")
Back to Journals » Clinical Ophthalmology » Volume 15
The Antibacterial Comparison of 5% and 2.5% Povidone Iodine to 0.01% Hypochlorous Acid Using Corneoscleral Tissue as a Solid-Phase Medium
Authors Kowalski R , Kamyar R, Rhee M, Mammen A, Dhaliwal D, Romanowski EG , Jhanji V, Eller AW
Received 15 July 2021
Accepted for publication 23 August 2021
Published 1 September 2021 Volume 2021:15 Pages 3697—3704
DOI https://doi.org/10.2147/OPTH.S328696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Regis Kowalski,1 Roheena Kamyar,1 Michelle Rhee,2 Alex Mammen,1 Deepinder Dhaliwal,1 Eric G Romanowski,1 Vishal Jhanji,1 Andrew W Eller1
1University of Pittsburgh Medical Center (UPMC), The Charles T. Campbell Ophthalmic Microbiology Laboratory, Department of Ophthalmology, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA; 2The Eye-Bank for Sight Restoration, New York, NY, USA
Correspondence: Regis Kowalski
The Charles T. Campbell Ophthalmic Microbiology Laboratory at the University of Pittsburgh School of Medicine, The Eye and Ear Institute, 203 Lothrop Street, Pittsburgh, Pa, 15213, USA
Tel +1 412-647-7211
Email [email protected]
Purpose: Prophylactic topical antiseptics used to eliminate bacteria on the ocular surface prior to ocular surgery should be both effective and non-irritating. Five percent povidone iodine (PI) is an accepted antiseptic used for prophylaxis. Dilute 2.5% PI and 0.01% hypochlorous acid (HOCl) may be more patient comfortable and equally effective. PI at 5% and 2.5% were compared to HOCl against a battery of bacterial endophthalmitis isolates using corneoscleral tissue as a solid-phase medium to determine antiseptic efficacy.
Methods: Bacteria from 20 cases of endophthalmitis were tested for the elimination of growth against topical 5% PI, 2.5% PI, HOCl, and no antiseptic using donor corneoscleral tissue. The tissue was inoculated with 103 colony forming units of bacteria prior to a 3-minute contact time with the antiseptics, placed in liquid growth medium, and monitored for growth at three days. No growth indicated antiseptic treatment success. Differences were analyzed using Chi square (χ 2).
Results: For 20 isolates, 5% PI was comparable to 2.5% PI for preventing bacteria growth (p=0.71), and both were more effective than HOCl (p=0.004). Estimated weighted comparison over a 27-year period indicated that for all bacterial groups, except Streptococcus viridans, 5% PI was equally effective to 2.5% PI for preventing bacterial growth (p=1.0). For Streptococcus viridans, 5% PI was more effective than 2.5% PI (p=0.0001). Both concentrations of PI were more effective than HOCl (p=0.00001).
Conclusion: Five percent PI appears to be optimal as a prophylaxis prior to ocular surgery.
Keywords: povidone iodine, hypochlorous acid, endophthalmitis prophylaxis, intravitreal injection, corneoscleral tissue, antiseptic susceptibility
Introduction
Endophthalmitis after intravitreal injection is a rare but severe complication. Unlike endophthalmitis after cataract surgery, each patient has multiple chances of intraocular infection. Patients often require monthly injections of anti-vascular endothelial growth factor (VEGF) to control age-related macular degeneration (AMD), diabetic macular edema (DME), and retinal vein occlusion (RVO).1 Even oral flora spread through speech has been implicated as a vector for intraocular infection.2 The rate of endophthalmitis after intravitreal injections has been reported by Gregori3 to be 0.02% to 0.5%, McCannel5 0.025% (based on 26 culture positive cases out of 105,536 injections), and Merani5 0.028%. Cheung6 reported the endophthalmitis rate after intravitreal injection of steroids was higher than the intravitreal injection of VEGF. Grzybowski7 reported that 5.9 million intravitreal injections were administered in the US during 2016.
