")
Back to Journals » Open Access Emergency Medicine » Volume 12
Telephone CPR: Current Status, Challenges, and Future Perspectives
Authors Fukushima H, Bolstad F
Received 24 April 2020
Accepted for publication 12 August 2020
Published 7 September 2020 Volume 2020:12 Pages 193—200
DOI https://doi.org/10.2147/OAEM.S259700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Hidetada Fukushima,1 Francesco Bolstad2
1Department of Emergency and Critical Care Medicine, Nara Medical University, Kashihara City, Nara, Japan; 2Department of Clinical English, Nara Medical University, Kashihara City, Nara, Japan
Correspondence: Hidetada Fukushima Email [email protected]
Abstract: With each successive update of the cardiopulmonary resuscitation (CPR) guidelines, the role of dispatchers in sudden cardiac arrest (CA) has grown. Dispatchers instruct callers in how to perform CPR until the arrival of emergency medical service (EMS) professionals. This is widely known as telephone CPR (TCPR) or dispatch-assisted CPR (DACPR). Studies have shown the efficacy of TCPR in increasing the survival rate of sudden CA. The TCPR process, however, is challenging and needs to be constantly evaluated and refined in order to improve the survival rate of sudden CA victims throughout the world. In this review article, the current status, challenges, and future perspectives of TCPR are discussed with a view to providing a research foundation from which to launch further studies into the effective role of dispatchers in sudden CA.
Keywords: out of hospital cardiac arrest, telephone cardiopulmonary resuscitation, emergency medical dispatcher
Introduction
Sudden out-of-hospital cardiac arrest (OHCA) is a leading cause of death in many countries. The incidence is reported to be 84 to 110.8 per 100,000 people in Europe and the United States.1,2 However, the rate of survival with favorable neurological outcomes rarely exceeds 10%.3–5 Bystander cardiopulmonary resuscitation (BCPR) before emergency medical services (EMS) arrival can more than double the chance of survival from OHCA.6 The significance of early BCPR is well established and the probability for survival decreases by 7% to 10% per minute if BCPR is not performed.7 Bystanders, however, often hesitate to start CPR, because they are not sure if the patient is in cardiac arrest and are not confident to perform CPR. The frequency of BCPR has been reported to be as high as 97.9%, but also as low as 5.5% in independent studies and is most commonly reported at around 40%.1,3,5,8 Emergency medical dispatchers can play a critical role in maximizing the frequency of BCPR before EMS arrival. Dispatchers can recognize CA and assist emergency callers to perform CPR via telephone. This procedure is called telephone CPR (TCPR) or dispatch-assisted CPR (DACPR). The impact of TCPR was already illustrated in the 1980s by Eisenberg et al.9 According to the literatures, TCPR accounts for the majority of BCPR.10–12 This life saving procedure is now integrated in the international resuscitation guideline.13 By identifying CA via telephone and assisting callers to initiate immediate CPR, dispatchers strengthen the chain of survival.
How Dispatchers Identify CA?
When lay people encounter a cardiac arrest case, they usually call regional emergency numbers and ask EMS to dispatch an ambulance. Call takers immediately dispatch ambulances and identify the exact location of emergency. In addition to this process, dispatchers confirm the cardiac arrest from all the various information reported by callers. Identification of CA is a fundamental part of the TCPR process. Emergency callers report various information concerning the victim such as unconsciousness, not breathing, ill facial color, cold body, and the location where they found the victims.14 Several key pieces of information can indicate a possible cardiac arrest. However, some of this information is complex and can be misleading.14,15
The recommended protocol to identify CA is called 2-question protocol.16 This standardized CA identification procedure is: 1) to assess victim’s responsiveness and 2) to make sure that the victim is not breathing normally. The sensitivity and specificity of this protocol for CA identification is reported to be 38–90% and 95–99%, respectively.9,17-21 With this protocol, there is a chance that dispatchers misdiagnose non-CA victims such as stroke, drug intoxication or syncope with CA.22,23 However, there is currently no other superior protocol available that can help dispatchers identify CA more correctly and immediately, which explains why this 2-question protocol has been adopted in many regions around the world.
When following this protocol, confirming “not breathing normally” can be surprisingly challenging.
Agonal Respiration
There are many obstacles to the dispatchers identifying CA during conversations with callers. The major and critical one is the agonal respiration that may appear right after the victim collapses. Agonal respiration is a common mammalian preterminal phenomenon in response to medullary hypoxia. This abnormal breathing appears soon after CA and disappears within a short period of time.24,25 Agonal respiration is an early sign of CA and studies indicate it is significantly associated with a high likelihood of initial shockable rhythm, which may contribute to good neurological outcomes.25–27 Lay rescuers, however, usually do not consider this movement as a sign of CA and report that CA victims with agonal respiration are unconscious, but still breathing.
