")
Back to Archived Journals » Smart Homecare Technology and TeleHealth » Volume 6
Telemedicine in Resource-Limited Setting: Narrative Synthesis of Evidence in Nepalese Context
Authors Siddiquee NKA , Poudyal A , Pandey A , Shrestha N , Karki S , Subedi R , Sah AK , KC D
Received 21 August 2019
Accepted for publication 13 December 2019
Published 3 January 2020 Volume 2019:6 Pages 1—14
DOI https://doi.org/10.2147/SHTT.S227854
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yelena Yesha
Noor Kutubul Alam Siddiquee, Anil Poudyal, Ashok Pandey, Namuna Shrestha, Shristi Karki, Ranjeeta Subedi, Arun Kumar Sah, Dirghayu KC
Nepal Health Research Council, Kathmandu, Nepal
Correspondence: Noor Kutubul Alam Siddiquee
FK Exchange Fellow. Nepal Health Research Council, Apt- 11D, Mars Tower, Grande Towers, Tokha, Kathmandu, Nepal
Tel +977 9840260572
Email [email protected]
Abstract: The traditional model of health services imposes limitations, especially in resource-limited countries like Nepal. Introduction to information technology can mitigate various challenges like geographic complexity, urban-rural disparity, poor accessibility, shortage of healthcare professionals, inadequate health facilities, higher cost, and time. Nepal is a resource-limited country with diverse geographic features making it hard to have proper access to healthcare facilities. Telemedicine service has the potential to improve service quality and accessibility of the disadvantaged and underserved population by overcoming the existing challenges. The objective of this review was to explore the roles of telemedicine in vanquishing existing challenges. Seven data sources (namely CINAHL, PubMed, POPLINE, Web of Science, Scopus, DOAJ and Summon) were consulted using five keywords (telemedicine, telehealth, eHealth, mHealth and Nepal to find the literature using the Boolean operator AND) to obtain the relevant materials. The narrative synthesis method was used to review papers and to analyze the findings. This review selected 27 papers for further analysis by scrutinizing 1161 initial search results. The most common features of telemedicine services so far, implemented or piloted in Nepal, were addressing geographic remoteness (21%), a shortage of in healthcare service providers (11%), saving time (11%), addressing challenges of extreme conditions (10%), cost saving (9%), service quality (9%) and real-time services (8%). Some other features of telemedicine were communication, transportation, referral, collaboration, addressing challenges in proper diagnosis and the shortage of health professionals. In a nutshell, the review findings suggested improved service quality, increased collaboration and accessibility and decreased the disparity in comparison with traditional health service models. Although it cannot be said that telemedicine in Nepal has been mainstreamed, yet the appeal is increasing due to its positive impact, especially in rural and hard-to-reach areas where with a lack of healthcare set-up and professionals.
Keywords: barriers, health facilities, health professionals, opportunities, quality
Introduction
Enhancing accessibility for the population as a whole and utilization of health services is paramount to achieving faster and sustained improvement in health status.1 People’s accessibility in healthcare varies from and within cultures and countries. In general, people of Low and Middle Income (LMICs) countries have comparatively less access to health services. LMICs account for 90% of the world’s diseases but compose only 12% of the world’s health expenditures.2 In LMICs, proper accessibility is still to be ensured, there is a lack of adequate number of health service providers, required skills and adequate resources including healthcare settings.2 The perception about accessibility also varies greatly, from one perspective it can refer to geographic availability.3 Penchansky and Thomas (1981) present a far broader definition of accessibility highlighting four dimensions: availability, accessibility, affordability, and acceptability.4
The need for a more comprehensive and people-friendly method of providing quality healthcare services, coupled with relevant development in information and communications technology (ICT) has caused increased use of ICT applications over the past decade.5 The application of ICTs in healthcare services has helped to expand healthcare provision in several ways. For example, telemedicine and other forms of technology-based distant services have contributed significantly to provide quality services in terms of diagnosis, patient care, capacity building of healthcare professionals, coverage, referrals, etc.
Telemedicine is comparatively a new method to provide healthcare services for patients in a resource-efficient way. Patients do not need to travel distant places to get expert consultation; rather treatment-related decisions are made at the local level, close to the patient’s location using information and communication technologies (ICTs). Telemedicine did not arise as a separate and well-defined discipline with separate technologies but combines existing technologies in the healthcare sector to overcome geographical barriers, shortage of service providers, inadequate infrastructures and increase overall accessibility.6 This innovation is especially beneficial for rural, marginal, underserved communities in developing countries and in emergency or extreme conditions.5
Distance between patients and health professionals can limit healthcare provision significantly, especially in rural areas. Telemedicine in this regard can make healthcare services available for a greater population. According to the WHO Global Observatory for eHealth series – Volume 2, telemedicine has increased the accessibility which effectively helped to meet the previously unfulfilled needs and has a positive impact on health services.5 The same report mentioned four elements as germane to telemedicine-
- To provide clinical support.
- To overcome geographical barriers.
- Use of various forms of ICT.
- Improved health outcomes.
According to the government of Nepal and the UN, Nepal is one of the underdeveloped countries with a low human development index.7 The country is geographically diverse containing hill, mountains and plain lands; and around 83% of its total population still live in the rural areas. Over the last couple of decades, Nepal has worked hard to expand its healthcare network throughout the country and to reduce inequality.8 Despite this progress, the country is still confined by some dominant health challenges. Many citizens face financial, socio-cultural, geographical, and institutional barriers in terms of accessibility to healthcare. Disparities exist depending on the social status, geographic positionality, remoteness, communication system, availability of skilled healthcare service providers and an adequate number of healthcare facilities.8
The traditional model of health service delivery requires physical visits of patients to the healthcare facilities. Physical visit of the patients and their caregivers can be described from the perspectives of transportation, communication, skilled workforce and adequate equipment. While poor communication, distance and travel time impose a challenge to access quality healthcare services, telemedicine has the potential to overcome geographic barriers and connects patients with specialized service providers efficiently.9 Thus, telemedicine can be particularly beneficial for people living in underserved and hard-to-reach areas where lack of both health facilities and healthcare professionals exist.10–12
This paper has been prepared based on a narrative review of available literature in order to understand the role of telemedicine to reduce existing inequality and to increase overall accessibility to healthcare services. The review was conducted following some specific questions:
- Role of telemedicine services in Nepal helping to minimize the barriers of geographic difficulties and emergency situations.
- The role of telemedicine services in Nepal helping to increase people’s accessibility regardless of economic capacity, gender difference, age difference, ethnic difference, religious difference, etc.
- Whether telemedicine has helped to overcome the limitations of not having adequate number of healthcare facilities and skilled health service providers.
Materials and Methods
This review work used a narrative synthesis method in order to meet the objectives. A comprehensive literature search was included in the review work using a stepwise system to identify all relevant literature. Then, relevant information was extracted through narrative synthesis using a qualitative approach.
Search Strategy
In this review, we used seven data sources, namely CINAHL, PubMed, POPLINE, Web of Science, Scopus, DOAJ (Directory of Open Access Journals Search) and Summon in order to find out the relevant materials. We considered telemedicine as a communication term and used other words and concepts which followed the broad description of telemedicine. We identified the MESH terms of telemedicine using the PubMed search engine. This review included three other terms, such as telehealth, eHealth and mHealth; which are synonymous in this review and will be used interchangeably.
Finally, we used keywords including telemedicine, telehealth, eHealth, mHealth and Nepal to find the literature using the Boolean operator AND.
