")
Back to Journals » International Journal of General Medicine » Volume 14
The Association of Systemic Interleukin 6 and Interleukin 10 Levels with Sarcopenia in Elderly Patients with Chronic Obstructive Pulmonary Disease
Authors Lin B, Bai L, Wang S, Lin H
Received 24 May 2021
Accepted for publication 9 August 2021
Published 18 September 2021 Volume 2021:14 Pages 5893—5902
DOI https://doi.org/10.2147/IJGM.S321229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Baiyang Lin,1 Li Bai,2 Shenglong Wang,2 Hong Lin3
1Department of Pneumology, Shanxi Provincial People’s Hospital, Taiyuan, 030000, People’s Republic of China; 2Department of Pneumology, Shanxi Hospital of Integrated Traditional and Western Medicine, Taiyuan, 030000, People’s Republic of China; 3Department of Orthopedics, The Sixth Hospital of Shanxi Medical University, Taiyuan, 030000, People’s Republic of China
Correspondence: Li Bai
Department of Pneumology, Shanxi Hospital of Integrated Traditional and Western Medicine, No. 13 of Fudong Street, Xinghualing District, Taiyuan, Shanxi Province, 030000, People’s Republic of China
Tel +86 15935129231
Email [email protected]
Objective: Chronic obstructive pulmonary disease (COPD) is often associated with sarcopenia, and systemic inflammation is an underlying pathogenesis of COPD. In this study, the effects of interleukin (IL)- 6 and IL-10 levels on sarcopenia in patients with COPD were investigated.
Methods: Seventy-three patients (59 males and 14 females), aged 60– 93 years old, who had stable COPD (not including patients with advanced lung decline) were enrolled in this study. The patients were classified according to four stages of lung function, based on the Global Initiative for Chronic Obstructive Lung Disease 2018, and their symptoms were evaluated using the COPD assessment test and mMRC dyspnea Scale. The skeletal muscle index (SMI) was evaluated using a dual-energy X-ray absorptiometry test, and walking pace and handgrip strength were measured to reflect muscle mass and function. The diagnosis of sarcopenia was made according to the Asian Working Group for Sarcopenia and China guide recommendations. The inflammation biomarkers IL-6 and IL-10 were measured by enzyme-linked immunosorbent assay. Albumin (Alb) was measured using the bromocresol green method.
Results: Twenty-eight patients (38.36%) were diagnosed with sarcopenia. IL-6 (r = − 0.38, P = 0.001) and IL-10 (r = − 0.38, P = 0.001) were negatively correlated with the SMI, while the IL-10/IL-6 ratio had no correlation with sarcopenia. Multiple regression analysis showed that age (OR = 1.11, P = 0.02) and IL-6 (OR = 1.07, P< 0.05), had a strong correlation with sarcopenia, while IL-10 was not statistically significant in sarcopenia. However, body mass index (OR = 0.54, P = 0.002) had an opposite effect on muscle reduction.
Conclusion: The increase of IL-6 might be a factor associated with sarcopenia. However, the relationship between IL-10 and sarcopenia is unclear.
Keywords: chronic obstructive pulmonary disease, sarcopenia, cytokine, interleukin-6, interleukin-10
Introduction
Sarcopenia is a progressive disease characterized by systemic skeletal muscle loss, and it is an important component of geriatric syndrome.1 The risk factors include age, long-term bed rest, inadequate nutrient intake, and intestinal dysfunction.1,2 A significant reduction in muscle can jeopardize a person’s general safety and reduce their quality of life3 by increasing the incidence rate of fractures and disability. Sarcopenia can aggravate cardiovascular, respiratory, and endocrine diseases, increasing the mortality rate of those who also have these diseases.4 It has been found that chronic systemic inflammation is closely related to the occurrence of sarcopenia.5 It is known that elderly people with sarcopenia have increased levels of pro-inflammatory cytokines and proteins.6 Systemic inflammation associated with chronic diseases can accelerate aging and muscle loss, and higher levels of inflammatory factors such as interleukin (IL)-6 and C-reactive protein will increase the risk of muscle attenuation.7 The mechanism may be related to Frasca’s findings that inflammatory mediators can affect muscle protein metabolism.8 The treatment for sarcopenia is currently based on aerobic exercise, but some studies have shown that the use of drugs such as vitamin D and omega-3 can attenuate the chronic low-grade inflammation in patients with sarcopenia,9 but the significance of muscle mass recovery is still unclear.
Chronic obstructive pulmonary disease (COPD) is a persistent, obstructed-airway disease mainly characterized by progressive and irreversible dyspnea, and it is directly related to sarcopenia.10 Tobacco smoking is an independent risk factor for COPD, and smoking may promote muscle breakdown and cause sarcopenia,11,12 and patients with COPD often experience weight loss and malnutrition. Studies have shown that body weight is inversely proportional to length of hospitalization13 and that patients with malnutrition have more acute exacerbations and a poor prognosis.14 Malnutrition is also known to promote the progression of sarcopenia,2 and albumin (Alb) is significantly related to nutrition and can be used to predict nutritional levels.15 Therefore, this study has chosen Alb to reflect the patient’s nutritional status.
Chronic inflammation plays an important role in the development of COPD. It not only acts in the acute exacerbation phase but also plays a role in the stable phase.16 The increase of systemic inflammation markers can lead to decreased lung function.16 IL is a classification of inflammatory mediator, regulating the occurrence and progress of chronic inflammation. The role of IL in sarcopenia is still under investigation, and this study investigates the effect of IL on sarcopenia in patients with COPD. To illustrate the problem, the following were measured: the skeletal muscle index (SMI) to assess muscle mass and diagnose sarcopenia; IL-6 and IL-10 to reflect systemic inflammation; and lung function, which can be used to reflect the degree of COPD, according to the forced expiratory volume in the first second of a forced exhalation (FEV1)% value. It was found that the serum concentration of IL-6 and IL-10 and the severity of COPD are related to sarcopenia, and the levels of IL-6 and IL-10 are directly proportional to the severity of COPD.
Materials and Methods
Patient Population
Seventy-three patients with COPD were recruited for this study between April 2017 and July 2018, after being registered with the Department of Respiratory Medicine of Shanxi Hospital of Integrated Traditional Chinese and Western Medicine. The researchers explained the aims and methodology of the study to the patients.