Callers also describe this form of abnormal breathing as: gasping, snoring, or moaning.15,28 Descriptors for agonal respirations often vary depending on the culture or language. Each local agency should investigate how lay people in the community are likely to describe agonal respiration and try to improve CA identification based on these results. Sometimes agonal respiration can be heard in the background of the call and may help dispatchers identify CA immediately. However, it often delays CA identification.28 While dispatchers are required to identify CA from various breathing styles, according to the literature they often miss the opportunity to identify CA victims with agonal respirations.29–31
Other Obstacles to CA Identification
Other obstacles such as the callers who are upset, hang up the phone, and callers who have left the side of the victim also impede dispatch CA identification.32–34 The frequency of these obstacles varies between CAs which occur at private residencies and those which occur in public locations. Callers with victims at private residencies are more often upset than those in public places.35 Dispatchers often need to calm the callers in order to grasp the patient’s condition. On the other hand, in CA cases in public locations, dispatchers often face difficulties in obtaining information about the patient, because callers often are not by the victims’ side when they make the call. In some cases, the caller has had no contact with the victim and was simply requested to make the emergency call.35 Language barrier is another obstacle in some nations. This barrier can significantly delay the whole TCPR process.34,36
Recent study done by Stangenes et al showed that caller descriptions of victim’s medical history or chief complaints (eg, chest pain, stroke, etc.) can significantly delay dispatcher’s identification of CA when compared to descriptions of the sign or symptoms (eg, not breathing, collapsed, turning blue, etc.).37
At present, the obstacles described above are quite difficult to overcome, and there is a real need to identify new and effective measures to overcome these barriers in the future.
Improving Identification of Agonal Respiration
Generally, dispatch training includes interview techniques, computer training, medical knowledge and CPR certification. In addition to this training, educating dispatchers specifically with regard to agonal respiration through lectures can improve CA identification.31,38 Simulation training can also make a big difference.39,40 Dispatchers know that CA identification is critical, but specific education and scenario practice for CA identification, especially agonal breathing, can fill their knowledge gaps. More importantly, feedback and systematic reviews of CA dispatch calls can continuously improve the CA identification rate.15,21
Dispatch Instruction for CPR
Once dispatchers identify CA, they instruct callers to perform CPR. The various versions for CPR instruction steps described in the literature are quite similar.16,41,42 A standard sample of the steps for chest-compression only CPR is shown in Box 1.
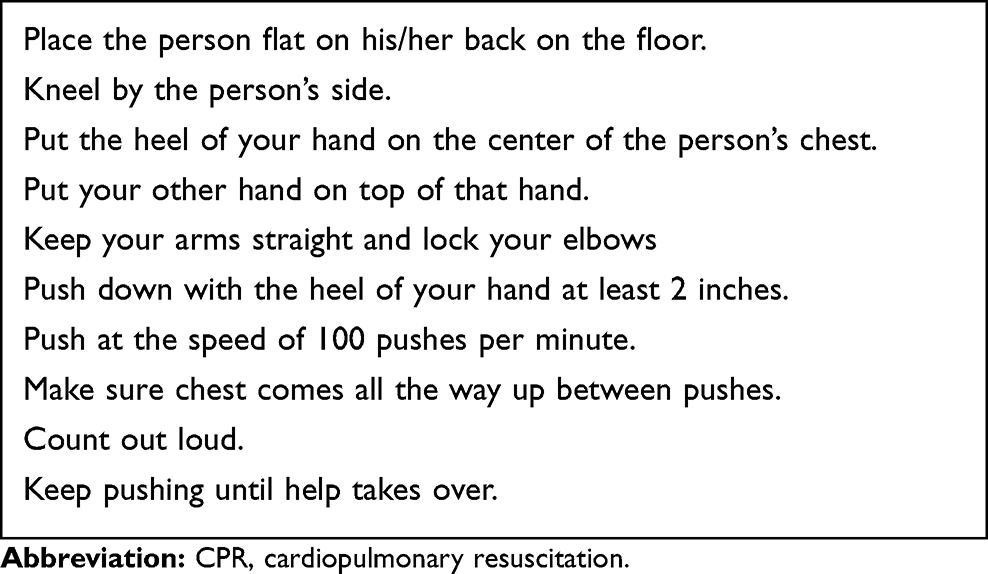 |
Box 1 Example of Telephone CPR Steps |
Nowadays, activating the speaker function of the phone has become common, reflecting the smartphone era.43,44 With this speaker function, callers can follow the dispatcher’s instruction with their hands free.