Ophthalmologist has turned to antiseptics instead of antibiotics for surgical prophylaxis, which includes intravitreal prophylaxis, because of the potential of acquired resistance due to frequent antibiotic application.8 The prophylaxis consensus prior to intravitreal injection and other ocular surgeries is the application of the antiseptic, 5% povidone iodine (PI), to the ocular surface and the clearance of the eyelid and lashes from the injection site.9,10 PI is a composite of elemental iodine, hydrogen iodine, and povidone.11 It is an antibacterial broad-spectrum, in which free iodine is the active component, and it has minimal residual activity. It can be an irritant when left on tissue surfaces for a long time. The stinging and burning nature of 5% PI has prompted retinal specialists, especially in cases of multiple intravitreal injections, and other ocular surgeons to seek other effective prophylactic measures. This includes lower dilutions of PI and 0.01% hypochlorous acid (HOCl). It has been reported that PI at lower concentrations may be as active as higher concentrations due to the release of free iodine.12–14 Hypochlorous acid is a strong oxidizing agent used in the hospital setting as a cleaning and disinfecting agent.15 At a neutral pH of 7.0, it is non-toxic and leaves no residual. (Infection Control Today.com/view/hypochlorous-acid-definitive-terminal-cleaning-hospital-environment) (Dimmitt D, June 9, 2014) (accessed 01/14/2021). HOCl has been marketed (NovaBay Pharmaceuticals Inc, Emeryville, CA) (www.avenova.com/hypochlorous/acid) for eyelid hygiene and eye health to reduce bacteria that may cause blepharitis and exasperate dry eye. It has no indication for prophylaxis and contact with the ocular surface.
In two previous in vitro studies, we compared 5% PI and 0.01% HOCl. In the Chronister study,16 we found 5% PI to be more effective than HOCl (Sterilid®) (HOCl spray foam that contains tea tree oil). Using a liquid formulation of hypochlorous acid, Klocek17 demonstrated similar activity between 5% PI and 0.01% HOCl (Avenova®), but the bactericidal effect by 0.01% HOCl was reduced from 2 to 1 minute. In an eyelid study by Gonzalez18 on volunteers, with 5% PI applied to one eyelid and 0.01% HOCl (Avenova®) applied to the other eyelid, the reduction of bacterial flora was equivalent. It must be noted that Kanclerz compared 10% PI to HOCl for cataract surgery prophylaxis. They found conjunctiva lavage with 10% PI decrease bacterial load and HOCl did not. HOCl was more comfortable to the patient and no endophthalmitis was noted for either treatment group.19
The present unique study utilizes corneoscleral tissue to evaluate antiseptic susceptibility on a solid phase medium. The corneoscleral tissue would be a better reality assimilation of the ocular surface than bacterial dispersion in a liquid medium. The antiseptics would be tested against a panel of bacterial endophthalmitis isolates. The design of the study was to eliminate bacteria and not demonstrate a reduction, because dead bacteria do not cause infection. We hypothesize that 5% PI, 2.5% PI and HOCl will prevent equally bacterial growth within the recommended time frame of 3 minutes (Betadine packet insert®). Analysis will include a projected weighted comparison over a 27-year period.
Methods
Bacterial Endophthalmitis Isolates
Twenty bacterial endophthalmitis isolates were tested for this study: 1) Staphylococcus aureus (Sa) E904, 2) coagulase negative Staphylococcus (CNS) E820, E923, E922, and E 920, 3) Enterococcus faecalis (Ef) E913, 4) Streptococcus viridans group (Sv) (also referred to some as viridans Streptococcus) E927, E926, E919, and E910, 5) Beta-hemolytic Streptococcus E819 (Beta-Strep,) 6) Pseudomonas aeruginosa (Pa) E915, 7) Serratia marcescens (Sm) E886), 8) Bacillus cereus (Bc) E776, 9) Methicillin Resistant Staphylococcus aureus (MRSA) E897, 10) Streptococcus pneumoniae (Sp) E891, E845, E737, E709, and 11) Haemophilus influenzae (Hi) E789. Single isolates of the 11 groups were initially tested. Antiseptic resistance was noted for the single isolates of CNS, Sv, and Sp. It was decided to test three additional isolates for these groups to determine whether there was consistent resistance. All isolates were stocked in a clinical tissue bank, de-identified for patient identification, and were used to support antibiotic susceptibility validation and laboratory certification. The 20 isolates were selected from a collection of 689 isolates that included intraocular infection due to intravitreal infection, surgery, trauma, and an endogenous route.20 The number of endophthalmitis cases due to intravitreal injection could not be precisely deduced.
