")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
The Anti-Psoriatic Efficacy and Safety Profile of Topical and Intralesional Methotrexate: A Literature Review
Authors Chaiyabutr C , Punnakitikashem P, Silpa-archa N, Wongpraprarut C , Chularojanamontri L
Received 27 June 2022
Accepted for publication 29 September 2022
Published 26 October 2022 Volume 2022:15 Pages 2253—2274
DOI https://doi.org/10.2147/CCID.S380218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Chayada Chaiyabutr,1 Primana Punnakitikashem,2 Narumol Silpa-archa,1 Chanisada Wongpraprarut,1 Leena Chularojanamontri1
1Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Department of Biochemistry, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Leena Chularojanamontri, Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Wanglang Road, Bangkok Noi, Bangkok, 10700, Thailand, Tel +66 2 419 4333, Fax +66 2 411 5031, Email [email protected]
Abstract: Methotrexate (MTX) has long been considered the first-line oral systemic pharmacotherapy for psoriasis. The drug has several well-known systemic side effects, such as bone marrow suppression and hepatotoxicity. To avoid them, the use of topical or intralesional administrations of MTX has become an interesting option. With the advent of novel drug delivery systems, especially nanocarriers, the usage of a high-efficacy and safe topical MTX for psoriasis has nearly been attained. This review examined the development, anti-psoriatic efficacy and adverse effects of topical forms of MTX (plain MTX; MTX with chemical enhancer; MTX using nanotechnology; MTX with protein transduction domains; MTX with liquid crystalline systems; and MTX with physical enhancer/laser) and intralesional MTX in psoriasis patients and psoriasis-induced animals. The efficacy of topical MTX varied with the drug delivery technology employed. Nevertheless, the overall safety profile of the topical forms was favourable. A 25 mg/mL MTX solution injected intralesionally at the nail matrix worked well for nail psoriasis recalcitrant to topical treatment. To improve the standard of care for patients with psoriasis, randomized controlled trials that establish the most effective MTX-delivery system are needed.
Keywords: drug delivery, intralesional, liposome, methotrexate, psoriasis, topical
Introduction
Although biological agents are being increasingly used, sometimes as the first-line treatment for moderate-to-severe psoriasis, methotrexate (MTX) is still the cornerstone conventional systemic treatment for psoriasis. This drug has been approved for psoriasis treatment by United States Food and Drug Administration since 1972 and currently situated in the latest guideline as the primary treatment for moderate to severe psoriasis.1,2 It acts primarily by inhibiting dihydrofolate reductase enzyme, resulting in decreased DNA synthesis and cell proliferation.3,4 MTX has immunosuppressive and anti-inflammatory properties as it promotes T cell apoptosis and reduces tumour necrosis factor-alpha production.5 There is also evidence that it inhibits Janus kinase-signal transducer and activator of transcription (JAK-STAT) pathway signalling.6 All mechanisms lead to a reduction in inflammation and a decrease in epidermal hyperplasia in psoriasis.
The most common side effects that curtail the utilisation of oral MTX are nausea and/or vomiting. Moreover, the systemic administration of MTX carries a high risk of systemic side effects, such as bone marrow suppression and hepatotoxicity. Thus, topical and intralesional administrations of MTX are preferred as they can substantially reduce oral-MTX side effects.7 The initial major obstacle in developing a topical MTX was its physicochemical properties. MTX has hydrophilic properties, whereas the lipid constituents of the stratum corneum are lipophilic, which limits the permeation of hydrophilic molecules such as MTX.8 Moreover, MTX has a high molecular weight and exists in a dissociated form at physiological pH: this leads to low passive-diffusion, or a low skin-penetration ability.3,4
