")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
The Association of Aspartate Aminotransferase/Alanine Aminotransferase Ratio with Diabetic Nephropathy in Patients with Type 2 Diabetes
Received 27 July 2021
Accepted for publication 27 August 2021
Published 7 September 2021 Volume 2021:14 Pages 3831—3837
DOI https://doi.org/10.2147/DMSO.S330741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Jing Xu, Xiaomin Shi, Youjin Pan
Department of Endocrinology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
Correspondence: Youjin Pan
Department of Endocrinology, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Lucheng District, Wenzhou, Zhejiang Province, People’s Republic of China
Tel +86 15068256508
Fax +86 577-85678813
Email [email protected]
Purpose: To investigate the relationship between aspartate aminotransferase to alanine aminotransferase ratio (AST/ALT) and diabetic nephropathy (DN).
Patients and Methods: A total of 402 patients with type 2 diabetes mellitus were divided into three groups, such as normoalbuminuria (n = 196), microalbuminuria (n = 131) and macroalbuminuria (n = 75) groups. Basic information and laboratory results were collected. Serum AST/ALT, tumor necrosis factor-α (TNF-α), interleukin (IL)-2, IL-4, IL-6, IL-10 and interferon- γ (INF- γ) were also measured. DN was defined as microalbuminuria or macroalbuminuria. The estimated glomerular filtration rate (eGFR) was calculated using the following formula: 186 × (serum creatinine)− 1.154× (age)− 0.203× (0.742 if female).
Results: The AST/ALT in the macroalbuminuria group was higher than in the microalbuminuria and normoalbuminuria groups. The concentrations of tumor necrosis factor-α (TNF-α), IL-2, IL-4, IL-10 and INF-γ in the macroalbuminuria group were significantly higher than those in the two other groups. Multivariate logistical analysis showed that after adjusting confounding factors, TNF-α and high AST/ALT were independent risks for DN and macroalbuminuria. Furthermore, the AST/ALT had significantly positive correlation with TNF-α (r = 0.101, P = 0.048), IL-4 (r = 0.185, P = 0.005) and IL-6 (r = 0.274, P < 0.001) levels.
Conclusion: This study showed that high AST/ALT was an independent risk factor for the DN. Additionally, AST/ALT was positively correlated with inflammation cytokines, such as TNF-α, IL-4 and IL-6 levels.
Keywords: AST/ALT, diabetic nephropathy, inflammatory factors, tumor necrosis factor-α
Introduction
China has the highest incidence rate of diabetes mellitus in the world, and there is a growing trend. In China, the latest publications show that the prevalence of diabetes mellitus has risen to 12.8% nationwide.1 By the year 2045, an estimated 693 million people had diabetes mellitus.2 DN affects about 25% of patients with type 2 diabetes mellitus (T2DM), which is the main cause of end-stage renal disease (ESRD) in high income countries.3,4 In addition, the cardiovascular risk of DN is very high, and the cardiovascular risk is similar to that of patients with coronary heart disease.5,6 Therefore, it is very important to identify and manage the risk factors of DN and diagnose and treat the disease in time.
Serum transaminase, aspartate transaminase (AST) and alanine transaminase (ALT) are routine indexes of liver function. In 1957, the serum AST and ALT activity ratio of was first proposed as De Ritis ratio.7 AST/ALT is correlated with oxidative stress and systemic inflammation.8 Although it was originally proposed as a feature of viral hepatitis, such a ratio seems to serve as a practical biomarker for other diseases. It has been reported that AST/ALT is correlated with chronic kidney disease (CKD) and metabolic syndrome (MetS).9,10 However, there are no studies about the relationship between AST/ALT and DN.
Inflammation plays a crucial role in the development and progression of DN, as many inflammatory cytokines such as interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor α (TNF-α) contribute in the pathogenesis of DN.8 This study aims to analyze the correlation between AST/ALT and inflammatory factors and DN.
Materials and Methods
Study Design and Participants
Patients with type 2 diabetes (T2DM) were recruited in Department of Endocrinology, the second affiliated hospital of Wenzhou Medical University from October 2019 to March 2021. There were 402 T2DM patients aged 40–83 years with complete data. According to the American Diabetes Association standard, the 75g oral glucose tolerance test was diagnosed as diabetes mellitus. The exclusion criteria included type 1 diabetes, alcohol consumption equal to or greater than 20g/day in the last 3 month, viral or autoimmune hepatitis, previous diagnosis of acute or chronic liver disease, intake of hepatotoxic drugs, inflammatory diseases, malignancy. All participants in our study were divided into three group, such as diabetes mellitus with normoalbuminuria (n=196), microalbuminuria (n=131) and macroalbuminuria (n=75) groups. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (No. LCKY2019-21, date: Jan 2019) and written informed consent was obtained from all subjects in accordance with the Declaration of Helsinki.
