")
Back to Journals » Advances in Medical Education and Practice » Volume 6
Teacher training program for medical students: improvements needed
Authors van Diggele C, Burgess A , Mellis C
Received 21 December 2014
Accepted for publication 22 January 2015
Published 1 April 2015 Volume 2015:6 Pages 265—270
DOI https://doi.org/10.2147/AMEP.S79671
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Christie van Diggele,1 Annette Burgess,2 Craig Mellis2
1The University of Sydney, Sydney, NSW, Australia; 2Sydney Medical School – Central, The University of Sydney, Sydney, NSW, Australia
Introduction: Skills in peer teaching, assessment, and feedback are increasingly documented internationally as required graduate attributes in medicine. Yet these skills are rarely taught in medical schools. We sought to design and deliver a short but effective teacher training (TT) program for medical students that could be easily integrated into the professional development curriculum. This study sought to evaluate such a pilot program, based on student perception.
Methods: The study took place at a major metropolitan teaching hospital, where 38 medical students were invited to attend a voluntary, newly designed four-module TT program. In total, 23/38 (61%) of invited students attended. Mixed methods were used for evaluation. Questionnaires were completed by 21/23 (91%) of students, and 6/23 (26%) of students participated in a focus group.
Results: Students reported that as a result of the program they felt more confident to facilitate small group teaching activities and to provide feedback to peers using the suggested frameworks. Students would like the program to contain more in-depth educational theory and to allow a more time for small group learning activities. They would also like to see opportunities for participation across all clinical schools.
Conclusion: The TT program was successful in increasing student awareness of educational theory and practice, thereby improving their confidence in teaching and assessing their peers and making them feel better prepared for their careers as medical practitioners. Key improvements to the program are needed in terms of more in-depth theory and more time spent on small group learning. This might be achieved by complementing the course with e-learning.
Keywords: teacher training, medical students, peer teaching, peer assessment
Introduction
Skills in peer teaching, assessment, and feedback are now increasingly documented internationally as required graduate attributes for medical students. Notably, the Australian Medical Council1 requires a graduate to demonstrate “fundamental skills in educating colleagues”, and the UK’s General Medical Council2 requires a graduate to “function effectively as a mentor and teacher”. Medical practitioners are expected to supervise, teach, facilitate, assess, and provide feedback to colleagues and contribute to the teaching of future generations of medical students. However, these skills are rarely taught in medical schools.3
In order to address students’ need to develop these professionalism skills, a teacher training (TT) program for medical students was established at Sydney Medical School - Central, Sydney, NSW, Australia, in 2010. This program has been previously described.4 Although highly valued by students, the program was time and resource intensive. The initial program was run over 18 hours, across six evenings, requiring a large commitment from both student participants and staff facilitators. For example, five academic staff members were required to facilitate teaching and small group activities. Largely due to the required time commitment, only 17/53 (32%) of students participated.4 As it was not possible to sustain such a resource-intensive program, a new, shorter program was designed.
Brown5 (2000) states that “teaching in higher education is too important to be left to chance.” By integrating the professionalization of teaching into the medical curricula, teaching and educational scholarship is highlighted by appealing to the moral responsibilities of those entering the medical profession.6 Teaching and assessing peers also has the potential to alleviate teaching duties for academic staff and clinicians by engaging senior medical students to teach junior students.7 Finding an effective design and delivery of a program that would concurrently widen participation was therefore an important priority for faculty.
The new TT program was first piloted in 2013 and formally evaluated in 2014, as reported in this paper. Targeted at senior students, development was informed by medical educational literature, highlighting associated cognitive, pedagogical, attitudinal, and social benefits of peer teaching, assessment, and feedback.7,8 The program addresses the identified needs of senior students: to develop professionalism skills in teaching and feedback. The program aims to help students prepare for peer-assisted learning activities within the medical program, including acting as peer teachers and assessors in various peer teaching and assessment activities, and also to better prepare them for future careers in medicine.
Our study sought to examine students’ perceived effectiveness of the TT program. Our specific aims were twofold: to explore students’ experience of the course and how the course impacted on their confidence to participate in peer-assisted learning activities, particularly in teaching, assessing, and providing feedback to peers.
Methods
Context
The setting in which this study took place was the Royal Prince Alfred Hospital (RPAH), where Sydney Medical School – Central students spend the final 2 years of their 4-year, graduate entry, problem-based medical program. The TT program being evaluated was implemented at the RPAH in March 2014.
