")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
The Bronchiectasis in COPD-OSA Overlap Syndrome Patients
Authors Yang X, Tang X, Cao Y, Dong L, Wang Y, Zhang J, Cao J
Received 26 December 2019
Accepted for publication 6 March 2020
Published 18 March 2020 Volume 2020:15 Pages 605—611
DOI https://doi.org/10.2147/COPD.S243429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chunxue Bai
Xia Yang, Xin Tang, Yaoqian Cao, Lixia Dong, Yan Wang, Jing Zhang, Jie Cao
Department of Respiratory and Critical Care Medicine, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
Correspondence: Jie Cao
Department of Respiratory and Critical Care Medicine, Tianjin Medical University General Hospital, Tianjin 300052, People’s Republic of China
Tel +8613682187319
Fax +8602260361720
Email [email protected]
Purpose: COPD-OSA (chronic obstructive pulmonary disease–obstructive sleep apnea) overlap syndrome is associated with more frequent COPD acute exacerbations than COPD without OSA. With the application of high-resolution computed tomography (HRCT) in COPD, bronchiectasis is commonly detected and is associated with disease severity. Sleep respiratory disease is also associated with bronchiectasis; however, the correlation between OSA and coexisted bronchiectasis in COPD (COPD-Bx) has not been reported yet.
Patients and Methods: A total of 124 consecutive patients with stable COPD were enrolled. All subjects completed the chest HRCT and nocturnal polysomnography (PSG). The scores of extent and severity in bronchiectasis were assessed based on the Smith method and the Bhalla scoring system. Clinical data, questionnaire, routine blood test data, blood levels of C-reactive protein (CRP) and Immunoglobulin E, and the lymphocyte subtype were collected.
Results: Among all enrolled patients, 56.45% (70/124) were diagnosed as COPD-OSA based on the results of PSG screening. Bronchiectasis was detected in 42.86% (30/70) of the patients with COPD-OSA, but in 18.52% (10/54) of the patients without OSA (χ 2=8.264, p=0.004). PSG screening revealed that COPD with OSA had a significantly higher apnea-hypopnea index and percent of time spent with oxygen saturation below 90% (T90). Higher values of CRP, T90, and lower CD4/CD8 in the COPD-Bx with OSA were detected compared to COPD-Bx without OSA. Correlation analysis showed that the Bhalla severity score was related to CD8 cell count (r=0.446, p< 0.05) and CD4/CD8 (r=− 0.357, p< 0.05) in all the COPD-Bx patients. The Smith extent score was also associated with the values of CD8 count (r=0.388, p< 0.05) and CD4/CD8 (r=− 0.381, p< 0.05).
Conclusion: The comorbid bronchiectasis was more common in COPD-OSA overlap syndrome patient and may be related to more severe hypoxia and increased systemic inflammation.
Keywords: chronic obstructive pulmonary disease, bronchiectasis, obstructive sleep apnea
Introduction
Chronic obstructive pulmonary disease (COPD) with obstructive sleep apnea (OSA) is defined as the overlap syndrome (COPD-OSA).1 Overlap syndrome is more prevalent during patients diagnosed with COPD or OSA than in the general population. It has gained increased attention recently.2 Because of the different study populations and the different diagnostic criteria of COPD or OSA, the reported prevalence of COPD-OSA was not consistent. In COPD patients, the prevalence of OSA had been estimated to be about 0.5–65%.2–5 Approximately 11% of OSA patients have airflow limitation based on pulmonary function test.1
Patients with overlap syndrome have higher decrease in nocturnal oxygen desaturation than patients with either disease alone.3 More frequent acute exacerbations and higher mortality are also observed in patients with overlap syndrome than COPD alone.2,6,7 The treatment of continuous positive airway pressure (CPAP) reduces acute exacerbations and mortality in COPD-OSA patients.8–10 The potential mechanisms associated with increased acute exacerbations and positive effects of CPAP therapy in COPD-OSA are not well known.
The application of high-resolution computed tomography (HRCT) in COPD patients has shown that bronchiectasis is common in COPD.11 Bronchiectasis is one of the known comorbidities of COPD and may be associated with COPD severity.12 However, the causes and risk factors of bronchiectasis in COPD remain to be determined.
Epidemiological studies have demonstrated relationships between sleep disorders and bronchiectasis.13–16 Previous research shows that hypoxia might be a pathogenic mechanism in cystic fibrosis, primary ciliary dyskinesia, and lung tissue remodeling.16–18 However, the correlation between OSA and coexisted bronchiectasis in COPD (COPD-Bx) has not been reported yet. The purpose of our study was to investigate the relationship between OSA and bronchiectasis in COPD patients.
