")
Back to Journals » Journal of Blood Medicine » Volume 9
Thalassemia minor presenting with vitamin B12 deficiency, paraparesis, and microcytosis
Authors Lardhi A, Alhaj Ali R , Ali R, Mohammed T
Received 25 January 2018
Accepted for publication 29 May 2018
Published 4 September 2018 Volume 2018:9 Pages 141—144
DOI https://doi.org/10.2147/JBM.S163722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin Bluth
Arwa Lardhi, 1 Rania Alhaj Ali, 1 Rola Ali, 2 Tarek Mohammed 1
1Internal Medicine Department, Doctor Soliman Fakeeh Hospital, Jeddah, Saudi Arabia; 2An-Najah National University, Nablus, West Bank, Palestine
Abstract: Vitamin B 12 is essential for proper neurological functioning, and its deficiency may cause a wide range of neuropsychiatric and hematological manifestations. We report a case of a previously healthy 32-year-old female who was admitted to our hospital with sudden onset of bilateral lower limb paraparesis and loss of sensation. The serum level of vitamin B 12 was mildly decreased with high methylmalonic acid and homocysteine levels. However, her complete blood count showed no evidence of anemia or macrocytosis; instead, her mean corpuscular volume was low. Hemoglobin electrophoresis showed thalassemia trait, and that probably masked the megaloblastic features of vitamin B 12 deficiency. She responded fully to vitamin B 12 replacement therapy.
Keywords: thalassemia trait, microcytosis, pernicious anemia, paraparesis, cobalamin deficiency
Corrigendum for this paper has been published
Background
Vitamin B12 is classified as a water-soluble vitamin that is fundamental for cellular metabolism and appropriate nervous system functioning. Vitamin B12 deficiency can lead to inefficient erythropoiesis, megaloblastic anemia, and neuropsychiatric manifestations such as neuropathy, myelopathy, depression, and dementia.1
Vitamin B12 level is generally evaluated in patients with macrocytic anemia; however, it ought to be remembered that its deficiency in some individuals could be unacknowledged due to other associated conditions as thalassemia minor or iron deficiency that would conceal the macrocytosis.2
We present a case of vitamin B12 deficiency presenting with sudden onset of paraparesis, normal hemoglobin level, and low mean corpuscular volume (MCV) and mean corpuscular hemoglobin (MCH).
Case report
A 32-year-old female patient, who was not known to have any medical illness, presented to the emergency with sudden onset of lower limbs paraparesis. She was in her usual state of health until 2 weeks back when she started to complain of recurrent attacks of vertigo, vomiting, and generalized weakness. The patient was not able to move her lower limbs, stand, or walk. It was associated with sensory loss.
There was no history of trauma, visual or speech disorder, or change in her mental status. No suggestive history of autoimmune disease or focus of infection or any source of bleeding was demonstrated. There was no history of change in weight or bowel habits, and she denied any alcohol intake or illicit drug consumption. She was not vegetarian, and there was no drug history.
On physical examination, the patient was pale but not jaundiced. She was conscious, alert, and oriented to place, person, and time. Upon neurological examination, all cranial nerves were intact. The patient was not able to stand or move her lower limbs, with hypotonia, loss of sensation and proprioception, and a power rating of 0/5. On the other hand, her upper limbs had normal tone, intact sensation, and a power rating of 5/5. Reflexes were normal in upper and lower limbs. Babinski sign was negative. Cerebellar examination was normal except for shin-to-heel test and gait, which could not be evaluated. The rest of the examination was unremarkable.
All initial laboratory investigations are shown in Table 1. The patient’s hemoglobin electrophoresis was diagnostic for thalassemia trait. Her vitamin B12 level was low with high methylmalonic acid and homocysteine.
