")
Back to Archived Journals » Smart Homecare Technology and TeleHealth » Volume 3
Telephone support and adherence in patients with chronic disease – a qualitative review of reviews
Authors Balasubramanian D, Yoong J, Vrijhoef HJM
Received 5 November 2014
Accepted for publication 29 January 2015
Published 8 May 2015 Volume 2015:3 Pages 107—118
DOI https://doi.org/10.2147/SHTT.S77031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Yelena Yesha
Divya Balasubramanian,1 Joanne Yoong,1–3 Hubertus JM Vrijhoef1,3–6
1Saw Swee Hock School of Public Health, National University Singapore, Singapore; 2Center for Economic and Social Research, University of Southern California, California, USA; 3Center for Health Services and Policy Research, National University Health System, Singapore; 4Scientific Center for Care and Welfare, Tilburg University, Tilburg, The Netherlands; 5Department of Patients & Care, Maastricht University Medical Center, Maastricht, The Netherlands; 6Department of Family Medicine and Chronic Care, Vrije Universiteit Brussels, Brussels, Belgium
Abstract: Among patients with a chronic disease, low adherence to prescribed treatments is very common, leading to substantial morbidity, mortality, and increase in health care costs. Telephone or mobile phone support is a common form of intervention that can be used to improve their adherence. We reviewed existing systematic and nonsystematic reviews to analyze the effectiveness of telephone interventions to improve treatment adherence in patients with chronic disease. Secondary aims were to evaluate the selected reviews in terms of cost-effectiveness of the intervention and frequency of messages affecting the adherence outcomes. A search for reviews was conducted in three databases, including PubMed, the Cochrane Library, and CINAHL, and three reviews that met the inclusion criteria were selected for final analysis. A qualitative review of the selected reviews was conducted, and reviews were evaluated to extract and summarize the characteristics and outcomes. Two of the selected reviews studied mobile phone text messaging, and one review studied telephone or mobile phone consultation. All three reviews reported an overall improvement in adherence, but the reviews varied in the types of research and the outcome measures. However, none of the reviews reported costs as an outcome. The evidence from reviews to characterize the effectiveness or cost-effectiveness of telephone support as an intervention to improve adherence among people with chronic diseases is fairly small and weak. Telephone support interventions have to be evaluated more systematically in routine practice against a comprehensive set of criteria, including their relative costs and outcomes.
Keywords: literature review, compliance, telemedicine, communicable diseases, cost-effectiveness
Introduction
It can be particularly challenging to support adherence among patients with a chronic disease who have multiple related medications and medical regimens that change in response to exacerbations that occur indefinitely.1 The occurrence of quiescent symptoms with the need for long-term treatment may affect the patient’s daily use of maintenance medications.2 Adherence in the context of chronic diseases also requires long-term permanent changes in lifestyle behaviors, including diet, physical activity, and smoking.1 As a result, among patients with chronic disease, low adherence to prescribed treatments is very common, leading to substantial morbidity, mortality, and increase in health care costs. In the United States, for instance, it has been estimated that half of all medications for chronic conditions are not taken as prescribed, and the costs of nonadherence are between US $110 and US $289 billion for the US healthcare system annually.3 Increasing the effectiveness of adherence interventions may have a far greater impact on the health of the population than any improvement in specific medical treatment for chronic disease.1
Attention and care for patients with a chronic disease are often impacted by health care provision deficits, physician shortages, and the inability of many patients to increase their clinic visits. These factors have prompted the search for feasible and cost-effective solutions to support adherence.4 Most methods currently used to improve adherence involve combinations of behavioral interventions and reinforcements to increase the supervision or attention given to patients.5 Evidence shows that patients who miss appointments are often those who need the most help to improve their ability to adhere to a medication regimen; such patients will often benefit from assistance in clinic scheduling and reminders to optimize their adherence.6 Such support interventions are highly amenable to being carried out via telemedicine.7 The American Telemedicine Association has defined telemedicine as “the use of medical information exchanged from one site to another via electronic communications to improve a patient’s clinical health status.”4
Among telemedicine methods, telephone support is increasingly implemented for assumed advantages like the coordination of care between different health care professionals within a consultation and the greater possibility of providing continuity of care for patients.8 Studies in the past have shown high patient satisfaction with consulting their doctors via telephone. Clinicians also seem to appreciate this mode of communication because of the convenience and flexibility it offers in facilitating regular follow-ups and, in certain cases, even obviating home visits. On the other hand, some clinicians are concerned about the risk of missing serious conditions when diagnosing via telephone intervention.8
Telephone support includes mobile technology, and in recent years mobile applications have increasingly been used to offer better care and services to patients because of the flexible way of communicating they facilitate. It has been predicted that this ubiquitous technology, which offers real-time data to patients, doctors, suppliers, and insurers, will revolutionize patient–doctor communication.9
The success of specific interventions on adherence may be influenced by multiple background factors related to the patient’s self-management capability, socioeconomic conditions, therapy-induced effects, and health care system-dependent conditions.10,11 Given the potential complexity of the relationships between interventions and the above-mentioned factors, we decided to review existing systematic and nonsystematic reviews of original studies and to consolidate the evidence of effectiveness and cost-effectiveness achieved from using telephone support as an intervention for improving adherence in patients with a chronic disease.