Patients and Methods
Research Subjects
A total of 124 stable COPD patients (45 to 80 years old) visiting Tianjin Medical University General Hospital were consecutively enrolled between February 2017 and March 2019. All subjects completed pulmonary function tests performed by two trained technicians according to international standards. The diagnosis of COPD is in accordance with the Global Initiative for Chronic Obstructive Lung Disease (GOLD).19 All subjects were former or current smokers with a minimum smoking index of 10 packs-year. The exclusion criteria included subjects with asthma, pre-diagnosed bronchiectasis, and any other diagnosed respiratory diseases. All subjects signed written informed consent. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Tianjin Medical University General Hospital (IRB2019-KY-133).
Evaluation of OSA
Nocturnal polysomnography (PSG) was performed for all subjects in the sleep center of Tianjin Medical University General Hospital, Tianjin, China. All PSG was performed by two trained technicians according to the international standards specified by the American Academy of Sleep Medicine (AASM) and manually scored by a single technologist.20 The recording time was longer than 7 hrs. The presence of OSA was defined using the apnea-hypopnea index (AHI ≥ 5), which was based on the number of apneas/hypopneas events per hour during all the sleep time. Subjects with central sleep apnea/hypopnea were excluded.
Clinical Data and Laboratory Tests
The demographic characteristics and smoking history of all the subjects were collected. Dyspnea and total symptoms of COPD were evaluated using the modified Medical Research Council Dyspnea Scale (mMRC) and the COPD Assessment Test (CAT).
Fractionated exhaled nitric oxide (FeNO), an eosinophilic airway inflammation marker, was detected according to the guidelines in the user manual training with the NIOX Mino® device (Aerocrine AB, Solna, Sweden). Fasting venous blood samples were collected in the morning. The blood routine test, C-reactive protein (CRP), and serum total Immunoglobulin E (IgE) level were measured by the department of laboratory.
Analysis of the blood lymphocyte subtypes was performed using flow cytometry. The freshly obtained blood was stained with anti-CD3 (total T lymphocytes), anti-CD4, and anti-CD8 (all from Becton Dickinson (BD), San Jose, California, USA). The sample was analyzed using FACS Calibur (BD Pharmingen, San Jose, CA, USA) and FlowJo software Version 10 (TreeStar, Ashland, OR, USA).
Chest HRCT Scanning
All the subjects completed HRCT scan of the chest by a skilled technician in the department of radiology. Two professional radiologists scored the images blindly. If the results were inconsistent, the scores were determined after a discussion by the research team. Diagnosis of bronchiectasis was obtained according to the criteria published by Naidich.21 Imaging scores of bronchiectasis were determined as we reported previously11 including the extent score according to the Smith method and the severity score based on the Bhalla scoring system.22,23 The Smith method is mainly based on the percentage of abnormal bronchi in each lobe. The Bhalla severity scoring system is completed according to the ratio of the luminal diameter to the diameter of adjacent blood vessel.
Statistical Analysis
All data were analyzed using SPSS version 21.0 (Statistics Package for the Social Sciences, Inc., Chicago, IL, USA). The normal distribution parameters were described as mean ± standard deviation. The Non-normal distribution parameters were defined as medians (interquartile range). To compare the difference between two groups, we used t-test or Mann–Whitney U-test for continuous data according to distribution and χ2 test for categorical variables. The correlation between the score of bronchiectasis and other variables was analyzed using Spearman correlations. Statistically significance was defined as p-values<0.05.
Results
Demographic Characteristics
We enrolled 124 patients with COPD and 60.48% were male. The median age was 68.00 years. There were 13 (10.48%), 28 (22.58%), 40 (32.26%), and 43 (34.68%) subjects in stage I, II, III and IV of GOLD, respectively. All subjects had a positive history of smoking. The results are shown in Table 1.
