")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
The Association of Circulating Selenium Concentrations with Diabetes Mellitus
Authors Liao XL, Wang ZH, Liang XN, Liang J, Wei XB, Wang SH, Guo WX
Received 26 September 2020
Accepted for publication 4 November 2020
Published 3 December 2020 Volume 2020:13 Pages 4755—4761
DOI https://doi.org/10.2147/DMSO.S284120
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Xiao-Long Liao, Zhong-Hua Wang, Xiu-Na Liang, Jun Liang, Xue-Biao Wei, Shou-Hong Wang, Wei-Xin Guo
Department of Critical Care Medicine, Guangdong Provincial Geriatrics Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou 510080, People’s Republic of China
Correspondence: Shou-Hong Wang; Wei-Xin Guo
Department of Critical Care Medicine, Guangdong Provincial Geriatrics Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, 106 Zhongshan Road 2, Guangzhou 510080, People’s Republic of China
Tel/Fax +86-20-83827812
Email [email protected]; [email protected]
Purpose: The relationship between circulating selenium and diabetes mellitus (DM) remains inconsistent. Therefore, the relationship between circulating selenium and DM was investigated in the present study.
Patients and Methods: All participants (aged ≥ 18 years) were included from the National Health and Nutrition Examination Survey (NHANES) 1999– 2006. Selenium concentrations from the fasting serum samples were determined using inductively coupled mass spectrometry, then grouped into quartiles. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated by using multivariate logistic regression analysis and the results were stratified by age and sex.
Results: A total of 2,903 (61.9± 13.7 years old) participants (49.3% males) were enrolled, and 580 (19.97%) of them had DM. The mean levels of selenium were 136.4± 19.6 μg/L. Patients with DM (138.76± 20.02 vs 135.88± 19.44, P=0.002) had higher selenium levels compared to those without DM. The OR for DM was 1.12 (95% CI=1.01– 1.24; P=0.0270) for each 10 μg/L increment in selenium, and subjects in the highest quartile of selenium levels (> 147.00 uμg/L) had 2.82 (95% CI=1.55– 5.11; P=0.0007) times higher risk of DM compared to the lowest quartile of selenium levels. Subgroup analysis showed that selenium was independently associated with DM only in female aged < 65 years.
Conclusion: Circulating selenium levels were positively associated with the odds of DM, but difference in sex and age.
Keywords: diabetes mellitus, selenium, relationship
Introduction
Diabetes mellitus (DM) has become a public burden worldwide.1 To elucidate the pathogenesis of DM, some previous studies have suggested the roles of trace elements.2–6 Selenium serves as the redox center for the form of selenoproteins, and is an essential trace element in the human and animal’s diet.7,8 The roles of selenium in the maintenance of human health has attracted attention from researchers.9–12 Selenium forms part of the active site of peroxide-destroying enzyme glutathione peroxidase, and involves antioxidant decency, biotransformation, inflammatory progress, detoxification, and immune response.13,14 Epidemiological, experimental and clinical studies have provided evidence for the roles of selenium in coronary heart disease,15 hypertension,16 metabolic syndrome,17 and dyslipidemia prevention.18 In addition, selenium was significantly associated with disease prognosis,19,20 and the use of high-dose selenium might be associated with a reduced risk of 28-day mortality in critically ill patients.21 However, a systematic review of randomized controlled trials showed no evidence to support Se supplementation in treating people with diabetes.22
Many previous studies have shown that circulating selenium may play an important role in the pathogenesis of abnormal glucose metabolism.23,24 Although a large number of studies have analyzed the relationship between selenium and diabetes, findings are highly controversial, and only few studies have analyzed the age or sex-specific relationship between selenium and DM. Therefore, the purpose of this study is to analyze the association of circulating selenium level with DM, and further explore their relationship through sex and age subgroups.
Patients and Methods
Study Population
Data was extracted from the 1999–2006 National Health and Nutrition Examination Survey (NHANES, n=41,474). The NHANES study was designed to provide a representative sample of non-institutionalized civilian population and assess the health and nutritional status of adults and children in the United States.25,26 Subjects who was missing selenium data (n=19,721) and aged <18 years (n=18,850) were excluded. Participants from NHANES aged ≥18 years and with data on circulating selenium were included in the present analysis (n=2,903). The survey protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention (protocol #98-12 and protocol #2005-2006). Written informed consent was obtained from all participants.