Inclusion Criteria
(1) patients (≥60 years old) with a diagnosis of COPD, according to the Global Initiative for Chronic Obstructive Lung Disease (version 2018) stages, made at least three years before joining the study; (2) patients with a good self-care ability, meaning they can carry out daily life and sports activities. The specific indicators are evaluated based on the Barthel index and include independent eating, bathing, grooming, dressing, going to the toilet, transfer between beds and chairs, walking on flat ground, going up and down stairs, and autonomous control of urine and bowel, with a light dependence or no dependence score (≥60 points), at a stable stage.
Exclusion Criteria
(1) patients who were disabled and unable to give an autonomous response or who showed some cognitive abnormality; (2) patients with long-term (>2 months)17 oral administration of corticosteroids (corticosteroids can regulate metabolism in skeletal muscle by increasing protein breakdown and decreasing protein synthesis)18; (3) patients with diabetes; (4) patients with cardiac pacemaker placement, myocardial infarction, cerebral hemorrhage, acute cerebral infarction, or obvious sequelae of cerebral infarction; (5) patients with inflammatory bowel disease, obstructive sleep apnea syndrome, hyperthyroidism and hypothyroidism, tumor, severe osteoarthritis, or an autoimmune system disease; (6) patients with an acute exacerbation of COPD or those taking anti-infective drugs in the month previous to the study; and (7) patients whose experimental data was missing.
Diagnosis of Sarcopenia
All enrolled patients completed the following examinations:19 ① Pace measurement: the patient performs a 4 m walking test to measure their pace. It is intermittently measured two times, and the pace is averaged. If the pace is >0.8 m/s; ② Grip force measurement: the patient holds the grip to have their dominant handgrip strength measured; a grip strength of >26 kg is normal for a male and one of >18 kg is normal for a female; ③ a dual energy X-ray absorptiometry (DEXA) scan: a DEXA is used to measure the appendicular skeletal muscle mass (ASM) of the extremities. Accordingly, the four-limb SMI, which is ASM/height2, should be an SMI <7.0 kg/m2 for males and an SMI <5.4 kg/m2 for females. Sarcopenia can be diagnosed using the data in two combinations, either ①+ ③or ② + ③.
In total, 73 patients (60–93 years old, 59 males and 14 females) completed the study. At the baseline assessment, structured interviews were conducted, and the sociodemographic characteristics, COPD clinical history, and health status of these patients were collected, including height, weight (calculation of BMI), comorbidities, history of smoking (smoking time, smoking quantity), history of drinking (drinking time, alcohol consumption). This was a cross-sectional study, and all the data were collected during one interview with each participant. The study protocol was approved by the Ethics Committee of the Shanxi Hospital of Integrated Traditional Chinese and Western Medicine and Shanxi Medical University.
Measurement of Pulmonary Function and Quality of Life
The percentages of FEV1/the full forced vital capacity (FVC) and FEV1% were recorded, and the patients were graded. The modified Medical Research Council Dyspnea Scale (mMRC) and the COPD Assessment Test (CAT) questionnaire were used to assess the level of dyspnea and quality of life. Among them, mMRC and CAT score divided into groups below and above 2 and 10 points.
Measurement of Muscle Mass and Function
In this study, a DEXA scan was used to measure the ASM or the SMI. The method was selected based on the assessment accuracy and the patient’s economic situation. Limb muscle function was evaluated by a 4 m walking test and handgrip force test.
Measurement of IL-6 and IL-10 and Alb
IL-6 and IL-10 are two cytokines that are partly released into the blood to regulate immune and inflammatory reactions. Therefore, plasma was used to measure these interleukin levels.20 The patients gave 3 mL of peripheral venous blood in the early morning on an empty stomach. It was then centrifuged at room temperature (4000 rpm for 8 min), and the upper serum was stored in a refrigerator at −80°C. After thawing, the IL-6 and IL-10 indicators were determined, and IL-10/IL-6 was calculated to clarify the proportional relationship between the two indicators.
The serum IL-6 and IL-10 contents were measured by enzyme-linked immunosorbent assay (ELISA). A standard curve was prepared according to the specification, and the plasma to be tested was measured. The optical density value was measured at a wavelength of 450 nm, using a spectrophotometer (provided by the laboratory of Shanxi Medical University) to calculate the serum IL-6 (ELSA kit, Shanghai Xitang Biotechnology Co., Ltd.) and IL-10 (ELSA kit, Shanghai Xitang Biotechnology Co., Ltd.) content.
The Alb content was measured using the bromocresol green method (Alb kit, Kehua Biotechnology Co., Ltd.). After the standard curve was prepared, the plasma Alb level was measured. The optical density value was measured in 30 seconds at a wavelength of 630 nm, using an automatic biochemical analyzer (Hitachi 7600–110, provided by Shanxi Hospital of Integrated Traditional Chinese and Western Medicine) to obtain the Alb concentration.
Statistical Analyses
Statistical analyses were performed using SPSS software (version 23.0). All data were expressed as means ± SD or medians with interquartile ranges. The Kolmogorov–Smirnov test was used to analyze the normality of distribution. Continuous variables were described as means ± SD, and the Student’s t-test was used for comparative analysis. A rank-sum test was used to compare the parameters of non-normal distribution data between the groups. Categorical variables were analyzed using an χ2 test and a t-test with 95% confidence intervals. Pearson’s correlation and Spearman correlation analysis was used to determine the relationships between walking pace, grip strength, SMI and other clinical parameters, such as IL-6,IL-10 and FEV1/FVC,CAT score. Multiple logistic regression analysis, which was performed on all patients, was aimed to find significant determinants of sarcopenia, and P < 0.05 was deemed to indicate statistical significance.
Results
Patient Characteristics
Table 1 gives details of the patients with stable COPD who participated in the study. Of the 73 patients, 14 (19.2%) were female, and 59 (80.8%) were male. Sarcopenia was diagnosed in 28 (38.36%) patients, with an average age of 76.46 ± 9.45 years. Of the 45 (61.64%) patients without sarcopenia, 39 were male, and 6 were female with an average age of 71.18 ± 9.12 years. The patients with sarcopenia were significantly older, had lower BMI values, and they had been smokers for longer. The CAT score was higher in the sarcopenia group (P < 0.05), and the difference was statistically significant, indicating that the quality of life of COPD patients with sarcopenia was worse than that of patients without it. There were no significant differences in gender, hypertension, arrhythmia, smoking quantity, cigarette grade, duration of drinking, or alcohol consumption between patients with and without sarcopenia.
