")
Back to Journals » Clinical Ophthalmology » Volume 15
Ten-Year Real-World Outcomes of Anti-Vascular Endothelial Growth Factor Therapy in Neovascular Age-Related Macular Degeneration
Authors Cheema MR , DaCosta J , Talks J
Received 2 July 2020
Accepted for publication 27 November 2020
Published 22 January 2021 Volume 2021:15 Pages 279—287
DOI https://doi.org/10.2147/OPTH.S269162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Muhammad Raza Cheema, Joanna DaCosta, James Talks
Department of Ophthalmology, Royal Victoria Infirmary, Newcastle Upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, UK
Correspondence: Muhammad Raza Cheema
Department of Ophthalmology, Royal Victoria Infirmary, Newcastle Upon Tyne NE1 4LP, UK
Tel +44-191-233-6161
Email [email protected]
Background: Neovascular age-related macular degeneration (nAMD) has been treated with anti-vascular endothelial growth factor (anti-VEGF) therapy since 2006 with initial efficacy evidence of 2 years. In many, long-term therapy is required, and evidence for benefit is required from real-world data collection.
Methods: Retrospective review of electronic medical records of a consecutive series of patients treated with anti-VEGF therapy for nAMD over a 10-year period. Age, lens status and loss to follow-up was recorded. Primary outcome was change in VA at 10 years; secondary outcomes included proportion of eyes losing < 15 letters at 3, 5, 7 and 10 years, number of injections and anatomic outcome.
Results: Of 196 patients (197 eyes), 90 patients had 10 years of follow-up data. Visual acuity (VA) declined by − 11.2 letters (p=0.001), but 63.3% of eyes lost ≤ 15 letters. The proportion of eyes maintaining ≥ 70 letters was 17.7%, and the mean number of injections (±SD) was 47 ± 16. Retinal fluid was still present in 72.2% of eyes at 10 years. Forty-six percent of patients continued to receive anti-VEGF injections 10 years after treatment was commenced.
Conclusion: Anti-VEGF treatment for nAMD over a ten-year period showed 63.3% of eyes lost ≤ 15 letters. Eyes with better baseline vision were more likely to continue receiving anti-VEGF treatment, but the frequency of injection treatment decreased.
Keywords: neovascular age-related macular degeneration, visual acuity, real-world, anti-vascular endothelial growth factor injections
Introduction
Age-related macular degeneration is a leading cause of blindness in elderly populations.1 Over the last decade, the advent of anti-vascular endothelial growth factor (anti-VEGF) therapy has been a significant advance in preserving and improving vision in patients with neovascular AMD (nAMD).2 Repeated prolonged treatment is often necessary due to the short duration of action of anti-VEGF agents. Landmark clinical trials have demonstrated short-term visual gains over the course of 1–2 years, in response to anti-VEGF treatment, utilizing frequent (monthly, bimonthly, observe and plan) as dosing regimens.2–5 The CATT study and a follow-up observational study of the phase 3 pivotal studies MARINA, ANCHOR and HORIZON: SEVEN-UP examined medium-term treatment outcomes of anti-VEGF treatment over 5 to 7 years.6
Treatment regimens have been subject to adaptation in clinical practice such as pro-re-nata (PRN), fixed dosing and treat and extend. In addition, factors such as choice of anti-VEGF agent, reimbursement considerations and changing guidelines have led to a wide variation in outcomes throughout the world.7 The SEVEN-UP study included a heterogeneous group of participants receiving anti-VEGF agents in various treatment regimens including fixed dosing along with PRN dosing regimens (SEVEN). The CATT study had two different dosing regimens, monthly injections and PRN dosing (CATT). This reflects the wide variation in real-world treatment regimens and outcomes.
In the United Kingdom, the National Health Service (NHS) provides treatment free at the point of entry. The National Institute for Health and Care Excellence (NICE) produces evidence-based guidelines for treatment. Few studies have reported the long-term outcomes of anti-VEGF therapy in clinical practice.
The purpose of this study was to examine real-world outcomes of treating nAMD at set time points, in a series of patients who had the potential for 10 years of follow-up.
Materials and Methods
Study Design
This study was a single-centre, retrospective observational consecutive case series cohort study. Data was extracted from electronic medical records (EMR) (Medisoft Ophthalmology; Medisoft Limited, Leeds, UK) at the Royal Victoria Infirmary, Newcastle, UK. The lead clinician and Caldicott Guardian (nominee responsible for data protection) at the hospital gave written approval for anonymized data extraction. Anonymized database analyses of this type do not require ethical permission because they are viewed as audit or service evaluations (see http://www.hra.nhs.uk/research-community/beforeyou-apply/determine-whether-your-study-is-research/). This study was conducted in accordance with the Declaration of Helsinki 2013 and the United Kingdom’s Data Protection Act 2018.
