")
Back to Journals » Cancer Management and Research » Volume 15
Targeted Treatment of Relapsed or Refractory Follicular Lymphoma: Focus on the Therapeutic Potential of Mosunetuzumab
Authors Lopedote P , Shadman M
Received 8 January 2023
Accepted for publication 10 March 2023
Published 14 March 2023 Volume 2023:15 Pages 257—264
DOI https://doi.org/10.2147/CMAR.S381493
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Rudolph Navari
Paolo Lopedote,1 Mazyar Shadman2,3
1Department of Medicine, St Elizabeth’s Medical Center, Boston, MA, USA; 2Clinical Research Division, Fred Hutchinson Cancer Center, Seattle, WA, USA; 3Department of Medicine, University of Washington, Seattle, WA, USA
Correspondence: Mazyar Shadman, Clinical Research Division, Fred Hutchinson Cancer Center, 1100 Fairview Ave, Seattle, WA, 98109, USA, Tel +1 206-667-5467, Email [email protected]
Abstract: Follicular lymphoma is the most common indolent non-Hodgkin’s lymphoma, and because of the incurable nature of this disorder, new therapies are constantly needed. The recently approved T-cell-dependent bispecific antibody mosunetuzumab showed promising results and manageable toxicities for patients with relapsed or refractory follicular lymphoma. Namely, as opposed to cellular immunotherapy options, this agent has the potential of being effective in patients with unfavorable features with a tolerable rate and severity of cytokine release syndrome, immune effector cell-associated neurotoxicity, and infectious complications. Given the recent withdrawal from the market of PI3K inhibitors and the practical challenges in utilizing with chimeric antigen receptor T-cells (CAR-T) for some patients, mosunetuzumab represents a “breath of fresh air” for both patients and hemato-oncologists. More data are required to better define the real potential of this molecule, either alone or in combination with other agents, including antibody drug conjugates, immunomodulators, and checkpoint inhibitors. Future studies will also shed light on the efficacy of mosunetuzumab compared with CAR-T, in well-designed registries or ideally in randomized controlled trials.
Keywords: mosunetuzumab, follicular lymphoma, T-cell-dependent bispecific, bispecific antibody
Introduction
Follicular lymphoma (FL) is a mature B cell neoplasm with a germinal center differentiation.1 It represents approximately 30% of all lymphomas and is the most common indolent non-Hodgkin lymphoma (iNHL).2 As other slowly proliferating NHLs, FL has a high 5-year survival rate and, with the exception of early stage (I–II) disease, is substantially uncurable.3–5 With the majority of patients having disease progression (PD) after initial treatment and the duration of response (DoR) becoming progressively shorter after subsequent lines, there is a continuous need to identify novel strategies for relapsed or refractory (r/r) FL.6,7 Results from a large national retrospective analysis showed a dramatic decrease of the median progression-free survival (PFS) following the first, second, and third relapse (6.6, 1.5, and 0.83 years, respectively).8 This necessity is even more impelling for patients experiencing PD within 2 years from first-line therapy (POD-24), a population with a particularly poor prognosis.9–11 In response to this clinical need, the landscape of treatment options for r/r FL has witnessed significant changes in the last decade (Figure 1). An initial expansion resulted from the accelerated approval of many small molecule inhibitors (ie, copanlisib, duvelisib, tazemetostat, umbralisib) and lenalidomide with rituximab (R2) from late 2017 to early 2021, which added to the already available idelalisib. This growth was followed in late 2021 by the approval of chimeric antigen receptor (CAR) T-cell, axicabtagene ciloeucel (axi-cel) and tisagenlecleucel (tisa-cel), as a result reported in the ELARA and ZUMA-5 trial.12,13 Since the introduction of CAR T-cell, the indication of idelalisib, duvelisib, and umbralisib has been voluntary withdrawn, as a consequence of the growing concerns raised by additional safety analysis and the excess of deaths in the more recent UNITY-CLL study. Notwithstanding their impact, CAR T-cell therapy can only partially alleviate the burden of r/r FL and fill the large void left by the withdrawal of most PI3K inhibitors. When looking at large B-cell lymphoma, access to CAR T-cell is precluded in up to 50% of the patients at need because of the exclusion criteria of the pivotal studies, boosting the necessity of alternative therapies.14,15 Additionally, only a minority of the eligible patients are able to access CAR-T. The reasons are multiple and include the limited number of authorized centers, the long manufacturing time and the financial burden for patients and families. Furthermore, a limited number of effective treatments are currently available for patients with PD after CAR-T. Therefore, besides expanding access to this revolutionizing platform, a constant search of new approaches is mandatory.
 |
Figure 1 Timeline of the approval and withdrawal of the agents for the treatment of relapsed and refractory follicular lymphoma. |
In this scenario, a promising option is represented by the T-cell-dependent bispecific (TDB) antibody mosunetuzumab-axgb, which has been recently approved by the Food and Drug Administration (FDA) in December 2022 for treatment of patients with FL after two prior lines of therapy. Herein, we summarize the available literature on this agent in the setting of r/r FL, with a focus on the recent Phase II studies and the ongoing clinical trials.