Several drug delivery techniques—such as chemical and/or physical penetration enhancers, intralesional injection and nanocarrier drug-delivery systems—have been investigated and used to overcome the problem of the low skin-penetration ability of MTX. The results of those studies have varied between no benefits to a marked clinical improvement. The objective of the current study was to systematically review the efficacy of topical MTX (focusing on new drug-delivery systems) and intralesional MTX for psoriasis.
Methods
The Embase and Medline databases were searched from inception to July 2022 for English-language articles related to the research topic. The keywords related to “topical MTX”, “intralesional MTX” and “psoriasis”. To be considered for inclusion, studies had to investigate the anti-psoriatic efficacy of topical and/or intralesional MTX in psoriasis patients or an animal induced-mouse model of psoriasis. In all, 46 articles were retrieved. Ten of those related to topical MTX in an aqueous gel or cream, or with chemical enhancers (Table 1).9–18 Nineteen related to topical MTX with nanotechnology, supramolecular hydrogels, protein transduction domains and liquid crystalline systems (Table 2).8,19–36 Seven related to topical MTX with physical enhancers/laser/photodynamic therapy (Table 3).37–43 Eleven related to intralesional MTX injections (Table 4).15,44–53 Notably, 1 study conducted 2 experiments on the topical and intralesional treatment of psoriasis.15 Of the 46 articles, 27 were conducted on patients with psoriasis, whereas 19 used animal models of psoriasis.
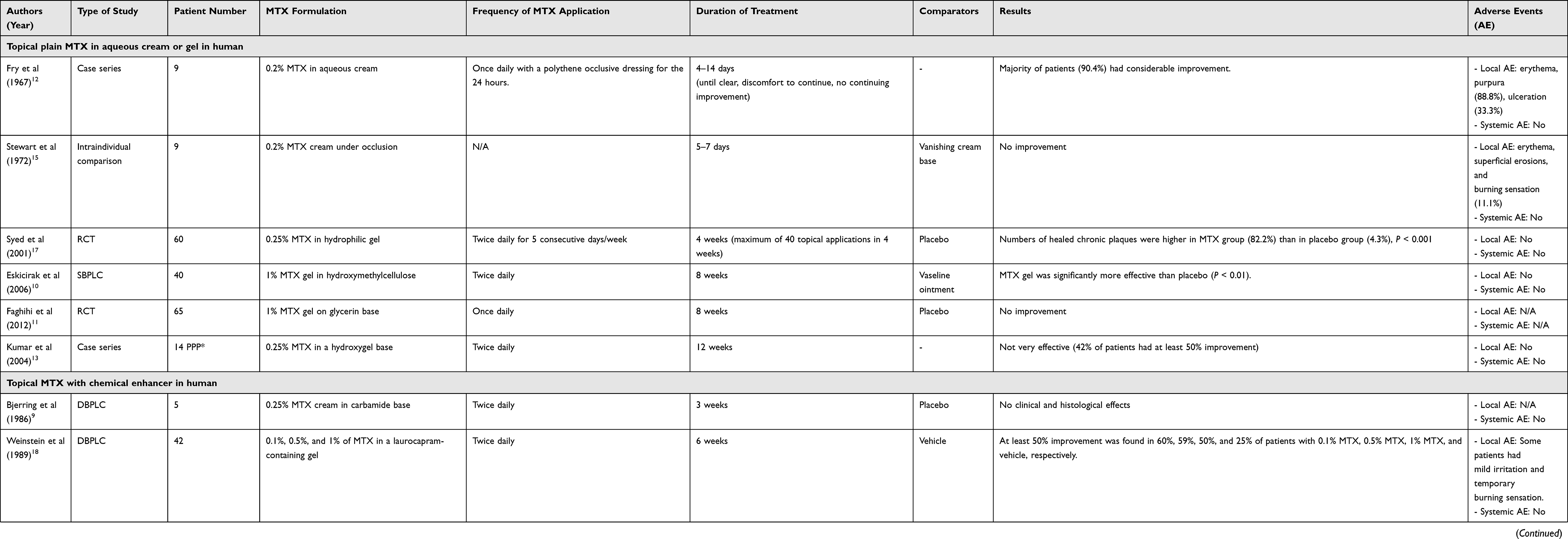 |
Table 1 Previous Studies Related to Topical Methotrexate (MTX) in Aqueous Cream or Gel, and to Topical MTX with Chemical Enhancers |
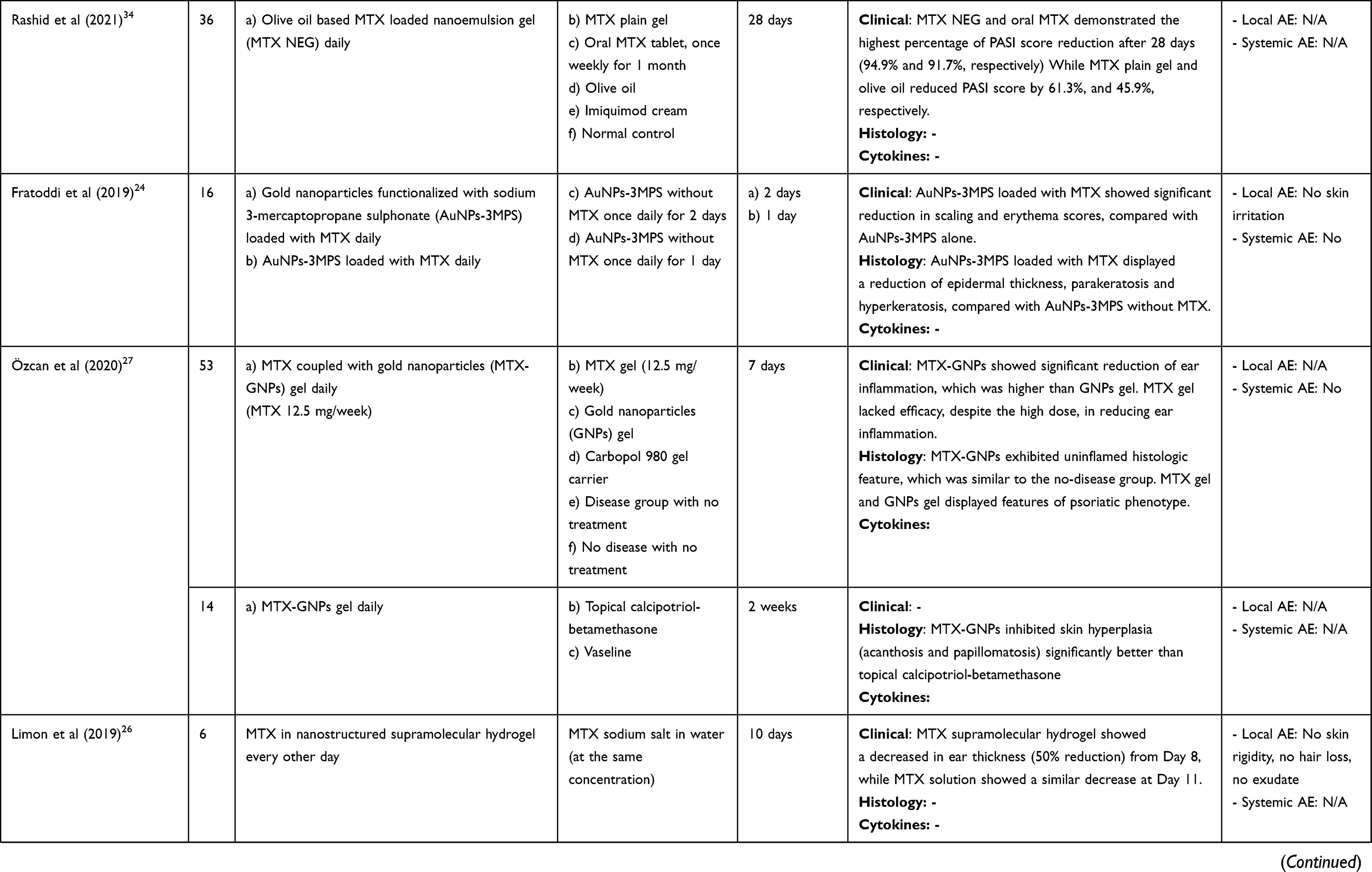 |
Table 2 Topical Methotrexate (MTX) Using Nanotechnology and Protein Transduction Domain |
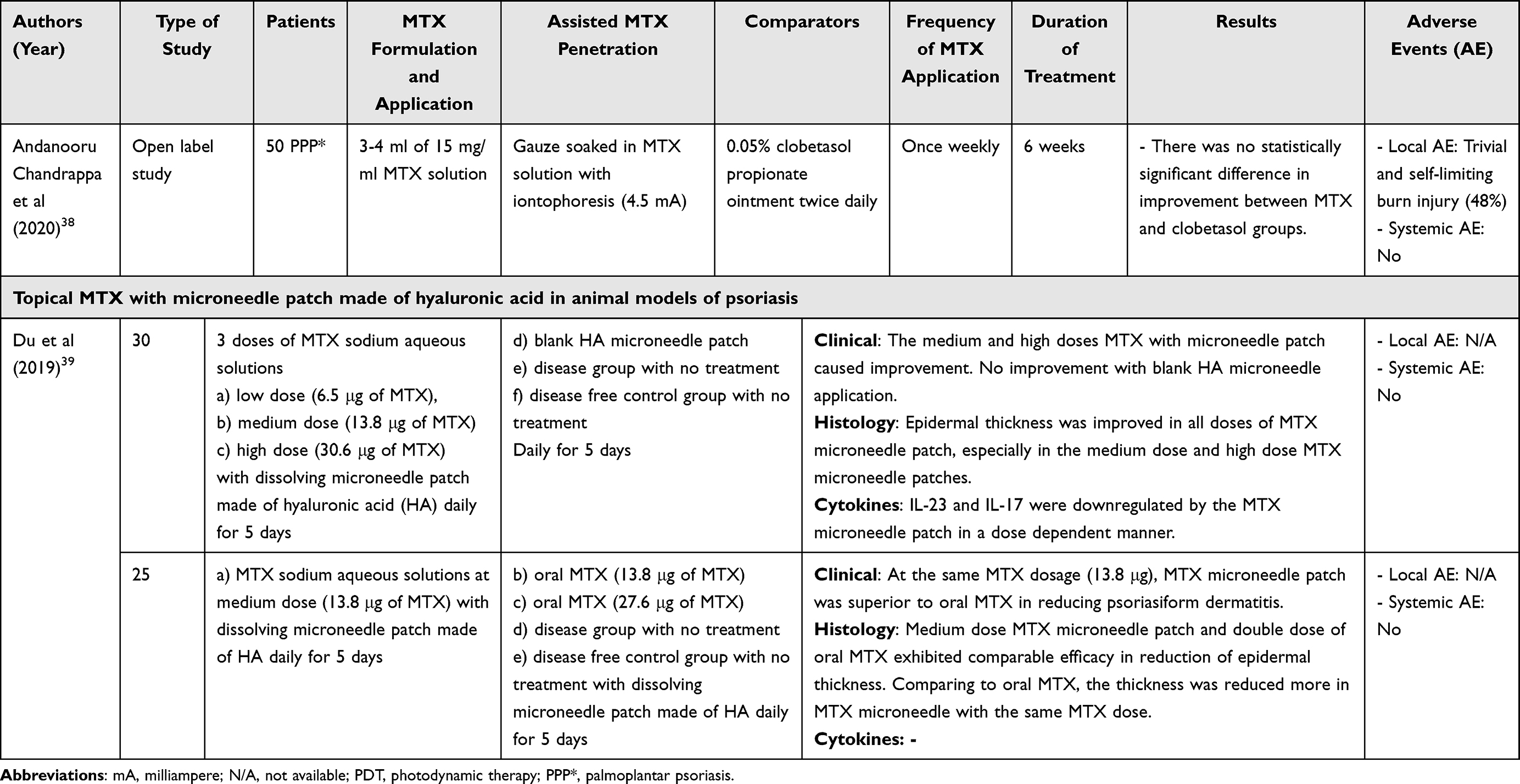 |
Table 3 Previous Studies Related to Topical Methotrexate (MTX) with Physical Enhancers/Laser/Photodynamic Therapy |
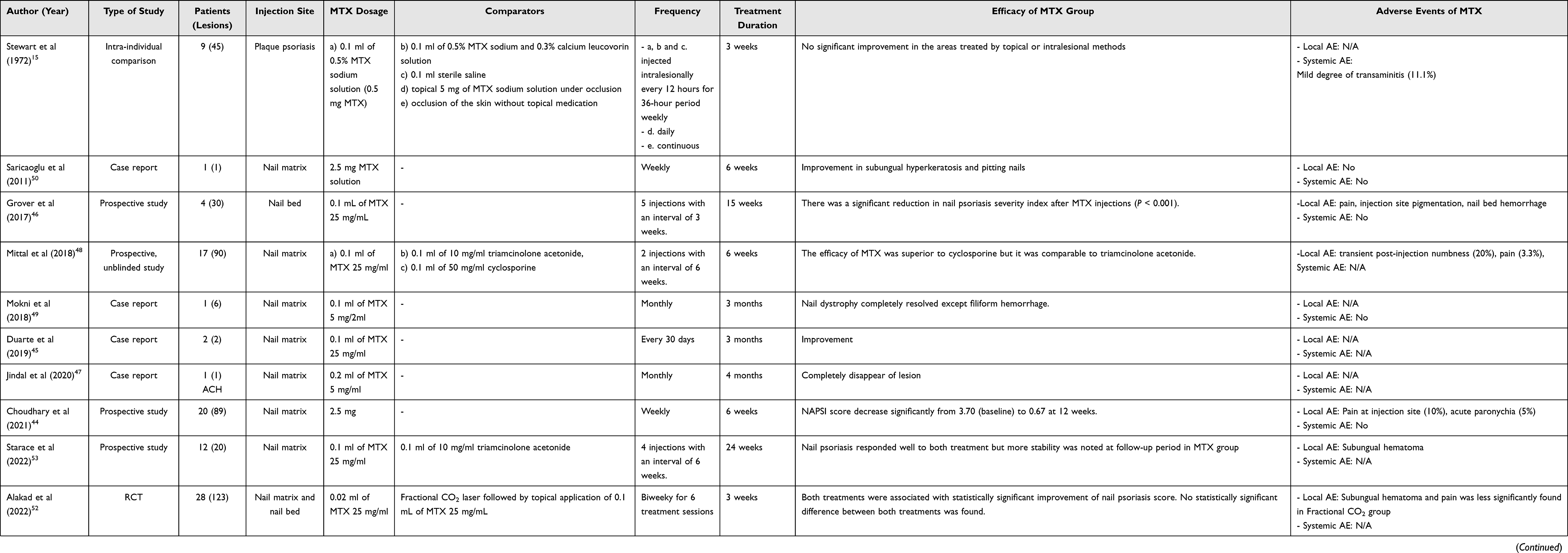 |
Table 4 Previous Studies Related to Intralesional Methotrexate (MTX) Injections |
Results and Discussion
Topical Plain MTX in Aqueous Cream or Gel
This platform was investigated in the early stages of topical MTX development. Topical plain MTX was produced by dissolving MTX in an aqueous cream or gel without using any enhancers or drug-assisted technology. Table 1 summarises 6 studies related to topical plain MTX in psoriasis.10−13,15,17 Three of those showed promising results: 1 case series; 1 randomized controlled trial (RCT); and 1 single-blind, placebo-controlled study.10,12,17 The remaining three showed ineffective results (1 intra-individual comparison, 1 RCT and 1 case series).11,13,15
Fry et al and Stewart et al reported a small case series of topical plain MTX in patients with plaque psoriasis in years 1967 (n = 9) and 1972 (n = 9), respectively. Both used 0.2% MTX in aqueous cream with occlusion, but the duration of treatment was slightly shorter in the work by Stewart et al. Although Fry et al found that 90.4% of the patients demonstrated considerable improvements, Stewart et al demonstrated no clinical benefits. Skin irritation was found in 88.8% and 11.1% of the former and the latter studies, respectively.12,15
Topical MTX gel formulations were developed later. Two of the four studies reported benefits from employing topical MTX gel to treat psoriasis.10,17 Syed et al (year 2001; n = 60) used 0.25% MTX in a hydrophilic gel twice daily for 4 weeks, and Eskicirak et al (year 2006; n = 40) used 1% MTX in hydroxymethylcellulose twice daily for 8 weeks in patients with chronic plaque-type psoriasis. Both studies compared the effects of MTX with placebos. Each investigation found a statistically significant higher number of patients achieved clinical improvements following MTX hydrogel therapy, compared with the placebo group (82.2% vs 4.3% in Syed et al’s study, and 97.5% vs 60% in Eskicirak et al’s study).10,17 In contrast, the results of topical plain MTX gel in other vehicle bases and for palmoplantar psoriasis were disappointing. Faghihi et al compared the efficacy of 1% MTX gel in a glycerine base with a placebo.11 Glycerine is an inert substance and humectant, and it is commonly used as a vehicle in topical medications. Nevertheless, Faghihi et al’s study did not find any significant differences in the clinical improvements shown by the treatment and placebo groups. Kumar et al studied the use of 0.25% MTX in a hydroxygel base twice daily for 12 weeks in 14 patients with palmoplantar psoriasis. The author concluded that, while the formulation was well tolerated, it was not very effective.13 The MTX gel did not induce any systemic or local adverse effects.
