")
Back to Journals » Journal of Inflammation Research » Volume 15
The Associated of the Risk of IVIG Resistance in Kawasaki Disease with ZNF112 Gene and ZNF180 Gene in a Southern Chinese Population
Authors Lu Z, Zheng Z, Xu Y, Wang C, Lin Y, Lin K, Fu L, Zhou H, Pi L, Che D, Gu X
Received 10 June 2022
Accepted for publication 5 August 2022
Published 2 September 2022 Volume 2022:15 Pages 5053—5062
DOI https://doi.org/10.2147/JIR.S378080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Zhaojin Lu,1,* Zepeng Zheng,1,* Yufen Xu,1,* Chenlu Wang,1 Yueling Lin,1 Kun Lin,1 LanYan Fu,1 Huazhong Zhou,1 Lei Pi,1 Di Che,1 Xiaoqiong Gu1,2
1Department of Clinical Biological Resource Bank, Guangzhou Institute of Pediatrics, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangzhou, People’s Republic of China; 2Department of Clinical Laboratory, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Di Che, Department of Clinical Biological Resource Bank, Guangzhou Institute of Pediatrics, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, 9 Jinsui Road, Guangzhou, 510623, Guangdong, People’s Republic of China, Tel/Fax +86-20-38076562, Email [email protected] Xiaoqiong Gu, Department of Clinical Biological Resource Bank, Department of Clinical Laboratory, Guangzhou Institute of Pediatrics, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, 9 Jinsui Road, Guangzhou, 510623, Guangdong, People’s Republic of China, Tel/Fax +86-20-38076561, Email [email protected]
Background: Kawasaki disease (KD) was one of the most common primary vasculitis. IVIG resistance was associated with an increased risk of coronary artery aneurysm. Accumulating evidences demonstrated that inflammatory gene polymorphisms might play important roles in IVIG resistance, and zinc finger proteins were closely related to immune inflammation regulation, but the effect of ZNF112/rs8113807 and ZNF180/rs2571051 on IVIG resistance in KD patients has not been reported.
Methods: A total of 996 KD patients were recruited, and the assay of TaqMan-real-time polymerase chain reaction was used for ZNF112/rs8113807 and ZNF180/rs2571051 genotyping. Odds ratio (OR) and 95% confidence interval (CI) were calculated for estimating the relationship between the polymorphisms of the both SNPs (ZNF112/rs8113807 and ZNF180/rs2571051) and the risk of IVIG resistance.
Results: Both of the ZNF112/rs8113807 CC/TC genotype and the ZNF180/rs2571051 TT/CT genotype increased the risk of IVIG resistance in KD (rs8113807: CC vs TT: adjusted OR = 1.83, 95% CI = 1.06– 3.16, p = 0.0293; CC/TC vs TT adjusted: OR = 1.49, 95% CI = 1.10– 2.02, p = 0.0094. rs2571051: TT vs CC adjusted: OR = 2.64, 95% CI = 1.62– 4.29, p < 0.0001; TT/CT vs CC adjusted: OR = 2.14, 95% CI = 1.37– 3.37, p = 0.0009; TT vs CC/CT adjusted: OR = 1.66, 95% CI = 1.22– 2.27, p = 0.0014). Furthermore, the combinative analysis of risk genotypes in ZNF112/rs8113807 and ZNF180/rs2571051 showed that patients with two unfavorable genotypes were more likely to increase risk of IVIG resistance than those who carried with zero or one unfavorable genotypes (adjusted: OR = 1.68, 95% CI = 1.24– 2.27, p = 0.0008).
Conclusion: Our findings enriched the genetic background of IVIG resistance risk in the KD development and suggested that the ZNF112/rs8113807 C-carrier and the ZNF180/rs2571051 T-carrier were associated with increased risk of IVIG resistance in KD patients in Chinese southern population.
Keywords: Kawasaki disease, ZNF112/rs8113807, ZNF180/rs2571051, IVIG resistance, inflammatory gene, polymorphism
Introduction
Kawasaki disease (KD) was an acute, self-limiting vasculitis mainly in infants and young children1–3 and due to the unknown etiology of KD, this posed a great challenge to clinical treatment. Failure to receive timely IVIG treatment and IVIG resistance (persistent or recrudescent fever at least 36 hours and <7 days after completion of first IVIG infusion4) in clinical practice were associated with increased risk of life-threatening complications.5 Such as vascular stenosis, arterial thrombosis, coronary artery disease6,7 and Kawasaki shock syndromes or KD-Macrophage activation syndrome leading to death.8,9 Research found that the incidence of IVIG resistance in children was increasing, with approximately 10–20% of patients not responding to IVIG. In recent years, studies have shown that IVIG resistance in KD patients might be related to genetic factors, among which HMGB1 and SAMD9L gene polymorphisms were related to IVIG resistance.10,11 Studies have reported that the level of IL-6 in KD patients’ serum was related to IVIG resistance, and KD patients with IVIG resistance were treated with anti-TNF -α or anti-IL-1 therapy (for their inflammation and immune response).12–14 Therefore, we speculated that some genes regulating inflammatory response might be related to IVIG resistance.
