")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
The Associations of Perceived and Oxidative Stress with Hypertension in a Cohort of Police Officers
Authors Janczura M , Rosa R, Dropinski J, Gielicz A, Stanisz A, Kotula-Horowitz K, Domagala T
Received 4 January 2021
Accepted for publication 13 March 2021
Published 23 April 2021 Volume 2021:14 Pages 1783—1797
DOI https://doi.org/10.2147/DMSO.S298596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Miroslaw Janczura,1 Rafal Rosa,2 Jerzy Dropinski,3 Anna Gielicz,3 Andrzej Stanisz,4 Katarzyna Kotula-Horowitz,5 Teresa Domagala6
1Faculty of Health Sciences, Jagiellonian University School of Medicine, Krakow, Poland; 2Health Care Centre of the Ministry of the Interior and Administration, Department of Anesthesiology and Intensive Care, Krakow, Poland; 3Department of Internal Medicine, Jagiellonian University School of Medicine, Krakow, Poland; 4Department of Bioinformatics and Telemedicine, Jagiellonian University School of Medicine, Krakow, Poland; 5Health Care Centre of the Ministry of the Interior and Administration, Department of Internal Medicine, Krakow, Poland; 6Department of Medical Biochemistry, Jagiellonian University School of Medicine, Krakow, Poland
Correspondence: Teresa Domagala
Department of Medical Biochemistry, Jagiellonian University School of Medicine, Krowoderska 68/11, Krakow, 31-158, Poland
Tel +48 12 422 74 00
Fax +48 12 422 32 72
Email [email protected]
Purpose: Associations between perceived stress and oxidative stress marker and metabolic syndrome (MetS) components were investigated in a cohort of police officers.
Methods: Cross-sectional data from a cohort of non-diabetic subjects (n=233; 19F), median [interquartile range] age 50 [37– 44] years, were analysed. MetS was construed in line with International Diabetes Federation (IDF) criteria and perceived stress with Cohen’s 10-item Perceived Stress Scale. Plasma oxidative stress marker (free 8-iso-prostaglandin F2α; 8-iso-PGF2α), presence of coronary plaque, carotid artery intima-media thickness (cIMT), and physical activity level were also determined.
Results: Obesity was established in 100 (42.92%), hypertension in 111 (47.64), whereas MetS was identified in 104 (44.63%) of the study subjects. A significant difference (p=0.003) in plasma 8-iso-PGF2α level, depending on the MetS components status, was noted. The associations of perceived stress with plasma 8-iso-PGF2α level and the select study variables were gender-specific. In multivariate analysis (adjusted for age and current smoking), positive associations of plasma 8-iso-PGF2α levels with PSS score (B=0.108, 95% CI [0.008, 0.209], p=0.03) and systolic blood pressure (B=0.029, 95% CI [0.003, 0.057], p=0.02) in men only were established. Both the perceived stress (OR 1.101, 95% CI [1.001– 1.202], p=0.03) and plasma 8-iso-PGF2α levels (OR 1.223, 95% CI [1.046– 1.432], p=0.01) impacted the prevalence of hypertension. Out of the MetS components, the effect of waist circumference (OR=1.138, 95% CI [1.064– 1.218], p=0.0001) and glucose (B=2.696, 95% CI [1.081– 6.725], p=0.03) were also encountered. No such associations were noted in women, though, neither in univariate nor in multivariate analyses. The prevalence of coronary plaque (0.001), obesity (p< 0.001), hypertension (p< 0.001) and median cIMT value (p=0.005), as well as leisure-time (p=0.04) and total walking physical activity (p=0.03), differed significantly between the subgroups stratified by MetS components status.
Conclusion: Both the perceived and oxidative stress were found instrumental in promoting hypertension in a cohort of police officers under study, whereas all study outcomes were conclusively gender-related.
Keywords: metabolic syndrome, obesity, hypertension, perceived stress, oxidative stress, physical activity
Introduction
The clustering risk factors, as is the case of metabolic syndrome (MetS), may exacerbate systemic inflammation and oxidative stress (an imbalance between antioxidants and reactive oxygen substance; ROS), ie, specific processes actually underlying cardiovascular disease (CVD) and type 2 diabetes.1–3 The global prevalence of hypertension was estimated to be in adults of around 30%–45% and is an important cause of CVD morbidity and mortality worldwide.2,4 Excess weight gain, especially when associated with increased visceral adiposity, accounting for 65%–75% of the risk for human primary hypertension.5 Contributive role of psychological stress appears steadily on the rise among the many environmental factors entailed in the origination and development of both hypertension and MetS; this being predominantly owed to appreciably altered individual lifestyle paradigms and rapid rate of technological advances.6–9
Many common factors contribute to the etiology of hypertension and obesity, as lifestyle (eating habits, low physical activity), metabolic disorders (diabetes, dyslipidemia), sleep problems, and high psychological stress. Furthermore, the etiology of hypertension is multifactorial, and a large number of the separate causative factors (hyperactivity of sympathetic nervous and renin–angiotensin–aldosterone systems, endothelial dysfunction, and arterial stiffness) were also documented. Causative factors pertaining to arterial hypertension also seem to hold true for obesity and MetS, whose common feature consists in an increased oxidative stress caused by excessive ROS production.10
The increased ROS in vascular cells, primarily induced by NADPH oxidase, reduce the bioavailability of the protective vasodilator nitric oxide and can modulate endothelial function, vascular tone and cardiac function.11,12 It has been evidenced that psychological stress or administration of exogenous corticosteroids induced oxidative stress in animal studies.13,14 Moreover, lower blood pressure was found in mouse models with deficient in ROS-generating enzymes, as compared with wild-type ones, as well as, angiotensin II (Ang II) infusion fails to induce hypertension in these mice.15 Classical CVD risk factors are associated with higher plasma or urine levels of oxidative stress markers.16,17 Out of F2-isoprostanes, 8-iso-prostaglandin F2α (8-iso-PGF2α) has been the most studied isomer, and consequently its measurement has been incorporated into a large number of clinical studies.16–19 Studies on the relations of oxidative stress markers and MetS, or with some of its components, are rather scarce, and their outcomes inconclusive.16,18,20,21
There are no published studies, though, taking into account both the perceived and oxidative stress, and their association with MetS components. Police officers are widely acknowledged to be exposed to more stressors than individuals pursuing other occupations, also a systematic review of published studies has attested to this exposure to stressors having been associated with CVD risk.22 Therefore, our main objective was to investigate the cross-sectional associations of perceived and oxidative stress with hypertension, which is one of the main components of the MetS and important cause of CVD morbidity and mortality. In line with our working hypothesis, perceived stress is believed to be associated with increased systemic oxidative stress and the prevalence of hypertension.
Methods
Study Population
We carried out a cross-sectional study on the cohort of police officers from the southern region of Poland, who had volunteered for a comprehensively structured panel of clinical and lab exams, pursued with principal focus set on the CVD, at the University Hospital in Krakow. The following inclusion criteria were adopted: police officer on active duty for a minimum period of five years (the median [interquartile range] duration of duty was 15 [11–20] years). The following exclusion criteria from the study protocol were applied: history of myocardial infarction or stroke, congestive heart failure, atrial fibrillation, diabetes mellitus, liver injury, or kidney insufficiency, cancer, current anticoagulant therapy, and vitamin supplementation. The subjects with arterial hypertension and lipid disorders (defined as the ones previously diagnosed and treated with statins or serum total cholesterol >5.2 mmol/L) were regarded eligible. The subjects who had quit smoking at least 6 months previously were included in the study as the non-smokers. As established through the interviews individually conducted with each study subject by the investigators, none of the subjects had been following any alternative dietary profile and/or used any food supplementation with a standard dietary intake. Out of the 243 subjects who had undergone medical examinations, ultimately 233 (19F), median [interquartile range] age 50 [37–44] years, were found fully compliant with the inclusion criteria. The examinations followed all related tenets of the Declaration of Helsinki, and the study was approved by the Human Research Ethics Committee of the Jagiellonian University (Application Ref. No KBET/90/B2011, dated June 30, 2011). All study subjects provided written informed consent for participation in the study protocol.
Physical Examination
Physical examination, medical and structured interviews were applied to acquire personal and clinical information. Anthropometric examinations were carried out in the morning on the participants who had fasted overnight. Anthropometric measurements, ie, circumference of waist and hips, height, and body weight were also completed. Body mass index (BMI) was calculated as weight in kilograms divided by the square of height in metres. Obesity was defined as BMI>30.0 kg/m2, and overweight as BMI >25.0 kg/m2. MetS was defined in line with the criteria proposed by the International Diabetes Federation (IDF), ie, waist circumference ≥94 cm for men, and ≥80 cm for women (central obesity), fasting glucose ≥5.6 mmol/L, triglycerides ≥1.7 mmol/L, or specific treatment for this lipid abnormality, HDL-cholesterol <1.03 mmol/L in men, and <1.29 mmol/L in women, systolic/diastolic blood pressure ≥130/≥85 mmHg, or treatment of previously diagnosed hypertension.23 The blood pressure in the study subjects was measured with a calibrated mercury sphygmomanometer, according to the protocol recommended by the guidelines for hypertension management.24 The participants needed to have refrained from cigarette smoking and drinking caffeinated beverages for at least 30 min before measurement. Blood pressure was recorded as the means of two measurements (in 10-minute intervals).
