")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 10
The Burden Of Visits For Fever At A Paediatric Emergency Room: A Retrospective Study On Patients Presenting At The Cantons Hospital Of Fribourg, A Peripheral Public Hospital Of Switzerland
Received 20 June 2019
Accepted for publication 23 October 2019
Published 15 November 2019 Volume 2019:10 Pages 147—152
DOI https://doi.org/10.2147/PHMT.S219759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Sarah Piller, Denise Herzog
Department of Paediatrics, Cantons Hospital of Fribourg, Fribourg, Switzerland
Correspondence: Denise Herzog
Department of Pediatrics, Cantons Hospital of Fribourg, Chemin Des Pensionnats 2-6, 1700, Fribourg, Switzerland
Tel +41 26 306 3510
Fax +41 26 306 3519
Email [email protected]
Introduction: Fever is the chief complaint of up to one-third of all paediatric office visits in many places. The high number of consultations at our emergency department (ED) led us to hypothesise that this increase was due to febrile paediatric patients with lower urgency seeking medical advice.
Methods: We retrospectively analysed the number and characteristics of patients 3 months to 5 years of age consulting for a body temperature of 38.5°C or higher during the 6 winter months of 2011–2012.
Results: Twenty-four percent of all consultations were requested by the patients included in our group. None of the 835 patients had to be hospitalised, 95% of these patients had additional respiratory or gastrointestinal symptoms, 36.7% required antibiotic therapy, and 17.6% (laryngitis and lower respiratory tract infection (RTI)) required temporary respiratory support. A total of 56.2% of patients sought advice outside of the normal working hours.
Conclusion: The majority of patients had fever accompanied by additional symptoms justifying a medical consultation. However, most of these did not require the infrastructure of an ED for their health care problem and probably visited the ED because of the open hours.
Keywords: fever, emergency department, child, infection
Introduction
Fever is the chief complaint in up to one-third of all paediatric office visits in many countries. Previous studies have reported that many parents are unable to determine the normal temperature for their child, and this is the reason they are excessively concerned about the harm that they expect to be associated with fever, such as brain damage and seizures. In the USA, it has been reported that overly zealous, potentially harmful home practices and unnecessary emergency department (ED) visits for the assessment and treatment of fever in children are widespread. In Australia, children under 5 years of age are among the highest users of EDs, and approximately two-thirds of presentations of children are classified as having lower urgency, raising the question of whether a meaningful proportion of paediatric ED presentations may be more appropriately cared for in less-urgent primary care settings.1–3
The term “fever” basically represents an elevated body temperature above the normal physiological range of 36.5°C to 37.5°C.4,5 Young children are particularly affected by febrile illnesses, and hospital-based studies as well as a recent population-based study suggest that boys are more affected by infections than girls.6,7
Rectal temperature is considered to be the most accurate for estimating core body temperature and is recommended by the American Academy of Paediatrics for children less than 4 years of age. However, its use is discouraged by other clinical guidelines because of safety and practical issues, as well as for the physical and psychological discomfort it may cause. Current pediatric guidelines recommend paracetamol 15–20 mg/kg/dose every 4–6 hrs to alleviate the discomfort associated with febrile body temperatures.3
Our ED, open for children 0 to <17 years, is the only paediatric ED for the over 250,000 inhabitants of Canton Fribourg, a rural region. Between 2010 and 2017, the number of consultations per year increased from 6000 to 17,000, as the consequence of a recent economic immigration of young Swiss and foreign families to a region where life has remained more affordable than in other parts of Switzerland, of an increased birth rate and an unaltered offer of primary care settings. For our ED this demographic change resulted in an increased number of the same type of patients and disorders as before.