During their instructions, dispatchers need to encourage callers to perform CPR until EMS arrival, which generally takes not less than 6 to 8 minutes.8,45,46 Continuing push hard and fast chest compressions for this time period is quite hard, even for young callers.47
High-quality chest compression is essential in obtaining better outcomes of OHCA. However, it is currently impossible to monitor how well callers are performing CPR. Still, continuous verbal support from dispatchers has been shown to improve the quality of BCPR until EMS arrival.42
Instruction of Chest Compression Only CPR versus Conventional CPR
As the CPR guidelines have been revised, chest compression only CPR has become popular and has contributed to an increased frequency of bystander CPR. Many previous studies showed that both CPR techniques were equivalent in terms of prehospital return of spontaneous circulation (ROSC), survival to hospital discharge, and favorable neurological outcome.48–50 The 2015 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendation emphasize that dispatchers should provide instructions of compression only CPR for adults with suspected cardiac arrest.51 Yet, there are debates over which CPR method is better than the other.52–56 Various studies showed that conventional CPR is much better than compression only CPR for CA victims with non-cardiac origins.52–54 It is, however, almost impossible to identify the cause of cardiac arrest via emergency call. TCPR programs should adopt either one of the CPR instructions based on the presumed etiologies, distribution of CPR education, rescuers’ familiarity with CPR and the bystander CPR rate in the community. In Japan, many regional TCPR programs have adopted compression only CPR for untrained lay rescuers and this now accounts for the majority of bystander CPR.57
Telephone CPR for the Child
Even for pediatric cardiac arrest victims, TCPR can significantly increase bystander CPR and contribute to improvement in both survival and favorable neurological outcome.58–60 The debate between compression only CPR and conventional CPR is more relevant in this population. Since the major etiology of cardiac arrest is non-cardiac such as acute respiratory compromise or drowning, it is relevant that chest compression with rescue breathing can contribute more than compression only CPR to survival and favorable neurological outcome.52,53,60,61 However, the impact of both CPR techniques are equivalent for those pediatric arrests of cardiac cause.52,53 Again, dispatchers need to choose which CPR techniques to use based on both the presumed cardiac etiology and rescuers’ familiarity with CPR techniques.
Obstacles to Providing CPR Instruction
Frequently cited obstacles to the effective provision of CPR are callers’ physical disability or refusal to preform CPR.35,62 The victims’ physical position may also impede CPR. If the victim is on sofa or bed, callers need to move the victim onto a hard-flat surface such as the floor before starting CPR. Langlais reported that these obstacles appeared in 26% of CA calls and caused an average delay of more than 100 seconds to the start of CPR when compared to CA cases with no obstacles.63
Adverse Effects of TCPR for Non-CA Victims
TCPR CA identification protocol is quite simple. Thus, it is quite often that unconscious victims who are not in CA are misjudged to be in CA and receive chest compressions.22,23,30 However, chest compressions on these unconscious non-CA victims are reported to be quite safe. White et al investigated 247 unconscious non-CA victims who received CPR and reported that their most frequent complaint was chest discomfort, and rib fractures.22 Severe injuries rarely occur due to CPR on non-CA victims. If the victim is not in CA, he/she may open their eyes or try to remove rescuers hands from their chest soon after compressions are started and the damage can be quite minor. As guidelines state, no CPR for CA is more dangerous than CPR for Non-CA victims.13
The Impact on Survival
Several population-based studies have shown that introducing TCPR can increase the rate of BCPR and improve survival with favorable neurological outcome of CA.11,64–67 TCPR is reported to be independently associated with functional neurological outcomes. It is reported that its impact on survival is comparable to BCPR without dispatch CPR instruction.11,64-67 A study done by Wu et al reviewed 2310 adult OHCA with cardiac origin over 130 EMS agencies in Arizona and reported that TCPR was independently associated with favorable neurological outcome when compared to OHCA victims with BCPR without dispatch instruction (odds ratio: 1.58 and 1.56, respectively).11 Ro et al reported that the impact of TCPR was much greater than BCPR without dispatch assistance in terms of favorable neurological outcome (odds ratio: 1.58 vs 1.28).67 Although many studies reported that TCPR is an effective approach to improve CA survival, most of these are observational studies, and no randomized study has been performed yet. On the other hand, some studies reported that TCPR’s effect is similar to no BCPR and have failed to show any positive effect.68–70 It is therefore very important to focus on what leads to this difference between studies in order to improve CA survival in all communities.
TCPR Process Analysis
In order to improve the quality of TCPR, it is necessary to measure the key TCPR metrics and adjust the delivery of TCPR in order to improve these values. There is, however, no universal standardized key metrics for TCPR. Key TCPR metrics proposed or recommended in literature are shown in Table 1.
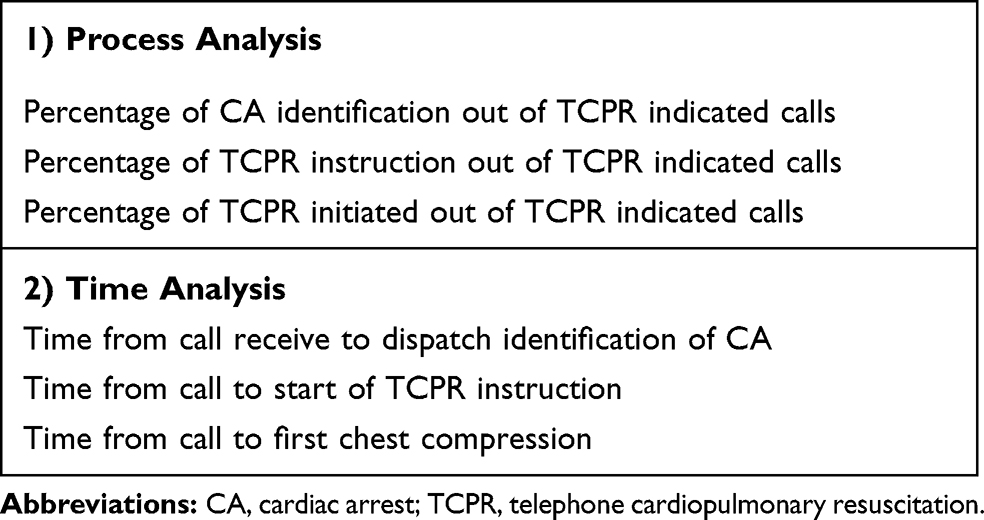 |
Table 1 The Performance of Telephone CPR |
Among the literature, the proportion of CA recognition by dispatchers ranges from around 70% to 75%.12,45,71,72 The proportion of TCPR initiation, however, drops down to 5% to 50%.12,45,71,72 Studies reported that time from call receipt to dispatch CA identification and start of CPR instruction is approximately 60 and 150 seconds.28,32,45 The time from the bystander initiating the call to the first chest compression also varies widely. It is reported to be 180 seconds to over 5 minutes.28,32,45,72 Assessing and improving local TCPR with these clearly measurable metrics will contribute to a high-performance TCPR and an improved CA survival rate.
