")
Back to Journals » Advances in Medical Education and Practice » Volume 10
Teaching methods used by internal medicine residents on rounds: what works?
Authors Kulkarni VT, Salgado SM, Pelletier SR, Shields HM
Received 22 August 2018
Accepted for publication 23 December 2018
Published 21 January 2019 Volume 2019:10 Pages 15—21
DOI https://doi.org/10.2147/AMEP.S181153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Vivek T Kulkarni,1 Sanjay M Salgado,2,3 Stephen R Pelletier,4 Helen M Shields3,5,6
1Division of Cardiovascular Medicine, Department of Medicine, Hospital of the University of Pennsylvania, Philadelphia, PA, USA; 2Hospitalist Service, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 3Harvard Medical School, Boston, MA, USA; 4Office of Educational Quality Improvement, Harvard Medical School, Boston, MA, USA; 5Division of Medical Communications, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 6Division of Gastroenterology, Hepatology, and Endoscopy, Department of Medicine, Brigham and Women’s Hospital, Boston, MA, USA
Background: The specific teaching methods used by internal medicine residents on walk rounds are unknown.
Objectives: 1) To characterize in real time the specific teaching methods used by internal medicine residents on rounds and 2) to identify attributes of successful resident teaching on rounds.
Materials and methods: We conducted a prospective mixed-methods study on inpatient medical services at a single academic medical center from September 2016 to January 2017. Participants were internal medicine residents (postgraduate year [PGY]-1, PGY-2, and PGY-3) and attending physicians. Teachers were PGY-2 and PGY-3 residents, and learners were PGY-1 residents. Residents’ teaching on rounds was observed and characterized according to resident demographics, specific teaching methods, and length of time. Participants completed a survey with Likert scale and free-text questions.
Results and conclusion: Among 136 surveys across 28 separate teaching encounters, we noted that PGY-3 residents’ teaching was rated significantly better than PGY-2 residents’ teaching. Teaching lasting >1 minute was rated significantly better than teaching lasting
Keywords: internal medicine, resident teaching, mixed methods, direct observation
Introduction
Internal medicine (IM) residents are expected to teach. The Accreditation Council for Graduate Medical Education’s Program Requirements for Graduate Medical Education in Internal Medicine state that “Residents are expected to demonstrate the ability to manage patients in a variety of roles within a health system […including] as a teacher to […] other physicians.”1
In particular, inpatient walk rounds (“rounds” for short) form the core of teaching for IM residents. On inpatient medical services, rounds consist of a team of physicians (usually one attending physician and several residents) seeing and discussing the care of each patient on their service. Because rounds are primarily focused on the practical content of creating plans of care, teaching on rounds is often ad hoc, with topics varying each day based on the specific patients admitted. Furthermore, because of its variable and unpredictable nature, the specific content of teaching on rounds is usually not included in the curriculum design for residency programs.
Residents, not just attending physicians, usually play an important teaching role on rounds. Yet, to our knowledge, no prior studies have focused exactly on how residents teach on rounds. This absence of data is striking given the abundance of recent work focusing on resident-as-teacher programs2 and various studies addressing how attending physicians should teach during rounds.3–6 In fact, we might expect that successful teaching by residents differs from successful teaching by attending physicians because residents are “near-peer” educators who spend the majority of the working day (not just rounds) with their learners.
Prior studies of feedback on resident teaching suggest that residents are receptive to targeted information that might improve their teaching;7,8 but to our knowledge, no studies have addressed which resident teaching methods are considered the most effective and helpful by other team members. Our aims were to observe and characterize resident teaching methods on rounds and capture team members’ perceptions of teaching in real time.
Materials and methods
Study design
This was a prospective, single-center, mixed-methods study conducted on inpatient medical services at Brigham and Women’s Hospital (BWH; Boston, MA, USA) from September 2016 through January 2017. The Partners Healthcare Institutional Review Board concluded that this study met the criteria for exemption because this research was conducted in established or commonly accepted educational settings involving normal educational practices.