Compliance and adherence
Cramer et al12 define compliance as “the extent to which a patient acts in accordance with the prescribed interval and dose of a dosing regimen,” with adherence as a synonym of compliance. However, a global research report on this theme defines “patient adherence” as a combination of persistence and compliance with medication as well as general advice by the physician. In this regard, adherence can be defined as the extent to which a patient follows a prescribed treatment regimen, which includes taking a drug and following lifestyle advice from the physician.13 Understanding of the issue has evolved from the narrow scope of compliance, which places the entire responsibility upon a passive patient, to a broader definition where adherence is a more-collective responsibility between health care providers and patients who are active participants in their own care. Horne et al14 have a slightly different explanation about the relationship between the terms: “adherence” and “compliance” describe the patient’s perspective to the prescriber or physician’s advice, whereas “concordance” relates to the process and outcomes of prescribing. Although all three terms are used interchangeably, extracting from the above definitions, we define adherence in this review as the patient’s consistency in following recommended health behavior and treatments as prescribed by the physician or the health care provider. Following from this, it is nonadherence that compromises both patient health outcomes and the efficient spending of financial means within health care.
Research questions
Nonadherence to chronic medication treatment is common and leads to morbidity, mortality, and increase in health care costs.11 Evidence-based information about interventions targeted to improve adherence would enhance the long-term viability of solutions like telephone support. In this study, we sought to derive such evidence from reviews of existing original papers that studied the outcomes of telephone-support interventions on adherence in a set of common chronic conditions. By “chronic conditions” we refer to diseases that require long-term, regular clinic visits and ad-hoc changes to medication and lifestyle for which adherence has significance and for which support via telephone has been evaluated and published in peer-reviewed scientific papers. We shortlisted five chronic diseases: cancer, diabetes mellitus, heart failure, human immunodeficiency virus infection/acquired immune deficiency syndrome (HIV/AIDS), and obesity. We focused on these five diseases because the burden of these diseases differs for various societies and because we expected to be able to identify a large amount of relevant information about interventions targeting these conditions.
The main question for this research study is: Among those patients who are under treatment for any of the above-mentioned chronic diseases, does structured telephone support improve adherence compared with no telephone support as primary mode of intervention? We aimed to conduct a review of systematic and nonsystematic reviews to carefully compare the context in which the intervention is implemented and the effectiveness of interventions in each context. By “context” we refer to the sphere of influence, including adherence to medication only or to exercise, diet plans, and lifestyle as well. The cost-effectiveness of the intervention was identified as an important factor that influences the patient’s intention to consistently follow the intervention.14 To answer the main research question we defined three subquestions:
- To what extent does structured telephone support improve adherence among patients with chronic disease?
- To what extent does the frequency of telephone interventions affect adherence outcomes for patients with chronic disease?
- To what extent is structured telephone support for patients with chronic disease cost-effective, as calculated in the reviews, compared to traditional clinic visits?
Methods
Although the use of telephone for patient–physician communication and crisis hot lines began in the 1980s, more-pronounced implementation of telephone as an intervention, including modes of delivery like cell-phone calls and text messaging, began in the later years. Moreover, in the last 10 years such intervention approaches have been further expanded to adherence monitoring and adherence improvement.
We performed a review of systematic and nonsystematic reviews published in peer-reviewed health care journals between January 1, 2004 and August 31, 2014. The search was performed using the Cochrane Library, PubMed, and CINAHL. The search was limited to systematic or nonsystematic literature reviews written in English. We used search terms related to the study, including adherence (adherence, compliance, medication adherence, nonadherence, treatment adherence, concordance), telephone support (phone, mobile phone, cell phone, SMS, messaging, structured calls) and the chronic disease population (cancer, diabetes, obesity, heart failure, hypertension, HIV/AIDS). Search terms and parameters were adjusted for every database while maintaining a basic structure in the search criteria. The details of the search terms are listed in Table 1.