Participants
All Year 3 medical students attending the RPAH were invited to attend (n=30). We also invited four final year medical students from the University of Western Sydney (n=4), two Sydney Medical School – Northern students (n=2), and two Sydney Medical School – Concord students (n=2) to attend. Thus, a total of 38 students were invited.
Facilitators
Facilitation was led by two academic staff from the University of Sydney and the University of Western Sydney. Five final year medical students who had completed the course in 2013 (as Year 3 Sydney Medical School – Central students) assisted in facilitation.
Structure and content
The program was run over two 3-hour sessions on two afternoons. The program was delivered as a four-module face-to-face program, providing theoretical background, practical examples, and active participation in “skills teaching”, “small group teaching”, “clinical teaching”, plus “assessment and feedback”. The outcomes of the program included the ability to plan small group learning activities, understand the steps in teaching a skill, and understanding the steps in providing effective feedback. Facilitation included interactive large group PowerPoint presentations, as well as two small group sessions. Each small group consisted of three to four students and was facilitated by either a final year medical student or an academic staff member. During the small group sessions, participants were required to teach their peers a short 5- to 10-minute microteaching activity. The first activity was to teach a nonmedical skill using Peyton’s9 four-step approach. The second was a teaching presentation on a medical topic using Peyton’s model of “set, dialogue, closure”.9 Small group participants were required to provide feedback during small group sessions using Pendleton’s10 positive critique method.
The study was conducted using mixed methods to collect quantitative and qualitative data to assess student perception of the TT program. A structured questionnaire and a semistructured focus group were used. The items within the questionnaire and the focus group questions were based on the outcomes of the TT program and students’ perceived ability to take part in peer teaching and assessment activities.
Quantitative data
Quantitative data were collected by questionnaire, reflecting on how participants perceived their learning outcomes for each of the four modules. Students were asked to respond to 12 closed questions, such as “As a result of this course, I feel more confident to plan a small group teaching activity using set, dialogue, and closure.” A five-point Likert scale ranging from “strongly disagree” (1) to “strongly agree” (5) was used. Data were entered into Excel and analyzed using descriptive statistics.11 Immediately after completion of the program, all students (n=23) were asked to complete the questionnaire.
Qualitative data
The questionnaire also included three open-ended questions aimed at identifying what students found to be the most useful aspects of the course and suggestions for improvement. Additionally, at the completion of the course, all participants (n=23) were invited to attend focus groups. The focus group questions were semistructured and were designed to explore students’ perceptions of the course in greater depth. Focus group data were transcribed verbatim. The combined data were read by the first author and analyzed to identify themes. Following negotiation of meaning with the second and third authors, a coding framework was developed and applied to the full data set.11
Ethics approval was obtained from the University of Sydney Human Research Ethics Committee.
Results
In total, 23/38 (61%) of invited students chose to participate in the course. Of the participants, 13 were male and ten were female.
Questionnaires were completed by 21/23 (91%) of students; two students failed to hand in their questionnaires. Of these 21 students, 13 were male and eight were female. The median age was 24 years (n=16), with a range of 23–28 years. In total, 6/23 (26%) of students participated in the focus group session. Three students were male and three female.
Quantitative
The questionnaire results are reported in Figure 1. Notably, almost all (95%) of the students reported that as a result of the course they felt more confident to plan small group teaching activities using the provided structure. Further, almost all (95%) of the students reported being likely to use the positive critique methods as shown in the program.