For testing, the bacterial isolates were retrieved from frozen stocks (−80O C) and grown overnight on trypticase soy agar plates supplemented with 5% sheep’s blood (Becton, Dickinson, and Company, Sparks, MD). The following day, the bacterial isolates were suspended in 5 mL of saline to a 0.5 McFarland standard which corresponded to a growth of approximately 1×108 CFU/mL. Colony counts were determined by plating serial dilutions of the suspension. The dilutions were 10−2, 10−3, 10−4, 10−5, and 10−6. The 10−3 dilution would contain approximately 1×105 colony forming units (CFU) per mL of bacteria. A 0.01 mL (10 µL) sample of this would contain 103 CFU of bacteria. This was the inoculum aliquoted to the corneal tissue in this experiment.
Human Corneoscleral Tissue
Excess corneoscleral donor tissues (rims) were used to test susceptibility in this study as a solid phase instead of using liquid media. In general, the rims were excess tissue received from corneal surgeons after keratoplasty surgery and not from the eye bank. Corneoscleral rims were cultured for microbial contamination after keratoplasty by placing the rims in 10 mL of enriched thioglycollate broth (BBL™, Becton, Dickinson and Co., Sparks, MD). After 5 days of incubation at 37O C, the culture-negative rims were removed from the enriched thioglycollate broth and soaked in 50 mL of PBS (phosphate buffered saline) for 72 hours to elute any inhibitory factors (ie gentamicin as part as Optisol-GS®). The rims were stored at −80°C for research purposes in a clinical tissue bank. In addition, whole corneas deemed not suitable for surgical use, but biologically safe research tissue, were donated by the Eye Bank (The CORE Eye Bank of Pittsburgh Pennsylvania). These corneas were also cultured for bacteria and fungi, eluted in 50 mL of PBS for 72 hours, and stored at −80°C. It must be re-emphasized that we only controlled for inhibitory factors that could inhibit bacterial growth.
Antiseptics
Five percent povidone iodine (pH= 4.0) (Betadine, Alcon, Fort Worth, TX) (Lot #KWB002) and 0.01% hypochlorous acid (pH=3.78) (Avenova, NovaBay Pharmaceuticals, Emeryville, CA) (Lot # 57653) were purchased for this study. Five percent PI was diluted 1:2 in phosphate buffer saline (pH 7.2, Gibco, Grand Island, NY) to make 2.5% PI (pH=5.34).
Experimental Protocol
The retrospective study did not require an Institutional Review Board/Ethics committee approval because direct patient contact and personal information were not involved. The CORE Eye Bank of Pittsburgh Pennsylvania has given permission for the research use of these excess corneal tissues. Figure 1 is a diagram detailing the experimental steps for the elimination of bacteria attached to corneoscleral tissue by topical antiseptics.
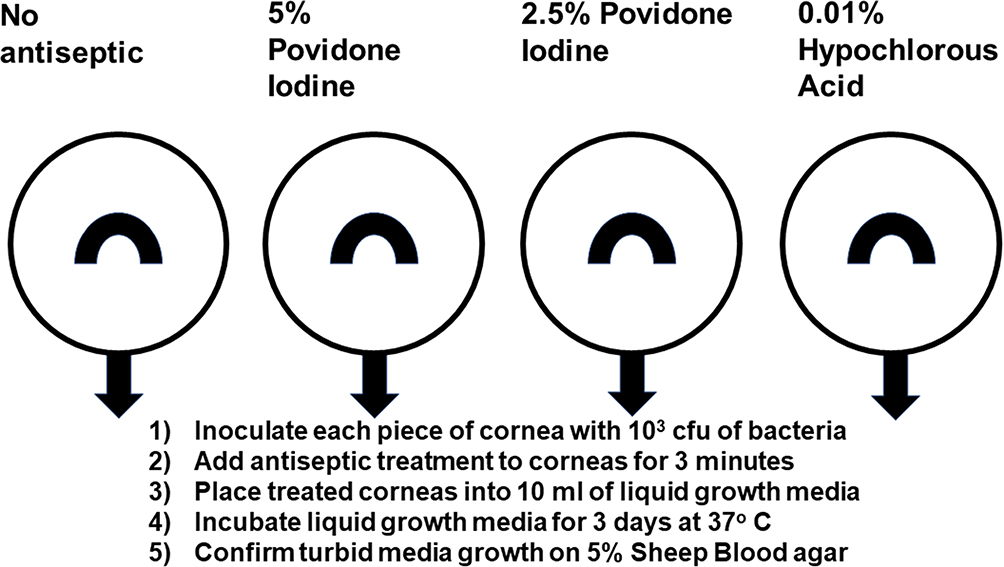 |
Figure 1 Diagram detailing the experimental steps for the elimination of bacteria attached to corneoscleral tissue by topical antiseptics. |
2. 103 CFU of bacteria in a 10 µL volume was placed on each quarter of corneal tissue.
