")
Back to Journals » Psychology Research and Behavior Management » Volume 16
The Association of Experienced Long Working Hours and Depression, Anxiety, and Suicidal Ideation Among Chinese Medical Residents During the COVID-19 Pandemic: A Multi-Center Cross-Sectional Study
Authors Li Z, Liu D , Liu X, Su H, Bai S
Received 15 February 2023
Accepted for publication 14 April 2023
Published 26 April 2023 Volume 2023:16 Pages 1459—1470
DOI https://doi.org/10.2147/PRBM.S408792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zhiyuan Li,1 Dongmei Liu,1 Xiuping Liu,2 Hui Su,3 Song Bai1
1Department of Urology, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China; 2Department of General Surgery, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China; 3Department of Sleep Medical Center, Shengjing Hospital of China Medical University, Shenyang, People’s Republic of China
Correspondence: Song Bai, Department of Urology, Shengjing Hospital of China Medical University, 36 Sanhao Street, Shenyang, Liaoning, 110004, People’s Republic of China, Tel +86-18940255568, Fax +86-024-83955092, Email [email protected]
Background: Long working hours are common among medical residents and may increase the risk of mental disorders. We aimed to investigate the association between experienced long working hours and depression, anxiety, and suicidal ideation among Chinese medical residents during the COVID-19 pandemic.
Methods: This study was conducted in September 2022; 1343 residents from three center in Northeastern China were included in the final analysis (effective response rate: 87.61%). The data were collected from participants via online self-administered questionnaires. Depression and anxiety were measured by the Patient Health Questionnaire (PHQ-9) and the General Anxiety Disorder (GAD-7) scale, respectively. Adjusted odds ratios and 95% confidence intervals were determined after adjusting for potential confounders by binary unconditional logistic regression.
Results: The effective response rate was 87.61%. Among the 1343 participants, 12.88% (173), 9.90% (133), and 9.68% (130) had experienced major depression, major anxiety, and suicidal ideation, respectively. We found that longer weekly worktime increased the risk of major depression, particularly in those who worked for more than 60 hours per week (≥ 61 hours vs ≤ 40 hours, OR=1.87, P for trend = 0.003). However, this trend was not observed for either major anxiety or suicidal ideation (P for trend > 0.05 for both).
Conclusion: This study revealed that there was a considerable incidence of poor mental health among medical residents; furthermore, the longer weekly worktime was associated with a higher risk of major depression, especially for those who worked more than 60 hours per week, but this association was not observed in either major anxiety or suicidal ideation. This may help policymakers to develop targeted interventions.
Keywords: long working hours, mental disorders, medical residents, depression, anxiety, COVID-19
Introduction
Anxiety and depression are common mental disorders.1,2 Anxiety is characterized by chronic and persistent feelings of uncertainty, dread, and fearfulness, while persistent anhedonia (the inability to experience pleasure) is characteristic of major depression.3 Both are global health threats, increasing the risk of mental and physical impairment and drug consumption, leading to suicidal ideation and even excess mortality.4–7 According to the World Health Organization 2016, depression accounts for 10% of the total non-fatal disease burden and is the leading cause of disability worldwide.8 In America, about 10% of the general population experiences depression in their lifetime,9 and the current global incidence of anxiety disorders is 7.3%.10 Since the coronavirus disease 2019 (COVID-19) outbreak, in addition to the physical health, the mental health impacted by the COVID-19 pandemic is also serious. The cases of major depressive disorders and the cases of anxiety disorders globally during the COVID-19 pandemic increased 27.6% and 25.6%.11 The rate of suicidal ideations during COVID-19 pandemic is also higher than prior to pandemic.12 Previous studies have reported that healthcare professionals are at a higher risk of mental illness, including depression and anxiety, than the general population.13–16 Among Chinese physicians, the incidence of depression has been reported as high as 48.28–57.2%.17,18 Poor mental health results in significant psychosocial impairment and even excess mortality among affected physicians5 and leads to low-quality patient care and medical errors.19
Many previous studies have shown that long working hours often affect mental health, contributing to diseases such as depression and anxiety.20,21 Since 2003, the Statement of Justification for the work hour limits issued by the USA Accreditation Council for Graduate Medical Education indicated that the standards for residents’ hours of duty should be less than 80 hours weekly to improve their education and well-being. The European Working Time Directive restricts residents throughout the European Union to 48 hours of work per week.22 Australia does not limit hours but cautions that working more than 50 hours weekly and places the residents who worked over 70 hours at higher risk.23 It varies across different countries and regions. The Labor Law of China clearly states that the legal working hours cannot exceed 44 hours per week. However, there is no study addressing worktime restrictions in Chinese residents; therefore, no reliable recommendations can be made.
In 2014, the State Health and Family Planning Commission in China launched a standardized residency training program to guarantee the quality of medical care as a national strategy. China imposed a “five plus three” model to become a qualified physician (a five-year medical education program in a university plus a three-year standardized training in a hospital for residents).24 This initially established standardized residency training program faces many challenges and needs improvements. China has the largest population globally but a low ratio of doctors to patients.25,26 Moreover, Chinese medical residents usually suffer from overwork, poor doctor-patient relationships, workplace violence, low incomes, and high academic stress,26–29 which may induce excessive work intensity and psychological disorders. Appropriate working hour limits have benefited both physicians’ health and patients’ safety.30–32
Therefore, it is necessary to pay more attention to the mental health of Chinese medical residents. To the best of our knowledge, no study has focused on worktime restriction and their role in reducing the risk of mental disorders, such as depression and anxiety, among Chinese medical residents. Therefore, we aimed to cover this gap through a large multi-center cross-sectional study by adjusting extensive confounding factors.