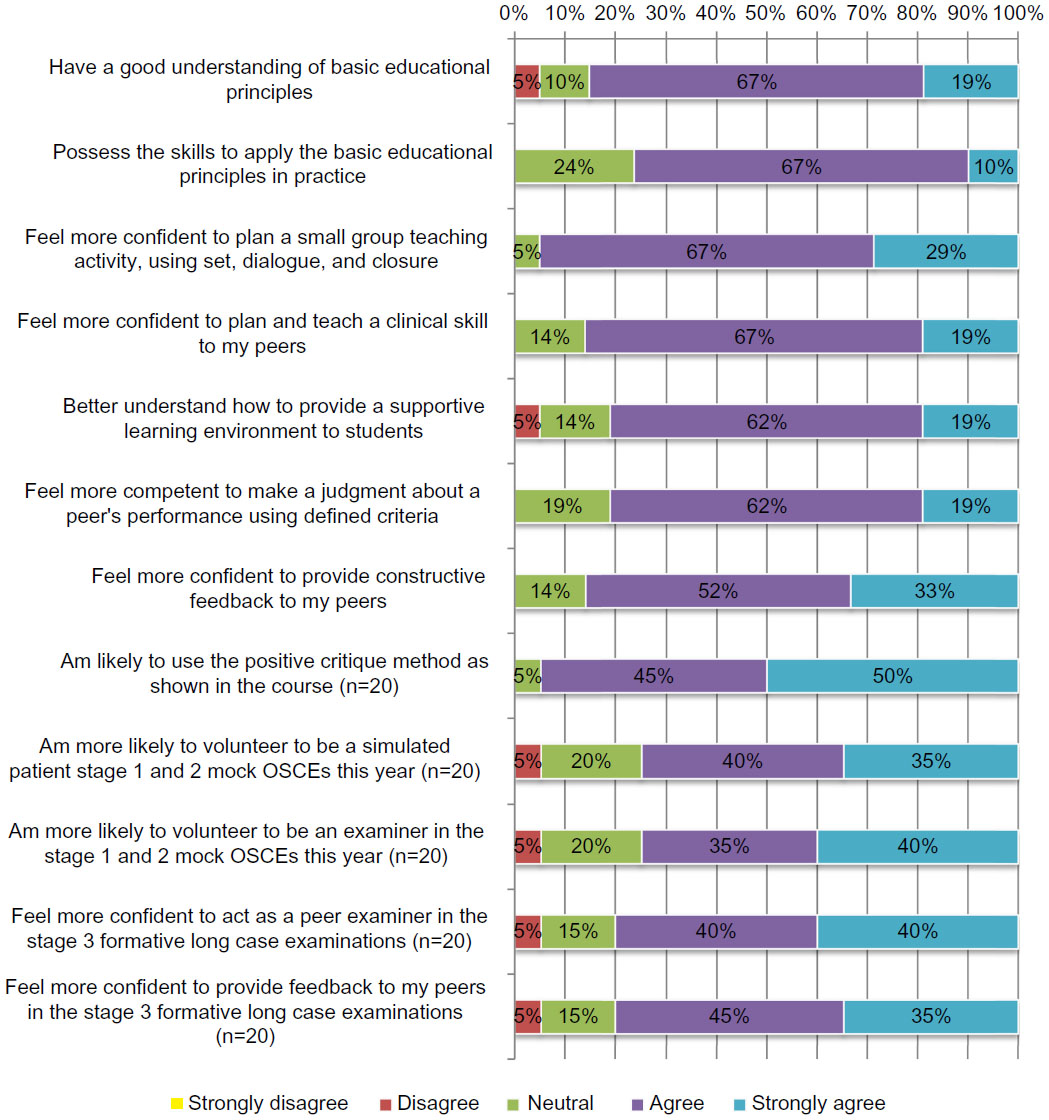 | Figure 1 Students’ perception as to intended teacher training outcomes (N=21). |
Qualitative
Qualitative data consisted of responses to open-ended questions (response rate 21/23 [91%]) and one focus group, in which 26% (6/23) of students participated. The qualitative findings contextualized 1) students’ perceived best features of the course and 2) students’ perceived areas for improvement of the course. These emerging themes are summarized in Tables 1 and 2.
