")
Back to Journals » Drug Design, Development and Therapy » Volume 17
The Application of Dupilumab to Pediatric Patients Aged 6–11yrs with Moderate-to-Severe Atopic Dermatitis Whose Disease is Not Adequately Controlled: The Clinical Data so Far
Authors Balboul S, Kahn J, Tracy A, Peacock A, Cline A
Received 1 March 2023
Accepted for publication 21 April 2023
Published 1 May 2023 Volume 2023:17 Pages 1323—1327
DOI https://doi.org/10.2147/DDDT.S281626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Sarah Balboul,1 Julia Kahn,1 Alexis Tracy,2 Anjelica Peacock,3 Abigail Cline2– 4
1School of Medicine, New York Medical College, Valhalla, NY, USA; 2Department of Dermatology, New York Medical College, Valhalla, NY, USA; 3Department of Dermatology, Metropolitan Medical Center, New York, NY, USA; 4Department of Dermatology, Lincoln Medical Center, Bronx, NY, USA
Correspondence: Abigail Cline, Email [email protected]
Background: While dupilumab has shown efficacy in improving atopic dermatitis, few studies have assessed the long-term clinical data of dupilumab use in pediatric patients.
Objective: In the present study, we reviewed the current literature to assess reported efficacies, side effects, and risks of using dupilumab to treat atopic dermatitis in pediatric populations.
Methods: Using PRISMA guidelines, the authors searched PubMed/MEDLINE and Embase for studies related to dupilumab treatment for atopic dermatitis in pediatric patients aged 6– 11 years old.
Results: A total of 512 pediatric patients (ages 6– 11) were included. Outcome measures assessed by EASI, SCORAD, P-NRS, IGA and C-DLQI showed significant improvements in scores from those observed at baseline to the last treatment of dupilumab. Most reported adverse effects on dupilumab were conjunctivitis and infection site reactions. All studies reported that dupilumab was well-tolerated.
Limitations: Limitations include the low number of studies available and observation periods of up to 16 weeks, which may be too short to evaluate the drug’s effectiveness and occurrence of adverse effects. This also limits our knowledge on whether there are sustained benefits and/or diminished efficacy as well as long-term side effects.
Conclusion: Thus far, the data demonstrates dupilumab to be safe and effective in the management of moderate-to-severe atopic dermatitis in children aged 6– 11 years. Future studies should evaluate long-term dupilumab use and sustained effects.
Keywords: pediatric, pediatric dermatology, atopic dermatitis, dupilumab
Introduction
Atopic dermatitis (AD) is one of the most common inflammatory skin diseases affecting approximately 15–25% of children.1 It is characterized by outbreaks of pruritic skin lesions and xerosis that classically manifest in early childhood.2 Comorbid conditions including asthma, food allergies, eosinophilic esophagitis, sleep impairment, as well as mental health and behavioral problems that negatively impact the quality of life of both those affected and their families.3 Food allergies and eosinophilic esophagitis are early components of atopic march, where such cutaneous manifestations may precede the onset of secondary pathologies and dermatologists represent the sentinels for the early identification of this group of patients with AD.4 Significant medical, personal, societal, and financial burdens are also associated with AD. Estimated annual costs for families to care for a child with AD are comparable to those of a child with insulin-dependent diabetes and much higher than those of a child with asthma.5 AD can be difficult to treat, however, there are a number of available treatment options that aim to reduce symptoms, prevent exacerbations, and minimize therapeutic risks.1
Initial treatment for pediatric AD consists mostly of topical emollients and corticosteroids (TCs).6 TCs are typically well-tolerated medications when used properly; however, TCs pose higher risks in the pediatric population given increased absorption due to a higher body surface area-to-weight ratio.1,6 Alternative treatments include topical calcineurin inhibitors (TCIs), particularly for sensitive skin sites such as the face and skin folds. While TCIs have the advantage of not imposing risk for cutaneous atrophy, TCIs are not as effective as TCs and are more costly.1 Although phototherapy is another treatment option available, it is not commonly used in pediatric populations as it requires biweekly visits to the doctor’s office and not all healthcare facilities have access to the equipment.1 Systemic corticosteroids and off-label drugs (cyclosporine, methotrexate, azathioprine) can also be used, but management with these is challenging. These medications require forewent lab morning, increase the risk of systemic adverse effects, and are not recommended for long-term use.7,8
Emerging drug therapies for AD target its immune response elements. AD is characterized by an immune response that increases the expression of cytokines IL-4-, IL-13, and IL-5 secreted from Th2 helper T-cells. Dupilumab is a fully human monoclonal antibody that blocks the shared receptor for IL-4 and IL-13, thereby blocking the signaling cascade for these cytokines.9 Dupilumab is approved for the treatment of moderate-to-severe AD, and has been shown to improve AD symptoms and quality of life with an acceptable safety profile.10 Given the majority of patients suffering from AD are children, dupilumab holds great promise in providing a safe, effective therapy for pediatric patients. At present, there are few studies evaluating the long-term clinical data of dupilumab use in pediatric patients aged 6–11 years with moderate-to-severe atopic dermatitis. The most prevalent side effects of dupilumab included conjunctivitis, nasopharyngitis, headaches, and injection-site reaction.11–14 This study aims to investigate the current literature and further compare the use of dupilumab to leading treatments in terms of efficacy, side effects, and risks.