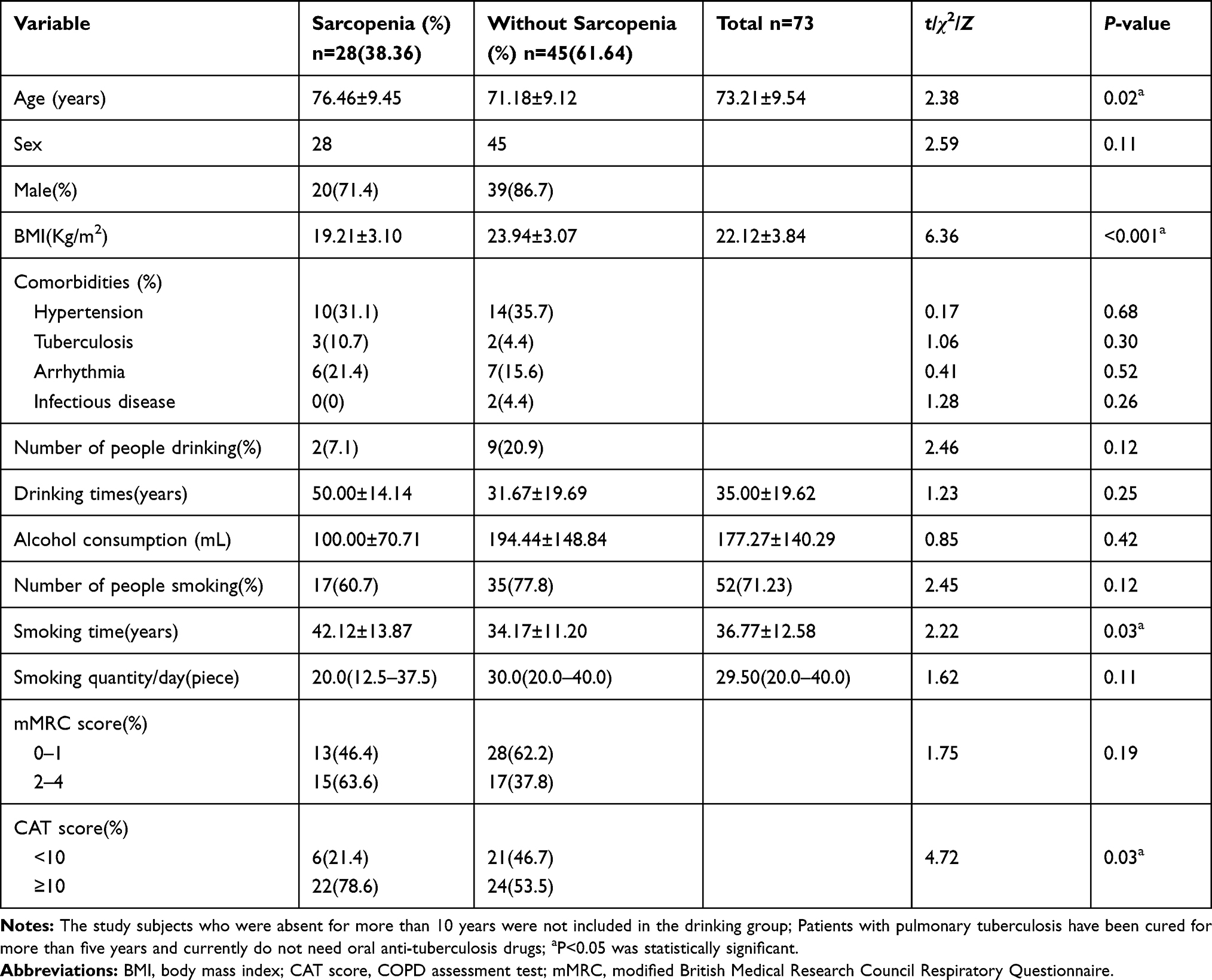 |
Table 1 Baseline Characteristics of Study Subjects |
Clinical Characteristics
Table 2 compares the group of patients with sarcopenia with the group without sarcopenia. The pace of the 4 m walking test was measured, and the grip strength of the electronic gripper, as well as the ASM of the extremities, and nutritional indicators, such as Alb, were significantly lower in the group with sarcopenia than in the non-sarcopenia group (P < 0.001). Since females have a significantly lower SMI and grip strength, the patients were separated again according to gender, and the comparison of SMI and grip strength between those with and without sarcopenia was carried out for the different genders. The grip strength and SMI of the sarcopenia group was significantly lower, regardless of gender (P < 0.05). A comparison of the clinical indicators related to COPD shows that FEV1/FVC was lower, and the difference was statistically significant (P < 0.05). There were no statistically significant differences between the two groups in terms of the time of disease and grade of lung function. The expression of pro-inflammatory factor IL-6 and anti-inflammatory factor IL-10 was significantly higher in the serum of COPD patients with sarcopenia than in the non-sarcopenia group, but the IL-10/IL-6 ratio showed no significant difference between the two groups.