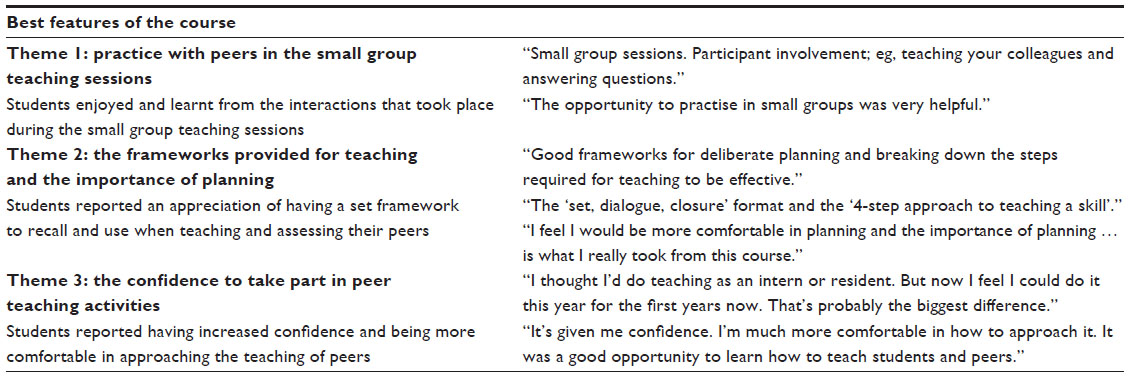 | Table 1 Student qualitative responses regarding the best features of the teacher training program |
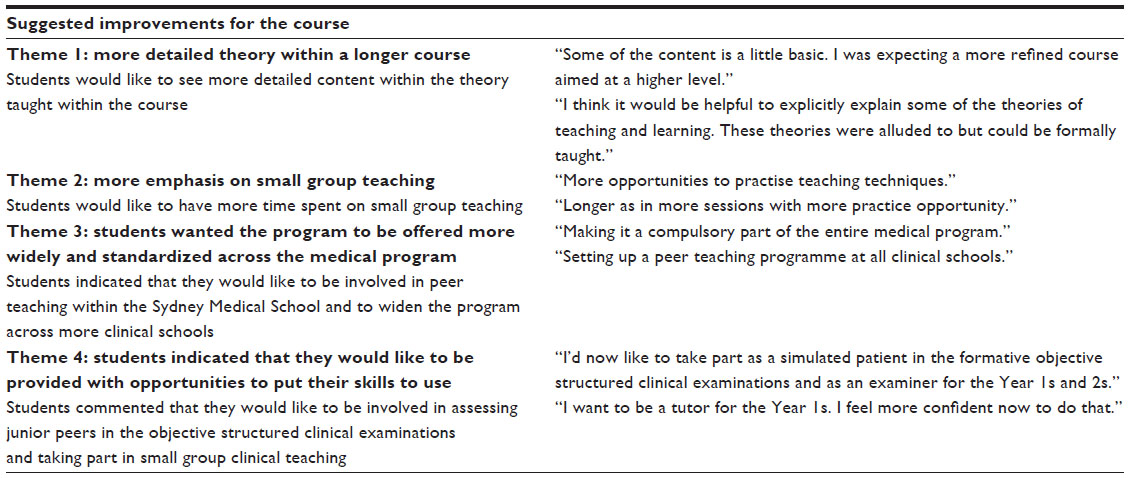 | Table 2 Student qualitative responses regarding suggested improvements to the teacher training program |
Discussion
Students generally perceived the program to be effective in increasing their perceived understanding of basic educational principles and their ability to apply them. In particular, students found the course useful in providing a framework to design teaching activities and provide feedback to peers. This was reflected in the survey responses, where 95% of students agreed or strongly agreed that they felt more confident to “plan a small group teaching activity using set, dialogue, and closure” and were likely to “use the positive critique method as shown in the course”. It was also reflected in students’ qualitative responses, where students found one of the most useful aspects of the course to be the “good frameworks for deliberate planning and breaking down the steps required for teaching to be effective”. However, students did express a desire for longer small group sessions with “more practice opportunities”. Students value small, interactive group learning, with opportunities to receive feedback.12 Additionally, active learning opportunities that engage students provide metacognitive benefits, including a deeper understanding and greater retention of knowledge.13
Surprisingly, students reported finding the content “a little basic” and were “expecting a more refined course aimed at a higher level”. They felt that some of the information conveyed was too simple. Perhaps this suggests that students are more interested in teaching than we thought. This finding might be attributed to the medical program being graduate entry, with students having various previous experiences. Given the lack of available time for teaching within the curriculum, perceived benefits of practical skills, and the students’ desire for extended small group sessions, a greater amount of theory could be provided and taught through e-learning, allowing more in-class time for small group practical sessions.
Students perceived an increased likelihood that they will take part in future formative clinical teaching and assessment activities such as the formative objective structured clinical examinations, where Year 4 students act as examiners and Year 3 students act as simulated patients. However, students indicated that they need to be provided with additional opportunities to develop their new skills. Although the school provides formal opportunities in formative assessment activities, at the time of the TT program implementation, there were no formal opportunities for practice in small group peer teaching. Evidence suggests that active learning opportunities that engage students provide a deeper understanding of knowledge and extended retention.14,15
Students indicated a desire for widening opportunities for participation in the program. They suggested that the program be embedded in the medical curriculum and standardized across the clinical schools. Certainly, medical programs are increasingly addressing competencies such as patient safety, bioethics, and community involvement within personal and professional development curricula.16 However, in the 21st century, as evidenced by required graduate competences,1,2 medical programs have an additional responsibility to ensure that opportunities are made available to students to develop skills in medical education.