TCPR Education for Lay Rescuers
The survival rate of sudden CA is a quality indicator of how efficiently emergency systems are working in the communities. This system is comprised of not only EMS and health care providers, but citizens who also play an important role. CPR training courses are usually available in many communities, and citizens usually have at least one chance to learn CPR in their lives. For citizens, however, it is quite difficult to maintain CPR skills, which usually decay after training.73 Therefore, dispatchers play a big role in the EMS prearrival period, and lay rescuers expect a lot from dispatchers in helping them perform CPR correctly.74 In order to familiarize citizens with TCPR, training courses which include the TCPR process are worth trialing.75
Quality Improvement Metrics for TCPR Program
In order to improve the TCPR program in the community, several key metrics should be monitored. A policy statement for TCPR from the American Heart Association76 recommends several action items: designating a medical director, evaluating how dispatchers correctly identify CA cases, measuring the time intervals of TCPR process, percentage of TCPR provision out of all OHCA cases, education in TCPR for dispatchers, and introducing a continuous quality improvement process. The policy statement also puts emphasis on encouraging the outstanding individuals who provide TCPR at exceptional level.
Future Perspectives
The new Utstein guideline has been updated and now recommends the collection of data showing whether dispatchers suspect CA or not as a core data metric.77 It is likely that the data for dispatch CA identification will soon become a quality indicator for CA survival in each community. Furthermore, standardized TCPR process analysis including the above mentioned TCPR key metrics will enable each community to compare its performance to others and to enhance its impact on survival outcomes.
In future, technological innovations can be a game changer in TCPR. Back in the 1980s, TCPR was performed through wired landlines. In this smartphone era, callers can transfer visual information of the CA to a dispatch center which may help dispatchers identify CA. Smart devices may also in the future transfer information regarding BCPR quality such as depth and rate of chest compressions so that dispatchers can support high-performance CPR.78,–80 Although these technologies are still at the experimental level, they will surely change TCPR significantly in the near future.
Conclusions
TCPR plays a major role in improving the survival of CA victims. In many regions, TCPR has been introduced and the rate of bystander CPR has been successfully improved. However, this on its own is not enough, in the future not only the frequency, but also the quality of TCPR will need further investigation. It is critical to measure TCPR metrics, improve them, and deploy high-performance TCPR.76 As we head into an unprecedented era of connectivity, it is clear that while there are still unresolved issues for TCRP that need to be addressed, TCPR will evolve further and save sudden CA victims in many regions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Virani SS, Alonso A, Benjamin EJ, et al. Heart disease and stroke statistics-2020 update: a report from the American heart association. Circulation. 2020;141:e139–e596.