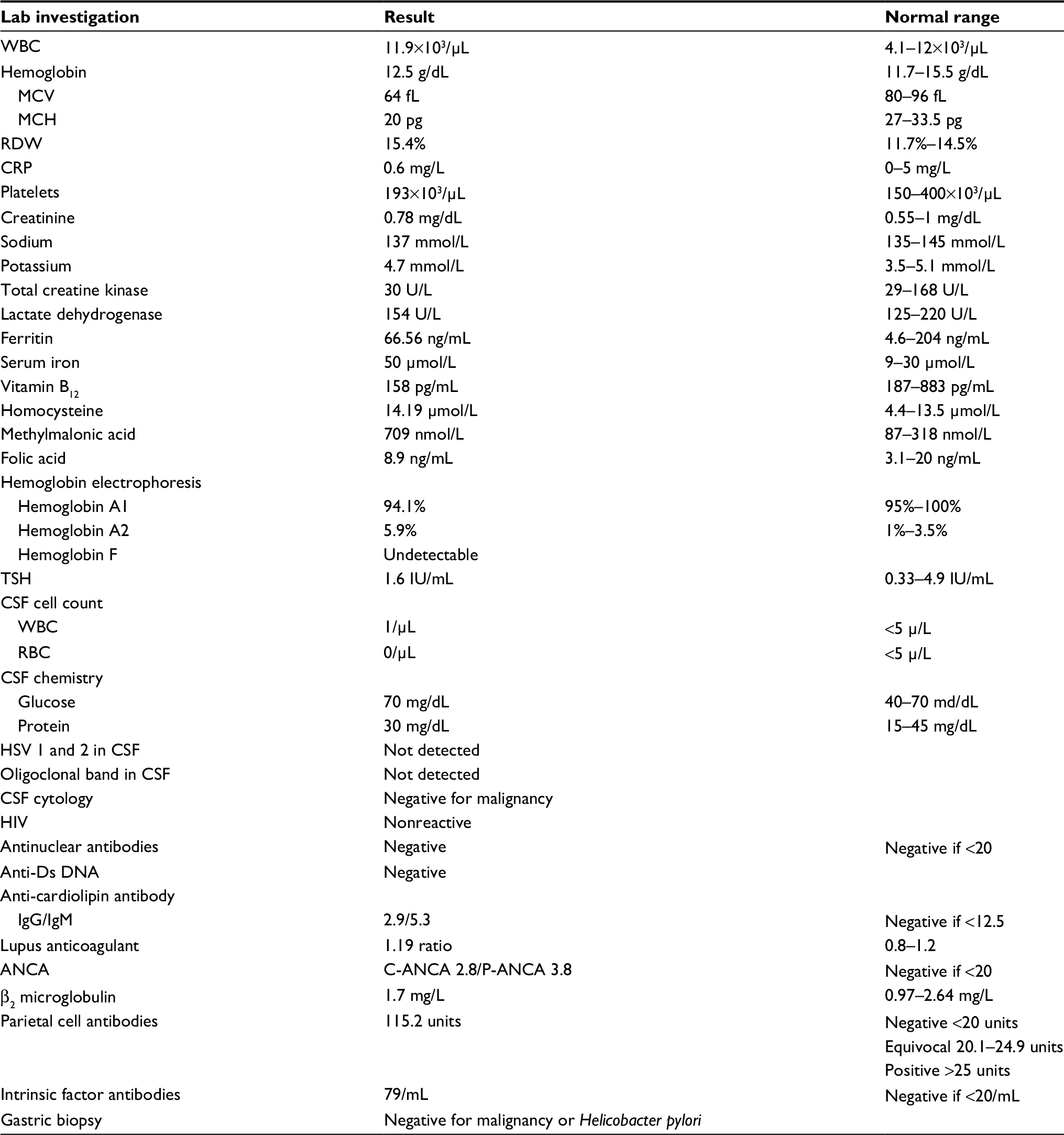 | Table 1 Lab investigations at time of presentation Abbreviations: ANCA, antineutrophil cytoplasmic antibody; CSF, cerebrospinal fluid; CRP, C-reactive protein; HSV, herpes simplex virus; MCH, mean corpuscular hemoglobin; MCV, mean corpuscular volume; RBC, red blood count; RDW, red blood cell distribution width; TSH, thyroid stimulating hormone; WBC, white blood count. |
Lumbar puncture was done, and the analysis was normal. Herpes simplex and oligoclonal antibodies in cerebrospinal fluid (CSF) were negative. MRI of the brain and whole spine was normal. Nerve conduction study was normal.