Data Collection
Detailed clinical history, included gender, age. The weight and height of each participant were measured to the nearest 0.1kg and 0.1cm, respectively. The formula of body mass index (BMI) is as follows: BMI = weight (kg)/height (m2). Their blood pressure was measured with automatic instruments while they were sitting (HEM-907, Omron, Kyoto, Japan). The use history of oral RAAS inhibitor drugs and statins were recorded.
Blood samples were collected from the anterior cubital vein during fasting at night. Renal function, liver function, blood glucose, alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum uric acid, serum creatinine, urea, glycated hemoglobin (HbA1c) and lipid profiles, including total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C). Urinary albumin and creatinine excretion were measured by immunoturbidimetric assay and enzymatic method, and the clinical stage of proteinuria was evaluated by the urine albumin and creatinine ratio (UACR, mg/g) (macroalbuminuria, ACR≥300; microalbuminuria, ACR 30–299; normoalbuminuria, ACR <30). eGFR was calculated using the following formula: 186 × (serum creatinine)−1.154× (age)−0.203× (0.742 if female). DN is defined as microalbuminuria or macroalbuminuria.
Serum Cytokine Levels
Serum samples for cytokine detection were collected and stored at −70°C. The serum levels of TNF-α, INF-γ, IL-10, IL-6, IL-4, IL-2, were detected by Luminex xMAP (Ceger Biotechnology Co., Ltd., China) according to the manufacturer’s instructions. Serum levels were measured in pg/mL.
Statistical Analysis
SPSS 21.0 software (SPSS Inc., Chicago, IL) was used for statistical analysis. Data were expressed as mean ± (SD), percentage or median with quartile range. The differences between groups were analyzed by ANOVA. Count data were analyzed by χ2 test. Spearman correlation was used to analyze the correlation between AST/ALT and clinical/biochemical parameters. The independent variables were analyzed by multivariate logistic analysis, and the odds ratio (OR) between the two groups was calculated by 95% confidence interval (CI). All tests were bilateral, P < 0.05, with statistical significance. Multicollinearity was tested using the variance inflation factor (VIF) and tolerance test. For this study multicollinearity was ruled-out with VIF <1.8/tolerance >0.54.
Results
A total of 402 patients aged 40–83 years old were recruited. Table 1 shows the baseline characteristics. No significant difference in BMI, gender and waist/hip ratio was found among the normoalbuminuria, microalbuminuria and macroalbuminuria groups (all P>0.05). No significant differences in the levels of HbA1c, HDL-c, TC and LDL-c was observed among the three groups (all P>0.05). The levels of 24-hour urinary protein, UACR, age, systolic blood pressure (SBP), blood urea, serum creatinine, the proportion of oral RAAS inhibitor and statin in the microalbuminuria and macroalbuminuria groups were significantly higher than those in the normoalbuminuria group (all P<0.05). The level of eGFR in the microalbuminuria and macroalbuminuria groups were significantly lower than that in the normoalbuminuria group (P<0.05). The levels of TG and diastolic blood pressure (DBP) in the macroalbuminuria group were significantly higher than those in the normoalbuminuria and the microalbuminuria groups (all P<0.05).