2. Gräsner JT, Lefering R, Koster RW, et al. EuReCa ONE 27 Nations, ONE Europe, ONE Registry. Resuscitation. 2016;105:188–195. doi:10.1016/j.resuscitation.2016.06.004
3. Kaneko H, Hara M, Mizutani K, et al. Improving outcomes of witnessed out-of-hospital cardiac arrest after implementation of international liaison committee on resuscitation 2010 consensus: a nation wide retrospective observational population-based study. J Am Heart Assoc. 2017;6(8):e004959. doi:10.1161/JAHA.116.004959
4. Hwang SS, Ahn KO, Do Shin S, et al. Temporal trends in out-of-hospital cardiac arrest outcomes in men and women from 2008 to 2015: a national observational study. Am J Emerg Med. 2020. doi:10.1016/j.ajem.2020.01.055
5. Dyson K, Brown SP, May S, et al. International variation in survival after out-of-hospital cardiac arrest: a validation study of the Utstein template. Resuscitation. 2019;138:168–181. doi:10.1016/j.resuscitation.2019.03.018
6. Sasson C, Rogers MA, Dahl J, Kellermann AL. Predictors of survival from out-of-hospital cardiac arrest: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3:63–81. doi:10.1161/CIRCOUTCOMES.109.889576
7. Nagao K. Chest compression-only cardiocerebral resuscitation. Curr Opin Crit Care. 2009;15:189–197. doi:10.1097/MCC.0b013e3283295f2c
8. Okubo M, Kiyohara K, Iwami T, Callaway CW, Kitamura T. Nationwide and regional trends in survival from out-of-hospital cardiac arrest in Japan: a 10-year cohort study from 2005 to 2014. Resuscitation. 2017;115:120–128. doi:10.1016/j.resuscitation.2017.03.036
9. Eisenberg MS, Hallstrom AP, Carter WB, Cummins RO, Bergner L, Pierce J. Emergency CPR instruction via telephone. Am J Public Health. 1985;75:47–50. doi:10.2105/AJPH.75.1.47
10. Shimamoto T, Iwami T, Kitamura T, et al. Dispatcher instruction of chest compression-only CPR increases actual provision of bystander CPR. Resuscitation. 2015;96:9–15. doi:10.1016/j.resuscitation.2015.07.009
11. Wu Z, Panczyk M, Spaite DW, et al. Telephone cardiopulmonary resuscitation is independently associated with improved survival and improved functional outcome after out-of-hospital cardiac arrest. Resuscitation. 2018;122:135–140. doi:10.1016/j.resuscitation.2017.07.016
12. Song KJ, Shin SD, Park CB, et al. Dispatcher-assisted bystander cardiopulmonary resuscitation in a metropolitan city: a before-after population-based study. Resuscitation. 2014;85:34–41. doi:10.1016/j.resuscitation.2013.06.004
13. Travers AH, Perkins GD, Berg RA, et al. Part 3: adult basic life support and automated external defibrillation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2015;132:S51–83. doi:10.1161/CIR.0000000000000272
14. Berdowski J, Beekhuis F, Zwinderman AH, Tijssen JG, Koster RW. Importance of the first link: description and recognition of an out-of-hospital cardiac arrest in an emergency call. Circulation. 2009;119:2096–2102. doi:10.1161/CIRCULATIONAHA.108.768325
15. Bång A, Herlitz J, Martinell S. Interaction between emergency medical dispatcher and caller in suspected out-of-hospital cardiac arrest calls with focus on agonal breathing. A review of 100 tape recordings of true cardiac arrest cases. Resuscitation. 2003;56:25–34. doi:10.1016/S0300-9572(02)00278-2
16. Lerner EB, Rea TD, Bobrow BJ, et al. Emergency medical service dispatch cardiopulmonary resuscitation prearrival instructions to improve survival from out-of-hospital cardiac arrest: a scientific statement from the American Heart Association. Circulation. 2012;125:648–655. doi:10.1161/CIR.0b013e31823ee5fc
17. Clark JJ, Culley L, Eisenberg M, Henwood DK. Accuracy of determining cardiac arrest by emergency medical dispatchers. Ann Emerg Med. 1994;23:1022–1026. doi:10.1016/S0196-0644(94)70097-4
18. Flynn J, Archer F, Morgans A. Sensitivity and specificity of the medical priority dispatch system in detecting cardiac arrest emergency calls in Melbourne. Prehosp Disaster Med. 2006;21:72–76. doi:10.1017/S1049023X00003381
19. Garza AG, Gratton MC, Chen JJ, Carlson B. The accuracy of predicting cardiac arrest by emergency medical services dispatchers: the calling party effect. Acad Emerg Med. 2003;10:955–960. doi:10.1197/S1069-6563(03)00314-2
20. Kuisma M, Boyd J, Väyrynen T, Repo J, Nousila-Wiik M, Holmström P. Emergency call processing and survival from out-of-hospital ventricular fibrillation. Resuscitation. 2005;67:89–93. doi:10.1016/j.resuscitation.2005.04.008
21. Ma MH, Lu TC, Ng JC, et al. Evaluation of emergency medical dispatch in out-of-hospital cardiac arrest in Taipei. Resuscitation. 2007;73:236–245. doi:10.1016/j.resuscitation.2006.09.005
22. White L, Rogers J, Bloomingdale M, et al. Dispatcher-assisted cardiopulmonary resuscitation: risks for patients not in cardiac arrest. Circulation. 2010;121:91–97. doi:10.1161/CIRCULATIONAHA.109.872366