Topical MTX with Chemical Enhancer
The use of a chemical enhancer is one of the most convenient ways to facilitate the penetration of drugs into the stratum corneum. It disrupts the stratum corneum and then decreases the skin barrier resistance.54,55 Several chemical enhancers have been incorporated into topical MTX, such as carbamide (also known as urea), azone (also termed laurocapram) and propylene glycol. Carbamide increases the permeability of the stratum corneum by raising the amount of water absorbed by corneocytes and dissociating corneocyte adhesion (at high concentrations of carbamide).56 Azone is a polymeric chemical enhancer which can cause fluidisation and disruption of the liposomal lipids of the skin. Integrating azone into topical MTX can enhance both lipophilic and hydrophilic drug delivery to the skin.57 Propylene glycol is a hydrophilic molecule which increases drug permeation by improving the partition properties of active drugs in the skin.54
Four studies explored the use of topical MTX with a chemical enhancer. Three were double-blind, placebo-controlled trials: one investigated topical MTX with carbamide, while two considered azone gel. The fourth work, a case series, examined propylene glycol (Table 1).9,14,16,18 In 1986, Bjerring et al showed that 0.25% MTX cream with a carbamide base failed to demonstrate either clinical or histological improvements in 5 patients with plaque-type psoriasis.9 Weinstein et al (0.1%, 0.5%, 1% MTX) and Sutton et al (1% MTX) investigated topical MTX in an azone gel vehicle at different concentrations, ranging from 0.1% to 1%, in patients with plaque-type psoriasis.16,18 Both studies showed a superior efficacy of MTX in the azone gel than a placebo. With the MTX-treatment groups, the efficacy was not related to the concentration of MTX. Skin irritation was the common side effect of the azone-containing formulation.16,18 In 1999, Ravi Kumar et al showed clinical improvement in 80% and 64% of patients with palmar and plantar psoriasis, respectively, by using 1% MTX in propylene glycol. No local or systemic side effects were reported.14
Although three of the four studies showed clinical benefits from the use of topical MTX with a chemical enhancer, there are some difficulties associated with its use in practice. As the macromolecular weight of MTX is quite high, a high concentration of chemical enhancer is needed to permeate the skin effectively, resulting in skin irritation.58
Topical Methotrexate Using Nanotechnology
In recent years, nanoscale drug delivery systems, or drug nanocarriers, have developed rapidly. This technology greatly enhances the efficacy of transdermal drug delivery. It uses nanomaterial as a transporter to carry an active drug to a target site, leading to a localized and increased drug concentration at the site. This system has several advantages over chemical penetration enhancers. Among them are a sustained drug release, and protection of the active drug from degradation processes. Together, these attributes result in a lower amount of active drug usage and fewer cutaneous side effects.58
The formulations of nanocarriers can be classified by their size, structure, chemical properties, composition of materials, and main constituents.59 Several types of nanomaterials for topical MTX have been recently reported. Nanocarriers can be divided into several groups: lipid-based nanocarriers, polymer-based nanocarriers, metal-based nanocarriers, and composite materials drug delivery system. Sixteen studies investigated topical MTX using nanotechnology delivery techniques: two with humans, and fourteen using animal-models of psoriasis.8,19–21,23–30,32,34–36 In the 2 human studies, the reported clinical efficacy of MTX in liposomes conflicted (Table 2). In the animal models of psoriasis, topical MTX using nanotechnology demonstrated promising results in all studies. Overall, there were no local and systemic side effects.