Clinical Tests
All study subjects were subjected to exercise electrocardiography, and in 63.52% of them (71.15% and 53.64% subjects with MetS, and non-MetS, respectively) computed tomography coronary angiography (CTCA) was completed. Imaging studies, aimed at measuring the surrogate marker of atherosclerosis carotid intima-media thickness (cIMT) was also completed using an ultrasonograph (Sequoia 512, Mountain View, CA, USA) with a 6 MHz linear transducer.
Measurement of Self-Perceived Stress
Perceived stress was measured with the aid of Cohen’s 10-item Perceived Stress Scale (PSS-10) in Polish adaptation.25 Specifically structured questions were designed to probe the respondents how unpredictable, uncontrollable, and overloaded they actually found their lives. They were asked to respond to each question on a 5-point Likert scale, ranging from 0 (never) to 4 (very often), indicating how often they have felt or thought in a certain way within the past month. Scale scores ranged 0–40, with the higher scores indicating higher levels of stress. The reliability of the scale was assessed by Cronbach’s alpha, while exploratory and confirmatory factor analyses were applied to evaluate validity of PSS-10. The PSS-10 demonstrated good reliability, as Cronbach’s alpha was 0.85 (0.84–0.86).
Biochemical Measurements
Blood sampling was carried out between 8:00 and 8:30 a.m. (after a 12-h overnight fast). The samples of separated plasma (and serum) were stored at −80°C, pending assays. Basic biochemical tests (liver enzymes, glucose, urea, uric acid, and creatinine were carried out with the aid of Vitros 350 Chemistry System (Ortho Clinical Diagnostics). Fibrinogen level in plasma was determined by coagulometry using the BCT camera (Behring Coagulation Timer, Dade-Behring, Germany) and the Multifibren U kit. Ultrasensitive CRP (hs-CRP) in the serum was determined by nephelometry (BN II System, Siemens), using CardioPhase assay (Siemens Healthcare Diagnostics Products GmbH, Marburg, Germany). Tissue necrotic factor-α (TNF-α) in the plasma was measured by ELISA (Quantikine HS Human TNF-α, R&D Systems, England). Insulin in the serum was determined by an immunoassay using a commercial kit (Insulin ELISA, DRG Instruments GmbH; Germany). The homeostasis model assessment of insulin resistance (HOMA-IR) index was calculated as fasting insulin x fasting glucose/22.5. Value of HOMA-IR >80 percentile designated in the subgroup of police officers (n=33) without any metabolic abnormalities was assumed the threshold of IR, ie, 2.04. The intra- and inter-assay coefficients of variation were 3.7% and 5.3%, respectively.
Free isoprostane 8-iso-PGF2α in plasma was determined by gas chromatography coupled with mass spectrometry (GC-MS).26 In order to prevent artefactual oxidation ex vivo, 25 µL of 1% butylated hydroxytoluene (BHT) was added to 1 mL of plasma. The measurements were carried out using a mass spectrometer (MS Engine 5989B Hewlett Packard, Palo Alta, CA, USA) coupled with a gas chromatograph (GC 5890 series II Hewlett Packard, Palo Alta, CA, USA). The intra- and inter-assay coefficients of variation were 3.35% and 5.82%, respectively.
Physical Activity
The details assessment of physical activity had previously been addressed.7 In short, International Physical Activity Questionnaire-Long Form (IPAQ-LF) used to evaluate a subject’s estimated metabolic equivalent of Task (MET) based on 5 domains of physical activity (work, domestic tasks, transportation, leisure/sport/recreation, and the time spent sitting). By making use of Ainsworth et al Compendium an average Metabolic Equivalent of Task (MET), a score was derived for each type of activity.27 The MET values were corrected, so as to account for personal variation in gender, body mass, height, and age, to provide more accurate estimates of individual physical activity level.28 The final MET value was referred to as a “corrected MET” value and expressed as the corrected MET-minutes/kg of body weight.
Statistical Analysis
The normality of data distribution was verified by the Shapiro–Wilk’s test. Continuous variables are presented as median (interquartile range). For comparison of the variables between the gender-related groups, non-parametric (Mann–Whitney U, Kruskal–Wallis) tests were applied. Categorical data were expressed as frequencies (percentages), and their differences were analysed by the Chi-squared test.
Univariate linear analyses were conducted for the total study population to assess the interrelationships between perceived stress scores, plasma 8-iso-PGF2α levels, and commonly acknowledged CVD risk factors, including age, BMI, LDL cholesterol, fibrinogen, CRP, and physical activity. Univariate and multivariable linear regression analysis were also conducted separately for gender to determine the associations of plasma 8-iso-PGF2α (as dependent variable) with the perceived stress score, and with the select variables whose values, when exceeding the reference range (ie, abnormal) are the key identification attributes of MetS. These independent variables comprised perceived stress score, waist circumference, triglycerides, HDL cholesterol, glucose, and systolic blood pressure only (to eliminate multicollinearity). Multivariate linear models were adjusted for age and current smoking.
To determine the impact of select variables under study on the prevalence of hypertension, separately for men and women, 6 univariate and 2 multivariate (adjusted for age and current smoking) logistic regression analyses were conducted.
Blood pressure systolic/diastolic ≥140/≥90 mm Hg, or the previously diagnosed hypertension currently treated with anti-hypertensive medications, served as the dichotomous dependent variable. The independent variables comprised perceived stress score, plasma 8-iso-PGF2α, waist circumference, triglycerides, HDL cholesterol, and glucose. The resultant crude and adjusted (for age, and current smoking) odds ratios (ORs) and 95% confidence intervals (CIs) were reported. The value p<0.05 was considered to be statistically significant. Statistical analysis was pursued with the aid of STATISTICA 13.1 PL software package.
Results
The clinical characteristics of the study participants, divided into respective groups according to their MetS status, are outlined in Table 1. The MetS subjects (44.63%), as compared to the non-MetS ones, significantly differed in age, and clinical variables, ie, FRS (p<0.0001), BMI (p<0.0001), prevalence of stable CHD (p=0.02), coronary plaque burden (p=0.007), systolic/diastolic blood pressure (p<0.0001) and carotid IMT (0.0001). Out of metabolic variables, the majority were also significantly higher in the MetS subjects. The median [interquartile range] level of perceived stress was also significantly higher in the MetS subjects, as compared to the non-MetS ones (18.00 [15.00–22.00], and 16.00 [12.00–20.00], p=0.02). With regard to gender, the level of perceived stress was non-significantly higher in women, as compared to men (18.50 [16.00–23.50] vs 16.00 [13.00–21.00], p=0.09; data not comprised in the table).
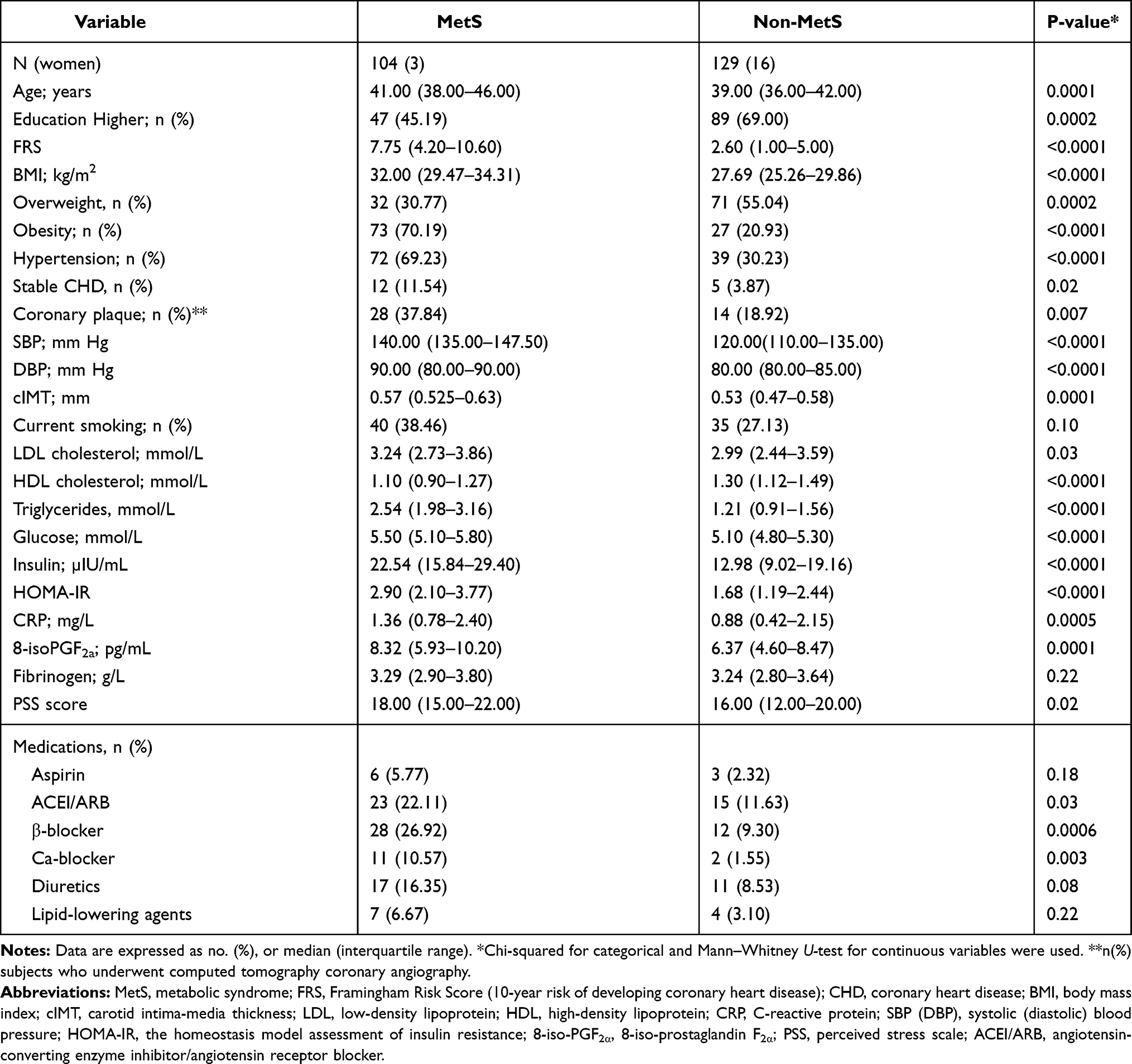 |
Table 1 Characteristics of the Study Subjects, as Stratified by MetS Status |
Prevalence of Metabolic Syndrome Components
We also stratified the subjects with regard to the actual number of MetS components (Table 2). The individual MetS components, ie, central obesity, blood pressure systolic ≥130 mm Hg or/and diastolic ≥85 mm Hg, hypertriglyceridemia, low HDL cholesterol, and higher fasting glucose were found in 70.94%, 59.66%, 47.64%, 24.46%, and 22.32% of the subjects, respectively. Only 33 (14.16%) of the subjects had no MetS components, while the clusters comprising 2 and 3 components were most frequently found (24.46% and 24.90%, respectively) (Table 2). The subjects with 4 and 5 MetS components are presented together as ≥4. The number of MetS components increased with the subjects’ age (median 38.00 [interquartile range 35.00–39.00] years) for the subjects without any, and median 42.00 [interquartile range 40.00–47.00] years) for the subgroup of subjects with ≥4 MetS components). As the total number of MetS components rose, the proportion (%) of subjects with a specific MetS component also increased, especially those in each subgroup with the higher values of waist circumference, systolic (diastolic) blood pressure, and plasma triglyceride levels (Table 2). The cluster comprising higher “waist circumference, blood pressure and triglycerides” was found in 72 (69.23%) of the MetS subjects (data not comprised in the table).