Methods
Design and Study Population
This cross-sectional survey was done in September 2022. This study was undertaken by the postgraduate administration department. The total number of medical residents from the three centers was 1533. Finally, 1343 (first center 780, second center 307, third center 256) participants responded effectively (effective response rate: 87.61%). Figure 1 is a flowchart depicting the process in detail. Adopted was a set of online anonymous self-administered questionnaires. The average questionnaire took 15 to 20 min. It signifies their voluntary consent to participate. Reminders were sent every 48–72 h through WeChat to increase a high feedback rate.
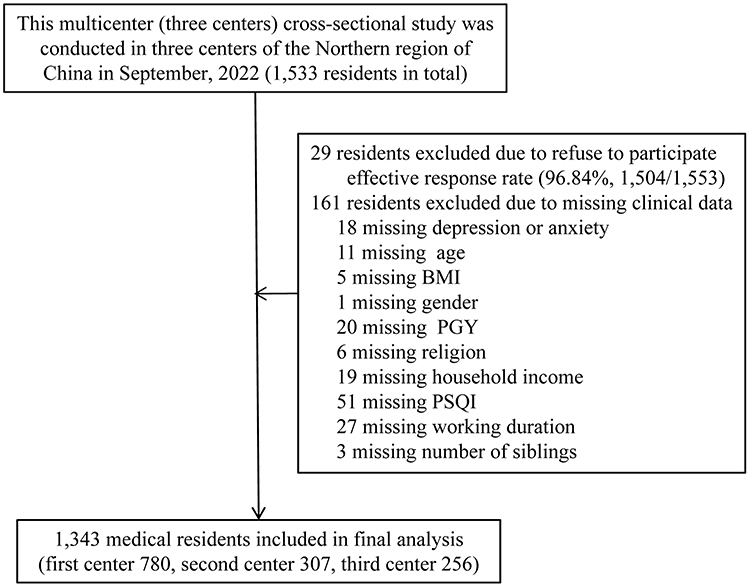 |
Figure 1 Flowchart of this study. Abbreviations: BMI, body mass index; PSQI, Pittsburgh sleep quality index; PGY, post graduation year. |
Ethical Considerations
Institutional Research and Ethics Committee of Shengjing Hospital Affiliated China Medical University granted ethical approval (2022PS993K). All centers adhered to the aforementioned ethical criteria. The informed permission of all eligible participants was acquired. The UIN for the register of clinical research is ChiCTR1900027707. To ensure anonymity and confidentiality, personal details were concealed and only the research team can access the collected data. The study procedure including data collection and storage, adhered to the ethical principles of the Helsinki Declaration of 1975 and followed the STROBE guidelines.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: hospital-employed, professionally active medical residents. The following exclusion criteria were applied: medical residents who had participated in employment for less than three months and who did not submit a comprehensive psychological assessment and clinical data were eliminated.
Measurement of Characteristics
In this study, demographic variables included age, gender, and body mass index (kg/m2). Dietary-habits comprised smoking disorder (current versus never versus former), alcohol consumption, and coffee consumption (current versus never versus former). Sleep quality (PSQI, Pittsburgh sleep quality index scores), physical activity (IPAQ, International Physical Activity Questionnaire, Mets hour/week), religions (yes vs no), marital status (single/divorce/separation/widow vs married/cohabitation), siblings (yes vs no), household income monthly (RMB, yuan) was categorized as, poor (< 5000), good (≧5000, < 10,000), and excellent (≧10,000). Post-graduation year (1st vs 2nd vs 3rd), specialization (surgery vs internal medicine and others vs obstetrics and gynecology vs pediatrics), and night shifts (times/month) are work-related variables. The smoking habit was classified as current smoker (1 cigarette per day for 6 months), past smoker (quit 6 months ago), or never smoker. Alcohol habit and coffee habit are classified as current drinker (1 time per day and within the past six months), former drinker (stopped drinking within the past six months), and never drinker.
The most recent week’s physical activity (PA) was assessed using the International Physical Activity Questionnaire (IPAQ) short form.33 Buysse et al34 created the Pittsburgh sleep quality index (PSQI) to measure sleep quality. There are 18 questions in this self-report on subjective sleep quality during the past four weeks. Significant life events experienced included separation/divorce, death or serious illness of close family members, serious injury/traffic accident, violence, unemployment, natural disasters, death or serious illness of partner, serious conflict with family, medical disputes, and income reduction/debt. Responses (“Yes” or “No”) to questions about a history of diseases (including systemic lupus erythematosus, nasosinusitis, rhinitis, gallbladder stone, polycystic ovary syndrome, Guillain-Barré syndrome, hypothyroidism, hyperthyroidism, rheumatoid arthritis, chronic glomerulonephritis, chronic gastritis (including diabetes, hypertension, and metabolic syndrome).
Measurement of Anxiety Symptoms
Anxiety symptoms were measured with the Chinese version of the GAD07.35 The GAD07 consists of 7 items, and each item is answered on a 4-point Likert-type scale responses ranging from 0 (never) to 3 (always). A higher score means more severe anxiety symptoms. The presence of major anxiety symptoms was defined as a GAD07 standardized score ≧ of 10.36 In this study, Cronbach’s α coefficient was 0.913.