Date Collection and Definition
All participants have provided information on demographics, data on physical examination, and disease history. Total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), fasting blood glucose (FBG), and C-reactive protein were determined according to standardized method. Serum TG and TC were measured enzymatically, while HDL-C was measured by direct immunoassay or precipitation. LDL-C was calculated by Friedewald formula if TG ≤400 mg/dL.27 Body mass index (BMI) was defined as mass (kg) divided by the square of height (m2).28 HbA1c levels were measured using HPLC (Bio-Rad DIAMAT glycosylated hemoglobin analyzer system).29 Diabetes (FBG ≥126 mg/dL or self-report or taking hypoglycemic drugs or HbA1C ≥ 6.5%)30 and hypertension (blood pressure ≥140/90 mmHg or self-report)31 were identified from laboratory analysis or self-reported status.
Measurement of Selenium
The laboratory method for detecting circulating selenium in NHANES was described in detail previously.32 Selenium concentrations were determined using inductively coupled mass spectrometry from the morning fasting serum sample. In brief, circulating selenium was measured at the Trace Elements Laboratory at the Wadsworth Center of the New York State Department of Health (Albany, NY, USA) using inductively coupled plasma–dynamic reaction cell–mass spectrometry, a multi-element analytical technique capable of trace level elemental analysis.
Statistical Analysis
All continuous variables were presented as mean±standard deviation, and categorical variables were presented in frequency or as a percentage according to baseline levels of circulating selenium in quartiles. The One-Way ANOVA, Kruskal Wallis H-test and chi-square