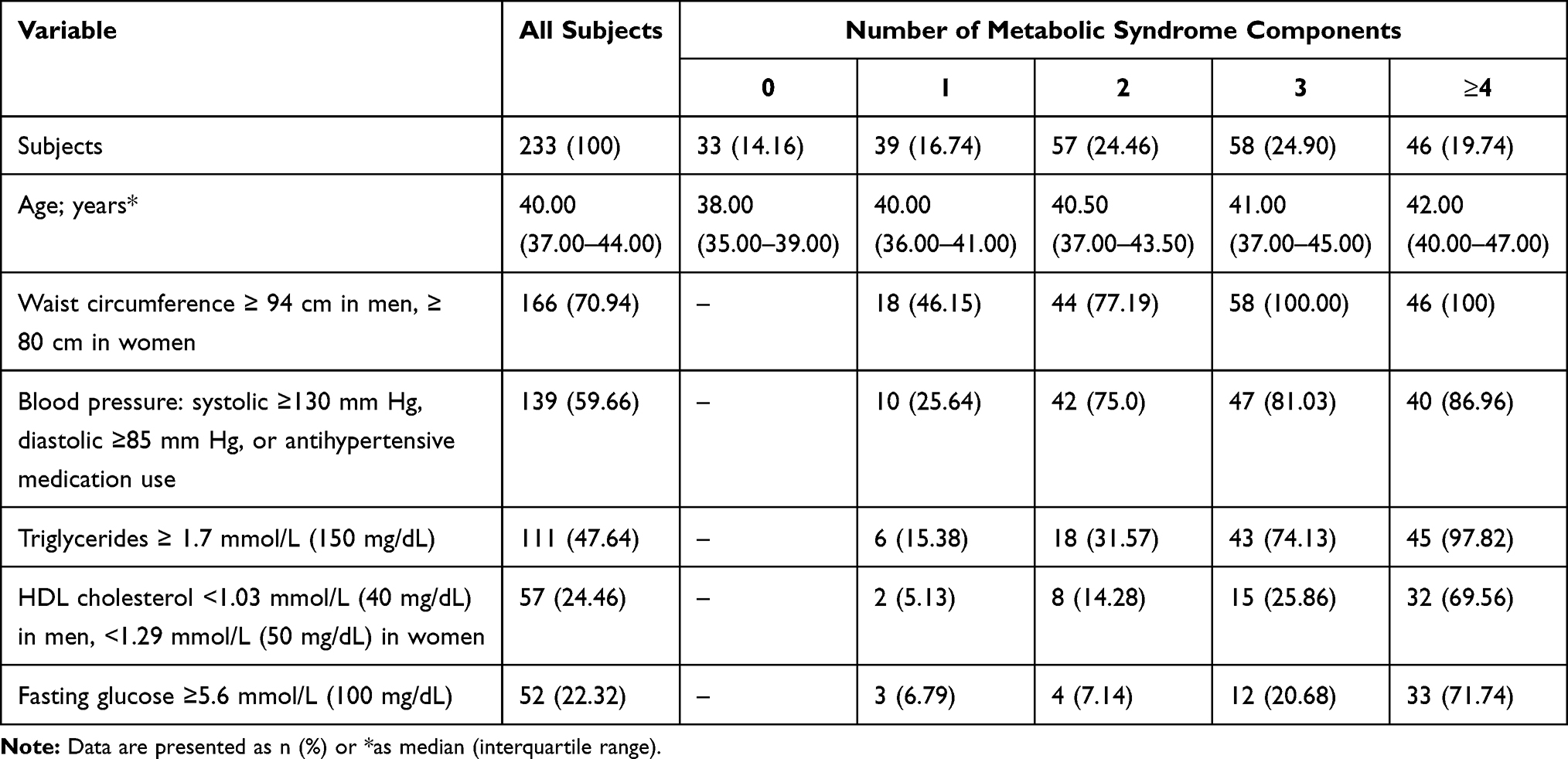 |
Table 2 Prevalence of Metabolic Syndrome Components |
Clinical Variables, Plasma 8-iso-PGF2α Levels Depending on the MetS Components Status
In Table 3, the values of clinical variables were presented depending on the actual number of MetS components. Obesity and hypertension were confirmed in 100 (42.92), 111 (47.64%), whereas coronary artery plaques in 42 (27.63%) of the subjects, respectively. The prevalence of subjects with coronary plaque, obesity, and hypertension differed significantly between the subgroups stratified by MetS components status (p<0.001 for obesity hypertension, and p=0.001 for coronary plaques) (Table 3). The highest prevalence of any type of coronary artery atherosclerosis (coronary plaque and/or stenosis) was found in the subjects with ≥4 MetS components, as compared to those with 1 MetS component (p=0.02). No statistical significance was established in the prevalence of coronary plaque in the remaining subgroups (ie, with 2, and 3 MetS components), as compared to the subjects with 1 MetS component.
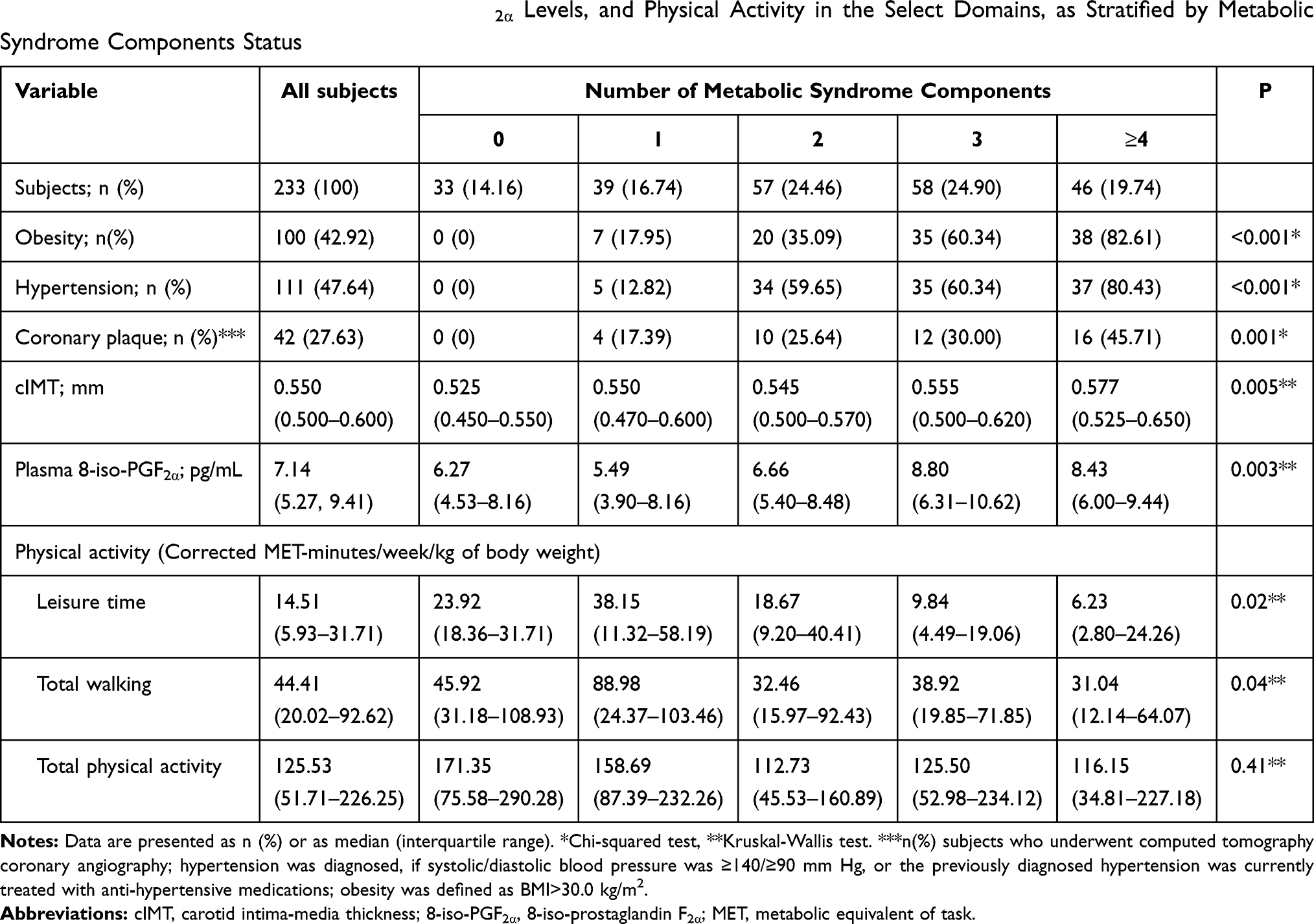 |
Table 3 Clinical Variables and Plasma 8-Iso-PGF2α Levels, and Physical Activity in the Select Domains, as Stratified by Metabolic Syndrome Components Status |
The median [interquartile range] values of cIMT were significantly higher in the subjects with 3 (0.555 [0.500–0.620]) mm, and ≥4 MetS components (0.577 [0.525–0.650]) mm, as compared to the ones without MetS components (0.525 [0.450–0.550]) mm, p=0.003, and p<0.0001, respectively (Table 3). Also in the subjects with 1 and 2 MetS components, the median of cIMT values was higher, although the differences were approximated to the significance level (p=0.051, and p=0.53, respectively) (Table 3).