Zinc finger protein and related genes were demonstrated to play an important role in cardiovascular disease and inflammatory response. Okada et al have shown that Zinc finger transcript factor Early Growth Response gene-1 mediates inflammation from damage to blood vessels and thrombosis (KD was also vasculitis).15 Other studies have confirmed that ZNF174 affects the course of vascular injury through PDGF-B.16,17 Cattaruzza et al demonstrated the inhibitory effect of zinc finger motif-1 (ZFM1) on proinflammatory gene expression in vascular smooth muscle cells.18 Zinc finger protein 180 (ZNF180), also known as HHZ168, was a protein-coding gene that acts as a molecular regulator of immune cell infiltration in melanoma cells, enhancing CD8+T cell toxicity and negatively correlated with PAI-1 expression.19 Therefore, ZNF180 might also modulate immune cell infiltration by affecting PAI-1. At present, there were few studies on ZNF112, but many of them have shown that the ZNF family was related to inflammation, and ZNF112 (member of ZNF family) might also be involved in inflammation. In addition, studies have also shown that ZNF-related regions were associated with IVIG resistance.20 The genetic susceptibility of ZNF112 and ZNF180 gene polymorphisms in IVIG resistance in KD patients has not been studied. Therefore, in this study, we focused on whether ZNF112/rs8113807 T>C and ZNF180/rs2571051 C>T were related to IVIG resistance in KD patients from a southern Chinese population.
Materials and Methods
Study Population
A total of 996 KD patients were recruited by Department of Pediatric Cardiology of Guangzhou Women and Children’s Medical Center. The diagnosis of KD was based on guidelines issued by the American Heart Association;1,21 IVIG resistance inclusion criteria accorded that persistent or recrudescent fever at least 36 hours and less than 7 days after completion of first IVIG infusion.4,5 All parents of patients signed the informed consents. The research followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Guangzhou Women and Children’s Medical Center (2014073009, 2018052702, 2021093A01).
DNA Extraction and SNP Genotype
We selected two SNPs of ZNF112/rs8113807and ZNF180/2571051. Total genomic DNA was isolated from 200μL blood samples using TIANamp Blood DNA Kit (Tiangen, Beijing, China) according to the reagent company’s instructions. Genotyping was carried on by real-time fluorescence quantitative PCR (QuantStudio™ 6 Flex Real-Time PCR System, Thermo Fisher Scientific, CA, USA). Later, the 10% of the samples (randomly selected) were repeated genotyping, and the results were consistent to the first genotyping.
Statistical Analysis
All the statistical analysis was performed on the SAS software (version 9.4, SAS Institute, Cary, NC, United States). The differences of genotype frequencies distributions between IVIG resistance and IVIG sensitivity in the KD patients were assessed via using two-sided χ2 test. The strength of the association between rs8113807/rs2571051 polymorphisms and IVIG resistance in the KD progression was assessed by using unconditional multivariate logistic regression for calculating odds ratio (OR) and 95% confidence interval (CI), including adjustment of age and gender. Via the same statistical method, the further analysis of age/gender stratification was carried out to explore the relationship of the two SNPs’ polymorphisms and IVIG resistance in the KD progression. P-value less than 0.05 was considered statistically significant.
Analysis of Expression Quantitative Trait Loci (eQTL) and Splicing Quantitative Trait Loci (sQTL)
The expression quantitative trait loci (eQTL) and splicing quantitative trait loci (sQTL) of rs8113807 and rs2571051 were analyzed by genotype-tissue expression (GTEx) (http://www.gtexportal.org/).
Results
Characteristics of KD Patients
The characteristics of patients are presented in Table 1. In this study, 996 KD patients were recruited from Guangzhou Women and Children’s Medical Center and divided into IVIG resistance group (KD-IVIG resistance, 219 patients) and IVIG sensitivity group (KD-IVIG sensitivity, 777 patients). The age range of the KD-IVIG resistance group was 2–132 months (Mean ± SD = 25.09± 21.33), while the KD-IVIG sensitivity group was 1–131 months (Mean ± SD = 25.79± 20.61). There was no significant difference in the distributions of age (p = 0.7633) and gender (p = 0.1658) between the two groups.
 |
Table 1 Characteristics in Kawasaki Disease Patients with IVIG Resistance and Sensitive Therapy |
Association Between Selected SNP and IVIG Resistance Susceptibility in KD Patients
The genotype frequencies distributions of ZNF112/rs8113807 and ZNF180/rs2571051 in KD patients are shown in Table 2. We found that the CC/TC genotype of ZNF112/rs8113807 was a risk factor for IVIG resistance in KD patients (CC vs TT adjusted: OR = 1.83, 95% CI = 1.06–3.16, p = 0.0293; Dominant model: CC/TC vs TT adjusted: OR = 1.49, 95% CI = 1.10–2.02, p = 0.0094) and ZNF180/rs2571051 TT/CT genotype was a dangerous factor for IVIG resistance in KD patients (TT vs CC adjusted: OR = 2.64, 95% CI = 1.62–4.29, p = <0.0001; Dominant model: TT/TC vs CC adjusted: OR = 2.14, 95% CI = 1.37–3.37, p = 0.0009; Recessive model: CC/TC vs TT adjusted: OR = 1.66, 95% CI = 1.22–2.27, p = 0.0014). In the current study, via combining effect of the two risk genotypes of ZNF112/rs8113807 and ZNF180/rs2571051 genotypes, we found that there was a higher risk of IVIG resistance in patients carrying two genotypes rather than those carrying 0–1 genotypes (adjusted: OR = 1.68, 95% CI = 1.24–2.27, p = 0.0008).