The patient was initially managed as Guillain Barre syndrome and was prescribed 5 doses of intravenous immunoglobulin. By the end of the investigation, the diagnosis of vitamin B12 deficiency was established, and the patient was started on 1 mg of intravenous methylcobalamin (1,000 µg) daily for 10 days, followed by 1 mg intramuscular injection once weekly for another month.
The patient showed immediate response by gradually gaining back her sensation. Therefore, she was discharged with prescription of intramuscular vitamin B12 weekly for 2 months and physiotherapy.
One month after commencing treatment, she showed marked improvement in her symptoms and was able to walk with minimal assistance. Neurological examination showed power of 4/5 and mildly decreased sensation in the lower limbs. After 2 months of weekly vitamin B12 therapy, she was finally able to walk without assistance.
Eventually, she was diagnosed with pernicious anemia following gastritis on upper endoscopy. A trial of oral vitamin B12 was tried, but she failed the treatment because of recurrence of her previous symptoms. Patient resumed her intramuscular injections with complete resolution of symptoms, and she is maintained on a lifelong monthly vitamin B12 injection therapy.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report. A copy of the written consents is available for review by the Editor-in-Chief of this journal.
Discussion
We report a case of cobalamin deficiency in which the diagnosis was delayed because of concomitant thalassemia trait. She was admitted due to sudden-onset lower limb paraparesis and sensory loss. The hemoglobin level was normal with microcytosis and mildly low vitamin B12 level. After treatment with B12 injections, the patient regained her normal functional status.
Vitamin B12 cannot be synthesized in the body; instead it should be ingested from exogenous sources. It is absorbed mainly in the terminal ileum, and its uptake requires an intrinsic factor that is synthesized by gastric parietal cells.3 Cobalamin is essential for DNA synthesis, erythropoiesis, and the formation and maintenance of myelin sheath. It functions as a cofactor for methionine synthase and l-methylmalonyl-CoA mutase. A deficiency thereby causes elevated homocysteine and methylmalonic acid,4 as was shown in this patient. Such cases can help in early detection of vitamin B12 deficiency as 50% of the patients might have normal B12 levels in the blood.5 Vitamin B12 deficiency also has a secondary effect on the enterocytes, leading to more loss of iron storage.6
Pernicious anemia is characterized by chronic atrophic gastritis and is the most common cause of vitamin B12 deficiency. The gastritis results in the loss of parietal cells in the fundus and body of the stomach due to the presence of specific autoantibodies.7,8 Two types of antibodies were described, parietal cells and intrinsic factor. The sensitivity of these antibodies in diagnosing pernicious anemia is 90% and 60%, respectively.9 Upper endoscopy in the case presented showed gastritis with positive antibodies. Therefore, upper endoscopy should be part of the diagnostic workup of vitamin B12 deficiency.
Multiple factors can lead to misdiagnosis of vitamin B12 deficiency. Many physicians and healthcare providers overlook cobalamin deficiency until the patient develops macrocytic anemia, which is often a late sign of advanced vitamin B12 disease.10 Relying on MCV alone to rule out vitamin B12 is not sufficient, as it lacks the sensitivity and specificity for cobalamin deficiency, especially with concurrent conditions such as iron deficiency anemia or thalassemia trait. These conditions lead to absence of macrocytosis; therefore, MCV should not be the only parameter used to diagnose vitamin B12 deficiency.11,12 Another important element that can lead to misdiagnosis of cobalamin deficiency is the absence of anemia despite low levels of vitamin B12, as was shown in a previous study in which only 21.5% of the patients had anemia.13
The patient presented here initially had microcytosis, and thalassemia trait was ultimately diagnosed in this case. Probably this misled the physicians to think of vitamin B12 deficiency as a cause of her paraparesis that led to unnecessary invasive procedures and invasive management. Normal vitamin level is one of many conditions that might lead to underdiagnosed B12 deficiency, and that is why physicians need to check methylmalonic acid and homocysteine levels before excluding B12 deficiency.