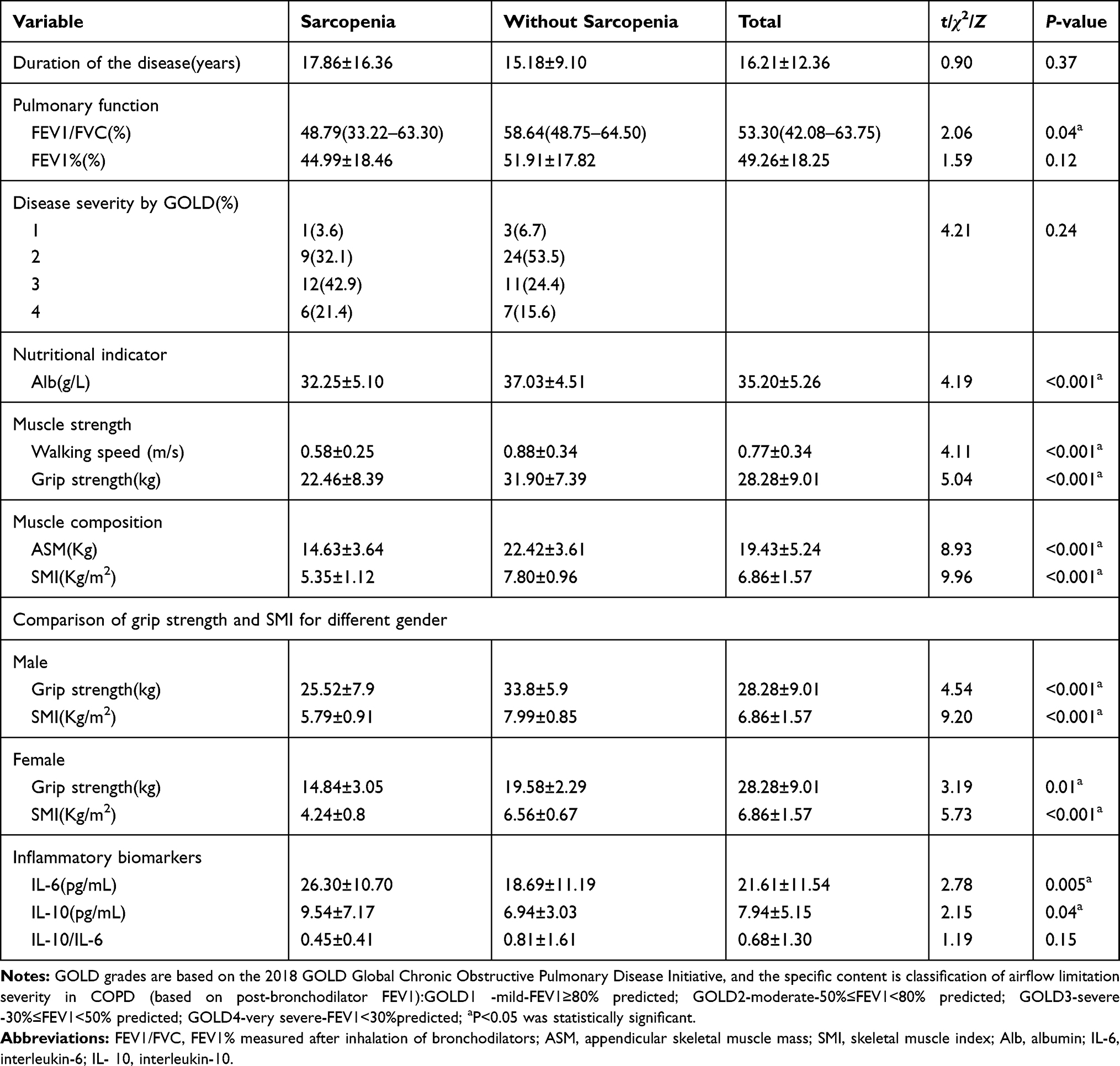 |
Table 2 Clinical Outcomes According to Presence or Absence of Sarcopenia |
The Correlation Between SMI and Inflammation Indicators
To further study the correlation between the different indexes and sarcopenia in Tables 1 and 2, a Pearson correlation test was performed. Tables 3 and 4 shows that the walking pace, grip strength, and SMI have strong positive correlations. Age and IL-10 are significantly negatively correlated with walking pace, handgrip strength, and SMI (P < 0.05). However, IL-6 is only negatively correlated with SMI (P < 0.01), and weakly correlated with grip strength and pace (Figure 1). Pulmonary function indexes (FEV1/FVC, FEV1%), BMI, and serum Alb concentration were positively correlated with walking pace, grip strength, and SMI (P < 0.05). There was also a significant negative correlation between the CAT score and grip strength (P < 0.05), but the correlation between IL-10/IL-6 ratio and SMI was weak. There was no significant correlation between smoking time and walking pace, grip strength, and SMI. In order to exclude the influence of age on serum IL-6 and IL-10, the levels of IL-6 and IL-10 were adjusted for age, and the correlation with SMI was analyzed again. And the conclusion was the same as before (P < 0.05) (Tables 3 and 4).
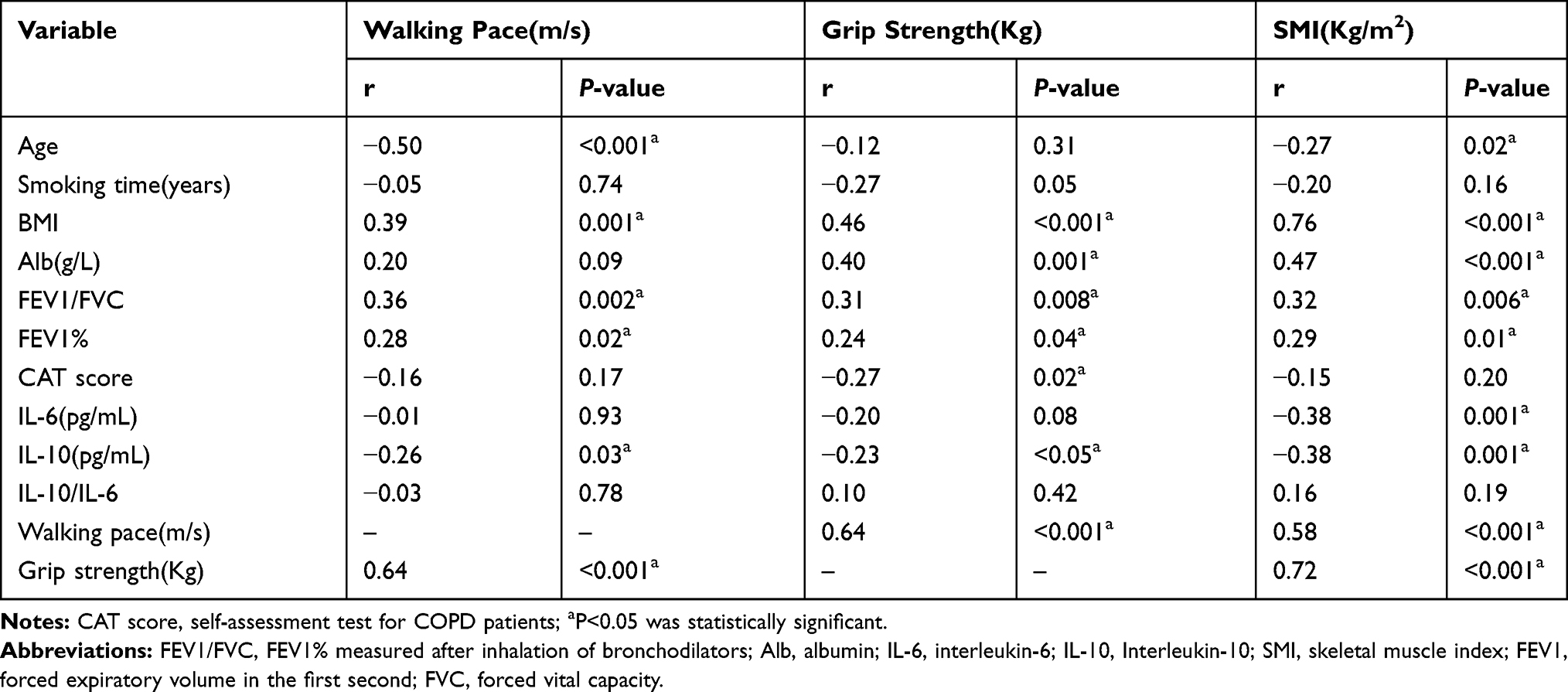 |
Table 3 Correlation Between Sarcopenia Indicators and Inflammatory Mediators |
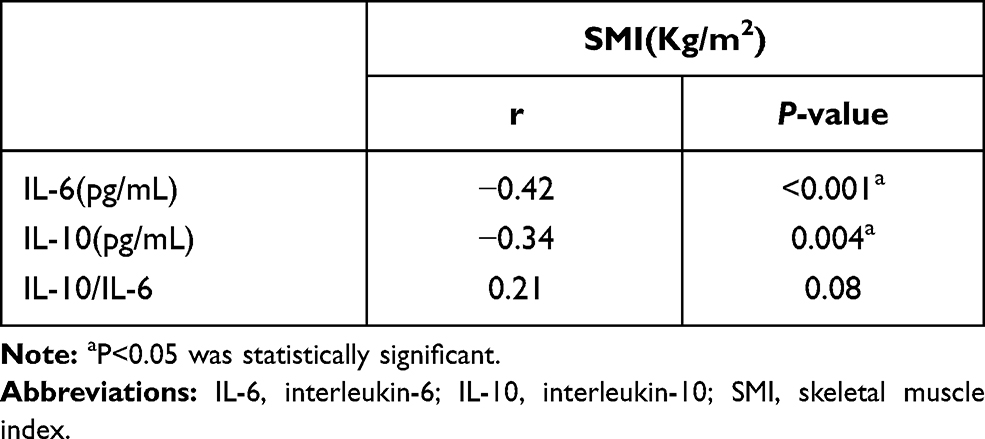 |
Table 4 Correlation Between SMI and Age-Corrected IL-6, IL-10 Levels, IL-10/IL-6 |
Factors Related to Sarcopenia in Patients with COPD
Clinical data including inflammatory factors, clinical characteristics and indicators of patients were collected. The variables that are indistinguishable between the two groups were eliminated as confounding variables, and the indicators with statistical differences between the groups were subjected to multiple linear regression analysis. The number of smokers was not included in the regression analysis because the number of smokers did not match the number of participants in the regression analysis. Finally, SPSS software was used to clarify the stability and goodness of fit of the model. Variables including age, BMI, CAT score, Alb level, FEV1/FVC, IL-6 and IL-10 levels were analyzed in the multivariate unconditional logistic regression analysis. Multivariate unconditional logistic regression analysis showed that age (OR = 1.11, P = 0.02) and IL-6 (OR = 1.07, P < 0.05) were closely associated with the incidence of sarcopenia. In other words, with the increase of age and IL-6, the incidence of sarcopenia increases, while the level of IL-6 has a weaker effect. Meanwhile, BMI (OR = 0.54, P = 0.002) were related to preventing muscle loss (Table 5). In addition, the CAT score and serum Alb content has no significant effect on the incidence of sarcopenia.
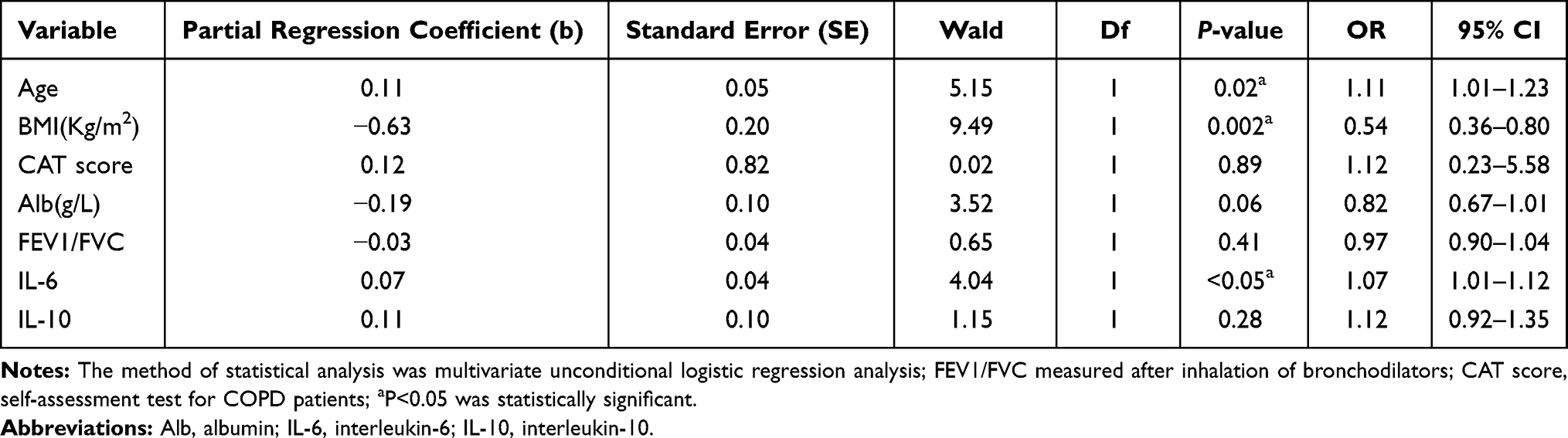 |
Table 5 Analysis of Risk Factors for Sarcopenia |