Because of the increasing demand for consultations at the ED, and to evaluate the need for an out-of-hour primary care practice in the same building, as already in operation in adult EDs, we decided to assess the number and type of patients consulting with fever. Our hypothesis was that we would have as many consultations for febrile paediatric patients with lower urgency as other paediatric EDs.2,9–11
The primary outcome of our retrospective study was the evaluation of the number of patients between 3 months and 5 years of age consulting the ED for fever, and the secondary outcomes were the rate of health conditions found to be causative for or possibly related to this febrile state, the need for antibiotic therapy and antipyretic therapy given before or during the consultation and prescribed at dismissal or transfer to hospitalisation, and lastly the evaluation of the necessity to consult at an ED rather than an office of the primary care setting.
Methods
This was a retrospective observational study reviewing charts of children presenting at the ED of the Cantons Hospital of Fribourg, a peripheral public hospital, between October 1, 2011 and March 31, 2012, including children aged 3 months to ≤5 years, with body temperature ≥38.5°C, or lower as measured at the ED but under antipyretic effect given within 8 hrs before their visit to the ED for fever ≥38.5°C, and treated as outpatients. Children >5 years of age, children with normal or sub-febrile body temperature without antipyretic therapy during the 8 hrs preceding the consultation, children suffering from a chronic disease and under ongoing treatment, and children for whom body temperature, weight or age data were lacking were excluded.
Because of the long interval between the mainly unique consultations at the ED, because our ED does not offer follow-up consultations, and because domicile addresses are not updated by the administration of our hospital, the local ethics committee approved the study protocol without requesting written consent from the patients whose records we analysed. The following data were retrieved from the patient records, and recorded on a standardized collection form using Windows Excel, 2010: date and hour of consultation, the patient’s age calculated from date of birth, the duration of fever before the consultation (date, time and body site of temperature measurement, and measured temperature), the dose, the date and the time of the administration of antipyretics. At the ED, vital signs and body temperature, weight, weight z-score, and doses of antipyretics given at the ED before the examination by the physician, as well as the final diagnosis and antipyretic therapy prescribed before discharge or transfer to hospitalisation, were recorded.
Body temperature at our ED is taken using a device measuring the body temperature at the eardrum in children. A body temperature of ≥38.5°C is defined as the limit for the nurses to administer paracetamol without prescription by the physician. A body temperature of ≥38.5°C reported by parents and measured at home is considered fever, a limit that is communicated to the parents by their paediatrician. Antipyretics are administered according to the guidelines published in Paediatrica.12
To calculate z-scores, the CDC/NCHS Infant Weight for Age calculators13–15 were used.
Statistics
For the analyses, we used descriptive statistics such as percentages for categorical and medians and 95% confidence intervals or means and standard deviations for continuous data. Groups were compared using the chi-square test for categorical and Gaussian data and the Mann–Whitney U-test for continuous non-Gaussian data. For the purpose of the present study, a p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS statistics 23.0 (IBM, Armonk, New York, USA).
Results
Of 4936 visits to the paediatric ED between October 1, 2011 and March 31, 2012, 1182 (24%) children ≥3 months to ≤5 years of age sought medical advice for fever ≥38.5°C or lower as measured at the ED but under antipyretic effect given within 8 hrs before their visit to the ED for fever ≥38.5°C. After exclusion of 347/1182 charts for incomplete data, and 587 (11.9%) children consulting with sub-febrile body temperature (37.6°C to 38.4°C), 835 charts could be analysed. For patient characteristics, see Table 1.