Mosunetuzumab, Results from the Pivotal Studies
CD20 is a four-transmembrane-domains molecule whose expression spans from late pre-B cells to post-germinal center B-cells and is notably expressed in the majority of B-cell lymphoma.16 The TDB mosunetuzumab is a full-length humanized Ig-1 antibody consisting of two antigen-binding Fab arms, targeting CD3 and the B-cell antigen CD20, both linked to a Fc fragment.17 Binding of these targets redirects CD8+ T-cells towards tumoral cells, facilitating their cytotoxic action. While this approach is similar to that of bispecific T-cell engager (ie, blinatumomab), the latter consists of two single-chain antibodies fused into a single polypeptide chain, lacking a typical Fc region.18 Conversely, mosunetuzumab was generated using a novel molecular format, known as knobs-into-holes, allowing to create distinct Fab arms without affecting the IgG structure.19,20 These differences result in a diverse pharmacokinetic, including a longer half-life of mosunetuzumab, which does not require continuous infusion.18,21 Its clinical activity was first explored in the phase I/Ib part of the GO29781 (NCT02500407), where diffuse large B-cell lymphoma (DLBCL), transformed FL, and FL who failed ≥2 lines of therapy were enrolled.22 Patients were initially assigned to either a fixed-dose every 21 days (group A) or a step-up dosing (group B) cohort, but enrollment to group A was prematurely stopped to mitigate the risk of cytokine release syndrome.23 A step-up protocol of 1 mg on cycle 1 day 1, 2 mg on cycle 1 day 8, 60 mg on cycle 1 day 15 and cycle 2 day 1, and 30 mg on day 1 of cycle 3 and onwards was selected for subsequent studies. Frequent adverse events (AE) included neutropenia (28.4%), cytokine release syndrome (CRS) (27.4%), diarrhea (21.8%) and anemia (18.8%). Notably, grade ≥3 CRS occurred in 1% of the patients, while the most frequent severe AE were neutropenia (25.4%), anemia (9.1%), and hypophosphatemia (15.2%). Three percent had febrile neutropenia and 7 patients (3.6%) had to stop mosunetuzumab due to side effects. Budde et al recently published the results of the phase II analysis of the GO29781 trial and the updated analysis has been presented at the ASH meeting.24,25 Among the 90 patients enrolled, ORR was 80% and 54 (60%) had a CR, with a median PFS which was not reached in the updated analysis. CRR was not significantly lower in patients refractory to both an anti-CD20 and an alkylating agent (double-refractory), heavily pre-treated (≥3 lines), or POD-24 patients, which constituted >50% of the cases. Interestingly, responses were observed even among patients previously treated with CAR-T (ORR 100%, CR 33%), but the absolute number of this subgroup was too small (n=3) to establish the significance of this finding. Similarly to the phase I/Ib analysis, neutropenia was the most frequent grade ≥3 adverse event (26%), followed by hypophosphatemia (17%) and infection (14%). Forty-two