“a” was the untreated control (no antiseptic),
“b” was treated with 5% PI,
“c” was treated with 2.5% PI, and
“d” was treated with 0.01% HOCl.
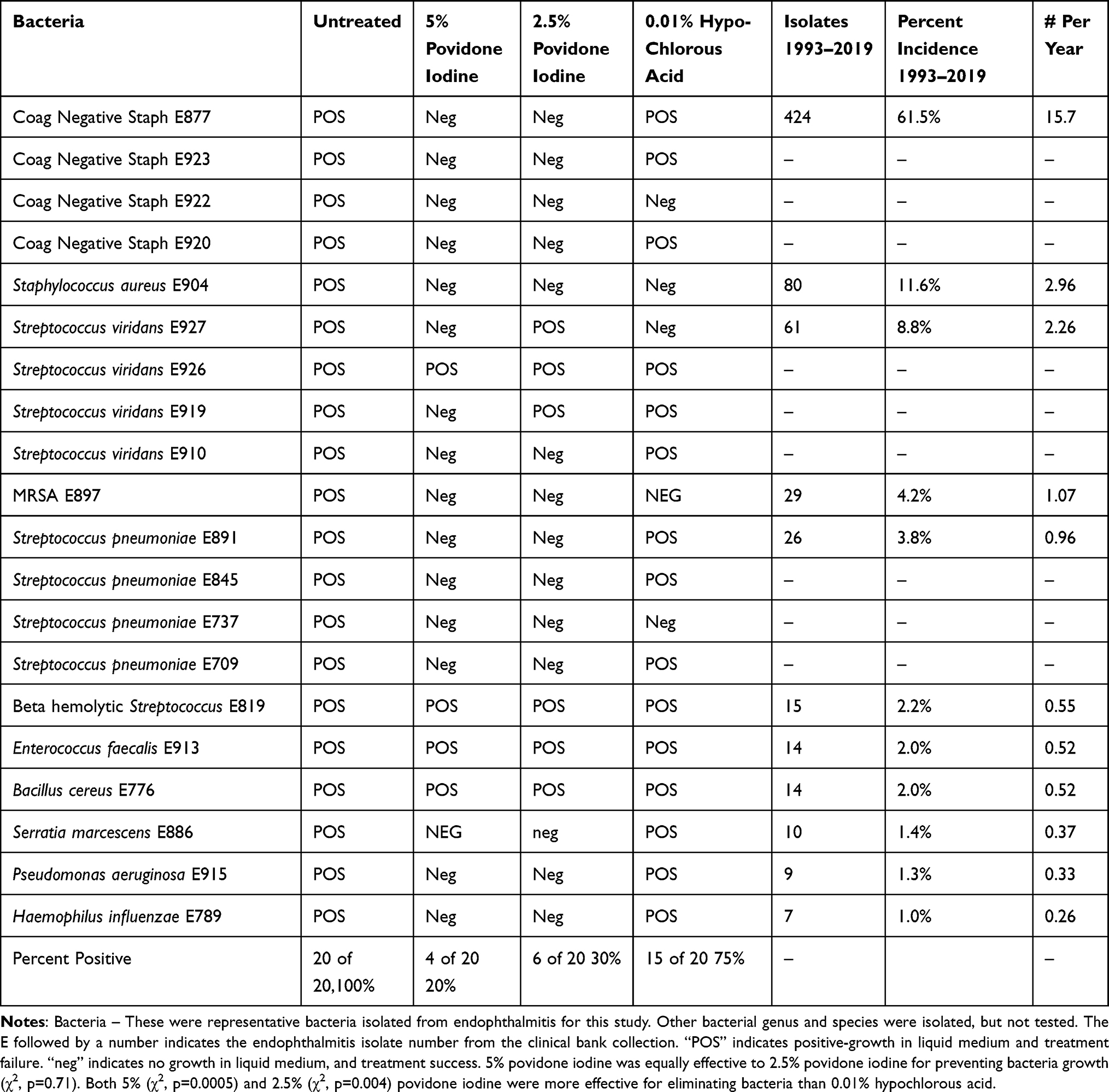 |
Table 1 Comparison of 5% and 2.5% Povidone Iodine Antibacterial Efficacy to 0.01% Hypochlorous Acid Using Bacteria Isolated from Endophthalmitis. Corneoscleral Tissue Was Used as a Solid-Phase Medium to Assimilate the Ocular Surface. Prevention of Bacterial Growth After Antiseptic Application Indicated Success of the Antiseptic |
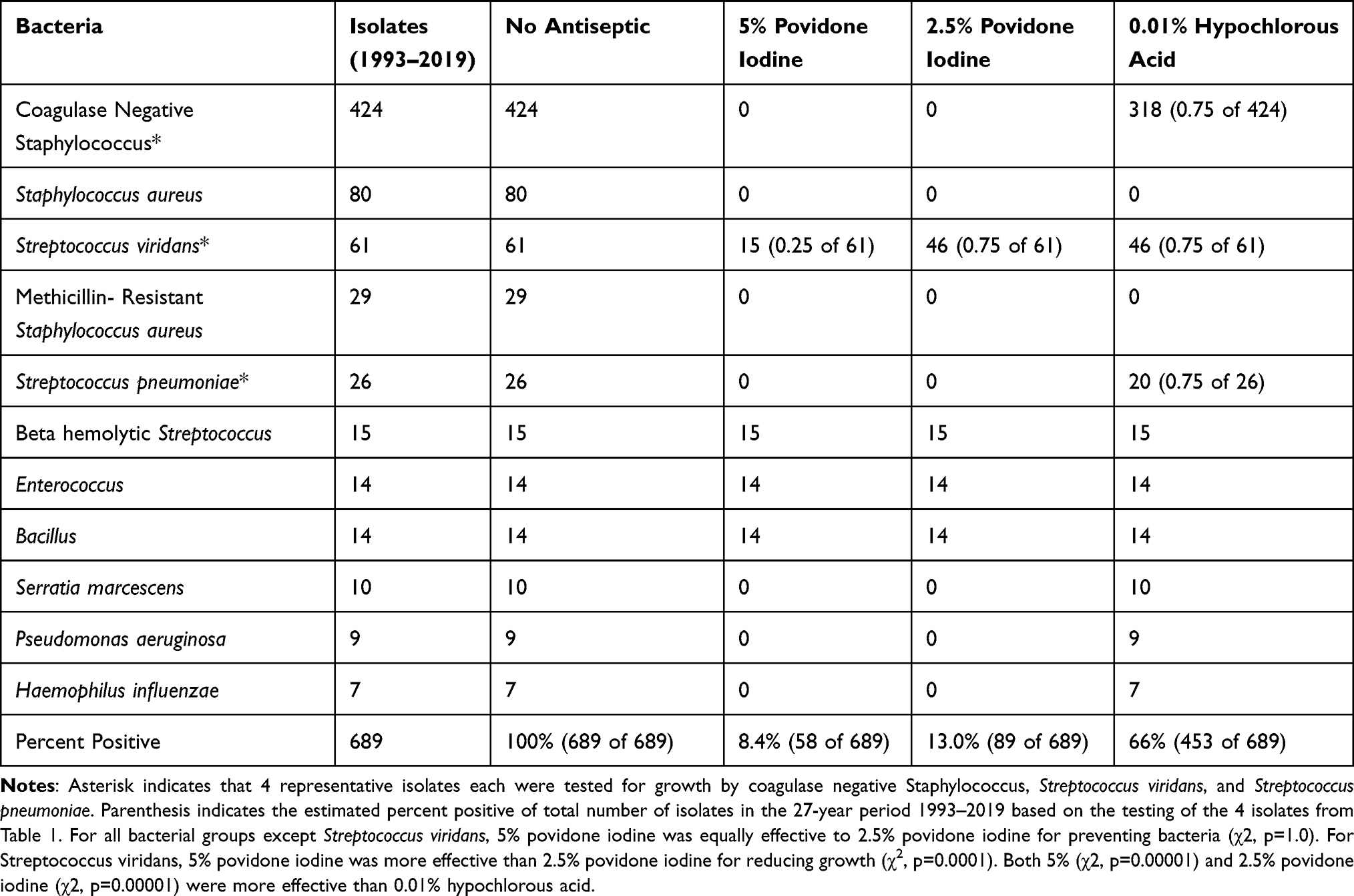 |
Table 2 Weighted Comparison of 5% and 2.5% Povidone Iodine Antibacterial Activity to 0.01% Hypochlorous Acid Based on Bacteria Isolated from Endophthalmitis Over a 27-Year Period (1993–2019). Corneoscleral Tissue Was Used as a Solid-Phase Medium to Assimilate the Ocular Surface. Prevention of Bacterial Growth After Antiseptic Application Indicated Success of the Antiseptic |
Results
Table 1 details a comparison of 5% and 2.5% PI antibacterial efficacy to 0.01% HOCl using bacteria isolated from endophthalmitis attached to corneoscleral tissue. Five percent PI was comparably effective to 2.5% PI for preventing bacteria growth (χ2, p=0.71). Both 5% and 2.5% PI were more effective in preventing bacterial growth than 0.01% HOCl (χ2, p=0.004).