Topical MTX with Liposomes
Liposomes are lipid-based nanocarriers which are considered safe and non-toxic because of their main constituent, a phospholipid bilayer. They are small, nanosized, spherical-shaped structures in which amphiphilic lipid molecules arrange themselves in a bilayer pattern.60 Due to their structure, liposomes can encapsulate and improve the stability of both hydrophilic and hydrophobic drugs at target sites. With their vesicular structure, liposomes act as a biological membrane that has the ability to carry a drug and avoid drug destabilization. Therefore, loading MTX in liposomes can enhance its transdermal drug delivery. A low amount of MTX in a liposome preparation but a high MTX concentration presented to the epidermis may improve psoriatic skin lesions with fewer cutaneous and systemic side effects than are produced by using conventional methods.37,60 However, the drawbacks of conventional liposomes have been found to be instability and drug leakage from the vesicles.37 Moreover, some of the liposomes fail to penetrate deep into the epidermis, remaining instead in the upper part of the stratum corneum.61 To overcome these challenges, niosomes (1st generation), transfersomes (2nd generation) and ethosomes (3rd generation) have been developed to increase the skin penetration of the active drug.62
Although having a bilayered structure similar to liposomes, niosomes are mainly composed of non-ionic surfactants (non-ionic, surfactant-based vesicles). Due to their biodegradable and non-toxic nature, niosomes are now widely studied as an alternative to conventional liposomes because of their greater stability, higher drug entrapment efficiency and lower cost.25,63 Lakashmi et al reported the method to encapsulate MTX into niosomes and then incorporate the structure within chitosan gel. This gel promotes the absorption effect of MTX in niosomes by increasing the adhesive effect between the formulation and the stratum corneum. Lakashmi et al performed an RCT study of 0.25% niosomal MTX, incorporated into chitosan gel, comparing it with an 0.25% marketed MTX gel and a placebo in 30 patients with plaque-type psoriasis. The 0.25% niosomal MTX gel was significantly more efficacious than the 0.25% marketed MTX gel and the placebo.25 In 2021, Yang et al developed MTX-nicotinamide niosomes based on ceramide (cerosomes).36 As nicotinamide has an anti-inflammatory property, this substance was proposed to synergize the efficacy of MTX. They tested this formulation in imiquimod induced psoriasis mouse model and compared the efficacy with oral MTX and other topical MTX/nicotinamide formulations. They found that Psoriasis Area and Severity Index (PASI) score and epidermal thickness after applying MTX-nicotinamide cerosomes daily for 7 days were significantly lower than other treatment groups.
Transfersomes, also termed deformable liposomes, are elastic lipid vesicle carriers which are composed of phospholipids and an edge activator-like surfactant that is a membrane-softening agent.61 When transfersomes reach the skin pores, they are capable of deforming their membranes and squeezing through the pores spontaneously. This ability stems from the elastic nature of transfersomes.64 When compared with conventional liposomes, transfersomes demonstrated an increased drug penetration depth and improved drug efficacy and stability.30 Vanaja et al compared the effects of an 0.25% ultra-deformable liposomal MTX gel with those of a 1% plain MTX gel in 25 patients with psoriasis.30 The 2 gels demonstrated comparable efficacy. However, they concluded that the ultra-deformable liposomes demonstrated an improved topical drug delivery of MTX because a lower MTX concentration was used in the liposomes.30 Bahramizadeh et al developed MTX-entrapped deformable liposomes containing oleic acid; their efficacy was investigated in an imiquimod-induced mouse model of psoriasis. It was found that treatment with 0.05% MTX liposomes significantly reduced the severity of psoriasis. A reduction in epidermal thickness, as determined by histopathology, was significantly achieved with both 0.05% and 0.1% MTX liposomes.21
Ethosomes are elastic lipid vesicle carriers which are composed of phospholipids and ethanol, resulting in a high deformability and elasticity of the vesicle carriers. They can pass through the intracellular space of the skin, and they have a high drug-entrapment ability.61 Moreover, ethanol disrupts the lipid bilayer of the stratum corneum, resulting in high drug penetration to deep skin layers.60 Chandra et al studied an ethosomal gel of 0.25% MTX incorporated with 2% salicylic acid in a mouse model of psoriasis (n = 12). The clinical and histopathological skin severities were reduced more in the MTX ethosomal group than in the blank gel group.23
Topical MTX with Solid Lipid Nanoparticles
Solid lipid nanoparticles (SLNs) are comprised of biodegradable lipids, and a surfactant which has a solid lipid core and is able to encapsulate both hydrophilic and hydrophobic drugs. Nanostructured lipid carriers (NLCs) are a new generation of solid lipid nanoparticles to overcome the limitations of SLNs, which are limited drug loading capacity, drug leakage and stability. NLCs are colloidal carriers that are developed from a blend of solid and liquid lipids to form a drug-incorporated matrix.65,66 Unlike solid lipid nanoparticles, NLCs have defects in their crystal lattice that provide more space to load drug encapsulations. The advantages of NLCs are their high drug-loading capacity, minimal drug leakage and controlled drug-release rate. Moreover, they can form a thin film overlying the skin, thereby increasing skin hydration.19,59,67 Two mouse models of psoriasis revealed clinical and histological benefits of MTX-NLC.19,20 The work by Avasatthi et al established that an MTX-NLC nanogel has a superior efficacy to an MTX gel formulation.20 Agrawal et al compared the anti-psoriatic efficacy of MTX-NLC with that of conventional MTX in carbopol gel. The MTX-NLC group achieved a significant reduction in histological severity and inflammatory-cytokine levels than the MTX in carbopol gel. Nevertheless, the improvement in the clinical severity of the MTX-NLC group was comparable to that achieved by the MTX in carbopol gel.19
Topical MTX with Polymeric Nanoparticles
Polymeric nanocarriers can be developed from natural, semi-synthetic or synthetic polymers.58 Many types of polymeric carriers are used for transdermal drug delivery, for example, polymeric micelles, dendrimers, nanocapsules and nanogels.68 Polymeric nanogels are three-dimensional hydrogel materials formed by entangled networks of polymeric particles that can trap a large amount of water molecules within the networks. In addition, they have a relatively high drug encapsulation capacity and stability. Polymeric nanogels have shown promising results as a good candidate as a drug nanocarrier.69 Panonumal et al developed an MTX-loaded nanogel of chitin (MCNG), which is a natural biodegradable nontoxic polymer. Two MCNG formulations (100 and 150 μg/cm2) were applied daily for 3 weeks in an imiquimod-induced mouse model for psoriasis. Comparisons were made between 150 μg/cm2 of conventional MTX in carbopol gel, carbopol gel, control chitin nanogel and a positive control. The results showed that 150 μg/cm2 MCNG was superior to 100 μg/cm2 MCNG as well as to 150 μg/cm2 conventional MTX carbopol gel. The remaining groups were less efficacious than those 3 groups. Moreover, the MCNG-treated group at both MTX doses exhibited less features of histopathological findings of psoriasis than the other groups. No systemic or local adverse effects were reported for MCNG.28 Asad et al developed MTX based nanoparticle-loaded chitosan hydrogel and tested in an imiquimod induced psoriatic mouse model for 10 consecutive days.32 Their formulation was compared with free MTX hydrogel and marketed cream. They found that PASI score was decreased in all of these three groups, but a mark decreased was observed in MTX based nanoparticle-loaded chitosan hydrogel. TNF-α and IL–6 were mostly reduced by MTX based nanoparticle-loaded chitosan hydrogel groups, compared to other treatments.
Topical MTX with Micro-Emulsion and Nano-Emulsion
Micro-emulsion and nano-emulsion are both colloidal dispersion systems. They can be defined as the nanometric dispersion of one liquid phase to another insoluble liquid phase.70 They have many similarities and differences in terms of their composition and stabilities. Micro-emulsions are thermodynamically stable colloidal dispersions composed of oil, water and a surfactant.66,71,72 Micro-emulsions have hydrophilic and lipophilic domains that react with lipids on the skin. This results in a modification of the intercellular space of the stratum corneum, thereby permitting drug transportation.8,73 The dispersed domain sizes are usually between 10 to 50 nm.74 Amarji et al compared an 0.25% MTX-loaded micro-emulsion in poloxamer gel with an 0.1% topical dexamethasone and a poloxamer gel (placebo).8 Although the MTX-loaded micro-emulsion in poloxamer gel improved clinical psoriasis skin from the third day onwards, a faster onset and higher efficacy was achieved with the topical dexamethasone.8
Nano-emulsions resemble micro-emulsions in that both are dispersions of nano-sized particles, but they are thermodynamically unstable. The oil droplet containing the active drug is stabilized by an emulsifier and acts as a drug carrier with the characteristics of lipophilic and solid spheres. Another difference between micro- and nano-emulsions is that the former can develop spontaneously, whereas the latter is obtained by mechanical force.74 Rajitha et al developed an MTX-nano-emulsion gel in a chaulmoogra-oil base and demonstrated its anti-psoriatic efficacy in animal models. Chaulmoogra oil is a traditional medicine containing many bioactive fatty acids that have anti-inflammatory properties. A daily application of MTX-nano-emulsion gel in a chaulmoogra-oil base for a month (cumulative MTX dose = 25 mg/week) produced a better clinical improvement than oral MTX (15 mg/week for a month).29 Rashid et al developed olive oil-based MTX nanoemulsion gel (MTX NEG) and tested the efficacy in imiquimod-induced mouse model of psoriasis. MTX NEG was applied daily for 28 days and its efficacy was compared with MTX plain gel, olive oil and oral MTX.34 MTX NEG and oral MTX demonstrated the highest percentage of PASI score reduction at the end of study (94.9% and 91.7%, respectively). While MTX plain gel and olive oil showed less improvement in PASI score reduction (61.3%, and 45.9%, respectively).