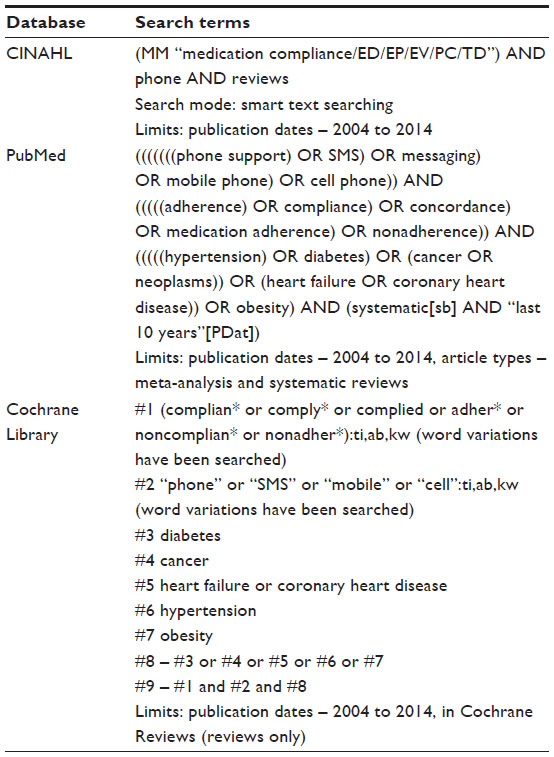 | Table 1 Search terms |
Reviews were included if they reported measured outcomes related to the usability and feasibility of the telephone as an intervention in improving adherence. Reviews that evaluated more than one intervention with the telephone or mobile phone were included if specific outcomes from telephone or mobile phone interventions were reported in the results. Interventions for adherence could vary and could include mail, fax, hand-distributed material, phone calls, and text messages. Text messages or calls and structured or unstructured telephone support with any or all of the other modes of delivery were included in the analysis. Reviews were included only if at least one of the primary outcomes measured was adherence to medication, treatment, diet, or lifestyle.
Reviews were excluded if the intervention studied did not support tasks that were directly performed by the patients, which means that the patient had to be the person on the phone in order to avoid the bias that may result when a caregiver or another person responded on behalf of the patient. Reviews that evaluated follow-up phone calls were excluded, as follow-up phone calls are most often used for gathering feedback to assess satisfaction during hospitalization or treatment and not as adherence measurements. Reviews that did not have either cost/economic analysis or frequency of messaging as one of their secondary outcomes were excluded.
One author [DB] shortlisted the eligible review articles and assessed them for the final selection (see eligible reviews in Table 2). The final list of reviews were evaluated for methodological quality, and findings were reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) Checklist, a checklist of items to be reported in a systematic review or a meta-analysis that is used to improve or evaluate the quality of reporting in health research.15 The PRISMA Checklist was not used to screen out reviews; it was used in the consideration of the strength and the reliability of findings in the included reviews. The other two authors provided regular feedback during the selection process and analysis of data. They independently verified whether the selected reviews met the inclusion criteria and if the final analysis was in line with what was identified in the included reviews. Discrepancies were discussed amongst all authors and resolved through consensus. The flow diagram of review selection (Figure 1) also follows the PRISMA Flow Diagram to ensure that the selection process is clearly depicted.