Inclusion Criteria
This review has taken the definition of telemedicine from WHO, which states – a system of “healing at a distance” signifying the use of ICT to improve patient outcomes by increasing access to care and medical information.13 In order to present a broad definition, we also considered the definition adopted by WHO containing the following description:
The delivery of health care services, where distance is a critical factor, by all health care professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of health care providers, all in the interests of advancing the health of individuals and their communities.14
Initially, we wanted to put no further barriers as the number of scholarly documents were limited in the Nepalese context. Later, we only included materials produced based on activities related to telemedicine.
Detailed inclusion criteria aimed to include materials focused on-
- If it addresses the accessibility issue of underserved, marginalized, rural and disadvantaged population in general.
- If it addresses communication gaps and the problem regarding the distance of healthcare facilities.
- If it aims to save time and to overcome geographical differences.
- If it aims to minimize the challenges due to inadequate infrastructure and a shortage of healthcare service providers.
Selection of Material
This search yielded 1161 materials, including project reports, review articles, clinical trials, original research articles, opinion pieces, communication materials, technical notes, workshop/conference preceding, observational notes, study/project protocols, editorials, strategy papers, etc. Reviewers then scrutinized the titles, context, objectives and abstract (where available). Sometimes reviewers had to face problems selecting the right materials by going through titles, context (country), objectives and abstract. In that case, they had to go through and review the full text. Following this review procedure, reviewers identified a total of 27 materials.
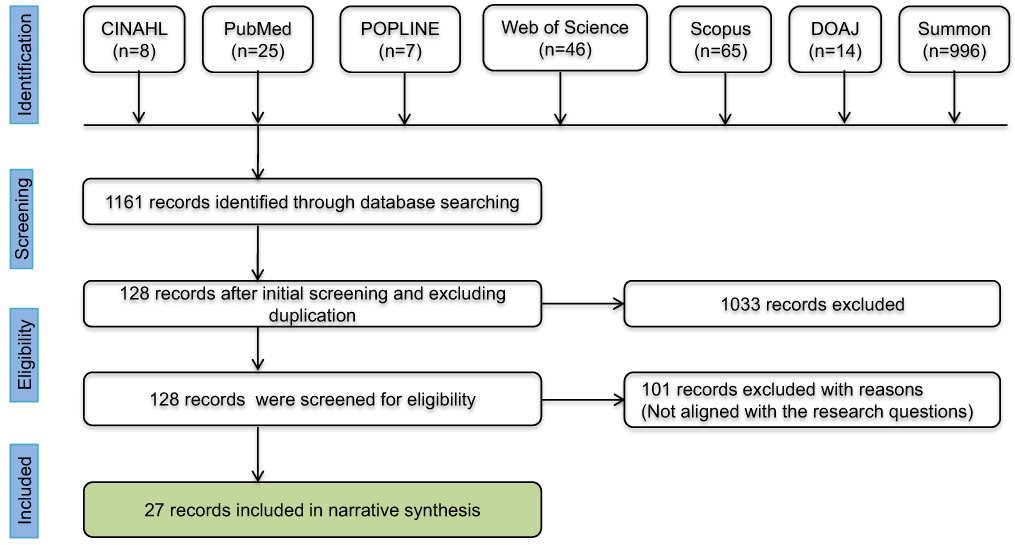 |
Figure 1 Stepwise flow diagram on selection of materials for the review. Abbreviations: CINAHL, cumulative index to nursing and allied health literature; POPLINE, population information online; DOAJ, directory of open access journals. |
Analysis Methods
Data extraction and analysis for the scholarly materials selected through the screening process were undertaken by all the authors and the data was then recorded in a previously developed matrix. We did not summarize any outcome measures; therefore, assessment of bias was not done. Given the high levels of heterogeneity among the included materials, data analysis took the form of a narrative synthesis of the evidence.15 The narrative synthesis approach is especially helpful for synthesizing the information of documents crossing disciplinary boundaries and when scientific research fails to present to adequate evidence.16,17
Data extracted for each selected material included, where available:
- Subject area of intervention
- Types of the intervention/study
- Target population
- Brief overview of the intervention/study
- Target group/population
- Geographic area
- Background/context details
- Outcomes/findings
- Technology used
Limitations of the Review
It is likely that many of the evidence on Telemedicine in Nepal were excluded from this review because of fixed inclusion criteria. This review considered pieces’ evidence in only the Nepalese context. But there are many other countries with similar types of challenges, where authorities are also implementing telemedicine. If those evidence could have included, this review would have provided a more comprehensive scenario. In that case, the findings of this review cannot be generalized to other contexts with similar characteristics and challenges.
The research questions were not relevant to issues like theoretical framework, methodology, sampling, ethical issues, etc.; which leaves room for reporting bias. As a result, this review did not assess these issues. In addition to these, this review only included seven electronic search databases, grey literature, thesis and, dissertations were excluded. These limitations may increase the selection bias.
Definition of Key Terms
Telemedicine: The delivery of healthcare services, where distance is a critical factor, by all healthcare professionals using information and communication technologies for the exchange of valid information for diagnosis, treatment and prevention of disease and injuries, research and evaluation, and for the continuing education of healthcare providers, all in the interests of advancing the health of individuals and their communities.14
Telehealth: Telehealth involves the use of telecommunications and virtual technology to deliver health care outside of traditional health-care facilities. Telehealth examples include virtual home health care, where patients such as the chronically ill or the elderly may receive guidance in certain procedures while remaining at home. Telehealth has also made it easier for healthcare workers in remote field settings to obtain guidance from professionals elsewhere in diagnosis, care and referral of patients.18
mHealth: mHealth is a component of eHealth. The Global Observatory for eHealth (GOe) defined mHealth or mobile health as medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants (PDAs), and other wireless devices. mHealth involves the use and capitalization on a mobile phone’s core utility of voice and short messaging service (SMS) as well as more complex functionalities and applications including general packet radio service (GPRS), third and fourth generation mobile telecommunications (3G and 4G systems), global positioning system (GPS), and Bluetooth technology.19
eHealth: eHealth is an emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the Internet and related technologies. In a broader sense, the term characterizes not only a technical development, but also a state-of-mind, a way of thinking, an attitude, and a commitment for networked, global thinking, to improve health care locally, regionally, and worldwide by using information and communication technology.20
Accessibility: World Health Organization (WHO) defines accessibility in three layers. In this study, we have considered all these types of accessibility. Key issues of accessibility are21 -
- Availability of good health services within reasonable reach of those who need them and of the opening hours, appointment systems and other aspects of service organization and delivery that allow people to obtain the services when required.
- People’s ability to pay for services without financial hardship. It takes into account not only the price of the health services but also indirect and opportunity costs (e.g. the costs of transportation to and from facilities and of taking time away from work).
- Rights to seek, receive and impart information and ideas concerning health issues.