Data acquisition
At BWH, IM resident schedules for the year are divided into 2-week blocks. At the beginning of each block, all residents (postgraduate year [PGY]-1, PGY-2, and PGY-3) and attending physicians on inpatient medical services were eligible for enrollment. A nonrandom convenience sample of teams on inpatient medical services was chosen, including general medical and subspecialty services. Each team consisted of one or two teaching residents (PGY-2 or PGY-3), two to four learning residents (PGY-1), and one or two attending physicians. All potential participants who provided verbal informed consent were enrolled. PGY-2 and PGY-3 residents were given a demographic survey asking questions about their age, gender, PGY number, and other advanced degrees.
Residents were notified in person at the beginning of each 2-week schedule block that they would be observed for 90 minutes each day on rounds for the remainder of the block. During the block, one study investigator (VTK) accompanied the team on rounds in order to observe and characterize resident teaching in real time. Discrete periods of resident teaching were identified and defined as “teaching encounters”. Teaching encounters were identified when the resident indicated verbally the intention to teach about a specific topic (eg, “Now let’s talk about volume overload”). Multiple teaching encounters occurring in the same observation were counted separately, provided that they were not contiguous in time and that their topics were distinct.
Each teaching encounter was characterized (VTK) for specific teaching methods using an observer checklist (Figure 1). This checklist was designed (VTK, SRP, and HMS) beforehand to be unambiguous and easily completed. The checklist contained readily verifiable yes-or-no questions and a measure of time. After a meeting to establish consensus, an initial draft was piloted, and then one iterative amendment was made based on the first several observations. Although many questionnaires have been developed previously to assess clinical teaching,9 to our knowledge, none have focused primarily on the specific methods that residents use to teach. Two study investigators (VTK and HMS) simultaneously observed two teaching encounters and independently completed checklists in order to ensure content validity before the actual research study began; these initial observations were included in the final analyses. All subsequent observations were conducted by one study investigator (VTK).
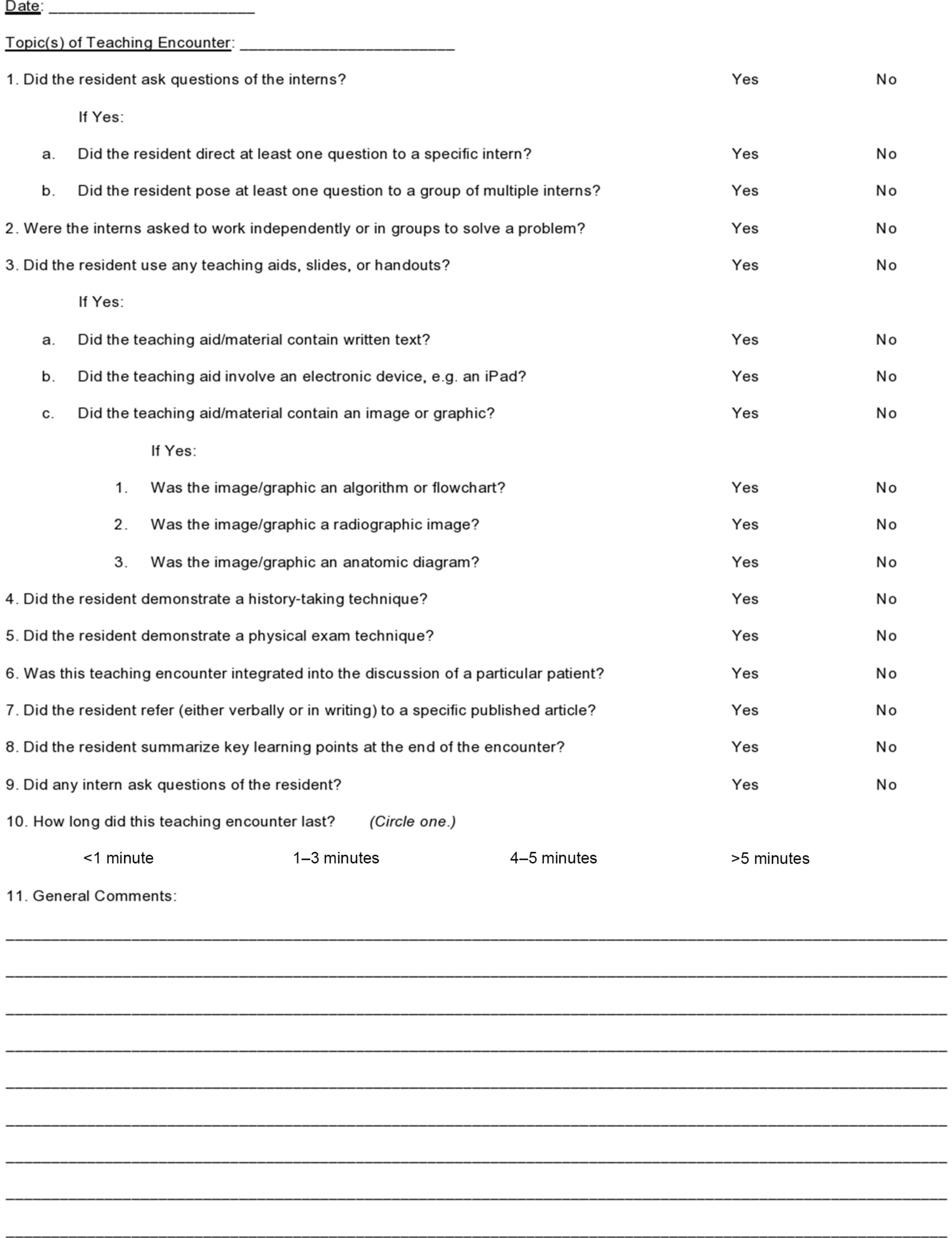 | Figure 1 Observer checklist. |