Topical MTX with Metal Nanoparticles
Metallic nanocarriers have gained attention in biomedical applications because of their small size, relatively high surface area to volume ratio, ease of preparation, and versatile surface modifications. Examples of these nanocarriers are gold nanoparticles (AuNPs) and silver nanoparticles (AgNPs).59 AuNPs are very small (1–100 nm), inert and low toxicity materials which can easily penetrate cells and deliver active drugs. Moreover, AuNPs have an immunomodulatory effect that can reduce the production of proinflammatory cytokines such as tumour necrosis factor-α and interleukin-6, both of which are related to the pathogenesis of psoriasis.75 To date, the anti-psoriatic benefits of AuNP have only been demonstrated in animal studies.
Fratoddi et al developed gold nanoparticles that were functionalized with sodium 3-mercaptopropane sulfonate (AuNPs-3MPS) and loaded with MTX. Although the nanoparticle was applied daily for only 1–2 days, it reduced clinical scaling and erythema more significantly than AuNPs-3MPS alone.24 Özcan et al also compared the efficacy of MTX coupled with a gold nanoparticle (MTX-GNP) gel (MTX 12.5 mg/kg) with the effects of an MTX gel (MTX 12.5 mg/kg), a GNP gel and a carbopol 980 carrier. The MTX-GNPs showed the significantly highest reduction in ear inflammations of all the groups. Moreover, MTX-GNPs have demonstrated a better histopathological improvement than the topical calcipotriol-betamethasone.75
Topical MTX with Nanocomposite Hydrogels
Supramolecular hydrogels are a novel class of three-dimensional hydrophilic polymers cross-linked by non-covalent bonds. They show high physical stability and drug-loading capacity.67 Limon et al developed nanostructure supramolecular hydrogels of MTX and compared their efficacy with that of a topical MTX sodium salt solution at the same concentration in a mouse model of psoriasis.26 The nanostructured supramolecular hydrogels of MTX showed a comparable treatment efficacy to MTX solution, but the hydrogels induced a swifter response. The faster onset of action may be due to an enhancing of the drug permeation or to a prolonging of the drug retention by the supramolecular gel.26 In 2022, Xu et al developed MTX-Zinc oxide/Ag (ZA) embellished with nanomicelles (NMs) and further embedded with carbopol(Car); (Car@NMs@MTX-ZA hydrogels). This formulation was applied on skin of the psoriatic-induced mouse model daily for 6 days. The efficacy was compared with Car@NMs@MTX hydrogel, Car@NMs@ZA hydrogel, Car@MTX hydrogel, Car@ZA hydrogel, Car@MTX-ZA hydrogel, zinc oxide and blank carbopol hydrogel.35 They found that Car@NMs@MTX-ZA hydrogels exhibited the best effect in PASI score reduction, improvement of psoriatic histopathological changes and suppression of several pro-inflammatory cytokines.
Topical MTX with Protein Transduction Domains or Cell-Penetrating Peptides
Protein transduction domains (PTDs) are small cationic molecules which consist of 30 or fewer amino acids residues. They can transport and deliver drug molecules through cell membranes.58 PTDs also have the potential to convey lipid nanoparticles (liposomes and NLC) across the skin layers.58 Byamba et al developed PTDs conjugated with MTX, which could be considered as a skin-permeable MTX. One injection of intraperitoneal MTX (35 mg/kg) was compared with 0.1% and 1% skin-permeable MTX daily for 3 days. The anti-psoriatic efficacy (measured by the decrease in the PASI score) of the 1% skin‐permeable MTX was better than that achieved with the intraperitoneal MTX.22 While PTD systems have shown good efficacy and favourable safety profiles, the number of human and animal-model studies on psoriasis is very limited.
Topical Methotrexate with Liquid Crystalline System
Liquid crystals are designated as state that is located between solid and liquid state. It has gained attention in drug delivery development as they have the ability to include either lipophilic or hydrophilic drug regardless of drug dimensions.76 This system could be able to enhance drug solubility and control drug release rate. Furthermore, liquid crystals are easy to scale up, cheap, and thermodynamically stable.77 However, the result of two studies applying MTX-loaded liquid crystalline system on psoriatic-induced animal models was disappointed. Their histopathological results after using these formulations in psoriatic-induced mouse model were not improved and inflammatory cytokine parameters after using these formulations were higher, comparing to the control.31,33
Topical Methotrexate with Physical Enhancers/Laser/Photodynamic Therapy
Seven published studies investigated the use of topical MTX with physical enhancers/laser/photodynamic therapy. Two examined the use of topical MTX with lasers for human psoriasis skin lesions. One investigated the use of topical MTX coupled with photosensitizer in photodynamic therapy in animal models of psoriasis. Three considered topical MTX with iontophoresis for palmoplantar psoriasis treatment. The seventh study explored the application of topical MTX via microneedle patches with hyaluronic acid in animal models of psoriasis (Table 3).
Topical MTX with Diode Laser
Ali et al conducted an RCT study using 0.25% deformable liposome MTX hydrogel once daily with 650 nm diode laser irradiation 3 times weekly for 12 weeks. The results were compared with those of a plain MTX gel with a similar diode laser, and of a placebo (laser alone), in 30 patients with psoriasis.37 After exposure to visible or ultraviolet light, the deformable liposomes break down and release MTX, with no effect on MTX chemical stability. This expedites or enhances MTX release from deformable liposomes, which leads to a high MTX concentration in the epidermal layer. The investigations by Ali et al revealed that 46.6%, 13.3% and 0% of the patients administered the deformable liposomal MTX gel, plain MX gel and placebo, respectively, achieved complete clearance of the psoriatic lesions at the end of the 12-week treatment period.37
Topical MTX with Fractional Laser
An ablative fractional laser modifies the stratum corneum by partial removal of the skin surface. It creates microchannels in the skin, enabling delivery of hydrophilic and high molecular weight drugs like MTX.78 Drug diffusion is increased not only by the enlargement of the absorption area, but also by the microchannels, which act as a reservoir for drug delivery.78 Ramez et al combined the fractional erbium: YAG (yttrium aluminium garnet) laser with a 0.1% nanoparticulated MTX micro-emulsion based on jojoba oil. Intra-individual left-right comparisons were also made of the MTX micro-emulsion with, and without, fractional erbium: YAG assisted delivery. Both sides showed a reduction in thickness, erythema and scale, but the side with fractional erbium: YAG showed a higher significant reduction.41
Topical MTX with Photodynamic Therapy
Photodynamic therapy (PDT) is a treatment that uses photosensitizing drug along with light to destroy abnormal cells. 5-Aminolevulinic acid (ALA) is the well-known photosensitizing agent that was approved by the Food and Drug Administration to use for PDT treatment.79 Wang et al reported the successful usage of chitosan/hyaluronan co-loading with MTX-ALA nanogels plus the irradiation with 635 nm laser.43 They performed their experiment in imiquimod induced mouse model of psoriasis and compared their formulation with oral MTX and other topical MTX or ALA plus irradiation. They found that MTX-ALA nanogels exhibited the best effect in decreasing the PASI score, compared to other treatment groups. Moreover, only MTX-ALA nanogels group can normalize the levels of TNF-α and IL-17A to those of the normal control group. The safety of topical MTX-ALA nanogels was confirmed by the histological analyses in heart, liver, spleen, lung, and kidney of the mouse which was not showing any abnormalities.
Topical MTX with Iontophoresis
Iontophoresis utilises micro-electrical assistance to achieve transdermal drug delivery. A direct electrical current drives ionically charged drugs through the skin. The dose of the delivered drug depends on the total electric charge. Generally, iontophoresis is used to deliver hydrophobic, low-molecular-weight drugs.80 However, the ionic structure of MTX is also suitable for the mechanism of iontophoresis.42 Two studies and 1 case report, all from India, used a topical MTX solution with iontophoresis for palmoplantar psoriasis treatment.38,40,42 Overall, the efficacy of MTX plus iontophoresis was not remarkable. This was probably due to the large MTX molecule-size and the recalcitrant nature of palmoplantar psoriasis.