Results
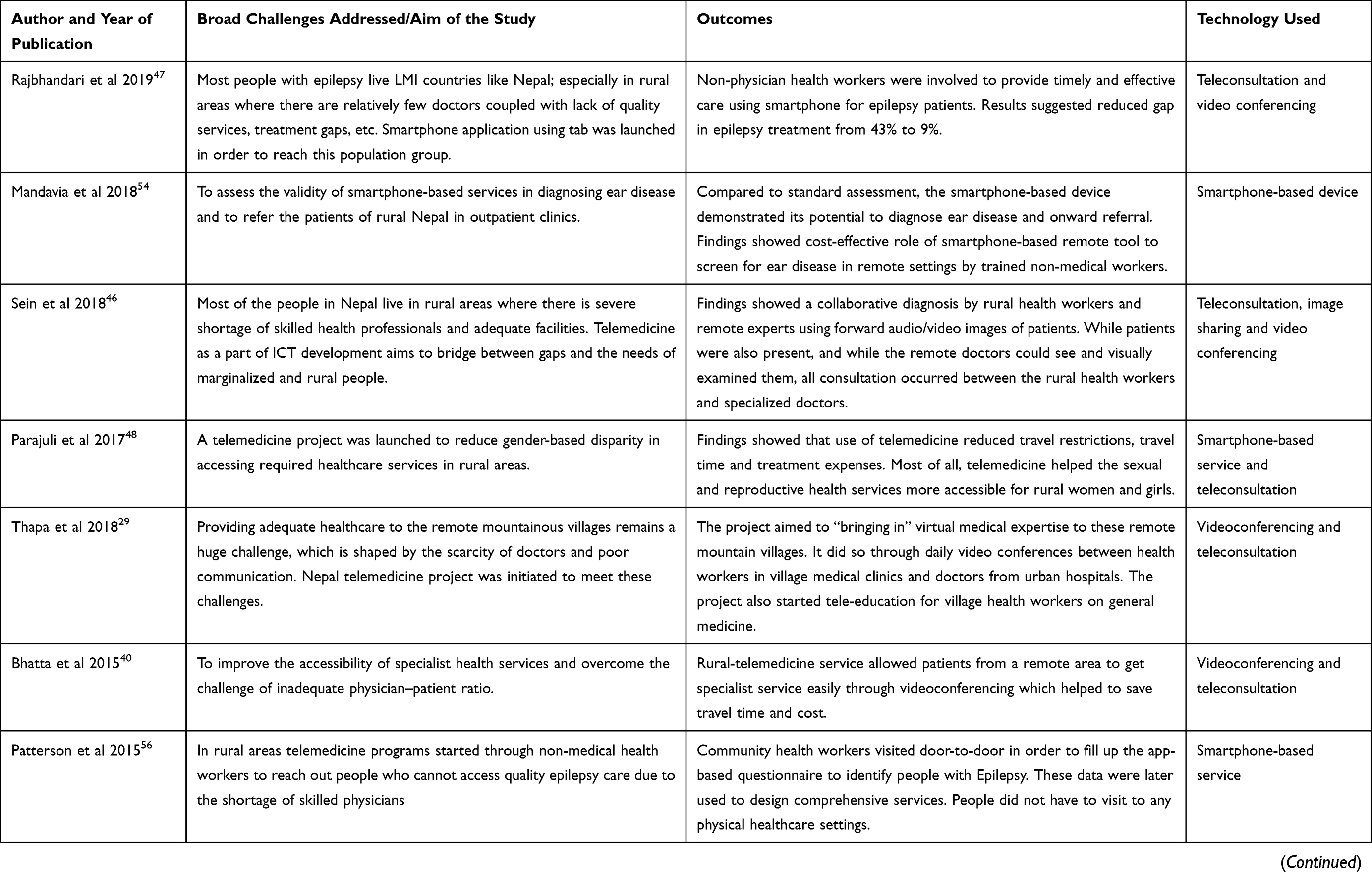
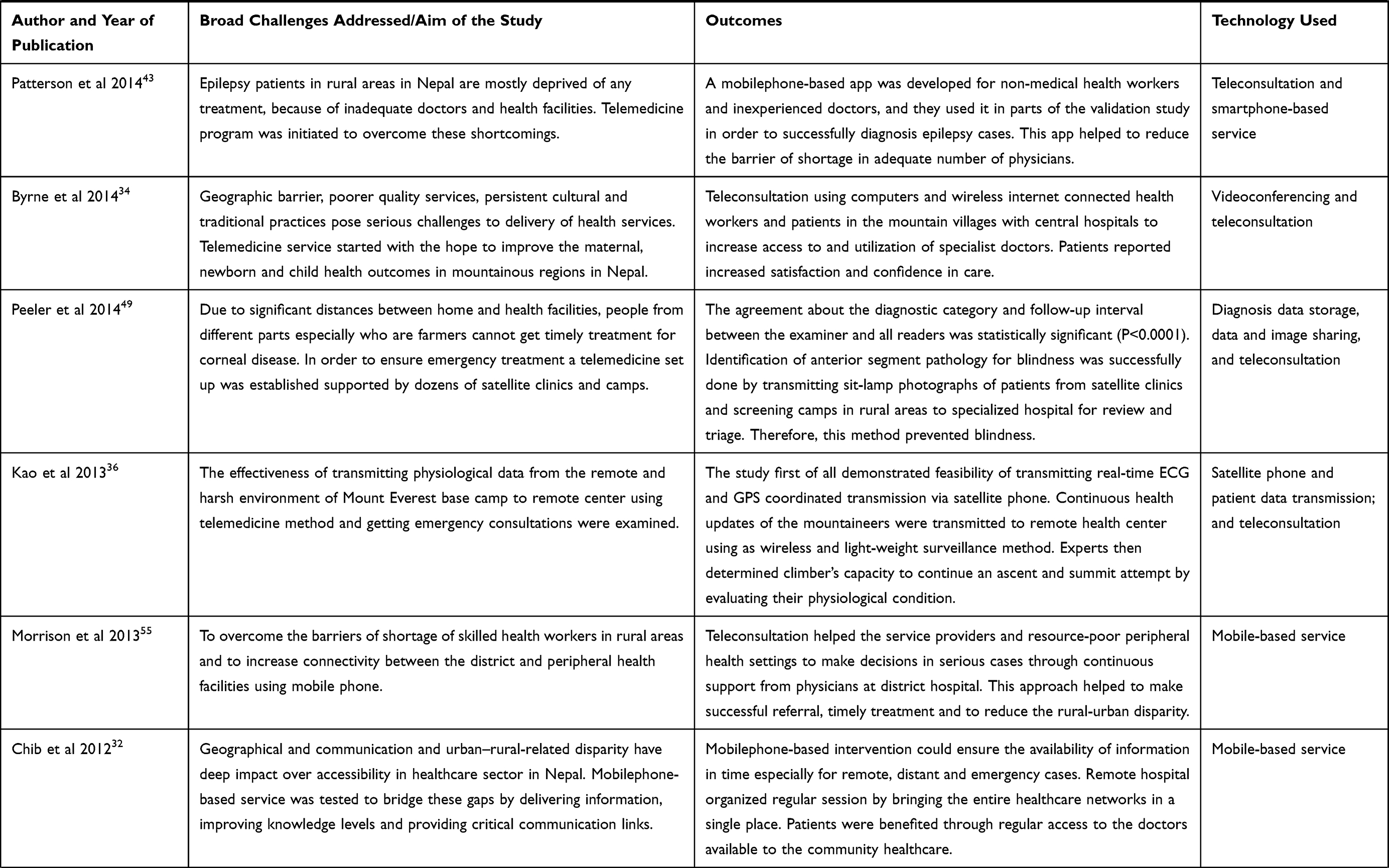
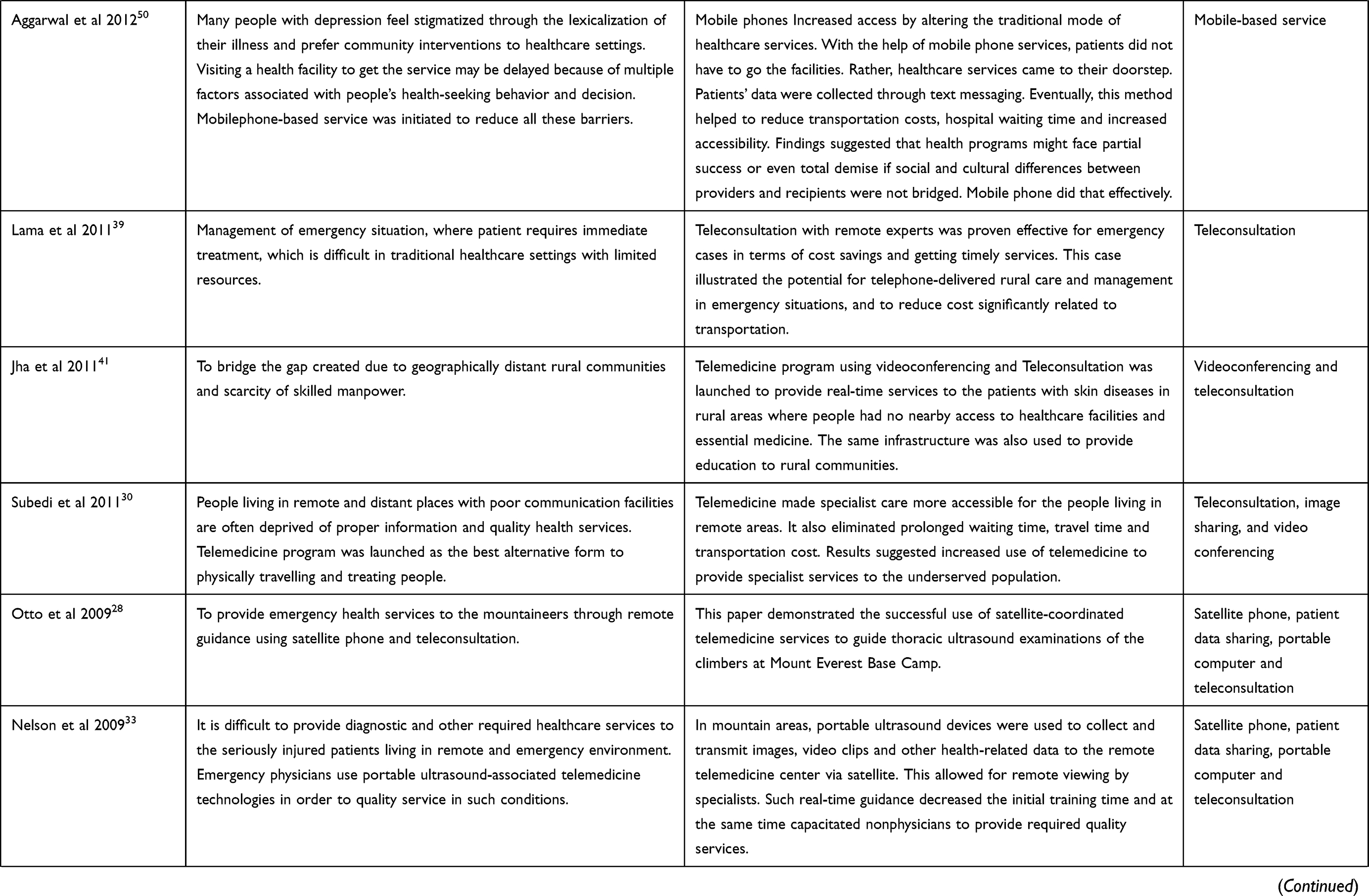
A total of 1161 results were yielded during the initial search. After completing the preliminary screening, 128 results were further assessed and finally 27 papers were included in the review. The detail search strategy and selection process has been shown in Figure 1. Table 1 illustrates the overall summary of the selected papers and observation from the review team. For every paper in the selected sample, we made observation and analysis for challenges addressed in the papers, outcomes and used technology. First two columns are for identification of the selected papers. Third column presents the