time- and resource-consuming, and the positivity rate of the test is low, meaning a definite diagnosis cannot always be made on the first visit. Previous epidemiological data showed that 43% (26/61) of children with COVID-19 exhibited characteristics of infection from epidemic exposure and between 56% (34/61) and 90.1% (154/171) of children with COVID-19 demonstrated clear evidence of transmission through a family cluster,19,20 indicating the important role of epidemiological history. In this study, we analyzed the clinical characteristics of 47 pediatric patients with a definite epidemic history in order to provide useful and supplementary indexes for differentiating COVID-19 confirmed and suspected cases. Statistically, the two groups differed significantly in history of travel or residence in Wuhan, with the proportion of children with these characteristics in the confirmed group much lower than that in the suspected group. Therefore, a specific history of exposure to Hubei or Wuhan no longer seems to be a requisite for patients with the suspected disease to be diagnosed with COVID-19, especially now that the epidemic status in Hubei province is lifted and the global epidemic continues to spread. Detailed information showed that family clusters of disease were more common in the confirmed group (12/15, 80%) than in the suspected group (6/32, 18.8%), with statistical significance, which confirmed that close contacts with adults in the family is the main way that children become infected.
In our study, the median age of children confirmed with COVID-19 was 9 years, which was significantly older than the median age of 5.5 years in suspected cases, with no significant difference in sex between two groups. It has been accepted that people of all ages are susceptible to COVID-19, with no sex differences.15,21,22 Our results may be attributed to a low positivity rate using NAT detection in younger children. Difficulty in pharyngeal swab sampling or lower viral loads may add to the confusion. Somehow, children of older age were more easily singled out for COVID-19.
In our study, fever and cough were the main reasons for children visiting hospital. However, the proportion of children with fever was significantly lower in the COVID-19 confirmed group than in the suspected group, and the symptom of cough was not significantly different between the two groups. The high seasonal incidence of respiratory diseases2–4,23,24 such as influenza and respiratory syncytial virus infections may account for these results. In addition, an increasing number of asymptomatic infections being admitted to ward because of positive detection by NAT contributed to this. However, fever and cough are considered the most common initial clinical symptoms in COVID-19;15,21 thus, some of the 32 patients in the suspected group may have been infected with COVID-19 even with negative detection by NAT.
Although WBC counts in the confirmed group were lower than those in the suspected group, the difference was not statistically significant; neither was the proportions of patients with reduced or normal leucocytes and with reduced lymphocytes, between the two groups. The median value for lymphocytes was the same between the two groups, with only one case of lymphopenia. Lymphopenia reflects the consumption of lymphocytes by SARS-CoV-2 and signals severe disease.1,3,4 It may account for milder or less severe symptoms in children with COVID-19, but does not provide strong diagnostic support. However, it can serve to exclude other pathogens to some extent. The proportions of children with abnormal CRP, LDH, ESR, and D-dimer in the confirmed group were statistically lower than those in the suspected group. Although these indexes are commonly abnormal in adults with COVID-19, especially in severe cases,1–4 indicating more intense inflammatory reaction and more serious organ injury, these changes are less often seen in pediatric COVID-19,13,25 and lack specificity because of coinfection.24
Patchy consolidation and GGO were the most common radiographic features. GGO is a known feature of COVID-1920,21 and our study also demonstrated this. However, patchy consolidation was also common in the suspected group, and cannot be differentiated as a typical feature. Besides, children who did not have symptoms of infections or radiological features of pneumonia accounted for 25.0% and 33.3% in the suspected and confirmed groups, respectively. Furthermore, we found no statistically significant differences between the two groups in other CT abnormalities, lung involvement, and other lung changes, such as consolidation and pleural effusion, which are commonly seen in adults with COVID-19. In other words, the CT manifestations of children with COVID-19 shared many common features with pneumonia caused by other pathogens such as influenza virus, parainfluenza virus, adenovirus, SARS-CoV, mycoplasma, chlamydia, and bacterial infection, and they may even present with no chest abnormalities, increasing the difficulty of diagnosis on the initial clinical visit.
