")
Back to Journals » Medical Devices: Evidence and Research » Volume 11
Tensometric tremorography in high-precision medical diagnostic systems
Authors Aleksanyan Z, Bureneva O , Safyannikov N
Received 21 March 2018
Accepted for publication 12 May 2018
Published 13 September 2018 Volume 2018:11 Pages 321—330
DOI https://doi.org/10.2147/MDER.S168831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zoya Aleksanyan,1 Olga Bureneva,2 Nikolay Safyannikov2
1Institute of the Human Brain, Russian Academy of Sciences, Saint Petersburg, Russia; 2Department of Computer Science and Engineering, Saint-Petersburg State Electrotechnical University “LETI”, Saint Peterburg, Russia
Background: The objective of the study was to develop a system for the precision diagnostics of pathologies of motor brain regions based on tensometric measurement and to explore its diagnostic capabilities.
Materials and methods: Tremor is a syndrome that indicates the abnormal state of the central nervous system, primarily in the motor brain regions. Analysis of tremor parameters provides significant information about the changes in the body motion control and can be used as an objective index of the central nervous system state. Existing methods are aimed at the analysis of visible tremor based on the use of different sensors. We suggest an alternative approach based on the use of a tensometric system performing tremor measurements when the tremor appears on the background of voluntary isometric efforts. The key advantage of our approach is that it allows to determine the tremor before its visible manifestation. In the article, we describe hardware implementation of our tremor analysis system.
Results: In the article, we represent the new methodology and the original equipment based on the control of isometric effort. Isometric effort formed by a patient is controlled with the use of a feedback system on the patient’s monitor. We evaluated the performance of our equipment with more than 400 healthy volunteers and patients with various pathologies of the central nervous system motor regions, and the results of the investigations, allowing to identify tremor parameters typical for parkinsonism, are represented in our article.
Conclusion: Testing of the system confirmed its high diagnostic validity and reliability, high sensitivity, simplicity and high speed of information processing. The approach based on tensometric measurements is very promising for the diagnostics of Parkinson disease and dysfunctions of a central nervous system.
Keywords: isometric method, hands oscillations, biological feedback, precision diagnostics, tremor
Introduction
One of central nervous system state demonstrations, including pathologic ones, is tremor, defined as a rhythmical involuntary oscillatory movement of at least one of functional body regions.1
Different levels and mechanisms of the nervous system’s damage lead to relatively similar tremor manifestation, so the task of tremor’s cause discovery is not easy. Pathological tremor is the most frequent hyperkinesis that can emerge either on its own or alongside other symptoms during various nervous system breakdowns, endocrine and somatic diseases and/or intoxications. In addition, each person has physiological tremor that cannot be seen with the naked eyes due to its negligible amplitude, while it has its characteristic frequency. Under specific conditions, for instance, under the influence of adrenalin that is secreted because of fear or worry as well as in response to pharmacological stimulation, physiological tremor increases and becomes noticeable, but its frequency remains the same.2,3
Objective of study
Tremor is a complex process involving both central and peripheral central nervous system mechanisms. The most specific of changes in endogenous activity, appearing in case of motor structures’ central pathology, are identified as syndromes of different diseases. As a result, tremor parameter analysis enables us to get detailed information about the changes in different body systems, primarily in the motor regions of a brain, and can be used as an objective index of central nervous system state.4
Tremor can develop in different situations, so we distinguish between rest tremor and active one. The latter can be observed under voluntary muscle contraction conditions such as motions intended to posture maintaining (postural), muscle tension when their action is directed against a fixed object (isometric), and any purposeful and purposeless motion (kinetic).
The most frequent tremor type is essential tremor,5 typically occurring in 0.08–220 cases out of 1,000 people.6 It can be an independently inherited disease – essential tremor – and it can be “essential” trembling hyperkinesis. Another cause of tremor is Parkinson disease.7 There are three types of tremor observed during Parkinson disease, differing from each other with their frequency characteristics. Type 1 is classic parkinsonian rest tremor with 4–6 Hz frequency or rest tremor together with postural tremor of the same frequency. Type 2 is manifested by postural tremor of a higher frequency (up to 9 Hz) that can dominate over rest tremor. Type 3 is primarily postural tremor with 4–9 Hz frequency.
Precise differential diagnostics appears non-trivial.8 First, it derives from different neurological and somatic diseases that are associated with tremor. Second, quite similar tremor manifestations for different levels and pathogenetical mechanisms of the nervous system breakdown can often be observed. With around 30% of cases exhibiting diagnostic difficulties when defining nosologic nature of tremor by traditional measures, there is an urgent need for novel and precise methods and diagnostics equipment design.9,10
Modern research methods
Currently, various instrumental methods of tremor parameter assessment (tremorography) are being actively developed and implemented into clinical practice for the diagnostics of motor regions of the central nervous system, including mechanographic and electromyographic measurements, video registration-based methods, sensor network-based approaches, etc.
Modern solutions based on the mechanographic approach typically utilize a graphical digital tablet connected to a PC.11 However, the key disadvantage of this method is the difficulty of the measurement result interpretation due to the strong nonlinear dependence of motion on effort characterized by multiple factors that influence the test results.
Electromyographic measurements are based on the registration of the bioelectrical muscle activity that occurs under voluntary muscle contraction and tonic tension.12,13 Electromyographic measurements provide us with parameters such as wave amplitudes, frequency, duration and form of oscillations, thus enabling us to obtain detailed information about neurotransmission pathologies or muscle diseases, while providing only indirect information about biomechanical motions characteristics.
Video registration methods are used for the examining of a human limb motion path. They allow to perform research in vivo without the usual motion path distortions.14–16 However, video registration provides information only about visible disease symptoms.