objectives and broad challenges addressed in the papers. Fourth column lists the outcomes, results and suggestions derived from the papers. The last column lists the tools and technologies discussed in the papers. Studies are listed in order of publication year with the most recent at the top. The reference numbers correspond to those in the references section.
 |
 |  |
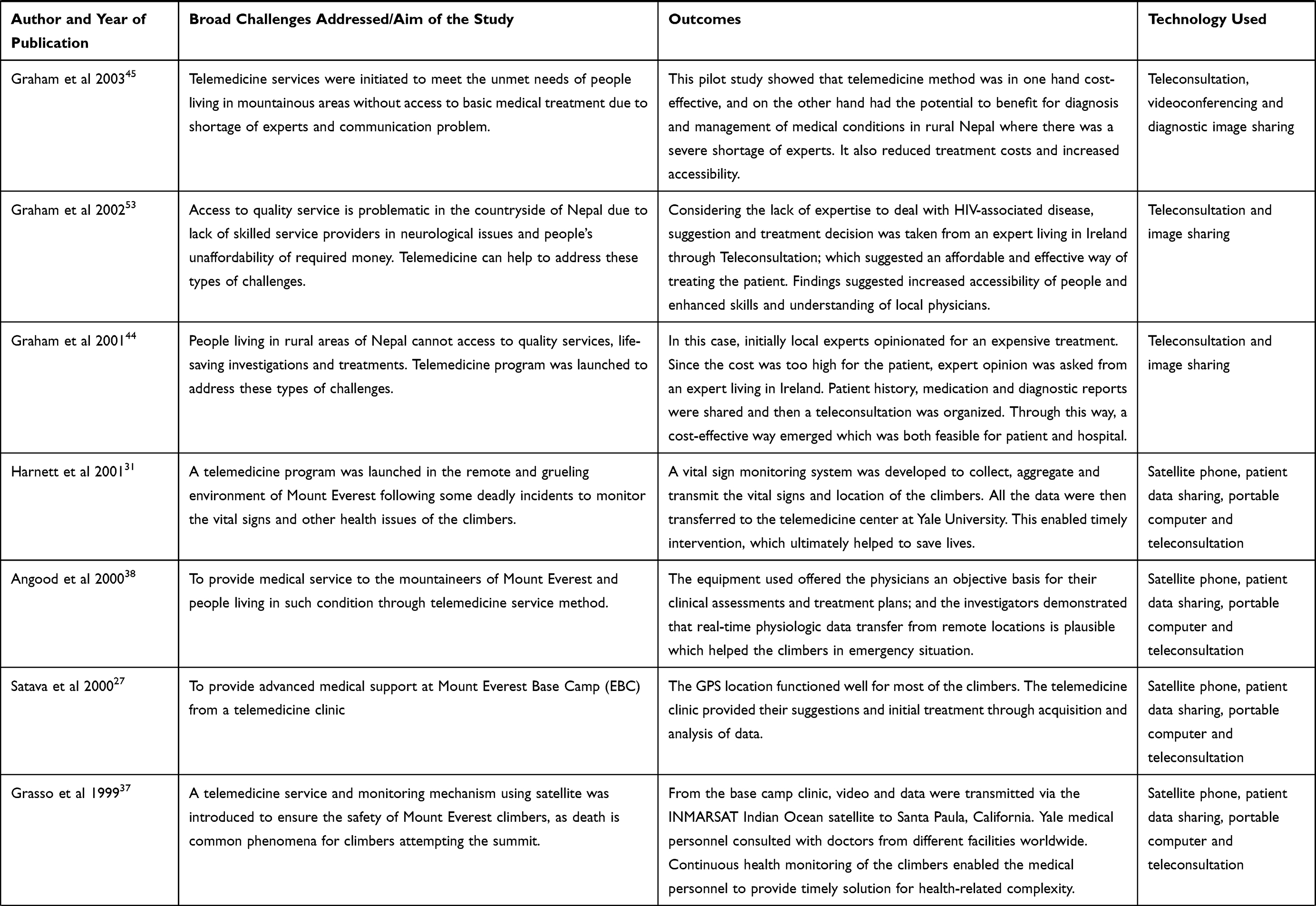 |
Table 1 Summary of Selected Papers |
Narrative synthesis was done to all the evidence relevant for inclusion criteria and the research questions. In total, this synthesis identified 16 factors or characteristics of telemedicine services in Nepal. Factor wise distribution of papers has been outlined in Affinity Matrix (Table 2).