percent experienced grade 1–2 CRS, as opposed to 2% who instead had a grade ≥3. All the immune effector cell-associated neurotoxicity (ICANS) (5%) were grade 1–2 and they all resolved. Treatment discontinuation due to an AE occurred in 4% of the patients and two patients (2%) had a grade 5 AE. Of note, a low number of COVID-19 infection was detected during the study (two grade 1 and two grade 3) and all resolved. Given the mild impact of COVID-19 on the study population, it is not easy to determine the effect of mosunetuzumab on the clinical course of COVID-19 infection. However, it is reasonable to think that it may be comparable to that of other anti-CD-20 monoclonal antibodies, which have been associated with a higher mortality rate.26–28 These promising results prompted the FDA and the European Medicines Agency (EMA) to approve this medication for r/r FL who failed ≥2 lines of therapy.29
Consistently with the data from the pivotal study, a step-up protocol of administration is advised in the FDA label. This involves a progressive dose increase, starting from 1mg on day 1 of cycle 1 (d1c1), followed then by 2mg on day 8 (d8c1), and then eventually a dose of 60mg on day 15 (d15c1). Subsequent administrations are repeated every 21 days for a total of 8 cycles for patients achieving a CR and the possibility of extending to a total of 17 cycles for those achieving a PR or a stable disease. A dose of 60mg is employed on day 1 of cycle 2 (d1c2), but this is decreased to 30mg from cycle 3. To minimize reactions, infusion occurs over 4 hours during the first cycle and can be reduced to 2 hours from cycle 2 if it was well tolerated. Lastly, as an additional strategy to mitigate CRS, premedication with steroids (dexamethasone 20mg or methylprednisolone 80mg intravenously) in association with oral acetaminophen and antihistamine (oral or intravenous) is administered before cycle 1 and 2, and is continued from cycle 3 for patients experiencing CRS of any grade. Depending on the cycle, a different median time to onset of CRS was noted in the main study24 (5 hours for d1c1, 25 hours for d15c1, 46 hours for d1c2), and patients should be educated accordingly. As for CAR-T cell therapy, ASTCT consensus guidelines are used to assess severity of CRS.30 Besides holding the medication with a CRS of any grade, a 50% dose reduction can be considered for grade 2 and should be implemented for grade 3, while a recurrent grade 3 or a grade 4 CRS should lead to a permanent discontinuation of mosunetuzumab. However, as the majority will experience only low-grade symptoms (fever, headache), with a median duration of 3 days,24 many patients can be effectively managed in the outpatient setting.
Mosunetuzumab in the Therapeutic Landscape for r/r FL