Tremor parameter registration can be made with the use of different sensors17–21 such as force registration sensors, capacity sensors and sensors that register magnetic field ramp when in motion. However, in most cases only a particular type of tremor (rest tremor or action tremor) or only a specific parameter of hyperkinesis (only frequency) or relative amplitude is registered.
The majority of implementations require fastening onto a human body some sensor units, and their physical parameters, such as volume and weight, influence the measurement results. Besides that, in most cases wired electric connection with the recording and assessing equipment is needed.
The most common accelerometric sensors allow to examine biomechanics of human motions in vivo without the usual motion path distortion, assuming the use of special sensors – accelerometers that measure linear acceleration taking place during all movements.22–25 The drawback of the accelerometers use is connected with the influence of the human limb inertial mass on the results.
An alternative approach is provided by the tensometric measurement-based technique that is implemented with tensometric sensors mounted on a contact surface.26,27 They provide detailed information about motions by means of decreasing or increasing pressure. However, this method focuses on analyzing external symptoms and does not reveal latent forms of tremor.
Thus, existing methods are limited both in their applicability and accuracy, and there is an urgent need for novel and precise methods to increase the evaluation objectivity level of central nervous system motor regions states, thus improving the diagnostic accuracy.
Materials and methods
We suggest an approach to the tremor analysis based on isometric measurements.28 It implies separation of voluntary isometric effort from involuntary oscillations.
The approach is based on the idea of hierarchic multilevel organization of the central (motor) nervous system with the circular control on the basis of sensor corrections.29 The basis for these conceptions was set up by the founder of the modern biomechanics, N.A. Bernstein.30,31
It was discovered on the model of segmental level neuronal structures of muscle contraction control that cyclic activity is supported in a ring structure. Its frequency is defined by the length of uplink and downlink paths, excitement conduction speed and delay for signal processing in every functional brain area. It is deemed that out of all types of analyzed motions, the parameters of voluntary isometric effort provide the fullest information about the integral activity of motor system central structures.28
While moving, muscles can realize eccentric (stretching) or concentric (shortening) contractions; the third type of muscle contraction is isometric: muscles contract, but they do not change their length.32 Isometric load is made in a static position and on its background subconscious oscillatory muscle contractions appear actively. The obtained characteristics of isometric effort will contain information about its constant component and tremor. The following task will be to isolate constant and frequency components with the acquisition of their amplitude-frequency characteristics, and it will result in the frequency component allowing to estimate tremor parameters.33
Procedure for measurement of limbs’ involuntary oscillation parameters
The suggested approach can be realized by the following procedure. A person under test sits at a table placing his elbows on its surface and presses his fingers of both hands against appropriate platforms and controls his force on a monitor in front of him, as is shown in Figure 1. The marks for the right and left hands move along the vertical axis on the monitor, their travel being proportional to the applied force. The controlled forces are set by the operator in the range from minimal ones when the marks should not move from their initial location to maximal ones the patient can apply. The maximal force is limited to 20 kg. The operator specifies due efforts using the horizontal grid shown on the screen.
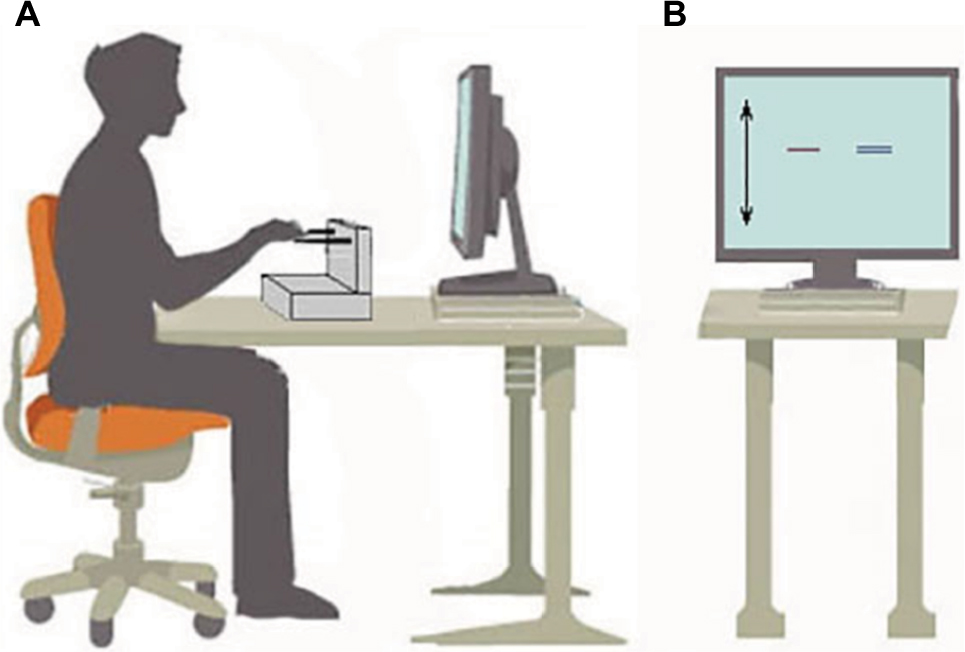 | Figure 1 Test process. Notes: (A) The person being tested sits in front of the monitor, rests with his elbows on the table and acts upon the measuring platform with his fingers, visually controlling the force by the marks on the monitor and (B) there are two marks on the monitor, one for the right hand and the other for the left; the marks move along the vertical axis. The effort level is set with the grid. |
The task of the tested person is to form the same forces by the right and left hands, ie, the marks on the screen should be on the same level. Stiffness of the measuring platforms must guarantee hands effort recording in the isometric mode, ie, without a visible displacement in the contact point of a hand and a measuring unit.