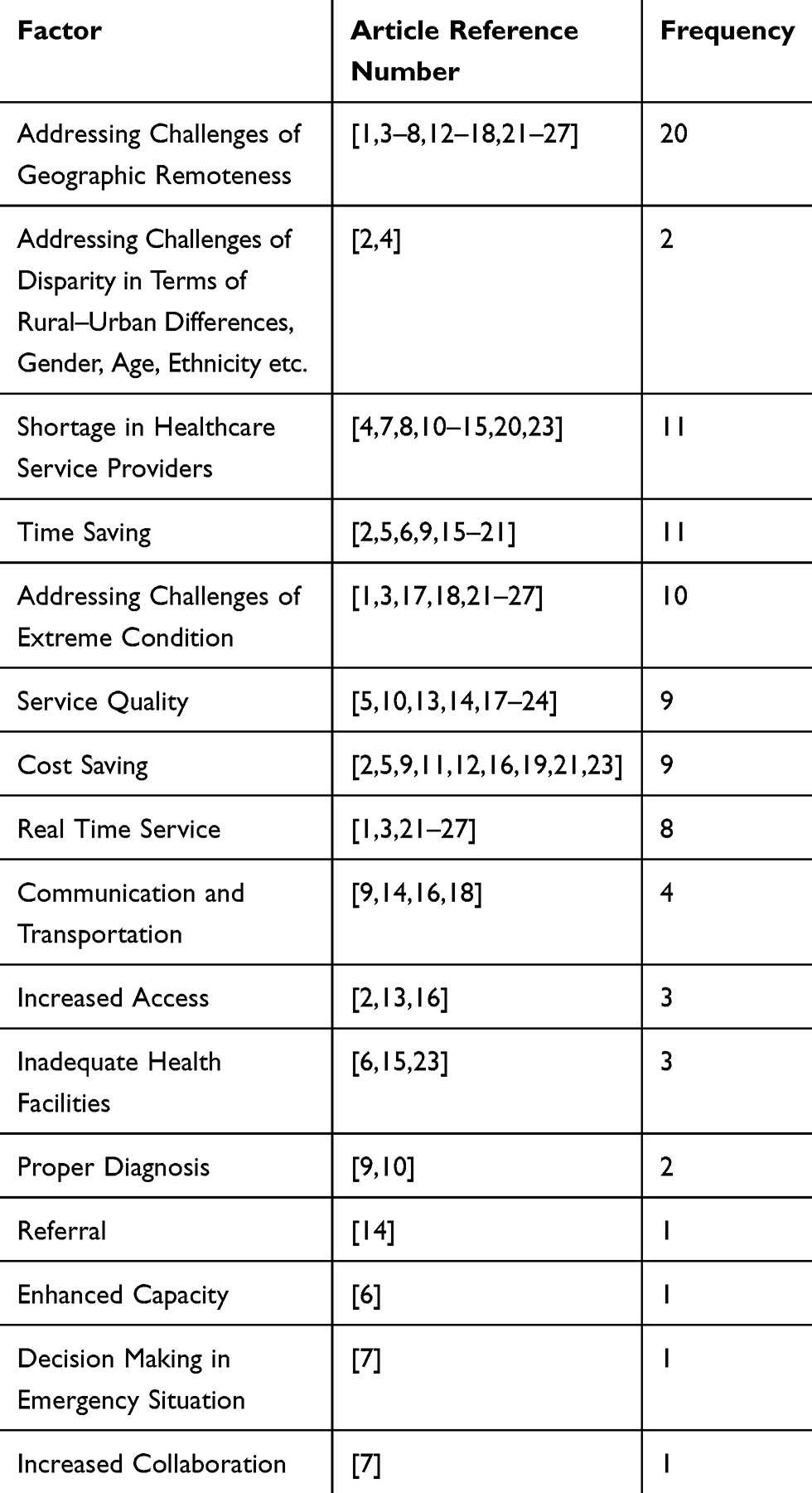 |
Table 2 Affinity Matrix |
This affinity matrix compiles commonalities among different selected papers. It will help the reader to understand the trend and frequency at a glance. The frequency presented in the above table does not necessarily define importance, but many review literatures have used it just to show probability and occurrences in diverse disciplinary areas.22–26
Synthesis of Results
Theme 1: Geographic Difficulties and Emergency Context
A common finding emerging in this review was that telemedicine contributed significantly to overcome geographic hurdles and remoteness. People living in remote areas had less access to healthcare services. Review identified many reasons behind the lack of accessibility, such as poor communication system, land slide or flash flood during rainy season, etc. In total 20 papers reported the telemedicine features of addressing challenges of geographic remoteness27–46 and 11 papers reported time saving29–33,40,41,47–50 character. 4 papers reported communication and transportation30,32,46,49 related issues. Review found significant delays between the injury and medical evaluation due to distance, poor communication and lack of proper information.
Another dominant factor in the healthcare sector of Nepal is that, because of the vast Himalayan peninsula; it is very difficult to provide quality services to people in extreme weather conditions. This includes people coming from all over the world to visit the Himalayan summit. A total of 10 evidences has been reported, addressing the challenges of extreme condition27,28,31–38 8 papers reported providing real-time service.27,28,33–38 People living in extreme environments, especially mountaineers often experience complications in breathing and in their respiratory system. In these circumstances, rapid decision-making is a prerequisite to avoid any unexpected situation. Review reported the feature of telemedicine regarding decision-making during emergency situation36,38,42 in 3 papers.
Theme 2: Accessibility Issue in Terms of Rural–Urban Disparity, Economic Capacity, Age-Gender Difference, Ethnic and Religious Difference
Increasing accessibility in general is one of the key steps in achieving Universal Health Coverage.51 In low and middle-income countries, this accessibility needs to be ensured without causing financial damage.52 Telemedicine services in Nepal also encountered such issues. Review found 9 papers discussing about cost-effectiveness30,33,40,45,48–50,53,54 and 3 papers about increased access.30,44,48 Rural-urban disparity and lack of services in rural areas block the way to increased accessibility. 2 papers reported the issue of addressing challenges of disparity in terms of rural-urban difference in healthcare provision. In addition, 2 papers reported the role of telemedicine in overcoming challenges in terms of gender, age, ethnicity, etc.39,48
Theme 3: Address Shortage of Healthcare Facilities and Skilled Health Service Providers
Quality healthcare service depends largely on the presence of adequate number of healthcare facilities and healthcare service providers respective to the total amount of population. Availability of equipment and logistic facilities are also some of the most important contributing factors. In Nepal, access to quality service is limited due to lack of healthcare facilities in rural areas which is coupled with inadequate health service providers. The current review identified 11 papers reporting the issue of shortage of healthcare service providers.29,39,42–47,53–56 3 papers have highlighted the issue of inadequate health facilities.29,41,54 These three papers discussed one common thing, which was the lack of skilled and specialized healthcare service providers outside of the mega cities of Nepal. They argued that this is one of the key issues behind poor accessibility to quality services.
A vast majority of people living in rural areas cannot visit specialized service centers and therefore cannot access quality health services. Challenges of ensuring quality services in rural areas create an extra burden when Nepal is working hard to reach the coverage of health service and proper diagnosis to all its population with limited resources. This review found 9 papers discussing about service quality31,32,35,40,44,46,47,50,56 and 2 paper discussing about proper diagnosis49,56 as key benefits of using telemedicine.
Few other issues were also highlighted through the review although in a small scale. Referral,46 enhanced capacity,41 and increased collaboration42 had been reported in 1 paper, respectively.