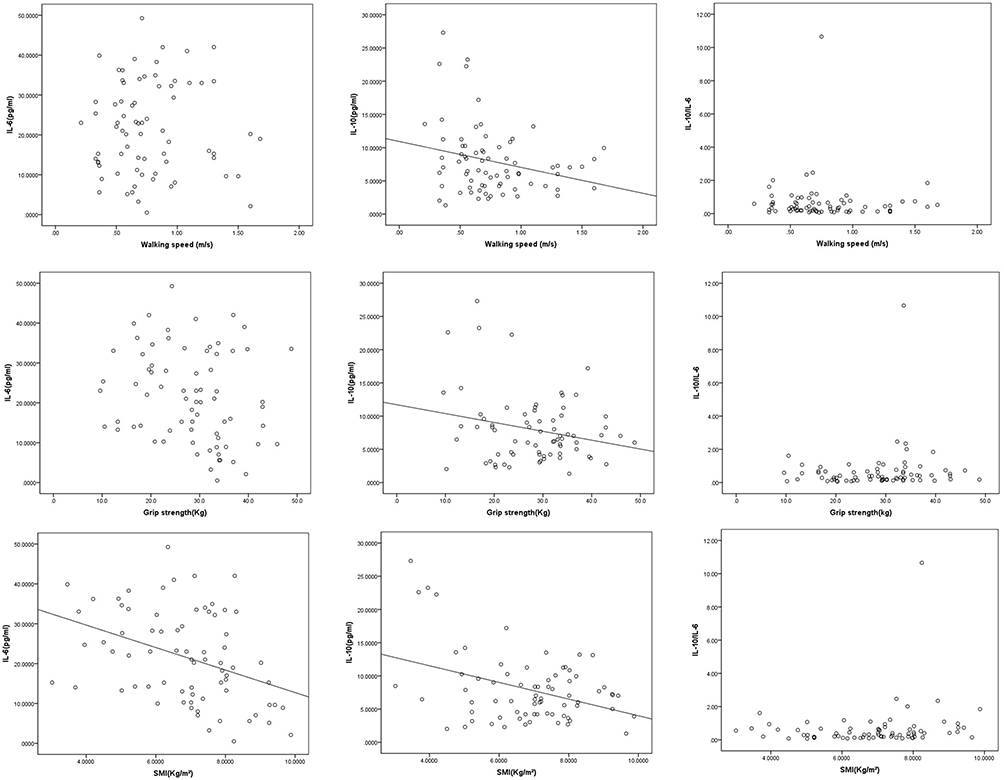 |
Figure 1 Correlation between IL-6, IL-10 content,IL-10/IL-6 ratio and SM. |
Discussion
This study found that COPD patients with sarcopenia have greater circulating levels of IL-6 and IL-10 when compared to those without. IL-6, IL-10, and age have a negative correlation trend with SMI. Pulmonary function indexes FEV1/FVC, FEV1%, BMI, and nutritional index serum Alb are positively correlated with SMI. In addition, the incidence of sarcopenia increases with age and IL-6 levels. On the contrary, increases in BMI is related to a decrease in the incidence of sarcopenia. However, the IL-10/IL-6 ratio is not significantly associated with sarcopenia.
Sarcopenia is a progressive skeletal muscle disorder which involves the accelerated loss of muscle mass and function, and it is clearly associated with increasing age.4 Similarly, age is often listed as a risk factor for COPD.10 In addition to age, gender is also considered to be one of the factors affecting the progression of COPD.10 However, Foreman found that the prevalence of COPD is almost equal in men and women,21 and it has been found that while gender can affect the prevalence of sarcopenia, the gender differences are also influenced by age.22 In this study, patients in the sarcopenia group were significantly older than those in the non-sarcopenia group, but there was no significant difference between the sexes.
At present, it is recognized that the pathogenesis of COPD is related to systemic or local chronic inflammation. Continuous low-grade inflammation affects airway epithelial cell damage and repair.23 IL-6 and IL-10 play an indispensable role in the occurrence and progression of inflammation, and it has been shown that serum IL-6 levels in patients with COPD are higher than in healthy adults.16,24 Muscle reduction in elderly patients with COPD is a common complication. In this study, the proportion of patients with COPD and sarcopenia accounted for 38.36% of the total number of patients, indicating that sarcopenia is very common in patients with COPD, and activity tolerance is reduced due to muscle loss. It is currently believed that chronic low-grade inflammation is closely related to the occurrence of muscle loss,5 and Byun et al25 found that muscle reduction is related to inflammatory mediators, such as tumor necrosis factor-α levels.
The contracting skeletal muscle may synthesize and release IL-6,26 but it is dependent on the intensity and duration of the exercise. In order to increase the concentration of IL-6 in the blood, it is necessary to participate in long-term exercise involving a significant muscle mass in the contractile activity.27 IL-6 increases caused by short-term strenuous exercise will also rapidly decrease.26 However, the patients in this study were all elderly people who were retired, did not participate in high-intensity long-term exercise, and did not perform pulmonary rehabilitation exercise therapy. Therefore, the effect of exercise on IL-6 