Methods
A consecutive series of treatment-naïve eyes commenced on anti-VEGF treatment for nAMD between 1st Jan 2007 and 31st Dec 2009 was studied. The diagnosis had been determined by a retinal specialist, and all patients had been assessed and treated based on the guidelines at the time, including NICE criteria.8,15,16 Data extracted was: demographic details, visual acuity (VA) at annual time points and/or last visit, injection numbers, and OCT findings.
VA was recorded as an Early Treatment Diabetic Retinopathy Study (ETDRS) VA letter score at 2 m at each visit. The total letter score was adjusted for the distance used. Most VA values were recorded using habitual correction rather than with full refraction. This is a standard method for measuring VA in clinical practice but likely to underestimate the VA. Regular refraction by the patient’s optometrist was encouraged, and if there were significant changes in VA in-house refraction was carried out.
Values corresponding to counting fingers, hand movements, light perception and no light perception were substituted with values of 0 letters.
The primary outcome measurement was mean change in vision from baseline at 3, 5, 7 and 10-year intervals after treatment initiation. The proportion of eyes achieving ≥70 letters, 50–69 letters, 30–49 letters and ≤30 letters was also measured at baseline, and at 3, 5, 7 and 10-year intervals. For those eyes where 10 years of follow-up was not completed the VA at the last recorded follow-up visit was recorded.
Secondary outcomes included the number of anti-VEGF injections received, retinal morphology (classified as dry or wet) and central macular thickness for eyes completing 10 years of active treatment with anti-VEGF compared to eyes not completing 10 years of treatment.
The 2008 to 2013 treatment protocol included an induction phase of three monthly injections of ranibizumab followed by a PRN regime. At this time, ranibizumab was the only anti-VEGF drug approved for use in the NHS.15 With the introduction of aflibercept in 2013, following NICE approval, the majority of patients were gradually moved across to aflibercept in an attempt to reduce treatment burden.16
Data was entered onto an Excel spreadsheet. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 26.0 (IBM Corp. Armonk, NY, USA). Mean, median and standard deviation were measured for age and baseline vision, and standard error of the mean was calculated for changes in VA. The data did not follow normal distribution curve, and therefore Wilcoxon signed rank test was used to assess statistical significance. Multiple linear regression was used to assess the correlation of mean baseline VA, age, central macular thickness (CMT) and number of injections received compared with change in VA at the end of 10 years.
Results
Baseline Characteristics of the Whole Cohort
From 1st January 2007 till 31st December 2009, a total of 197 eyes of 196 patients were initiated on anti-VEGF injections for nAMD. Only one patient had bilateral involvement at baseline, so for the majority of the patients only one eye was included to reduce statistical bias in the results.9 Mean age was 80.7 ± 8 years, and 53% of patients were male. Mean baseline VA was 59.8 ± 14 letters; 51% eyes were phakic.
Outcomes for Cohort Completing 10 Years of Treatment
Visual Outcomes
Out of 197 eyes, 90 eyes (45.9%) completed active treatment for 10 years. Mean age was 79.2 ± 8. Mean baseline vision was 62.6 ± 13.6 letters. Mean final vision was 51.4 ± 18.9 (p=0.001). Mean change in VA over 10 years (95% CI) was −11.2 (−15.1 - −7.3) letters. Median final vision at 10 years was 54.5 letters.
Table 1 shows vision being maintained at 3, 5 and 7 years from baseline vision. Mean change in VA (95% CI) at 3 years was +1.3 (−1.38 - +3.98) letters, at 5 years was −1.5 (−4.42 - +1.42) letters and at 7 years was −2.5 (−5.78 - +0.78) letters. By the 10-year follow-up vision had declined by −11.2 (−15.1 - −7.3) letters from baseline.