Measurement of Depressive Symptoms
Depressive symptoms were measured by clinically validated scales for PHQ09.37 The PHQ09 scale comprises nine items, and each item includes 4-point Likert-type scale responses that describe the frequency of subjects’ feelings in the past two weeks ranging from 0 to 3. The summed score ranges from 0 to 27, with a higher score indicating more severe depressive symptoms. The presence of major depression was defined as a PHQ09 score ≧ of 10. Suicidal ideation was defined as number nine question score of PH09 (thoughts that you would be better off dead or of hurting yourself in some way) ≧1. The Cronbach’s α coefficient for this study was 0.888 in the present study.
Statistical Analysis
Windows SPSS 22.0 was used to analyze the data (SPSS Inc., Chicago, IL, USA). Median values for continuous variables were given (interquartile range). As a count, categorical variables were reported (percentage). The independent-samples Student’s t-test was applied to compare the means of two continuous normally distributed variables. Two continuous, non-normally distributed variables were compared with the Mann–Whitney U-test. The categorical variable was given as a number (percentage). To compare categorical variables, the chi-squared test and Fisher’s exact test were used.
Based on the distribution of all participants, the hours of weekly worktime were divided into four quartiles (≤ 40 h, 41–50 h, 51–60 h, and ≥ 61 h) and used for further analysis. Using binary unconditional logistic regression analysis, the relationships between quartiles of weekly worktime and mental disorders (major depression, major anxiety, and suicidal thoughts) were investigated. Mental illness was used as the dependent variable, and weekly worktime was employed as the independent variable. The crude OR was calculated using the crude model, with model 1 additionally adjusting for age, gender, and BMI. Model 2 additionally adjusted for baseline variables that were deemed clinically relevant or that had a p-value < 0.10 in the univariate analysis. Adjusted odds ratios and 95% confidence intervals (CI) were determined by binary unconditional logistic regression after adjusting for potential confounders. Using the median value of each quartile as a continuous variable, a linear trend across increasing quartiles was examined. All P values were two-tailed, and a significant difference was determined as P < 0.05.