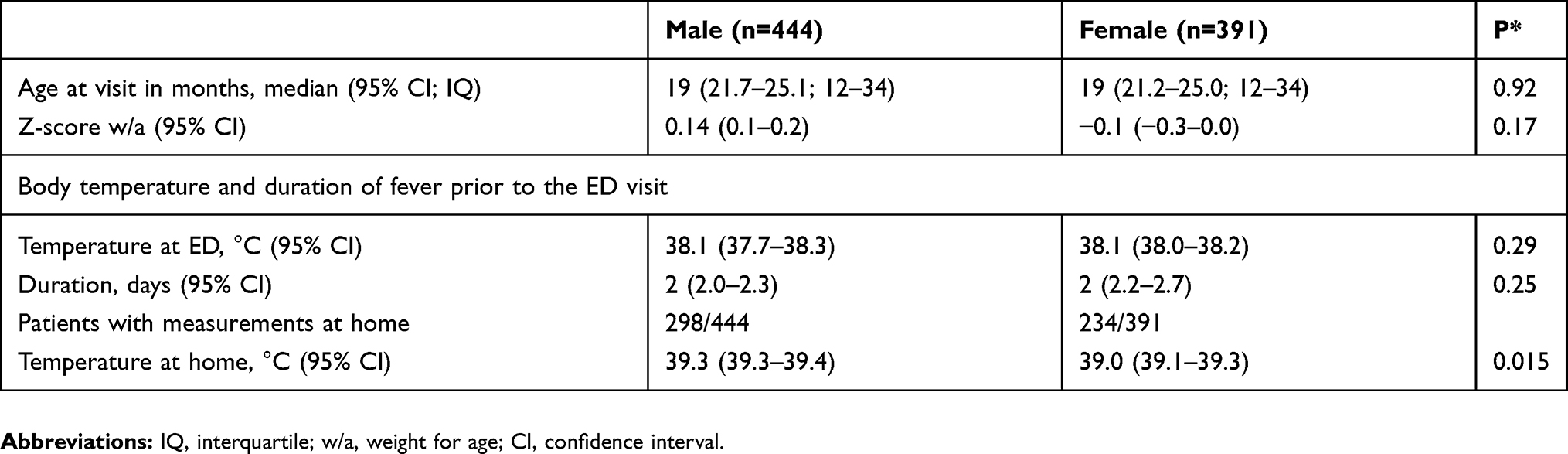 |
Table 1 Characteristics Of The Patients |
There were more male than female patients (47% female and 53% male, p=0.01), but the age distribution was similar for both groups. The z-scores for weight for age were approximately 0 in both groups, thus representing patients with normal growth. None of the patients required hospitalisation.
Febrile temperatures measured at home were noted in the charts of more boys (67%) than girls (59.9%, p=0.03), and the body temperature of female patients measured at home was lower than that of boys. The fact that fewer female patients visited the ED and fewer had exact body temperature recorded in their charts made it difficult to interpret this sex difference (Table 1).
The duration of fever before the visit to the ED was a maximum of 2 days in 61.2% and 65.5% of patients with acute otitis media and upper respiratory tract infection (RTI), respectively. In 64.3%, 61% and 53.4% of cases with laryngitis, fever of unknown origin (FUO) or acute gastroenteritis, respectively, the patients presented at the ED within 24 hrs of the increase in body temperature. The duration of fever was similar in female and male patients (Table 1).
Body temperature as measured at the ED was similar in both sexes (Table 1). Because no ATS scales were available for the years of our analysis and none of the patients were admitted to inpatient care, we attributed an ATS score of 3 to patients presenting with laryngitis (5%) and lower RTI (12.6%) and ATS scores of 4 and 5 to the remaining patients (82.4%).
Except for a small number of mainly female patients with acute gastroenteritis and acute pyelonephritis, there was no difference between female and male patients for the prevalence of additional symptoms. Acute bronchitis, acute gastroenteritis, and acute pyelonephritis occurred in the youngest patients of both sexes. For the additional symptoms associated with fever, see Table 2, and for the prevalence of these disorders at different ages see Figure 1.