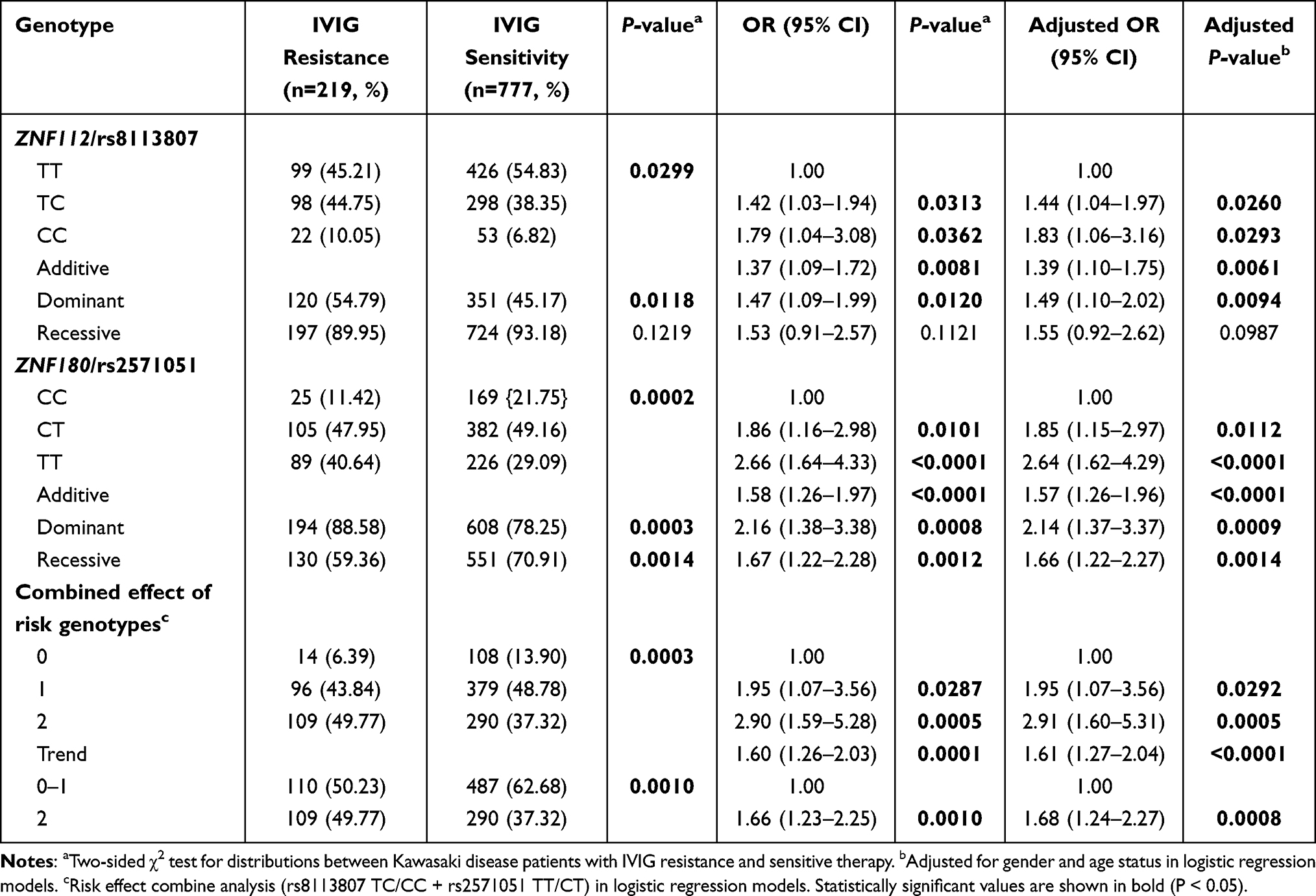 |
Table 2 Genotype Frequency Distribution of Polymorphisms in ZNF112/rs8113807 and ZNF180/rs2571051 Between KD Cases with IVIG Resistance and Sensitive Therapy |
Stratification Analysis
We conducted a stratified analysis of the risk of IVIG resistance for the two SNPs in KD patients by age and gender. The results are shown in Table 3. The results indicated that both age and gender were associated with IVIG resistance in KD patients. Compared to ZNF112/rs8113807 TT genotypes, a significantly increasing risk of IVIG resistance in KD patients carried with ZNF112/rs8113807 TC/CC genotypes was observed in children younger than 60 months of age (adjusted: OR = 1.48, 95% CI = 1.80–2.02, p = 0.0146) or female (adjusted: OR = 2.73, 95% CI = 1.47–5.07, p = 0.0015); Meanwhile, ZNF180/rs2571051 TT/CT genotypes increased the risk of IVIG resistance compared with CC genotypes in KD patients who were younger than 60 months of age (adjusted: OR = 2.13, 95% CI = 1.35–3.38, p = 0.0013) or male (adjusted: OR = 2.16, 95% CI = 1.25–3.72, p = 0.0057). Furthermore, the combined analysis of the two risk genotypes (ZNF112/rs8113807 TC/CC + ZNF180/rs2571051 TT/CT) indicated that two risk genotypes apparently increased IVIG resistance in patients younger than 60 months of age (adjusted: OR = 1.65, 95% CI = 1.21–2.25, p = 0.0017) and female (adjusted: OR = 2.83, 95% CI = 1.57–5.10, p = 0.0005).