tests were used to determine any statistical differences between subgroups. Circulating selenium levels were grouped by quartiles (Q1: <124.00 µg/L; Q2: 124.00–134.90 µg/L; Q3: 135.00–146.90 µg/L; and Q4 > 147.00 µg/L). Odds ratios (ORs) and 95% confidence intervals (CIs) for DM were estimated by multivariate logistic regression analysis with the lowest quartile as the reference. A logistic regression model was used to evaluate association between selenium and DM. Age, sex, BMI, SBP, TC, TG, LDL-C, CRP, smoking, race, and hypertension were adjusted in regression models. Results of the logistic regression model were also stratified by sex and age. A 2-sided P<0.05 was considered as statistically significant. All statistical analyses were performed using R version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline Characteristics
A total of 2,903 subjects (mean age=61.94 years, 49.29% male) were divided into two groups according to diabetes status at baseline. The mean selenium levels of the study population were 136.43±19.60 µg/L. The baseline features of the study population are shown in Table 1. In brief, DM patients have higher selenium levels (138.76±20.02 vs 135.88±19.44; P=0.002) compared to those without DM. When stratifying the clinical characteristics by selenium levels in quartiles in Table 2, the mean HbA1C (5.67±0.81 vs 5.76±0.93 vs 5.80±1.00 vs 6.00±1.40; P<0.001) and the prevalence of DM (17.27% vs 18.24% vs 19.41% vs 25.41%; P<0.001) were gradually increased in parallel with the quartiles of selenium. There were significant differences in BMI, FBG, TG, TC, LDL-C, CRP, sex, and smoking among the quartiles (all P<0.005).
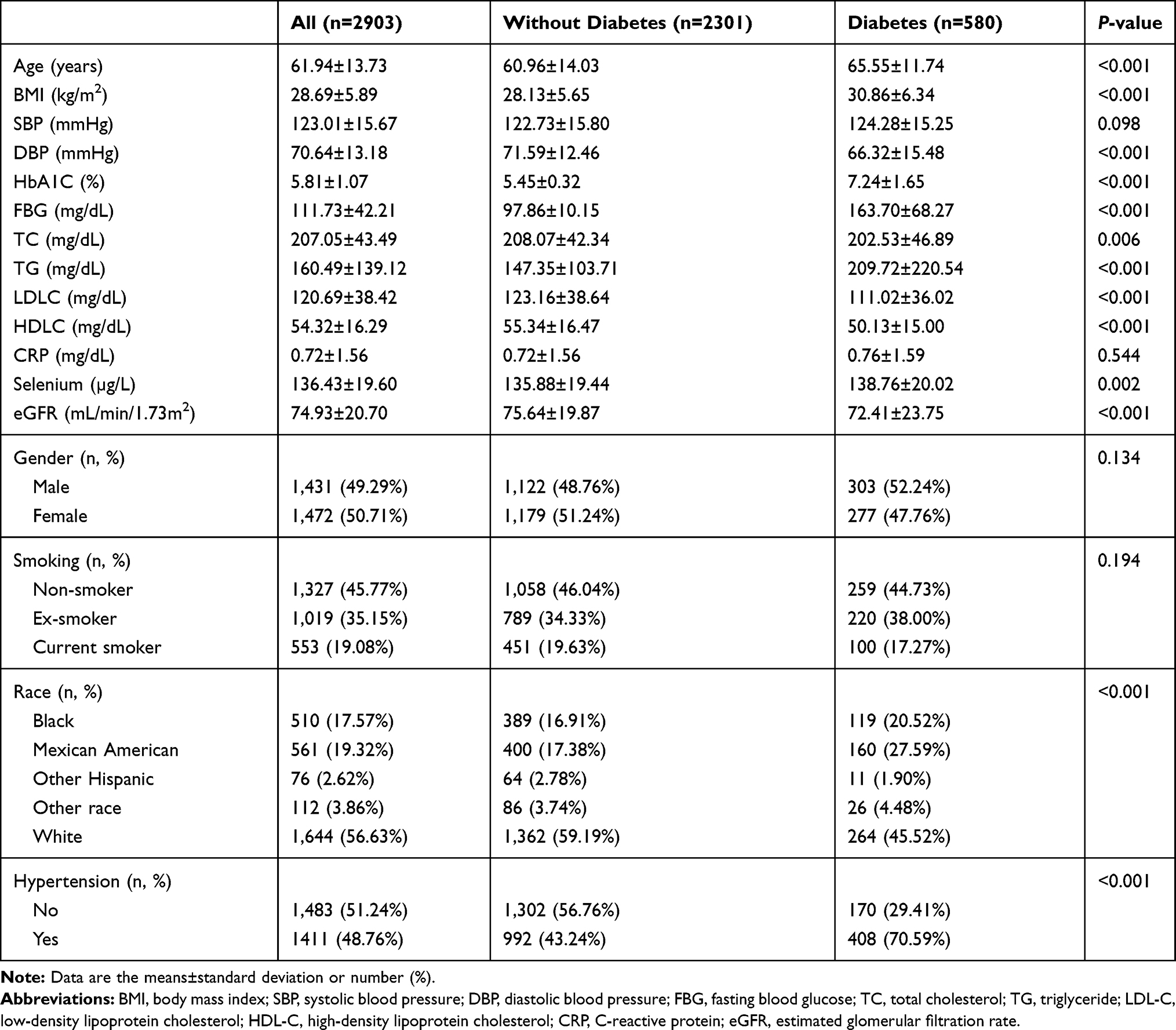 |
