")
Back to Journals » Risk Management and Healthcare Policy » Volume 13
The Association of Subscapular Skinfold with All-Cause, Cardiovascular and Cerebrovascular Mortality
Authors Liu XC , Liu L, Yu YL , Huang JY, Chen CL , Lo K , Huang YQ, Feng YQ
Received 12 May 2020
Accepted for publication 16 July 2020
Published 30 July 2020 Volume 2020:13 Pages 955—963
DOI https://doi.org/10.2147/RMHP.S262300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Xiao-Cong Liu, 1 Lin Liu, 1 Yu-Ling Yu, 1 Jia-Yi Huang, 1 Chao-Lei Chen, 1 Kenneth Lo, 2 Yu-Qing Huang, 1 Ying-Qing Feng 1
1Department of Cardiology, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, School of Medicine, South China University of Technology, Guangzhou 510080, People’s Republic of China; 2Centre for Global Cardiometabolic Health, Department of Epidemiology, Brown University, Providence, RI, USA
Correspondence: Yu-Qing Huang; Ying-Qing Feng
Department of Cardiology, Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, School of Medicine, South China University of Technology, Guangzhou 510080, People’s Republic of China
Tel/ Fax +86-20-83827812
Email [email protected]; [email protected]
Purpose: Previous studies suggested inconsistent relationship between subscapular skinfold and all-cause, cardiovascular, and cerebrovascular mortality. Therefore, the present study aimed to investigate the associations between subscapular skinfold with all-cause, cardiovascular, and cerebrovascular mortality.
Patients and Methods: Data were collected from the National Health and Nutrition Examination Survey (NHANES, 1999– 2006) with follow-up data through 31 December 2015. Participants were categorized by subscapular skinfold quartiles. The hazard ratios (HRs) and 95% confidence intervals (CIs) were evaluated using the multivariate Cox regression model and subgroup analysis. Kaplan–Meier curves were used to present cause-specific mortalities and used Cox cubic regression splines to examine the association of subscapular skinfold with cause-specific mortalities.
Results: A total of 16,402 subjects (49.61% male) were involved in our study. After a mean follow-up of 141.73 months, there were 3078 (18.77%), 392 (2.39%), and 128 (0.78%) cases of all-cause, cardiovascular, and cerebrovascular mortality, respectively. Participants in the highest quartile of subscapular skinfold (≥ 24.80mm) versus the lowest (< 13.20mm) had lower risk for all-cause mortality (HR, 0.71; 95% CI, 0.57– 0.89; P for trend = 0.007) and cardiovascular mortality (HR, 0.44; 95% CI, 0.23– 0.83; P for trend = 0.023) in the fully adjusted model. In the age-stratified analysis, subscapular skinfold was only inversely associated with all-cause and cardiovascular disease mortality in people ≥ 65 years of age (all P-interaction < 0.001). No significant difference was found between subscapular skinfold and cerebrovascular mortality (all P > 0.05).
Conclusion: Subscapular skinfold showed an inverse association with all-cause and cardiovascular disease mortality in people aged ≥ 65 years.
Keywords: all-cause mortality, cardiovascular disease, cerebrovascular disease, NHANES, subscapular skinfold
Introduction
According to the Global Burden of Disease study data, the prevalence of obesity has doubled in more than 70 countries and has continuously increased worldwide since 1980, approximately 107.7 million children and 603.7 million adults with obesity all over the world in 2015.1 Overweight and obesity are established risk factors for multiple chronic diseases, including cardiovascular diseases,2–4 cerebrovascular diseases,5 type 2 diabetes,6 cancer,7 and other disease conditions,8,9 as well as all-cause mortality.10 Body mass index (BMI) is the most common indicator for adiposity in epidemiological research. However, “obesity paradox” has been consistently reported.11–13 One of the essential explanations is that BMI fails to describe body fat distribution as an index of adiposity,14,15 when studies have emphasized that the accumulation of visceral and ectopic fat is an independent risk marker of cardiovascular and metabolic morbidity and mortality.2,3 Moreover, visceral and ectopic fat is usually measured by magnetic resonance imaging (MRI) and computerized tomography (CT) imaging. However, the measurement of visceral and ectopic fat is limited in clinical practice and research studies due to the high operation cost. Therefore, alternative indicators were explored, such as skinfold thickness. Skinfold thickness is a simple-to-use index to examine trunk and overall obesity.16 Some reports suggested that skinfold thickness could be used to measure obesity with the advantage of indicating fat distribution.17,18 An increase in subscapular skinfold was associated with cardiovascular mortality in previous studies,19,20 but few studies have examined its link with all-cause and cerebrovascular mortality. Therefore, the aim of the present study was sought to examine the association of subscapular skinfold thickness with all-cause, cardiovascular, and cerebrovascular disease mortalities in US adults from the National Health and Nutrition Examination Survey (NHANES) 1999–2006.
Patients and Methods
Study Design and Study Population
The NHANES is designed to assess the health and nutritional status of adults and children in the United States. Data for analyses were included from the NHANES 1999–2006 with follow-up data through 31 December 2015. Details of recruitment, procedures, population characteristics, and study design for NHANES are available for online access at https://www.cdc.gov/nchs/nhanes/index.htm. Our study included 16,402 participants who were ≥18 years of age with data of subscapular skinfold thickness, and we excluded subjects who missed mortality data (Figure 1).