23. Haley KB, Lerner EB, Pirrallo RG, Croft H, Johnson A, Uihlein M. The frequency and consequences of cardiopulmonary resuscitation performed by bystanders on patients who are not in cardiac arrest. Prehosp Emerg Care. 2011;15:282–287. doi:10.3109/10903127.2010.541981
24. Manole MD, Hickey RW. Preterminal gasping and effects on the cardiac function. Crit Care Med. 2006;34:S438–41. doi:10.1097/01.CCM.0000246010.88375.E4
25. Bobrow BJ, Zuercher M, Ewy GA, et al. Gasping during cardiac arrest in humans is frequent and associated with improved survival. Circulation. 2008;118:2550–2554. doi:10.1161/CIRCULATIONAHA.108.799940
26. Zhang Q, Liu B, Qi Z, Li C. Prognostic value of gasping for short and long outcomes during out-of-hospital cardiac arrest: an updated systematic review and meta-analysis. Scand J Trauma Resusc Emerg Med. 2018;26:106. doi:10.1186/s13049-018-0575-1
27. Debaty G, Labarere J, Frascone RJ, et al. Long-term prognostic value of gasping during out-of-hospital cardiac arrest. J Am Coll Cardiol. 2017;70:1467–1476. doi:10.1016/j.jacc.2017.07.782
28. Fukushima H, Panczyk M, Hu C, et al. Description of abnormal breathing is associated with improved outcomes and delayed telephone cardiopulmonary resuscitation instructions. J Am Heart Assoc. 2017;6:e005058. doi:10.1161/JAHA.116.005058
29. Brinkrolf P, Metelmann B, Scharte C, Zarbock A, Hahnenkamp K, Bohn A. Bystander-witnessed cardiac arrest is associated with reported agonal breathing and leads to less frequent bystander CPR. Resuscitation. 2018;127:114–118. doi:10.1016/j.resuscitation.2018.04.017
30. Fukushima H, Imanishi M, Iwami T, et al. Implementation of a dispatch-instruction protocol for cardiopulmonary resuscitation according to various abnormal breathing patterns: a population-based study. Scand J Trauma Resusc Emerg Med. 2015;23:64. doi:10.1186/s13049-015-0145-8
31. Bohm K, Stålhandske B, Rosenqvist M, Ulfvarson J, Hollenberg J, Svensson L. Tuition of emergency medical dispatchers in the recognition of agonal respiration increases the use of telephone assisted CPR. Resuscitation. 2009;80:1025–1028. doi:10.1016/j.resuscitation.2009.06.004
32. Dameff C, Vadeboncoeur T, Tully J, et al. A standardized template for measuring and reporting telephone pre-arrival cardiopulmonary resuscitation instructions. Resuscitation. 2014;85:869–873. doi:10.1016/j.resuscitation.2014.02.023
33. Alfsen D, Møller TP, Egerod I, Lippert FK. Barriers to recognition of out-of-hospital cardiac arrest during emergency medical calls: a qualitative inductive thematic analysis. Scand J Trauma Resusc Emerg Med. 2015;23:70. doi:10.1186/s13049-015-0149-4
34. Case R, Cartledge S, Siedenburg J, et al. Identifying barriers to the provision of bystander cardiopulmonary resuscitation (CPR) in high-risk regions: a qualitative review of emergency calls. Resuscitation. 2018;129:43–47. doi:10.1016/j.resuscitation.2018.06.001
35. Fukushima H, Panczyk M, Spaite DW, et al. Barriers to telephone cardiopulmonary resuscitation in public and residential locations. Resuscitation. 2016;109:116–120. doi:10.1016/j.resuscitation.2016.07.241
36. Nuño T, Bobrow BJ, Rogge-Miller KA, et al. Disparities in telephone CPR access and timing during out-of-hospital cardiac arrest. Resuscitation. 2017;115:11–16. doi:10.1016/j.resuscitation.2017.03.028
37. Stangenes SR, Painter IS, Rea TD, et al. Delays in recognition of the need for telephone-assisted CPR due to caller description of chief complaint. Resuscitation. 2020;149:82–86. doi:10.1016/j.resuscitation.2020.02.013
38. Tanaka Y, Taniguchi J, Wato Y, Yoshida Y, Inaba H. The continuous quality improvement project for telephone-assisted instruction of cardiopulmonary resuscitation increased the incidence of bystander CPR and improved the outcomes of out-of-hospital cardiac arrests. Resuscitation. 2012;83:1235–1241. doi:10.1016/j.resuscitation.2012.02.013
39. Hardeland C, Skåre C, Kramer-Johansen J, et al. Targeted simulation and education to improve cardiac arrest recognition and telephone assisted CPR in an emergency medical communication centre. Resuscitation. 2017;114:21–26. doi:10.1016/j.resuscitation.2017.02.013
40. Meischke H, Painter IS, Stangenes SR, et al. Simulation training to improve 9-1-1 dispatcher identification of cardiac arrest: a randomized controlled trial. Resuscitation. 2017;119:21–26. doi:10.1016/j.resuscitation.2017.07.025
41. Rodriguez SA, Sutton RM, Berg MD, et al. Simplified dispatcher instructions improve bystander chest compression quality during simulated pediatric resuscitation. Resuscitation. 2014;85:119–123. doi:10.1016/j.resuscitation.2013.09.003
42. Birkenes TS, Myklebust H, Neset A, Kramer-Johansen J. Quality of CPR performed by trained bystanders with optimized pre-arrival instructions. Resuscitation. 2014;85:124–130. doi:10.1016/j.resuscitation.2013.09.015