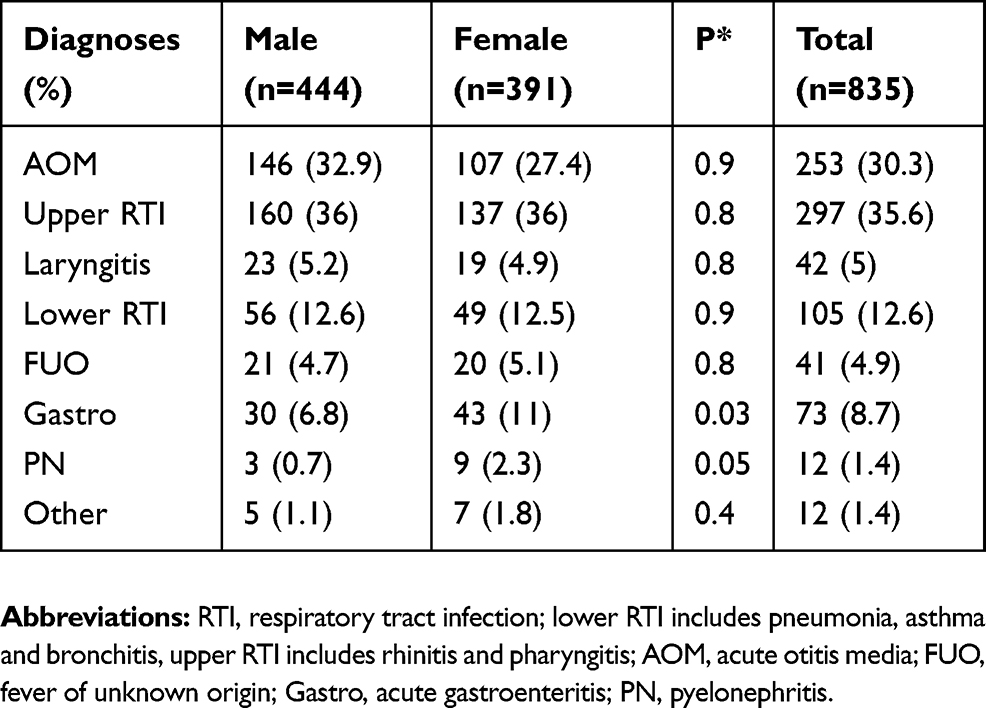 |
Table 2 Final Diagnoses Of The Febrile Patients |
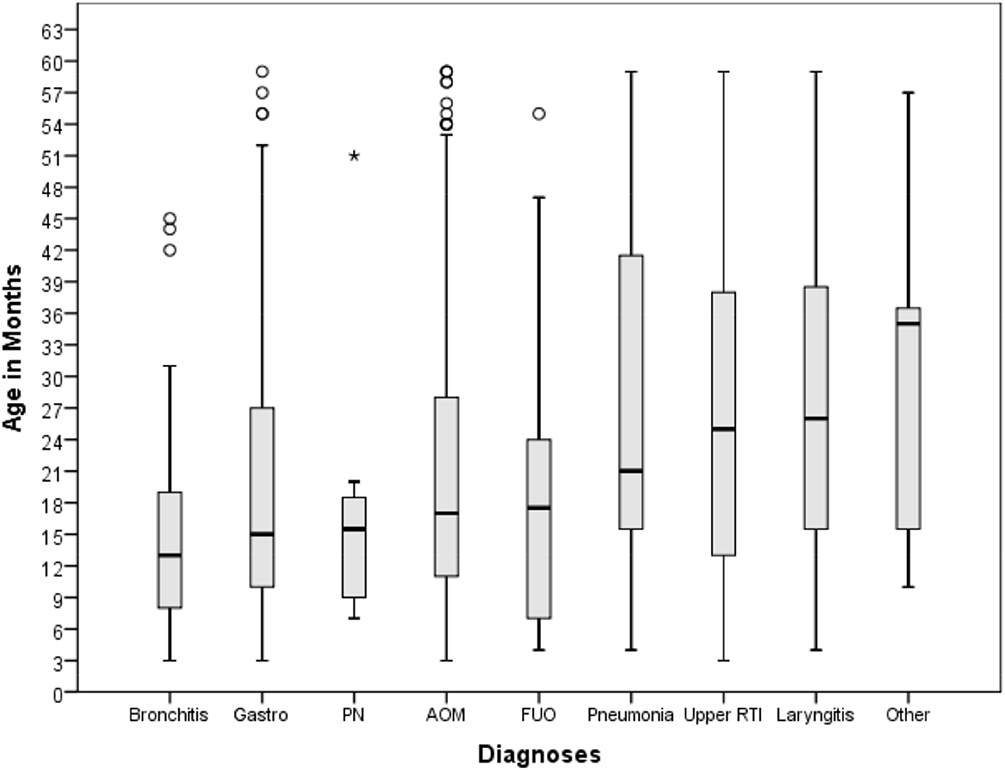 |
Figure 1 Median age and 95% confidence interval for each additional diagnosis and ages of the patients presenting at the ED with fever. Abbreviations: PN, pyelonephritis; AOM, acute otitis media; FUO, fever of unknown origin; RTI, respiratory tract infection. |
Antibiotic therapy was prescribed at discharge for 195 (77.1%) patients with acute otitis media, for 78 (100% of those with pneumonia) with lower RTI, and for 12 (100%) with acute pyelonephritis (PN), representing 63.7%, 25.5%, and 3.4% of all antibiotic prescriptions, respectively. Most antibiotics were prescribed in patients 6 to 23 months of age (in 30.3–57.9% of patients of these ages). No difference between male and female patients was found for antibiotic prescription (160 male (36%) and 146 female (37.3%) patients, p=0.38) (Table 3).