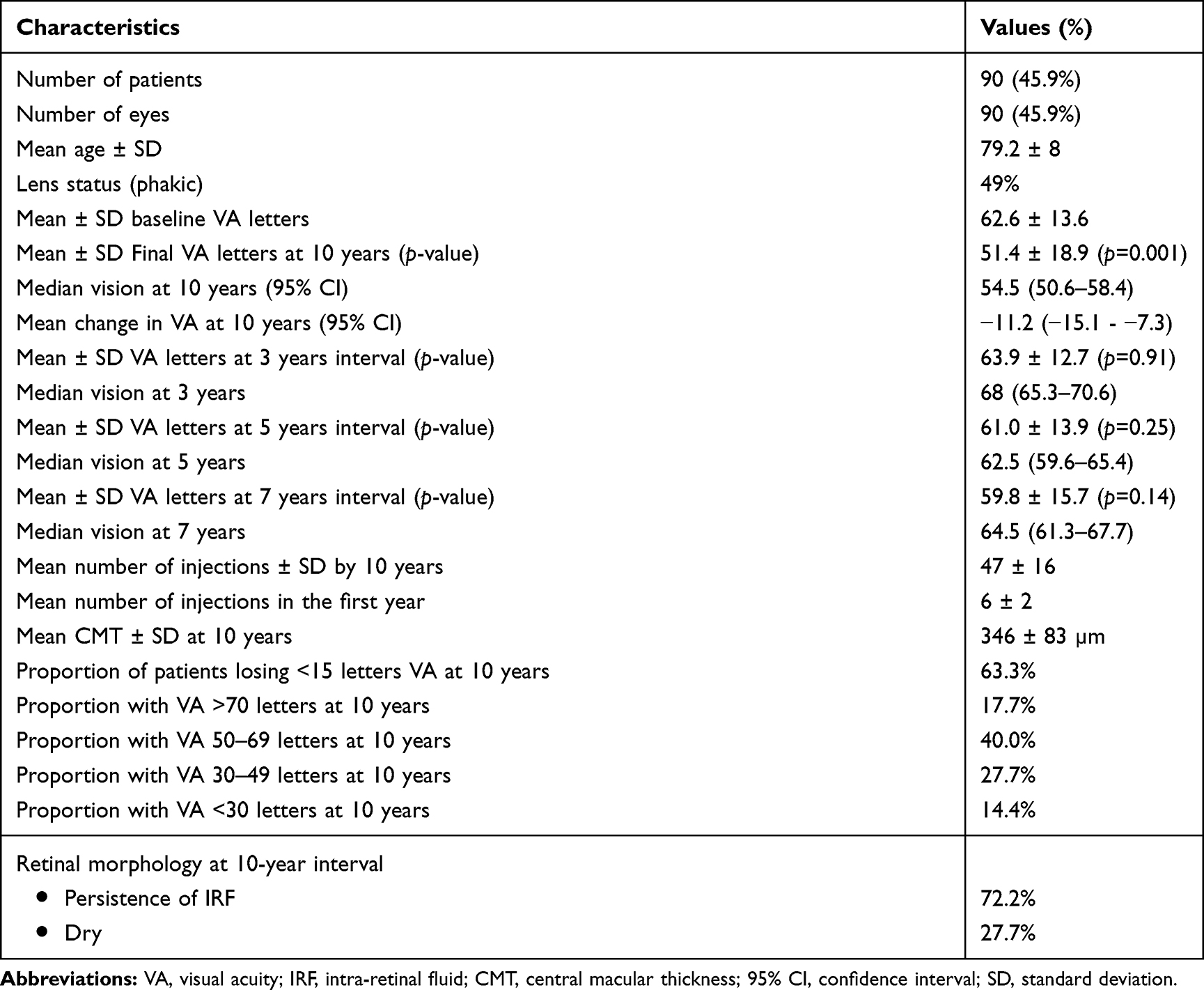 |
Table 1 Outcomes in Eyes Completing a Full 10 Years of Active Treatment |
Figure 1 shows median vision over time in the cohort completing 10 years of follow-up compared to the cohort not completing 10 years of follow-up. A visual decline is noted over the years in “remainder group”. It also shows the number of patients left in the remainder group per year. Figure 2 shows the proportion of eyes achieving different levels of vision over the course of 10 years. Overall, 57.7% of patients maintained their vision at >50 letters by the end of 10 years of active treatment.
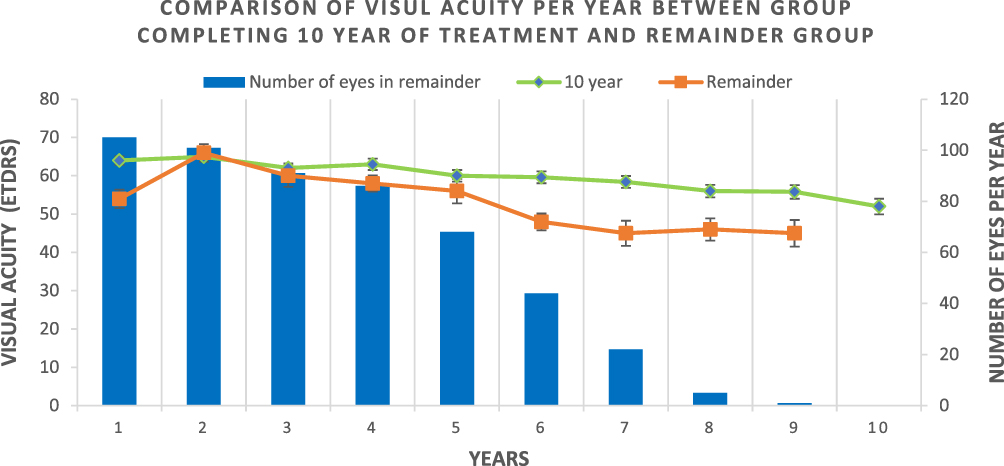 |
Figure 1 Comparison of visual acuity per year between group completing 10 year of treatment and remainder group treatments. |
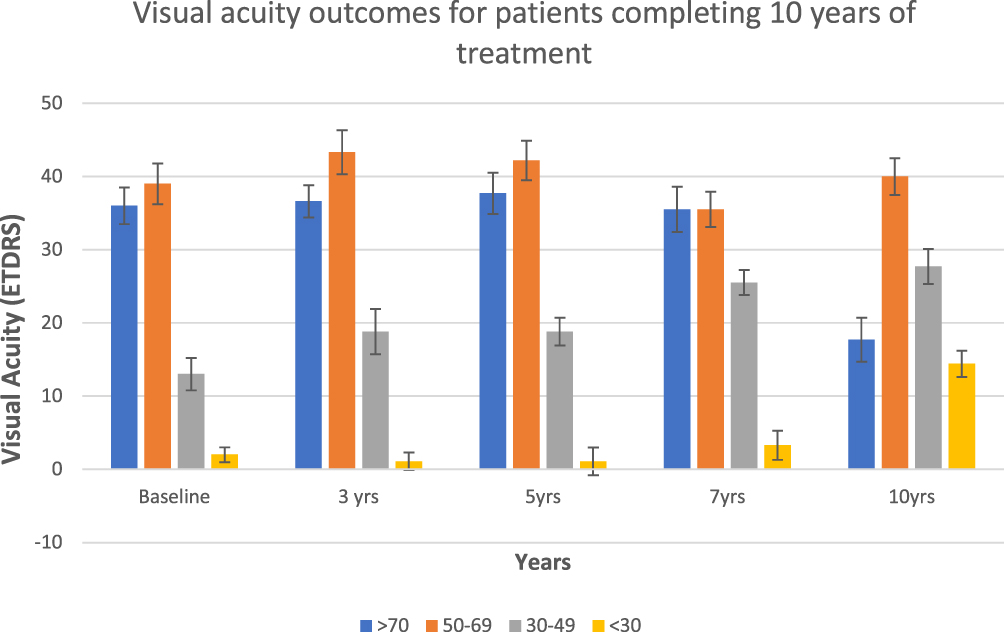 |
Figure 2 Visual acuity outcomes for patients completing 10 years of treatment. |
Number of Injections
Mean number of injections administered was 47 ± 16, and mean number of injections (±SD) during the first year was 6 ± 2. Figure 3 shows the mean number of injections received per year during the 10-year course of anti-VEGF treatment. The number of injections per year reduces steadily from 6 in the 1st year to 3.9 in the 10th year. The number of injections required to maintain vision decreases over the 10-year period as shown in Figure 3.