As far as we know, even if the early-stage NAT is negative, some patients may be finally confirmed as having COVID-19. SARS-CoV-2 can be positively detected after a long period, as a result of prolonged viral shedding in feces, or in the form of immunoglobulin such as IgM or IgG antibody, which can be used as a tool for delayed or retrospective diagnosis.26–28
There were several limitations to our study. First, it was a retrospective, single-center study with a small sample of patients and the characteristics of all suspected patients could not be reflected. Second, some pathogenic tests were not carried out due to biosafety issues during the epidemic period. Finally, we did not perform serological tests due to a lack of materials in the early epidemic period. Finally, in the early epidemic period, triage system was not perfect and needed continual improvement. Telephone triage gives us a new direction for combating COVID-19.29
Conclusions
Children of older age and with family clusters of infection were more easily diagnosed with COVID-19, and chest CT GGO changes were more often seen in confirmed cases. Laboratory tests of WBC, lymphocytes, CRP, ESR, LDH, and D-dimer helped in differential diagnosis to some extent. Nevertheless, their use as a basis for early clinical diagnosis of COVID-19 was not credible. Furthermore, although obvious clinical manifestations increased our awareness of COVID-19, children without manifestations of fever or cough should not be ignored as they are asymptomatic carriers. Thus, we recommend strict medical quarantine and observation of all patients with suspected COVID-19 in dedicated quarantine facilities for the diagnosis, prevention, and control of COVID-19.
Abbreviations
COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; NAT, SARS-CoV-2 nucleic acid test; CT, computed tomography; GGO, ground glass shadow; IQR, Interquartile range; RT-qPCR, Real-time quantitative PCR; WBC, white blood cell; CRP, C-reactive protein; LDH, lactate dehydrogenase; ESR, erythrocyte sedimentation rate; AST, glutamic oxaloacetic transaminase; CKMB, creatine kinase isoenzyme; PCT, procalcitonin; ALT, glutamic-pyruvic transaminase.
Data Sharing Statement
The datasets are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This work was in accordance with the protocols of ethical committees of Xiangyang Central Hospital for clinical retrospective study (No.2021-021). Oral consent was obtained from the legal guardians in this study. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The author thank all the team members of this review for corporation.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81771621), the Natural Science Foundation of Liaoning Province (No. 2019JH8/10300023).
Disclosure
All authors declare no conflict of interest.
References
1. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
2. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
3. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
4. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
5. Zhang JJ, Dong X, Cao YY, et al. Clinical characteristics of 140 patients infected by SARS-CoV-2 in Wuhan, China. Allergy. 2020;75(7):1730–1741. doi:10.1111/all.14238
6. The International Committee on Taxonomy of Viruses (ICTV) Coronaviridae Study Group. Naming the 2019 coronavirus. Available from: https://talk.ictvonline.org/.
7. World Health Organisation. Novel coronavirus (2019-nCoV) situation report – 22. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200211-sitrep-22-ncov.pdf?sfvrsn=fb6d49b1_2.
8. World Health Organization.WHO director-general’s statement on ihr emergency committee on novel coronavirus (2019-nCoV). Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-statement-on-ihr-emergency-committee-on-novel-coronavirus-(2019-ncov).
9. World Health Organization. WHO characterizes COVID-19 as a pandemic. Geneva, Switzerland; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen.
10. Shen KL, Yang YH. Diagnosis and treatment of 2019 novel coronavirus infection in children: a pressing issue. World J Pediatr. 2020;16(3):219–221. doi:10.1007/s12519-020-00344-6
11. WHO-China Joint Mission. Report of the WHO-China joint mission on coronavirus disease 2019 (COVID-19). Geneva; 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-jointmission-on-covid-19-final-report.pdf.
12. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72,314 cases from the chinese center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
13. Wang D, Ju XL, Xie F, et al. Clinical analysis of 31 cases of 2019 novel coronavirus infection in children from six provinces (autonomous region) of northern China. Zhonghua Er Ke Za Zhi. 2020;58(4):269–274. doi:10.3760/cma.j.cn112140-20200225-00138
14. Sun D, Li H, Lu XX, et al. Clinical features of severe pediatric patients with coronavirus disease 2019 in Wuhan: a single center’s observational study. World J Pediatr. 2020;16(3):251–259. doi:10.1007/s12519-020-00354-4
15. Dong Y, Mo X, Hu Y, et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145(6):e20200702. doi:10.1542/peds.2020-0702
16. Xia W, Shao J, Guo Y, et al. Clinical and CT features in pediatric patients with COVID-19 infection: different points from adults. Pediatr Pulmonol. 2020;55(5):1169–1174. doi:10.1002/ppul.24718
17. Li W, Cui H, Li K, et al. Chest computed tomography in children with COVID-19 respiratory infection. Pediatr Radiol. 2020;50(6):796–799. doi:10.1007/s00247-020-04656-7
18. Chen Z, Jf FU, Shu Q, et al. Diagnosis and treatment recommendation for pediatric coronavirus disease-19 (second edition). Zhejiang Da Xue Xue Bao Yi Xue Ban. 2020;49(1):139–146. doi:10.3785/j.issn.1008-9292.2020.02.01
19. Fang F, Luo XP. Facing the pandemic of 2019 novel coronavirus infections: the pediatric perspectives. Zhonghua Er Ke Za Zhi. 2020;58(2):81–85. doi:10.3760/cma.j.issn.0578-1310.2020.02.001
20. Lu X, Zhang L, Du H, et al. SARS-CoV-2 Infection in Children. N Engl J Med. 2020;382(17):1663–1665. doi:10.1056/NEJMc2005073
21. Chang T-H, Wu J-L, Chang L-Y. Clinical characteristics and diagnostic challenges of pediatric COVID-19: a systematic review and meta-analysis. J Formos Med Assoc. 2020;119(5):982–989. doi:10.1016/j.jfma.2020.04.007
22. Zheng F, Liao C, Fan QH, et al. Clinical characteristics of children with coronavirus disease 2019 in Hubei, China. Curr Med Sci. 2020;40(2):275–280. doi:10.1007/s11596-020-2172-6
23. Liu W, Zhang Q, Chen J, et al. Detection of Covid-19 in children in early January 2020 in Wuhan, China. N Engl J Med. 2020;382(14):1370–1371. doi:10.1056/NEJMc2003717
24. Jiang S, Liu P, Xiong G, et al. Coinfection of SARS-CoV-2 and multiple respiratory pathogens in children. Clin Chem Lab Med. 2020;58(7):1160–1161. doi:10.1515/cclm-2020-0434
25. Henry BM, Lippi G, Plebani M. Laboratory abnormalities in children with novel coronavirus disease 2019. Clin Chem Lab Med. 2020;58(7):1135–1138. doi:10.1515/cclm-2020-0272
26. Zhang T, Cui X, Zhao X, et al. Detectable SARS-CoV-2 viral RNA in feces of three children during recovery period of COVID-19 pneumonia. J Med Virol. 2020;92(7):909–914. doi:10.1002/jmv.25795
27. Qu J, Wu C, Li X, et al. Profile of IgG and IgM antibodies against severe acute respiratory syndrome coronavirus 2(SARS-CoV-2). Clin Infect Dis. 2020;71(16):2255–2258. doi:10.1093/cid/ciaa489
28. Pan Y, Li X, Yang G, et al. Serological immunochromatographic approach in diagnosis with SARS-CoV-2 infected COVID-19 patients. J Infect. 2020;81(1):e28–e32. doi:10.1016/j.jinf.2020.03.051
29. Gabriele C, Giacomo O. COVID-19 pandemic and telephone triage before attending medical office: problem or opportunity? Medicina (Kaunas). 2020;56(5):250. doi:10.3390/medicina56050250
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.