After each teaching encounter, each team member (PGY-1 residents, PGY-2 and/or PGY-3 residents, and attending physicians) filled out a short survey answering four questions. Surveys were provided as physical pieces of paper to all team members immediately after each teaching encounter and were collected immediately upon completion (<30 seconds after administration). We administered surveys to all the team members (including the attending and the teaching resident) instead of just surveying the learners, in order to get a broader perspective on the perception of resident teaching. The first two questions were on a 5-point Likert scale: Question 1, “Overall, how would you rate this teaching encounter?” (1=“Excellent” and 5=“Poor”) and Question 2, “How helpful was this teaching encounter in covering the topic(s) presented?” (1=“Extremely helpful” and 5=“Not Helpful”). The second two questions were free-text responses: Question 3, “What did you like best about this teaching encounter?” and Question 4, “How would you improve this teaching encounter?” Surveys were collected anonymously and delivered to the statistician (SRP).
Analyses
The study was designed in consultation with the study statistician (SRP), who provided input on the observation checklist, surveys, and analytic plan. For the quantitative analysis, teaching encounters were the unit of analysis. Independent variables were resident demographic data, time during the academic year (before October 15, 2016 vs after), length of time (<1 minute vs 1 minute or longer), and teaching methods used. Dependent variables were the mean values of answers to Question 1 and Question 2. Differences across variables were assessed with Mann–Whitney U tests. For the qualitative analysis, two coders (VTK and SMS) independently coded the free-text responses using the contextual method of manifest coding10,11 in order to group the responses into themes.
As a post hoc secondary analysis, we also determined whether the attending physicians had different ratings for teaching encounters than the residents participating in the same encounters. For this analysis, we again used teaching encounters as the unit of analysis and assessed differences with Mann–Whitney U tests.
Results
Quantitative analysis
Across 26 days of observation, there were 28 total teaching encounters. On 24 days of observation, one teaching encounter occurred in the observation period and on 2 days of observation, two teaching encounters occurred in the observation period. The number of PGY-1 residents present was as follows: 8 encounters (29%) with one PGY-1 resident, 5 (18%) encounters with two PGY-1 residents, and 15 encounters (54%) with three PGY-1 residents. The number of attending physicians present was as follows: 2 encounters (7%) with no attending physician, 16 encounters (57%) with one attending physician, and 10 encounters (36%) with two attending physicians.
A total of 136 surveys were distributed, and all 136 were completed and returned (100% response rate). Across all teaching encounters, attending physicians completed 37 surveys (27%), PGY-2 and PGY-3 residents completed 38 surveys (28%), and PGY-1 residents completed 61 surveys (45%).