Of the bacteria that comprised of 4 isolates each, CNS (n=4), 5% PI (4 of 4) and 2.5% PI (4 of 4) were more effective for preventing bacterial growth than HOCl (1 of 4). For Sv (n=4), 5% PI (3 of 4) was more effective for preventing bacterial growth than 2.5% PI (1 of 4) and HOCl (1 of 4). For Sp (n=4), 5% PI (4 of 4) and 2.5% PI (4 of 4) were more effective for preventing bacterial growth than HOCl (1 of 4).
Both concentrations of PI and HOCl did not prevent the growth of Beta-Strep (isolated after an intravitreal injection), Ef, and Bc. Based on an intravitreal injection infection rate of 0.000252–4 and a yearly endophthalmitis infection probability of approximately 0.5 per year (Table 1), the infection rate for each of these bacteria would be 1 per 10,000 per year (this is based on endophthalmitis cases, not the total number of intravitreal injections). In other words, out of 10,000 endophthalmitis cases in any one year, there is only a single chance that it would be by Beta-Strep, Ef, or Bc.
Table 2 details a weighted comparison of 5% and 2.5% PI to 0.01% HOCl based on bacteria isolated from endophthalmitis over a 27-year period (1993–2019). For all bacterial groups except Sv, 5% PI was equally effective to 2.5% PI for preventing bacteria (χ2, p=1.0). Both 5% and 2.5% PI were more effective than 0.01% HOCl (χ2, p=0.00001). For Sv, 5% PI was more effective than 2.5% PI for reducing growth (χ2, p=0.0001). The probability of a Sv endophthalmitis based on a 0.00025 infection rate and an estimate yearly rate of 2.26 would indicate 5.65 infections per 10,000. In contrast, CNS would be 39.25 per 10,000.
Discussion
Antibiotic susceptibility testing for systemic treatment is based on the concentrations of antibiotic in the blood serum. There are no standards for topical treatment or intravitreal injection. Testing is performed in liquid medium with varying concentrations of antibiotic to determine an inhibitory concentration and not a bactericidal concentration. This dispersion of bacteria in antibiotic supplemented medium requires 24 hours of incubation time. This indirect approach is cost-effective and is the standard to estimate in vitro to in vivo correlation in a timely manner, but this does not necessarily represent the true reality of treatment. A more accurate approach to test susceptibility would be to use a solid medium to simulate an infection in tissue (ie skin, cornea). The anti-infective would be applied to the tissue with attached bacteria at different time frames to determine efficacy of treatment. This method of clinical susceptibility would be near impossible for each patient.