Table 1 Baseline Demographic and Clinical Parameters Between Diabetes and Without Diabetes |
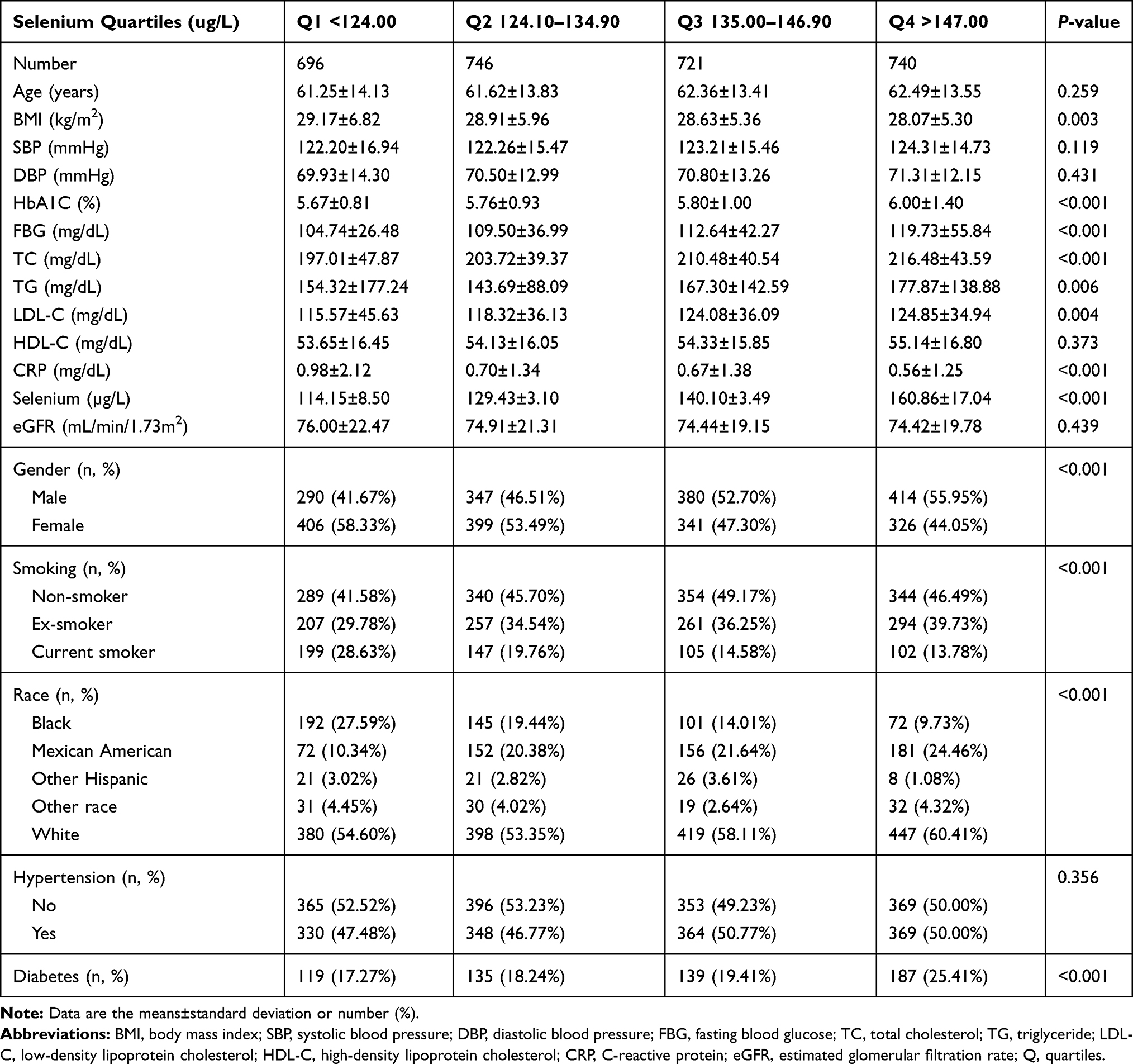 |
Table 2 Baseline Demographic and Clinical Parameters Among Participants |
Association of Selenium Concentration with Diabetes Mellitus
As shown in Table 3, for every 10 uµg/L increment in selenium concentration, the risk for DM increased by 12% (95% CI=1.01–1.24, P=0.0270) after being adjusted for age, sex, BMI, SBP, TC, TG, LDL-C, CRP, smoking, race, and hypertension history. Moreover, when using the lowest quartile of selenium as a reference, the ORs for DM increased in parallel with the quartiles of selenium (ORs were 1.15 (95% CI=0.65–2.03; P=0.6257), 1.49 (95% CI=0.83–2.70; P=0.1842), and 2.82 (95% CI=1.55–5.11; P=0.0007) from the second to the fourth quartiles, respectively, P<0.001 for trend).
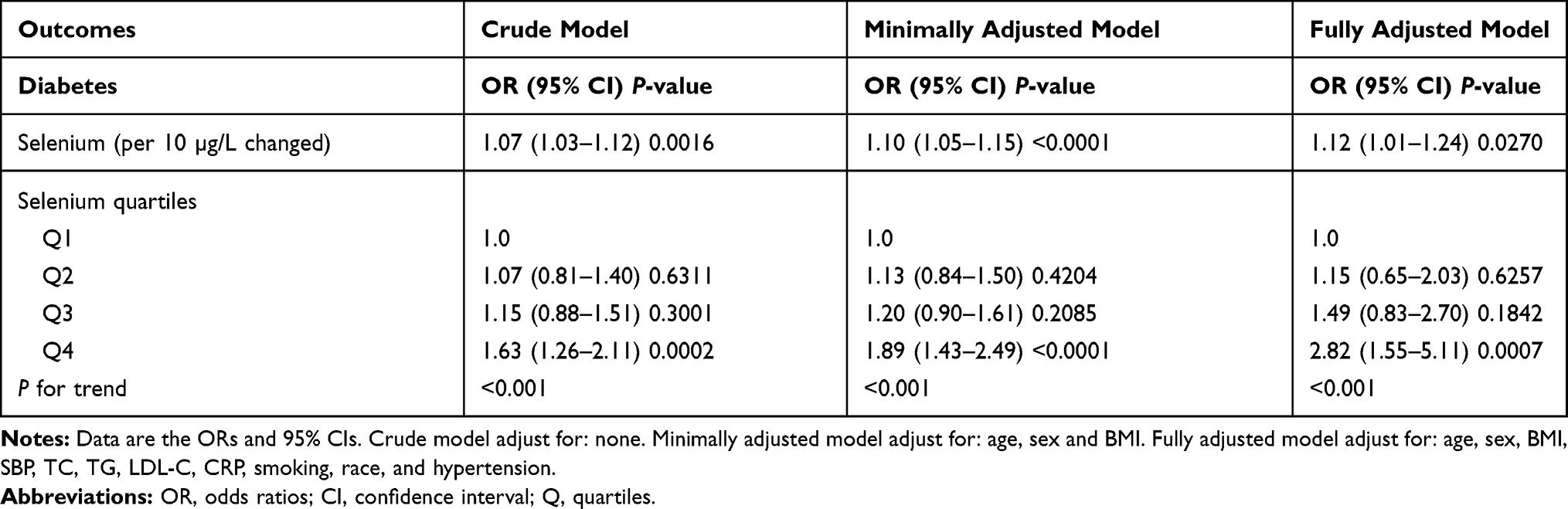 |
Table 3 The Association Between Selenium and Diabetes in Different Models |
Subgroup Analysis
As shown in Table 4, for every 10 uµg/L increment in selenium concentration, associated with an increased risk of DM in men (OR=1.07; 95% CI=0.93–1.22; P=0.3362) and in women (OR=1.21; 95% CI=1.02–1.43; P=0.0260), in participants aged <65 years (OR=1.43; 95% CI=1.21–1.69; P<0.001), and aged ≥65 years (OR=0.99; 95% CI=0.86–1.13; P=0.8659), respectively. When selenium was treated as a categorical variable, patients in Q4 had a significantly elevated risk for DM compared with those in Q1 among females (OR=5.51, 95% CI=2.11–14.37; P=0.0005) and those aged <65 years (OR=5.87, 95% CI=2.52–13.65; P<0.0001), but this difference did not reach statistical significance in male subjects (OR=1.87, P=0.1272) and those aged ≥65 years (OR=1.40; 95% CI=0.57–3.45; P=0.4680).