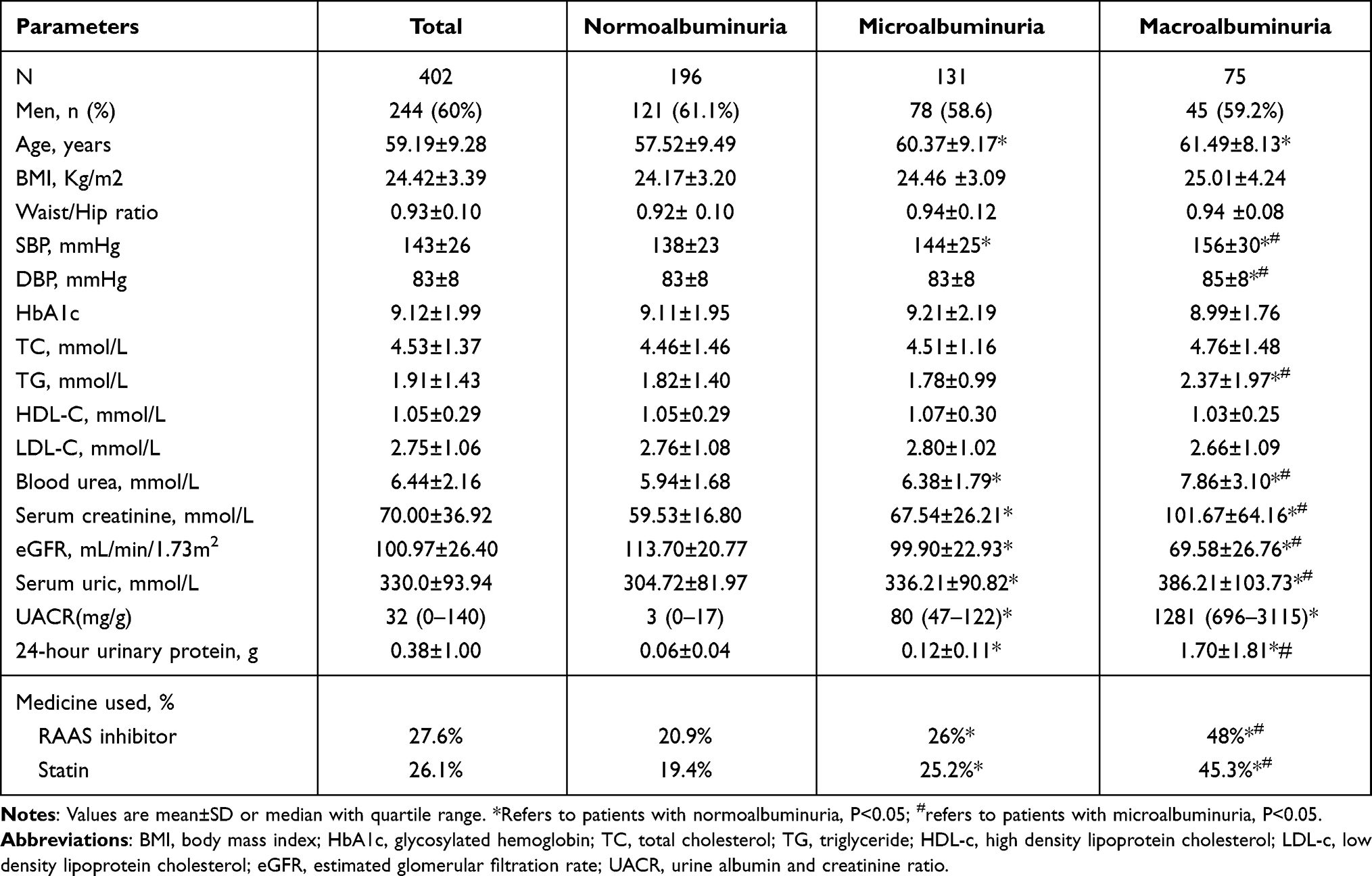 |
Table 1 Characteristics of the Study Populations |
There was significant difference in the AST/ALT level was found among the three groups (Table 2). The levels of AST/ALT in normoalbuminuria, microalbuminuria and macroalbuminuria groups were 0.95±0.34, 1.01±0.44, 1.25±0.71, respectively (P<0.05). No significant difference was observed in IL-6, INF-γ levels among the three groups. The macroalbuminuria group had significantly higher AST/ALT levels compared with the normoalbuminuria and the microalbuminuria groups (all P<0.01). The microalbuminuria and the macroalbuminuria groups had significantly higher serum IL-10, TNF-α levels compared with the normoalbuminuria group (all P<0.05). The macroalbuminuria group had significantly higher serum IL-2, IL-4 levels compared with the normoalbuminuria group.