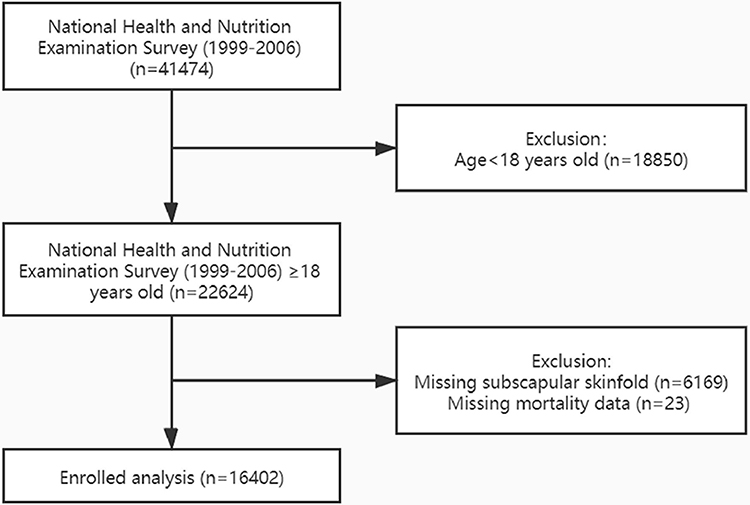 |
Figure 1 The research flow chart. |
Subscapular Skinfold Measurement
Subscapular skinfold was measured in millimeters using the Holtain skinfold caliper by trained personnel at the inferior angle of the right scapula according to NHANES protocols. The protocol stipulates that each skinfold should consist of a double thickness of skin and underlying adipose tissue. The Holtain calipers are designed to provide accurate measurements up to a maximum of 45.0 mm.
Covariates
Weight, height, and blood pressure were measured by trained personnel in a Mobile Examination Center (MEC). BMI was calculated as weight divided by height (kg/m2). Information on age, gender, race (dichotomized into white or non-white), marital status (dichotomized into married or others), education level (dichotomized into less than high school or high school or above), alcohol consumption, smoking (dichotomized into yes or no), and history of cardiovascular diseases (CVD) were self-reported through questionnaire interviews. Prescription medication use was assessed by self-report and verified by interviewers through the examination of medication containers. The biochemistry profile, including total cholesterol (TC, mg/dl), high-density lipoprotein cholesterol (HDL-C, mg/dl), and C-reactive protein (CRP, mg/dl), was collected from laboratory measurements. Estimated glomerular filtration rate (mL/min/1.73 m2) (eGFR) was calculated based on the Modification of Diet in Renal Disease formula (MDRD).21 Hypertension was defined as systolic blood pressures (SBP) ≥140mmHg and/or diastolic blood pressure (DBP) ≥90mmHg, taking antihypertensive medications, or self-reported history of hypertension.22 Diabetes was defined as FBG ≥ 126mg/dl, hemoglobin A1c (HbA1C) ≥6.5%, self-report, or using hypoglycemic agents.23 Full detailed procedures on questionnaires and test methods can be found on the website (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx).
Mortality Data
National Center for Health Statistics has linked mortality data from NHANES to death certificate data in the National Death Index. Mortality data were extracted from the data of the survey participants, based on a probabilistic match between NHANES and the National Death Index records through 31 December 2015. All-cause mortality included deaths from all causes. Cardiovascular (I00-I09, I11, I13, I20-I51) and cerebrovascular (I60-I69) mortality as defined by International Classification of Diseases, 10th Edition, Clinical Modification System codes derived from death-certificate data. Detailed mortality variables can be referred to on the website (https://www.cdc.gov/nchs/data-linkage/mortalitypublic.htm).
Statistical Methods
Subjects were categorized by subscapular skinfold thickness in quartiles (Q1:<13.20mm, Q2:13.20–18.70mm, Q3:18.71–24.79mm, Q4≥24.80mm). Baseline characteristics for the groups of participants were described using frequencies with percentages for categorical variables, and means with standard deviations (SD) for continuous variables. Subgroup difference was examined using chi-square tests, one-way ANOVA, Fisher test, or Kruskal–Wallis H-test whenever appropriate. The Kaplan–Meier curves were used to present the rate of all-cause, cardiovascular, and cerebrovascular mortality. Survival rates by subscapular skinfold thickness were compared using the Log rank test. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox proportional hazards regression models. Several regression models were built. Model I only included subscapular skinfold thickness, Model II was adjusted for age, gender, and BMI. Model III was additionally adjusted for race, education level, married, smoking, alcohol consumption, SBP, eGFR, HDL-C, TC, CRP, comorbidities (hypertension, diabetes, and cardiovascular disease), and medication use (antihypertensive drugs, hypoglycemic agents, antiplatelet drugs, and lipid-lowering drugs). A test of the trend across the quartiles of subscapular skinfold thickness was also performed. Cox cubic spline regression models, adjusted for the same covariates in Model III, were used to examine the potential associations of subscapular skinfold thickness with cause-specific mortalities. Subgroup analyses were conducted by stratifying age (<65 or ≥65 years), gender (male or female), race (white or non-white), and BMI (<25 or ≥25 kg/m2) to investigate potential sources of heterogeneity. Statistical significance was detected by P < 0.05. All analyses were performed with R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
A total of 16,402 participants were involved in the study and 8137 (49.61%) were males. The average age was 45.80 (SD=20.78) years. Table 1 shows the baseline characteristics of all participants. In general, the mean values of subscapular skinfold thickness from the lowest to highest quartiles were 10.05 (SD, 1.95), 15.95 (SD, 1.59), 21.58 (SD, 1.74), and 30.03 (SD, 3.96). There were 3078 (18.77%) participants died during the mean follow-up period of 141.73 (SD, 42.14) months, 392 (2.39%) from cardiovascular diseases, and 128 (0.78%) from cerebrovascular diseases. Significant differences were detected in most variables (all P < 0.01), except for education level, the prevalence of cardiovascular diseases, the use of antiplatelet drug, and cerebrovascular mortality.