in the two groups of patients included in the study can be ruled out. In this study, in patients with COPD with sarcopenia, the serum IL-6 concentration was significantly higher than that in normal muscle patients, and it was negatively correlated with the SMI. IL-6 has a two-way effect on skeletal muscle. It is an important muscle cell molecule released during skeletal muscle movement, promoting muscle fiber metabolism and regeneration.28 However, when IL-6 activates cells with a trans-signaling pathway, it has a pro-inflammatory effect,29 which is also involved in the induction of chronic inflammation in patients with COPD. Xia et al30 found that pro-inflammatory factors, such as IL-6, may be involved in promoting skeletal muscle proteolytic activation and insulin resistance, both of which are important factors for muscle atrophy. At the same time, elevated plasma levels of pro-inflammatory factors, such as IL-6, may increase the formation of reactive oxygen species (ROS), which may further promote muscle protein hydrolysis by activating the ubiquitin-proteasome system forkhead box O3a-mediated pathway,31 but the current mechanism is still uncertain. Haddad et al32 found that long-term chronic low levels of IL-6 may induce the down-regulation of ribosomal S6 kinase, signal transducer and activator of transcription proteins, and other myocyte growth factor phosphorylation, thereby affecting myocyte atrophy. The data from this study suggest that the increase of IL-6 has a significant relationship with sarcopenia, but whether IL-6 is the cause of muscle atrophy still needs to be verified.
This study also found that the concentration of IL-10 in patients with COPD and sarcopenia was significantly higher than that in normal patients. Studies have shown that the nuclear factor kappa-light chain enhancer (NF-κB) expression of activated B cells is enhanced in mice knocking out the IL-10 gene,33 while NF-κB binds to the IL-10 promoter and enhances transcription of the IL-10 gene.34 In addition, NF-κB can also induce ubiquitin-proteasome pathway activation,35 which specifically recognizes muscle protein and hydrolyzes it. This is an important pathway for skeletal muscle atrophy and myocyte apoptosis. Katherine36 and other studies have found that increased plasma levels of IL-10 are associated with increased female fat mass and may increase the incidence of metabolic syndrome. In obesity and insulin resistance, growth hormone secretion is reduced, resulting in reduced muscle weight and strength.37 However, IL-10 increases with IL-6 during the inflammation process,38 so it is necessary to use the IL-10/IL-6 ratio to indicate whether IL-10 concentration is associated with sarcopenia alone. This study found no significant correlation between the IL-10/IL-6 ratio and SMI, and multiple logistic regression shows that IL-10 concentration has no relationship with the occurrence of sarcopenia, so the association between IL-10 and sarcopenia needs further study.