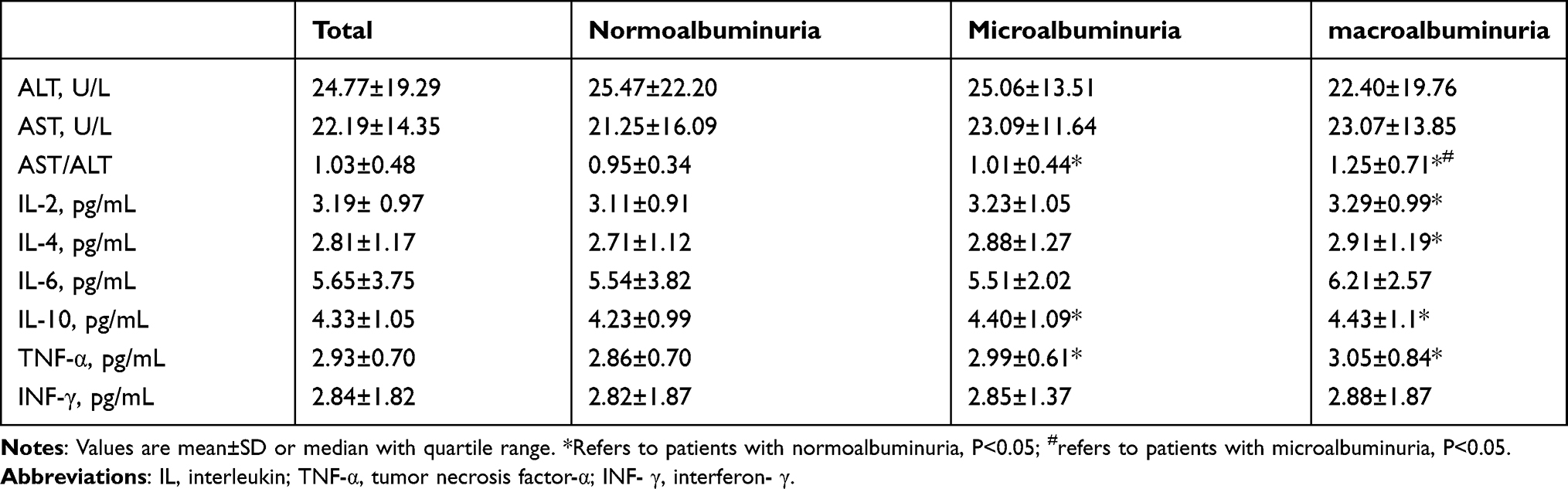 |
Table 2 AST/ALT Level and Serum Cytokine in Study Subjects |
The Spearman correlations between the AST/ALT and biochemical and clinical parameters are shown in Table 3. The age (r=0.208, P<0.001), TG (r=0.208, P<0.001), UACR (r=0.188, P<0.001), 24-hour urinary protein (r=0.154, P<0.001), IL4 (r=0.185, P=0.005), IL-6 (r=0.274, P<0.001) and TNF-α (r=0.101, P=0.048) showed significantly correlations with AST/ALT. The Spearman correlations analyses showed that the AST/ALT level was negatively associated with HDL-c (r=−0.170, P=0.001) and BMI (r=−0.144, P=0.004).
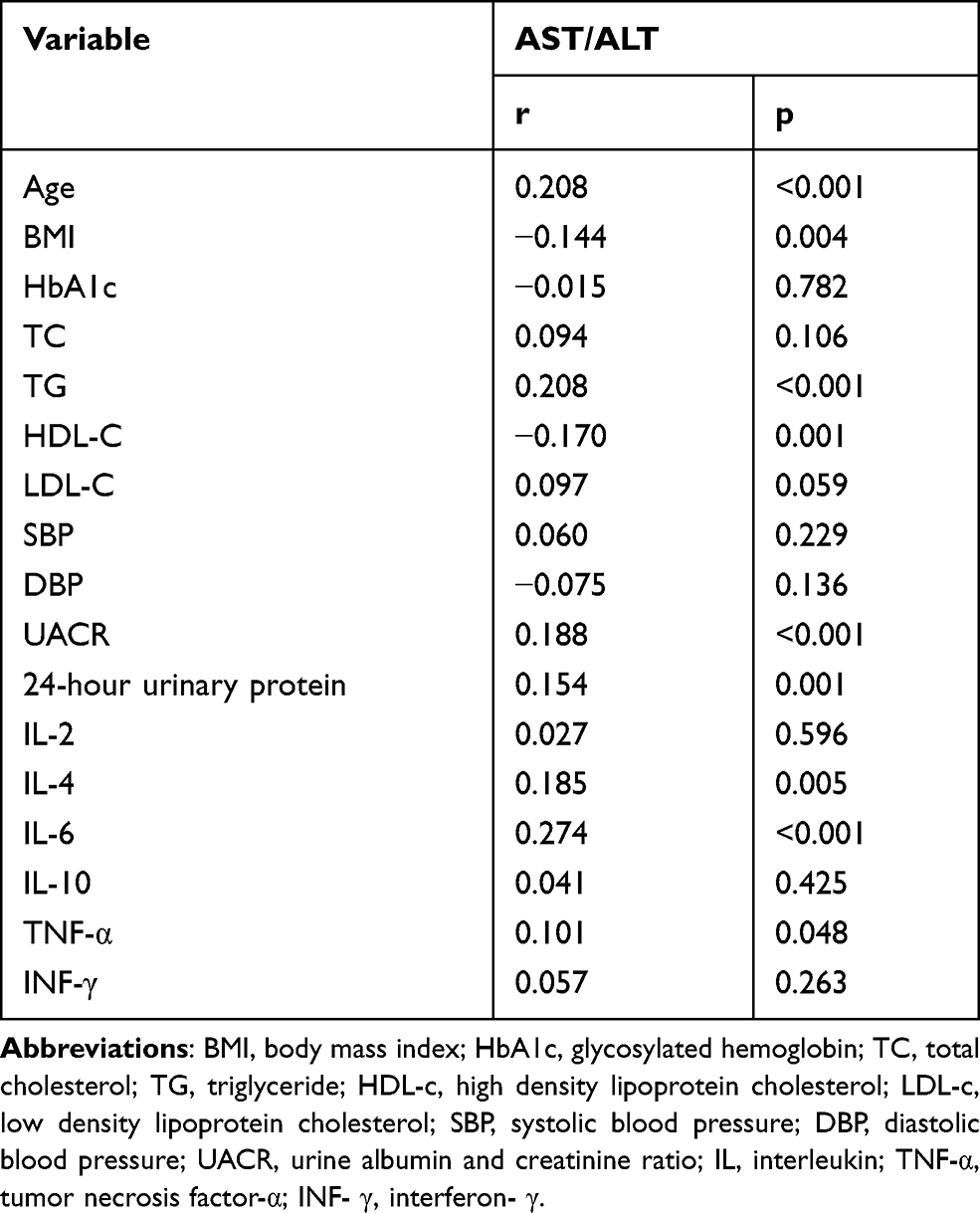 |
Table 3 Spearman Correlation of AST/ALT Levels with Clinical and Biochemical Parameters |
Multivariate logistic model was constructed to detect the risk factors of DN and macroalbuminuria. As shown in Table 4, the multivariate analysis after adjusting age, gender, waist/hip ratio and using RAAS inhibitor, statin, SBP, DBP, TG, serum creatine, serum uric and urea nitrogen, AST/ALT was still strongly associated with DN (OR=1.770, 95% CI, 1.002–3.127, P=0.044), macroalbuminuria (OR=2.471, 95% CI=1.113–5.487, P=0.026) and TNF-α levels were also significantly associated with the DN (OR=1.590, 95% CI,=1.081–2.374, P=0.047), macroalbuminuria (OR=2.347, 95% CI, 1.185–4.651, P=0.014).
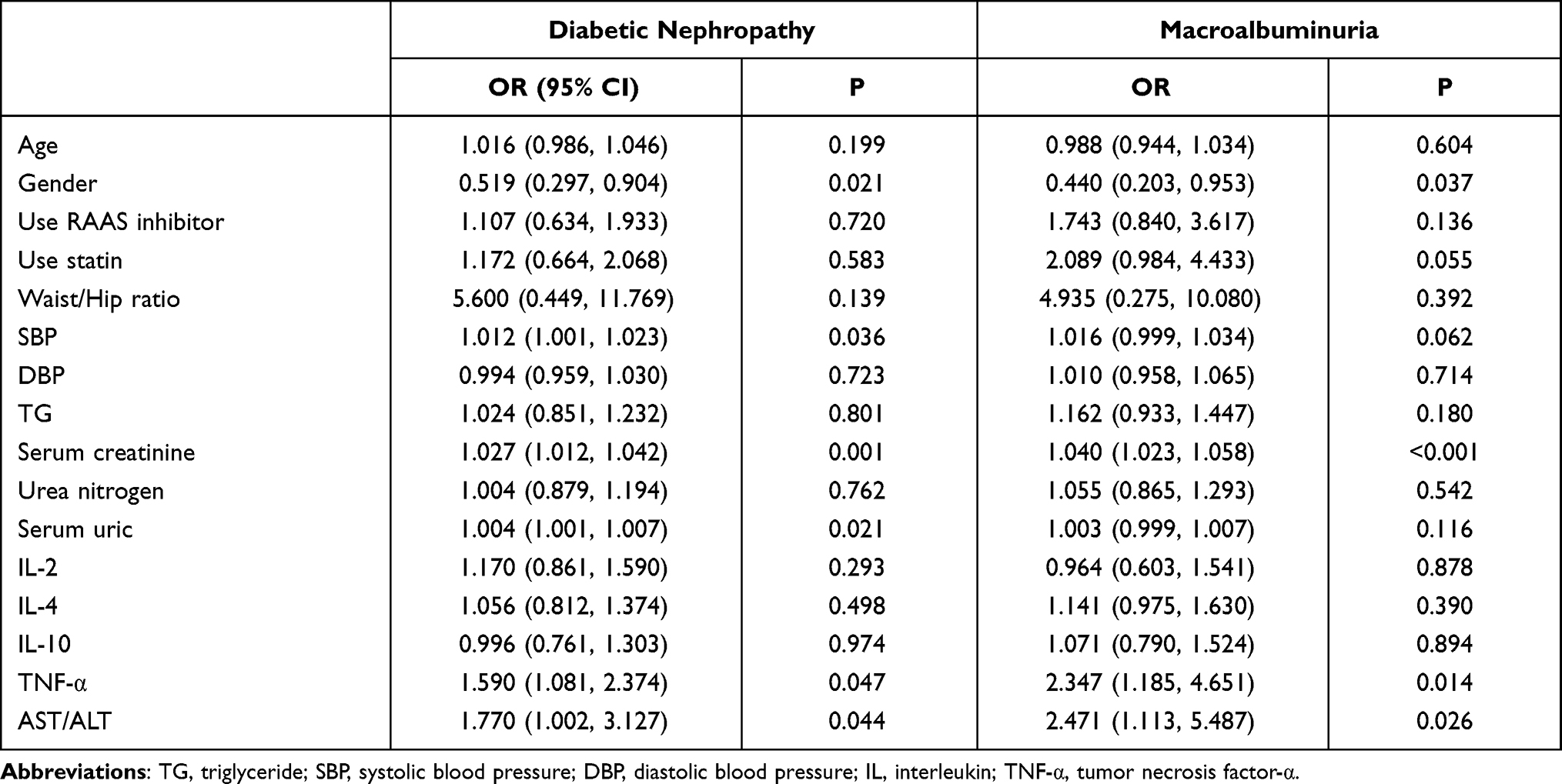 |
Table 4 AST/ALT Associated with the Presence of Diabetic Nephropathy and Macroalbuminuria in Logistic Regression |
Discussion