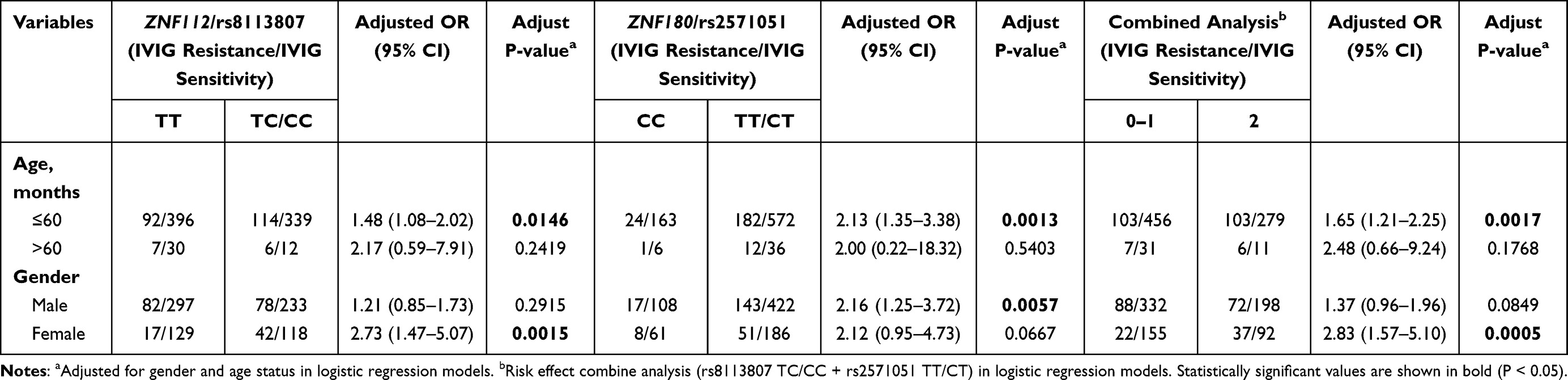 |
Table 3 Stratification Analysis of Polymorphisms in ZNF112/rs8113807 and ZNF180/rs2571051 Between KD Cases with IVIG Resistance and Sensitive Therapy |
Analysis of eQTL and sQTL
We further used GTEx database to analyze the eQTLs and sQTLs of rs2571051/rs8113807. As shown in Figure 1, rs2571051 polymorphisms was significantly associated with ZNF180 mRNA expression, meanwhile the TT genotype showed higher expression in Muscle-skeletal (P = 1.40×10−11) (Figure 1A), Thyroid (P = 1.6×10−5) (Figure 1B), Brain-Cerebellar Hemisphere (P = 2.3×10−5) (Figure 1C), and Brain-Frontal Cortex (BA9) (P = 3.6×10−5) (Figure 1D) and influenced ZNF180 splicing events in Cells-Cultured fibroblasts (P = 1.70×10−9) (Figure 1E), Vagina (P = 3.10×10−7) (Figure 1F), Artery-Tibial (P = 4.1×10−6) (Figure 1G), and Adipose-Subcutaneous (P = 5.4×10−6) (Figure 1H). We did not find any messages related to rs811380 (eQTLs or sQTLs) in GTEx database, and the relationship between rs8113807 and the expression of ZNF112 needs to be further explored.