Hardware implementation of the system
The suggested approach is implemented by a tensometric system,34 the structure of which is shown in Figure 2, and corresponds to the suggested testing procedure.
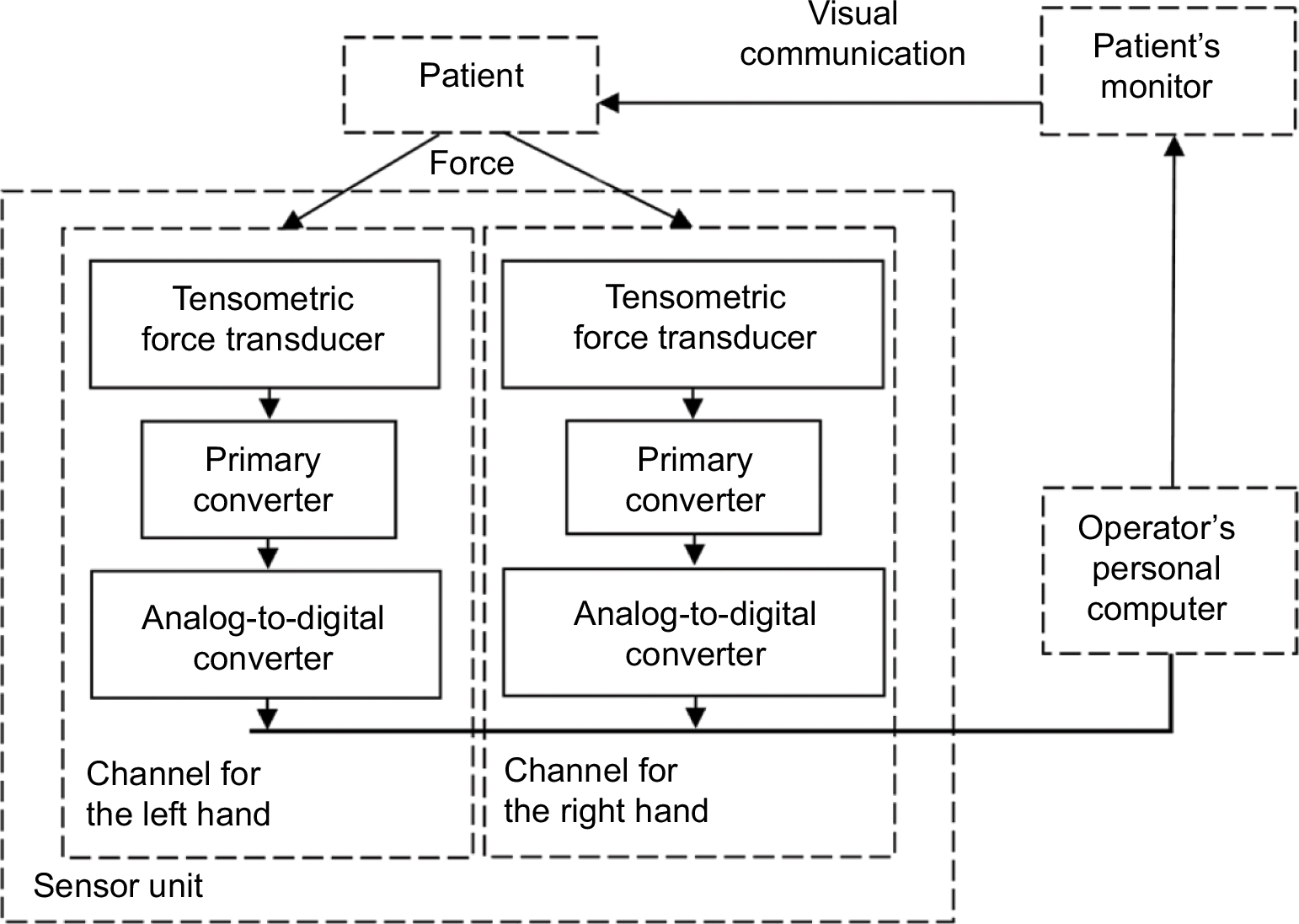 | Figure 2 The structure of the tensometric system and its interaction with a patient. |
The sensor unit provides a direct contact between a patient and a measuring system of the analytical gadget and senses oscillatory hands motions. The contact is made with the use of tensometric force transducers mounted on the platform; the force could be directed from the top downwards as well as from the bottom upwards.
The sensor unit is designed on the basis of two tensometric force transducers used for the analysis of tremor parameters for the left and right hands at the same time. They convert parameters of human limbs’ mechanical movements into electrical signals. Characteristics of voluntary efforts (consciously formed by a patient so as to hold the marks on the screen at the assigned level) and involuntary ones (tremor) are extracted from the signals with appropriate primary converters and transformed to digital form by analog-to-digital converters.
Digitized data pass to an operator’s personal computer where their mathematical processing is carried out. Besides that, the marks on the patient’s monitor are moved based on this data, ensuring visualization of the formed effort and the user’s feedback.
S-shaped tensometric sensors are used for retrieving information about the influence of patient’s hands. In accordance with the requirements imposed to the sensor unit and expected parameters of isometric efforts, they provide the analysis of both compression and stretching, accept the load up to 20 kg and have the sensitivity of 2.0/3.0 mV/V.
While conducting the tests the following parameters are recorded:
- Voluntary efforts, with the limit value of 20 kg
- Amplitude of oscillations
- Efforts made by involuntary hands oscillations primarily of periodic nature with significant oscillations in the 0–25 Hz range.
Recording of isometric effort parameters is made for both hands, and so there are two recording channels in the sensor unit.
The registering device transmits signals in the range from 0 Hz (constant current) to 150 Hz inclusive, with the dynamic range of encoded signal levels not less than 90 db.