Results
Baseline Data of Major Depression, Suicidal Ideation, and Major Anxiety of Chinese Medical Residents
Among the 1343 participants enrolled in the final analyses, the median age was 26.00 years, and the BMI was 21.48 kg/m2; most participants were female (68.10%, 915/1343). There were 12.88% (173/1343) of medical residents suffered from major depression, 9.68% (130/1.343) experienced suicidal ideation, and 9.90% (133/1343) suffered from major anxiety. The ratio of participants categorized by weekly worktime (≤ 40 h, 41–50 h, 51–60 h, and ≥ 61 h) was 26.40% (355/1343), 31.4% (422/1343), 26.20% (352/1343), 15.90% (214/1343), see details in Table 1 and Table 2.
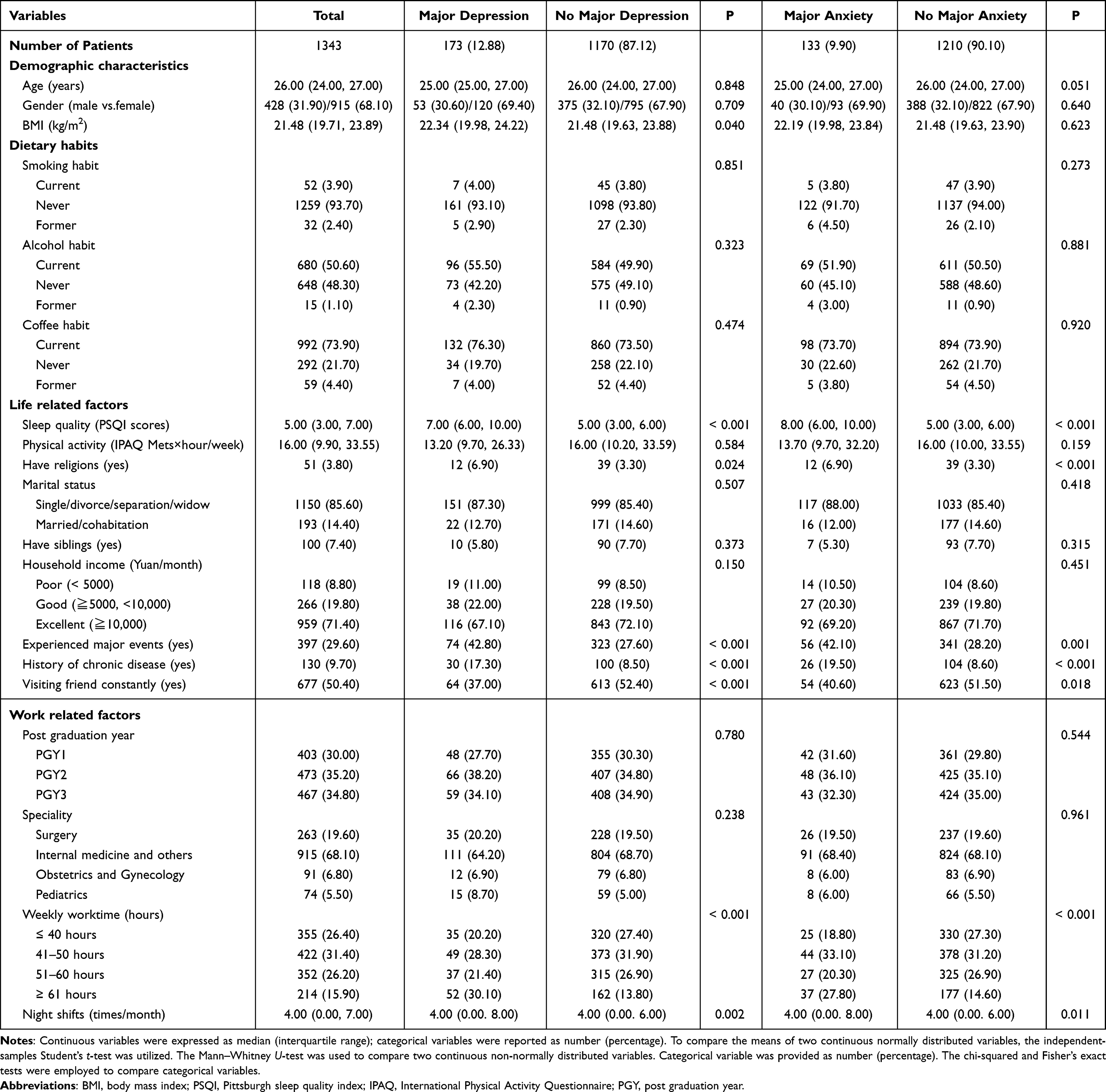 |
Table 1 Univariate Analysis of the Risk Factors for Major Depression and Major Anxiety of Chinese Medical Residents |
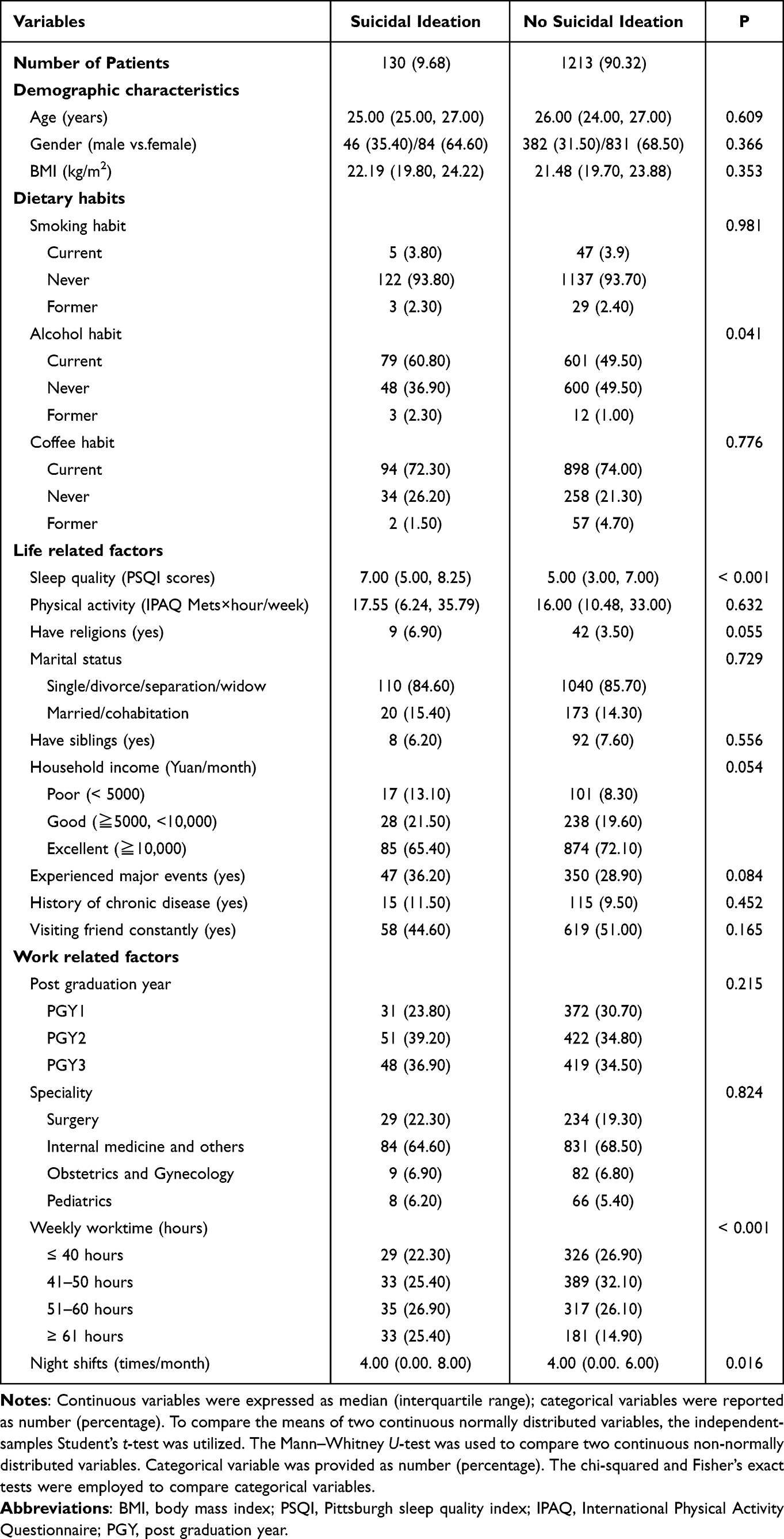 |
Table 2 Univariate Analysis of the Risk Factors for Suicidal Ideation of Chinese Medical Residents |
Univariate Analysis of Major Depression, Suicidal Ideation, and Major Anxiety of Chinese Medical Residents
The medical residents with major depression tended to be a higher BMI, had longer weekly worktime and more frequent night shifts, had poor sleep quality, had a high incidence of religious belief, experienced major events, had a history of chronic disease, and visited friends rarely. The medical residents with major anxiety tended to be younger, had longer weekly worktime and more frequent night shifts, had poor sleep quality, had a high incidence of religious belief, experienced major events, had a history of chronic disease, and visited friends rarely. Participants with suicidal ideation tended to intake more alcohol, have longer weekly worktime and more frequent night shifts, have poor sleep quality, have less household income, and have a high incidence of religious belief and experiencing major events. As shown in Table 1 and Table 2. All the characteristics mentioned above were statistically different in univariate analysis and then were included in multivariate analysis.