In 2003, Tiwari et al reported the successful treatment of a palmoplantar psoriasis patient by using a topical MTX disodium solution (10 mg/mL) soaked in gauze, combined with iontophoresis.42 Haseena et al conducted an intra-individual comparison study using an MTX solution (50 mg/2 mL) diluted in 50 mL of water soaked in gauze plus iontophoresis.40 The side treated with MTX plus iontophoresis showed a statistically significant reduction in palmoplantar-psoriasis severity, compared with the control side.40 Andanooru Chandrappa et al conducted a prospective, randomized, unblinded study on 50 palmar psoriasis patients, comparing the efficacy of cotton gauze soaked in MTX solution (15 mg/mL) plus iontophoresis, with the effects of 0.05% clobetasol propionate ointment.38 With its greater number of patients, the research revealed that the efficacy of the MTX solution plus iontophoresis once weekly was comparable with that of a twice daily application of topical clobetasol propionate. However, it should be noted that fewer milliamperes of iontophoresis were used in the work by Andanooru Chandrappa et al. A considerable number of trivial and self-limiting burn injuries were observed in that study.38
Topical MTX with Microneedle Patches
Microneedle techniques use needles to create micro-pores in the skin prior to the application of a topical drug. This physical technique facilitates drug penetration. The microneedles are made from a variety of materials, and are available in solid or hollow forms. However, drug uptake can be limited once the needles are removed from the skin and the micropores begin to close. Microneedles using hyaluronic acid (HA), or HA-based dissolving microneedles, have been developed to overcome these limitations. HA-based microneedles dissolve upon insertion while simultaneously releasing drug into the skin. This innovation both simplifies the administration of the drug and increases its uptake by the skin.39
Du et al developed an MTX-loaded HA-microneedle patch and conducted the study in an imiquimod-induced mouse model of psoriasis. Firstly, they compared the antipsoriatic efficacy of MTX-loaded HA-microneedle patches at a low MTX dose (6.5 μg), medium MTX dose (13.8 μg) and high MTX dose (30.6 μg). They found that the MTX-loaded HA-microneedle patches improved the clinical, histological and inflammatory outcomes in a dose-dependent manner. Secondly, they compared the efficacy of a medium-dose HA-microneedle patch (13.8 μg of MTX) with that of oral MTX at the same dose (13.8 μg) and at a double dose (27.6 μg of MTX). The medium-dose HA-microneedle patch was superior to the oral MTX of the same dose level. An analysis of the epidermal thicknesses achieved with the medium-dose HA-microneedle patch and with the double dose of oral MTX revealed comparable efficacy levels. Both therapies were significantly superior to oral MTX at the same dose as for the microneedle patch. This indicated that an MTX microneedle patch had a higher antipsoriatic efficacy than oral MTX at the same dose.39
Intralesional MTX
Eleven studies examined the use of intralesional MTX for psoriasis (Table 4).15,44–53 One study of its efficacy for psoriasis skin lesions found no significant improvements. By contrast, all 10 studies investigating its efficacy for nail psoriasis demonstrated significant improvements in the nail matrix and nail bed. The most common treatment for the nail psoriasis was a 2.5 mg MTX solution injected at the nail matrix. As psoriasis nails are usually recalcitrant to both conventional topical and systemic treatments, an intralesional MTX injection which gives a high drug concentration to the target nail tissue is an interesting choice. Nevertheless, its side effects—especially pain, subungual hematoma and transient post-injection numbness—may limit its usage.44,46,48,53
There were 3 studies comparing the efficacy of intralesional MTX (25 mg/mL) for nail psoriasis with intralesional triamcinolone acetonide (10 mg/mL).48,51,53 Two studies reported the good and comparable efficacy of intralesional methotrexate and triamcinolone acetonide with more stability of the result from MTX group in one study.48,53 While Abdelmeniem et al reported that the mean Nail Psoriasis Severity Index (NAPSI) score improvement of intralesional MTX was less than intralesional triamcinolone acetonide and topical 0.005% calcipotriol cream plus 20% urea under occlusion at psoriatic nail.51
The efficacy of intralesional MTX for nail psoriasis was compared with fractional laser assisted drug delivery in one study.52 Fractional carbon dioxide (CO2) laser plus topical application of 0.1 mL of MTX 25 mg/mL and intralesional MTX (25 mg/mL) were given biweekly for 6 weeks in 28 patients with nail psoriasis. They found that Fractional CO2 laser plus topical MTX displayed a comparable improvement to intralesional MTX but the laser group was associated with less side effects (pain and subungual hematoma).
Conclusion
Studies related to topical MTX in patients with psoriasis are limited. The efficacy of plain MTX in an aqueous cream or gel and of topical MTX with chemical enhancers do not seem promising due to their difficulty achieving skin penetration and their high risk of skin irritation. Nanoscale-based drug delivery—with and without physical enhancers such as an ablative laser or microneedle patches—are an interesting option. Most nanoscale drug delivery systems have shown good efficacy in animal models of psoriasis. However, data on the use of those techniques in patients with psoriasis are scarce. This review will benefit researchers worldwide who are pursuing the development of the most suitable formations of topical MTX. Further studies with a larger number of patients are needed to establish the most effective drug delivery system for psoriasis treatment.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest or financial support to declare.
References
1. Nast A, Smith C, Spuls PI., et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–2498. doi:10.1111/jdv.16915
2. Weinstein GD. Drugs five years later: methotrexate. Ann Intern Med. 1977;86(2):199–204. doi:10.7326/0003-4819-86-2-199
3. Tripathi P, Kumar A, Jain PK, Patel JR. Carbomer gel bearing methotrexate loaded lipid nanocontainers shows improved topical delivery intended for effective management of psoriasis. Int J Biol Macromol. 2018;120(Pt A):1322–1334. doi:10.1016/j.ijbiomac.2018.08.136
4. Aickara D, Bashyam AM, Pichardo RO, Feldman SR. Topical methotrexate in dermatology: a review of the literature. J Dermatolog Treat. 2020;3:1–6.
5. Law JH, Koo B, Koo JYM. Methotrexate update: mechanism of action in psoriasis therapy. Psoriasis Forum. 2008;14a(1):17–28. doi:10.1177/247553030814a00105
6. Thomas S, Fisher K, Snowden J, Danson S, Brown S, Zeidler M. Effect of methotrexate on JAK/STAT pathway activation in myeloproliferative neoplasms. Lancet. 2015;385(Suppl 1):S98. doi:10.1016/S0140-6736(15)60413-5
7. Javadzadeh Y, Hamishehkar H. Enhancing percutaneous delivery of methotrexate using different types of surfactants. Colloids Surf B Biointerfaces. 2011;82(2):422–426. doi:10.1016/j.colsurfb.2010.09.015
8. Amarji B, Garg NK, Singh B, Katare OP. Microemulsions mediated effective delivery of methotrexate hydrogel: more than a tour de force in psoriasis therapeutics. J Drug Target. 2016;24(2):147–160. doi:10.3109/1061186X.2015.1058804
9. Bjerring P, Beck HI, Zachariae H, Sogaard H. Topical treatment of psoriatic skin with methotrexate cream: a clinical, pharmacokinetic, and histological study. Acta Derm Venereol. 1986;66(6):515–519.
10. Eskicirak B, Zemheri E, Cerkezoglu A. The treatment of psoriasis vulgaris: 1% topical methotrexate gel. Int J Dermatol. 2006;45(8):965–969. doi:10.1111/j.1365-4632.2006.02911.x
11. Faghihi G, Ghafghazi T, Nilforoushzadeh MA. The effect of methotrexate 1% topical gel on psoriasis. J Isfahan Med Sch. 2012;29(173):3087–3092.
12. Fry L, McMinn RM. Topical methotrexate in psoriasis. Arch Dermatol. 1967;96(5):483–488. doi:10.1001/archderm.1967.01610050005001
13. Kumar B, Sandhu K, Kaur I. Topical 0.25% methotrexate gel in a hydrogel base for palmoplantar psoriasis. J Dermatol. 2004;31(10):798–801. doi:10.1111/j.1346-8138.2004.tb00602.x
14. Ravi Kumar BC, Kaur I, Kumar B. Topical methotrexate therapy in palmoplantar psoriasis. Indian J Dermatol Venereol Leprol. 1999;65(6):270–272.