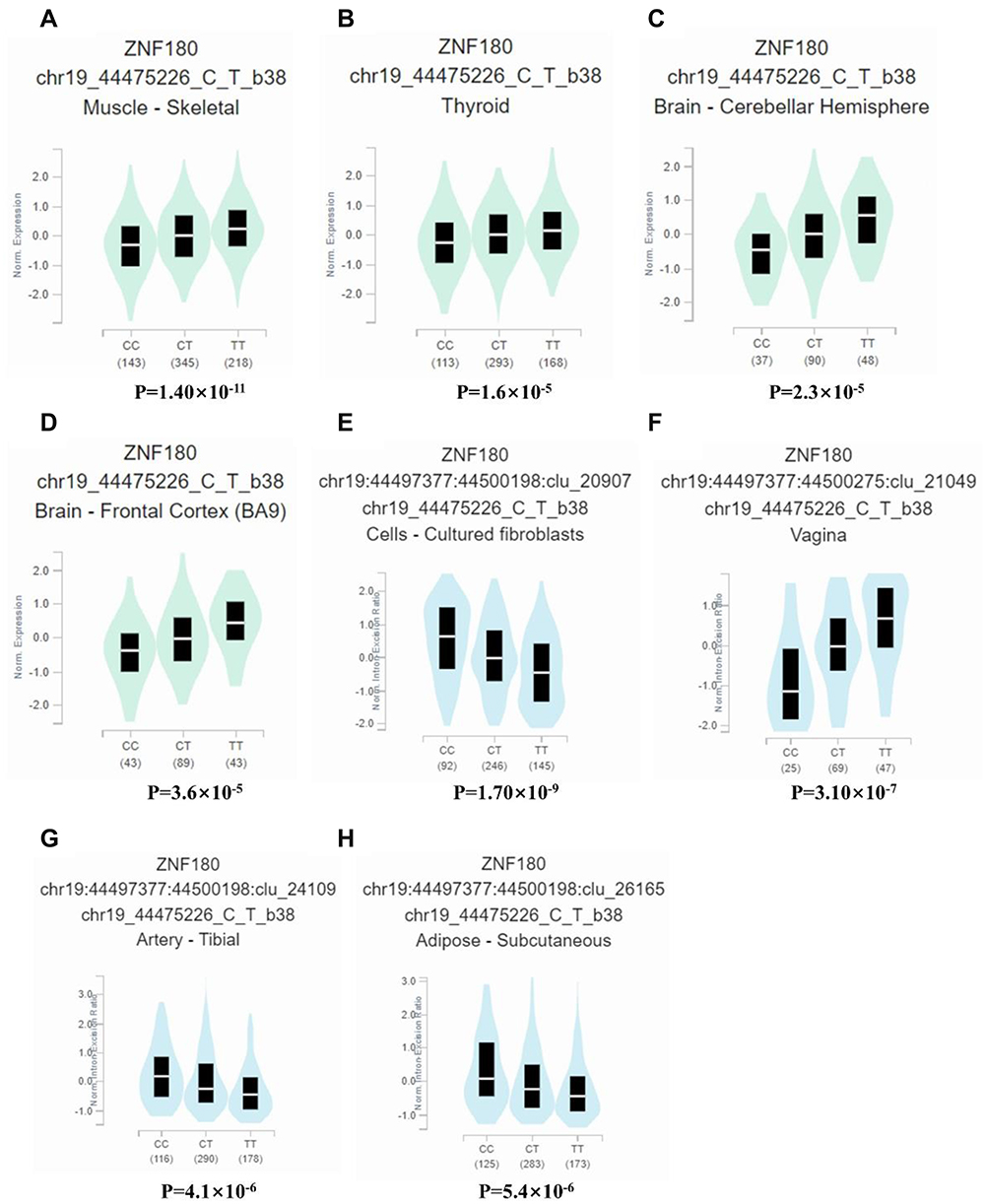 |
Figure 1 Functional relevance of rs2571051 on gene expression and splicing events in GTEx database. rs2571051 was significantly associated with ZNF180 level in the (A) Muscle-skeletal (P = 1.40×10−11), (B) Thyroid (P = 1.6×10−5), (C) Brain-Cerebellar Hemisphere (P = 2.3×10−5) and (D) Brain-Frontal Cortex (BA9) (P = 3.6×10−5); rs2571051 can affect the splicing events of (E) Cells-Cultured fibroblasts (P = 1.70×10−9), (F) Vagina (P = 3.10×10−7), (G) Artery-Tibial (P = 4.1×10−6) and (H) Adipose-Subcutaneous (P = 5.4×10−6). |
Discussion
Previous studies have indicated that 10–20% of KD patients did not respond to initial IVIG therapy, and these patients were at higher risk of developing CALs or CAA.5 The cause of non-response to IVIG therapy and the mechanism of action of IVIG therapy were still unknown. Therefore, it is important to elucidate the mechanisms to prevent the development of CALs or CAA. In this study of 219 cases in the IVIG resistance group and 777 cases in the IVIG sensitivity group, we revealed that ZNF112/rs8113807 TC/CC genotype and ZNF180/rs2571051 TT/CT genotype were associated with the incidence of IVIG resistance in KD patients. ZNF112/rs8113807 TC/CC genotype significantly increased the susceptibility of KD to IVIG resistance, and also the TT/CT genotype of ZNF180/rs2571051 was a dangerous factor of KD patients with IVIG resistance. These findings further assessed the risk of IVIG resistance in KD patients from the level of genetic variation, which might help to elucidate the mechanisms or risk factors of IVIG non-response and have the opportunity to predict the risk of IVIG resistance in KD patients.