Later on, the signal values characterizing voluntary effort will be digitized and used to display movement of the marks on the patient’s monitor, and the signal parameters characterizing involuntary force after digitizing will be used to determine the tremor parameters.
Options for diagnostic procedures
There are a variety of diagnostic procedures, for instance, recording of fingers efforts, which correspond to cortex component analysis, or of straightened arms that characterizes automatic posture regulation. In both cases, the activity in structures of the motion control system of a central nervous system is proportional to isometric muscle tension.
The patient receives a task of forming certain isometric effort, for example, of creating a maximum/minimum isometric effort when holding the marks of the right and left hands at the former place, or holding the marks on some specific level. The process of measurement starts; details of its passing and the copy of patient’s monitor are displayed on the operator’s personal computer monitor. The time of the test can range from 30 to 600 seconds. It is possible to disconnect biological feedback channel and to carry out diagnostic procedures without visual control of actions on the part of a patient.
Results
In accordance with the designed circuits, the prototype of the device was manufactured. Photo of the prototype of the hardware system implementing the method of tensometric tremorography is shown in Figure 3.
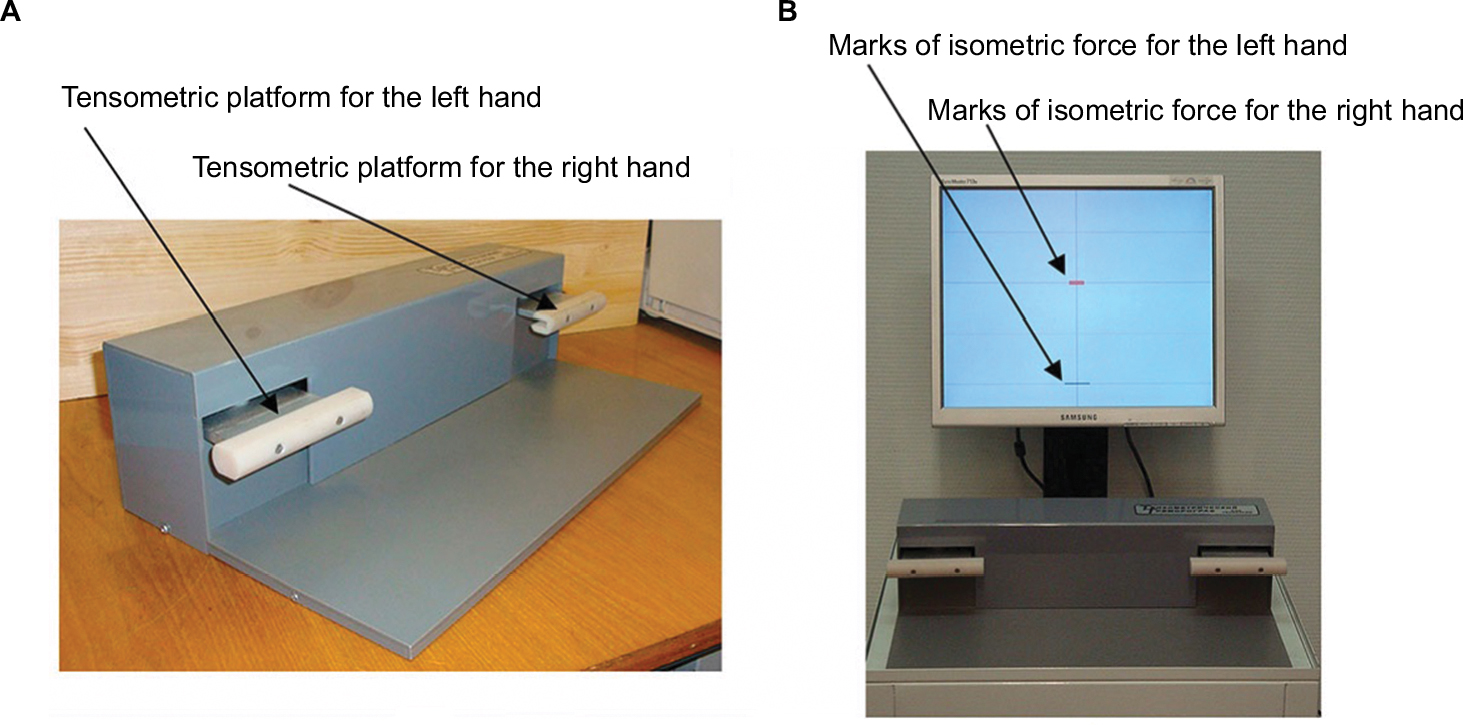 | Figure 3 Hardware system for tensometric tremorography. Notes: (A) Tensometric platform and (B) tensometric platform and patient’s monitor with the marks of isometric force. |
The prototype was used when carrying out tests for healthy people and patients with different pathologies of central nervous system motor regions. In total, 400 people have been examined. The written informed consent statement for taking part in the studies was received from all the examined people. Regulations for the test procedure were approved by the Medical Ethics Commission of the Institute of the Human Brain, Russian Academy of Sciences. The obtained results allowed to find out typical spectral characteristics of involuntary isometric forces for healthy people and people with various diseases. Typical plots of the spectral characteristics of a healthy person and a patient with the diagnosis of parkinsonism are shown in Figure 4.