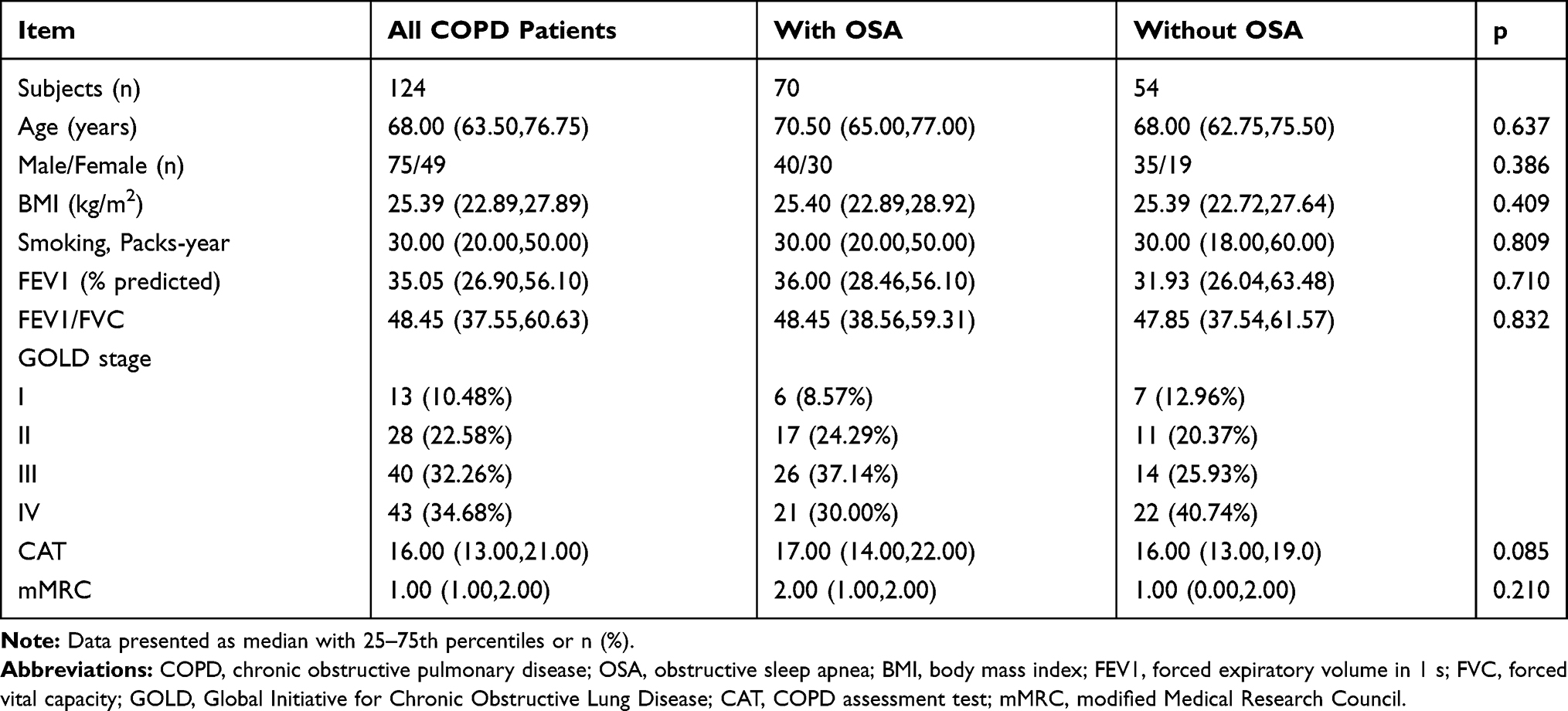 |
Table 1 Characteristics of COPD Patients with or Without OSA |
Bronchiectasis and OSA in COPD
HRCT findings showed that 32.26% (40/124) of the patients with COPD had bronchiectasis. Most of them were cylindrical bronchiectasis (80.0%), while a minority of them appeared to be mixed bronchiectasis (20.0%). The anatomic distributions of bronchiectasis were the right lower lobe (21.9%), right upper lobe (21.9%), right middle lobe (18.8%), lingula (15.6%), left upper lobe (12.5%) and left lower lobe (9.4%) and bilateral lesions were common. OSA was diagnosed in 56.45% (70/124) of the COPD patients. Among them, the AHI of 60.00% (42/70) patients was less than 15, 25.71% (18/70) was between 15 and 30, and 14.29% (10/70) with AHI≥30.
Clinical Characteristics of COPD-OSA and COPD Alone
Clinical characteristics of subjects with COPD-OSA and COPD alone are summarized in Table 1. There were no differences in both CAT and mMRC scores between the two groups. In addition, there were no differences in pulmonary function, smoking index, BMI, and gender between the two groups.