KD was an acute vascular inflammation, and its development causes inflammatory response and the release of pro-inflammatory factors. IVIG treatment was a commonly used treatment method, and the changes in clinical patients treated with IVIG explain more about the anti-inflammatory effect. For example, Franco et al22 reported that the number of Treg cells in peripheral blood of KD patients in convalescence was increased after initial IVIG injection but was not found in the coronary arteries of patients who did not respond to IVIG therapy. This suggested that Treg regulation might play a role in the mechanism of IVIG action on KD; Shrestha et al ‘s23 newly finding indicated that the NA1 variant of FcγRIIB was associated with lack of response to IVIG. Studies have shown that the initial IVIG resistant patients with increasing risk of coronary artery anomalies occur.24,25 As a transcription factor that played a role in both inflammation and anticoagulation, many studies have confirmed that the ZNF family played an important role in the transcription regulation of various cardiovascular diseases and inflammatory responses in physiological or pathological processes. Weiss et al found that ZNF263 was a transcription inhibitor of heparin and HS-specific biosynthetic enzymes (HS3ST1 and HS3ST3A1).26 Zinc finger motif-1 (ZFM1) inhibits pro-inflammatory gene expression in vascular smooth muscle cells (SMC)18 and zinc finger protein Miz1 limited hepatocellular driven inflammation to inhibit Hepatocellular carcinoma (HCC).27 Lv et al28 demonstrated that zinc finger protein 191 (ZFP191) played a key role in proliferation and migration of aortic vascular smooth muscle cells (VSMC) through animal modeling. Some studies have confirmed that ZEB1 was associated with migration and invasion of hemangioma cells and that gene polymorphisms in the ZEB2 region were associated with the risk of coronary artery disease.29,30 According to the current studies on ZNF180, studies have shown the potential immune regulation effect and promotes the proliferation of tumor cells.19 In summary, the ZNF family was associated with cardiovascular diseases, ZNF180 was associated with inflammatory immune regulation, and IVIG treatment affects the immune response of KD patients. Although there are just few studies on ZNF112, there was a potential possibility that ZNF112 was associated with the occurrence of IVIG resistance. Therefore, in this study, we selected ZNF112/rs8113807 and ZNF180/rs2571051 as our research objects to analyze the relationship between them and patients with IVIG non-response, and achieved inspiring results. KD was an age-related disease. The incidence of KD was high in children under 5 years old, and it would be more serious in older children over 10 years old.31,32 According to the results of this study, the risk effect of ZNF112/rs8113807 TC/CC vs TT and the ZNF180/rs2571051 TT/CT vs CC were significantly associated with children younger than 5 years (≤60 months). It partly justified the prevalence of KD among children under 5 years old and explained why the condition could be severe in older children.
Disease-related SNPs in most complex diseases (such as KD) were located in non-coding sequences and were thought to affect regulatory genetic elements, resulting in changes in transcriptional activity, splicing, and epigenetic markers. Some studies have shown that eQTL was closely related to biological factors such as cell type and activation state.33,34 Genetic variations could regulate the expression of genes that affect phenotypes and susceptibility to complex diseases. In this study, the effects of rs2571051 on gene expression and splicing events were evaluated by GTEx database. The mRNA expression of rs2571051 in ZNF180 (the TT genotype presented high expression and the TT genotype was a risk factor in our study) and splicing events were found. Biologically, the changes in ZNF180 expression and splicing caused by rs2571051 may affect the regulation of immune inflammation, and then affect the treatment of IVIG in KD patients (IVIG resistance), but the specific mechanism is still unknown.
In the early years, our team has been focused on the progress of KD disease and the therapeutic effect, and achieved some exciting results. We found that single nucleotide polymorphisms (SNPs) of several genes (P2RY12, MRP4 and EIF2AK435–37) were closely associated with IVIG treatment efficacy in KD; interestingly, these genes played important roles in immune response and cardiovascular-related functions. This study was the first one to focus on the effect of ZNF family (ZNF180 and ZNF112) on IVIG treatment resistance of KD. Our findings enriched the genetic background of IVIG resistance to risk and provide new insights into the treatment of KD, which might be a predictor of IVIG resistance in KD patients.
This study is to evaluate the relationship between ZNF112 and ZNF180 polymorphisms and IVIG resistance susceptibility in KD patients, but it still had the following limitations: Firstly, the sample size of children older than 60 months is not large enough, and it should be further expanded. Future studies with larger sample size and functional experiments should be conducted to confirm the results obtained in this study. Secondly, only age and gender were considered in stratified analysis, more factors such as medical history and medication environment should be considered. Thirdly, only two SNPs (rs8113807 and rs2571051) were evaluated in this study, and more SNPs should be included in future studies.
Summary up, we found that ZNF112/rs8113807 TC/CC genotype and ZNF180/rs2571051 TT/CT genotype were the risk factors for IVIG resistance of KD in southern Chinese. The two genotypes (ZNF112/rs8113807 TC/CC + ZNF180/rs2571051 TT/CT) indicated a higher risk for children with both genotypes (versus 0–1 genotype) in children younger than 60 months.