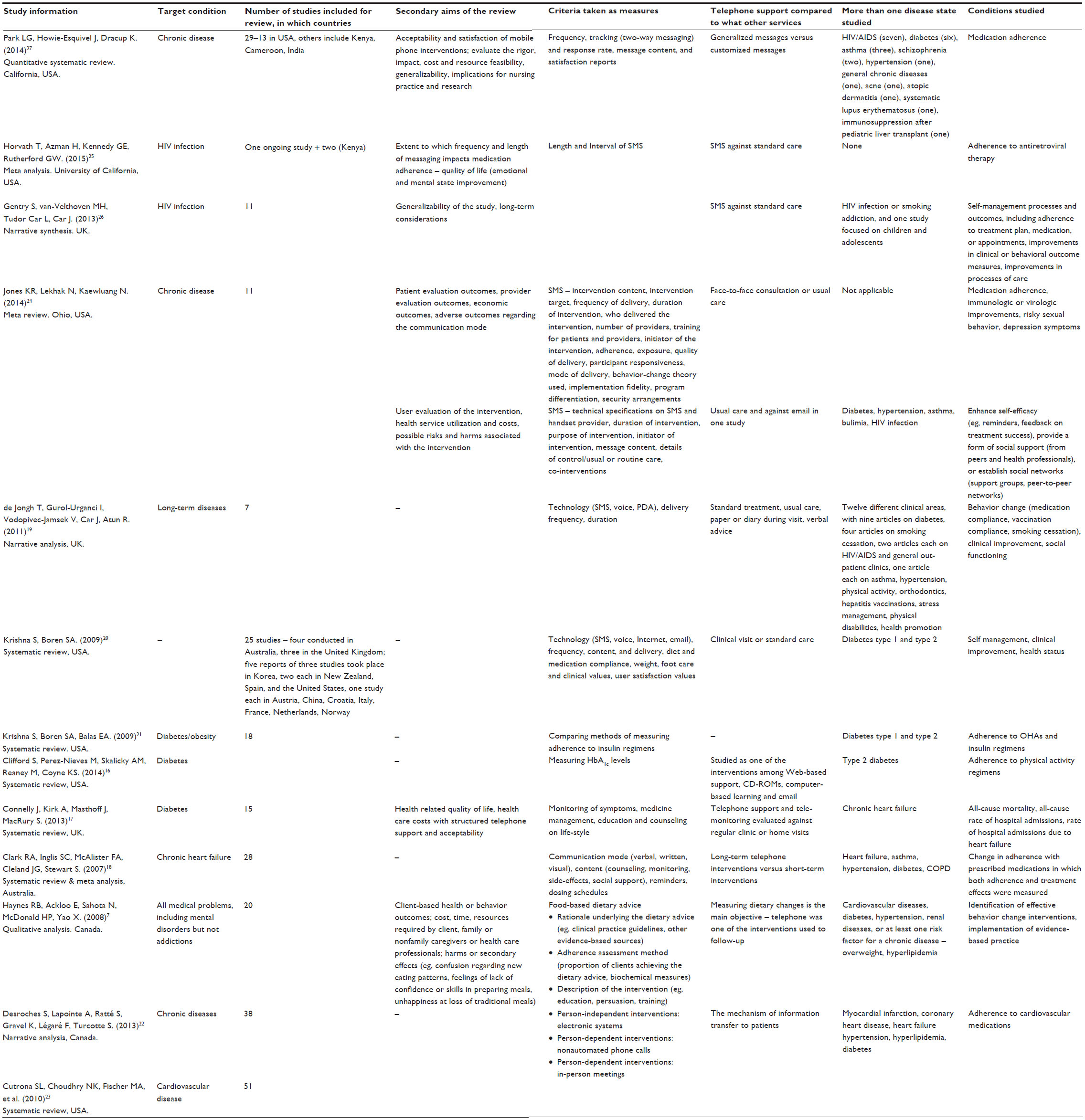 | Table 2 Reviews remaining after title screening |
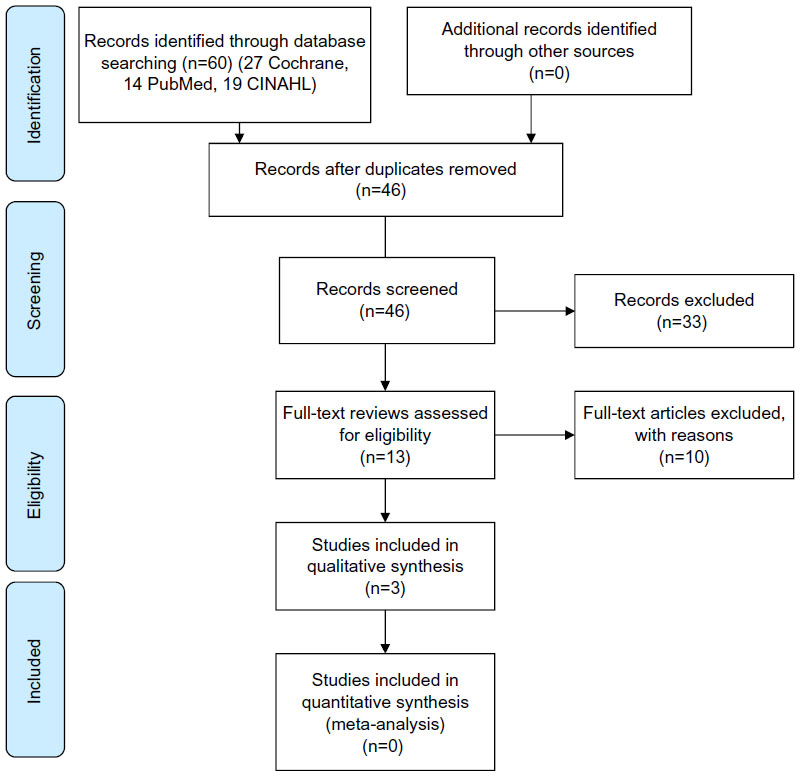 | Figure 1 Flow diagram of review selection (based on PRISMA 2009 Flow Diagram). |
Results
Study selection
The literature search from the three databases identified 60 records. After removing the duplicates, 46 unique records were left. After screening these 46 records for relevant titles and abstracts, 33 were excluded either because the telephone was not one of the interventions or the outcomes were not about treatment or medication adherence. As a result, 13 potentially relevant reviews were identified.