There were 8 residents in total who taught the 28 total teaching encounters. The only demographic variable that correlated with encounter ratings was PGY number. Encounters by PGY-3 residents were rated significantly better (mean: 1.17 vs 1.47; P=0.01) and significantly more helpful (mean: 1.23 vs 1.57; P=0.005) than those by PGY-2 residents (Table 1). Gender, age, and educational background were not correlated with encounter ratings.
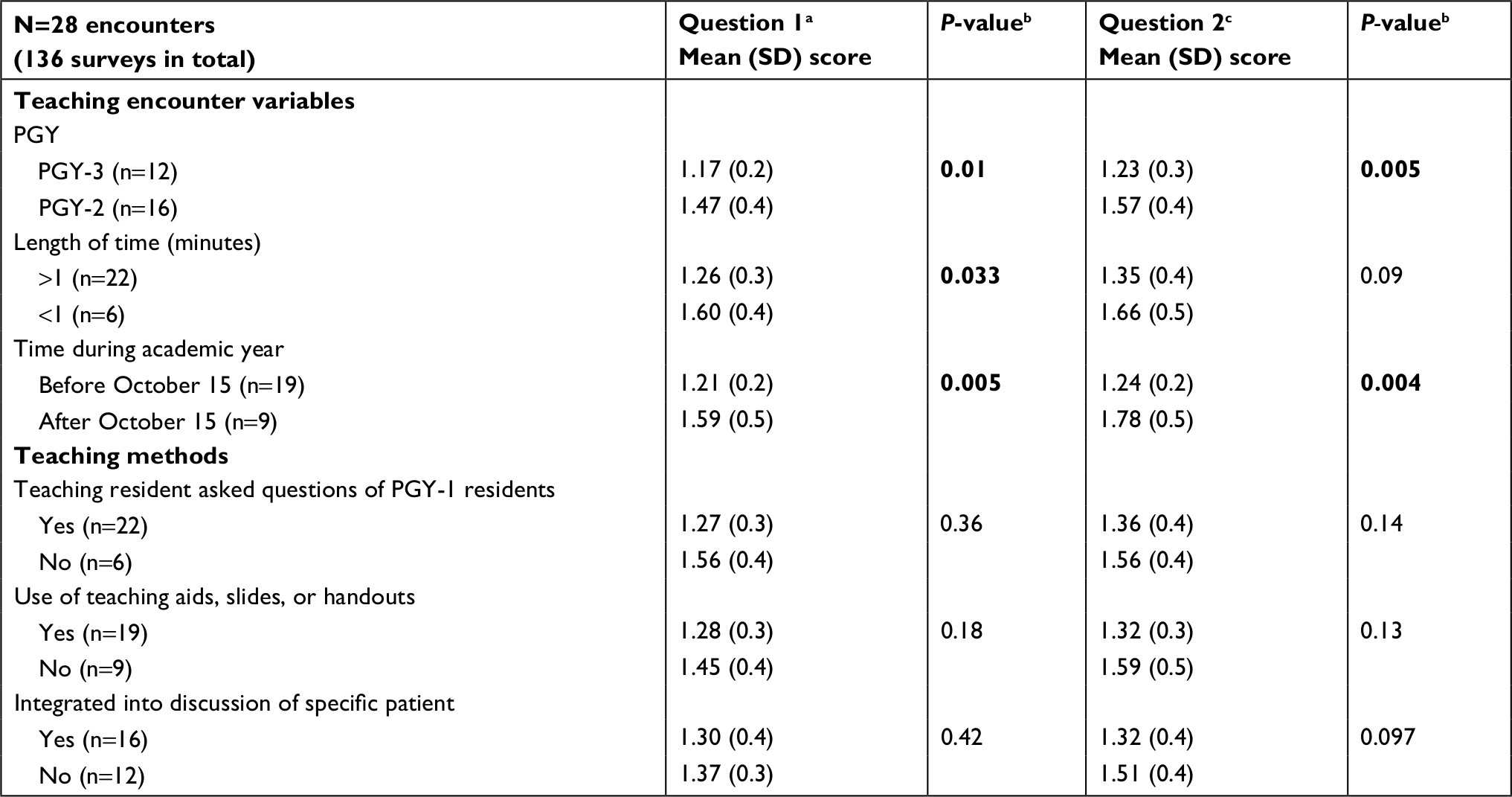 | Table 1 Mean teaching ratings compared by teaching encounter variables and selected teaching methods Notes: aQuestion 1: “Overall, how would you rate this teaching encounter?” (1=“Excellent” and 5=“Poor”). bP-values were calculated using Mann–Whitney U test and were considered significant if <0.05. Significant values appear in bold. cQuestion 2: “How helpful was this teaching encounter in covering the topic(s) presented?” (1=“Extremely helpful” and 5=“Not helpful”). Abbreviation: PGY, postgraduate year. |
Among the encounter variables, length of time and time of year were both associated with encounter ratings. Encounters lasting >1 minute were rated significantly better (mean: 1.26 vs 1.60; P=0.033) than those lasting <1 minute, with a nonsignificant trend toward being rated more helpful (mean: 1.35 vs 1.66; P=0.09). Additionally, encounters earlier in the academic year (before October 15, 2016) were rated significantly better (mean: 1.21 vs 1.59; P=0.005) and significantly more helpful (mean: 1.24 vs 1.78; P=0.004) than those later in the academic year.