One of the main causes of sarcopenia is malnutrition, which can be caused by reduced nutrient intake, increased catabolism, and reduced intestinal absorption. This study found that the BMI and Alb concentrations in patients with COPD and sarcopenia were significantly different from those in the normal muscle group, and is positively correlated with SMI. The decrease of BMI were significantly associated with the progression of sarcopenia. According to Table 5, the relationship between albumin concentration and sarcopenia cannot be shown, the result might be related to the sample size included in the trial. Inflammatory mediators can affect many aspects of nutrient intake and absorption. Martinez et al39 and other studies have found that the secretion of interleukin in the blood of patients with anorexia is significantly increased, indicating that increased interleukin can promote anorexia. Further studies have found that inflammatory factors, such as IL-6, can promote the release of leptin, reduce the intake of patients, inhibit the synthesis of fat cells, increase energy metabolism, and cause muscle atrophy.40 Pro-inflammatory cytokines, such as IL-6, have the effects of reducing protein synthesis and promoting protein hydrolysis,41 thereby affecting muscle synthesis and metabolism and promoting muscle fiber reduction and muscle atrophy. In addition, IL-6 can affect the absorption, decomposition, and metabolism of nutrients by regulating the secretion of hormones such as glucagon, cholecystokinin, and adrenocorticotropic hormone.41 Therefore, IL-6 can also influence sarcopenia by affecting nutrition and metabolism.
Smoking is the most important risk factor for COPD, and some studies have found a link between cigarette smoke and muscle loss. According to Robison et al,11 cigarette smoke can cause calcium ion (Ca2+) reduction in muscle fibers and abnormal Ca2+ signaling through various mechanisms, thereby accelerating myocyte death. Cigarette smoke also promotes the production of ROS, induces the activation of NF-κB, promotes the degradation of muscle proteins by the proteasome, and promotes muscle atrophy.12 Therefore, although the specific mechanism of smoking-induced muscle atrophy is not fully understood, it appears to be one of the risk factors for muscle atrophy. This study found that patients with COPD and sarcopenia had smoked for significantly longer than patients without sarcopenia, but the correlation was not clear. The longer a patient has smoked, the more likely it is that they will have changed the number of cigarettes they smoke a day, as well as the brand and grade of tobacco they smoke. These factors would all have affected the correlation between smoking and muscle atrophy in this experiment. Thus, more data concerning patients’ smoking habits need to be collected so that further clinical research can be carried out.
Conclusion
Sarcopenia is a common complication of COPD. The concentrations of IL-6 in patients with COPD and sarcopenia were significantly higher than those with only COPD, and they were negatively correlated with the skeletal muscle index of the extremities, which is related to an increased incidence of sarcopenia. Therefore, high inflammatory mediator concentrations and chronic persistent inflammation can be strongly linked to sarcopenia. However, since the role of IL-10 in sarcopenia is not yet clear, further studies should be conducted.
Funding
Project supported by the Foundation of Health Commission of Shanxi Province, China (Grant No. 2018100). The Foundation of the Key discipline construction project of Shanxi University of traditional Chinese medicine, China (Grant No.1006Z3).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cruz-Jentoft AJ, Baeyens TP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European working group on sarcopenia in older people. Age Ageing. 2010;39(4):412–423. doi:10.1093/ageing/afq034
2. Landi F, Calvani R, Tosato M, et al. Protein intake and muscle health in old age: from biological plausibility to clinical evidence. Nutrients. 2016;8(5):295. doi:10.3390/nu8050295
3. Bischoff-Ferrari HA, Orav JE, Kanis JA, et al. Comparative performance of current definitions of sarcopenia against the prospective incidence of falls among community-dwelling seniors age 65 and older. Osteoporos Int. 2015;26(12):2793–2802. doi:10.1007/s00198-015-3194-y
4. Cruz-Jentoft AJ, Sayer AA. Sarcopenia. Lancet. 2019;393(10191):2636–2646. doi:10.1016/S0140-6736(19)31138-9
5. Zembron-Lacny A, Dziubek W, Rogowski L, et al. Sarcopenia: monitoring, molecular mechanisms, and physical intervention. Physiol Res. 2014;63(6):683–691. doi:10.33549/physiolres.932692
6. Dalle S, Rossmeislova L, Koppo K. The role of inflammation in age-related sarcopenia. Front Physiol. 2017;8:1045. doi:10.3389/fphys.2017.01045
7. Schaap LA, Pluijm SM, Deeg DJ, Visser M. Inflammatory markers and loss of muscle mass (sarcopenia) and strength. Am J Med. 2006;119(6):526–e9. doi:10.1016/j.amjmed.2005.10.049
8. Frasca D, Blomberg BB. Inflammaging decreases adaptive and innate immune responses in mice and humans. Biogerontology. 2016;17(1):7–19. doi:10.1007/s10522-015-9578-8
9. Custodero C, Mankowski RT, Lee SA, et al. Evidence-based nutritional and pharmacological interventions targeting chronic low-grade inflammation in middle-age and older adults: a systematic review and meta-analysis. Ageing Res Rev. 2018;46:42–59. doi:10.1016/j.arr.2018.05.004
10. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
11. Robison P, Sussan TE, Chen H, et al. Impaired calcium signaling in muscle fibers from intercostal and foot skeletal muscle in a cigarette smoke-induced mouse model of COPD. Muscle Nerve. 2016;56(2):282. doi:10.1002/mus.25466