Association Between Weekly Worktime and Major Depression, Suicidal Ideation and Major Anxiety of Chinese Medical Residents
Quartiles were categorized across the hours of weekly worktime (≤ 40 h, 41–50 h, 51–60 h, and ≥ 61 h) based on the distribution for all participants and used for multiple logistic regression analysis. After multiple adjustments, we found that the longer weekly worktime, especially for those who worked for more than 60 hours per week (P for trend = 0.03), was associated with a higher risk of experiencing major depression, and the ORs for the extreme quartile was 1.87 (95% CI 1.12–3.14); however, this trend was undetected in suicidal ideation (P for trend > 0.05). Moreover, there was also a negative association between weekly worktime and major anxiety (P for trend > 0.05). As shown in Table 3.
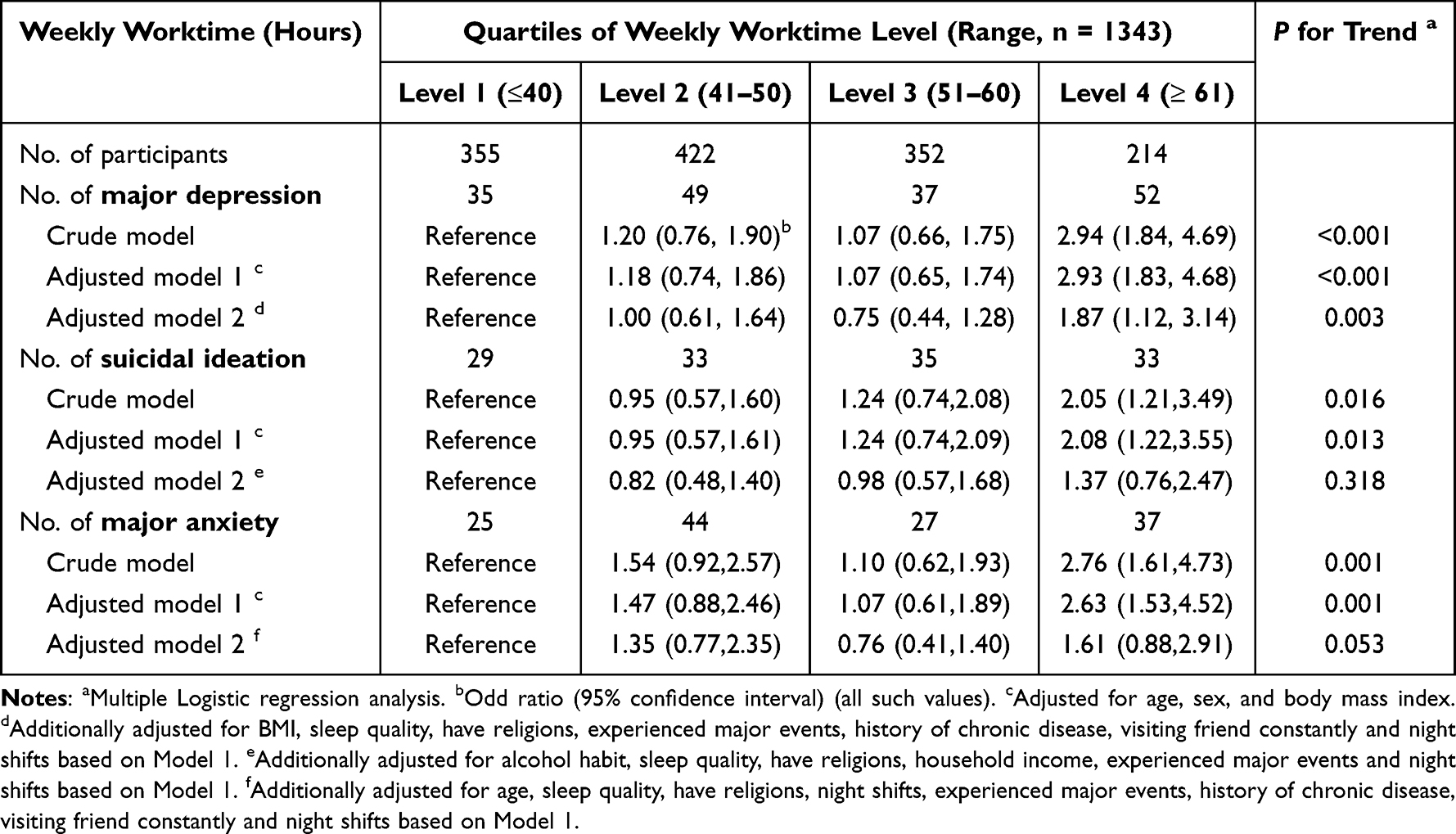 |
Table 3 Association Between Weekly Worktime and Major Depression, Suicidal Ideation and Major Anxiety of Chinese Medical Residents (n = 1343) |
Discussion
In 2014, China established the standardized residency training program for medical residents to guarantee the quality of medical care. However, there was no standard agreement concerning the appropriate worktime duration and its role in reducing the risk of mental disorders among Chinese medical residents. This is the first multi-center study to determine the association between working hours and mental disorders among Chinese medical residents based on a large population in the COVID-19 context. This study revealed that there is a considerable incidence of mental disorders among them and longer weekly worktime is associated with a higher incidence of major depression, particularly in those who work for more than 60 hours per week. However, this association was not observed for either major anxiety or suicidal ideation.