No specific teaching method was associated with encounter ratings – including asking questions, using handouts, or integrating the teaching into the discussion of a particular patient.
In our post hoc secondary analysis, among the 26 encounters for which at least one attending physician was present, attending physicians rated the same encounters as significantly better overall (mean: 1.04 vs 1.42; P=0.0006) and significantly more helpful (mean: 1.17 vs 1.48; P=0.002) than did the residents.
Qualitative analysis
Across the 136 surveys, there were 161 total free-text responses to Question 3 and Question 4. Coding of these responses revealed five core positive attributes of teaching encounters: 1) immediate clinical relevance; 2) citing published evidence; 3) conciseness; 4) clarity; and 5) pertinence to the patient. Representative free-text responses highlighting these attributes can be found in Table 2. These five attributes alone accounted for ~58% of the total content of the free-text responses. The remainder of the responses emphasized the importance of the following: focusing on fundamentals, using visual aids, using an interactive and natural style, being brief, and explaining pathophysiology.
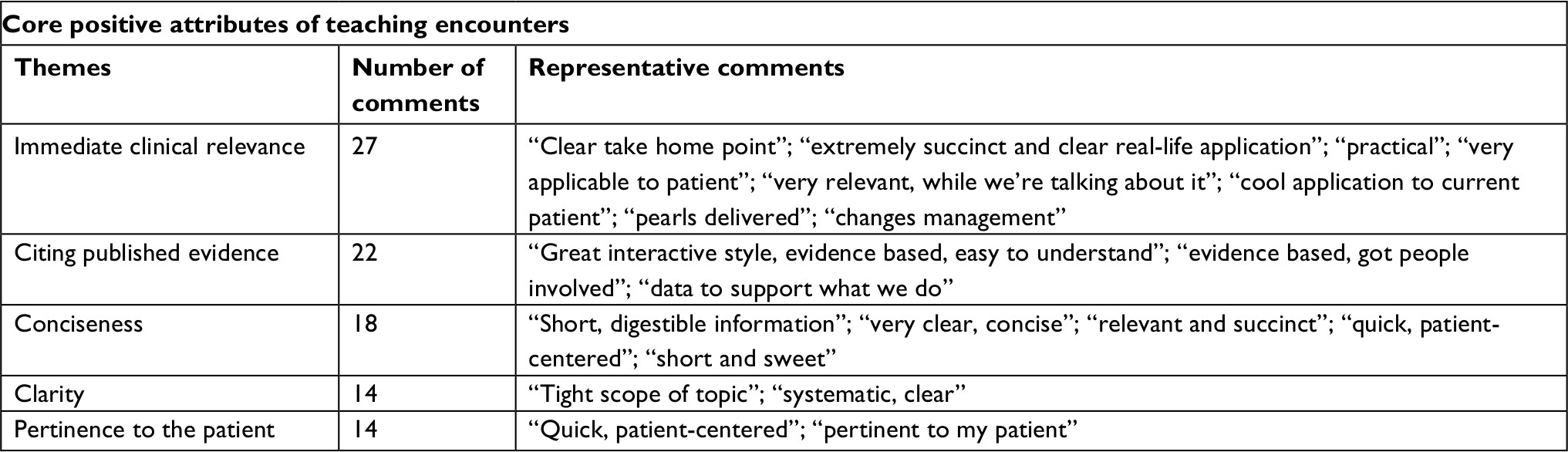 | Table 2 Summary of qualitative free-text responses |
Discussion
In our study, we observed and characterized resident teaching and captured team members’ attitudes in real time in a single academic medical center. Our key findings are that teaching encounters were better rated when conducted by PGY-3 residents (vs PGY-2 residents) and when they lasted >1 minute (vs <1 minute). We also identified five core positive attributes of resident teaching based on the residents’ and attending physicians’ free-text responses: 1) immediate clinical relevance; 2) citing published evidence; 3) conciseness; 4) clarity; and 5) pertinence to the patient.