The data abstracted from all 13 reviews to which the inclusion criteria were applied can be found in Table 2. Among the 13 reviews, two of them, Clifford et al16 and Connelly et al,17 were excluded because they focused on how adherence is measured. The review by Clark et al18 examined how nonadherence to medication leads to hospital admissions and mortality. Because the direct relationship between the intervention and adherence rates was not discussed, this review was also excluded. De Jongh et al,19 Krishna and Boren,20 and Krishna et al21 performed reviews that studied self-efficacy in managing the disease and behavior change in dealing with the treatment, but these reviews did not directly report adherence. Desroches et al,22 Cutrona et al,23 and Haynes et al7 performed reviews that included telephone support among other types of interventions. These three reviews were excluded either because the outcome of telephone support was not reported or adherence was not directly measured as an outcome. Finally, the study by Jones et al24 is itself a meta-review of systematic reviews. As the reviews included in that article largely did not meet the inclusion criteria for our study, we excluded it.
After reading the full articles and applying the inclusion criteria as above, there were three review articles in the final selection. These three remaining reviews vary in their analysis methods. Horvath et al25 and Gentry et al,26 both retrieved from the Cochrane Library, use meta-analysis for measuring adherence. The review by Horvath et al25 presents costs and other secondary outcomes by means of a narrative analysis. The study by Park et al27 is a quantitative systematic review. All three reviews satisfied at least 20 of the 27 items in the PRISMA checklist, which indicates that the reviews can be rated moderate to high in methodological quality (Table 3).
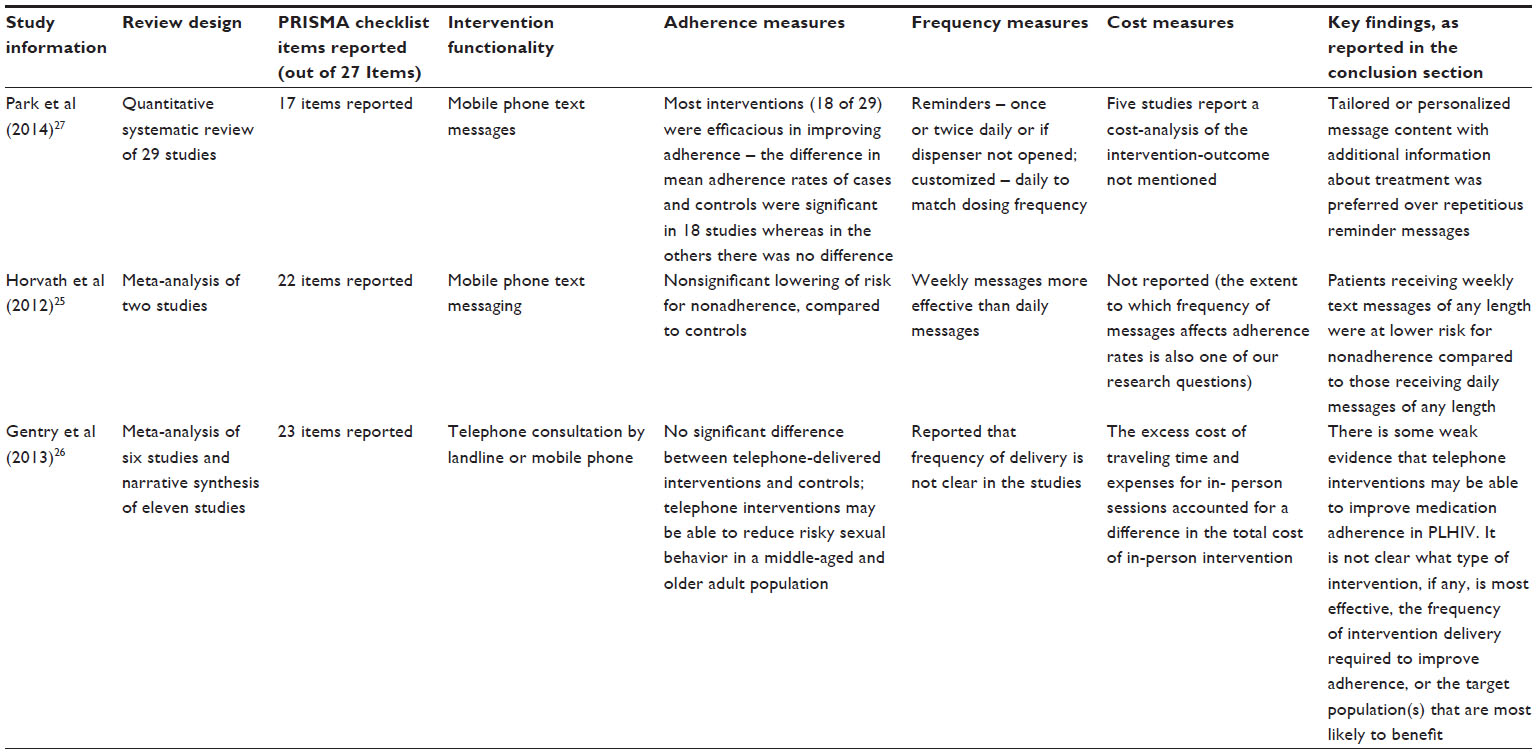 | Table 3 Effectiveness and cost-effectiveness of telephone support |
Effectiveness and cost-effectiveness of telephone support
Most of the original studies included in the reviews were conducted in the United States, and other studies were conducted in Italy, Kenya, India, Cameroon, Taiwan, Korea, and Japan. The reviews included studies conducted for preventive care as well as for the management of chronic diseases. Gentry et al26 studied the reduction of depression symptoms and risky sexual behavior in addition to medication adherence, whereas Horvath et al25 looked into adherence to antiretroviral therapy, and Park et al27 examined medication adherence in patients with chronic disease in general. The population of focus, target outcomes, and the methods of outcomes measurement varied across reviews.
As shown in Table 3, the individual reviews varied significantly in type of research design, number of studies included, mode of using the intervention, and the outcome measures. The outcomes in general were improvement in adherence, but they varied across medication, therapies, and lifestyle attributes in each study in each review. The information conveyed through telephone intervention ranged from just a reminder to take medications to educational and motivational content to change lifestyle.