The TT program has proven successful in increasing student awareness of the quality of educational practice, thereby improving their confidence in teaching and assessing their peers and better preparing them for careers as medical practitioners and educators. The current TT program has the potential to help shape the school’s community and add to its social capital. By offering a program that fits the needs of the students, and one that can be offered to the wider student community, participation and the associated benefits may be increased.
Implications of findings
Students’ comments reflect the need for:
- an increased number of small group sessions;
- provision of more detailed educational theory;
- opportunities for wider participation in the TT program across the medical student community;
- a move to blended learning, with extended theory provided online; and
- additional formal opportunities for students to practice their teaching and feedback skills with peers on completion of the program.
Study limitations
The limitation of this study may be the small number of participants and the fact that the evaluation was undertaken on a single iteration of the TT program. The course was voluntary, and it is likely that students who chose to participate in the course were those with a pre-existing interest in education. The survey and focus group questions were based only on student perception of the course. It is possible that these students would respond positively to surveys and focus group questions. The low response rate to the focus group session should also be noted.
Conclusion
Participation in the TT program has helped to emphasize students’ significant roles and responsibilities as medical students and develop their future roles as medical practitioners with teaching, assessment, and lifelong learning responsibilities. With the provision of set frameworks and opportunities for practice in small groups, the program helped to increase students’ confidence to take part in peer teaching opportunities. Key improvements to the TT program are needed in terms of more in-depth theory and greater time spent on small group teaching activities. There is potential for achieving this with the assistance of e-learning. On completion of the program, additional opportunities to practice their newly acquired teaching skills would also benefit students.
Disclosure
The authors report no conflicts of interest in this work.
References
Australian Medical Council. 2012. Accreditation Standards for Primary Medical Education Providers and their Program of Study and Graduate Outcome Statements; 2012. | |
General Medical Council. 2009. Tomorrow’s Doctor Outcomes and Standards. London, UK: General Medical Council. Available at: http://www.gmc-uk.org/static/documents/content/tomorrows_doctors_1214.pdf. Accessed February 16, 2015. | |
Gibson DR, Campbell RM. Promoting effective teaching and learning: hospital consultants identify their needs. Med Educ. 2000;34: 126–130. | |
Burgess A, Black K, Chapman R, Clark T, Roberts C, Mellis C. Clinical teaching skills for students: our future educators. Clin Teach. 2012;9(5):312–316. | |
Brown S. The Institute of Learning and Teaching and UK approaches to accrediting teaching: looking at the future. Med Tech. 2000;22(5): 513–516. | |
Hill F, Stephens C. Negotiating strategic direction for education staff development: the Southampton experience. Med Teach. 2004;26(7):645–649. | |
Ten Cate O, Durning S. Peer teaching in medical education: twelve reasons to move from theory to practice. Med Teach. 2007;29(6): 591–599. | |
Sluijsman D, Dochy F, Moerkerke G. Creating a learning environment by using self-, peer-, and co-assessment. Learning Environment Research. 1999;1:293–319. | |
Peyton JRW. Teaching and Learning in Medical Practice. Rickmansworth, UK: Manticore Europe Limited; 1998. | |
Pendleton D. The Consultation: An Approach to Learning and Teaching. Oxford, UK: Oxford University Press; 1997. | |
Creswell J. Educational Research: Planning, Conducting and Evaluating Quantitative and Qualitative Research. Upper Saddle River, NJ: Merrill; 2002. | |
O’Malley KJ, Moran BJ, Haidet P, et al. Validation of an observation instrument for measuring student engagement in health professions settings. Eval health Prof. 2003;26:86–103. | |
Bransford J, Brown A, Cocking R. How People Learn: Brain, Mind, Experience and School. Washington, DC: National Academy Press; 1999. | |
Graffan B. Active learning in medical education: strategies for beginning implementation. Med Teach. 2007;29:86–103. | |
Biggs J. Teaching for Quality Learning at University. 2nd ed. Berkshire, UK: Open University Press; 2003. | |
Irby DM, Wilkerson L. Educational innovations in academic medicine and environmental trends. J Gen Intern Med. 2003;18(5):370–376. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.