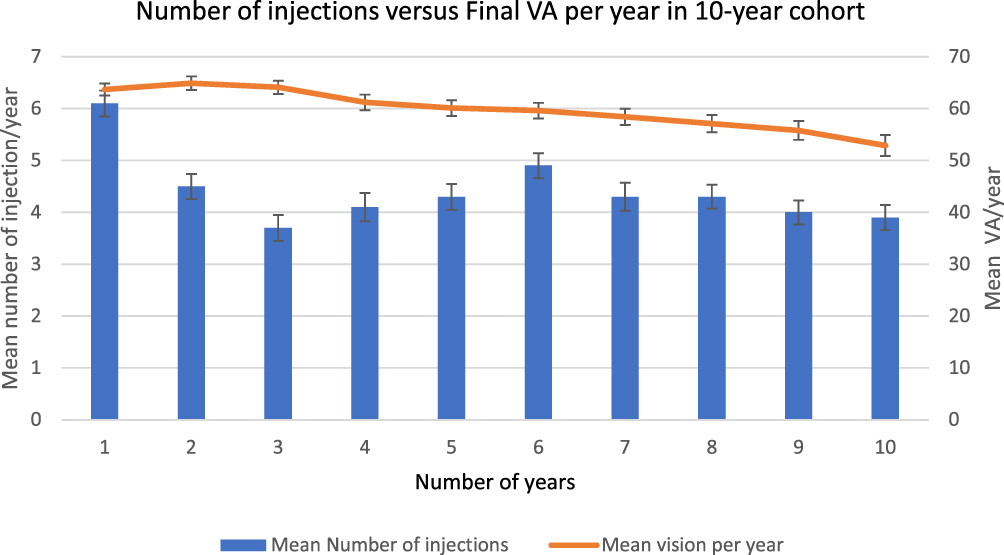 |
Figure 3 Number of injections versus final VA per year in 10-year cohort. |
Forty-two patients received less than the mean number of injections. Their baseline mean VA was 60.0 ±16.9 letters and at end of 10 years was 49.9 ± 19.8 letters. Mean change in vision was therefore −10.1 letters in this group. Forty-eight patients received injections more than the mean. Their baseline mean VA was 64.9 ± 9.4 letters and at 10 years was 52.8 ± 18 letters. Mean change in vision was therefore −12.1 letters in this group.
Other Parameters
Mean CMT for this cohort at 10 years was 346 ± 83 µm; however, this included 72.2% of patients with a “wet macula” (intra-retinal or sub-retinal fluid or a combination), and 27.7% had a dry macula.
Mean baseline VA, age, CMT and numbers of injections were assessed using multiple linear regression (p-value; 95% CI) to report any correlation to change in final vision. Poorer baseline VA was associated with a higher mean change in VA (p=0.004; −0.87 - −0.03). CMT (p=0.14; −0.01–0.09), number of injections (p=0.20; −0.10–0.47) and age (p=0.93; −0.54–0.49) were not found to be associated with change in vision.