The review by Park et al27 focused on prevention and management of chronic diseases. The frequency of use of telephone intervention, tracking of messages (two-way), response rate for the messages, message content, and satisfaction reports were abstracted for each study. Original studies were analyzed for medication adherence and patient-reported satisfaction. According to this review, text messages sent as reminders used basic and repetitive content and were commonly found to have negative outcomes. In contrast to this, the studies using tailored messages with educational and motivational content had positive outcomes. The timing of the message delivery was also an important consideration reported in this review. In some studies messages were delivered to match the dosing frequencies, and in one study a message was delivered if the medication dispenser was not opened on any particular day. The variations in adherence caused by message delivery time or frequency were not reported in this review. The measurement of adherence varied across studies and discordance was noted between self-reported and electronically monitored adherence rates. Cost analysis from only one study was reported.
In the review by Horvath et al,25 the content of the message and the frequency of delivery were examined. Unlike the first study, in which a range of chronic diseases in different settings were compared, in this study only HIV infection was examined. The outcome measured was adherence to antiretroviral therapy. The results were in general significant for those who received the text messages compared with the control group. However, surprisingly, in the comparison between weekly messages of any length (short or long) and the daily messages of any length, patients who received weekly messages were at lower risk for nonadherence. Cost analyses were not reported in this review.
The population studied in the review by Gentry et al26 was also HIV-infected patients. However, the outcome here was not only adherence to antiretroviral therapy, but also improvement in medication adherence, reduction of risky sexual behavior, and reduction in symptoms of depression. A high degree of clinical heterogeneity between the included studies was reported in this review. Intervention characteristics, type of provider of the intervention, characteristics of participants, and context of study population and outcome were the factors that differed. Among the six studies that reported adherence, three studies concluded that there was no statistically significant improvement in adherence by telephone intervention, while the other three studies suggested improvement. One other key finding was the low adherence in participants who received a higher number of calls. This suggested that the frequency of intervention had an impact on adherence. Telephone intervention was found to help in reducing risky sexual behavior and depression symptoms, even if the evidence is considered weak. Cost of the intervention implementation was discussed in one study and was found to be slightly lower than the in-person sessions, due to savings from travel costs. However, none of the reviews reported the cost-effectiveness of the intervention.