Ethics Approval and Consent to Participate
The research followed the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of Guangzhou Women and Children’s Medical Center (2014073009, 2018052702, 2021093A01). All parents of patients knew the purpose of this study and signed informed consent forms.
Consent for Publication
All authors consent to publication.
Acknowledgments
The authors would like to thank the Clinical Biological Resource Bank of Guangzhou Women and Children’s Medical Center for providing all the clinical samples.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Guangdong Basic and Applied Basic Research Foundation (grant numbers 2021B1515230003, 2019A1515012061, 2021A1515011207, 2022A1515012558), the Guangzhou Science and Technology Program Project, China (grant numbers 201904010486, 202102010197), Postdoctoral Research Initiation Fund from Guangzhou Institute of Pediatrics, Guangzhou Women and Children’s Medical Center (grant numbers 3001162).
Disclosure
The authors report no conflicts of interest.
References
1. Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110(17):2747–2771. doi:10.1161/01.CIR.0000145143.19711.78
2. Rowley AH, Shulman ST. The epidemiology and pathogenesis of Kawasaki disease. Front Pediatr. 2018;6:374. doi:10.3389/fped.2018.00374
3. Singh S, Vignesh P, Burgner D. The epidemiology of Kawasaki disease: a global update. Arch Dis Child. 2015;100(11):1084–1088. doi:10.1136/archdischild-2014-307536
4. McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, treatment, and long-term management of Kawasaki Disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927–e999. doi:10.1161/CIR.0000000000000484
5. Phuong LK, Curtis N, Gowdie P, Akikusa J, Burgner D. Treatment options for resistant Kawasaki disease. Paediatr Drugs. 2018;20(1):59–80. doi:10.1007/s40272-017-0269-6
6. Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364(9433):533–544. doi:10.1016/S0140-6736(04)16814-1
7. Sundel RP. Kawasaki disease. Rheum Dis Clin North Am. 2015;41(1):63–73. doi:10.1016/j.rdc.2014.09.010
8. Duignan S, Doyle SL, McMahon CJ. Refractory Kawasaki disease: diagnostic and management challenges. Pediatric Health Med Ther. 2019;10:131–139. doi:10.2147/PHMT.S165935
9. Zhang RL, Lo HH, Lei C, Ip N, Chen J, Law BY. Current pharmacological intervention and development of targeting IVIG resistance in Kawasaki disease. Curr Opin Pharmacol. 2020;54:72–81. doi:10.1016/j.coph.2020.08.008
10. Ahn JG, Bae Y, Shin D, Nam J, Kim KY, Kim DS. HMGB1 gene polymorphism is associated with coronary artery lesions and intravenous immunoglobulin resistance in Kawasaki disease. Rheumatology. 2019;58(5):770–775. doi:10.1093/rheumatology/key356
11. Kim JJ, Yun SW, Yu JJ, et al. Identification of SAMD9L as a susceptibility locus for intravenous immunoglobulin resistance in Kawasaki disease by genome-wide association analysis. Pharmacogenomics J. 2020;20(1):80–86. doi:10.1038/s41397-019-0085-1
12. Garcia-Pavon S, Yamazaki-Nakashimada MA, Baez M, Borjas-Aguilar KL, Murata C. Kawasaki disease complicated with macrophage activation syndrome: a systematic review. J Pediatr Hematol Oncol. 2017;39(6):445–451. doi:10.1097/MPH.0000000000000872
13. Xie T, Wang Y, Fu S, et al. Predictors for intravenous immunoglobulin resistance and coronary artery lesions in Kawasaki disease. Pediatr Rheumatol Online J. 2017;15(1):17. doi:10.1186/s12969-017-0149-1
14. Nozawa T, Imagawa T, Ito S. Coronary-artery aneurysm in tocilizumab-treated children with Kawasaki’s disease. N Engl J Med. 2017;377(19):1894–1896. doi:10.1056/NEJMc1709609
15. Okada M, Wang CY, Hwang DW, et al. Transcriptional control of cardiac allograft vasculopathy by early growth response gene-1 (Egr-1). Circ Res. 2002;91(2):135–142. doi:10.1161/01.RES.0000027815.75000.33
16. Khachigian LM, Santiago FS, Rafty LA, et al. GC factor 2 represses platelet-derived growth factor A-chain gene transcription and is itself induced by arterial injury. Circ Res. 1999;84(11):1258–1267. doi:10.1161/01.RES.84.11.1258
17. Rafty LA, Khachigian LM. Zinc finger transcription factors mediate high constitutive platelet-derived growth factor-B expression in smooth muscle cells derived from aortae of newborn rats. J Biol Chem. 1998;273(10):5758–5764. doi:10.1074/jbc.273.10.5758
18. Cattaruzza M, Nogoy N, Wojtowicz A, Hecker M. Zinc finger motif-1 antagonizes PDGF-BB-induced growth and dedifferentiation of vascular smooth muscle cells. FASEB J. 2012;26(12):4864–4875. doi:10.1096/fj.12-210302
19. Song WM, Agrawal P, Von Itter R, et al. Network models of primary melanoma microenvironments identify key melanoma regulators underlying prognosis. Nat Commun. 2021;12(1):1214. doi:10.1038/s41467-021-21457-0
20. Kuo HC, Wong HS, Chang WP, et al. Prediction for intravenous immunoglobulin resistance by using weighted genetic risk score identified from genome-wide association study in Kawasaki disease. Circ Cardiovasc Genet. 2017;10(5). doi:10.1161/CIRCGENETICS.116.001625.