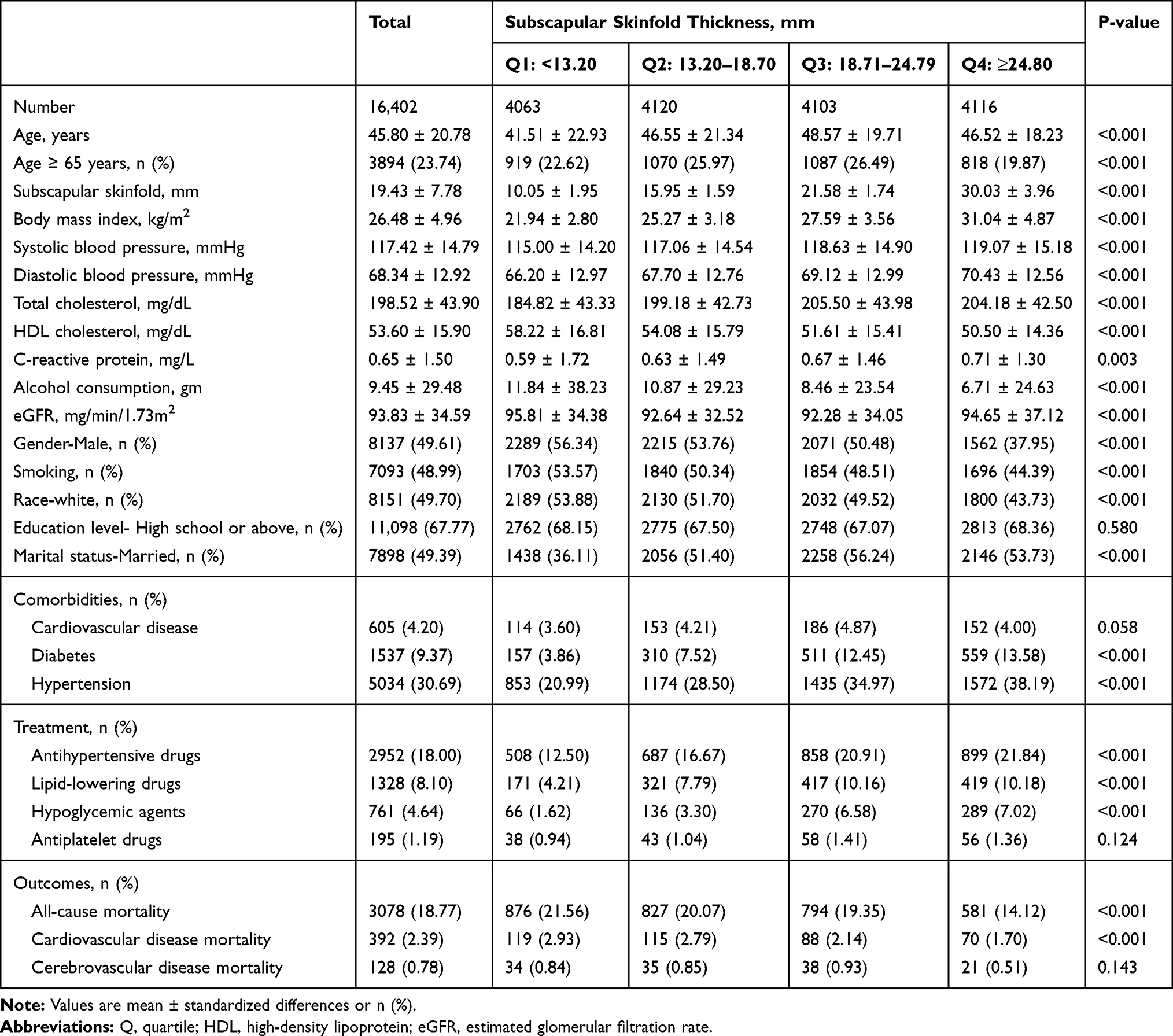 |
Table 1 Baseline Demographic and Clinical Parameters Among Participants by Subscapular Skinfold Quartiles |
The Relationship Between Subscapular Skinfold and All-Cause, Cardiovascular, and Cerebrovascular Diseases Mortality
Multivariable-adjusted Cox Cubic spline regression models showed an inverse association between subscapular skinfold and all-cause and cardiovascular mortality (Figure 2). The association between subscapular skinfold and cerebrovascular mortality showed no statistical significance. As shown in Table 2, when treating subscapular skinfold as a categorical variable, people in the upper (Q4) versus the lowest quartile (Q1) had a reduced risk of all-cause (HR, 0.71; 95% CI, 0.57–0.89; P = 0.002) and cardiovascular mortality (HR, 0.44; 95% CI, 0.23–0.83; P = 0.011) after adjusted for multivariate in Model III. When treating subscapular skinfold as a continuous variable, subscapular skinfold was inversely associated with all-cause (HR, 0.98; 95% CI, 0.97–0.98; P < 0.001) and cardiovascular mortality (HR, 0.97; 95% CI, 0.96–0.98; P < 0.001) in univariate analysis. However, after being adjusted for confounders (Model III), subscapular skinfold inversely associated with all-cause mortality (HR, 0.98; 95% CI, 0.97–0.99; P < 0.001) but showed no significant association with cardiovascular mortality (HR, 0.97; 95% CI, 0.94–1.00; P = 0.083). Kaplan–Meier survival curves, as shown in Figure 3, also demonstrate the significant differences in all-cause mortality and cardiovascular mortality (all P < 0.001). No analyses showed significant associations between subscapular skinfold and cerebrovascular mortality.