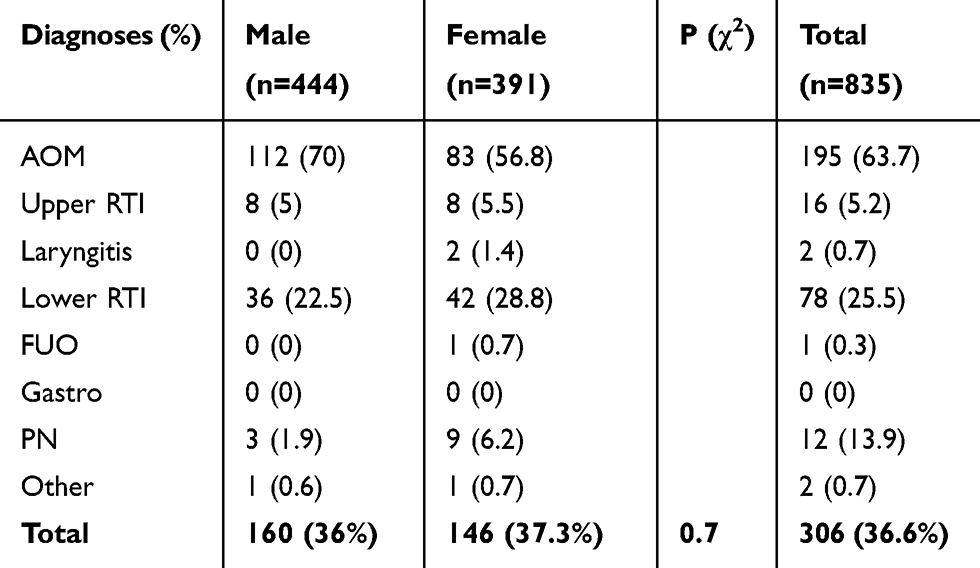 |
Table 3 Number Of Patients Prescribed Antibiotics For A Specific Diagnose |
At the ED, antipyretic medication was administered to 97 patients with acute otitis media and 111 with upper RTI, representing 60.1% of all antipyretics prescribed at the ED (28.5% of patients with acute otitis media (AOM) and 32.6% with upper RTI).
At discharge, 159 patients with otitis media and 259 with upper RTI were prescribed antipyretic medication for administration at home, representing 68.9% (26.2% and 42.7%, respectively) of all prescriptions of antipyretics at discharge (Table 4).