43. Birkenes TS, Myklebust H, Kramer-Johansen J. Time delays and capability of elderly to activate speaker function for continuous telephone CPR. Scand J Trauma Resusc Emerg Med. 2013;21:40. doi:10.1186/1757-7241-21-40
44. Steensberg AT, Eriksen MM, Andersen LB, et al. Bystander capability to activate speaker function for continuous dispatcher assisted CPR in case of suspected cardiac arrest. Resuscitation. 2017;115:52–55. doi:10.1016/j.resuscitation.2017.04.002
45. Lewis M, Stubbs BA, Eisenberg MS. Dispatcher-assisted cardiopulmonary resuscitation: time to identify cardiac arrest and deliver chest compression instructions. Circulation. 2013;128:1522–1530. doi:10.1161/CIRCULATIONAHA.113.002627
46. Kragholm K, Wissenberg M, Mortensen RN, et al. Return to work in out-of-hospital cardiac arrest survivors: a nationwide register-based follow-up study. Circulation. 2015;131:1682–1690. doi:10.1161/CIRCULATIONAHA.114.011366
47. Nebsbjerg MA, Rasmussen SE, Bomholt KB, et al. Skills among young and elderly laypersons during simulated dispatcher assisted CPR and after CPR training. Acta Anaesthesiol Scand. 2018;62:125–133. doi:10.1111/aas.13027
48. SOS-KANTO Group. Cardiopulmonary resuscitation by bystanders with chest compression only (SOS-KANTO): an observational study. Lancet. 2007;369:920–921. doi:10.1016/S0140-6736(07)60451-6
49. Iwami T, Kawamura T, Hiraide A, et al. Effectiveness of bystander-initiated cardiac-only resuscitation for patients with out-of-hospital cardiac arrest. Circulation. 2007;116:2900–2907. doi:10.1161/CIRCULATIONAHA.107.723411
50. Bohm K, Rosenqvist M, Herlitz J, et al. Survival is similar after standard treatment and chest compression only in out-of-hospital bystander cardiopulmonary resuscitation. Circulation. 2007;116:2908–2912. doi:10.1161/CIRCULATIONAHA.107.710194
51. Nolan JP, Hazinski MF, Aickin R, et al. Part 1: executive summary: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Resuscitation. 2015;95:e1–31. doi:10.1016/j.resuscitation.2015.07.039
52. Kitamura T, Iwami T, Kawamura T, et al. Conventional and chest-compression-only cardiopulmonary resuscitation by bystanders for children who have out-of-hospital cardiac arrests: a prospective, nationwide, population-based cohort study. Lancet. 2010;375:1347–1354. doi:10.1016/S0140-6736(10)60064-5
53. Ogawa T, Akahane M, Koike S, et al. Outcomes of chest compression only CPR versus conventional CPR conducted by lay people in patients with out of hospital cardiopulmonary arrest witnessed by bystanders: nationwide population based observational study. BMJ. 2011;342:c7106. doi:10.1136/bmj.c7106
54. Panchal AR, Bobrow BJ, Spaite DW, et al. Chest compression-only cardiopulmonary resuscitation performed by lay rescuers for adult out-of-hospital cardiac arrest due to non-cardiac aetiologies. Resuscitation. 2013;84:435–439. doi:10.1016/j.resuscitation.2012.07.038
55. Iwami T, Kitamura T, Kiyohara K, Kawamura T. Dissemination of chest compression-only cardiopulmonary resuscitation and survival after out-of-hospital cardiac arrest. Circulation. 2015;132:415–422. doi:10.1161/CIRCULATIONAHA.114.014905
56. Balzanelli MG, Lazzaro R, Distratis P, et al. Consequences of compression-only cardiopulmonary resuscitation performed by bystanders under telephone instructions in out-of-hospital cardiac arrests. Minerva Anestesiol. 2020;86:354–355. doi:10.23736/S0375-9393.19.14036-9
57. Kitamura T, Kiyohara K, Nishiyama C, et al. Chest compression-only versus conventional cardiopulmonary resuscitation for bystander-witnessed out-of-hospital cardiac arrest of medical origin: a propensity score-matched cohort from 143,500 patients. Resuscitation. 2018;126:29–35. doi:10.1016/j.resuscitation.2018.02.017
58. Akahane M, Ogawa T, Tanabe S, et al. Impact of telephone dispatcher assistance on the outcomes of pediatric out-of-hospital cardiac arrest. Crit Care Med. 2012;40:1410–1416. doi:10.1097/CCM.0b013e31823e99ae
59. Chang I, Ro YS, Shin SD, Song KJ, Park JH, Kong SY. Association of dispatcher-assisted bystander cardiopulmonary resuscitation with survival outcomes after pediatric out-of-hospital cardiac arrest by community property value. Resuscitation. 2018;132:120–126. doi:10.1016/j.resuscitation.2018.09.008
60. Naim MY, Burke RV, McNally BF, et al. Association of bystander cardiopulmonary resuscitation with overall and neurologically favorable survival after pediatric out-of-hospital cardiac arrest in the United States: a report from the cardiac arrest registry to enhance survival surveillance registry. JAMA Pediatr. 2017;171:133–141. doi:10.1001/jamapediatrics.2016.3643