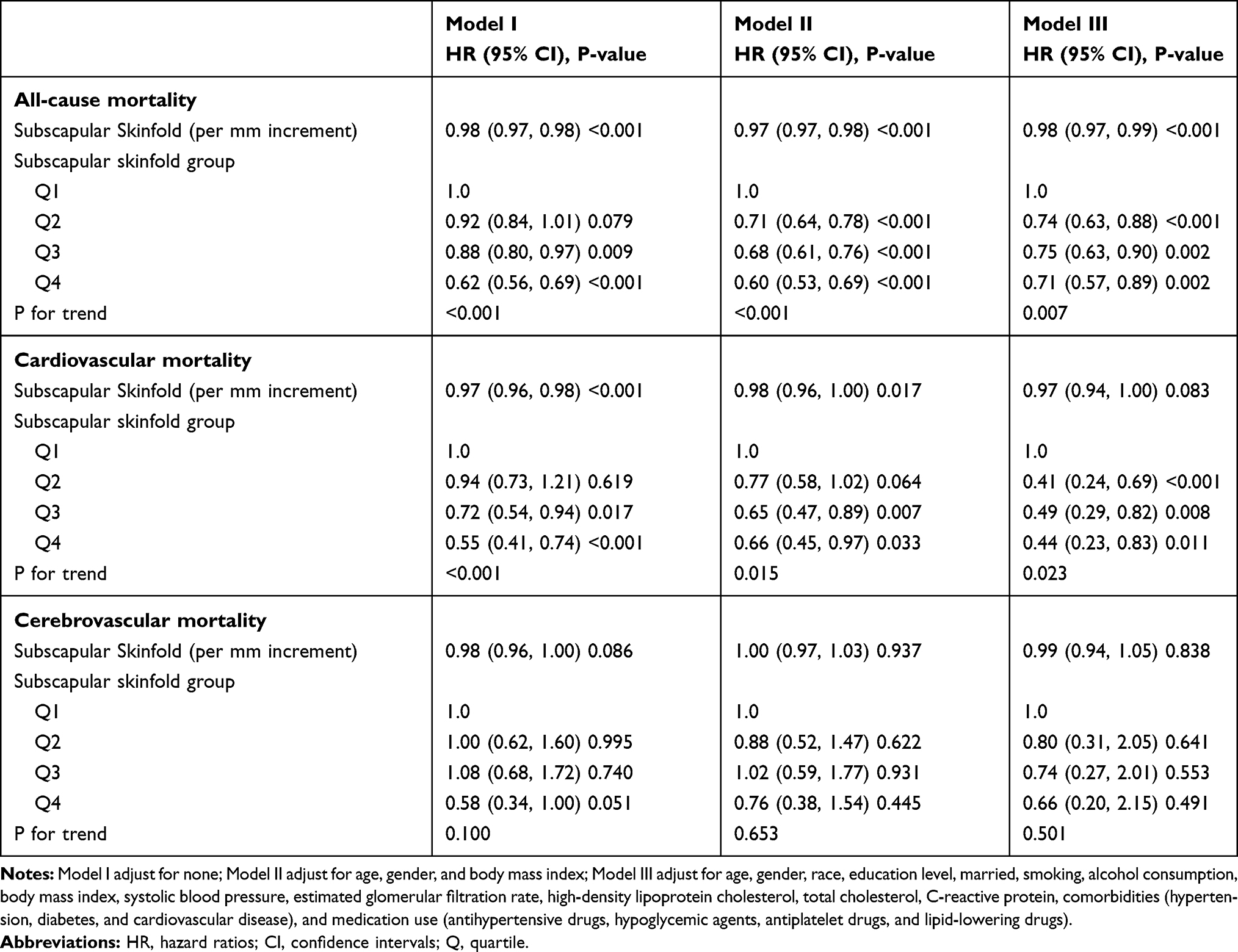 |
Table 2 Multivariate Cox Regression Analysis of Subscapular Skinfold with Cause-Specific Mortality |
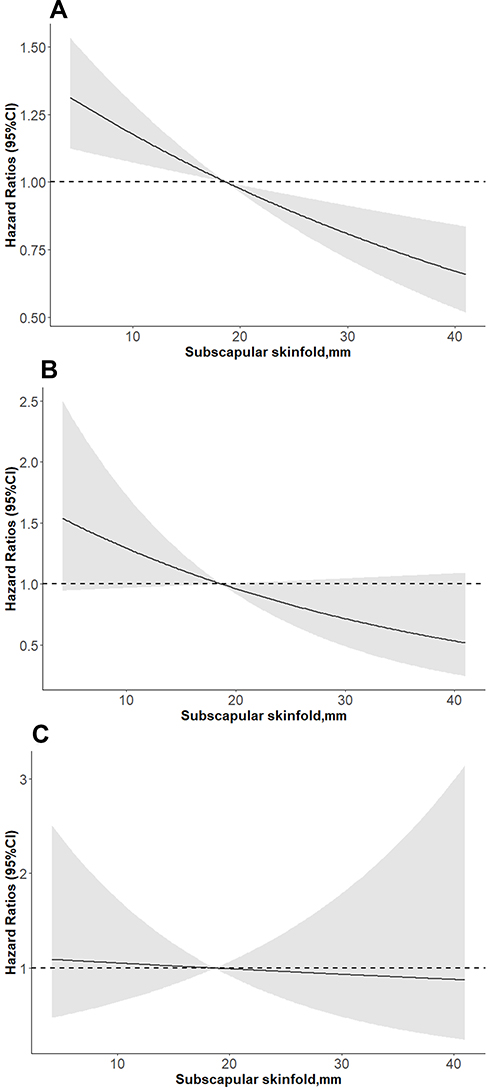 |
Figure 2 Association of subscapular skinfold thickness with all-cause (A), cardiovascular (B), and cerebrovascular (C) mortality using Cox cubic spline regression models. Adjusted for age, gender, race, education level, married, smoking, alcohol consumption, body mass index, systolic blood pressure, estimated glomerular filtration rate, high-density lipoprotein cholesterol, total cholesterol, C-reactive protein, hypertension, diabetes, cardiovascular disease, antihypertensive drugs, hypoglycemic agents, antiplatelet drugs, and lipid-lowering drugs. |