The MetS subjects had higher plasma median [interquartile range] 8-iso-PGF2α level (8.32 [5.93–10.20]) pg/mL, as compared to the non-MetS ones (6.37 [4.60–8.47]) pg/mL, p=0.0001 (Table 1). With regard to gender, the median level of 8-iso-PGF2α was non-significantly lower in women, as compared to men (5.86 [4.19–9.06] vs 7.21 [5.30–9.52], p=0.14) (not comprised in the table). A significant difference (p=0.003) in plasma of 8-iso-PGF2α level, depending on the number of MetS components, was also encountered (Table 3). The subjects with 3 and ≥4 components had significantly higher plasma 8-iso-PGF2α levels, as compared to those with no MetS components (8.80 [6.31–10.62] pg/mL and 8.43 [6.00–9.44] pg/mL vs 6.27 [4.53–8.16] pg/mL), p=0.001, p=0.01, respectively. In turn, the median levels of 8-iso-PGF2α in the subjects with 1 and 2 MetS components were non-significantly different, as compared to the subjects with no MetS components (p=0.62, p=0.44, respectively).
Physical Activity Depending on the MetS Components Status
The results in select domains of physical activity (expressed as MET-minutes/week/kg of body weight depending on the actual number of MetS components) are demonstrated in Table 3. Significant differences were found in leisure-time physical activity (p=0.02), and total walking (p=0.04), but not in total physical activity (p=0.41). As compared to the subjects with no MetS components, significantly lower median leisure-time physical activity (23.92 [18.36–31.71] vs 6.23 [2.80–24.26], p=0.04) and total walking (45.92 [31.18–108.93] vs 31.04 [12.14–64.07], p=0.03) were found in the subjects with ≥4 MetS components. As compared to those with a single MetS component, median leisure-time physical activity was significantly lower (38.15 [11.32–58.19] vs 9.84 [4.49–19.06], p=0.003), and total walking approximated the significance level (88.98 [24.37–103.46] vs 38.92 [19.85–71.85], p=0.06) also in the subjects with 3 MetS components.
In univariate linear analyses, negative associations were found between waist circumference and leisure-time physical activity (B=−0.074, 95% CI [−0.147, −0.002], p=0.04), total walking (B=−0.032, 95% CI [−0.060, −0.003], p=0.02) and total physical activity (B=−0.013, 95% CI [−0.026, −0.001], p=0.03). Similar associations between those domains of physical activity and plasma triglycerides level were also observed (p=0.04, p=0.03 and p=0.02, Table 4). There were no any associations between selected domains of physical activity and other variables, such as S(D)BP, HOMA-IR, or glucose, HDL cholesterol, and plasma 8-iso-PGF2α.
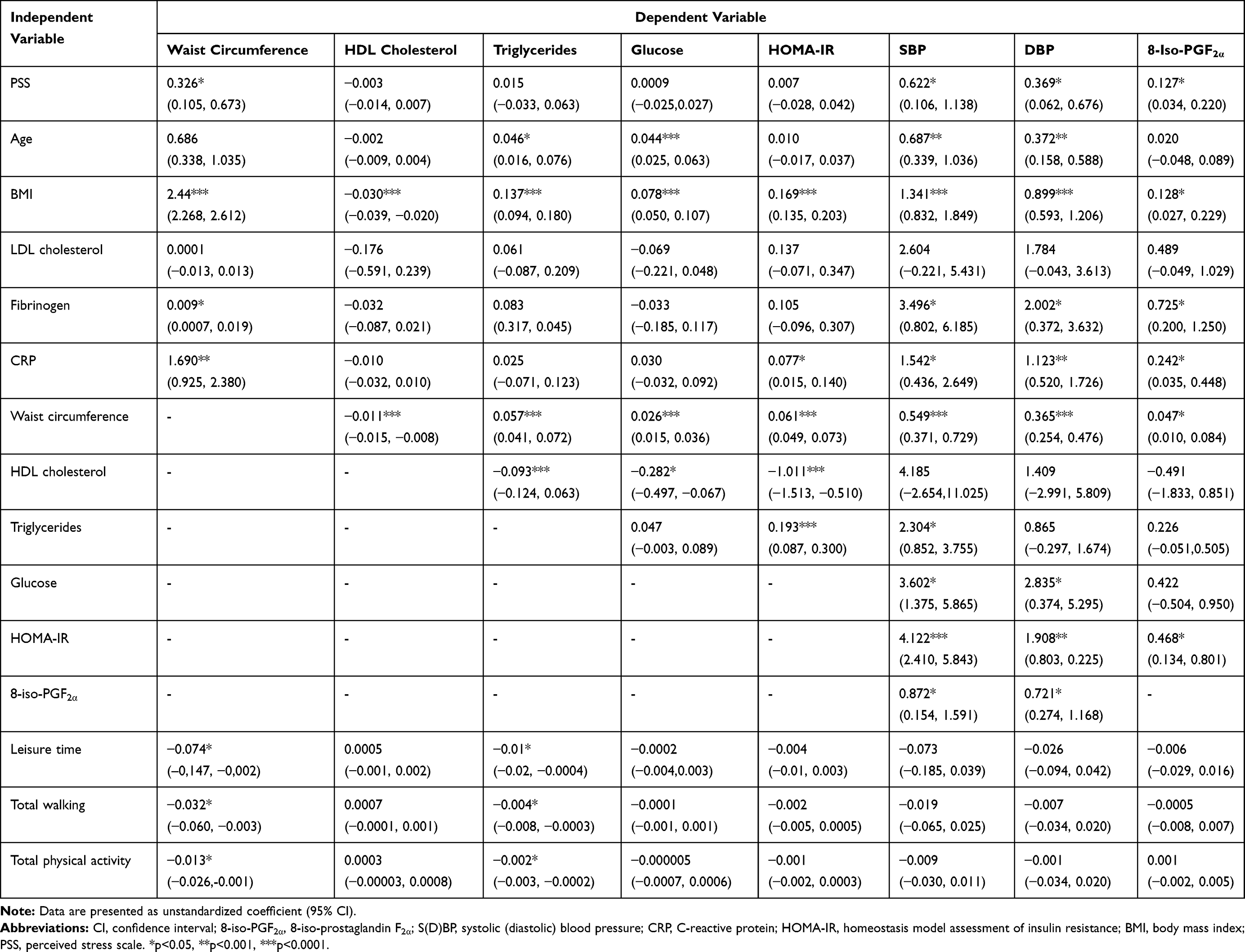 |
Table 4 Associations Between Respective Variables in Univariate Linear Analyses, for All Study Subjects |
Associations Between Perceived Stress, Plasma 8-iso-PGF2α and CVD Risk Factors for All Study Subjects
The associations between perceived stress level, plasma 8-iso-PGF2α and CVD risk factors from the univariate analyses for all study subjects are presented in Table 4. Perceived stress was positively associated with waist circumference (B=0.326, 95% CI [0.105, 0.673], p=0.03), blood pressure (B=0.622, 95% CI [0.106, 1.138], and B=0.369, 95% CI [0.062, 0.676], p=0.01); for systolic and diastolic, respectively, and plasma 8-iso-PGF2α levels (B=0.127, 95% CI [0.034, 0.220], p=0.01). On the other hand, in the analyses taking account of gender separately, positive associations of PSS score with waist circumference (B=0.378, 95% CI [0.078, 0.678], p=0.01), systolic (B=0.648, 95% CI [0.118, 1.178], p=0.01), and diastolic (B=0.431, 95% CI [0.108, 0.754], p=0.009) blood pressure were established in men only (data not comprised in the table).