Methods
A systematic literature search of PubMed/MEDLINE and Embase was conducted using the following terms: “atopic dermatitis”, “eczema”, “children”, “pediatric patients”, “Dupixent”, “dupilumab”. Terms were combined using appropriate Boolean operators. No limitations in language, publication type, or publication period were applied.
This systematic review was performed in accordance with guidelines provided by Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist. The inclusion criteria were: (1) studies looking at patients who were between the ages of 6 and 11 years old, (2) the article was a randomized controlled trial or clinical review. The following exclusion criteria were then applied: (1) the article was not in English (or no English-translated versions were available from the publisher), (2) the article was a conference abstract, letter, or note, (3) studies looking at the infant, adolescent, or adult populations. Ultimately, four studies met all criteria and were used for analysis. The reporting of this systemic review was guided by the standards of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Statement (Supplement 1).
Results
The four trials included a total of 512 patients whose detailed characteristics (Table 1). All trials administered dupilumab using subcutaneous injection. Treatment groups received dupilumab monotherapy in two trials12,13, while the other two by Paller et al and Yang et al included patients applying concomitant TCs.14,15 Measures used to assess disease severity in these studies included the Eczema Area Severity index (EASI), SCORing Atopic Dermatitis (SCORAD), and Investigator’s Global Assessment (IGA). Three of the studies included patient reported outcomes such as the Dermatology Life Quality Index (DLQI) and the Pruritic Numeric Rating Scale for itch (P-NRS). Change in mean EASI score from baseline to the final 16th week of treatment showed significant improvement for the following studies; Paller (p < 0.0001); Napolitano (p < 0.001); Yang (p < 0.001). Significant improvements in average SCORAD were reported by; Paller (p < 0.0001); Yang (p < 0.0001); Losek (p < 0.0001). Similarly, improvements in patient reported outcomes assessed by DQLI and P-NRS were significant; Paller (DQLI p < 0.0001, P-NRS p < 0.0001); Napolitano (DQLI p < 0.0001, P-NRS p < 0.001); Yang (DQLI p < 0.001). Rate of adverse effects on dupilumab was generally low, however, the most reported were conjunctivitis and injection site reactions. All studies reported that dupilumab was well-tolerated.