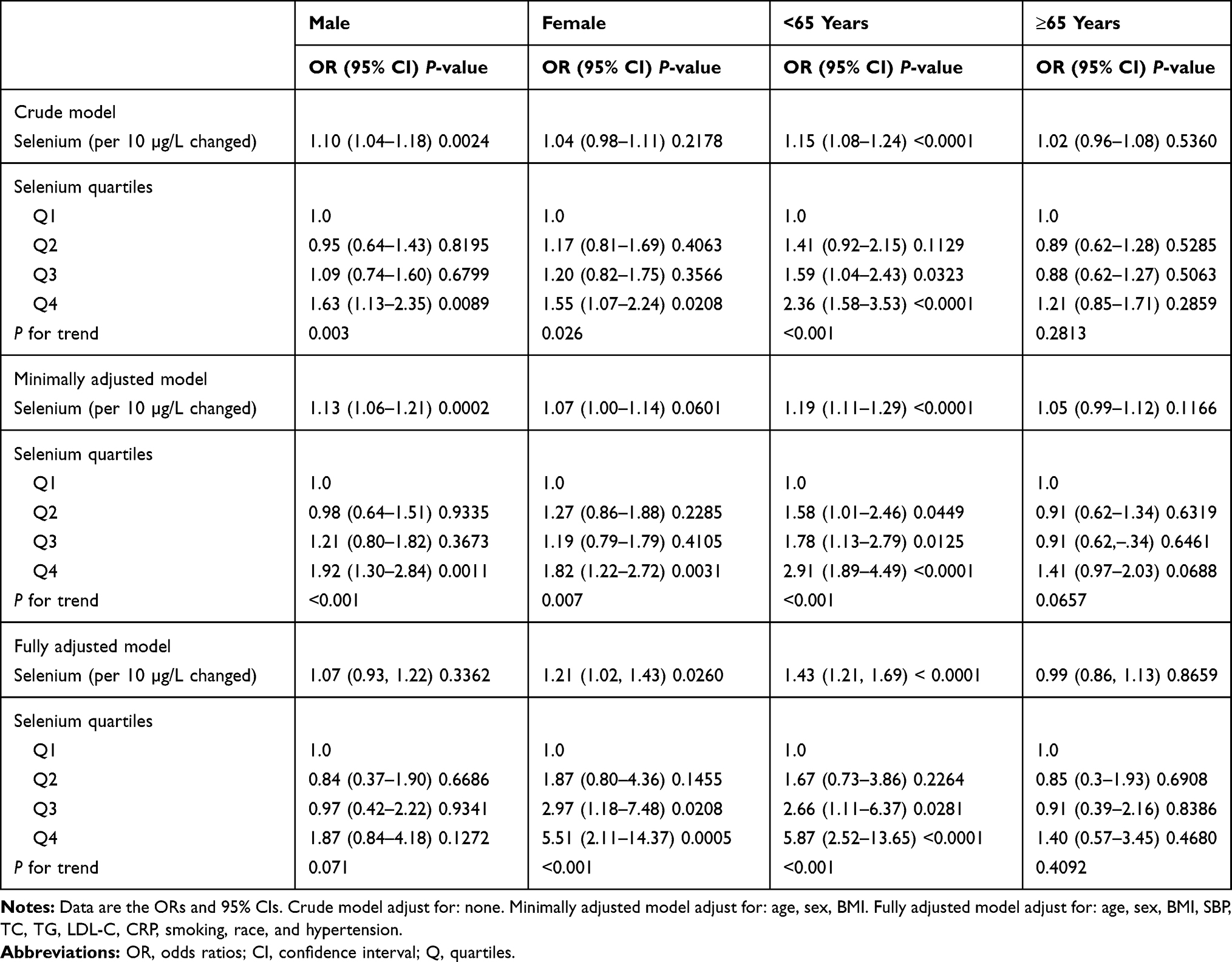 |
Table 4 The Association Between Selenium and Diabetes in Subgroups |
Discussion
The present study demonstrated that DM patients had higher selenium levels than those without DM among the general US population. The subgroup analysis according to sex showed significant results only in females aged <65 years.