In 1957, Italian pathologist Fernando De Ritis first described it as an enzyme for viral hepatitis.7 As a potential predictor of many diseases, the ratio of AST to ALT has attracted much attention in recent years. To our knowledge, it is the first study to detect the correlation between AST/ ALT and DN. According to our results, AST/ALT showed an independent correlation with DN, which was still obvious after adjustment for AST/ALT associated factors related to DN. Therefore, AST/ALT could serve as a strong predictor for DN.
More and more evidences emphasize the key role of inflammation in the development of DN.11 Macrophages are the main mediators.12 Macrophages are the main inflammatory cells involved in kidney damage, and their accumulation is related to the severity of DN.13–15 The aggregation of renal macrophages in patients with DN is associated with decreased renal function.16 Our findings are consistent with previous studies. It is found that the levels of IL-10, IL-4, IL-2, and TNF-α in patients in the macroalbuminuria group are significantly higher than those in the microalbuminuria and normoalbuminuria group (P<0.01). In addition, after adjusting age, gender, waist/hip ratio and using RAAS inhibitor, statin, SBP, DBP, TG, serum creatine, serum uric and urea nitrogen, TNF-α is independent risk factor for DN. Tumor necrosis factor receptors (TNFRs) are regulated by TNF- α, which plays an important role in the process of inflammation.17 TNFRs mainly exist in glomeruli and peritubular capillary endothelial cells.18 In T2DM patients, high levels of serum TNFRs are associated with global sclerosis, decreased glomerular filtration, and foot process regression.19