12. Bin Y, Xiao Y, Huang D, et al. Theophylline inhibits cigarette smoke-induced inflammation in skeletal muscle by upregulating HDAC2 expression and decreasing NF-kappaB activation. Am J Physiol Lung Cell Mol Physiol. 2019;316(1):L197–L205. doi:10.1152/ajplung.00005.2018
13. Girón R, Matesanz C, García-Río F, et al. Nutritional state during COPD exacerbation: clinical and prognostic implications. Ann Nutr Metab. 2009;54(1):52–58. doi:10.1159/000205960
14. Hallin R, Koivisto-Hursti UK, Lindberg E, Janson C. Nutritional status, dietary energy intake and the risk of exacerbations in patients with chronic obstructive pulmonary disease (COPD). Respir Med. 2006;100(3):561–567. doi:10.1016/j.rmed.2005.05.020
15. Smith SH. Using albumin and prealbumin to assess nutritional status. Nursing. 2017;47(4):65–66. doi:10.1097/01.NURSE.0000511805.83334.df
16. Gan WQ, Man SFP, Senthilselvan A, et al. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59(7):574–580. doi:10.1136/thx.2003.019588
17. Natsui K, Tanaka K, Suda M, et al. High-dose glucocorticoid treatment induces rapid loss of trabecular bone mineral density and lean body mass. Osteoporos Int. 2006;17(1):105–108. doi:10.1007/s00198-005-1923-3
18. Bodine SC, Furlow JD. Glucocorticoids and skeletal muscle. Adv Exp Med Biol. 2015;872:145–176. doi:10.1007/978-1-4939-2895-8_7
19. Chen LK, Liu LK, Woo J, et al. Sarcopenia in Asia: consensus report of the Asian working group for sarcopenia. J Am Med Dir Assoc. 2014;15(2):95–101. doi:10.1016/j.jamda.2013.11.025
20. Said EA, Al-Reesi I, Al-Shizawi N, et al. Defining IL-6 levels in healthy individuals: a meta-analysis. J Med Virol. 2021;93(6):3915–3924. doi:10.1002/jmv.26654
21. Foreman MG, Zhang L, Murphy J, et al.; COPDGene Investigators. Early-onset chronic obstructive pulmonary disease is associated with female sex, maternal factors, and African American race in the COPD gene study. Am J Respir Crit Care Med. 2011;184(4):414–420. doi:10.1164/rccm.201011-1928OC
22. Kirchengast S, Huber J. Gender and age differences in lean soft tissue mass and sarcopenia among healthy elderly. Anthropol Anz. 2009;67(2):139–151. doi:10.1127/0003-5548/2009/0018
23. Vitenberga Z, Pilmane M, Babjoniseva A. The evaluation of inflammatory, anti-inflammatory and regulatory factors contributing to the pathogenesis of COPD in airways. Pathol Res Pract. 2019;215(1):97–105. doi:10.1016/j.prp.2018.10.029
24. Lane N, Robins RA, Corne J, et al. Regulation in chronic obstructive pulmonary disease: the role of regulatory T-cells and Th17 cells. Clin Sci. 2010;119(2):75–86. doi:10.1042/CS20100033
25. Byun MK, Cho EN, Chang J, Ahn CM, Kim HJ. Sarcopenia correlates with systemic inflammation in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:669-675. doi:10.2147/COPD.S130790
26. Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiol Rev. 2008;88(4):1379–1406. doi:10.1152/physrev.90100.2007
27. Fischer CP. Interleukin-6 in acute exercise and training: what is the biological relevance? Exerc Immunol Rev. 2006;12:6–33.
28. Serrano AL, Baeza-Raja B, Perdiguero E, Jardí M, Muñoz-Cánoves P. Interleukin-6 is an essential regulator of satellite cell-mediated skeletal muscle hypertrophy. Cell Metab. 2008;7(1):33–44. doi:10.1016/j.cmet.2007.11.011
29. Scheller J, Chalaris A, Schmidt-Arras D, et al. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim Biophys Acta. 2011;1813(5):878–888. doi:10.1016/j.bbamcr.2011.01.034
30. Xia Z, Cholewa J, Zhao Y, et al. Targeting inflammation and downstream protein metabolism in sarcopenia: a brief up-dated description of concurrent exercise and leucine-based multimodal intervention. Front Physiol. 2017;8:434. doi:10.3389/fphys.2017.00434
31. Santilli F, Lapenna D, Barba SL, et al. Oxidative stress-related mechanisms affecting response to aspirin in diabetes mellitus. Free Radic Biol Med. 2015;80:101–110. doi:10.1016/j.freeradbiomed.2014.12.010
32. Haddad F, Zaldivar F, Cooper DM, et al. IL-6-induced skeletal muscle atrophy. J Appl Physiol. 2005;98(3):911–917. doi:10.1152/japplphysiol.01026.2004
33. Rennick D, Davidson N, Berg D. Interleukin-10 gene knock-out mice: a model of chronic inflammation. Clin Immunol Immunopathol. 1995;76(2):174–178. doi:10.1016/S0090-1229(95)90144-2
34. Saraiva M, O’Garra A. The regulation of IL-10 production by immune cells. Nat Rev Immunol. 2010;10(3):170–181. doi:10.1038/nri2711
35. Sandri M. Protein breakdown in muscle wasting: role of autophagy-lysosome and ubiquitin-proteasome. Int J Biochem Cell Biol. 2013;45(10):2121-2129. doi:10.1016/j.biocel.2013.04.023
36. Esposito K, Pontillo A, Giugliano F, et al. Association of low interleukin-10 levels with the metabolic syndrome in obese women. J Clin Endocrinol Metab. 2003;88(3):1055–1058. doi:10.1210/jc.2002-021437
37. Clasen BF, Poulsen MM, Carlos E, et al. Growth hormone signaling in muscle and adipose tissue of obese human subjects: associations with measures of body composition and interaction with resveratrol treatment. J Clin Endocrinol Metab. 2014;99(12):2565–2573. doi:10.1210/jc.2014-2215
38. Silva B, Lira FS, Ramos D, et al. Severity of COPD and its relationship with IL-10. Cytokine. 2018;106:95–100. doi:10.1016/j.cyto.2017.10.018
39. Martinez M, Arnalich F, Hernanz A. Alterations of anorectic cytokine levels from plasma and cerebrospinal fluid in idiopathic senile anorexia. Mech Ageing Dev. 1993;72(2):145–153. doi:10.1016/0047-6374(93)90096-A
40. Morley JE. Anorexia of ageing: a key component in the pathogenesis of both sarcopenia and cachexia. J Cachexia Sarcopenia Muscle. 2017;8(4):523–526. doi:10.1002/jcsm.12192
41. Michaud M, Balardy L, Moulis G, et al. Proinflammatory cytokines, aging, and age-related diseases. J Am Med Dir Assoc. 2013;14(12):877–882. doi:10.1016/j.jamda.2013.05.009
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.