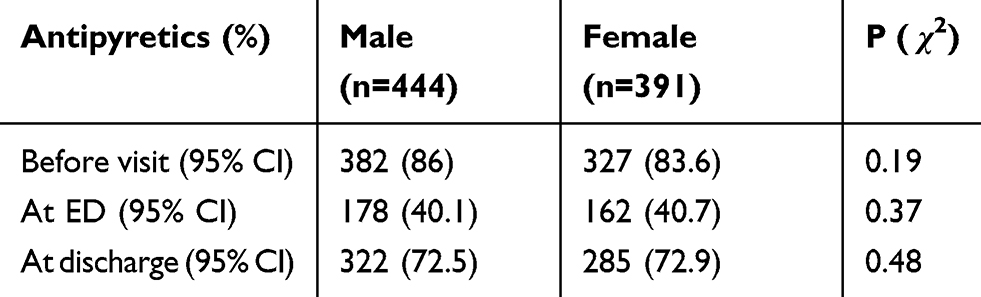 |
Table 4 Administration Of Antipyretics* |
Out-of-hour visits took place between 5 and 23 pm in 44.2% of patients and between 11 pm and 7 am in 12%, whereas only 43.8% of the patients sought advice during regular working hours, i.e., between 7 am and 5 pm.
Discussion
Fever as a marker of disease and as a primary motive for parents to seek medical advice at the ED accounted for 24% of all visits during the period analysed. In comparison to data published by other paediatric EDs, such as from Cambridge, UK where visits of children with elevated body temperature accounted for 27.5%, or from Trieste, Italy, where these accounted for 24.6% of the visits of 1 to <5 years old children,16 an Australian paediatric ED, with 1.6% of all children <6 years presenting with elevated body temperature,2 two EDs from the Netherlands and one from the UK, with 19.4%, 6% and 2% of the children 1 month to 15 years old presenting with fever,10 and an ED from the UK, including febrile children 0.5 to <6 years with 30.8%11 of their visits, our burden lies within the reported range. However, as our study had the most stringent inclusion criteria, including patients 3–60 months of age, a body temperature ≥38.5°C only, and only during winter months, the comparability of our results with these studies may be questioned.
The great majority of our patients presented one or more additional symptoms, and only 4.9% of the patients consulted with fever as the sole complaint. Most patients with additional symptoms were very young, e.g., between 12 and 34 months of age. Their complaints concerned the upper respiratory, the middle ear, the lower respiratory tract, and less frequently intestinal or laryngeal symptoms. Similar rates of additional symptoms have been described by others.2,16
As a measure of severity of the illnesses, we analysed the rate of prescription of oral antibiotics. Antibiotic medication had to be prescribed in 36.7% of our patients. In comparison to a Dutch study9 reporting the prescription of antibiotics in 27.5% of children 1–5 years old at an out-of-hours service and an Australian study2 where this medication was necessary in 2.7% of the children managed as outpatients, our rate is rather high and probably the result of our inclusion criteria for body temperature, age, and season.
When looking separately at the single features analysed, each rate appears comparable to those reported by other paediatric EDs. However, the patient group described in our study differs not only because of the inclusion criteria.
There was a high use of antipyretic medication before visiting the ED, showing that parents are able to recognise fever, and that they try to alleviate the discomfort associated with fever prior to seeking medical advice, an attitude resulting in a certain pre-selection. Other centres reported the use of antipyretics in 52% of children with temperature 38°C to 39°C at the ED8 or in 53.4% prior to and in 75.8% during the visit at the ED.2
Lastly, out-of-hour consultations occurred in 56.2% of our patients, representing a similar frequency compared to results reported by an Italian centre with 57%17 and a Dutch centre with 89.5%.9
In summary, the burden of children consulting with ≥38.5 body temperature in our centre is high, even more so when considering our restrictive inclusion criteria and the well-informed parents. Nearly all children had more than one additional symptom, and final diagnoses such as AOM with pain or RTI, with parents alarmed about pain or respiratory symptoms, entirely justified these consultations. However, none of our patients required hospital treatment, and most of them could have been seen in the primary care setting and did not require the infrastructure of an ED. The high number of out-of-hour consultations suggests more an organisational problem, such as restrictive open hours of the doctor’s offices and an insufficient number of primary care settings. Additionally, the ease of access to the ED also results from the indiscriminate coverage of expensive consultations at the ED and less costly consultations at the practitioner’s office by the insurances. Lastly, we included only patients with ≥38.5 body temperature, even though another 11.9% (a total of 537 patients) of all consultations were for children with sub-febrile body temperatures. Analysing this latter patient group and other types of complaints motivating an ED visit may finally justify the separation of the patient influx into children directed to a primary care office and patients who need to be treated to the ED.