Fellow Eye Results
Forty patients developed fellow eye involvement during the study period but did not meet the criteria for inclusion due to lack of a complete 10-year period of surveillance. Mean baseline VA ± SD at the time of presentation with fellow eye involvement was 58.2 ± 13.11 letters. Final VA was calculated at the last visit noted in the electronic medical records. Final VA ± SD was 44.8 ± 28.2 letters. The mean number of injections received in the fellow eyes was 22.9 ± 15.8. The mean number of injections during the first year was 6 ± 2.5; 35% of these eyes were still receiving active anti-VEGF treatment at the end of the study period. A total of 40% of eyes discontinued anti-VEGF treatment due to disciform scar formation, and 30% of the eyes were dry at the last recorded visit.
Outcomes for Cohort Not Completing Active Treatment for 10 Years
In this group 107 eyes did not complete 10 years of active treatment but were started on anti-VEGF injections during 2007–09. Last VA recorded was used to analyse the data before patients stopped treatment. Mean age ± SD for the cohort was 82.0 ± 7.8 years. Mean number of injections administered was 22.5 ± 12.6 over the treatment period.
Mean ± SD baseline vision of this cohort was 57.5 ± 14.5 letters. Final VA was calculated at 3, 5 and 7-year time points using last VA as their final vision. Final VA for patients completing 3 years of monitoring was 54.06 ± 15.2 letters, at 5 years was 49.78 ± 18.3 letters and at 7 years 46.24 ± 20.77 letters.
Table 2 shows a comparison of visual outcomes at 3, 5 and 7 years for cohorts completing 10 years of treatment and the cohort with less than 10 years follow-up. Reasons for not completing 10-year treatment were: 51.4% of patients were deceased, 36.4% were discharged, 12.1% were lost to follow-up. The mean number of injections for eyes completing 3 years of treatment was: 23.3 ± 12; 5 years: 25.7 ± 11.9; and 7 years: 27.8 ± 11.4 injections.
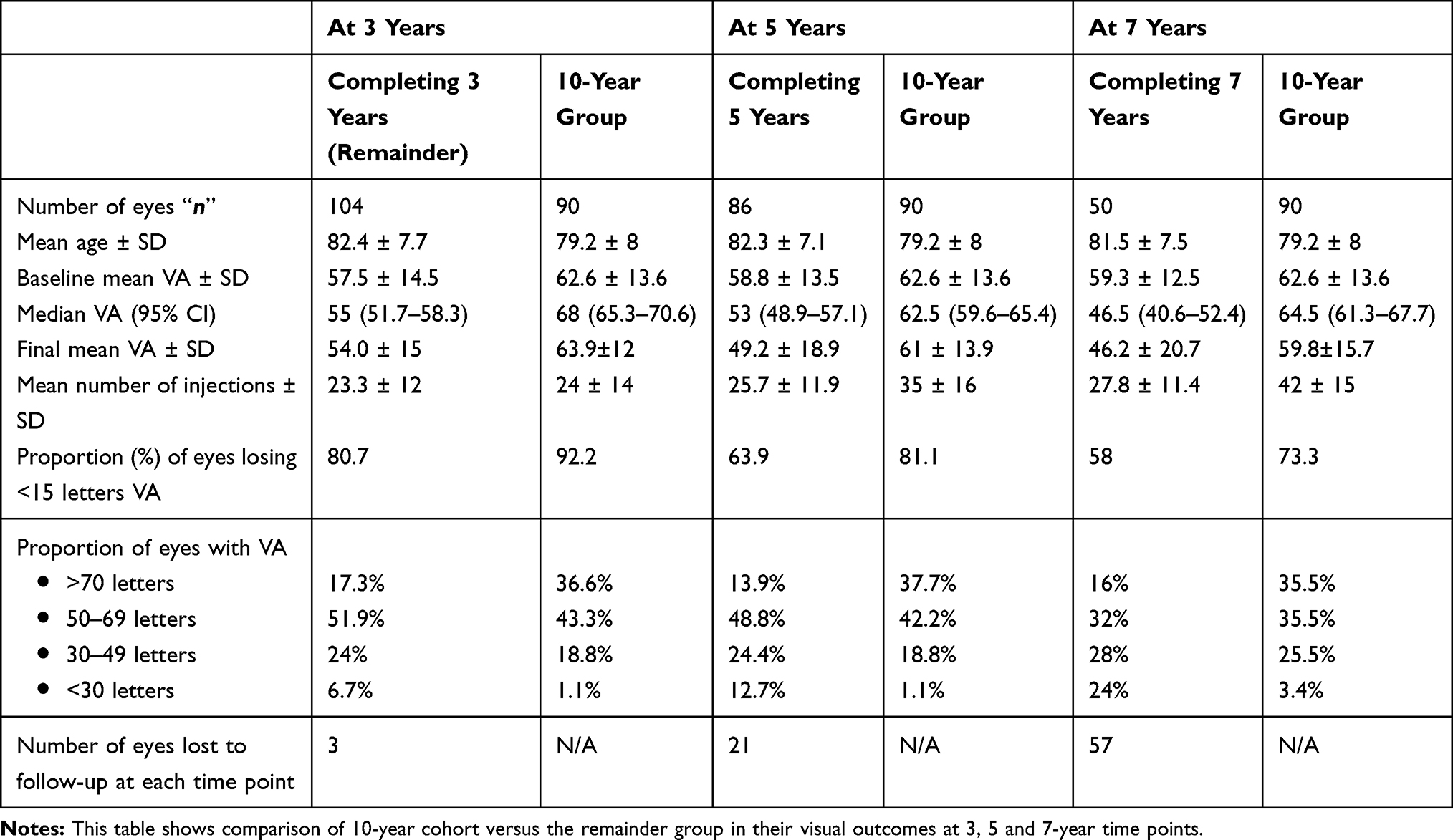 |
Table 2 Visual Acuity Outcomes for Patients Completing 10 Years of Active Treatment versus Rest of the Group (Includes Patients with Surveillance and Lost to Follow-Up Between 7 and 10 Year Intervals) |
The proportion of eyes losing <15 letters vision at 3-year time interval was 80%; at 5 years, 61%; and at 7 years, 58%. A total of 14% of eyes discharged at 7 years were dry on last visit.