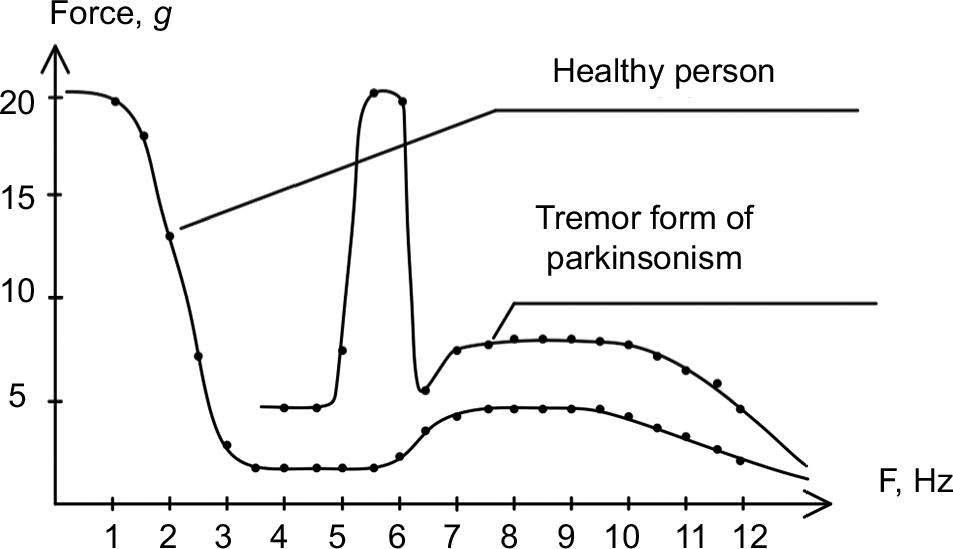 | Figure 4 Typical spectral characteristics of involuntary efforts for a healthy person and a patient with parkinsonism diagnosis. |
Normally, oscillatory amplitude of isometric effort does not exceed 2% of effort’s constant component. Significant oscillations are recorded in the 0–16 Hz range; the 0–2 Hz range is considered to be voluntary control for performing tracking movements. Automatic posture regulation corresponds to a frequency of more than 2 Hz. The amplitude of spectral components up to 3 Hz shrinks about 10 times, then it stays on the minimum level of 4–6 Hz range, after that it grows to the highest value of 7–10 Hz (with different tested people) and finally it shrinks to the background level with 12–14 Hz frequency and remains on the achieved level. Spectral components’ maxima in the 7–10 Hz range are less by more than one order than the amplitudes of spectral components in the 0–2 Hz range.
Under various pathologies, the picture can change.24 For example, under tremor form of parkinsonism, the higher level of activity in the whole frequency range is registered, with peak components in the 5–6 Hz range standing out against the background and having amplitude higher than the voluntary component in the range of 0–2 Hz. Under this and other forms of neurological disorders, the distribution of spectral components and the type of correlation functions change, thus reflecting disorder in cortical–subcortical interaction mechanisms.
Figure 5 shows 5-second record fragments of a held effort involuntary component, which are stored in the operator’s computer memory. For the estimation of central nervous system functional state, here are the examination results of a healthy 22-year-old person and also the results of the following patients: with symptomatic tremor diagnosis tangibly manifesting in the right hand, aged 68 years (patient 1), and with parkinsonian syndrome at the age of 72 years (patient 2).
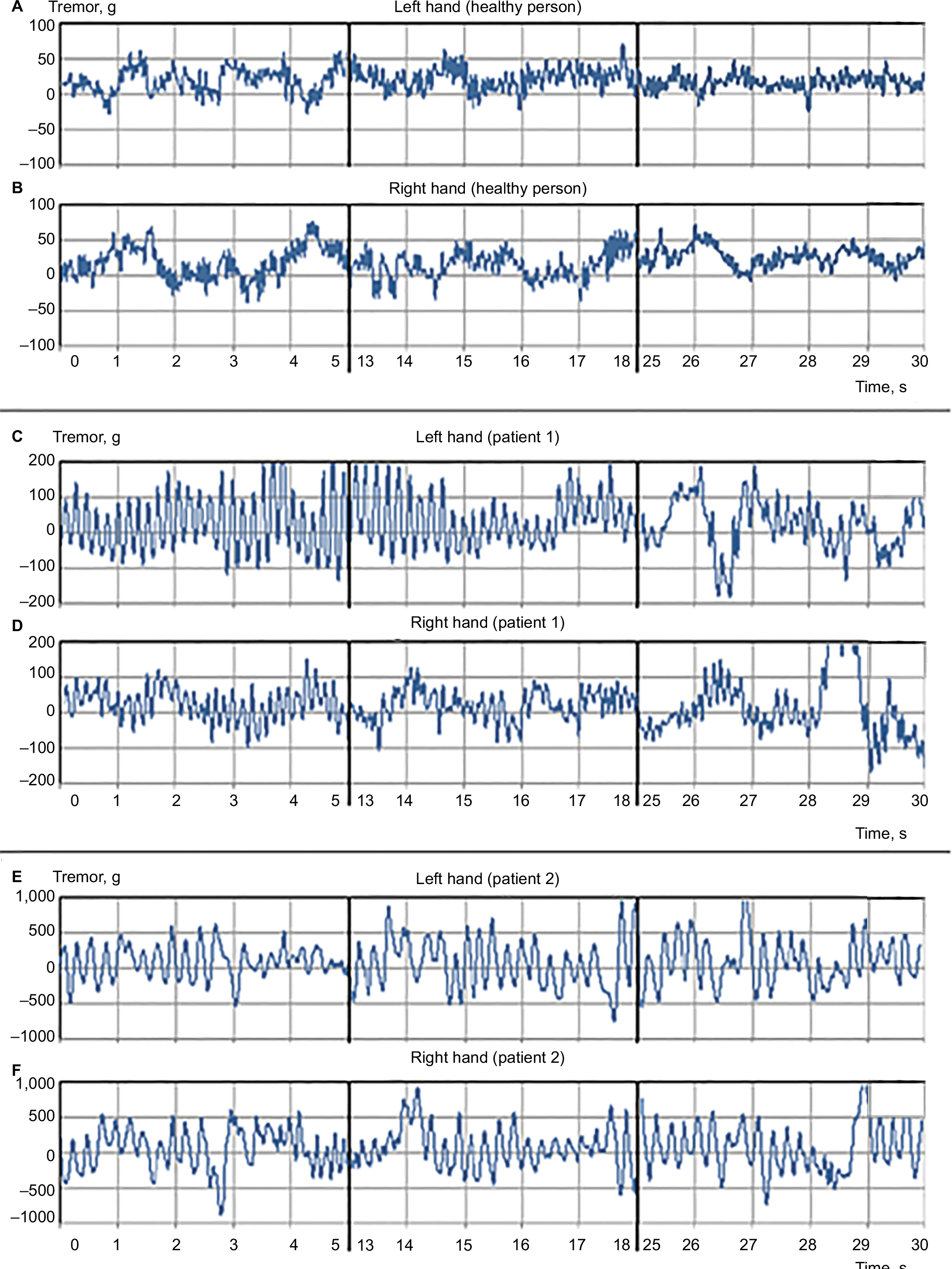 | Figure 5 Record fragments of a held effort involuntary component of a healthy person. Notes: (A) left hand, (B) right hand; of a patient with symptomatic tremor (patient 1): (C) left hand, (D) right hand; patient with parkinsonian syndrome (patient 2): (E) left hand, (F) right hand. |