61. Zhang X, Zhang W, Wang C, Tao W, Dou Q, Yang Y. Chest-compression-only versus conventional cardiopulmonary resuscitation by bystanders for children with out-of-hospital cardiac arrest: a systematic review and meta-analysis. Resuscitation. 2019;134:81–90. doi:10.1016/j.resuscitation.2018.10.032
62. Ho AF, Sim ZJ, Shahidah N, et al. Barriers to dispatcher-assisted cardiopulmonary resuscitation in Singapore. Resuscitation. 2016;105:149–155. doi:10.1016/j.resuscitation.2016.05.006
63. Langlais BT, Panczyk M, Sutter J, et al. Barriers to patient positioning for telephone cardiopulmonary resuscitation in out-of-hospital cardiac arrest. Resuscitation. 2017;115:163–168. doi:10.1016/j.resuscitation.2017.03.034
64. Rea TD, Eisenberg MS, Culley LL, Becker L. Dispatcher-assisted cardiopulmonary resuscitation and survival in cardiac arrest. Circulation. 2001;104:2513–2516. doi:10.1161/hc4601.099468
65. Noel L, Jaeger D, Baert V, et al. Effect of bystander CPR initiated by a dispatch centre following out-of-hospital cardiac arrest on 30-day survival: adjusted results from the French National Cardiac Arrest Registry. Resuscitation. 2019;144:91–98. doi:10.1016/j.resuscitation.2019.08.032
66. Nishi T, Kamikura T, Funada A, Myojo Y, Ishida T, Inaba H. Are regional variations in activity of dispatcher-assisted cardiopulmonary resuscitation associated with out-of-hospital cardiac arrests outcomes? A nation-wide population-based cohort study. Resuscitation. 2016;98:27–34. doi:10.1016/j.resuscitation.2015.10.004
67. Ro YS, Shin SD, Lee YJ, et al. Effect of dispatcher-assisted cardiopulmonary resuscitation program and location of out-of-hospital cardiac arrest on survival and neurologic outcome. Ann Emerg Med. 2017;69:52–61.e1. doi:10.1016/j.annemergmed.2016.07.028
68. Hatakeyama T, Kiguchi T, Kobayashi D, et al. Effectiveness of dispatcher instructions-dependent or independent bystander cardiopulmonary resuscitation on neurological survival among patients with out-of-hospital cardiac arrest. J Cardiol. 2020;75:315–322. doi:10.1016/j.jjcc.2019.08.007
69. Group JCSRSS. Chest-compression-only bystander cardiopulmonary resuscitation in the 30:2 compression-to-ventilation ratio era. Nationwide observational study. Circ J. 2013;77:2742–2750. doi:10.1253/circj.CJ-13-0457
70. Shibahashi K, Ishida T, Kuwahara Y, Sugiyama K, Hamabe Y. Effects of dispatcher-initiated telephone cardiopulmonary resuscitation after out-of-hospital cardiac arrest: a nationwide, population-based, cohort study. Resuscitation. 2019;144:6–14. doi:10.1016/j.resuscitation.2019.08.031
71. Hauff SR, Rea TD, Culley LL, Kerry F, Becker L, Eisenberg MS. Factors impeding dispatcher-assisted telephone cardiopulmonary resuscitation. Ann Emerg Med. 2003;42:731–737. doi:10.1016/S0196-0644(03)00423-2
72. Oman G, Bury G. Use of telephone CPR advice in Ireland: uptake by callers and delays in the assessment process. Resuscitation. 2016;102:6–10. doi:10.1016/j.resuscitation.2016.02.006
73. Chamberlain DA, Hazinski MF, Council ER, et al. Education in resuscitation: an ILCOR symposium: Utstein Abbey: Stavanger, Norway: june 22–24, 2001. Circulation. 2003;108:2575–2594. doi:10.1161/01.CIR.0000099898.11954.3B
74. Mathiesen WT, Birkenes TS, Lund H, Ushakova A, Søreide E, Bjørshol CA. Public knowledge and expectations about dispatcher assistance in out-of-hospital cardiac arrest. J Adv Nurs. 2019;75:783–792. doi:10.1111/jan.13886
75. Kim TH, Lee YJ, Lee EJ, et al. Comparison of cardiopulmonary resuscitation quality between standard versus telephone-basic life support training program in middle-aged and elderly housewives: a randomized simulation study. Simul Healthc. 2018;13:27–32. doi:10.1097/SIH.0000000000000286
76. Kurz MC, Bobrow BJ, Buckingham J, et al. Telecommunicator cardiopulmonary resuscitation: a policy statement from the American Heart Association. Circulation. 2020;141:e686–e700.
77. Perkins GD, Jacobs IG, Nadkarni VM, et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein resuscitation registry templates for out-of-hospital cardiac arrest: a statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation. Resuscitation. 2015;96:328–340. doi:10.1016/j.resuscitation.2014.11.002
78. Ecker H, Lindacher F, Adams N, et al. Video-assisted cardiopulmonary resuscitation via smartphone improves quality of resuscitation: a randomised controlled simulation trial. Eur J Anaesthesiol. 2020;37:294–302. doi:10.1097/EJA.0000000000001177
79. White AE, Ng HX, Ng WY, et al. Measuring the effectiveness of a novel CPRcard™ feedback device during simulated chest compressions by non-healthcare workers. Singapore Med J. 2017;58:438–445. doi:10.11622/smedj.2017072
80. Ecker H, Wingen S, Hamacher S, et al. Evaluation of CPR quality via smartphone with livestream-a study in a metropolitan area. Prehosp Emerg Care. 2020;1–6. doi:10.1080/10903127.2020.1734122.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.