These results were in agreement with a meta-analysis of 20 observational studies suggesting that higher concentrations of selenium (from blood, nail, urine, and dietary intake) were an independent risk factor for the DM.23 However, a meta-analysis also showed a modest association between blood selenium and DM, and further indicating a likely U-shaped relationship between blood selenium and DM.33 Although our findings suggested an obvious correlation between an increased exposure to selenium and DM, data from clinical trials of selenium supplementation have not been conclusive. A meta-analysis of randomized controlled trials on selenium supplementation and the risk of type 2 DM showed no significant relationship.34 In addition, in our study, the association between higher selenium concentration and higher the risk of DM might be attributed by the levels of blood lipids.
In the present study, we also found selenium to be an independent risk factor for DM only in women and the young population. Our results were similar to a previous study, where female subjects seemed to have higher risk for DM.35,36 However, a cross-sectional study among Chinese middle-aged and older adults suggested no significant association between selenium intake and DM both in males and females.37 We speculated that, on the one hand, the population selection and race of the study population were different. On the other hand, the difference mechanisms for hormonal control in females may also play a role in selenium metabolism. Moreover, sex-specific nutritional and health behaviors may contribute to observed discrepancies in selenium levels between men and women.38 Finally, selenoprotein biosynthesis was sexually dimorphic in the liver, indicating that hepatic metabolism of dietary selenium may differ in males and females.39,40 In this study, the average age of the patients was older than 60 years, suggesting that the effect of estrogen on secretion function of female patients have significantly reduced, and estrogen has played an important role in liver metabolism.41
Selenium has multiple and complex effects on the development of DM. The potential mechanism of action for any linkage between selenium and T2D may be mediated in part via the selenoprotein glutathione peroxidase-1 (GPx-1).42 Basic researchshowed that overexpression or prolonged activation of GPx-1 may result in dysregulation of insulin signaling and cause insulin resistance.43,44 Moreover, selenium metabolism is accompanied by oxidative stress, and the metabolites of oxidation could have toxic effects on pancreatic β cells.45 However, more researches are needed to clarify the relationship between selenium and diabetes.
There are some limitations in the present study. First, DM and hypertension history were obtained from self-reported data. Second, the present study was the cross-sectional design that did not reveal causal relationships between selenium concentrations with DM. In addition, dietary habits, living environment of the subjects, ethnicity, and medication use (such as vitamins, trace element supplements, diuretics) data were missing in this study. Finally, the lack of information about selenium supplementation would be an issue.
Conclusion
In conclusion, the present study suggested that circulating selenium concentrations were significantly associated with DM in the US adult population, but the association differed by sex and age. However, the potential mechanism between selenium levels and DM were not elucidated, and further research is needed to make this causal relationship clear.
Ethics Approval and Informed Consent
The survey protocol was approved by the Institutional Review Board of the Centers for Disease Control and Prevention (Protocol #98-12, Protocol #2005-06). Written informed consent was obtained from all subjects.
Funding
This work was supported by the Medical Scientific Research Foundation of Guangdong Province of China (No. A2020620) and the Project of Administration of Traditional Chinese Medicine of Guangdong Province of China (No. 20191050).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care. 2014;37(Suppl 1):S81–SS90. doi:10.2337/dc14-S081
2. Praveeena S, Pasula S, Sameera K. Trace elements in diabetes mellitus. J Clin Diagn Res. 2013;7:1863–1865.
3. Cancarini A, Fostinelli J, Napoli L, Gilberti ME, Apostoli P, Semeraro F. Trace elements and diabetes: assessment of levels in tears and serum. Exp Eye Res. 2017;154:47–52. doi:10.1016/j.exer.2016.10.020
4. Badran M, Morsy R, Soliman H, Elnimr T. Assessment of trace elements levels in patients with Type 2 diabetes using multivariate statistical analysis. J Trace Elem Med Biol. 2016;33:114–119. doi:10.1016/j.jtemb.2015.10.006
5. Ugurlu V, Binay C, Simsek E, Bal C. Cellular trace element changes in type 1 diabetes patients. J Clin Res Pediatr Endocrinol. 2016;8:180–186. doi:10.4274/jcrpe.2449
6. Li Z, Wang C, Li L, et al. The study on the correlation between six kinds of mineral elements and diabetes. Biol Trace Elem Res. 2018;183:226–232. doi:10.1007/s12011-017-1136-6