Positive associations were also established between plasma 8-iso-PGF2α levels and waist circumference (B=0.047, 95% CI [0.010, 0.084], p=0.01), BMI (B=0.128, 95% CI [0.027, 0.229], p=0.01), systolic (B=0.872, 95% CI [0.154, 1.591], p=0.01), and diastolic (B=0.721, 95% CI [0.274, 1.168], p=0.001) blood pressure. Furthermore, plasma 8-iso-PGF2α levels were positively associated with HOMA-IR (B=0.468, 95% CI [0.134, 0.801], p=0.01), plasma fibrinogen (B=0.725, 95% CI [0.200, 1.250], p=0.006) and CRP levels (B=0.242, 95% CI [0.035, 0.448], p=0.04).
Systolic blood pressure was positively associated with age (B=0.687, 95% CI [0.339, 1.036], p=0.001), BMI (B=1.341, 95% CI [0.832, 1.849], p<0.0001), waist circumference (B=0.549, 95% CI [0.371, 0.729], p<0.0001), HOMA-IR (B=4.122, 95% CI [2.410, 5.843], p<0.0001), glucose (B=3.602, 95% CI [1.375, 5.865], p=0.001), fibrinogen (B=3.496, 95% CI [0.820, 6.185], p=0.006), and CRP (B=1.542, 95% CI [0.436, 2.649], p=0.005). Similar correlations were related to diastolic blood pressure and the same variables. Other correlations between the variables are presented in Table 4.
With a view to assessing the inter-gender differences, univariate and multivariate linear analyses were pursued separately for men and women; their results are presented in Table 5. In univariate analysis, plasma 8-iso-PGF2α was positively associated with PSS score (B=0.122, 95% CI [0.029, 0.215], p=0.01) in men only. From the variables, whose values, when exceeding the reference range (ie, abnormal), are the key identification attributes of MetS, waist circumference (B=0.056, 95% CI [0.012, 0.101], p=0.01), and systolic blood pressure (B=0.030, 95% [0.004, 0.056], p=0.01) were positively associated with the plasma 8-iso-PGF2α level, also only in men. In multivariate analysis (after adjustment for age and current smoking), positive associations of plasma 8-iso-PGF2α levels with PSS score (B=0.108, 95% CI [0.008, 0.209], p=0.03) and systolic blood pressure (B=0.029, 95% CI [0.003, 0.057], p=0.02) were established. No associations were established in women between plasma 8-iso-PGF2α, PSS score and systolic blood pressure, neither in univariate nor in multivariate analyses (Table 5).
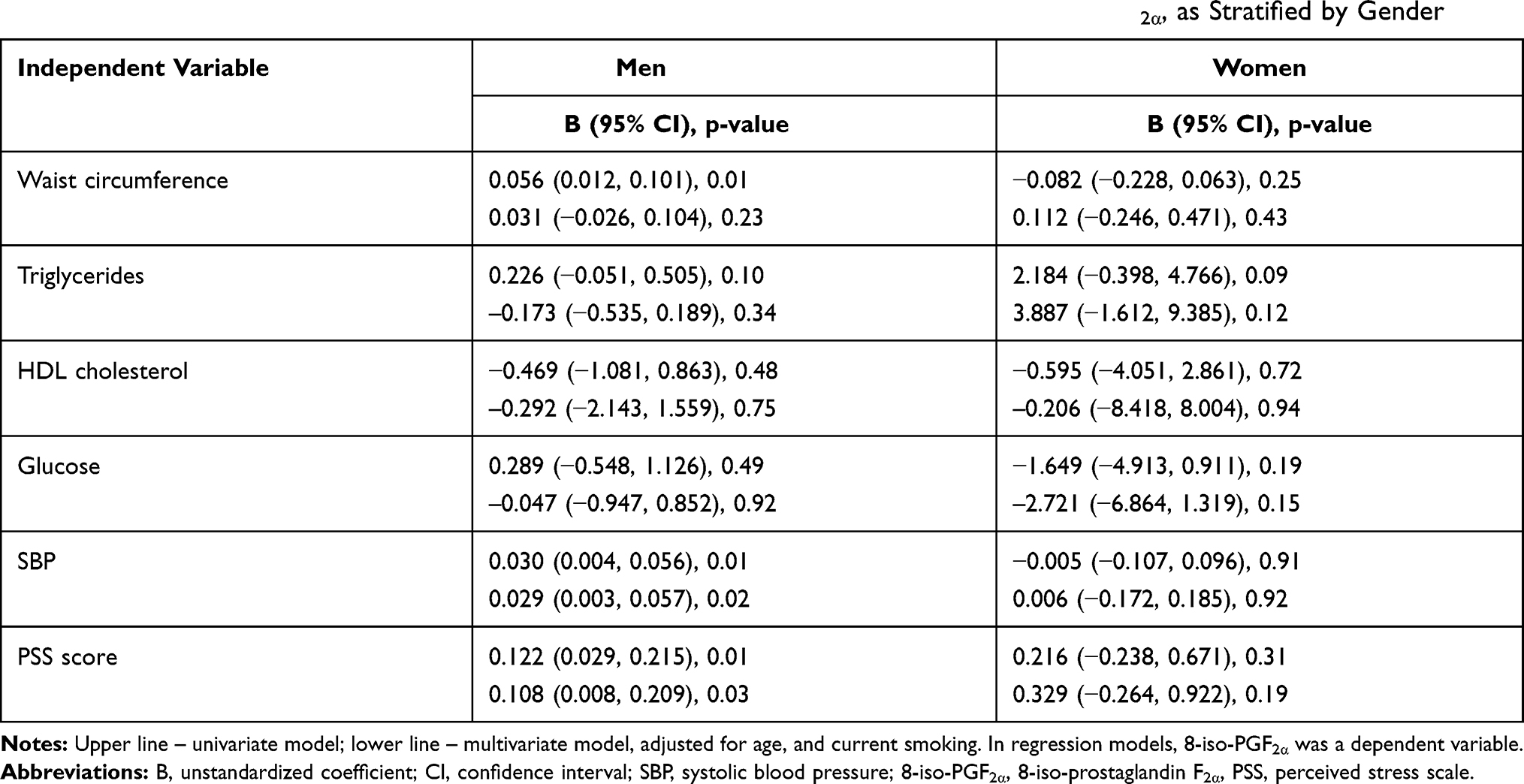 |
Table 5 Results of Linear Regression Regarding the Effect of Select Variables on Plasma 8-Iso-PGF2α, as Stratified by Gender |
Odds Ratios for the Prevalence of Hypertension
As evidenced in Table 6, separately for men and women, crude and adjusted OR (95% CI) regarding the impact of perceived stress, 8-iso-PGF2α and the select variables on the prevalence of hypertension. The effect of some variables on the prevalence of hypertension was encountered in men only. In the univariate analysis, perceived stress (OR=1.135, 95% CI [1.058–1.218], p=0.001), 8-iso-PGF2α levels (OR 1.172, 95% CI [1.064–1.290], p=0.004), waist circumference (OR=1.900, 95% CI [1.054–1.127], p<0.0001), triglycerides (OR=1.298, 95% CI [1.031–1.611], p=0.02), and glucose (OR=2.093, 95% CI [1.204–3.639], p=0.02) affected the prevalence of hypertension. Likewise, after adjustment for age, current smoking, both perceived stress (OR 1.101, 95% CI [1.001–1.202], p=0.03), and plasma 8-iso-PGF2α levels (OR 1.223, 95% CI [1.046–1.432], p=0.01) still affected the prevalence of hypertension in men. Out of the other variables listed in Table 6, the effect of waist circumference (OR=1.138, 95% CI [1.064–1.218], p=0.0001) and glucose (B=2.696, 95% CI [1.081–6.725], p=0.03) on the prevalence of hypertension was also established. None of the above-referenced variables had any effect on the prevalence of hypertension in women, neither in univariate nor in multivariate analyses (Table 6).