15. Stewart WD, Wallace SM, Runikis JO. Absorption and local action of methotrexate in human and mouse skin. Arch Dermatol. 1972;106(3):357–361. doi:10.1001/archderm.1972.01620120045009
16. Sutton L, Swinehart JM, Cato A, Kaplan AS. A clinical study to determine the efficacy and safety of 1% methotrexate/Azone® (MAZ) gel applied topically once daily in patients with psoriasis vulgaris. Int J Dermatol. 2001;40(7):464–467. doi:10.1046/j.1365-4362.2001.01244.x
17. Syed TA, Hadi SM, Qureshi ZA, Nordstrom CG, Ali SM. Management of psoriasis vulgaris with methotrexate 0.25% in a hydrophilic gel: a placebo-controlled, double-blind study. J Cutan Med Surg. 2001;5(4):299–302. doi:10.1177/120347540100500403
18. Weinstein GD, McCullough JL, Olsen E. Topical methotrexate therapy for psoriasis. Arch Dermatol. 1989;125(2):227–230. doi:10.1001/archderm.1989.01670140079014
19. Agrawal YO, Mahajan UB, Mahajan HS, Ojha S. Methotrexate-loaded nanostructured lipid carrier gel alleviates imiquimod-induced psoriasis by moderating inflammation: formulation, optimization, characterization, in-vitro and in-vivo studies. Int J Nanomedicine. 2020;15:4763–4778. doi:10.2147/IJN.S247007
20. Avasatthi V, Pawar H, Dora CP, Bansod P, Gill MS, Suresh S. A novel nanogel formulation of methotrexate for topical treatment of psoriasis: optimization, in vitro and in vivo evaluation. Pharm Dev Technol. 2016;21(5):554–562. doi:10.3109/10837450.2015.1026605
21. Bahramizadeh M, Bahramizadeh M, Kiafar B, et al. Development, characterization and evaluation of topical methotrexate-entrapped deformable liposome on imiquimod-induced psoriasis in a mouse model. Int J Pharm;2019. 569. doi:10.1016/j.ijpharm.2019.05.036
22. Byamba D, Kim DY, Kim DS, et al. Skin-penetrating methotrexate alleviates imiquimod-induced psoriasiform dermatitis via decreasing IL-17-producing gamma delta T cells. Exp Dermatol. 2014;23(7):492–496. doi:10.1111/exd.12448
23. Chandra A, Aggarwal G, Manchanda S, Narula A. Development of topical gel of methotrexate incorporated ethosomes and salicylic acid for the treatment of psoriasis. Pharm Nanotechnol. 2019;7(5):362–374. doi:10.2174/2211738507666190906123643
24. Fratoddi I, Benassi L, Botti E, et al. Effects of topical methotrexate loaded gold nanoparticle in cutaneous inflammatory mouse model. Nanomedicine. 2019;17:276–286. doi:10.1016/j.nano.2019.01.006
25. Lakshmi PK, Devi GS, Bhaskaran S, Sacchidanand S. Niosomal methotrexate gel in the treatment of localized psoriasis: Phase I and Phase II studies. Indian J Dermatol Venereol Leprol. 2007;73(3):157–161. doi:10.4103/0378-6323.32709
26. Limón D, Talló Domínguez K, Garduño-Ramírez ML, Andrade B, Calpena AC, Pérez-García L. Nanostructured supramolecular hydrogels: towards the topical treatment of Psoriasis and other skin diseases. Colloids Surf B Biointerfaces. 2019;181:657–670. doi:10.1016/j.colsurfb.2019.06.018
27. Özcan A, Sahin D, Impellizzieri D, et al. Nanoparticle-coupled topical methotrexate can normalize immune responses and induce tissue remodeling in psoriasis. J Invest Dermatol. 2020;140(5):1003–14.e8. doi:10.1016/j.jid.2019.09.018
28. Panonnummal R, Sabitha M. Anti-psoriatic and toxicity evaluation of methotrexate loaded chitin nanogel in imiquimod induced mice model. Int J Biol Macromol. 2018;110:245–258. doi:10.1016/j.ijbiomac.2017.10.112
29. Rajitha P, Shammika P, Aiswarya S, Gopikrishnan A, Jayakumar R, Sabitha M. Chaulmoogra oil based methotrexate loaded topical nanoemulsion for the treatment of psoriasis. J Drug Deliv Sci Technol. 2019;49:463–476. doi:10.1016/j.jddst.2018.12.020
30. Vanaja K, Rani RHS, Sacchidananda S. Formulation and clinical evaluation of ultradeformable liposomes in the topical treatment of psoriasis. Clin Res Regul Aff. 2008;25(1):41–52. doi:10.1080/10601330701885116
31. Alves CO, Novaes RD, Bernardes M, et al. Evaluation of methotrexate-loaded surfactants, ceramides and cholesterol-based lamellar phases as a topical treatment for psoriasis. J Pharm Pharmacol. 2022;74(9):1342–1352. doi:10.1093/jpp/rgac006
32. Asad MI, Khan D, Rehman AU, Elaissari A, Ahmed N. Development and in vitro/in vivo evaluation of ph-sensitive polymeric nanoparticles loaded hydrogel for the management of psoriasis. Nanomaterials. 2021;11(12):12. doi:10.3390/nano11123433
33. Bernardes M, Agostini SBN, Pereira GR, et al. Preclinical study of methotrexate-based hydrogels versus surfactant based liquid crystal systems on psoriasis treatment. Eur J Pharm Sci. 2021;165:105956. doi:10.1016/j.ejps.2021.105956
34. Rashid SA, Bashir S, Naseem F, Farid A, Rather IA, Hakeem KR. Olive oil based methotrexate loaded topical nanoemulsion gel for the treatment of imiquimod induced psoriasis-like skin inflammation in an animal model. Biology. 2021;10:11.
35. Xu J, Chen H, Chu Z, et al. A multifunctional composite hydrogel as an intrinsic and extrinsic coregulator for enhanced therapeutic efficacy for psoriasis. J Nanobiotechnology. 2022;20(1):155. doi:10.1186/s12951-022-01368-y
36. Yang X, Tang Y, Wang M, et al. Co-delivery of methotrexate and nicotinamide by cerosomes for topical psoriasis treatment with enhanced efficacy. Int J Pharm. 2021;605:120826. doi:10.1016/j.ijpharm.2021.120826
37. Ali MFM, Salah M, Rafea M, Saleh N. Liposomal Methotrexate hydrogel for treatment of localized psoriasis: preparation, characterization and laser targeting. Med Sci Monit. 2008;14(12):I66–I74.