7. Neve J. Physiological and nutritional importance of selenium. Experientia. 1991;47:187–193. doi:10.1007/BF01945424
8. Brtkova A. [Biological effects of selenium]. Bratisl Lek Listy. 1992;93:629–632. Slovak.
9. Tinkov AA, Ajsuvakova OP, Filippini T, et al. Selenium and selenoproteins in adipose tissue physiology and obesity. Biomolecules. 2020;10:658. doi:10.3390/biom10040658
10. Bastola MM, Locatis C, Maisiak R, Fontelo P. Selenium, copper, zinc and hypertension: an analysis of the National Health and Nutrition Examination Survey (2011–2016). BMC Cardiovasc Disord. 2020;20:45. doi:10.1186/s12872-020-01355-x
11. Zwierello W, Styburski D, Maruszewska A, et al. Bioelements in the treatment of burn injuries - The complex review of metabolism and supplementation (copper, selenium, zinc, iron, manganese, chromium and magnesium). J Trace Elem Med Biol. 2020;62:126616. doi:10.1016/j.jtemb.2020.126616
12. Vinceti M, Chawla R, Filippini T, et al. Blood pressure levels and hypertension prevalence in a high selenium environment: results from a cross-sectional study. Nutr Metab Cardiovasc Dis. 2019;29:398–408. doi:10.1016/j.numecd.2019.01.004
13. Huttunen JK. Selenium and cardiovascular diseases–an update. Biomed Environ Sci. 1997;10:220–226.
14. Zwolak I, Zaporowska H. Selenium interactions and toxicity: a review. Selenium interactions and toxicity. Cell Biol Toxicol. 2012;28:31–46.
15. Jossa F, Trevisan M, Krogh V, et al. Serum selenium and coronary heart disease risk factors in southern Italian men. Atherosclerosis. 1991;87:129–134. doi:10.1016/0021-9150(91)90015-U
16. Laclaustra M, Navas-Acien A, Stranges S, Ordovas JM, Guallar E. Serum selenium concentrations and hypertension in the US population. Circ Cardiovasc Qual Outcomes. 2009;2:369–376. doi:10.1161/CIRCOUTCOMES.108.831552
17. Retondario A, Fernandes R, Rockenbach G, et al. Selenium intake and metabolic syndrome: a systematic review. Clin Nutr. 2019;38:603–614. doi:10.1016/j.clnu.2018.02.021
18. Su L, Gao S, Unverzagt FW, et al. Selenium level and dyslipidemia in rural elderly Chinese. PLoS One. 2015;10:e136706.
19. Giovannini S, Onder G, Lattanzio F, et al. Selenium concentrations and mortality among community-dwelling older adults: results from IlSIRENTE study. J Nutr Health Aging. 2018;22:608–612. doi:10.1007/s12603-018-1021-9
20. Kenfield SA, Van Blarigan EL, DuPre N, Stampfer MJ, Giovannucci EL, Chan JM. Selenium supplementation and prostate cancer mortality. J Natl Cancer Inst. 2015;107:360. doi:10.1093/jnci/dju360
21. Landucci F, Mancinelli P, De Gaudio AR, Virgili G. Selenium supplementation in critically ill patients: a systematic review and meta-analysis. J Crit Care. 2014;29:150–156. doi:10.1016/j.jcrc.2013.08.017
22. Strozyk A, Osica Z, Przybylak JD, et al. Effectiveness and safety of selenium supplementation for type 2 diabetes mellitus in adults: a systematic review of randomised controlled trials. J Hum Nutr Diet. 2019;32:635–645. doi:10.1111/jhn.12670
23. Kim J, Chung HS, Choi MK, et al. Association between serum selenium level and the presence of diabetes mellitus: a meta-analysis of observational studies. Diabetes Metab J. 2019;43:447–460. doi:10.4093/dmj.2018.0123
24. Vinceti M, Filippini T, Rothman KJ. Selenium exposure and the risk of type 2 diabetes: a systematic review and meta-analysis. Eur J Epidemiol. 2018;33:789–810. doi:10.1007/s10654-018-0422-8
25. Palmer MK, Toth PP. Trends in lipids, obesity, metabolic syndrome, and diabetes mellitus in the United States: an NHANES analysis (2003–2004 to 2013–2014). Obesity (Silver Spring). 2019;27:309–314. doi:10.1002/oby.22370
26. Christensen K, Lawler T, Dietary Carotenoids MJ. Non-alcoholic fatty liver disease among US Adults, NHANES 2003(-)2014. Nutrients. 2019;11:1101. doi:10.3390/nu11051101
27. Huang YQ, Liu XC, Lo K, et al. The U shaped relationship between high-density lipoprotein cholesterol and all-cause or cause-specific mortality in adult population. Clin Interv Aging. 2020;15:1883–1896. doi:10.2147/CIA.S271528
28. Curry SJ, Krist AH, Owens DK, et al. Behavioral weight loss interventions to prevent obesity-related morbidity and mortality in adults: US preventive services task force recommendation statement. JAMA. 2018;320:1163–1171. doi:10.1001/jama.2018.13022
29. Kim C, Bullard KM, Herman WH, Beckles GL. Association between iron deficiency and A1C levels among adults without diabetes in the National Health and Nutrition Examination Survey, 1999–2006. Diabetes Care. 2010;33:780–785. doi:10.2337/dc09-0836
30. American Diabetes Association. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42:S13–S28. doi:10.2337/dc19-S002
31. Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension. 2003;42:1206–1252.