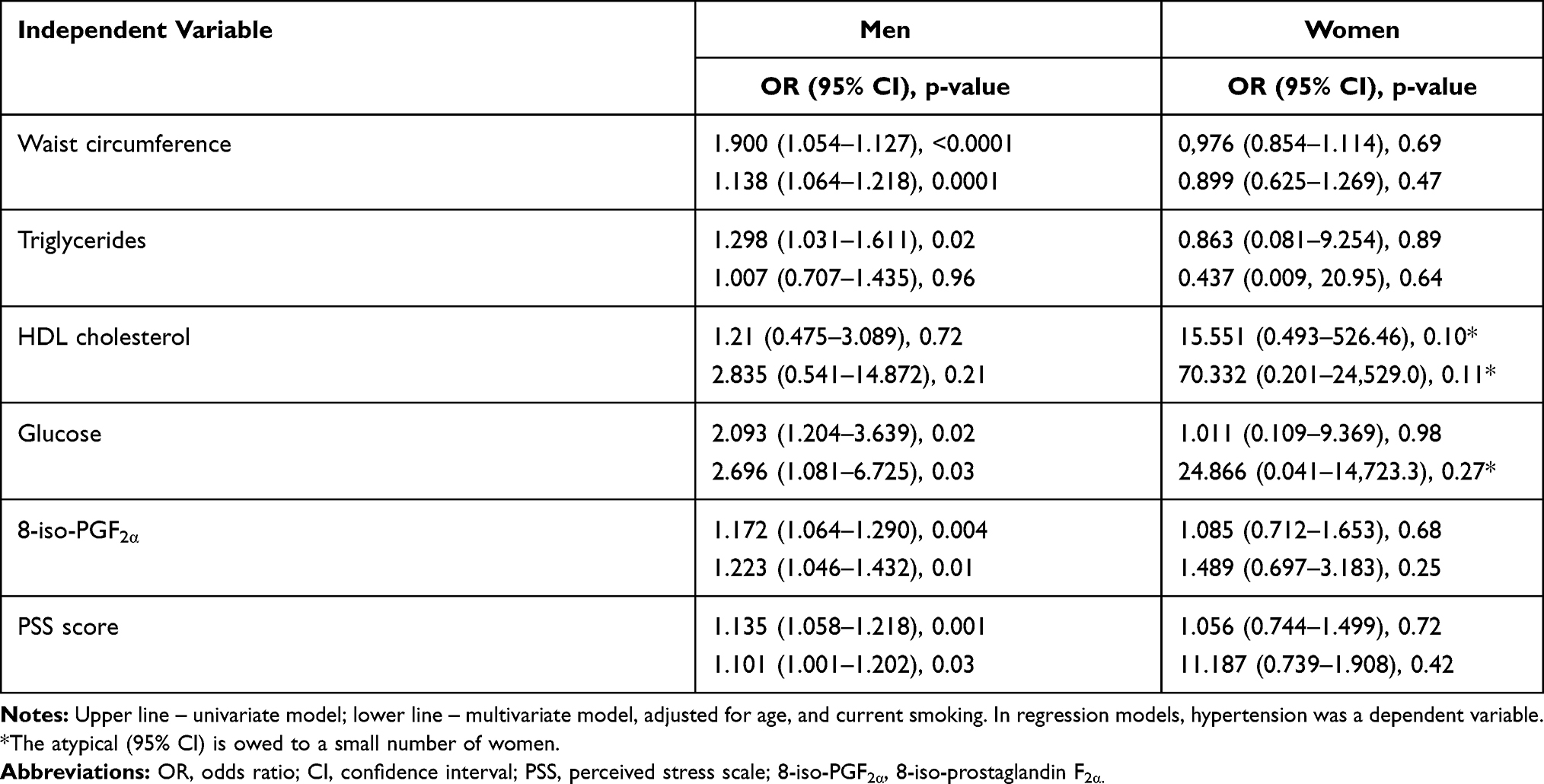 |
Table 6 Results of Logistic Regression Regarding the Prevalence of Hypertension, as Stratified by Gender |
Discussion
To the best of our knowledge, this cross-sectional study is the first one to address the prevalence of MetS components in a cohort of police officers, focused on assessing their association with perceived stress and a marker of systemic oxidative stress. High prevalence of obesity and hypertension, as well as positive association between plasma oxidative stress marker levels with blood pressure were established. Furthermore, perceived stress was found to be associated with plasma 8-iso-PGF2α levels, and consequently both factors were established as instrumental in the prevalence of hypertension, even though these associations were gender-related.
High prevalence of MetS in the study cohort was established, which remains in line with the results of other research.29,30 Almost all studies on MetS in police officers are cross-sectional, and the prevalence of MetS ranged from 23.3% to 70.0%.29–33 The discrepancies between the above-referenced studies may be attributable not only to the age differences within the surveyed populations and the adopted criteria of MetS identification but also to the actual constellation of the cluster of MetS components. The number of MetS components, as well as the prevalence of MetS increased with the subjects’ age in our own study, which also happened to be the case in the study pursued by Garbarino et al.33 As opposed to our own study, only 23.2% of the subjects had MetS in the large Chinese study of police officers, but 36.2% of that population was under 35 years of age, whereas in the Tharkar et al study, the entire population was >30 years old.29,32 Interestingly, in another one, from South India region, MetS was established in 70.0% and 48.0% of the subjects, respectively, whilst applying IDF and ATP III Asian Indian cut-offs for waist circumference.30
Central obesity, higher blood pressure, and triglycerides were most common, whereas the cluster of those MetS components was also found dominant in our own study. Our results happen to be fully consistent with those of other studies on police officers, in which abdominal obesity (or overall percentage of overweight and obesity) was established in 65.0%–85.0% of the subjects.29,30,33–35 A large percentage (57.32%) of our population sample had blood pressure ≥130/85 mm Hg, whereas hypertension was confirmed in 47.64% of the subjects. The published data indicated the prevalence of higher blood pressure in 31.0%–58.5%, and hypertension in 28.0%–51.5% of police officers.29,33–35 Higher prevalence of hypertension in police officers, as compared to general population (51.5% vs 36.2%), was also reported.34
High percentage of the subjects with higher plasma triglyceride levels was demonstrated in the study by Tharkar et al, whereas in yet another one, focused specifically on police officers, reduced HDL cholesterol levels was a most common feature.29,31 It was reported that specific clusters of MetS components rather than MetS as such were associated with a higher risk of cardiovascular events in the Framingham Heart Study.36,37 In our own study, clinical variables of atherosclerosis, increased cIMT, and coronary plaque were most often found in the subjects with ≥3 MetS components (a specific cluster “waist circumference, blood pressure and triglycerides” was found in 69.23% of them). Exposure to a job-specific stress among police officers increased the chances for the prevalence of MetS and accounted for the prevalence of coronary plaque.7
Our study highlighted that perceived stress was associated with two MetS components only, ie, excessive waist circumference and elevated blood pressure. The results may indicate a complex (possibly an additional) mechanism for the development of hypertension in this occupational group, as the perceived stress was related to waist circumference (obesity index), and plasma 8-iso-PGF2α (a marker of oxidative stress), and so all three variables increased the chance prevalence of hypertension. We did not measure the work-related stress, but total perceived stress instead. It is widely believed that specific source(s) of stress may be less important than overall perceived stress level, as well as individual perception of work environment may be more dependent on individual personality traits.8,25
In the present study, the gender-related differences were established. Higher levels of perceived stress in women were also documented by other investigators, remaining in full compliance with the norms proposed by Cohen.38–40 On the other hand, higher plasma of 8-iso-PGF2α levels, and the associations observed between the variables under study were encountered in men only, which may be related to a higher cardiovascular risk burden profile in men. Gender-related differences in the prevalence of obesity, hypertension and MetS were also established in Quebec police officers, as well as in the Chinese ones.32,41 Unlike to our own study, associations between abdominal obesity with police stress were reported in women only in the Hartley study.31 There were no associations whatsoever established between the study variables in women in the present study. It should therefore be duly noted at this juncture that the percentage of women was very small, so on no account would this render itself to any definitive conclusions to be drawn in this issue.
In our study, out of the non-MetS subjects, over 20% were obese, over 50% overweight, and 30% were hypertensive. Obesity is prevalent for years ahead of the actual development of other metabolic disorders which jointly stand for MetS. A positive association of cumulative and chronic psychological stress with a prevalent dietary paradigm and obesity indices was acknowledged. Besides, unhealthy lifestyle (low physical activity and potentially detrimental individual eating habits) also contributes to increasing the global prevalence rate of hypertension.42,43 Even though physical inactivity is a detrimental behavioural paradigm strongly associated with obesity and MetS, a large proportion of the world’s population remains physically inactive.44 Lack of regular physical activity, or physical inactivity, accounts for 6%–10% of major non-communicable diseases, whereas individual life expectancy may increase in the subjects boasting higher physical activity level.45 On the other hand, the meta-analysis of prospective cohort studies revealed that while a moderate level of work-related physical activity reduced the risk of CHD, high physical activity at work did not actually add to a potential protective effect.46
In our previous study of police officers, intensity of total physical activity was well above the average for adults. Furthermore, leisure-time physical activity reduced the chances of developing MetS in police officers, and similar results were demonstrated recently by Zhang et al.7,32 In the present study, intensity of leisure physical activity and total walking time variable were negatively associated with waist circumference and plasma triglycerides levels. On top of this, the lowest levels of physical activity within the two domains were found in the subjects with ≥4 MetS components. Similar to our own study, shorter total walking time in police officers, as compared to general population, was reported in the Tharhar et al.29 As established by Shiozaki et al, long-term exposure to stressful work and closely related, unhealthy lifestyle would account for a greater number of clustered CHD risk factors in police officers.47
Consequently, differences in the prevalence of obesity and MetS between respective studies of police officers, as pursued in different countries, may also be due to the differences in physical activity levels. Regretfully, only a few studies of police officers actually took due note of physical activity.7,29,32 Also shift work, and chronic sleep problems (disturbance/deprivation) stand for essential causal factors promoting prevalence of obesity, hypertension, and MetS in police officers.48–50 Shift work is associated with disruption of circadian rhythms, increased hormone levels, and overactivation of the sympathetic nervous system.
Catecholamines and adrenal glucocorticoids, following exposure to psychological stress, facilitate glucose availability and increase the metabolic rate, which in turn increases spontaneous mitochondrial production of ROS, leading to reduced bioavailability of nitric oxide and hypertension.51 In the present study, glucose also contributed to the prevalence of hypertension, whereas the association of insulin resistance with hypertension had previously been highlighted.21 Although large antioxidant supplementation trials, as pursued in the populations deemed exposed to high cardiovascular risk, exerted no mitigating effect on blood pressure, it was nevertheless demonstrated that the hypotensive effect of angiotensin-converting enzyme (ACE) inhibitors and Ang 1 receptor blockers was owed to inhibiting NADPH oxidase and decreased ROS production.52,53
Oxidative stress might be a contributing factor, as neither genetic, nor behavioural factors, nor indeed psychological stress at large, are fully capable of conclusively explaining the actual pathomechanism of hypertension. Vasoconstrictive properties of 8-iso-PGF2α might account for the association between oxidative stress marker and hypertension.54,55 Significantly higher plasma 8-iso-PGF2α levels were found in the MetS subjects, as well as an association with a number of MetS components was reported. Some investigators attested to the increased 8-iso-PGF2α levels in the MetS subjects, or to associations with some of the MetS components only, whereas others reported no such associations.16,18,19,56 As opposed to our own study design, those studies were focused exclusively on investigating plasma or urine total isoprostane levels.