As per Figure 1, the difference between the median VAs of the two cohorts increased after the fifth year. A number of eyes dropped out of the remainder group over the course of treatment, with no eyes completing more than 9 years of treatment.
The rate of adverse events was low, with 0.02% eyes developing post-injection uveitis and no reported cases of post-injection endophthalmitis.
Discussion
The aims of this study were to determine the outcomes of anti-VEGF treatment for nAMD over 10 years in a real-world clinical setting. In the UK, this study represents the second study to report 10-year outcomes of anti-VEGF injections in nAMD. This is an important issue as original NICE approval and funding was based on two years of treatment. It is therefore important to clarify how long ongoing treatment does provide benefit as clinical trials are not designed and funded to provide results for extended follow-up periods.
In this study, a total of 197 eyes were identified with nAMD where anti-VEGF treatment had been initiated 10 years earlier. The visual outcome of the cohort completing 10 years of treatment was better at each time interval when compared with the cohort not completing 10 years of treatment. From Table 2, it is evident that the cohort completing 10 years of treatment had a higher baseline VA, was of a younger age, had a greater number of injections and attained a better final visual outcome.
The main reasons for loss to follow-up were patient deaths and a shared decision with the patient regarding the futility of further treatment due to macular atrophy and fibrosis as determined by clinical examination. In addition, other systemic conditions in elderly patients and difficulties in transportation may cause challenges in attending clinic reviews, making loss to follow-up more likely. Patients with poor vision were more likely to be lost to follow-up and not complete the 10-year review.
In our study, multiple regression analysis did not reveal an association between better visual outcomes and increased number of injections. However, recent real-world outcome data from Australia and New Zealand indicated an increased likelihood of improved visual outcome in one of their study groups with an increased number of injections being administered.10 In our study, eyes starting with better baseline VA were more likely to receive longer duration of treatment and achieve overall better vision compared to patients with poorer baseline VA. Our study results are comparable to a recent study showing eyes receiving less than 4 injections per year were associated with poorer visual outcomes; however, eyes receiving 10 or more injections suffered a “plateauing effect” after one year.18 This highlights the inherent bias real-world studies may have in trying to maintain already higher baseline VA with a ceiling effect limiting visual gain. Our study is not able to ascertain the likely reasons for poorer VA gains in eyes with poorer baseline VA. It is postulated that this may be due to other pathophysiological processes such as fibrosis that occur in nAMD.
Treatment has also changed over 10 years with the addition of aflibercept after ranibizumab and different approaches to treatment from fixed dosing, PRN and treat and extend. NICE originally approved ranibizumab for nAMD in 2008, and aflibercept was approved for the treatment of nAMD in 2013.15,16 Clinical guidelines on treating patients were produced by the Royal College of Ophthalmologists but were replaced by NICE guidance issued in 2018 which stated that anti-VEGF treatment for nAMD is clinically effective before vision drops below 6/12 and may be cost-effective.8 Additionally, the 2018 NICE guidance stated that treatment can be considered if vision is worse than 6/96 if it would improve the overall visual function, for example, in a patient being treated in the better seeing eye of both eyes. In addition, 2018 NICE guidelines mention that anti-VEGF intravitreal treatment can be administered by suitably trained allied healthcare professionals.8 These different factors will also have influenced how many injections were given.
To date, no randomized clinical trials or prospective observational studies have been reported to show 10-year follow-up for patients receiving anti-VEGF treatment. The SEVEN-UP observational data from phase 3 pivotal trials reported 7-year visual outcome data showing a mean loss of −8.6 letters after 7 years, with only 23% achieving VA ≥70 letters.6 Our study reports a mean loss of -11.2 letters after 10 years, with 17.7% achieving VA ≥70 letters after 10 years of treatment with anti-VEGF injections. These results indicate that most eyes maintaining VA ≥70 letters at 2 years have continued to maintain the same level of VA by 10 years.