We found that the incidence of major depression among Chinese medical residents was 12.9%. A previous meta-analysis that included 54 observational studies (involving 17,560 individuals and excluding mainland China) estimated that the incidence of depressive symptoms was 28.8% (ranging from 20.9% to 43.2%) among medical residents.14 The discrepancy between the incidence rates identified may be attributed to the variations in the cutoff values of the questionnaires and assessment instruments used. We also found that the incidence of suicidal ideation among Chinese medical residents was 9.72%, which was reported for the first time; this is slightly higher than the incidence among the general population, which has been reported as 9.2% based on cross-national data on 84,850 adults from the WHO World Mental Health Survey.38 The incidence of major anxiety in our study was 9.9%, which was slightly higher than that among the general population. A meta-analysis of 84 observational studies across 44 countries has estimated that the current global incidence of anxiety disorders is around 7.3% (4.8–10.9%).10
Furthermore, this study found that 73.6% of the Chinese medical residents worked more than 40 hours per week, and 15.9% of them even worked more than 60 hours per week during COVID-19, although the Labor Law of China clearly states that working hours should not exceed 44 hours per week. In line with this, a study on the practices of Chinese physicians involving 7762 participants indicated that more than 90% of them worked over 8 hours per day, 13.5% of them worked more than 12 hours per day and more than 80% of respondents had no free weekends.39 Worse still, the COVID-19 pandemic situation has brought a considerable growth on the amount of patients and increased the workload of medical residents. Excessive working hours among medical residents are a common and urgent situation that should be addressed.
We found that longer weekly worktime is associated with a higher risk of major depression, especially among residents working more than 60 hours per week. Similarly, a recent meta-analysis that included 189,729 participants from 35 countries suggested a moderate association between long working hours and depression in Asian people (OR=1.50, 95% CI 1.13–2.01) and a weak positive association in European people (OR=1.11, 95% CI 1.00–1.22).40 Moreover, several previous studies also demonstrated that long working hours increased the risk of depression among medical residents.41–44 In line with this, during the COVID-19 pandemic, a cross-sectional study including 2318 participants of the Longitudinal Study of Adult Health who worked from home, they found that among women, long hours worked were associated with poor self-rated mental health (OR = 1.64; 95% CI = 1.13–2.38).45
However, this association was not observed for either major anxiety or suicidal ideation in our study. A previous prospective study including 2960 British participants found that working long hours is a risk factor for the development of anxiety symptoms in women, but not in men.20 The different definitions of long working hours, study populations, professions, and assessments of anxiety may contribute to such discrepancy. Regarding suicidal ideation, similar to our analysis, a study involving 980 residents from 22 countries did not identify any correlation with long working hours.44
The underlying mechanism remains unclear. Overworking in a deteriorating working environment (eg, uneven distribution of healthcare resources, occasional medical violence, poor doctor-patient relationships26) may cause psychological stress responses, which can induce a constellation of physiological responses. Hyperactivity of the hypothalamic-pituitary-adrenal axis is one of the most common neurobiological changes among those responses, which is closely related to depression.46 In addition, long working hours usually lead to insufficient rest and sleep, even circadian rhythm disorder. The brain areas responsible with modulating the circadian rhythm and sleep may interact with serotonergic neurotransmission,47 which is strongly linked to the pathophysiology of depression.48
There are some limitations to this study: first, the nature of the cross-sectional study design; second, the mental disorders were assessed by online self-administered questionnaires instead of clinical diagnosis; third, the lack of information on the intensity of work, such as case volume. Nevertheless, this is the first large multi-center study to explore the association between long working hours and mental disorders among Chinese medical residents in the COVID-19 context. A prospective study after long-term follow-up is needed to confirm our findings.
Implications to Medical Education
These findings enrich the existing literature on mental health among Chinese medical residents in the COVID-19 pandemic and demonstrate a critical need for establishing a proper worktime restriction, which could improve the mental health of residents.
Conclusion
This study revealed that there was a considerable incidence of poor mental health among medical residents; furthermore, the longer weekly worktime was associated with a higher risk of major depression, especially for those who worked more than 60 hours per week, but this association was not observed in either major anxiety or suicidal ideation. This may help policymakers to develop targeted interventions.