Establishment of positive associations between CRP and 8-iso-PGF2α, as well as with other select variables under study (waist circumference, blood pressure, HOMA-IR) appears to be a significant study finding. Inflammation plays a critical role in the development of MetS, and, being involved in the progression of atherosclerosis at every stage of its development, contributes to CVD risk. In the obese subjects, an enhanced production of pro-inflammatory cytokines by adipocytes induce liver CRP synthesis and have contributed to MetS and the development of insulin resistance. On the other hand, ROS stimulate a pro-inflammatory signalling pathway, linking oxidative stress with inflammatory state and also in insulin resistance and MetS.18,21,57 In a stressful situation, both an ingestion of calories-rich foods, and anabolic-catabolic imbalance (high cortisol, insulin, low levels of the opposite hormones), may lead to oxidative stress, and systemic inflammation associated with MetS.
Clinical studies regarding the association between of 8-iso-PGF2α levels and blood pressure or hypertension are scarce.58,59 Higher plasma 8-iso-PGF2α levels in the patients with resistant hypertension, as compared to well-controlled hypertensive patients, were reported by de Faria et al.17 The opposite results were yielded by the urine isoprostane studies. A positive association was established in the study of Horbal et al, whereas Melton et al, whilst measuring urine four F2-isoprostanes, established no prospective associations, neither for systolic nor diastolic blood pressure.59,60 Oxidative stress may constitute a unifying link between psychological stress and hypertension, especially in the police officers, although this supposition still calls for further research to make it fully credible. It has also been proposed that oxidative stress amplifies blood pressure elevation in the presence of other prohypertensive factors whose clustering is encountered in the MetS subjects.61
Exposure to a job-specific stress among police officers is associated with a higher prevalence of hypertension, which increases the risk of developing atherosclerosis. Our results may indicate a complex mechanism which underlays the development of hypertension, inclusive of the impact of perceived stress, and metabolic factors such as obesity and oxidative stress. By undertaking early medical check-ups aimed at general prevention, entailing regular measurement of blood pressure, ultrasound cIMT, or CTCA assessment, it might be feasible to identify the subjects particularly exposed to higher psychological stress in their occupations, who happen to be in need of more target-oriented therapeutic management, aimed specifically at reducing overall risk of atherosclerosis-related complications and mortality.
Limitations
Several likely limitations of the present study need to be acknowledged, though. The Authors were unable to make use of randomization, and consequently the entire study protocol was based on the subjects’ voluntary participation. Authors had no say whatsoever as to who would ultimately enrol into the study, which ultimately accounted for the selection bias. Also, a large percentage of the subjects with MetS does not reflect its prevalence in the country’s overall police population, as we estimated its prevalence in the group of individuals who had actually volunteered for the study protocol. The study was carried out on a relatively small population sample, so our results are still subject to prospective corroboration by the studies pursued on a larger population. Besides, the study subjects differed in their CVD risk factors and medication intake which might also affect the outcomes. Notably, we were unable to evaluate any specific sources of stress in the actual police work, for reasons beyond our control (ie, classified data). As the Authors had no access to the information regarding the operational specifics of police work, they were unable to make any inferences about any other factors that may potentially have influenced the select variables under study, nor indeed draw any conclusions as to the nature of their interrelationships within the study cohort. The Authors addressed a single marker of oxidative stress only, without pursuing assessment of antioxidative enzymes, or other substance which would provide information about the redox homeostasis in vivo. Finally, as the present study is of a cross-sectional design, the actual causal relationships do not really lend themselves to accurate inferences, anyway.
Conclusions
The present study is the first one to highlight the association between the perceived and oxidative stress with MetS components in police officers. Both the perceived and oxidative stress were found instrumental in promoting hypertension in a cohort of police officers under study, whereas all study outcomes were conclusively gender-related.
Abbreviations
MetS, metabolic syndrome; FRS, Framingham Risk Score (10-year risk of developing coronary heart disease); CHD, coronary heart disease; CVD, cardiovascular disease; CTCA, computed tomography coronary angiography; BMI, body mass index; cIMT, carotid intima-media thickness; LDL, low-density lipoprotein; HDL, high-density lipoprotein; CRP, C-reactive protein; SBP (DBP), systolic (diastolic) blood pressure; HOMA-IR, the homeostasis model assessment of insulin resistance. PSS-10, perceived stress scale; 8-iso-PGF2α, 8-iso-prostaglandin F2α; ACEI/ARB, angiotensin-converting enzyme inhibitor/angiotensin receptor blocker; OR, odds ratio; CI, confidence interval; MET, metabolic equivalent of task.
Data Sharing Statement
The datasets generated during and/or analysed during the present study are not publicly available due to statutory confidentiality constraints applicable to police work, but might be made accessible in a restricted, anonymised scope from the Corresponding Author, upon reasonable request.
Ethics Approval
The study was approved by the local Bioethics Review Committee (Ref. no KBET/90/B/2011); an informed, written consent to attend the study protocol was granted by all participants.
Consent for Publication
Not applicable.
Author Contributions
The Authors contributed to data analysis, drafting, or revising the article have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The present study was financed out of the University’s statutory resources for the pursuit of in-house research projects; no extra funding was provided by any external sources.
Disclosure
The authors have no competing interests to disclose.
References
1. Ninomiya JK, L’Italien G, Criqui MH, et al. Association of the metabolic syndrome with history of myocardial infarction and stroke in the Third National Health and Nutrition Examination Survey. Circulation. 2004;109(1):42–46. doi:10.1161/01.CIR.0000108926.04022.0C
2. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
3. O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet. 2010;376(9735):112–123. doi:10.1016/S0140-6736(10)60834-3
4. Lawes CM, Vander Hoorn S, Rodgers A. Global burden of blood-pressure-related disease, 2001. Lancet. 2008;371(9623):1513–1518. doi:10.1016/S0140-6736(08)60655-8
5. Hall JE, Do Carmo JM, da Silva AA, et al. Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ Res. 2015;116(6):991–1006. doi:10.1161/CIRCRESAHA.116.305697
6. Steptoe A. Psychosocial factors in the development of hypertension. Ann Med. 2000;32(5):371–375. doi:10.3109/07853890008995940
7. Janczura M, Bochenek G, Nowobilski R, et al. The relationship of metabolic syndrome with stress, coronary heart disease and pulmonary function - an occupational cohort-based study. PLoS One. 2015;10(8):e0133750. doi:10.1371/journal.pone.0133750
8. Spruill TM, Butler MJ, Thomas SJ, et al. Association between high perceived stress over time and incident hypertension in black adults: findings from the Jackson heart study. J Am Heart Assoc. 2019;8(21):e012139. doi:10.1161/JAHA.119.012139
9. Wiernik E, Pannier B, Czernichow S, et al. Occupational status moderates the association between current perceived stress and high blood pressure evidence from the IPC cohort study. Hypertension. 2013;61:571–577. doi:10.1161/HYPERTENSIONAHA.111.00302
10. Montezano AC, Touyz RM. Molecular mechanisms of hypertension–reactive oxygen species and antioxidants: a basic science update for the clinician. Can J Cardiol. 2012;28(3):288–295. doi:10.1016/j.cjca.2012.01.017
11. Grande MT, Pascual RAS, et al. Increased oxidative stress, the renin-angiotensin system, and sympathetic over activation induce hypertension in kidney androgen-regulated protein transgenic mice. Free Radic Biol Med. 2011;51(10):1831–1841. doi:10.1016/j.freeradbiomed.2011.08.014
12. Hamza SM, Dyck JR. Systemic and renal oxidative stress in the pathogenesis of hypertension: modulation of long-term control of arterial blood pressure by resveratrol. Front Physiol. 2014;5:292. doi:10.3389/fphys.2014.00292
13. Song L, Zheng J, Li H, et al. Prenatal stress causes oxidative damage to mitochondrial DNA in hippocampus of offspring rats. Neurochem Res. 2009;34(4):739–745. doi:10.1007/s11064-008-9838-y
14. Zafir A, Banu N. Modulation of in vivo oxidative status by exogenous corticosterone and restraint stress in rats. Stress. 2008;12(2):167–177. doi:10.1080/10253890802234168
15. Landmesser U, Cai H, Dikalov S, et al. Role of p47(phox) in vascular oxidative stress and hypertension caused by angiotensin II. Hypertension. 2002;40(4):511–515. doi:10.1161/01.hyp.0000032100.23772.98
16. Fujita K, Nishizawa H, Funahashi T, et al. Systemic oxidative stress is associated with visceral fat accumulation and the metabolic syndrome. Circ J. 2006;70(11):1437–1442. doi:10.1253/circj.70.1437
17. de Faria AP, Fontana V, Modolo R, et al. Plasma 8-isoprostane levels are associated with endothelial dysfunction in resistant hypertension. Clin Chim Acta. 2014;433:179–183. doi:10.1016/j.cca.2014.03.009
18. Black CN, Bot M, Scheffer PG, Penninx BW. Sociodemographic and lifestyle determinants of plasma oxidative stress Markers 8-OHdG and F2-isoprostanes and associations with metabolic syndrome. Oxid Med Cell Longev. 2016;2016:7530820. doi:10.1155/2016/7530820
19. Keaney JF
20. Seet RC, Lee CY, Lim EC, et al. Markers of oxidative damage are not elevated in otherwise healthy individuals with the metabolic syndrome. Diabetes Care. 2010;33(5):1140–1142. doi:10.2337/dc09-2124
21. Janczura M, Dropinski J, Gielicz A, et al. Potential roles of psychological and oxidative stress in insulin resistance: a cohort-based study. Diabetol Metab Syndr. 2020;12:58. doi:10.1186/s13098-020-00566-8
22. Magnavita N, Capitanelli I, Garbarino S, Pira E. Work-related stress as a cardiovascular risk factor in police officers: a systematic review of evidence. Int Arch Occup Environ Health. 2018;91(4):377–389. doi:10.1007/s00420-018-1290-y
23. Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645. doi:10.1161/CIRCULATIONAHA.109.192644
24. Williams B, Mancia G, Spiering W, et al. ESC Scientific Document Group. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39(33):3021–3104. doi:10.1093/eurheartj/ehy339
25. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
26. Morrow JD, Roberts LJ. Mass spectrometric quantification of F2-isoprostanes in biological fluids and tissues as measure of oxidant stress. Methods Enzymol. 1999;300:3–12. doi:10.1016/s0076-6879(99)00106-8
27. Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 Compendium of physical activities: the second update of activity codes and MET intensities to classify the energy cost of human physical activities. Med Sci Sports Med. 2011;43(8):1575–1581. doi:10.1249/MSS.0b013e31821ece12
28. Kozey S, Lyden K, Staudenmayer J, Freedson P. Errors in MET estimates of physical activities using 3.5 mL x kg(−1) x min(−1) as the baseline oxygen consumption. J Phys Act Health. 2010;7(4):508–516. doi:10.1123/jpah.7.4.508
29. Tharkar S, Kumpatla S, Muthukumaran P, Viswanathan V. High prevalence of metabolic syndrome and cardiovascular risk among police personnel compared to general population in India. J Assoc Physicians India. 2008;56:845–849.