The Frequency and Severity of Bronchiectasis in COPD-OSA and COPD Alone
Among COPD-OSA patients, 42.86% (30/70) showed comorbid bronchiectasis, which is more common than that in COPD without OSA group (18.52%, 10/54) (χ2=8.264, p=0.004). However, the bronchiectasis scores of severity and extent were not different between COPD-Bx with OSA or not. These results are shown in Table 2. Correlation analysis showed that the Bhalla severity score was related to CD8 cell count (r=0.446, p<0.05) and CD4/CD8 (r=−0.357, p<0.05) in all the COPD-Bx patients. The Smith extent score was also associated with CD8 cell count (r=0.388, p<0.05) and CD4/CD8 (r=−0.381, p<0.05). No correlation was found between the bronchiectasis score and any other sleep variables including AHI, the time spent with oxygen saturation below 90% (T90) and minimum peripheral capillary oxygen saturation (SpO2min).
 |
Table 2 The Prevalence and Severity of Bronchiectasis in COPD with or Without OSA |
Laboratory Characteristics in COPD-OSA or COPD Alone
The bronchiectasis identified through HRCT was more popular in the COPD with OSA. To investigate the possible mechanisms of the relationship between these two diseases in COPD patients, we compared FeNO, blood routine test, CRP, serum total IgE and T lymphocyte subtypes between COPD with and without OSA. Our PSG screening revealed that COPD with OSA had significantly higher AHI and T90. In addition, FeNO, routine blood test, CRP, serum total IgE and the T lymphocyte subtypes were not different between the two groups. The results are shown in Table 3.
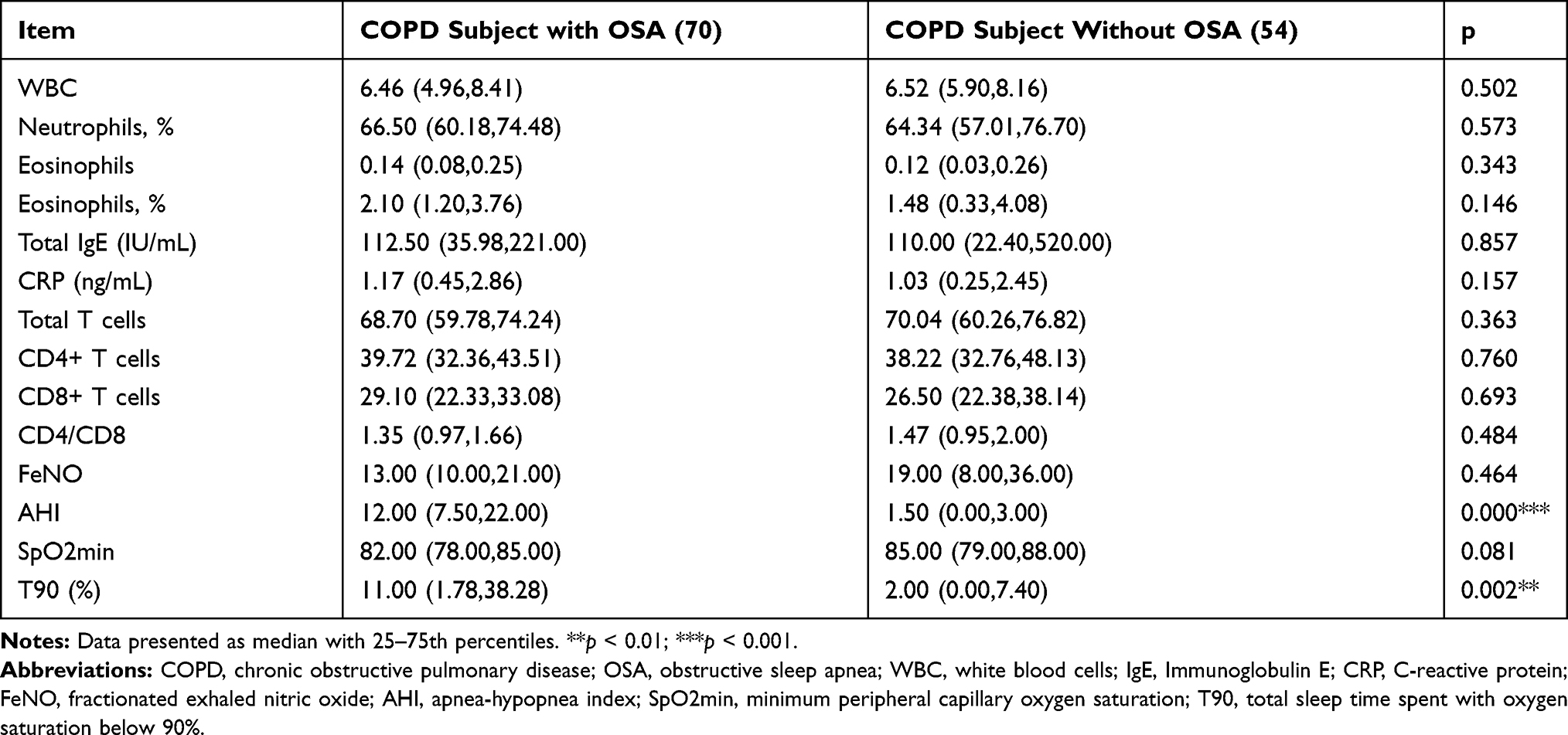 |
Table 3 Characteristics Comparison Between COPD with or Without OSA |
Characteristics of Clinical and Laboratory in COPD-Bx with OSA and Without OSA
We also compared the difference between the COPD-Bx with OSA or without OSA. There were no significant differences in pulmonary function test, smoking index, BMI, age, and gender between the two groups. We found that CRP and T90 increased significantly in COPD-Bx with OSA than those without OSA. The ratio of CD4/CD8 decreased significantly in COPD-Bx with OSA. We did not see any difference for the CD4 and CD8 cell counts between the two groups. The routine blood test, serum total IgE, SpO2min were not different between the two groups. The results are shown in Table 4.