32. Laclaustra M, Navas-Acien A, Stranges S, Ordovas JM, Guallar E. Serum selenium concentrations and diabetes in U.S. adults: National Health and Nutrition Examination Survey (NHANES) 2003–2004. Environ Health Perspect. 2009;117:1409–1413. doi:10.1289/ehp.0900704
33. Wang XL, Yang TB, Wei J, Lei GH, Zeng C. Association between serum selenium level and type 2 diabetes mellitus: a non-linear dose-response meta-analysis of observational studies. Nutr J. 2016;15:48.
34. Mao S, Zhang A, Huang S. Selenium supplementation and the risk of type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Endocrine. 2014;47:758–763. doi:10.1007/s12020-014-0298-7
35. Kohler LN, Florea A, Kelley CP, et al. Higher plasma selenium concentrations are associated with increased odds of prevalent type 2 diabetes. J Nutr. 2018;148:1333–1340. doi:10.1093/jn/nxy099
36. Moon S, Chung HS, Yu JM, et al. Association between serum selenium level and the prevalence of diabetes mellitus in U.S. population. J Trace Elem Med Biol. 2019;52:83–88. doi:10.1016/j.jtemb.2018.12.005
37. Wei J, Zeng C, Gong QY, et al. The association between dietary selenium intake and diabetes: a cross-sectional study among middle-aged and older adults. Nutr J. 2015;14:18. doi:10.1186/s12937-015-0007-2
38. Vinceti M, Filippini T, Del GC, et al. Selenium for preventing cancer. Cochrane Database Syst Rev. 2018;1:D5195.
39. Stoedter M, Renko K, Hog A, Schomburg L. Selenium controls the sex-specific immune response and selenoprotein expression during the acute-phase response in mice. Biochem J. 2010;429:43–51. doi:10.1042/BJ20091868
40. Riese C, Michaelis M, Mentrup B, et al. Selenium-dependent pre- and posttranscriptional mechanisms are responsible for sexual dimorphic expression of selenoproteins in murine tissues. Endocrinology. 2006;147:5883–5892. doi:10.1210/en.2006-0689
41. Palmisano BT, Zhu L, Stafford JM. Role of estrogens in the regulation of liver lipid metabolism. Adv Exp Med Biol. 2017;1043:227–256.
42. Sunde RA, Zemaitis EN, Blink AB, Lawinger JA. Impact of glutathione peroxidase-1 (Gpx1) genotype on selenoenzyme and transcript expression when repleting selenium-deficient mice. Biol Trace Elem Res. 2018;186:174–184. doi:10.1007/s12011-018-1281-6
43. McClung JP, Roneker CA, Mu W, et al. Development of insulin resistance and obesity in mice overexpressing cellular glutathione peroxidase. Proc Natl Acad Sci U S A. 2004;101:8852–8857. doi:10.1073/pnas.0308096101
44. Yang X, Feng L, Li C, Li Y. Tranilast alleviates endothelial dysfunctions and insulin resistance via preserving glutathione peroxidase 1 in rats fed a high-fat emulsion. J Pharmacol Sci. 2014;124:18–30. doi:10.1254/jphs.13151FP
45. Liu C, Fu Y, Li CE, Chen T, Li X. Phycocyanin-functionalized selenium nanoparticles reverse palmitic acid-induced pancreatic beta cell apoptosis by enhancing cellular uptake and blocking reactive oxygen species (ROS)-mediated mitochondria dysfunction. J Agric Food Chem. 2017;65:4405–4413. doi:10.1021/acs.jafc.7b00896
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.