In the group completing 10 years of treatment, our study reports that those patients receiving a higher number of injections than the mean had a better baseline and final outcome vision than the patients receiving less than the mean number of injections. The reasons for this may be a more favourable decision to re-treat eyes with functionally better vision to maintain this outcome or that eyes with better functional outcome required more injections. Our study also shows that the trend of number of injections received per year has a downward slope, with a reduction in number of injections received per year. A small peak is noted at the 6-year time point, whose significance is unclear. Fellow eye involvement was present in 44.4% of patients. A significant proportion (75%) of fellow eyes discontinued anti-VEGF treatment due to formation of disciform scar, plateauing of visual benefit, resolution of intra-retinal fluid or persistence of intra-retinal fluid without visual improvement. All fellow eyes were examined on each visit and commenced on anti-VEGF treatment when diagnosed with nAMD. The mean number of injections in the fellow eye was overall lower than in the primary eye. A total of 30% of the fellow eyes were dry at the last recorded visit. However, overall visual improvement in fellow eyes was lower than in the primary eye. The reasons for this might be treatment bias, with there being a tendency to focus treatment on the dominant eye and the eye with better VA as not all patients will want treatment to both eyes.
With only a few studies being published to date, there is significant paucity of real-world data showing outcomes of anti-VEGF treatment over a 10-year period. The published cohorts have been of small size, indicating difficulty in recruiting and maintaining follow-up for prolonged periods.10–12 Gillies et al reported 169 eyes, divided into two groups, receiving anti-VEGF injections for 10 years. One cohort of 132 patients achieved a final VA of 60.1 letters with only a mean change of −0.9 letters. The other cohort of 37 patients achieved a considerably lower final VA of 46.8 letters with a significant mean change of −14.9 letters.10 Brynskov et al reported 74 eyes receiving PRN anti-VEGF injections for 10 years achieving a mean final VA of 61.5 letters with mean change of −5.0 letters.11 Chandra et al reported 149 eyes completing 10-year follow-up for nAMD with 76.5% of eyes losing ≤15 letters and 67.1% of eyes achieving VA threshold of 20/70 (57 letters on 2 m ETDRS) letters at the end of 10 years.12
Our study showed 90 eyes receiving anti-VEGF injections achieving a mean final VA of 51.4 letters with a mean change of −11.2 letters from baseline. Our study also showed 63.3% of eyes lost ≤15 letters. This large disparity in real-world outcomes in final vision of published 10-year studies illustrates the varying clinical practice and uncertainty present in the response of nAMD to anti-VEGF injections after 10 years. Differences in mean VA levels may partly reflect differences in follow-up practice for patients with lower levels of vision. To date, it is difficult to know the magnitude of slowing of progression of nAMD with anti-VEGF injections; however, real-world outcomes, including our study, indicate a prominent halt in progression of nAMD in cohorts receiving anti-VEGF over a 10-year interval. This is further evidenced by a recent study with a ten-year follow-up showing that the proportion of patients with nAMD receiving ranibizumab who attained best-corrected visual acuity ≥70 letters was 21% at the final follow-up.14
Drop-out rates to follow-up over 10 years is expected and is an important finding in itself for capacity planning. It is also a challenge for reporting outcomes as the groups with longer follow-up are to some extent self-selecting as they have been deemed that it is worth continuing treatment.
Limitations
Our study has important limitations. To define vision stability as a loss of <15 ETDRS letters is a measure commonly used in clinical trials including phase 3 pivotal VIEW trial.17 Fifteen letters represents a doubling of the visual angle using ETDRS visual acuity testing. The VA score is a continuous variable, and statistical comparison between groups may involve measure of the mean. A restriction of comparison of means is that outliers may have undue influence. Hence, conceptually converting a continuous variable (VA score) to a binary measure (< or >15 letter gain) is easier to understand as results are reported at a patient level rather than group level. There are several disadvantages to this approach such as loss of information so reducing statistical power relative to the mean, misclassification of the outcome due to variability of the visual acuity measurement, and susceptibility to floor or ceiling effects of visual acuity measurements.13 Using habitual correction when testing VA, rather than a new refraction on each visit, might have underestimated the potential VA of some of the patients and is another difference between real-world data and a clinical trial.
A higher dropout rate was observed in the group not completing 10-year follow-up. However, the major strengths of this study included a very low overall loss to follow-up rate and achievement of sustained regular follow-up in eyes receiving anti-VEGF injections for 10 years. Over the course of 10 years, variation in dosing regimens and anti-VEGF agents was noted to begin with; however, a more standardized “Treat and Extend” regimen was primarily used subsequently. This variation in the patterns of treatment and choice of anti-VEGF agents is a reflection of real-world practice and influences the outcomes of our study.