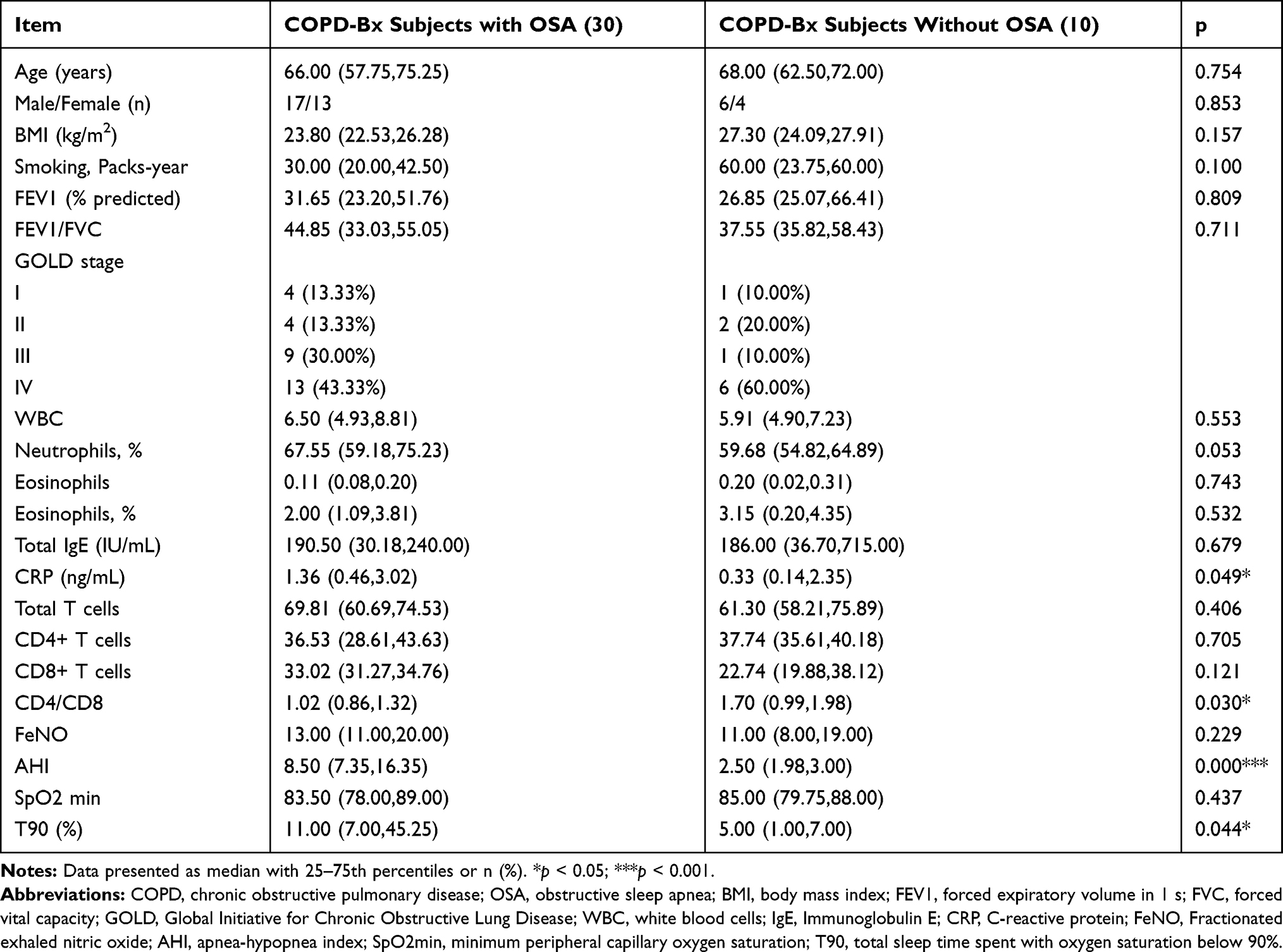 |
Table 4 The Comparison Between COPD-Bx with or Without OSA |
Discussion
This is the first study analyzing the relationship between OAS and bronchiectasis in COPD. The study has shown that bronchiectasis was more prevalent in the COPD-OSA overlap syndrome patients, which may associate with higher levels of AHI and T90. In our study, we also found that there were increased levels of CRP and T90, and lower CD4/CD8 in the COPD-Bx with OSA than those without. In addition, the Smith extent score and Bhalla severity score of bronchiectasis were both related to the values of CD8 cell count and CD4/CD8 in all the COPD-Bx patients.