This study confirmed that AST/ALT was associated with IL-4 (r = 0.185, P = 0.005), IL-6 (r = 0.274, P<0.001) and TNF- α (r=0.101, P=0.048). AST/ALT was positively correlated with inflammatory cytokines, which was consistent with previous studies. Wang et al have confirmed the significant effect of the AST/ALT, as well as the CRP level.8 Therefore, it is reasonable to guess that the increase of AST/ALT increased DN through inflammation cytokines.
AST/ALT is often used to evaluate liver function and reflect the severity of liver disease. The first report on AST/ALT appeared in 1957.20 AST/ ALT can be used to detect extrahepatic diseases and evaluate the prognosis of patients with renal function. Feng et al found that ALT level decreased with the progression of renal dysfunction, resulting in a higher prevalence of AST/ ALT in peritoneal dialysis patients.21 Miyuki et al found that subjects with high AST/ALT had lower BMI and eGFR levels.22 Zhao et al reported that high AST/ALT is a risk factor for insulin resistance.23 Weng et al reported that high AST/ALT was a risk factor for cardiovascular disease in males during a 10-year long-term follow-up.24 In addition, Canat et al reported that high AST/ALT value is a risk factor for poor prognosis of non-metastatic renal cell carcinoma.25 In the present study, our results also revealed that high AST/ALT values were as risk factor for DN.