In the present study, corneoscleral tissue (representing the ocular surface) was used as a solid medium; bacteria from endophthalmitis were tested; antiseptics were tested for efficacy; and a 3-minute time-period was the contact period. The limitation of this model was the paucity of corneoscleral tissue. Corneal rims are firstly offered to research within our department. Fortunately, the experience of the first author (RPK) allowed single testing with confidence in the results. The bacteria selected were based on frequent causes of endophthalmitis (CNS, Streptococcus species, Sa)20 and bacteria that produced severe endophthalmitis (Bc, Ef, Gram-negative bacteria). Longer contact times with antiseptics may be advantageous, but this may not be practical for the ophthalmologist who is administering an intravitreal injection; plus, the antiseptics may be uncomfortable to the patient. Our study does not include the antibacterial effect of the host defense of the ocular surface, which may be noteworthy, but not a variable in this report.
Endophthalmitis after intravitreal injection is a rare event, but our data indicate the best antiseptic to prevent infection is 5% PI. Except for Sv, 2.5% PI was just as effective as 5% PI. HOCl was less effective as an antiseptic to prevent bacterial growth in the present study, but HOCl may provide prophylaxis in those that are allergic to PI.
Bacteria such as Bc, Ef, and Beta-Strep may not be eliminated with PI and HOCl, but fortunately these are very rarely the causative agents in post-surgical endophthalmitis. It appears that both PI and HOCl have less activity to the Streptococci groups and Bacillus species that have cell wall components that inactivate free iodine and resist oxidation. These bacteria can have varying peptidoglycan and cell wall structures, and these bacteria frequently form capsules for antibiotic protection.
We reject our original hypothesis because both 5% PI and 2.5% PI were more effective than HOCl for preventing bacterial growth from corneoscleral tissue. Our model should be considered to evaluate other anti-infectives for preventing bacterial growth on ocular tissues.
Funding
This study was partially supported by the Eye Bank Association of America/Richard Lindstrom Research Grant. This work was supported by NIH CORE Grant P30 EY08098 to the Department of Ophthalmology, the Eye and Ear Foundation of Pittsburgh, and from an unrestricted grant from Research to Prevent Blindness, New York, NY.
Disclosure
Dr Michelle Rhee reports grants from Ocular Therapeutix, is a Medical Advisor Board member for NovaBay, and consultant for The Eye-Bank for Sight Restoration, outside the submitted work. Dr Deepinder Dhaliwal reports personal fees from Kala, personal fees from Trefoil, personal fees from Haag Streit, personal fees from Horizon Therapeutics, personal fees from Ocular Therapeutics, personal fees from Novartis, personal fees from Allergan, personal fees from Staar Surgical, grants from Noveome, grants from Avedro, grants from Kowa, outside the submitted work. The authors have no current “Significant Conflict of Interests” to disclose for the completion of this study as determined by the Office of Research, University of Pittsburgh, Pittsburgh, PA, USA.