38. Andanooru Chandrappa NK, Channakeshavaiah Ravikumar B, Rangegowda SM. Iontophoretic delivery of methotrexate in the treatment of palmar psoriasis: a randomised controlled study. Australas J Dermatol. 2020;61(2):140–146. doi:10.1111/ajd.13228
39. Du H, Liu P, Zhu J, et al. Hyaluronic acid-based dissolving microneedle patch loaded with methotrexate for improved treatment of psoriasis. ACS Appl Mater Interfaces. 2019;11(46):43588–43598. doi:10.1021/acsami.9b15668
40. Haseena K, George S, Riyaz N, Sasidharanpillai S, Puthussery P. Methotrexate iontophoresis versus coal tar ointment in palmoplantar psoriasis: a pilot study. Indian J Dermatol Venereol Leprol. 2017;83(5):569–573. doi:10.4103/ijdvl.IJDVL_185_16
41. Ramez SA, Soliman MM, Fadel M, et al. Novel methotrexate soft nanocarrier/fractional erbium YAG laser combination for clinical treatment of plaque psoriasis. Artif Cells Nanomed Biotechnol. 2018;46(sup1):996–1002. doi:10.1080/21691401.2018.1440236
42. Tiwari SB, Kumar BC, Udupa N, Balachandran C. Topical methotrexate delivered by iontophoresis in the treatment of recalcitrant psoriasis--A case report. Intl J Dermatol. 2003;42(2):157–159. doi:10.1046/j.1365-4362.2003.01718.x
43. Wang Y, Fu S, Lu Y, et al. Chitosan/hyaluronan nanogels co-delivering methotrexate and 5-aminolevulinic acid: a combined chemo-photodynamic therapy for psoriasis. Carbohydr Polym. 2022;277:118819. doi:10.1016/j.carbpol.2021.118819
44. Choudhary P, Mehta RD, Ghiya BC, Sharma D. Treatment of nail psoriasis with intramatrical methotrexate: an uncontrolled prospective study of 20 patients. J Am Acad Dermatol. 2021;84(2):526–528. doi:10.1016/j.jaad.2020.04.159
45. Duarte AA, Carneiro GP, Murari CM, Jesus LCB. Nail psoriasis treated with intralesional methotrexate infiltration. An Bras Dermatol. 2019;94(4):491–492. doi:10.1590/abd1806-4841.20198170
46. Grover C, Daulatabad D, Singal A. Role of nail bed methotrexate injections in isolated nail psoriasis: conventional drug via an unconventional route. Clin Exp Dermatol. 2017;42(4):420–423. doi:10.1111/ced.13087
47. Jindal A, Ramesh S, Noronha M, Pai K, Pai S. Intramatricial methotrexate for treatment of resistant acrodermatitis continua of Hallopeau: an alternative in COVID-19. Dermatol Ther. 2020;33(4):e13787. doi:10.1111/dth.13787
48. Mittal J, Mahajan BB. Intramatricial injections for nail psoriasis: an open-label comparative study of triamcinolone, methotrexate, and cyclosporine. Indian J Dermatol Venereol Leprol. 2018;84(4):419–423. doi:10.4103/ijdvl.IJDVL_73_16
49. Mokni S, Ameur K, Ghariani N, et al. A case of nail psoriasis successfully treated with intralesional methotrexate. Dermatol Ther (Heidelb). 2018;8(4):647–651. doi:10.1007/s13555-018-0261-2
50. Saricaoglu H, Oz A, Turan H. Nail psoriasis successfully treated with intralesional methotrexate: case report. Dermatology. 2011;222(1):5–7. doi:10.1159/000323004
51. Abdelmeniem IM, El Eryan IM, Nofal A, Fouda I, Omar SS. Topical calcipotriol combined with urea 20% versus intralesional injection of triamcinolone acetonide, 5-fluorouracil, and methotrexate in the treatment of nail psoriasis: a comparative study. Dermatol Ther. 2022;35(9):e15660. doi:10.1111/dth.15660
52. Alakad R, Nassar A, Atef H, Eldeeb F. Fractional CO2 laser-assisted delivery versus intralesional injection of methotrexate in psoriatic nails. Dermatol Surg. 2022;48(5):539–544. doi:10.1097/DSS.0000000000003418
53. Starace M, Alessandrini A, Iorizzo M, et al. A pilot study of intralesional methotrexate injections versus triamcinolone acetonide in patients affected by nail matrix psoriasis. Clin Exp Dermatol. 2022;47(6):1165–1168. doi:10.1111/ced.15110
54. Haque T, Talukder MMU. Chemical enhancer: a simplistic way to modulate barrier function of the stratum corneum. Adv Pharm Bull. 2018;8(2):169–179. doi:10.15171/apb.2018.021
55. Songkro S. An overview of skin penetration enhancers: penetration enhancing activity, skin irritation potential and mechanism of action. Songklanakarin J Sci Technol. 2009;31(3):299–321.
56. Celleno L. Topical urea in skincare: a review. Dermatol Ther. 2018;31(6):e12690. doi:10.1111/dth.12690
57. Kulkarni VS, Shaw C. Chapter 5 - Use of polymers and thickeners in semisolid and liquid formulations. In: Kulkarni VS, Shaw C, editors. Essential Chemistry for Formulators of Semisolid and Liquid Dosages. Boston: Academic Press; 2016:43–69.
58. Desai P, Patlolla RR, Singh M. Interaction of nanoparticles and cell-penetrating peptides with skin for transdermal drug delivery. Mol Membr Biol. 2010;27(7):247–259. doi:10.3109/09687688.2010.522203
59. Pradhan M, Alexander A, Singh MR, et al. Understanding the prospective of nano-formulations towards the treatment of psoriasis. Biomed Pharmacother. 2018;107:447–463. doi:10.1016/j.biopha.2018.07.156
60. Carita AC, Eloy JO, Chorilli M, Lee RJ, Leonardi GR. Recent advances and perspectives in liposomes for cutaneous drug delivery. Curr Med Chem. 2018;25(5):606–635. doi:10.2174/0929867324666171009120154
61. Wadhwa S, Garg V, Gulati M, Kapoor B, Singh SK, Mittal N. Nanovesicles for nanomedicine: theory and practices. In: Weissig V, Elbayoumi T, editors. Pharmaceutical Nanotechnology: Basic Protocols. New York: Springer New York; 2019:1–17.
62. Nayak N, Somanna P, Patil AB, Radhakrishnan A. Progress in novel ultradeformable vesicular drug carrier in the topical and transdermal treatment of psoriasis. Ther Deliv. 2020;11(12):807–819. doi:10.4155/tde-2020-0081
63. Kazi KM, Mandal AS, Biswas N, et al. Niosome: a future of targeted drug delivery systems. J Adv Pharm Technol Res. 2010;1(4):374–380. doi:10.4103/0110-5558.76435
64. Opatha SAT, Titapiwatanakun V, Chutoprapat R. Transfersomes: a promising nanoencapsulation technique for transdermal drug delivery. Pharmaceutics. 2020;12(9):855. doi:10.3390/pharmaceutics12090855
65. Salvi VR, Pawar P. Nanostructured lipid carriers (NLC) system: a novel drug targeting carrier. J Drug Deliv Sci Technol. 2019;51:255–267. doi:10.1016/j.jddst.2019.02.017
66. Vincent N, Ramya DD, Vedha HB. Progress in psoriasis therapy via novel drug delivery systems. Dermatol Rep. 2014;6(1):5451. doi:10.4081/dr.2014.5451
67. Majumder J, Taratula O, Minko T. Nanocarrier-based systems for targeted and site specific therapeutic delivery. Adv Drug Deliv Rev. 2019;144:57–77. doi:10.1016/j.addr.2019.07.010
68. Venditti I. Morphologies and functionalities of polymeric nanocarriers as chemical tools for drug delivery: a review. J King Saud Univ Sci. 2019;31(3):398–411. doi:10.1016/j.jksus.2017.10.004
69. Neamtu I, Rusu AG, Diaconu A, Nita LE, Chiriac AP. Basic concepts and recent advances in nanogels as carriers for medical applications. Drug Deliv. 2017;24(1):539–557. doi:10.1080/10717544.2016.1276232
70. Pavoni L, Perinelli DR, Bonacucina G, Cespi M, Palmieri GF. An overview of micro- and nanoemulsions as vehicles for essential oils: formulation, preparation and stability. Nanomaterials. 2020;10(1):1. doi:10.3390/nano10010135
71. Nastiti CMRR, Ponto T, Abd E, Grice JE, Benson HAE, Roberts MS. Topical nano and microemulsions for skin delivery. Pharmaceutics. 2017;9(4):37. doi:10.3390/pharmaceutics9040037
72. Erdal MS, Özhan G, Mat MC, Özsoy Y, Güngör S. Colloidal nanocarriers for the enhanced cutaneous delivery of naftifine: characterization studies and in vitro and in vivo evaluations. Int J Nanomedicine. 2016;11:1027–1037. doi:10.2147/IJN.S96243
73. Sharma AK, Garg T, Goyal AK, Rath G. Role of microemulsions in advanced drug delivery. Artif Cells Nanomed Biotechnol. 2016;44(4):1177–1185. doi:10.3109/21691401.2015.1012261
74. Kale S, Deore SL. Emulsion micro emulsion and nano emulsion: a review. Sys Rev Pharm. 2016;8(1):39–47. doi:10.5530/srp.2017.1.8
75. Özcan A, Bunton D, Macluskie G, Duric M, Barry J, Kolios A. Topical methotrexate gold nanoparticles reduce imiquimod-induced inflammation in mice. Br J Dermatol. 2017;177(5):e244–e5.
76. Rajak P, Nath L, Bhuyan B. Liquid crystals: an approach in drug delivery. Indian J Pharm Sci. 2019;81:32.
77. Nalone L, Marques C, Costa S, Souto EB, Severino P. Chapter 7 - Liquid crystalline drug delivery systems. In: Shegokar R, editor. Drug Delivery Trends. Elsevier; 2020:141–149.
78. Wenande E, Anderson RR, Haedersdal M. Fundamentals of fractional laser-assisted drug delivery: an in-depth guide to experimental methodology and data interpretation. Adv Drug Deliv Rev. 2020;153:169–184. doi:10.1016/j.addr.2019.10.003
79. Lang K, Schulte KW, Ruzicka T, Fritsch C. Aminolevulinic acid (Levulan) in photodynamic therapy of actinic keratoses. Skin Therapy Lett. 2001;6(10):1–2, 5.
80. Shah B, Surti N, Misra A. 12 - Other routes of protein and peptide delivery: transdermal, topical, uterine, and rectal. In: Misra A, editor. Challenges in Delivery of Therapeutic Genomics and Proteomics. London: Elsevier; 2011:623–671.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.