This study demonstrates that a significant proportion of eyes receiving anti-VEGF injections for nAMD for at least 10 years maintain vision, with better visual outcomes for those patients receiving continued regular anti-VEGF injection treatments. A low rate of macular scarring was seen in the actively treated group, and a higher proportion of eyes (57.7%) maintained vision >50 letters by the end of 10 years of active treatment.
What This Paper Adds
- Maintaining anti-VEGF intravitreal injection therapy for nAMD sustains vision over a 10-year period with 63.3% of eyes losing <15 letters VA after 10 years of treatment.
- Eyes with better baseline vision were more likely to continue receiving anti-VEGF injections.
- The number of injections required to maintain vision decreases over the 10-year period.
Disclosure
J. DaCosta has received a travel grant from Alimera. J. Talks serves on advisory boards for Bayer, Novartis, Allergan, Alimera and participated in research for Bayer, Novartis, Allergan, Alimera, Roche and Boehringer Ingelheim. The authors report no other conflicts of interest in this work.
References
1. Bourne RRA, Jonas JB, Flaxman SR, et al. Prevalence and causes of vision loss in high-income countries and in Eastern and Central Europe: 1990–2010. Br J Ophthalmol. 2014;98(5):629–638. doi:10.1136/bjophthalmol-2013-304033
2. Maguire MG, Ying G-S; CATT Research Group MD. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897–1908. doi:10.1056/NEJMoa1102673
3. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
4. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57–65.e5. doi:10.1016/j.ophtha.2008.10.018
5. Singer MA, Awh CC, Sadda S, et al. HORIZON: an open-label extension trial of ranibizumab for choroidal neovascularization secondary to age-related macular degeneration. Ophthalmology. 2012;119(6):1175–1183. doi:10.1016/j.ophtha.2011.12.016
6. Rofagha S, Bhisitkul RB, Boyer DS, et al. Seven-year outcomes in ranibizumab-treated patients in ANCHOR, MARINA, and HORIZON: a multicenter cohort study (SEVEN-UP). Ophthalmology. 2013;120(11):2292–2299. doi:10.1016/j.ophtha.2013.03.046
7. Talks J, Daien V, Finger RP, et al. The use of real-world evidence for evaluating anti-vascular endothelial growth factor treatment of neovascular age-related macular degeneration. Surv Ophthalmol. 2019;64(5):707–719. doi:10.1016/j.survophthal.2019.02.008
8. Excellence NIoHaC. NICE guideline [NG82]. Age-related macular degeneration; 2018. Available from: https://www.nice.org.uk/guidance/ng82.
9. Murdoch IE, Morris SS, Cousens SN. People and eyes: statistical approaches in ophthalmology. Br J Ophthalmol. 1998;82(8):971–973. doi:10.1136/bjo.82.8.971
10. Gillies M, Arnold J, Bhandari S, et al. Ten-year treatment outcomes of neovascular age-related macular degeneration from two regions. Am J Ophthalmol. 2020;210:116–124. doi:10.1016/j.ajo.2019.10.007
11. Brynskov T, Munch IC, Larsen TM, et al. Real-world 10-year experiences with intravitreal treatment with ranibizumab and aflibercept for neovascular age-related macular degeneration. Acta Ophthalmol. 2020. doi:10.1111/aos.14183
12. Chandra S, Arpa C, Menon D, et al. Ten-year outcomes of antivascular endothelial growth factor therapy in neovascular age-related macular degeneration. Eye. 2020. doi:10.1038/s41433-020-0764-9
13. Beck RW, Maguire MG, Bressler NM, Glassman AR, Lindblad AS, Ferris FL. Visual acuity as an outcome measure in clinical trials of retinal diseases. Ophthalmology. 2007;114:1804–1809. doi:10.1016/j.ophtha.2007.06.047
14. Arpa C, Khalid H, Chandra S, et al. Ten- year survival trends of neovascular age-related macular degeneration at first presentation. Br J Ophthalmol. 2020. doi:10.1136/bjophthalmol-2020-317161.
15. Excellence NIoHaC. NICE guideline [TA155].Ranibizumab and Pegatinib for the treatment of age-related macular degeneration; 2008. National Institute of Health and Care Excellence UK. Available from: www.nice.org.uk/guidance/ta155.
16. Excellence NIoHaC. NICE guideline [TA294]. Aflibercept solution for injection for treating wet age-related macular degeneration; 2013. National Institute of Health and Care Excellence UK. Available from: www.nice.org.uk/guidance/ta294.
17. Heir JS, Brown DM, Chong V, et al. Intravitreal Aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119:2537–2548. doi:10.1016/j.ophtha.2012.09.006
18. Ciulla TA, Hussain RM, Pollack JS, et al. Visual acuity outcomes and anti-vascular endothelial growth factor therapy intensity in neovascular age-related macular degeneration in patients: a real-world analysis of 49, 485 eyes. Ophthalmol Retina. 2020;4(1):19–30. doi:10.1016/j.oret.2019.05.017
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.