Discussion
On the basis of our criteria, we included three reviews only. Each of these reviews concluded that while adherence improves with telephone support, there is a lack of robust scientific evidence. Evidence on specific intervention details – including how and who should deliver the message or call, how deliverers should be trained, method of customizing the content to each patient, and frequency of delivery to each category of patients – were not discussed in detail in the included review (Gentry et al26), in which manual telephone interventions were used. Furthermore, reviews that report any systematically performed cost analysis are limited, as cost-effectiveness is examined in some papers in a review but outcomes of the analysis are not mentioned. In sum, the evidence to characterize the effectiveness or cost-effectiveness of telephone support to improve adherence among people with chronic diseases is fairly small and weak.
As the methodological quality of the reviews is rated moderate to high, the lack of sufficient evidence should be either because the studies have not reported the cost analysis data or not enough studies are conducted. Jones et al24 also reported that the studies with the highest quality scores did not report significant adherence outcomes. They used AMSTAR (Assessment of Multiple Systematic Reviews), a reliable measurement tool to assess the methodological quality of systematic reviews, to assess the included reviews.28
The frequency of telephone intervention used was measured in all three reviews, but the impact of frequency on adherence was discussed in detail in only one of the included reviews. The difference in impact between weekly and daily delivery of messages was shown in one included review, but the reason for preferring short or long messages was not discussed. It was found from these reviews that in addition to frequency of the message delivery, the content and the length of the content also created an impact on the outcome.
Other factors that (may) have affected the long-term sustainability and outcomes of the telephone intervention were not covered. The context of the population in terms of the severity of the disease might also have affected the use of the intervention.25 The symptoms patients expect and their experience of those symptoms influence their perceptions on the need for medication.13 Other issues like privacy, confidentiality, and data protection requirements, and the provider’s willingness to use the intervention,29 were not addressed in any of the reviews or the studies included in these reviews.
This review attempted to evaluate the cost effectiveness, if at all, of telephone intervention for improving adherence. However, perhaps surprisingly, of these reviews, only two reported on cost-effectiveness data and only on a very basic level. Horvath et al25 emphasized the need to keep patients sufficiently motivated to continue participation in the program and suggested that cost might be an impacting factor. Ahn et al30 reinforced that financial burden is a very important factor that influences patient preferences for use of interventions like telemedicine. The cost-effectiveness of this intervention was shown in only one study, and the results were not statistically significant. Very few studies have even addressed cost altogether. There were no details about cost analyses in the reporting or the discussion sections of any of the reviews, clearly indicating that the studies identified by the included reviews have either not intended to analyze cost-effectiveness or the results have not been reported.
This qualitative review of reviews has certain limitations. Scientific literature in the form of reviews from the three databases (Cochrane Library, PubMed, and CINAHL) have been extracted and analyzed. The results from any relevant grey literature or other original studies were not considered in this review. It is unlikely that by not including grey literature we overestimated the cost-effectiveness of telephone support.
The focus of our review was on chronic diseases and only the five mentioned chronic diseases were included in the search terms. Other chronic diseases and conditions may also be of interest when estimating the cost-effectiveness of telephone support. A recently published paper in this journal by Spinsante,31 for example, discusses the body of evidence of home telehealth in older patients with heart failure.
Finally, this is a qualitative review that discusses the outcomes from the included reviews; it does not include a quantitative analysis of the outcomes.
Conclusion
Policy makers seeking to tackle key issues and uncertainties related to specific telephone-based programs lack information from scientific studies that would help in structuring such programs in future. Estimating the cost-effectiveness is critical for implementing any new technology in health care, because widespread implementation of an intervention can be influenced by the cost to providers or other stakeholders, including the patient. Given the scarce evidence on cost-effectiveness, the telephone support interventions have to be evaluated against a comprehensive set of criteria, including their relative costs and outcomes. The content and frequency of messages also play a role in improving adherence. Compared to standard reminder messages, customized and frequent interaction with patients improves their attention to adherence. Improving adherence via telephone support is by no means a one-size-fits-all solution.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Geneva, Switzerland: World Health Organization; 2003. Available from: http://whqlibdoc.who.int/publications/2003/9241545992.pdf. Accessed November 3, 2014. | |