Our quantitative analyses revealed several useful and notable findings. First, PGY-3 residents were rated as better teachers than PGY-2 residents. This difference might suggest that progressing through residency improves teaching skills, perhaps because IM residents at BWH have mandatory resident-as-teacher training in their PGY-2 year. Further research may be able to directly address whether the resident-as-teacher training is the explanation for the observed difference. Alternatively, PGY-3 residents have had more time to receive feedback on their teaching skills from attending physicians, and prior work has shown that IM residents’ teaching skills improve with direct observation and feedback.7 Second, teaching encounters lasting >1 minute were rated better than teaching encounters lasting <1 minute. This finding suggests not only that extremely short teaching encounters may be less effective, but also that targeted brief teaching encounters may be as effective as longer teaching encounters; given the time limitations on modern inpatient teaching services,12 the threshold time of 1 minute may not be surprising. Third, we found no significant correlations with specific teaching methods such as use of questions, problem-solving exercises, mini-lectures, or high-yield visuals. One explanation for the lack of these correlations is the small sample size. Given the exploratory nature of our study, further work will be needed to definitively answer which of these teaching methods are more effective. Fourth, we found that encounters occurring earlier in the academic year were rated higher than those occurring later. We speculate that, as the year progresses, PGY-1 residents have rising expectations of teaching by PGY-2 and PGY-3 residents. Overall, this may lead to less satisfaction later in the academic year even with the same level of teaching skills because techniques and strategies that are novel and impressive earlier in the year may lose their luster as time progresses. Further studies are needed to directly address the relationship between time during the academic year and the appreciation and recognition of resident teaching skills. Finally, in our post hoc secondary analysis, we found that attending physicians tended to rate teaching encounters more favorably than residents did. One possible explanation of this finding is that attending physicians’ expectations for resident teaching may be lower than residents’ expectations; another is that attending physicians wish to encourage and support resident teaching efforts with their more favorable ratings.
In our qualitative analysis, we identified five core positive attributes of a resident teaching encounter: 1) immediate clinical relevance; 2) citing published evidence; 3) conciseness; 4) clarity; and 5) pertinence to the patient. These findings echo other studies that have shown similar findings concerning teaching by the attending physicians.4,9,13 For example, one recent paper aimed at hospitalists highlighted the importance of “embedding teaching moments into rounds”.4 Another recent qualitative study of exemplary clinician–educator hospitalists emphasized the importance of interaction and patient-centeredness.13 Additionally, a recently published pilot study of including the patient as a co-teacher on rounds14 suggests that creative methods may help to address multiple core positive attributes simultaneously.
Interestingly, our qualitative analyses identified attributes that were not found to be significant in our quantitative analyses, such as whether teaching was integrated into the discussion of a particular patient. These differences may be due to differences between the observing study investigator’s characterization of the teaching encounters and the participants’ perceptions of the teaching encounters.
Our study has several limitations. First, we were able to observe residents at only a single academic institution, which may limit the generalizability of our findings. Second, our sample of teaching encounters and surveys was nonrandom and limited in size, and a larger sample may have yielded more nuanced observations. Third, medical students were not included in the study due to the fact that the exemption from the Partners Healthcare Institutional Review Board did not encompass medical students. Finally, due to the in-person nature of the study, observations could not be hidden from the observers, and we were unable to protect against the Hawthorne effect.15 Specifically, because residents knew in advance that their teaching was being observed during a particular block, they might have changed their teaching in ways that we could not detect.