The decision to approve mosunetuzumab from the two regulatory agencies came with little if no surprise. Indeed, the ORR and CRR obtained by mosunetuzumab in the phase II cohort compared favorably to other products previously approved for the same target population (Table 1). Among those, duvelisib and umbralisib were also assessed in heavily treated populations, with a median of three previous lines of therapy.31,32 However, the rate of POD-24 and double-refractory was not reported. Despite the more favorable patients’ characteristics, response rates were significantly lower compared to mosunetuzumab (42.2% and 45.3% for duvelisib and umbralisib, respectively). As previously stated, following the approval of CAR-T cell, the indication of idelalisib, duvelisib, and umbralisib has been voluntary withdrawn, leaving copanlisib as the only remaining PI3K inhibitor still on the market. Copanlisib was assessed as single agent in the CHRONOS-1 study and in combination with rituximab in the CHRONOS-3 trial.33,34 Although the ORR for the combination treatment was 85% in FL, CRR was only 34%. Additionally, the population of the CHRONOS-3 study was substantially more favorable compared to the one of previous works, with a median of 2 previous therapies and no adequate representation of the POD-24 subgroup. Another popular chemotherapy-free option is represented by R2, which was evaluated in the AUGMENT and MAGNIFY study.35,36 As for the CHRONOS-3, enrolled patients were generally displaying less aggressive features, with about 30% POD-24 and only 25% exposed to >2 lines in the AUGMENT trial. While this combination was associated with high ORR (ranging 70–80%), CRR was lower (35–41%) and outcome of double-refractory patients were unsatisfactory (CRR 26%),36 suggesting this option could be more suitable earlier in the disease course. Lastly, the EZH2 inhibitor tazemetostat showed discrete results in the EZH2mut population with an ORR of 69%. However, two main limitations are the low CRR (13%) and the low frequency of the EZH2mut (less than a third of the FL population), further reducing its employability as single agent.37 Interestingly, the association of tazemetostat with R2 recently presented at ASH demonstrated promising results in the phase Ib analysis.38 Of the 41 evaluable patients, the ORR was 97.6% and the CRR was 51.2%, with excellent response in the POD24 subset (100% ORR). While these data are encouraging, they are not substantially different from those presented in the AUGMENT and MAGNIFY trial. Additionally, the included patients were generally not highly pre-treated (31.8% received >1 previous line) and the percentage of double-refractory was not specified. Therefore, given the discrepancy between the results attained by mosunetuzumab and the other novel agents, its natural term of comparison are the two CAR-T cells products. The ELARA and the ZUMA-5 trial assessed the efficacy of tisacel and axicel, respectively, in two populations which were comparable to the one of the GO29781 (ie, 55–62.9% of POD-24). Ninety-four patients were included in efficacy set of the ELARA trial, while 84 r/r FL were eligible for