21. Singh S, Jindal AK, Pilania RK. Diagnosis of Kawasaki disease. Int J Rheum Dis. 2018;21(1):36–44. doi:10.1111/1756-185X.13224
22. Franco A, Touma R, Song Y, et al. Specificity of regulatory T cells that modulate vascular inflammation. Autoimmunity. 2014;47(2):95–104. doi:10.3109/08916934.2013.860524
23. Shrestha S, Wiener H, Shendre A, et al. Role of activating FcgammaR gene polymorphisms in Kawasaki disease susceptibility and intravenous immunoglobulin response. Circ Cardiovasc Genet. 2012;5(3):309–316. doi:10.1161/CIRCGENETICS.111.962464
24. Amano Y, Akazawa Y, Yasuda J, et al. A low-frequency IL4R locus variant in Japanese patients with intravenous immunoglobulin therapy-unresponsive Kawasaki disease. Pediatr Rheumatol Online J. 2019;17(1):34. doi:10.1186/s12969-019-0337-2
25. Uehara R, Belay ED, Maddox RA, et al. Analysis of potential risk factors associated with nonresponse to initial intravenous immunoglobulin treatment among Kawasaki disease patients in Japan. Pediatr Infect Dis J. 2008;27(2):155–160. doi:10.1097/INF.0b013e31815922b5
26. Weiss RJ, Spahn PN, Toledo AG, et al. ZNF263 is a transcriptional regulator of heparin and heparan sulfate biosynthesis. Proc Natl Acad Sci USA. 2020;117(17):9311–9317. doi:10.1073/pnas.1920880117
27. Zhang W, Zhangyuan G, Wang F, et al. The zinc finger protein Miz1 suppresses liver tumorigenesis by restricting hepatocyte-driven macrophage activation and inflammation. Immunity. 2021;54(6):1168–1185 e1168. doi:10.1016/j.immuni.2021.04.027
28. Lv L, Zhang J, Wang P, Meng Q, Liang W, Zhang L. Zinc finger protein 191 deficiency attenuates vascular smooth muscle cell proliferation, migration, and intimal hyperplasia after endovascular arterial injury. J Vasc Surg. 2014;59(2):500–509. doi:10.1016/j.jvs.2013.03.049
29. Cui S, Wang L, Zhao H, Lu F, Wang W, Yuan Z. Benzyl butyl phthalate (BBP) triggers the migration and invasion of hemangioma cells via upregulation of Zeb1. Toxicol In Vitro. 2019;60:323–329. doi:10.1016/j.tiv.2019.06.013
30. Ma L, Chandel N, Ermel R, et al. Multiple independent mechanisms link gene polymorphisms in the region of ZEB2 with risk of coronary artery disease. Atherosclerosis. 2020;311:20–29. doi:10.1016/j.atherosclerosis.2020.08.013
31. Bresson V, Bonello B, Rousset-Rouviere C, et al. Maladie de Kawasaki chez le grand enfant et l’adulte jeune: expe´rience marseillaise sur 10 ans. Arch Pediatr. 2011;18(7):731–736. French. doi:10.1016/j.arcped.2011.04.014
32. Cai Z, Zuo R, Liu Y. Characteristics of Kawasaki disease in older children. Clin Pediatr. 2011;50(10):952–956. doi:10.1177/0009922811409027
33. Fairfax BP, Humburg P, Makino S, et al. Innate immune activity conditions the effect of regulatory variants upon monocyte gene expression. Science. 2014;343(6175):1246949. doi:10.1126/science.1246949
34. Fairfax BP, Makino S, Radhakrishnan J, et al. Genetics of gene expression in primary immune cells identifies cell type-specific master regulators and roles of HLA alleles. Nat Genet. 2012;44(5):502–510. doi:10.1038/ng.2205
35. Wang Y, Xu Y, Huang P, et al. Homozygous of MRP4 gene rs1751034 C allele is related to increased risk of intravenous immunoglobulin resistance in Kawasaki disease. Front Genet. 2021;12:510350. doi:10.3389/fgene.2021.510350
36. Wang Z, Xu Y, Zhou H, et al. Association between P2RY12 gene polymorphisms and IVIG resistance in Kawasaki patients. Cardiovasc Ther. 2020;2020:3568608. doi:10.1155/2020/3568608
37. Yu H, Liu F, Chen K, et al. The EIF2AK4/rs4594236 AG/GG genotype is a hazard factor of immunoglobulin therapy resistance in southern Chinese Kawasaki disease patients. Front Genet. 2022;13:868159. doi:10.3389/fgene.2022.868159
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.