From the perspective of elevated AST/ALT, it is speculated that the change of this ratio reflects the inconsistency between AST and ALT. ALT is mainly distributed in the cytoplasm of hepatocytes, and AST is widely distributed in muscle, kidney, lung, brain and liver mitochondria.26 The higher the value of AST/ALT is the more significant the release of AST. High AST/ALT can aggravate insulin resistance, and result in the release of a variety of proinflammatory, prooxidant and pro fibrinogen mediators, which are important in the pathogenesis of CKD and CVD.27,28 Insulin resistance can lead to the activation of renin-angiotensin system and atherosclerotic dyslipidemia, which is the key driving factor of renal and vascular injury.
There are several limitations in this study. Firstly, this study is a single center cross-sectional study with few cases. Secondly, due to other complications, T2DM usually needs to take multiple drugs at the same time. Therefore, it is difficult to determine which drugs may affect liver transaminase due to drug interactions. Further long-term prospective cohort studies or intervention studies are needed to confirm the causal relationship of DN.
Conclusion
In summary, the findings of our study indicate that elevated AST/ALT was an independent factor for risk of DN. In addition, AST/ALT was positively correlated with inflammation cytokines, such as TNF-α, IL-4 and IL-6 levels.
Abbreviations
AST/ALT, aspartate aminotransferase to alanine aminotransferase ratio; FBG, fasting blood glucose; BMI, body mass index; HbA1c, glycosylated hemoglobin; TNF-α, tumor necrosis factor-α; TC, total cholesterol; TG, triglycerides; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol.
Data Sharing Statement
The data that support the findings of this study are available from Institutional Review Board of the second affiliated hospital and Yuying Children’s Hospital of Wenzhou Medical University but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the Jing Xu and Youjin Pan upon reasonable request and with permission of Institutional Review Board of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University.
Ethics Approval and Consent to Participate
This study has obtained the approval from the Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University (No. LCKY2019-21) and has obtained the written informed consent of all subjects following the Declaration of Helsinki.
Acknowledgments
The authors thank the staff of the Department of Endocrinology of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, as well as all the patients who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the grants of Project of Zhejiang Provincial Department of Health(2016KYB194), General Research Project of Zhejiang Provincial Education Department(Y201534290), Wenzhou Science and Technology Bureau (Y20120163). The funders played no role in the design of this study, the collection, analysis and interpretation of data or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ 2020;369:m997. doi:10.1136/bmj.m997
2. Cho NH, Shaw JE, Karuranga S, et al. IDF Diabetes Atlas: global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res Clin Pract. 2018;138:271–281. doi:10.1016/j.diabres.2018.02.023
3. Hooper SR, Johnson RJ, Gerson AC, et al. Overview of the findings and advances in the neurocognitive and psychosocial functioning of mild to moderate pediatric CKD: perspectives from the Chronic Kidney Disease in Children (CKiD) cohort study. Pediatr Nephrol. 2021;1. doi:10.1007/s00467-021-05158-w
4. de Boer IH, Rue TC, Hall YN, Heagerty PJ, Weiss NS, Himmelfarb J. Temporal trends in the prevalence of diabetic kidney disease in the United States. JAMA. 2011;305(24):2532–2539. doi:10.1001/jama.2011.861
5. Tonelli M, Muntner P, Lloyd A, et al. Risk of coronary events in people with chronic kidney disease compared with those with diabetes: a population-level cohort study. Lancet. 2012;380(9844):807–814. doi:10.1016/S0140-6736(12)60572-8
6. Choi SW, Kim HY, Ahn HR, et al. Association of bone mineral density with albuminuria and estimated glomerular filtration rate: the Dong-gu Study. Kidney Blood Press Res. 2013;37(2–3):132–141. doi:10.1159/000350067
7. De Ritis F, Coltorti M, Giusti G. An enzymic test for the diagnosis of viral hepatitis: the transaminase serum activities. 1957. Clinica chimica acta. 2006;369(2):148–152. doi:10.1016/j.cca.2006.05.001