30. Ramakrishnan J, Majgi SM, Premarajan KC, et al. High prevalence of cardiovascular risk factors among policemen in Puducherry, South India. J Cardiovasc Dis Res. 2013;4(2):112–115. doi:10.1016/j.jcdr.2013.05.002
31. Hartley TA, Burchfiel CM, Fekedulegn D, et al. Associations between police officer stress and the metabolic syndrome. Int J Emerg Ment Health. 2011;13(4):243–256.
32. Zhang J, Liu Q, Long S, et al. Prevalence of metabolic syndrome and its risk factors among 10,348 police officers in a large city of China: a cross-sectional study. Medicine (Baltimore). 2019;98(40):e17306. doi:10.1097/MD.0000000000017306
33. Garbarino S, Magnavita N. Work stress and metabolic syndrome in police officers. A prospective study. PLoS One. 2015;10(12):e0144318. doi:10.1371/journal.pone.0144318
34. Ramey SL, Downing NR, Franke WD. Milwaukee police department retirees: cardiovascular disease risk and morbidity among aging law enforcement officers. AAOHNJ. 2009;57911:448–453. doi:10.3928/08910162-20091019-02
35. Ramey SL, Perkhounkova Y, Downing NR, Culp KR. Relationship of cardiovascular disease to stress and vital exhaustion in an urban, midwestern police department. AAOHN J. 2011;59(5):221–227. doi:10.3928/08910162-20110418-02
36. Franco OH, Massaro JM, Civil J, et al. Trajectories of entering the metabolic syndrome. The Framingham heart study. Circulation. 2009;120(20):1943–1950. doi:10.1161/CIRCULATIONAHA.109.855817
37. Scuteri A, Laurent S, Cucca F, et al. Metabolic syndrome across Europe: different clusters of risk factors. Eur J Prev Cardiol. 2015;22(4):486–491. doi:10.1177/2047487314525529
38. Andreou E, Alexopoulos EC, Lionis C, et al. Perceived stress scale: reliability and validity study in Greece. Int J Environ Res Public Health. 2011;8(8):3287–3298. doi:10.3390/ijerph8083287
39. Juczynski Z, Oginska-Bulik N. Narzędzia Pomiaru Stresu I Radzenia Sobie Ze Stresem [Tools for Measuring Stress and the Ways of Coping with It]. Warszawa: Pracownia Testow Psychologicznych; 2009.
40. Cohen S, Williamson G. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The Social Psychology of Health: Claremont Symposium on Applied Social Psychology. Newbury Park: CA: Sage Publications, Inc; 1988:31–67.
41. Gendron P, Lajoie C, Laurencelle L, Trudeau F. Cardiovascular health profile among Quebec male and female police officers. Arch Environ Occup Health. 2019;74(6):331–340. doi:10.1080/19338244.2018.1472063
42. Block JP, He Y, Zaslavsky AM, Ding L, Ayanian JZ. Psychosocial stress and change in weight among US adults. Am J Epidemiol. 2009;170(2):181–192. doi:10.1093/aje/kwp104
43. Steptoe A, Willemsen G. The influence of low job control on ambulatory blood pressure and perceived stress over the working day in men and women from the Whitehall II cohort. J Hypertens. 2004;22(5):915–920. doi:10.1097/00004872-200405000-00012
44. Petersen CB, Nielsen AJ, Bauman A, Tolstrup JS. Joint association of physical activity in leisure and total sitting time with metabolic syndrome amongst 15,235 Danish adults: a cross-sectional study. Prev Med. 2014;69:5–7. doi:10.1016/j.ypmed.2014.08.022
45. Lee IM, Shiroma EJ, Lobelo F, et al. Lancet Physical Activity Series Working Group. Effect of physical inactivity on the world’s major non-communicable diseases. Lancet. 2012;380(9838):219–229. doi:10.1016/S0140-6736(12)61031-9
46. Li J, Siegrist J. Physical activity and risk of cardiovascular disease - a meta-analysis of prospective cohort studies. Int J Environ Res Public Health. 2012;9(2):391–407. doi:10.3390/ijerph9020391
47. Shiozaki M, Miyai N, Morioka I, et al. Job stress and behavioral characteristics in relation to coronary heart disease risk among Japanese police officers. Ind Health. 2017;55(4):369–380. doi:10.2486/indhealth.2016-0179
48. Garbarino S, Magnavita N. Sleep problems are a strong predictor of stress-related metabolic changes in police officers. A prospective study. PLoS One. 2019;14(10):e0224259. doi:10.1371/journal.pone.0224259
49. Magnavita N, Garbarino S. Sleep, health and wellness at work: a scoping review. Int J Environ Res Public Health. 2017;14(11):1347. doi:10.3390/ijerph14111347
50. Ma CC, Burchfiel CM, Fekedulegn D, et al. Association of shift work with physical activity among police officers: the Buffalo cardio-metabolic occupational police stress study. J Occup Environ Med. 2011;53(9):1030–1036. doi:10.1097/JOM.0b013e31822589f9.PMID:21866054
51. Spiers JG, Chen HJ, Sernia C, Lavidis NA. Activation of the hypothalamic-pituitary-adrenal stress axis induces cellular oxidative stress. Front Neurosci. 2015;8:456. doi:10.3389/fnins.2014.00456
52. Yusuf S, Dagenais G, Pogue J, et al. Vitamin E supplementation and cardiovascular events in high-risk patients. The heart outcomes prevention evaluation study investigators. N Engl J Med. 2000;342(3):154–160. doi:10.1056/nejm200001203420302
53. Ghiadoni L, Magagna A, Versari D, et al. Different effect of antihypertensive drugs on conduit artery endothelial function. Hypertension. 2003;41(6):1281–1286. doi:10.1161/01.HYP.0000070956.57418.22
54. Takahashi K, Nammour TM, Fukunaga M, et al. Glomerular actions of a free radical-generated novel prostaglandin, 8-epi-prostaglandin F2α, in the rat. Evidence for interaction with thromboxane A2 receptors. J Clin Invest. 1992;90(1):136–141. doi:10.1172/JCI115826
55. Sametz W, Grobuschek T, Hammer-Kogler S, et al. Influence of isoprostanes on vasoconstrictor effects of noradrenaline and angiotensin II. Eur J Pharmacol. 1999;378(1):47–55. doi:10.1016/s0014-2999(99)00437-9
56. Ercan H, Kiyici A, Marakoglu K, Oncel M. 8-Isoprostane and Coenzyme Q10 levels in patients with metabolic syndrome. Metab Syndr Relat Disord. 2016;14(6):318–321. doi:10.1089/met.2016.0011
57. Romeo GR, Lee J, Shoelson SE. Metabolic syndrome, insulin resistance, and roles of inflammation–mechanisms and therapeutic targets. Arterioscler Thromb Vasc Biol. 2012;32(8):1771–1776. doi:10.1161/ATVBAHA.111.241869
58. Rodrigo R, Prat H, Passalacqua W, et al. Relationship between oxidative stress and essential hypertension. Hypertens Res. 2007;30(20):1159–1167. doi:10.1291/hypres.30.1159
59. Horbal SR, Seffens W, Davis AR, et al. Associations of Apelin, Visfatin, and Urinary 8-isoprostane with severe hypertension in African Americans: the MH-GRID study. Am J Hypertens. 2016;29(7):814–820. doi:10.1093/ajh/hpw007
60. Melton CD, Luo R, Wong BJ, et al. Urinary F2-isoprostanes and the risk of hypertension. Ann Epidemiol. 2017;27(6):391–396. doi:10.1016/j.annepidem.2017.05.005
61. Touyz R, Briones A. Reactive oxygen species and vascular biology: implications in human hypertension. Hypertens Res. 2011;34(1):5–14. doi:10.1038/hr.2010.201
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.