Discussion
Traditional healthcare services require the patient to physically visit healthcare facilities. This process demands a lot of time and high expenses. When it comes to the question of Low and Middle Income Countries (LMICs) like Nepal, the situation is worsened with resource-poor status and inadequate facilities. On the contrary, most of the people, especially poor, marginalized and rural population are primarily dependent on government health facilities. Unfortunately, the government of Nepal is struggling to meet all the existing demand with limited resources and budget. One study found the allocated budget was very limited considering the needs.57
Considering the limitations of health systems in (LMICs) to provide quality, affordable and timely services; policy-makers, donors and other interested parties were searching for an effective and feasible option. This concern and endeavor have resulted in the potential of telemedicine and other ICT-based healthcare services. This innovation is coupled with unprecedented increase of low-cost cell phones and internet.19 Application of telemedicine helps to extend geographic access to health care, which is particularly promising given the poor distribution of healthcare service providers and inadequate equipment in many (LMICs).58
The features of using telemedicine identified through this narrative synthesis are consistent with the findings and arguments of research conducted in (LMICs) contexts. Glinkowski and Ciszek (2007), Kifle et al (2010), Combi et al (2016), Kruse et al (2017) and Kvedar et al (2006) have stressed the value and importance of telemedicine in resource-limited country settings to overcome geographic and resource barriers.22,59–62 Alghamdi et al (2015) and Bali & Singh (2007) argued that mobile-based health services have the potential to improve the overall quality of healthcare delivery in developing countries because of certain features like building awareness among patients, disease self-management, decrease in healthcare costs, remote monitoring of patients, etc.63,64
This review has also identified the comprehensive use of telemedicine in Himalayan extreme condition among mountaineers and other local mountain dwellers. Telemedicine has also shown its effectiveness on healthcare delivery in extreme conditions.65 Otto (1999) discussed two telemedicine projects initiated in places with extreme weather in order to highlight the feasibility of telemedicine in similar environments.66 Latifi et al in their study showed the use of telemedicine among swimmers in the Atlantic Ocean.67
Health sector of developing countries is confined with numerous problems like acute shortage of healthcare professionals (e.g. physicians, nurses, pharmacists, public health workers) and inadequate healthcare facilities. Researchers around the world have identified the effective contribution of telemedicine to overcome these challenges. Edworthy (2001) showed the potential of telemedicine to link health professionals irrespective of where they were.68 Other scholars have also demonstrated the role of telemedicine to overcome the challenges related to shortage of healthcare professionals and healthcare centers.69 Thus, it enhances the scope of collaboration and enables specialists supporting the remote and isolated communities. A study by Kim et al (2014) found positive impacts in delivery patterns in non-NICU hospitals using telemedicine services.70 Ganesan et al presented a classic example of collaboration using ICTs in health sector to increase physical activity resulting in increased outcome. Academic researchers teamed up with the private sector professionals to implement and monitor the 100-day Stepathlon programme among 70,000 participants where most of the participants were from developing countries.71 Telemedicine also strengthens primary healthcare by developing the capacity of healthcare professionals living and working in rural and hard to reach areas. Application of mobile phone improves the capacity of the patients by enhancing the scope of self-management.72 At the same time, it increases the capacity of rural health professionals to be more responsive and to provide instant, timely services.72
Wang et al described telemedicine from the perspective of reduced cost and timely diagnosis.73 They argued in Chinese context that telemedicine connects specialists with healthcare facilities. Their study showed the net saving of some USD 2.3 million for patients USD 3.7 million for specialists, because patients received proper diagnosis services without moving to specialist’s health facilities and also specialists did not have to physically visit rural areas for providing services to them. A comprehensive review on telemedicine protects in emerging and developing country context by Combi et al found remote diagnosis, remote intervention, remote monitoring and remote education as some of the primary objectives of designing and implementing telemedicine services.61 The review included China, India, Sub-Saharan Africa, Amazonia, Egypt and Pacific Island.
Low cost of ICTs and its use in health sector have the potential to improve health outcomes. Hamine et al studied usability, feasibility, and acceptability of mobile-based intervention in healthcare. They found significant improvements in disease-specific clinical outcomes.74 Several other studies have also found positive outcomes of using telemedicine in the health sector. Angus et al (200) and Vespa (2005) in critical care; Lai (2009) and Silva et al (2013) in stroke treatment; and Boniface et al (2011) in diagnosis tests have found significant improvement of the robotic telepresence.75–79
Treatment, diagnosis and timely services have been coupled by remote monitoring, rapid decision-making, etc.; which has improved patient outcomes. Application of telemedicine in ICU is widely recognized in improving treatment outcomes.80–82
Conclusion
The reviewed papers demonstrated that telemedicine was designed and implemented in order to overcome the major challenges of health sector in resource-limited countries like Nepal had been suffering from. In most of the cases, geographical location, shortage of equipment and health facilities, poor communication system, income level and inadequate skilled workforce work as primary determinants of people’s access to quality health care in Nepal. Therefore, telemedicine certainly highlights its potential for large-scale use in order to triumph over these challenges. Overall, telemedicine has made great advancement from both research and institutional point of view. In order to gain more benefits from telemedicine services, we need to find the loopholes and to utilize the technologies according to it. Therefore, proper trial on telemedicine is suggested to measure the real impact and to scaling up. According to a different and broader point of view, telemedicine is still not an integral part of the health systems in low- and middle-income countries. The overall health systems will start getting gross benefits when telemedicine will become an integral part of health service delivery, not as a standalone approach. To reach that goal, more research is required to understand the sustainability status of already implemented programs, its cost-effectiveness, regulatory mechanism and so on. No well-established business model of telemedicine is visible in developing countries, which leads to unsustainability. In order to properly design and estimate the overall mechanism including human resource, equipment and costs, it is essential to undertake a comprehensive research from the perspectives of economy, policies and contextual needs.
Acknowledgments
The authors thank Dr. Meghnath Dhimal for his contribution in the conceptualization phase and reviewing the manuscript, and Shafina Shafiq for her assistance with the literature search and initial screening.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zere E, Suehiro Y, Arifeen A, Moonesinghe L, Chanda SK, Kirigia JM. Equity in reproductive and maternal health services in Bangladesh. Int J Equity Heal. 2013;12:90.
2. Peters DH, Garg A, Bloom G, Walker DG, Brieger WR, Rahman MH. Poverty and access to health care in developing countries. Ann N Y Acad Sci. 2008;1136:161–171. doi:10.1196/nyas.2008.1136.issue-1
3. O’Donnell O. Access to health care in developing countries: breaking down demand side barriers. Cad Saude Publica. 2007;23:2820–2834. doi:10.1590/S0102-311X2007001200003
4. Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19:127–140. doi:10.1097/00005650-198102000-00001
5. World Health Organization. Telemedicine: opportunities and developments in member states: report on the second global survey on EHealth; 2009. Available from: https://www.who.int/goe/publications/goe_telemedicine_2010.pdf.
6. Coiera E. Essentials of telemedicine and telecare. BMJ Br Med J. 2002;324:1104. doi:10.1136/bmj.324.7345.1104
7. Government of Nepal. Nepal Human Development Report 2014: Beyond Geography, Unlocking Human Potential. Kathmandu: National Planning Commission, Government of Nepal and United Nations Development Programme; 2014.