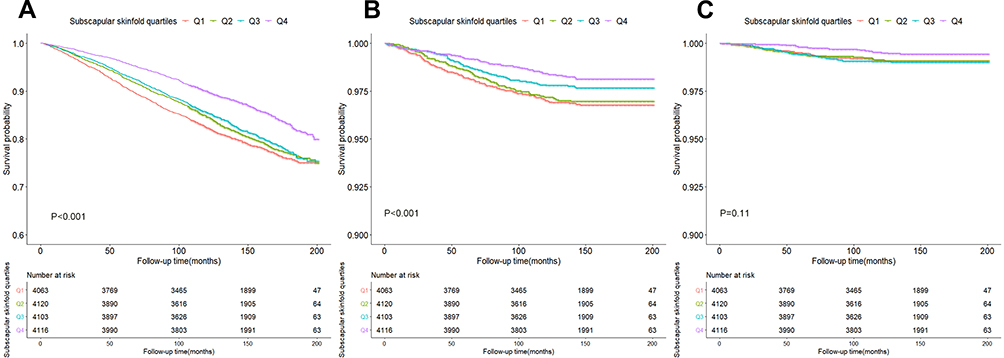 |
Figure 3 Kaplan–Meier survival curves of all-cause (A), cardiovascular (B), and cerebrovascular (C) mortality based on subscapular skinfold quartiles. |
Subgroup Analysis of Subscapular Skinfold with All-Cause, Cardiovascular and Cerebrovascular Mortality
Table 3 shows the subgroup analysis for the association of subscapular skinfold with all-cause and cardiovascular mortality, when being treated as a continuous variable. We found that subscapular skinfold was only associated with all-cause (HR, 0.97; 95% CI, 0.96–0.98, P < 0.001) and cardiovascular mortality (HR, 0.96; 95% CI, 0.92–0.99, P = 0.028) in people ≥65 years (all P-interaction <0.001). No significant difference was found in other subgroup analyses.