Abbreviations
ED, emergency department; SBI, severe bacterial infection; ATS, Australian triage score.
Ethics Approval
Ethics Committee Vaud, CER-VD No 2018-02030, Switzerland.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Elkon-Tamir E, Rimon A, Scolnik D, Glatstein M. Fever phobia as a reason for pediatric emergency department visits: does the primary care physician make a difference? Rambam Maimonides Med J. 2017;8(1):e0007. doi:10.5041/RMMJ.20769172
2. Bereznicki BJ, Tucker MG, Beggs SA, Zosky GR, Bereznicki LR. Emergency department presentations of febrile children to an Australian public hospital. J Paediatr Child Health. 2018;54(12):1308–1313. doi:10.1111/jpc.2018.54.issue-12
3. Barbi E, Marzuillo P, Neri E, Naviglio S, Krauss BS. Fever in children: pearls and pitfalls. Children. 2017;4(81):1–19. doi:10.3390/children4090081
4. El-Radhi ASM. Why is the evidence not affecting the practice of fever management? Arch Dis Child. 2008;93(11):918–920. doi:10.1136/adc.2008.139949
5. Prajitha N, Athira SS, Mohanan PV. Pyrogens, a polypeptide produces fever by metabolic changes in hypothalamus: mechanisms and detections. Immunol Lett. 2018;204(12):38–46. doi:10.1016/j.imlet.2018.10.006
6. Yang T, Huang W, Chen M, Huang K, Chen P. Sex differences in common childhood infections in Taiwan. Int J Infect Dis. 2018;75:115–117. doi:10.1016/j.ijid.2018.08.014
7. Colvin JM, Muenzer JT, Jaffe DM, et al. Detection of viruses in young children with fever without an apparent source. Pediatrics. 2012;130(6):e1455–e1462. doi:10.1542/peds.2012-1391
8. Nelson CE, Ostapenko S, Zorc JJ, Balamuth F. Utilization of antipyretics for nonurgent fever in a pediatric emergency department. Clin Pediatr. 2018;57:722–726. doi:10.1177/0009922817734356
9. De Bont EG, Lepot JM, Hendrix DA, et al. Workload and management of childhood fever at general practice out-of-hours care: an observational cohort study. BMJ Open. 2015;5(5):e007365. doi:10.1136/bmjopen-2014-007365
10. Nijman RG, Vergouwe Y, Thompson M, et al. Clinical prediction model to aid emergency doctors managing febrile children at risk of serious bacterial infections: diagnostic study. BMJ. 2013;346:f1706. doi:10.1136/bmj.f1706
11. Whitburn S, Costelloe C, Montgomery AA, et al. The frequency distribution of presenting symptoms in children aged six months to six years to primary care. Prim Health Care Res Dev. 2011;12(2):123–134. doi:10.1017/S146342361000040X
12. Diezi M. Fever and paracetamol in children. Paediatrica. 2014;25(5):29–31.
13. CDC/NCHS Infant Weight for Age Percentiles (< 36 months). Available from: https://reference.medscape.com/calculator/infant-weight-age-percentile.
14. CDC Weight for Age Percentiles for Girls (2–20 years). Available from: https://reference.medscape.com/calculator/weight-age-percentile-girls.
15. CDC Weight for Age Percentiles for Boys (2–20 years). Available from: https://reference.medscape.com/calculator/weight-age-percentile-boys.
16. Poropat F, Heinz P, Barbi E, Ventura A. Comparison of two European paediatric emergency departments: does primary care organisation influence emergency attendance? Ital J Pediatr. 2017;43:29. doi:10.1186/s13052-017-0339-y
17. Riva B, Clavenna A, Cartabia M, et al. Emergency department use by paediatric patients in Lombardy Region, Italy: a population study. BMJ Paediatrics Open. 2018;2(1):e000247. doi:10.1136/bmjpo-2017-000247
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.