8. Government of Nepal. Nepal health sector strategy 2015–2020. Population M of H and, ed; 2015.
9. Laxminarayan S, Istepanian RS. UNWIRED E-MED: the next generation of wireless and internet telemedicine systems. IEEE Trans Inf Technol Biomed. 2000;4(3):189–193. doi:10.1109/TITB.2000.5956074
10. Scalvini S, Vitacca M, Paletta L, Giordano A, Balbi B. Telemedicine: a new frontier for effective healthcare services. Monaldi Arch Chest Dis. 2004;61:226–233. doi:10.4081/monaldi.2004.686
11. Patterson V, Hoque F, Vassallo D, Farquharson Roberts M, Swinfen P, Swinfen R. Store-and-forward teleneurology in developing countries. J Telemed Telecare. 2001;7 Suppl 1:52–53. doi:10.1177/1357633X010070S121
12. Wootton R. Telemedicine and isolated communities: a UK perspective. J Telemed Telecare. 1999;5 Suppl 2:S27–S34. doi:10.1258/1357633991933495
13. Strehle EM, Shabde N. One hundred years of telemedicine: does this new technology have a place in paediatrics? Arch Dis Child. 2006;91(12):956–959. doi:10.1136/adc.2006.099622
14. World Health Organization. A health telematics policy in support of WHO’s HEALTH-FOR-ALL STRATEGY FOR GLOBAL HEALTH DEVELOPMENT; 1998. Available from: https://apps.who.int/iris/bitstream/handle/10665/63857/WHO_DGO_98.1.pdf?sequence=1&isAllowed=y.
15. Popay J, Roberts H, Sowden A. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. Economic and Social Research Council. Vol. 15. 2006. http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.178.3100&rep=rep1&type=pdf
16. Islam MM, Topp L, Day CA, Dawson A, Conigrave KM. The accessibility, acceptability, health impact and cost implications of primary healthcare outlets that target injecting drug users: a narrative synthesis of literature. Int J Drug Policy. 2012;23(2):94–102. doi:10.1016/j.drugpo.2011.08.005
17. Jeon Y-H, Glasgow NJ, Merlyn T, Sansoni E. Policy options to improve leadership of middle managers in the Australian residential aged care setting: a narrative synthesis. BMC Health Serv Res. 2010;10:190. doi:10.1186/1472-6963-10-190
18. World Health Organization. Telemedicine: health and sustainable development. Available from: https://www.who.int/sustainable-development/health-sector/strategies/telehealth/en/.
19. World Health Organization. MHealth: new horizons for health through mobile technologies: second global survey on EHealth. Switzerland; 2011. Available from: https://www.who.int/goe/publications/goe_mhealth_web.pdf.
20. Eysenbach G. What is e-health? J Med Internet Res. 2001;3(2):E20. doi:10.2196/jmir.3.2.e20
21. World Health Organization. Accessibility: gender, equity and human rights. Available from: https://www.who.int/gender-equity-rights/understanding/accessibility-definition/en/.
22. Kruse CS, Krowski N, Rodriguez B, Tran L, Vela J, Brooks M. Telehealth and patient satisfaction: a systematic review and narrative analysis. BMJ Open. 2017;7(8):e016242. doi:10.1136/bmjopen-2017-016242
23. Kruse CS, Kothman K, Anerobi K, Abanaka L. Adoption factors of the electronic health record: a systematic review. JMIR Med Inform. 2016;4(2):e19. doi:10.2196/medinform.5525
24. Kruse CS, Mileski M, Alaytsev V, Carol E, Williams A. Adoption factors associated with electronic health record among long-term care facilities: a systematic review. BMJ Open. 2015;5(1). doi:10.1136/bmjopen-2014-006615.
25. Zhang Y-F, Xu C, Lu H, Huang Y-M. Character identification in feature-length films using global face-name matching. IEEE Trans Multimed. 2009;11(7):1276–1288. doi:10.1109/TMM.2009.2030629
26. Sang J, Liang C, Xu C, Cheng J Robust movie character identification and the sensitivity analysis. In:
27. Satava R, Angood PB, Harnett B, Macedonia C, Merrell R. The physiologic cipher at altitude: telemedicine and real-time monitoring of climbers on Mount Everest. Telemed J E Heal. 2000;6:303–313. doi:10.1089/153056200750040165
28. Otto C, Hamilton DR, Levine BD, et al. Into thin air: extreme ultrasound on Mt Everest. Wilderness Env Med. 2009;20:283–289. doi:10.1580/08-WEME-BR-228R2.1
29. Thapa D, Sein MK. Trajectory of affordances: insights from a case of telemedicine in Nepal. Inf Syst J. 2018;28:796–817. doi:10.1111/isj.12160
30. Subedi R, Peterson C, Kyriazakos S Telemedicine for rural and underserved communities of Nepal. In:
31. Harnett BM, Satava R, Angood P, Merriam NR, Doarn CR, Merrell RC. The benefits of integrating internet technology with standard communications for telemedicine in extreme environments. Aviat Sp Env Med. 2001;72:1132–1137.
32. Chib A, Law FB, Ahmad MN, Ismail NB. Moving mountains with mobiles: spatiotemporal perspectives on mHealth in Nepal. J Media Commun Res. 2012;28.
33. Nelson BP, Melnick ER, Li J. Portable ultrasound for remote environments, part I: feasibility of field deployment. J Emerg Med. 2011;40:190–197. doi:10.1016/j.jemermed.2009.09.006
34. Byrne A, Hodge A, Jimenez-Soto E, Morgan A. What works? Strategies to increase reproductive, maternal and child health in difficult to access mountainous locations: a systematic literature review. PLoS One. 2014;9:e87683. doi:10.1371/journal.pone.0087683
35. White AP, Angood P. Advancing technologies in clinical medicine: the Yale-Mount Everest telemedicine project. Yale J Biol Med. 1999;72:19–27.
36. Kao WF, Huang JH, Kuo TB, et al. Real-time electrocardiogram transmission from Mount Everest during continued ascent. PLoS One. 2013;8:e66579. doi:10.1371/journal.pone.0066579
37. Grasso V. What works. Web-enabled Telemedicine project developed to monitor the health of Mt. Everest climbers. Heal Manag Technol. 1999;20:18.
38. Angood PB, Satava R, Doarn C, Merrell R. Telemedicine at the top of the world: the 1998 and 1999 Everest extreme expeditions. Telemed J E Heal. 2000;6:315–325. doi:10.1089/153056200750040174
39. Lama T, Karmacharya B, Chandler C, Patterson V. Telephone management of severe wasp stings in rural Nepal: a case report. J Telemed Telecare. 2011;17:105–108. doi:10.1258/jtt.2010.100606
40. Bhatta R, Aryal K, Opportunities EG. Challenges of a rural-telemedicine program in Nepal. J Nepal Health Res Counc. 2015;13(30):149–153.
41. Jha AK, Gurung D. Reaching the unreached: a model for sustainable community development through information and communication technology. JNMA J Nepal Med Assoc. 2011;51:213–214.
42. Joanna M, Naba S, Bruce H, Mark Z. Mobile phone support for rural health workers in Nepal through ‘Celemedicine’. J Nepal Med Assoc. 2013;52(191):538–542.
43. Patterson V. Telemedicine for epilepsy support in resource-poor settings. Front Public Heal. 2014;2(120):1–4.
44. Graham LE, Flynn P, Cooke S, Patterson V. The interdisciplinary management of cerebral haemorrhage using telemedicine – a case report from Nepal. J Telemed Telecare. 2001;7:304–306. doi:10.1258/1357633011936570
45. Graham LE, Zimmerman M, Vassallo DJ, et al. Telemedicine – the way ahead for medicine in the developing world. Trop Doct. 2003;33:36–38. doi:10.1177/004947550303300118
46. Sein MK, Thapa D. Social capital in enabling quality health care: the case of a telemedicine project in Nepal. Electron J Inf Syst Dev Ctries. 2018;84:e12046.