the primary analysis in the ZUMA-5. ORR was 86.2% (CRR 69%) for tisacel and 94% (CRR 79%) for axicel, with no differences across subtypes. Grade ≥ 3 infectious complications were similar across studies, with approximately 15% in the ZUMA-5, 15.2% in the ELARA (10% febrile neutropenia and 5.2% other infections), and 14% for mosunetuzumab. However, CRS was more frequent and more severe after axicel, with approximately 72% grade 1–2 events and 6% grade ≥ 3, including 1 grade 5 event. Similarly, grade ≥3 ICANS and neurological AE occurred in 15% following axicel and in 4% following tisacel. Lastly, only 2 deaths (2%) were reported in the mosunezutumab phase II study, as opposed to 5% grade 5 AE for axicel and 7 deaths (7%) for tisacel. Furthermore, CAR-T manufacture timing is still an obstacle to be taken into consideration. In the two pivotal studies, median time from enrolment to infusion was 46 days for tisacel, while time from apheresis to infusion was 17 days for axicel. Mosunetuzumab is a promising option with a favorable toxic profile, which appears to be effective in aggressive FL subgroups and can obviate some logistical limitations of CAR-T cells, including processing time and low number of equipped centers. Of particular interest is the possibility of administering this treatment in an outpatient setting, possibly making this option more sustainable. In this regard, it is worth to mention the preliminary data regarding the subcutaneous route of administration presented at the last ASH meeting, which are confirming a high rate of response (ORR 82% CR 60%) with similar toxicities.39 Should these data be confirmed, it may further increase convenience of mosunetuzumab over other alternatives. A last note
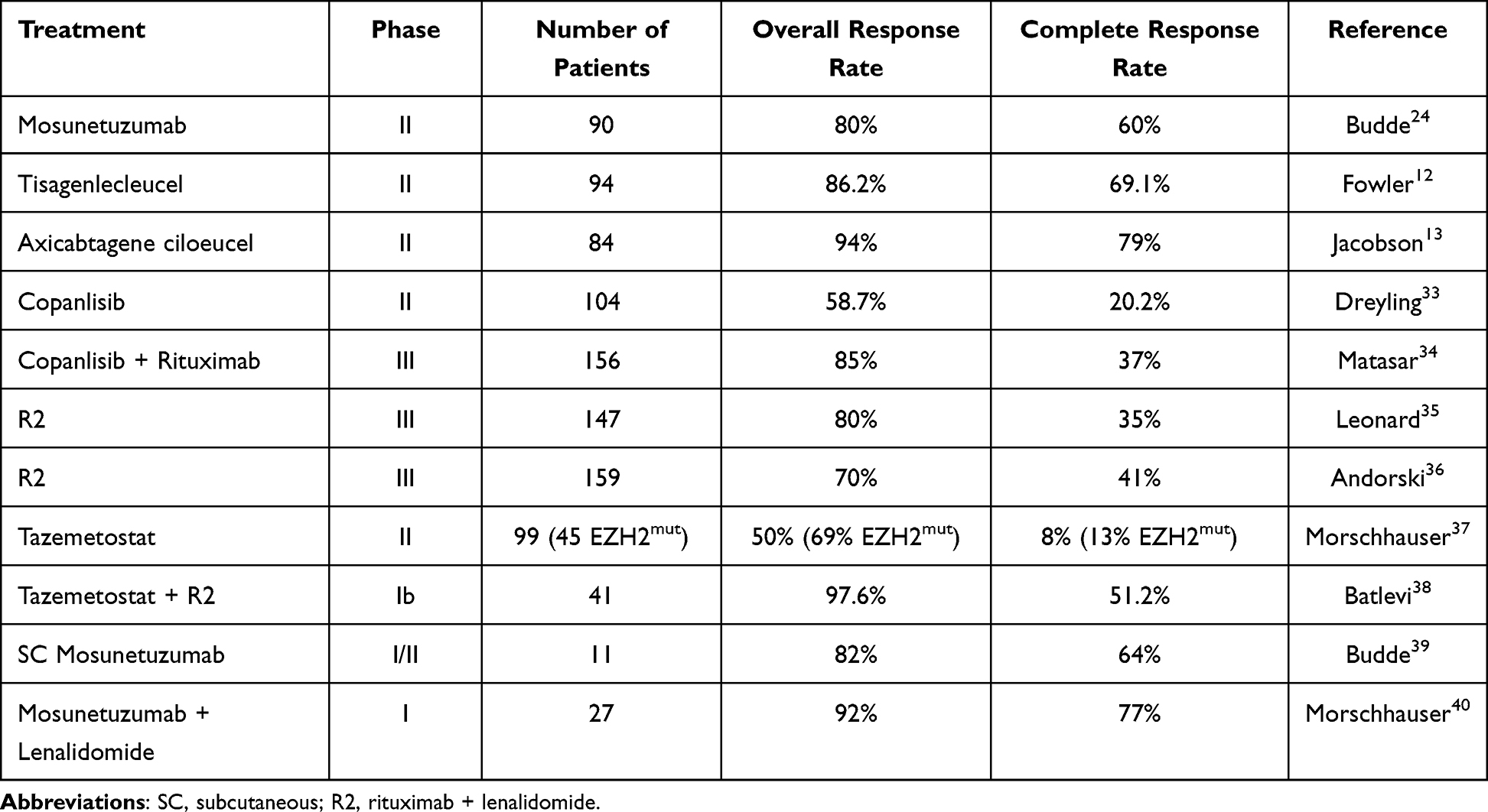 |
Table 1 Main Studies Involving Mosunetuzumab and the Approved Agents for the Treatment of Relapsed/Refractory Follicular Lymphomas |
Ongoing Trials and Future Perspectives
Following the results in patients treated with at least two lines, several studies are currently evaluating mosunetuzumab in combination with other agents in the setting of FL either untreated or exposed to one line of therapy (Table 2). An area of interest is represented by the combination of mosunetuzumab with lenalidomide. This association has already been explored in a phase Ib trial on 27 r/r FL, where no increased toxicities compared to monotherapy with mosunetuzumab were detected and encouraging response (ORR 92% CR 77%).40 This regimen is currently being evaluated for treatment-naïve FL (NCT04792502) and r/r FL after at least one line (NCT04712097, NCT04246086). Among the above mentioned trials, the Phase III study CELESTIMO is comparing R2 and mosunetuzumab-lenalidomide as a first salvage.41 Another option which is being currently evaluated in many trials (NCT05410418, NCT05169658, NCT03671018, NCT03677141) is the combination of mosunetuzumab and polatuzumab vedotin, which is already approved