The results showed that OSA was diagnosed in 56.45% of the COPD patients, which was higher than the previous research results. One possible explanation is that most of the subjects enrolled in our study were COPD patients with severe-to-very severe disease.3,5 The main finding of our study was a significant increase in the prevalence of bronchiectasis in overlap syndrome compared with COPD without OSA. But the study did not find significant differences in the bronchiectasis score between COPD-Bx with or without OSA. Our finding suggested that OSA may be involved in the occurrence and progression of combined bronchiectasis in COPD. The complex pathogenesis of bronchiectasis in COPD is not entirely understood. The previous studies suggested that persistent tissue injury and remodeling due to airway inflammation and protease/antiprotease imbalance in COPD may be involved in the occurrence of bronchiectasis.11,24,25 The findings from this study support this hypothesis.
The previous studies suggested that OSA may participate in tissue remodeling of COPD by elevating inflammation of the lower airway.18,26 In our study, we found that the COPD-Bx with OSA had increased CRP than those without OSA, which is a systemic inflammation marker. The results show that more severe systemic inflammation is present in COPD-Bx with OSA.
T lymphocytes are one of the primary cells involved in the regulation of COPD inflammation.27 Previous studies revealed that CD8+ T cells might lead to tissue injuries through direct cytopathic effects, recruitment and activation of inflammatory mediators.28,29 To study the role of T lymphocyte in the combined bronchiectasis with overlap syndrome patients, we investigated T-cell subsets of peripheral blood. Our findings showed that the values of CD4/CD8 in COPD-Bx patients with OSA were lower than those patients without OSA. The previous studies have shown that OSA might cause alterations in immune system which is associated with the occurrence of serious complications.30 Many studies have confirmed the presence of altered T lymphocyte function in OSA patients and most affected T lymphocyte subtype is CD8+ cells. OSA patients have increased number of CD8+ and decreased number of CD4+ cells, which were related to AHI.31–33 Elevated levels of CD8+ cells were also found in patients with bronchiectasis, which also supported the role of T lymphocyte in the pathogenesis of primary bronchiectasis.34,35 In our study, the correlation analysis showed that the bronchiectasis score of severity and extent related to the values of CD8 and CD4/CD8. Our results suggest that OSA may participate in the development of bronchiectasis by altering T lymphocyte function in COPD.
Although most COPD patients have a predominantly neutrophilic inflammation, some have an increase in eosinophil counts.27 We compared the differences of eosinophilic markers (FeNO, eosinophils, and total IgE) between the COPD patients with and without OSA and did not find any difference. In addition, there was no difference between the COPD-Bx patients with and without OSA for these markers. These results suggest that the role of eosinophilic inflammation in OSA induced higher prevalence of bronchiectasis in COPD needs to be further investigated.
Previous studies have revealed that hypoxia might be a pathogenic mechanism in cystic fibrosis and primary ciliary dyskinesia.16,17 Animal studies have also found that chronic intermittent hypoxia, the most important characteristics of OSA, could cause lung tissue remodeling, including fibrosis and emphysema.18 In our study, we found that the overlap patients had higher AHI and T90. And the levels of T90 were also elevated in COPD-Bx with OSA. Therefore, hypoxia, especially chronic intermittent hypoxia, might participate in the occurrence and development of bronchiectasis in overlap syndrome.
Our study has several limitations: 1) The sample size of our study is relatively small, and it is only the research results of one center. We did not assess the effect of other comorbidities on the disease. 2) We did not evaluate the lower airway inflammation. We could not clarify whether the relationship between OSA and bronchiectasis in the COPD related to the enhanced lower airway inflammation. 3) Since this study is a cross-sectional study, it could not assess the effect of OSA and combined bronchiectasis on the prognosis of COPD, such as the number of exacerbations.