47. Rajbhandari H, Joshi S, Malakar S, et al. Epilepsy field workers, a smartphone application and telephone telemedicine: safe and effective epilepsy care in rural Nepal. Seizure. 2019;64:54–58. doi:10.1016/j.seizure.2018.12.005
48. Parajuli R, Doneys P. Exploring the role of telemedicine in improving access to healthcare services by women and girls in rural Nepal. Telemat Informatics. 2017;34:1166–1176. doi:10.1016/j.tele.2017.05.006
49. Peeler CE, Dhakhwa K, Mian SI, et al. Telemedicine for corneal disease in rural Nepal. J Telemed Telecare. 2014;20:263–266. doi:10.1177/1357633X14537769
50. Aggarwal NK. Applying mobile technologies to mental health service delivery in South Asia. Asian J Psychiatr. 2012;5(3):225–230. doi:10.1016/j.ajp.2011.12.009
51. Evans DB, Hsu J, Ties B. Universal health coverage and universal access. Bull World Health Organ. 2013;91:546–546A. doi:10.2471/BLT.13.125450
52. Marziale MHP. Universal access to health and universal health coverage: nursing contributions. Rev Lat Am Enfermagem. 2016;24:e2667–e2667. doi:10.1590/1518-8345.0000.2667
53. Graham LE, Flynn P, Patterson V. Teleneuroradiology: a case from Nepal with clinical and educational benefit. J Telemed Telecare. 2002;8:356–358. doi:10.1258/135763302320939257
54. Mandavia R, Lapa T, Smith M, Bhutta MF. A cross-sectional evaluation of the validity of a smartphone otoscopy device in screening for ear disease in Nepal. Clin Otolaryngol. 2018;43:31–38. doi:10.1111/coa.2018.43.issue-1
55. Morrison J, Shrestha NR, Hayes B, Zimmerman M. Mobile phone support for rural health workers in Nepal through “celemedicine.”. JNMA J Nepal Med Assoc. 2013;52:538–542.
56. Patterson V, Singh M, Rajbhandari H, Vishnubhatla S. Validation of a phone app for epilepsy diagnosis in India and Nepal. Seizure. 2015;30:46–49. doi:10.1016/j.seizure.2015.05.011
57. Dulal RK, Magar A, Karki SD, Khatiwada D, Hamal PK. Analysis of health sector budget of Nepal. JNMA J Nepal Med Assoc. 2014;52(194):811–821. doi:10.31729/jnma.2757
58. World Health Orginasition. The World Health Report 2006: Working Together for Health. World Health Organization; 2006.
59. Glinkowski W, Ciszek B. WWW-based e-teaching of normal anatomy as an introduction to telemedicine and e-health. Telemed J E Health. 2007;13(5):535–544. doi:10.1089/tmj.2006.0077
60. Kifle M, Payton FC, Mbarika V, Meso P. Transfer and adoption of advanced information technology solutions in resource-poor environments: the case of telemedicine systems adoption in Ethiopia. Telemed J E Health. 2010;16(3):327–343. doi:10.1089/tmj.2009.0008
61. Combi C, Pozzani G, Pozzi G. Telemedicine for developing countries. A survey and some design issues. Appl Clin Inform. 2016;7(4):1025–1050. doi:10.4338/ACI-2016-06-R-0089
62. Kvedar J, Heinzelmann PJ, Jacques G. Cancer diagnosis and telemedicine: a case study from Cambodia. Ann Oncol off J Eur Soc Med Oncol. 2006;17 Suppl 8:viii37–viii42. doi:10.1093/annonc/mdl986
63. Alghamdi M, Gashgari H, Househ M. A systematic review of mobile health technology use in developing countries. Stud Health Technol Inform. 2015;213:223–226.
64. Bali S, Singh AJ. Mobile phone consultation for community health care in rural north India. J Telemed Telecare. 2007;13(8):421–424. doi:10.1258/135763307783064421
65. Anogianakis G, Maglavera S, Pomportsis A. Relief for maritime medical emergencies through telematics. IEEE Trans Inf Technol Biomed. 1998;2(4):254–260. doi:10.1109/4233.737580
66. Otto CA Telemedicine in the Canadian High Arctic and other remote environments. In:
67. Latifi R, Stanonik MD, Merrell RC, Weinstein RS. Telemedicine in extreme conditions: supporting the Martin Strel Amazon Swim Expedition. Telemed J E Health. 2009;15(1):93–100. doi:10.1089/tmj.2008.0057
68. Edworthy SM. Telemedicine in developing countries. BMJ. 2001;323(7312):524–525. doi:10.1136/bmj.323.7312.524
69. Rimsza M, Hotaling AJ, Keown ME, et al. The Use of Telemedicine to Address Access and Physician Workforce Shortages. Pediatrics. 2015;136:202–209.
70. Kim EW, Teague-Ross TJ, Greenfield WW, Keith Williams D, Kuo D, Hall RW. Telemedicine collaboration improves perinatal regionalization and lowers statewide infant mortality. J Perinatol off J Calif Perinat Assoc. 2013;33(9):725–730.
71. Ganesan AN, Louise J, Horsfall M, et al. International mobile-health intervention on physical activity, sitting, and weight: the stepathlon cardiovascular health study. J Am Coll Cardiol. 2016;67(21):2453–2463. doi:10.1016/j.jacc.2016.03.472
72. Kvedar JC, Nesbitt T, Kvedar JG, Darkins A. E-patient connectivity and the near term future. J Gen Intern Med. 2011;26 Suppl 2:636–638. doi:10.1007/s11606-011-1763-0
73. Wang -T-T, Li J-M, Zhu C-R, et al. Assessment of utilization and cost-effectiveness of telemedicine program in western regions of China: a 12-year study of 249 hospitals across 112 cities. Telemed J E Health. 2016;22(11):909–920. doi:10.1089/tmj.2015.0213
74. Hamine S, Gerth-Guyette E, Faulx D, Green BB, Ginsburg AS. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J Med Internet Res. 2015;17(2):e52. doi:10.2196/jmir.3951
75. Vespa PM. Multimodality monitoring and telemonitoring in neurocritical care: from microdialysis to robotic telepresence. Curr Opin Crit Care. 2005;11(2):133–138. doi:10.1097/01.ccx.0000155353.01489.58
76. Angus DC, Kelley MA, Schmitz RJ, White A, Popovich JJ. Caring for the critically ill patient. Current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284(21):2762–2770. doi:10.1001/jama.284.21.2762
77. Lai F. Stroke networks based on robotic telepresence. J Telemed Telecare. 2009;15(3):135–136. doi:10.1258/jtt.2009.003009
78. Silva GS, Farrell S, Shandra E, Viswanathan A, Schwamm LH. The status of telestroke in the United States: a survey of currently active stroke telemedicine programs. Stroke. 2012;43(8):2078–2085. doi:10.1161/STROKEAHA.111.645861
79. Boniface KS, Shokoohi H, Smith ER, Scantlebury K. Tele-ultrasound and paramedics: real-time remote physician guidance of the Focused Assessment With Sonography for Trauma examination. Am J Emerg Med. 2011;29(5):477–481. doi:10.1016/j.ajem.2009.12.001
80. Howell G, Ardilles T, Bonham AJ. Implementation of a remote intensive care unit monitoring system correlates with improvements in patient outcomes. Chest. 2008;134(4):58S. doi:10.1378/chest.134.4_MeetingAbstracts.s58003
81. Lilly CM, Cody S, Zhao H, et al. Hospital mortality, length of stay, and preventable complications among critically ill patients before and after tele-ICU reengineering of critical care processes. JAMA. 2011;305(21):2175–2183. doi:10.1001/jama.2011.697
82. Willmitch B, Golembeski S, Kim SS, Nelson LD, Gidel L. Clinical outcomes after telemedicine intensive care unit implementation. Crit Care Med. 2012;40(2):450–454. doi:10.1097/CCM.0b013e318232d694
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.