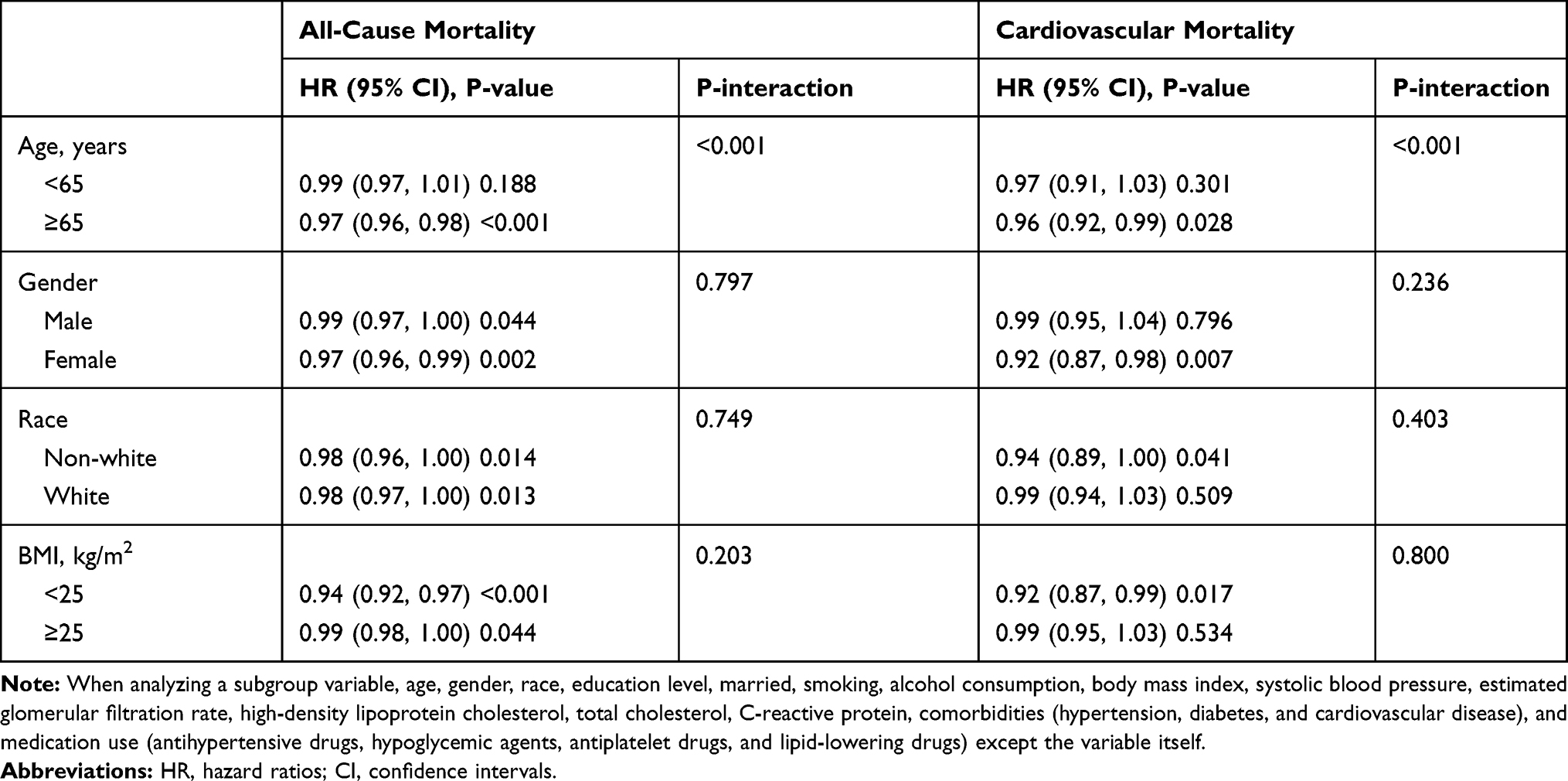 |
Table 3 Subgroup Analysis of Subscapular Skinfold with All-Cause and Cardiovascular Mortality |
Discussion
In the present study, subscapular skinfold was inversely associated with all-cause and cardiovascular mortality in people ≥65 years. No significant relationship had been found between subscapular skinfold and cerebrovascular mortality.
“Obesity paradox” has been widely reported in previous studies when using BMI as an index of adiposity,13 suggesting that people with higher than normal weight have lower all-cause mortality. Epidemiological data suggest that the relationship between obesity and all-cause mortality in the general population follows a U-shaped pattern, and the nadir of the curve was observed at the overweight population.24 Similar findings were reported in studies that used CHD, heart failure, atrial fibrillation, diabetes mellitus, and other disease conditions as outcomes.6,7,11,14,25 This is likely because BMI being an inaccurate indicator of body fatness.15 Skinfold thickness may serve as an alternative but its role in clinical practice and research investigation has not been confirmed.
The results from previous studies concerning the effects of subscapular skinfold are inconsistent. Studies conducted before the 1990s have mostly demonstrated a positive association of subscapular skinfold with all-cause and cardiovascular mortality.16,19,20,26 However, the more recent studies tended to have different findings. Kalmijn’s study in older Japanese-American men showed that higher subscapular skinfold was associated with lower mortality risk and Loh’s study in UK white males revealed no association.27,28 Our study found that subscapular skinfold shows an inverse association with all-cause and cardiovascular mortality, which was independent from BMI. The vast changes in people’s lifestyle and diet structure, as well as the widespread use of statins in recent years, might lead to a transition of the impact of obesity on public health, as the use of established lipid-modifying drugs has indisputably reduced the risk of having an ASCVD event.29 Subscapular skinfold may also reflect the level of subcutaneous fat.30 Therefore, subscapular skinfold may indicate subcutaneous fat storage. Inadequate subcutaneous adipose tissue expansion in face of excess dietary fat leads to visceral and ectopic fat deposition, inflammatory/adipokine dysregulation and insulin resistance.3,4 In contrary, certain subcutaneous fat regions appear to be metabolically, immunologically, and mechanically protective, and acting as a sink to sequester potentially lipotoxic fatty acids.31 Nevertheless, the precise role of subscapular skinfold in body-fat distribution remains to be investigated.