Conclusion
In conclusion, we found that the comorbid bronchiectasis was more common in COPD-OSA overlap syndrome patient and may be related to more severe hypoxia and increased systemic inflammation. These results indicated that OSA might play a role in the pathogenesis of bronchiectasis in COPD.
Acknowledgments
The authors acknowledge the economic support from the Tianjin Natural Science Foundation of China (18JCQNJC82900), the National Natural Science Foundation of China (81670084), and the 13th Five-Year Plan for First-Class Discipline Construction of China. The abstract of this paper was presented at the Asian Pacific Society of Respirology Congress 2019 as a conference talk with interim findings. The poster’s abstract was published in “Poster Abstracts” in Respirology: https://doi.org/10.1111/resp.13699_118.
Author Contributions
All authors contributed to conception and design, patients recruited, data acquisition, data analysis and interpretation, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chaouat A, Weitzenblum E, Krieger J, Ifoundza T, Oswald M, Kessler R. Association of chronic obstructive pulmonary disease and sleep apnea syndrome. Am J Respir Crit Care Med. 1995;151(1):82–86. doi:10.1164/ajrccm.151.1.7812577
2. Shawon MS, Perret JL, Senaratna CV, Lodge C, Hamilton GS, Dharmage SC. Current evidence on prevalence and clinical outcomes of co-morbid obstructive sleep apnea and chronic obstructive pulmonary disease: a systematic review. Sleep Med Rev. 2017;32:58–68. doi:10.1016/j.smrv.2016.02.007
3. Sanders MH, Newman AB, Haggerty CL, et al. Sleep Heart Health Study. Sleep and sleep-disordered breathing in adults with predominantly mild obstructive airway disease. Am J Respir Crit Care Med. 2003;167(1):7–14. doi:10.1164/rccm.2203046
4. López-Acevedo MN, Torres-Palacios A, Elena Ocasio-Tascón M, Campos-Santiago Z, Rodríguez-Cintrón W. Overlap syndrome: an indication for sleep studies?: A pilot study. Sleep Breath. 2009;13(4):409–413. doi:10.1007/s11325-009-0263-5
5. Soler X, Gaio E, Powell FL, et al. High prevalence of obstructive sleep apnea in patients with moderate to severe chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12(8):1219–1225. doi:10.1513/AnnalsATS.201506-379LE
6. Shaya FT, Lin PJ, Aljawadi MH, Scharf SM. Elevated economic burden in obstructive lung disease patients with concomitant sleep apnea syndrome. Sleep Breath. 2009;13(4):317–323. doi:10.1007/s11325-009-0266-2
7. Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med. 2010;182(3):325–331. doi:10.1164/rccm.200912-1869OC
8. Machado MC, Vollmer WM, Togeiro SM, et al. CPAP and survival in moderate-to-severe obstructive sleep apnoea syndrome and hypoxaemic COPD. Eur Respir J. 2010;35(1):132–137. doi:10.1183/09031936.00192008
9. Jaoude P, Kufel T, El-Solh AA. Survival benefit of CPAP favors hypercapnic patients with the overlap syndrome. Lung. 2014;192(2):251–258. doi:10.1007/s00408-014-9555-z
10. Stanchina ML, Welicky LM, Donat W, Lee D, Corrao W, Malhotra A. Impact of CPAP use and age on mortality in patients with combined COPD and obstructive sleep apnea: the overlap syndrome. J Clin Sleep Med. 2013;9(8):767–772. doi:10.5664/jcsm.2916
11. Yang X, Xu Y, Jin J, Li R, Liu X, Sun Y. Chronic rhinosinusitis is associated with higher prevalence and severity of bronchiectasis in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:655–662. doi:10.2147/COPD
12. Martínez-García MA, de la Rosa Carrillo D, Soler-Cataluña JJ, et al. Prognostic value of bronchiectasis in patients with moderate to severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(8):823–831. doi:10.1164/rccm.201208-1518OC
13. Erdem E, Ersu R, Karadag B, et al. Effect of night symptoms and disease severity on subjective sleep quality in children with non-cystic-fibrosis bronchiectasis. Pediatr Pulmonol. 2011;46(9):919–926. doi:10.1002/ppul.v46.9
14. Gao Y, Guan W, Xu G, et al. Sleep disturbances and health-related quality of life in adults with steady-state bronchiectasis. PLoS One. 2014;9(7):e102970. doi:10.1371/journal.pone.0102970
15. Faria Júnior NS, Urbano JJ, Santos IR, et al. Evaluation of obstructive sleep apnea in non-cystic fibrosis bronchiectasis: a cross-sectional study. PLoS One. 2017;12(10):e0185413. doi:10.1371/journal.pone.0185413
16. Santamaria F, Esposito M, Montella S, et al. Sleep disordered breathing and airway disease in primary ciliary dyskinesia. Respirology. 2014;19(4):570–575. doi:10.1111/resp.2014.19.issue-4
17. Montgomery ST, Mall MA, Kicic A, Stick SM; AREST CF. Hypoxia and sterile inflammation in cystic fibrosis airways: mechanisms and potential therapies. Eur Respir J. 2017;49(1):1600903. doi:10.1183/13993003.00903-2016
18. Owens RL, Macrea MM, Teodorescu M. The overlaps of asthma or COPD with OSA: a focused review. Respirology. 2017;22(6):1073–1083. doi:10.1111/resp.2017.22.issue-6
19. Global strategy for the diagnosis, management, and prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2019. Available from: http://www.goldcopd.org.