Vitamin B12 deficiency has been largely ignored in favor of other relevant diagnoses such as diabetic neuropathy, multiple sclerosis, Guillain Barre syndrome, and major depression. Thus, considering an early diagnosis and promptly initiating treatment is critical to prevent permanent neurologic disability and poor outcomes. Our center reported a similar case of a middle-aged man who was initially diagnosed with organic mood disorder but did not improve on antipsychotics. After further diagnostic workup, severe vitamin B12 deficiency was identified and he responded to cobalamin replacement therapy.14
As common as vitamin B12 deficiency may be, it is possible sometimes for it to be overlooked. The purpose of this case report is to show that vitamin B12 deficiency should be considered in the differential diagnosis in patients presenting with paralysis, even in the absence of macrocytosis. It emphasizes the fact that increased MCV is a hallmark in vitamin B12 deficiency, but it is not an obligatory sign. Vitamin B12 deficiency is a reversible condition; nonetheless, delaying the management can lead to irreversible complications. Consequently, awareness of this fact is vital in early detection, treatment, and prevention.
Disclosure
The authors report no conflicts of interest in this work.
References
Kumar N. Neurologic aspects of cobalamin (B12) deficiency. Handb Clin Neurol. 2014;120:915–926. | ||
Spivak JL. Masked megaloblastic anemia. Arch Intern Med. 1982;142(12):2111–2114. | ||
Hunt A, Harrington D. Vitamin B12 deficiency. BMJ. 2014;349:g5226. | ||
Ueland PM, Schneede J. [Measurement of methylmalonic acid, homocysteine and methionine in cobalamin and folate deficiencies and homocysteinuria]. Tidsskr Nor Laegeforen. 2008;128(6):690–693. Norwegian. | ||
Oh R, Brown DL. Vitamin B12 deficiency. Am Fam Physician. 2003;67(5):979–986. | ||
Stabler SP. Clinical practice. Vitamin B12 deficiency. N Engl J Med. 2013;368(2):149–160. | ||
Pruthi RK, Tefferi A. Pernicious anemia revisited. Mayo Clin Proc. 1994;69(2):144–150. | ||
Toh BH, van Driel IR, Gleeson PA. Pernicious anemia. N Engl J Med. 1997;337(20):1441–1448. | ||
Bizzaro N, Antico A. Diagnosis and classification of pernicious anemia. Autoimmun Rev. 2014;13(4–5):565–568. | ||
Bilic E, Bilic E, Zagar M, Juric S. Masked deficit of vitamin B12 in the patient with heterozygous β-thalassemia and spastic paraparesis. Acta Neurol Belg. 2004;104(4):173–175. | ||
Oosterhuis WP, Niessen RW, Bossuyt PM, Sanders GT, Sturk A. Diagnostic value of the mean corpuscular volume in the detection of vitamin B12 deficiency. Scand J Clin Lab Invest. 2000;60(1):9–18. | ||
Snow CF. Laboratory diagnosis of vitamin B12 and folate deficiency: a guide for the primary care physician. Arch Intern Med. 1999;159(12):1289–1298. | ||
Kara A, Eliacik E, Buyukasik Y, et al. Vitamin B12 deficiency with the absence of anemia in young and middle-aged population. Int J Hematol Oncol. 2014;3(24):190–194. | ||
Almoallim H, Mehdawi FS, Cheikh MM, Al-Dhaheri F, Aqeel AM. Reversible vitamin B12 deficiency presenting with acute dementia, paraparesis, and normal hemoglobin. Case Rep Neurol Med. 2016;2016:4301769. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.