The records are made with a 30-second held effort on a medium grading (~3 kg) and their 5-second fragments in different stages of the measurement process are demonstrated: at the beginning, in the middle and at the end, and they show a complex oscillation form, their wide frequency range, amplitude and possible oscillation asymmetry of involuntary component in the right and left limbs.
It is seen on the oscillograms that the estimation of a process over time allows to find out various manifestations of tremor:
- A healthy test person (Figure 5A and B), holding isometric effort, has tremor, but the tremor tends to calm down over the time.
- For a patient with symptomatic tremor diagnosis (Figure 5C and D), there is oscillation asymmetry between the right and left hands and distinctive decline of high-frequency tremor amplitude and asymmetry.
- For a patient with parkinsonian syndrome (Figure 5E and F), tremor is constantly present and it does not change fundamentally over the time.
Figure 6 displays statistics for 30-second recordings of isometric efforts of different gradations T1–T5 (T1 is minimal effort, T5 is the maximal one) while implementing standard tests for the arms straightened forwards and corresponding involuntary components.
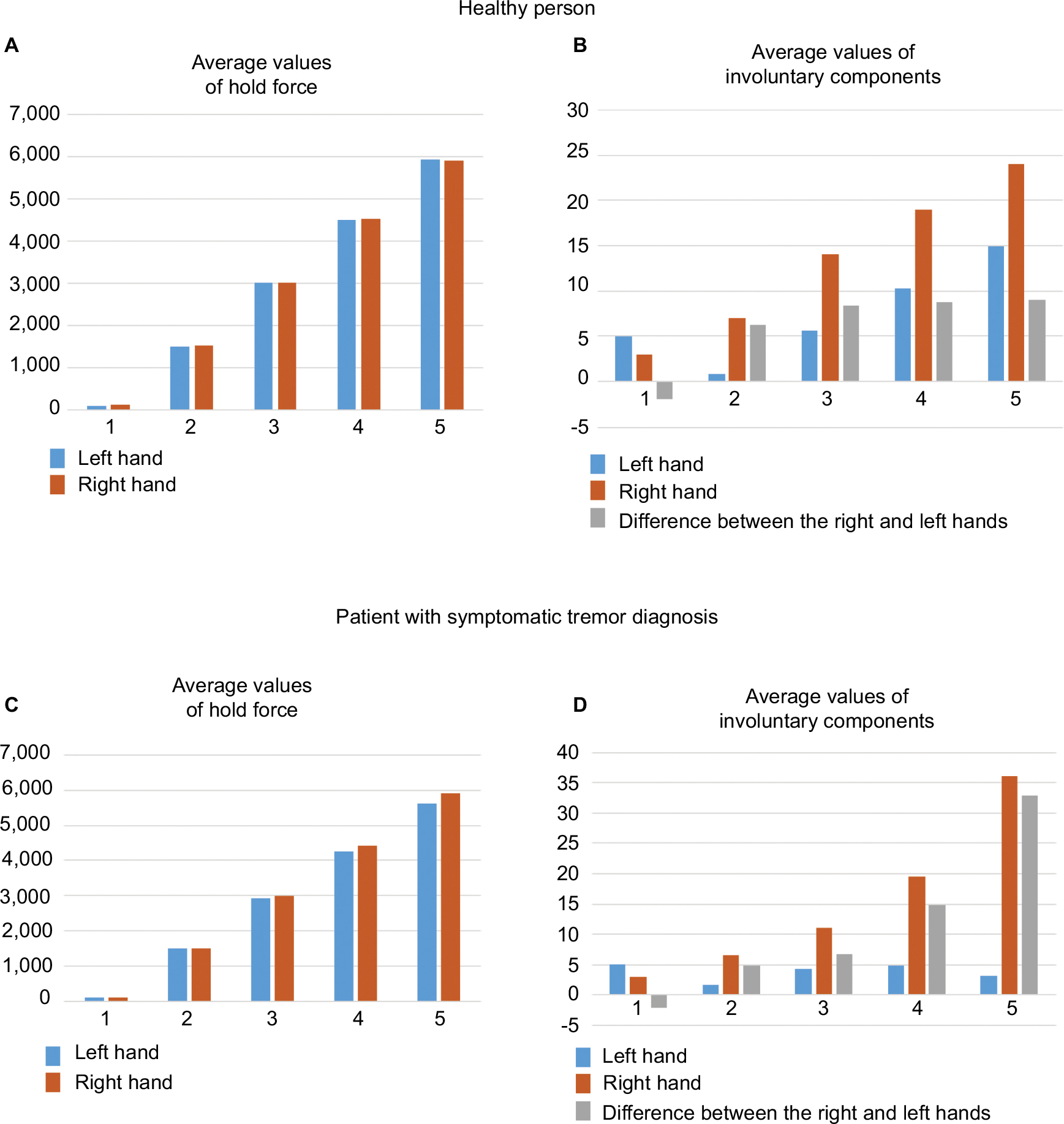 | Figure 6 Statistical diagrams of isometric efforts for the gradation T1–T5. Notes: (A and C) Average values of held efforts during the test time for a healthy person and a patient with symptomatic tremor diagnosis respectively, (B and D) average values of involuntary components accompanying the held efforts for a healthy person and a patient with symptomatic tremor diagnosis, respectively. The blue bars correspond to the readings received for the left hand, and the brown ones for the right. |
Statistical analysis characterizes average values of the efforts held during the test (Figure 6A and C), and average values of the accompanying involuntary components (Figure 6B and D).