Abbreviations
BMI, body mass index; PSQI, Pittsburgh sleep quality index, IPAQ, International Physical Activity Questionnaire; PGY, Post graduation year.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due [The multicenter datasets are new and afraid of being stolen by others or leaking] but are available from the corresponding author on reasonable request.
Ethical Statement
Ethical approval (No.2022PS993K) was offered by the Ethics Committee of Shengjing hospital Affiliated China Medical University in Shenyang, China. All informed consent of these patients in this study has been obtained.
Consent for Publication
Informed consent from all eligible patients was obtained.
Acknowledgments
We give special thanks to all the colleagues at Shengjing Hospital for their help and support. We thank International Science Editing (http://www.internationalscienceediting.com) for editing this manuscript. The authors would like to thank all of the study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
Zhiyuan Li, Dongmei Liu, Xiuping Liu, Hui Su, and Song Bai declare that they have no competing interests.
References
1. Liu Q, He H, Yang J, Feng X, Zhao F, Lyu J. Changes in the global burden of depression from 1990 to 2017: findings from the Global Burden of Disease study. J Psychiatr Res. 2019;126:134–140. doi:10.1016/j.jpsychires.2019.08.002
2. Stein MB, Sareen J. Generalized anxiety disorder. N Engl J Med. 2015;373:2059–2068. doi:10.1056/NEJMcp1502514
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
4. Cuijpers P, Vogelzangs N, Twisk J, Kleiboer A, Li J, Penninx BW. Differential mortality rates in major and subthreshold depression: meta-analysis of studies that measured both. Br J Psychiatry. 2013;202(1):22–27. doi:10.1192/bjp.bp.112.112169
5. Lasserre AM, Marti-Soler H, Strippoli MP, et al. Clinical and course characteristics of depression and all-cause mortality: a prospective population-based study. J Affect Disord. 2016;189:17–24. doi:10.1016/j.jad.2015.09.010
6. Sareen J, Jacobi F, Cox BJ, Belik SL, Clara I, Stein MB. Disability and poor quality of life associated with comorbid anxiety disorders and physical conditions. Arch Intern Med. 2006;166:2109–2116. doi:10.1001/archinte.166.19.2109
7. Robinson J, Sareen J, Cox BJ, Bolton JM. Role of self-medication in the development of comorbid anxiety and substance use disorders: a longitudinal investigation. Arch Gen Psychiatry. 2011;68:800–807. doi:10.1001/archgenpsychiatry.2011.75
8. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. PMID: 30496104; PMCID: PMC6227754. doi:10.1016/S0140-6736(18)32279-7
9. Kessler RC, Berglund P, Demler O, et al.; NationalComorbidity Survey, R. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication(NCS-R). JAMA. 2003;289(23):3095–3105. doi:10.1001/jama.289.23.3095
10. Baxter AJ, Scott KM, Vos T, Whiteford HA. Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychol Med. 2013;43(5):897–910. PMID: 22781489. doi:10.1017/S003329171200147X
11. COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. DOI:10.1016/S0140-6736(21)02143-7
12. Farooq S, Tunmore J, Wajid Ali M, et al. Suicide, self-harm and suicidal ideation during COVID-19: a systematic review. Psychiatry Res. 2021;306:114228. doi:10.1016/j.psychres.2021.114228
13. Harvey SB, Epstein RM, Glozier N, et al. Mental illness and suicide among physicians. Lancet. 2021;398(10303):920–930. doi:10.1016/S0140-6736(21)01596-8
14. Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: a systematic review and meta-analysis. JAMA. 2015;314(22):2373–2383. PMID: 26647259; PMCID: PMC4866499. doi:10.1001/jama.2015.15845
15. Grande RAN, Berdida DJE, Paulino RRJC, Anies EA, Ebol RRT, Molina RR. The multidimensionality of anxiety among nursing students during COVID-19 pandemic: a cross-sectional study. Nurs Forum. 2022;57(2):267–276. PMID: 34811767; PMCID: PMC9011543. doi:10.1111/nuf.12675
16. Berdida DJE, Grande RAN. Academic stress, COVID-19 anxiety, and quality of life among nursing students: the mediating role of resilience. Int Nurs Rev. 2023;70(1):34–42. PMID: 35639606; PMCID: PMC9347892. doi:10.1111/inr.12774
17. Chang Q, Xia Y, Bai S, et al. Association between Pittsburgh sleep quality index and depressive symptoms in Chinese resident physicians. Front Psychiatry. 2021;12:564815. doi:10.3389/fpsyt.2021.564815
18. Fang H, Zhao X, Yang H, et al. Depressive symptoms and workplace-violence-related risk factors among otorhinolaryngology nurses and physicians in Northern China: a cross-sectional study. BMJ Open. 2018;8:e019514. doi:10.1136/bmjopen-2017-019514
19. West CP, Huschka MM, Novotny PJ, et al. of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296(9):1071–1078. doi:10.1001/jama.296.9.1071
20. Virtanen M, Ferrie JE, Singh-Manoux A, et al. Long working hours and symptoms of anxiety and depression: a 5-year follow-up of the Whitehall II study. Psychol Med. 2011;41(12):2485–2494. PMID: 21329557; PMCID: PMC3095591. doi:10.1017/S0033291711000171
21. Bannai A, Tamakoshi A. The association between long working hours and health: a systematic review of epidemiological evidence. Scand J Work Environ Health. 2014;40(1):5–18. PMID: 24100465. doi:10.5271/sjweh.3388
22. Axelrod L, Shah DJ, Jena AB. The European Working Time Directive: an uncontrolled experiment in medical care and education. JAMA. 2013;309(5):447–448. doi:10.1001/jama.2012.148065
23. Pattani R, Wu PE, Dhalla IA. Resident duty hours in Canada: past, present and future. CMAJ. 2014;186(10):761–765. doi:10.1503/cmaj.131053
24. National Health and Family Planning Commission, State Commission Office for Public Sector Reform (SCOPSR), National Development and Reform Commission, Ministry of Education, Ministry of Finance, Ministry of Human Resources and Social Security, State Administration of Traditional Chinese Medicine. Guiding opinions on establishing the standardised residency training system; 2013. Available from: http://www.moh.gov.cn/qjjys/s3593/201401/032c8cdf2eb64a369cca4f9b76e8b059.shtml.