References
1. Goldberg RA. How to prevent endophthalmitis after intravitreal injection. Int J Retin Vitr. 2015;1:12. doi:10.1186/s40942-015-0012-9
2. Wen JC, McCannel CA, Mochon AB, Garner OB. Bacterial dispersal associated with speech in the setting of intravitrous injections. Arch Ophthalmol. 2011;129:1551–1554. doi:10.1001/archophthalmol.2011.227
3. Gregori NZ, Flynn HW, Schwartz SG, et al. Current infectious endophthalmitis rates after intravitreal injections of antivacualr endothelial growth factor agents and outcomes of treatment. Ophthal Surg Lasers Imaging Retina. 2015;46(6):643–648. doi:10.3928/23258160-20150610-08
4. McCannel CA. Meta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents. Causative organisms and possible prevention strategies. Retina. 2011;31:654–661. doi:10.1097/IAE.0b013e31820a67e4
5. Merani R, Hunyor AP. Endophthalmitis following intravitreal anti-vascular endothelial growth factor (VEGF) injection-A comprehensive review. Int J Retina Vitreous. 2015;1:9. doi:10.1186/s40942-015-0010-y
6. Cheung CS, Wong AW, Lui A, Kertes PJ, Devenyi RG, Lam WC. Incidence of endophthalmitis and use of antibiotic prophylaxis after intravitreal injection. Ophthalmology. 2012;119(8):1609–1614. doi:10.1016/j.ophtha.2012.02.014
7. Grzybowski AJ, Told R, Sacu S, Bandello F, Moisseiev LA. 2018 Update on intravitreal injections: euretina expert consensus recommendations. Ophthalmologica. 2018;239(4):181–193. doi:10.1159/000486145
8. Kim SJ, Toma HS, Midha NK, Cherney EF, Recchia FM, Doherty TJ. Antibiotic resistance of conjunctiva and nasopharynx evaluation study: a prospective study of patients undergoing intravitreal injections. Ophthalmology. 2010;117:2372–2378. doi:10.1016/j.ophtha.2010.03.034
9. Grzybowski AJ, Kanclerz P, Myers WG. The use of povidone-iodine in ophthalmology. Curr Opin Ophthalmol. 2018;29:19–32. doi:10.1097/ICU.000000000000437
10. Speaker MG, Menikoff JA. Prophylaxis of endophthalmitis with topical povidone-iodine. Ophthalmology. 1991;98:1769–1775. doi:10.1016/S0161-6420(91)32052-9
11. Bednarek RS, Nassereddin A, Ramsey Antiseptics: StatPearls [internet]. Treasure Island (FL): Stats Pearls Publishing; 2020. Available from: https://www.nlm.nih.gov/books/NBK507853/.
12. Peden MC, Hammer ME, Suñer IJ. Dilute povidone-iodine prophylaxis maintains safety while improving patient comfort after intravitreal injections. RETINA. 2019;39:2219. doi:10.1097/IAE.0000000000002290
13. Atemnkeng MA, Plaizer-Vercammen J, Schuermans A. Comparison of free and bound iodine and iodine species as a function of the dilution of three commercial povidone-iodine formulations and their microbicidal activity. Int J Pharm. 2006;317:161–166. doi:10.1016/j.ijpharm.2006.03.013
14. Prado SB, Ayora ACR, Campa AT. Measurement of free iodine in different formulations of povidone-iodine eye drops 5. Int J Pharm Compd. 2019;23:418–421.
15. Rutala WA, Weber DJ. Are room decontamination units needed to prevent transmission of environmental pathogens? Infect Control Hospital Epidemiol. 2011;32:743–747. doi:10.1086/661226
16. Chronister DR, Kowalski RP, Mah FS, Thompson PP. An independent in vitro comparison of povidone-iodine and sterilid. J Ocular Pharm Thera. 2010;26(3):277–280. doi:10.1089/jop.2010.0018
17. Klocek MS, Dhaliwal DK, Mammen A, Kowalski RP. Time-kill comparison of povidone iodine to hypochlorous acid against endophthalmitis isolates of Staphylococci. Ophthalmol and Vis Sci. 2018;CTOVS–108.
18. Gonzalez LG, Dhaliwal DK, Kowalski RP. Efficacy of topical 0.01% hypochlorous acid in reducing bacterial flora on lid margins and conjunctival sac compared to topical 5% povidone-iodine. JSM Ophthalmol. 2020;7(2):1074.
19. Kanclerz P, Grzybowski A, Olszewski B. Low efficacy of hypochlorous acid solution to povidone-iodine in cataract surgery antisepsis. Open Ophthalmol J. 2019;13:29–32. doi:10.2174/1874364101913010029
20. Kowalski RP, Nayyar SV, Romanowski EG, et al. The prevalence of bacteria, fungi, viruses, and acanthamoeba from 3004 cases of keratitis, endophthalmitis, and conjunctivitis. Eye Contact Lens. 2020;46:265–268. doi:10.1097/ICL.0000000000000642
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.