The difference between average values of the held efforts while changing effort gradings T1–T5 is negligible. The difference between neighboring average values of corresponding involuntary components for a healthy person almost does not change beginning from the effort T2 (no more than 10 g), and for a patient with symptomatic tremor diagnosis in the whole range of efforts from T2 to T5 it has a strong nonlinear increase at the approach to the highest effort value (the difference is from 2 to 35 g).
Thus, the prototype’s tests showed that tensometric tremorography as a part of isometric measurements can be used in medical diagnostics systems.35
Discussion
Recording and analysis of motions, as mentioned in Introduction, form the basis of the known methods and devices, but do not allow an objective assessment of the brain’s control structures state. Using such methods allows only analyzing motions and characterizing them as pathologic or not.4,10,11,20,22 At the same time it is hard to differentiate the forms of tremor that occurs as a result of damage of different brain structures, as oscillations of body parts are mainly defined by the parameters of their inertia masses.8,9
The suggested accuracy increase is achieved not by the increase of the used sensors’ precision and specific signal processing hardware, but by a conceptually new way of organizing analytics: extraction of involuntary motion components out of the background of isometric efforts.28,34 It simplifies the system and later on will allow transmitting its implementation to the microsystem level, ie, minimize the hardware by designing it in the form of a system-on-chip.
The following development of the suggested solutions can be related to the extension of their application field. Along with functional diagnostics on the basis of medical centers, tensometric tremorography can be used in sports medicine for biomedical selection and for the admission to sports classes, for control over functional readiness of athlete’s organism and for load level correction. It can also be useful for the systems of professional selection for the personnel state estimation that works with technically challenging and dangerous objects.
Conclusion
The advantages of the suggested method of central nervous system functional state estimation based on isometric approach and its hardware realization using tensometric measurements are the following:
- High reliability provided by isometric measurements that exclude distortions of oscillation parameters appearing because of extra efforts for limbs inertial mass moving
- Opportunity of test procedure standardization due to the analysis of only one parameter
- Opportunity to discover a wide range of functional peculiarities and central nervous system motor region dysfunctions
- High sensitivity: the method allows recording of latent physiological tremor and pathological changes in the motion control system without visible symptoms when the disease is still in the latent phase
- Extremely easy test procedure with a minimal impact on a person
- Minimal controlled test time
The suggested new method of tensometric tremorography based on the isometric measurements can be thought of as a prospective one and can be used for the precise medical diagnostics.
Acknowledgments
The work was implemented in Saint Petersburg State Electrotechnical University “LETI”. The sensor unit was designed with the use of a structurally functional approach which has been developed within the framework of the Russian Federation Ministry of Education state assignment (No.8.2080.2017/4.6). Medical support for the work and testing of the prototype among patients with various pathologies of central nervous system was provided by the specialists of the Institute of the Human Brain n.a. N.P. Behtereva of the Russian Academy of Sciences.
Disclosure
The authors report no conflicts of interest in this work.