25. Crisp N, Chen L. Global supply of health professionals. N Engl J Med. 2014;370:950–957. doi:10.1056/NEJMra1111610
26. Wu LX, Qi L, Li Y. Challenges faced by young Chinese doctors. Lancet. 2016;387(10028):1617. PMID: 27116071. doi:10.1016/S0140-6736(16)30202-1
27. Chen S, Pan Y, Yao Q, et al. Publication pressure on Chinese doctors--another view. Lancet. 2014;384:956. doi:10.1016/S0140-6736(14)61630-5
28. Shan HP, Yang XH, Zhan XL, et al. Overwork is a silent killer of Chinese doctors: a review of Karoshi in China 2013–2015. Public Health. 2017;147:98–100. doi:10.1016/j.puhe.2017.02.014
29. Ma Q. An analysis of the causes of frequent cases of violent injuries. Natl Med J China. 2014;94:1368–1370.
30. Weaver MD, Landrigan CP, Sullivan JP, et al. The association between resident physician work-hour regulations and physician safety and health. Am J Med. 2020;133(7):e343–e354. PMID: 32061733; PMCID: PMC7469904. doi:10.1016/j.amjmed.2019.12.053
31. Volpp KG, Rosen AK, Rosenbaum PR, et al. Mortality among hospitalized Medicare beneficiaries in the first 2 years following ACGME resident duty hour reform. JAMA. 2007;298(9):975–983. PMID: 17785642. doi:10.1001/jama.298.9.975
32. Poulose BK, Ray WA, Arbogast PG, et al. Resident work hour limits and patient safety. Ann Surg. 2005;241(6):847–56;discussion 856–60. PMID: 15912034; PMCID: PMC1357165. doi:10.1097/01.sla.0000164075.18748.38
33. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
34. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
35. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
36. Fu Y, Schwebel DC, Hu G. Physicians’ Workloads in China: 1998–2016. Int J Environ Res Public Health. 2018;15:1649. doi:10.3390/ijerph15081649
37. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
38. Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192:98–105. doi:10.1192/bjp.bp.107.040113
39. Cao Y. Doctors’ Karoshi into the pain of industry. China Hosp CEO. 2015;2:52e4. in Chinese.
40. Virtanen M, Jokela M, Madsen IE, et al. Long working hours and depressive symptoms: systematic review and meta-analysis of published studies and unpublished individual participant data. Scand J Work Environ Health. 2018;44(3):239–250. PMID: 29423526. doi:10.5271/sjweh.3712
41. Ogawa R, Seo E, Maeno T, Ito M, Sanuki M, Maeno T. The relationship between long working hours and depression among first-year residents in Japan. BMC Med Educ. 2018;18(1):50. PMID: 29587738; PMCID: PMC5870810. doi:10.1186/s12909-018-1171-9
42. Pereira-Lima K, Gupta RR, Guille C, Sen S. Residency program factors associated with depressive symptoms in internal medicine interns: a prospective cohort study. Acad Med. 2019;94(6):869–875. PMID: 30570500; PMCID: PMC6538448. doi:10.1097/ACM.0000000000002567
43. Nair N, Ng CG, Sulaiman AH. Depressive symptoms in residents of a tertiary training hospital in Malaysia: the prevalence and associated factors. Asian J Psychiatr. 2021;56:102548. PMID: 33454562. doi:10.1016/j.ajp.2021.102548
44. Jovanović N, Beezhold J, Tateno M, et al. Depression and suicidality among psychiatric residents - results from a multi-country study. J Affect Disord. 2019;249:192–198. PMID: 30772747. doi:10.1016/j.jad.2019.02.023
45. Griep RH, Almeida MDCC, Barreto SM, et al. Working from home, work-time control and mental health: results from the Brazilian longitudinal study of adult health (ELSA-Brasil). Front Psychol. 2022;13:993317. PMID: 36262442; PMCID: PMC9574257. doi:10.3389/fpsyg.2022.993317
46. Pariante CM, Lightman SL. The HPA axis in major depression: classical theories and new developments. Trends Neurosci. 2008;31(9):464–468. doi:10.1016/j.tins.2008.06.006
47. Ursin R. Serotonin and sleep. Sleep Med Rev. 2002;6:55–69. doi:10.1053/smrv.2001.0174
48. Mahar I, Bambico FR, Mechawar N, Nobrega JN. Stress, serotonin, and hippocampal neurogenesis in relation to depression and antidepressant effects. Neurosci Biobehav Rev. 2014;38:173–192. doi:10.1016/j.neubiorev.2013.11.009
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.