20. Berry RB, Albertario CL, Harding SM, et al. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Version 2.5. Darien, IL: American Academy of Sleep Medicine; 2018.
21. Naidich DP, McCauley DI, Khouri NF, Stitik FP, Siegelman SS. Computed tomography of bronchiectasis. J Comput Assist Tomogr. 1982;6(3):437–444. doi:10.1097/00004728-198206000-00001
22. Smith IE, Jurriaans E, Diederich S, Ali N, Shneerson JM, Flower CD. Chronic sputum production: correlation between clinical features and findings on high resolution computed tomographic scanning of the chest. Thorax. 1996;51(9):914–918. doi:10.1136/thx.51.9.914
23. Bhalla M, Turcios N, Aponte V, et al. Cystic fibrosis: scoring system with thin-section CT. Radiology. 1991;179(3):783–788. doi:10.1148/radiology.179.3.2027992
24. Patel IS, Vlahos I, Wilkinson TM, et al. Bronchiectasis, exacerbation indices, and inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;170(4):400–407. doi:10.1164/rccm.200305-648OC
25. Du Q, Jin J, Liu X, Sun Y. Bronchiectasis as a comorbidity of chronic obstructive pulmonary disease: a systematic review and meta-analysis. PLoS One. 2016;11(3):e0150532. doi:10.1371/journal.pone.0150532
26. Wang Y, Hu K, Liu K, et al. Obstructive sleep apnea exacerbates airway inflammation in patients with chronic obstructive pulmonary disease. Sleep Med. 2015;16(9):1123–1130. doi:10.1016/j.sleep.2015.04.019
27. Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
28. Monaco C, Andreakos E, Kiriakidis S, Feldmann M, Paleolog E. T-cell-mediated signalling in immune, inflammatory and angiogenic processes: the cascade of events leading to inflammatory diseases. Curr Drug Targets Inflamm Allergy. 2004;3(1):35–42. doi:10.2174/1568010043483881
29. Curtis JL. Cell-mediated adaptive immune defense of the lungs. Proc Am Thorac Soc. 2005;2(5):412–416. doi:10.1513/pats.200507-070JS
30. Domagała-Kulawik J, Kwiecień I, Bielicki P, Skirecki T. Fas-positive lymphocytes are associated with systemic inflammation in obstructive sleep apnea syndrome. Sleep Breath. 2019;23(2):673–678. doi:10.1007/s11325-018-1713-8
31. Dyugovskaya L, Lavie P, Hirsh M, Lavie L. Activated CD8+ T-lymphocytes in obstructive sleep apnoea. Eur Respir J. 2005;25(5):820–828. doi:10.1183/09031936.05.00103204
32. Dyugovskaya L, Lavie P, Lavie L. Phenotypic and functional characterization of blood γδ T cells in sleep apnea. Am J Respir Crit Care Med. 2003;168(2):242–249. doi:10.1164/rccm.200210-1226OC
33. Domagała-Kulawik J, Osińska I, Piechuta A, Bielicki P, Skirecki T. T, B, and NKT cells in systemic inflammation in obstructive sleep apnoea. Mediators Inflamm. 2015;2015:161579. doi:10.1155/2015/161579
34. Silva JR, Jones JA, Cole PJ, Poulter LW. The immunological component of the cellular inflammatory infiltrate in bronchiectasis. Thorax. 1989;44(8):668–673. doi:10.1136/thx.44.8.668
35. Lapa e Silva JR, Guerreiro D, Noble B, Poulter LW, Cole PJ. Immunopathology of experimental bronchiectasis. Am J Respir Cell Mol Biol. 1989;1(4):297–304. doi:10.1165/ajrcmb/1.4.297.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.