In addition, it is worth noting that subscapular skinfold was only associated with all-cause and cardiovascular mortality in people ≥65 years, which was in accordance with reports from other studies. Chinese Atrial fibrillation registry study found that the “obesity paradox” between high BMI and reduced mortality rate in patients with AF was confined to those with age ≥65 years.25 The Shizuoka Elderly Cohort Study and The Honolulu Heart Program also found that overweight/obesity was inversely associated with mortality in older people, whether defined by BMI or skinfold thickness.27,32 Previous epidemiological studies in the general population have indicated that the relative risk of mortality associated with excess adiposity is lower among older persons.33 It appears that adiposity may have less severe threats on health for older adults than that for young people. Instead, overweight/obesity was associated with lower risk of all-cause mortality in older persons.34 One probable explanation is that people with obesity may have a higher metabolic reserve than lean or normal weight individuals. Obesity might protect against cachexia and energy wasting, with a much more notable effect in older patients with frailty when comorbidities and poor homeostatic reserve are obvious.34 However, obesity and aging are both associated with a higher prevalence of hypertension and other chronic diseases, which may lead to a higher chance of early diagnosis and treatment for severe illnesses. Meanwhile, weight loss will almost certainly have preceded the diagnosis of cancer or be associated with other wasting chronic diseases from which participants may have died, and this would tend to confuse any real association.19 Further studies are needed to establish the precise role of advanced aging in obesity paradox and all-cause mortality.
However, our study has several limitations that should be noted. First, the study population was relatively young, which limited the power to reveal the true association. Second, there were no direct measurements of body fat distribution like MRI or CT that could help us to establish the relationship between subscapular skinfold thickness and adiposity. Third, our study is an observational study; no clear conclusions can be drawn when causality has not been involved. Fourth, we were not able to exclude pregnant and lactating ladies. Fifth, the sample of the general population in the United States may limit the applicability in other regions and ethnic populations.
Conclusions
Subscapular skinfold was inversely associated with all-cause and cardiovascular mortality, and the inverse association only occurred in people ≥65 years. Subscapular skinfold was not significantly associated with cerebrovascular mortality. The association of subscapular skinfold with all-cause and specific mortality is needed more researches to clarify.
Data Sharing Statement
The datasets analyzed during the current study are publicly available at https://www.cdc.gov/nchs/nhanes/index.htm.
Ethics Approval and Informed Consent
The survey protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention (Protocol #98-12, Protocol #2005-06, Continuation of Protocol #2005-06, Protocol #2011-17). Written informed consent was obtained from all subjects.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Collaborators TGO. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377(1):13–27. doi:10.1056/NEJMoa1614362
2. Neeland IJ, Ross R, Després J-P, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715–725. doi:10.1016/S2213-8587(19)30084-1
3. Piche ME, Poirier P, Lemieux I, Despres JP. Overview of epidemiology and contribution of obesity and body fat distribution to cardiovascular disease: an update. Prog Cardiovasc Dis. 2018;61(2):103–113. doi:10.1016/j.pcad.2018.06.004
4. Neeland IJ, Poirier P, Despres JP. Cardiovascular and metabolic heterogeneity of obesity: clinical challenges and implications for management. Circulation. 2018;137(13):1391–1406. doi:10.1161/CIRCULATIONAHA.117.029617
5. Marini S, Merino J, Montgomery BE, et al. Mendelian randomization study of obesity and cerebrovascular disease. Ann Neurol. 2020;87:516–524.
6. Abdullah A, Peeters A, de Courten M, Stoelwinder J. The magnitude of association between overweight and obesity and the risk of diabetes: a meta-analysis of prospective cohort studies. Diabetes Res Clin Pract. 2010;89(3):309–319. doi:10.1016/j.diabres.2010.04.012
7. Lennon H, Sperrin M, Badrick E, Renehan AG. The obesity paradox in cancer: a review. Curr Oncol Rep. 2016;18(9):56. doi:10.1007/s11912-016-0539-4
8. Reeves GK, Balkwill A, Cairns BJ, Green J, Beral V, Million Women Study C. Hospital admissions in relation to body mass index in UK women: a prospective cohort study. BMC Med. 2014;12:45. doi:10.1186/1741-7015-12-45
9. Guh DP, Zhang W, Bansback N, Amarsi Z, Birmingham CL, Anis AH. The incidence of co-morbidities related to obesity and overweight: a systematic review and meta-analysis. BMC Public Health. 2009;9(1). doi:10.1186/1471-2458-9-88