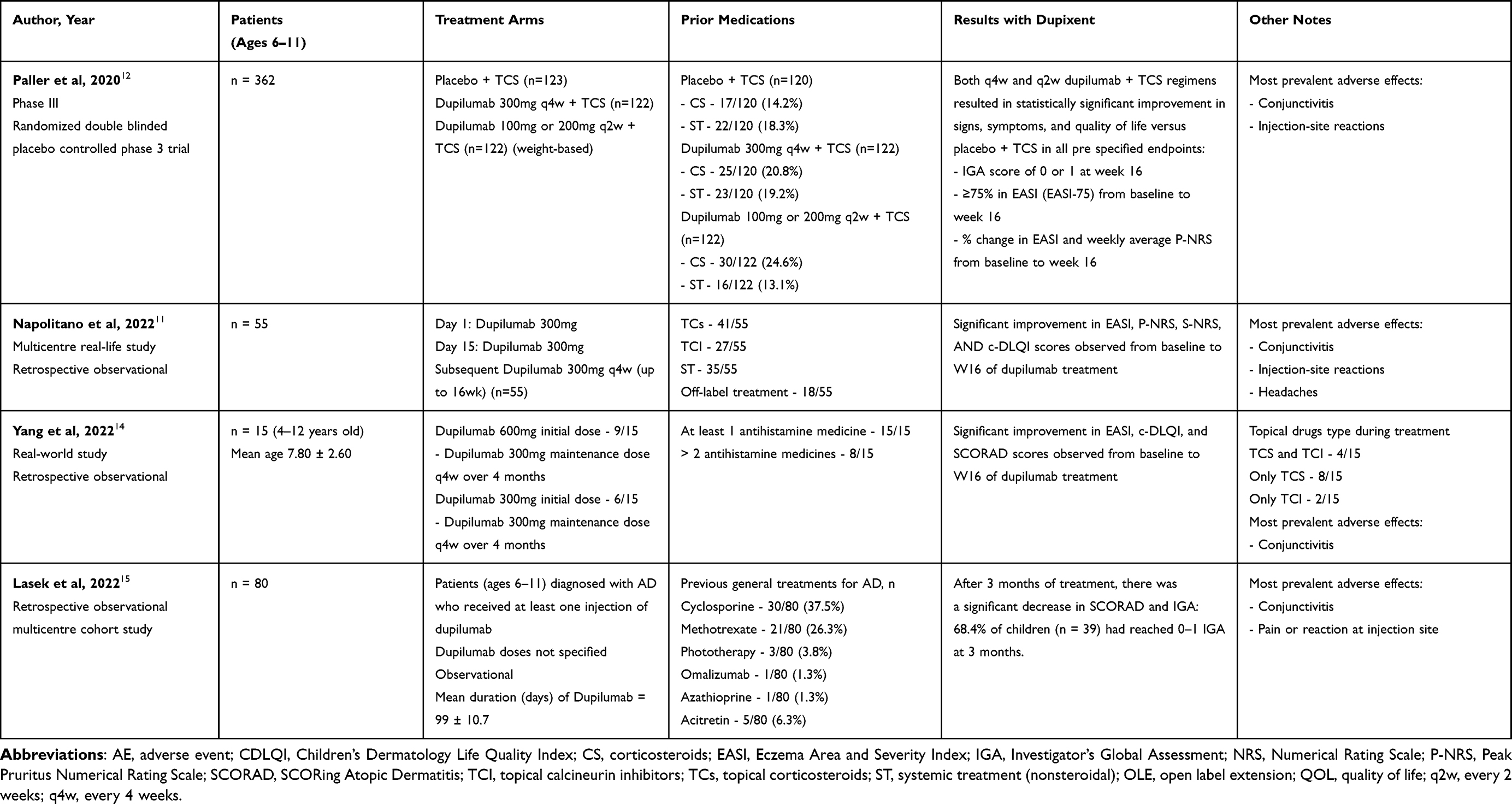 |
Table 1 Characteristics of Studies Included |
Discussion
Our findings demonstrate that the use of dupilumab improves symptoms and quality of life in children aged 6–11 years with moderate-to-severe AD. All scoring metrics used to assess disease severity and impact showed statistically significant improvement for patients given dupilumab when compared to baseline before starting treatment. Most children achieved mild or absent pruritus and improvement of severity or extent of AD, as measured through P-NRS, EASI, SCORAD, and IGA, by the end of the specified treatment period. By reducing pruritic skin lesions, dupilumab resulted in improved quality of life for these children as measured through c-DLQI.11,12,14,15
Of the studies included, no patients discontinued dupilumab due to severe treatment-emergent adverse events (TEAEs) related to dupilumab. Most prevalent side effects included conjunctivitis, nasopharyngitis, headaches, and injection-site reaction. While conjunctivitis was the most frequent side effect of dupilumab, most cases were of mild-to-moderate severity, resolved during treatment, and did not lead to discontinuation of treatment. Overall, dupilumab was well-tolerated and had an acceptable safety profile across all studies.11,12,14,15
This review has some limitations. Results were limited due to the low number of studies available. Additionally, observation periods for most of the included studies were up to 16 weeks, which may be too short to evaluate the drug’s effectiveness and occurrence of adverse events. The treatment arms used in the study by Paller et al 2020 included concurrent TC use in addition to dupilumab in both the control group and groups receiving dupilumab. While results from this study highlight dupilumab’s efficacy in treating pediatric AD, it is important to consider this variation in treatment arms when comparing results between the different studies reviewed.
These results support the use of dupilumab as a safe treatment for children aged 6–11 years with moderate-to-severe AD. Among all studies included, dupilumab results in clinically and statistically significant improvements in EASI, SCORAD, P-NRS, IGA, and c-DLQI. Dupilumab is shown to be effective for use in pediatric patients and improves the intensity of AD symptoms and quality of life, with a favorable safety profile and no severe adverse events such as serious infection or systemic hypersensitivity.