References
Baumann CR. Epidemiology, diagnosis and differential diagnosis in Parkinson’s disease tremor. Parkinsonism Relat Disord. 2012;18 Suppl 1: S90–S92. | ||
Grimaldi G, Manto M. Tremor: From Pathogenesis to Treatment. San Rafael, CA: Morgan & Claypool; 2008. | ||
Zou K, Guo W, Tang G, Zheng B, Zheng Z. A case of early onset Parkinson’s disease after major stress. Neuropsychiatr Dis Treat. 2013;9:1067–1069. | ||
Edwards R, Beuter A. Using time domain characteristics to discriminate physiologic and parkinsonian tremors. J Clin Neurophysiol. 2000;17(1):87–100. | ||
Zesiewicz TA, Chari A, Jahan I, Miller AM, Sullivan KL. Overview of essential tremor. Neuropsychiatr Dis Treat. 2010;6:401–408. | ||
Louis ED, Ottman R, Hauser WA. How common is the most common adult movement disorder? Estimates of the prevalence of essential tremor throughout the world. Mov Disord. 1998;13(1):5–10. | ||
Mazzoni P, Shabbott B, Cortés JC. Motor control abnormalities in Parkinson’s disease. Cold Spring Harb Perspect Med. 2012;2(6):a009282. | ||
Thenganatt MA, Louis ED. Distinguishing essential tremor from Parkinson’s disease: bedside tests and laboratory evaluations. Expert Rev Neurother. 2012;12(6):687–696. | ||
Jain S, Lo SE, Louis ED. Common misdiagnosis of a common neurological disorder: how are we misdiagnosing essential tremor? Arch Neurol. 2006;63(8):1100–1104. | ||
Mansur PH, Cury LK, Andrade AO, et al. A review on techniques for tremor recording and quantification. Crit Rev Biomed Eng. 2007;35(5):343–362. | ||
Aly NM, Playfer JR, Smith SL, Halliday DM. A novel computer-based technique for the assessment of tremor in Parkinson’s disease. Age Ageing. 2007;36(4):395–399. | ||
Ruonala V, Meigal A, Rissanen SM, Airaksinen O, Kankaanpää M, Karjalainen PA. EMG signal morphology and kinematic parameters in essential tremor and Parkinson’s disease patients. J Electromyogr Kinesiol. 2014;24(2):300–306. | ||
Breit S, Spieker S, Schulz JB, Gasser T. Long-term EMG recordings differentiate between parkinsonian and essential tremor. J Neurol. 2008;255(1):103–111. | ||
Dick SK, Tereh AS, Smirnov AV, Konopelko VK. Designing a system for video recording of man’s extremities tremor. PFMT. 2013;3(16):93–96. | ||
Uhríková Z, Sprdlík O, Hoskovcová M, et al. Validation of a new tool for automatic assessment of tremor frequency from video recordings. J Neurosci Methods. 2011;198(1):110–113. | ||
Chen SW, Lin SH, Liao LD, et al. Quantification and recognition of parkinsonian gait from monocular video imaging using kernel-based principal component analysis. Biomed Eng Online. 2011;10:99. | ||
Bächlin M, Plotnik M, Roggen D, et al. Wearable assistant for Parkinson’s disease patients with the freezing of gait symptom. IEEE Trans Inf Technol Biomed. 2010;14(2):436–446. | ||
Bächlin M, Plotnik M, Roggen D, Giladi N, Hausdorff JM, Tröster G. A wearable system to assist walking of Parkinson’s disease patients. Methods Inf Med. 2010;49(1):88–95. | ||
Mazilu S, Blanke Ulf, Calatroni A, Gazit E, Hausdorff JM, Tröster G. The role of wrist-mounted inertial sensors in detecting gait freeze episodes in Parkinson’s disease. Pervasive Mob Comput. 2016;33:1–16. | ||
Maetzler W, Domingos J, Srulijes K, Ferreira JJ, Bloem BR. Quantitative wearable sensors for objective assessment of Parkinson’s disease. Mov Disord. 2013;28(12):1628–1637. | ||
Neville C, Ludlow C, Rieger B. Measuring postural stability with an inertial sensor: validity and sensitivity. Med Devices (Auckl). 2015;8:447–455. | ||
Casale P, Pujol O, Radeva P. Human activity recognition from accelerometer data using a wearable device. Proceedings of the 5th Iberian conference on Pattern recognition and image analysis, 2011 June 8–10; Las Palmas de Gran Canaria, Spain. Heidelberg: Springer; 2011. | ||
Thanawattano C, Pongthornseri R, Anan C, Dumnin S, Bhidayasiri R. Temporal fluctuations of tremor signals from inertial sensor: a preliminary study in differentiating Parkinson’s disease from essential tremor. Biomed Eng Online. 2015;14:101. | ||
Veluvolu KC, Ang WT. Estimation of physiological tremor from accelerometers for real-time applications. Sensors (Basel). 2011;11(3):3020–3036. | ||
Zhang HH, Chen XY, Lin WY, Chou WC, Lee MY. A novel accelerometer-based method for the real-time assessment of Parkinson’s tremor. Proceedings of IEEE International Conference on Communication Problem-Solving, 5–7 December 2014. Beijing: IEEE; 2014:87–90. | ||
Kruchinin PA, Lebedev AV, Kholmogorova NV Specific characteristics of frequency analysis of force-torque sensors data in the physiological tremor research. Russian J Biomech. 2013;17 1(59):57–68. Russian. | ||
Romanov SP, Iakimovskiĭ AF, Pchelin MG. Метод тензометрии для количественной оценки тремора [A tensometric method for the quantitative assessment of tremor]. Fiziol Zh Im I M Sechenova. 1996;82(2):118–123. Russian [with English abstract]. | ||
Aleksanyan ZA, Bureneva OI, Razin NN, Romanov SP, inventors. Method of assessment of a functional condition of the central nervous system of the person. Russian Federation Patent RU N 2540534. 2014 Feb 10. | ||
Aleksanyan ZA, Romanov SP. Feature of activity of nervous system at a movement control. Inf Control Syst. 2012;5:57–68. Russian. | ||
Profeta VLS, Turvey MT. Bernstein’s levels of movement construction: a contemporary perspective. Hum Mov Sci. 2018;57:111–133. | ||
Bongaardt R, Meijer OG. Bernstein’s theory of movement behavior: historical development and contemporary relevance. J Mot Behav. 2000;32(1):57–71. | ||
Lindstedt SL, LaStayo PC, Reich TE. When active muscles lengthen: properties and consequences of eccentric contractions. News Physiol Sci. 2001;16:256–261. | ||
Vaillancourt DE, Newell KM. Aging and the time and frequency structure of force output variability. J Appl Physiol (1985). 2003;94(3):903–912. | ||
Aleksanyan ZA, Burenev PN, Kostrova OB, Razin NN, Safiannikov NM, inventors. Method of assessment of a functional condition of the central nervous system of the person and device for its realization. Russian Federation Patent RU N 2613446. 2017 Mar 16. | ||
Romanov SP, Aleksanyan ZA, Manoilov VV. Characteristics of tremor in normal subjects and in the diagnosis and treatment of Parkinsonism. Neurosci Behav Physiol. 2004;34(4):389–398. Russian. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.