10. Berrington de Gonzalez A, Hartge P, Cerhan JR, et al. Body-mass index and mortality among 1.46 million white adults. N Engl J Med. 2010;363(23):2211–2219. doi:10.1056/NEJMoa1000367
11. Chandramouli C, Tay WT, Bamadhaj NS, et al. Association of obesity with heart failure outcomes in 11 Asian regions: a cohort study. PLoS Med. 2019;16(9):e1002916. doi:10.1371/journal.pmed.1002916
12. Iliodromiti S, Celis-Morales CA, Lyall DM, et al. The impact of confounding on the associations of different adiposity measures with the incidence of cardiovascular disease: a cohort study of 296 535 adults of white European descent. Eur Heart J. 2018;39(17):1514–1520. doi:10.1093/eurheartj/ehy057
13. Elagizi A, Kachur S, Lavie CJ, et al. An overview and update on obesity and the obesity paradox in cardiovascular diseases. Prog Cardiovasc Dis. 2018;61(2):142–150. doi:10.1016/j.pcad.2018.07.003
14. Antonopoulos AS, Oikonomou EK, Antoniades C, Tousoulis D. From the BMI paradox to the obesity paradox: the obesity-mortality association in coronary heart disease. Obes Rev. 2016;17(10):989–1000. doi:10.1111/obr.12440
15. Prentice AM, Jebb SA. Beyond body mass index. Obes Rev. 2001;2(3):141–147. doi:10.1046/j.1467-789x.2001.00031.x
16. Tanne D, Medalie JH, Goldbourt U. Body fat distribution and long-term risk of stroke mortality. Stroke. 2005;36(5):1021–1025. doi:10.1161/01.STR.0000162584.39366.1c
17. Burkhauser RV, Cawley J, Schmeiser MD. The timing of the rise in U.S. obesity varies with measure of fatness. Econ Hum Biol. 2009;7(3):307–318. doi:10.1016/j.ehb.2009.07.006
18. Durnin JV, Womersley J. Body fat assessed from total body density and its estimation from skinfold thickness: measurements on 481 men and women aged from 16 to 72 years. Br J Nutr. 1974;32(1):77–97. doi:10.1079/BJN19740060
19. Kim J, Meade T, Haines A. Skinfold thickness, body mass index, and fatal coronary heart disease: 30 year follow up of the Northwick Park heart study. J Epidemiol Community Health. 2006;60(3):275–279. doi:10.1136/jech.2005.042200
20. Yarnell JWG, Patterson CC, Thomas HF, Sweetnam PM. Central obesity: predictive value of skinfold measurements for subsequent ischaemic heart disease at 14 years follow-up in the Caerphilly Study. Int J Obes. 2001;25(10):1546–1549. doi:10.1038/sj.ijo.0801676
21. Inker LA, Schmid CH, Tighiouart H, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20–29. doi:10.1056/NEJMoa1114248
22. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. doi:10.1001/jama.289.19.2560
23. Chamberlain JJ, Johnson EL, Leal S, Rhinehart AS, Shubrook JH, Peterson L. Cardiovascular disease and risk management: review of the American Diabetes Association Standards of Medical Care in Diabetes 2018. Ann Intern Med. 2018;168(9):640–650. doi:10.7326/M18-0222
24. Flegal KM, Kit BK, Orpana H, Graubard BI. Association of all-cause mortality with overweight and obesity using standard body mass index categories: a systematic review and meta-analysis. JAMA. 2013;309(1):71–82. doi:10.1001/jama.2012.113905
25. Wu S, Yang YM, Zhu J, et al. Impact of age on the association between body mass index and all-cause mortality in patients with atrial fibrillation. J Nutr Health Aging. 2017;21(10):1125–1132. doi:10.1007/s12603-016-0863-2
26. Allison DB, Zhu SK, Plankey M, Faith MS, Heo M. Differential associations of body mass index and adiposity with all-cause mortality among men in the first and second National Health and Nutrition Examination Surveys (NHANES I and NHANES II) follow-up studies. Int J Obes Relat Metab Disord. 2002;26(3):410–416. doi:10.1038/sj.ijo.0801925
27. Kalmijn S, Curb JD, Rodriguez BL, Yano K, Abbott RD. The association of body weight and anthropometry with mortality in elderly men: the Honolulu Heart Program. Int J Obes Relat Metab Disord. 1999;23(4):395–402. doi:10.1038/sj.ijo.0800832
28. Loh WJ, Johnston DG, Oliver N, Godsland IF. Skinfold thickness measurements and mortality in white males during 27.7 years of follow-up. Int J Obes. 2018;42(11):1939–1945. doi:10.1038/s41366-018-0034-0
29. Barter PJ, Rye KA. New era of lipid-lowering drugs. Pharmacol Rev. 2016;68(2):458–475. doi:10.1124/pr.115.012203
30. Ludescher B, Machann J, Eschweiler GW, et al. Correlation of fat distribution in whole body MRI with generally used anthropometric data. Invest Radiol. 2009;44(11):712–719. doi:10.1097/RLI.0b013e3181afbb1e
31. Tchkonia T, Thomou T, Zhu Y, et al. Mechanisms and metabolic implications of regional differences among fat depots. Cell Metab. 2013;17(5):644–656. doi:10.1016/j.cmet.2013.03.008
32. Yamazaki K, Suzuki E, Yorifuji T, et al. Is there an obesity paradox in the Japanese elderly population? A community-based cohort study of 13 280 men and women. Geriatr Gerontol Int. 2017;17(9):1257–1264. doi:10.1111/ggi.12851
33. Stevens J, Cai J, Pamuk ER, Williamson DF, Thun MJ, Wood JL. The effect of age on the association between body-mass index and mortality. N Engl J Med. 1998;338(1):1–7. doi:10.1056/NEJM199801013380101
34. Wang S, Ren J. Obesity paradox in aging: from prevalence to pathophysiology. Prog Cardiovasc Dis. 2018;61(2):182–189. doi:10.1016/j.pcad.2018.07.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.