Conclusion
AD is a complex disorder that poses a significant financial burden and a negative impact on quality of life on those affected. Traditional treatment modalities can be difficult to access and can pose side effects with long-term use. This review demonstrates that dupilumab is an effective treatment for moderate-to-severe AD that improves both AD symptoms and quality of life. The adverse effects of dupilumab were not severe enough to discontinue treatment and were generally well-tolerated among the patients in each of the studies.
Results were limited due to the low number of studies available and the short-term observation period of 16 weeks in most studies included. As the use of dupilumab becomes more common, futures studies can evaluate long-term use in pediatric populations.
IRB Status
Exempt.
Funding
There is no funding to report.
Disclosure
There are no conflicts or competing interests to disclose.
References
1. Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116–132. doi:10.1016/j.jaad.2014.03.023
2. Goh MS, Yun JS, Su JC. Management of atopic dermatitis: a narrative review. Med J Aust. 2022;216(11):587–593. doi:10.5694/mja2.51560
3. Huang AH, Roh YS, Sutaria N, et al. Real-world comorbidities of atopic dermatitis in the pediatric ambulatory population in the United States. J Am Acad Dermatol. 2021;85(4):893–900. doi:10.1016/j.jaad.2021.03.016
4. Russo F, Santi F, Cioppa V, et al. Meeting the needs of patients with atopic dermatitis: a multidisciplinary approach. Dermatitis. 2022;33(6s):S141–S143. doi:10.1097/der.0000000000000907
5. Su JC, Kemp AS, Varigos GA, et al. Atopic eczema: its impact on the family and financial cost. Arch Dis Child. 1997;76(2):159–162. doi:10.1136/adc.76.2.159
6. Napolitano M, Fabbrocini G, Martora F, et al. Children atopic dermatitis: diagnosis, mimics, overlaps, and therapeutic implication. Dermatol Ther. 2022;35(12):e15901. doi:10.1111/dth.15901
7. Drucker AM, Eyerich K, de Bruin-Weller MS, et al. Use of systemic corticosteroids for atopic dermatitis: international eczema council consensus statement. Br J Dermatol. 2018;178(3):768–775. doi:10.1111/bjd.15928
8. Smith Begolka W, Chovatiya R, Thibau IJ, et al. Financial burden of atopic dermatitis out-of-pocket health care expenses in the United States. Dermatitis. 2021;32(1s):S62–S70. doi:10.1097/der.0000000000000715
9. Gittler JK, Krueger JG, Guttman-Yassky E. Atopic dermatitis results in intrinsic barrier and immune abnormalities: implications for contact dermatitis. J Allergy Clin Immunol. 2013;131(2):300–313. doi:10.1016/j.jaci.2012.06.048
10. Simpson EL, Paller AS, Siegfried EC, et al. Efficacy and safety of dupilumab in adolescents with uncontrolled moderate to severe atopic dermatitis: a phase 3 randomized clinical trial. JAMA Dermatol. 2020;156(1):44–56. doi:10.1001/jamadermatol.2019.3336
11. Napolitano M, Fabbrocini G, Neri I, et al. Dupilumab treatment in children aged 6–11 years with atopic dermatitis: a multicentre, real-life study. Paediatr Drugs. 2022;24(6):671–678. doi:10.1007/s40272-022-00531-0
12. Paller AS, Siegfried EC, Thaçi D, et al. Efficacy and safety of dupilumab with concomitant topical corticosteroids in children 6 to 11 years old with severe atopic dermatitis: a randomized, double-blinded, placebo-controlled phase 3 trial. J Am Acad Dermatol. 2020;83(5):1282–1293. doi:10.1016/j.jaad.2020.06.054
13. Thaçi D, Simpson EL, Beck LA, et al. Efficacy and safety of dupilumab in adults with moderate-to-severe atopic dermatitis inadequately controlled by topical treatments: a randomised, placebo-controlled, dose-ranging phase 2b trial. Lancet. 2016;387(10013):40–52. doi:10.1016/S0140-6736(15)00388-8
14. Yang D-Y, Li L, Lu T, et al. Efficacy and safety of dupilumab in pediatric patients with moderate to severe atopic dermatitis: a real-world study. Arch Dermatol Res. 2022;315:1–6.
15. Lasek A, Bellon N, Mallet S, et al. Effectiveness and safety of dupilumab in the treatment of atopic dermatitis in children (6–11 years): data from a French multicentre retrospective cohort in daily practice. J Eur Acad Dermatol Venereol. 2022;36(12):2423–2429. doi:10.1111/jdv.18450
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.