8. Wang J, Li J, Ren Y, et al. Association between Alanine Aminotransferase/Aspartate Aminotransferase Ratio (AST/ALT Ratio) and coronary artery injury in children with Kawasaki disease. Cardiol Res Pract. 2020;2020:8743548. doi:10.1155/2020/8743548
9. Ochiai H, Shirasawa T, Yoshimoto T, et al. Elevated alanine aminotransferase and low aspartate aminotransferase/alanine aminotransferase ratio are associated with chronic kidney disease among middle-aged women: a cross-sectional study. BMC Nephrol. 2020;21(1):471. doi:10.1186/s12882-020-02144-6
10. Lin S, Tang L, Jiang R, et al. The relationship between aspartate aminotransferase to alanine aminotransferase ratio and metabolic syndrome in adolescents in Northeast China. Diabetes Metabol Syndr Obes. 2019;12:2387–2394. doi:10.2147/DMSO.S217127
11. Wada J, Makino H. Inflammation and the pathogenesis of diabetic nephropathy. Clin Sci. 2013;124(3):139–152. doi:10.1042/CS20120198
12. Tesch GH. Role of macrophages in complications of type 2 diabetes. Clin Exp Pharmacol Physiol. 2007;34(10):1016–1019. doi:10.1111/j.1440-1681.2007.04729.x
13. Pichler R, Afkarian M, Dieter BP, Tuttle KR. Immunity and inflammation in diabetic kidney disease: translating mechanisms to biomarkers and treatment targets. Am J Physiol Renal Physiol. 2017;312(4):F716–F731. doi:10.1152/ajprenal.00314.2016
14. Mora C, Navarro JF. Inflammation and pathogenesis of diabetic nephropathy. Metabol Clin Experimen. 2004;53(2):
15. Anders HJ. Innate versus adaptive immunity in kidney immunopathology. BMC Nephrol. 2013;14:138. doi:10.1186/1471-2369-14-138
16. Nguyen D, Ping F, Mu W, Hill P, Atkins RC, Chadban SJ. Macrophage accumulation in human progressive diabetic nephropathy. Nephrology. 2006;11(3):226–231. doi:10.1111/j.1440-1797.2006.00576.x
17. Al-Lamki RS, Mayadas TN. TNF receptors: signaling pathways and contribution to renal dysfunction. Kidney Int. 2015;87(2):281–296. doi:10.1038/ki.2014.285
18. Al-Lamki RS, Wang J, Skepper JN, Thiru S, Pober JS, Bradley JR. Expression of tumor necrosis factor receptors in normal kidney and rejecting renal transplants. Labor Investig. 2001;81(11):1503–1515. doi:10.1038/labinvest.3780364
19. Pavkov ME, Weil EJ, Fufaa GD, et al. Tumor necrosis factor receptors 1 and 2 are associated with early glomerular lesions in type 2 diabetes. Kidney Int. 2016;89(1):226–234. doi:10.1038/ki.2015.278
20. De Ritis F, Coltorti M, Giusti G. An enzymic test for the diagnosis of viral hepatitis; the transaminase serum activities. Clinica Chimica Acta. 1957;2(1):70–74. doi:10.1016/0009-8981(57)90027-X
21. Feng X, Wen Y, Peng FF, Wang N, Zhan X, Wu X. Association between aminotransferase/alanine aminotransferase ratio and cardiovascular disease mortality in patients on peritoneal dialysis: a multi-center retrospective study. BMC Nephrol. 2020;21(1):209. doi:10.1186/s12882-020-01840-7
22. Yokoyama M, Watanabe T, Otaki Y, et al. Association of the aspartate aminotransferase to alanine aminotransferase ratio with BNP level and cardiovascular mortality in the general population: the Yamagata study 10-year follow-up. Dis Markers. 2016;2016:4857917. doi:10.1155/2016/4857917
23. Zhao L, Cheng J, Chen Y, et al. Serum alanine aminotransferase/aspartate aminotransferase ratio is one of the best markers of insulin resistance in the Chinese population. Nutr Metab. 2017;14:64. doi:10.1186/s12986-017-0219-x
24. Weng SF, Kai J, Guha IN, Qureshi N. The value of aspartate aminotransferase and alanine aminotransferase in cardiovascular disease risk assessment. Open Heart. 2015;2(1):e000272. doi:10.1136/openhrt-2015-000272
25. Canat L, Ataly HA, Agalarov S, Alkan I, Altunrende F. The effect of AST/ALT (De Ritis) ratio on survival and its relation to tumor histopathological variables in patients with localized renal cell carcinoma. Int Braz J Urol. 2018;44(2):288–295. doi:10.1590/s1677-5538.ibju.2017.0173
26. Goessling W, Friedman LS. Increased liver chemistry in an asymptomatic patient. Clin Gastroenterol Hepatol. 2005;3(9):852–858. doi:10.1016/S1542-3565(05)00416-7
27. Francque SM, van der Graaff D, Kwanten WJ. Non-alcoholic fatty liver disease and cardiovascular risk: pathophysiological mechanisms and implications. J Hepatol. 2016;65(2):425–443. doi:10.1016/j.jhep.2016.04.005
28. Targher G, Byrne CD. Non-alcoholic fatty liver disease: an emerging driving force in chronic kidney disease. Nat Rev Nephrol. 2017;13(5):297–310. doi:10.1038/nrneph.2017.16
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.