Saini SD, Schoenfeld P, Kaulback K, Dubinsky MC. Effect of medication dosing frequency on adherence in chronic diseases. Am J Manag Care. 2009;15(6):e22–e33. | |
Agency for Healthcare Research and Quality. Medication Adherence Interventions: Comparative Effectiveness. Closing the Quality Gap: Revisiting the State of the Science. Evidence Report No 208 (AHRQ Publication No 12-E010-1). Rockville, MD: Agency for Healthcare Research and Quality; 2012. Available from: http://effectivehealthcare.ahrq.gov/ehc/products/296/1249/EvidenceReport208_CQGMedAdherence_ExecutiveSummary_20120904.pdf. Accessed November 3, 2014. | |
Wootton R. Twenty years of telemedicine in chronic disease management – an evidence synthesis. J Telemed Telecare. 2012;18(4):211–220. | |
Mathew EM, Rajiah K. Assessment of medication adherence in type-2 diabetes patients on poly pharmacy and the effect of patient counseling given to them in a multispecialty hospital. J Basic Clin Pharm. 2013;5(1):15–18. | |
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. | |
Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008CD000011. | |
Car J, Sheikh A. Telephone consultations. BMJ. 2003;326(7396):966–969. | |
Siau K, Shen Z. Mobile healthcare informatics. Med Inform Internet Med. 2006;31(2):89–99. | |
World Health Organization. The World Health Report 2008: Primary Health Care (Now More Than Ever) [webpage on the Internet]. Geneva, Switzerland: World Health Organization; 2008. Available from: http://www.who.int/whr/2008/en/. Accessed January 29, 2015. | |
Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. | |
Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. | |
Capgemini Consulting. Patient Adherence: the Next Frontier in Healthcare. Vision and Reality, 9th Edition. Global Research Report by Capgemini Consulting. Paris, France: Capgemini; 2011. Available from: http://www.capgemini.com/resource-file-access/resource/pdf/Patient_Adherence__The_Next_Frontier_in_Patient_Care.pdf. Accessed November 3, 2014. | |
Horne R. Compliance, adherence, and concordance: implications for asthma treatment. Chest. 2006;130(1 Suppl):65S–72S. | |
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6(7):e1000100. | |
Clifford S, Perez-Nieves M, Skalicky AM, Reaney M, Coyne KS. A systematic literature review of methodologies used to assess medication adherence in patients with diabetes. Curr Med Res Opin. 2014;30(6):1071–1085. | |
Connelly J, Kirk A, Masthoff J, MacRury S. The use of technology to promote physical activity in Type 2 diabetes management: a systematic review. Diabet Med. 2013;30(12):1420–1432. | |
Clark RA, Inglis SC, McAlister FA, Cleland JG, Stewart S. Telemonitoring or structured telephone support programmes for patients with chronic heart failure: systematic review and meta-analysis. BMJ. 2007;334(7600):942–945. | |
de Jongh T, Gurol-Urganci I, Vodopivec-Jamsek V, Car J, Atun R. Mobile phone messaging for facilitating self-management of long-term illnesses. Cochrane Database Syst Rev. 2012;12:CD007459. | |
Krishna S, Boren SA. Diabetes self-management care via cell phone: a systematic review. J Diabetes Sci Technol. 2008;2(3):509–517. | |
Krishna S, Boren SA, Balas EA. Healthcare via cell phones: a systematic review. Telemed J E Health. 2009;15(3):231–240. | |
Desroches S, Lapointe A, Ratté S, Gravel K, Légaré F, Turcotte S. Interventions to enhance adherence to dietary advice for preventing and managing chronic diseases in adults. Cochrane Database Syst Rev. 2013;2:CD008722. | |
Cutrona SL, Choudhry NK, Fischer MA, et al. Modes of delivery for interventions to improve cardiovascular medication adherence. Am J Manag Care. 2010;16(12):929–942. | |
Jones KR, Lekhak N, Kaewluang N. Using mobile phones and short message service to deliver self-management interventions for chronic conditions: a meta-review. Worldviews Evid Based Nurs. 2014;11(2):81–88. | |
Horvath T, Azman H, Kennedy GE, Rutherford GW. Mobile phone text messaging for promoting adherence to antiretroviral therapy in patients with HIV infection. Cochrane Database Syst Rev. 2012;3:CD009756. | |
Gentry S, van-Velthoven MH, Tudor Car L, Car J. Telephone delivered interventions for reducing morbidity and mortality in people with HIV infection. Cochrane Database Syst Rev. 2013;5:CD009189. | |
Park LG, Howie-Esquivel J, Dracup K. A quantitative systematic review of the efficacy of mobile phone interventions to improve medication adherence. J Adv Nurs. 2014;70(9):1932–1953. | |
Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007;7:10. | |
Holtz B, Lauckner C. Diabetes management via mobile phones: a systematic review. Telemed J E Health. 2012;18(3):175–184. | |
Ahn J, Shin J, Lee J, Shin K, Park H. Consumer preferences for telemedicine devices and services in South Korea. Telemed J E Health. 2014;20(2):168–174. | |
Spinsante S. Home telehealth in older patients with heart failure – costs, adherence and outcomes. Smart Homecare Technology and Telehealth. 2014;2:93–104. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.