Future directions of this work include the following: first, future studies may be able to expand the findings of this study by conducting observations on a larger scale or by observing residents without their prior knowledge in an attempt to minimize the Hawthorne effect. Second, future work will focus on designing a curriculum that teaches residents the core attributes identified in our study, and then on studying the impact of that curriculum on the educational outcomes of PGY-1 and PGY-2 residents.
In summary, our innovative findings serve as a useful guide to IM residents who wish to teach better on rounds. Our data indicate that residents on rounds should focus their teaching on immediate clinical relevance, citing published evidence, conciseness, clarity, and pertinence to the patient. Residents should also aim to teach for >1 minute to achieve the best peer and attending ratings. Our new findings provide the impetus for further research of specific resident teaching methods and their objective and subjective outcomes.
Disclosure
Dr Kulkarni completed this research as the fourth Nancy and Elliot Comenitz Fellow in Medical Education at Brigham and Women’s Hospital, as part of which he received a Master’s Degree in Education at the Harvard Graduate School of Education on May 25, 2018. The authors report no other conflicts of interest in this work.
References
Accreditation Council for Graduate Medical Education. ACGME 2017 program requirements for graduate medical education in internal medicine. Available from: http://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/140_internal_medicine_2017-07-01.pdf?ver=2017-06-30-083345-723. Accessed February 18, 2018. | ||
Ramani S, Mann K, Taylor D, Thampy H. Residents as teachers: near peer learning in clinical work settings: AMEE Guide No. 106. Med Teach. 2016;38(7):642–655. | ||
Walton JM, Steinert Y. Patterns of interaction during rounds: implications for work-based learning. Med Educ. 2010;44(6):550–558. | ||
Martin SK, Farnan JM, Arora VM. Future: new strategies for hospitalists to overcome challenges in teaching on today’s wards. J Hosp Med. 2013;8(7):409–413. | ||
Hauer KE, Irby DM. Effective clinical teaching in the inpatient setting. In: Wachter RM, Goldman L, Hollander H, editors. Hospital Medicine. Philadelphia, PA: Lippincott, Williams, and Wilkins; 2005. | ||
Ende J. What if Osler were one of us? Inpatient teaching today. J Gen Intern Med. 1997;12(Suppl 2):S41–S48. | ||
Snydman L, Chandler D, Rencic J, Sung YC. Peer observation and feedback of resident teaching. Clin Teach. 2013;10(1):9–14. | ||
Katz-Sidlow RJ, Baer TG, Gershel JC. Providing rapid feedback to residents on their teaching skills: an educational strategy for contemporary trainees. Int J Med Educ. 2016;7:83–86. | ||
Fluit CR, Bolhuis S, Grol R, Laan R, Wensing M. Assessing the quality of clinical teachers: a systematic review of content and quality of questionnaires for assessing clinical teachers. J Gen Intern Med. 2010;25(12):1337–1345. | ||
Weisberg H, Krosnick JA, Bowen BD. An Introduction to Survey Research, Polling, and Data Analysis. 3rd ed. Thousand Oaks, CA: SAGE; 1996. | ||
Vogt WP, Vogt ER, Gardner DC, Haeffele LM. Selecting the Right Analyses for Your Data: Quantitative, Qualitative, and Mixed Methods. New York, NY: Guilford Publications; 2014. | ||
Auger KA, Jerardi KE, Sucharew HJ, Yau C, Unaka N, Simmons JM. Effects of the 2011 duty hour restrictions on resident education and learning from patient admissions. Hosp Pediatr. 2014;4(4):222–227. | ||
Houchens N, Harrod M, Moody S, Fowler K, Saint S. Techniques and behaviors associated with exemplary inpatient general medicine teaching: an exploratory qualitative study. J Hosp Med. 2017;12(7):503–509. | ||
Perez AA, Pelletier SR, Klein IA, Shields HM. Patient as co-teacher on rounds: a pilot study. J Gen Intern Med. 2018;33(7):1010–1012. | ||
Sedgwick P, Greenwood N. Understanding the Hawthorne effect. BMJ. 2015;351:h4672. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.