for r/r DLBCL and has been explored in the POLARIX study in untreated DLBCL.42 Data regarding the efficacy of this antibody drug conjugate in association with rituximab for r/r FL are scarce and derives mostly from subset analysis of the ROMULUS study.43 Lastly, promising few trials are evaluating mosunetuzumab together with the PD-L1 inhibitor atezolizumab (NCT05315713, NCT02500407) following at least two prior treatments or for patients without other available options. Although there is still limited evidence regarding the combination of checkpoint inhibitor and TDB, this association has the promises of broadening the efficacy of endogenous T-cells by potentially circumventing a mechanism of resistance of neoplastic cells.44–47
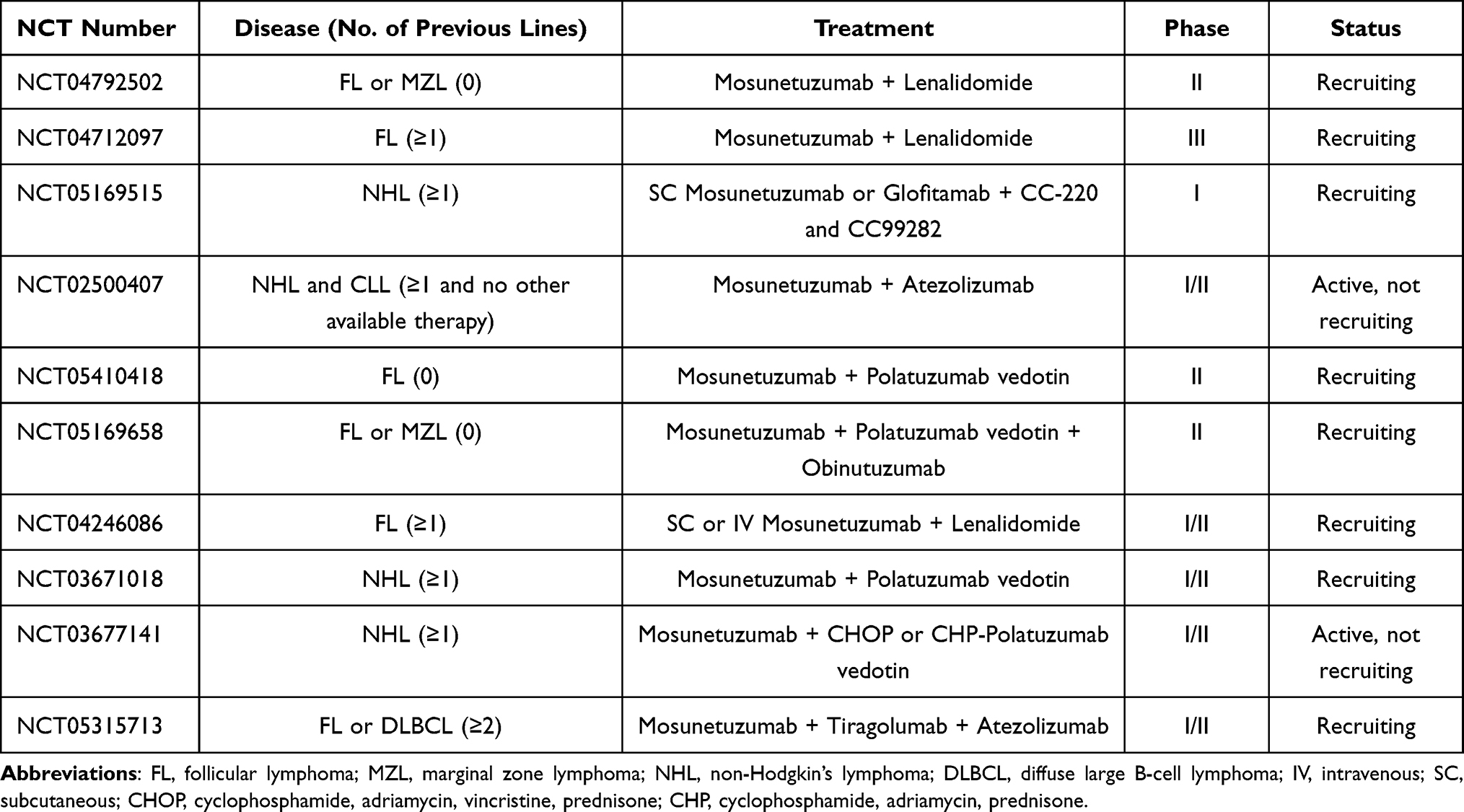 |
Table 2 Main Ongoing Trials Evaluating Mosunetuzumab in Follicular Lymphoma |
Conclusions
Patients and clinicians dealing with r/r FL were between two fires: the limited targeted options available and the logistical challenges of CAR-T. Mosunetuzumab, with its ease of administration and its manageable toxicity, has the potential to partially obviate this hiatus. While the updates from the phase II study of mosunetuzumab will certainly shed more light on its role in patients with r/r FL, many trials are ongoing and are investigating the association of this TDB with other immunomodulating or cytotoxic agents. Results of these analyses could not only reveal synergistic effect in patients with r/r FL but also possibly lead to an earlier use in the disease course. Furthermore, with a growing number of patients treated with CAR-T, more data on the efficacy of mosunetuzumab in FL in the post CAR-T setting will become available, hopefully filling what at the moment represents an unmet clinical need.
Funding
This paper was not funded.
Disclosure
M Shadman reports research funding from: Mustang Bio, BMS, Pharmacyclics, Genentech, AbbVie, TG Therapeutics, BeiGene, AstraZeneca, Genmab, MorphoSys/Incyte, Vincerx. Consulting for AbbVie, Genentech, AstraZeneca, Pharmacyclics, BeiGene, BMS, MorphoSys/Incyte, Kite, Eli Lilly, Mustang Bio, Regeneron, ADC therapeutics, Fate Therapeutics and MEI Pharma. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
References
1. Alaggio R, Amador C, Anagnostopoulos I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. 2022;36(7):1720–1748. doi:10.1038/s41375-022-01620-2
2. Cerhan JR. Epidemiology of follicular lymphoma. Hematol Oncol Clin North Am. 2020;34(4):631–646. doi:10.1016/j.hoc.2020.02.001
3. Guadagnolo BA, Li S, Neuberg D, et al. Long-term outcome and mortality trends in early-stage, grade 1–2 follicular lymphoma treated with radiation therapy. Int J Radiat Oncol Biol Phys. 2006;64(3):928–934. doi:10.1016/j.ijrobp.2005.08.010
4. Brady JL, Binkley MS, Hajj C, et al. Definitive radiotherapy for localized follicular lymphoma staged by 18F-FDG PET-CT: a collaborative study by ILROG. Blood. 2019;133(3):237–245. doi:10.1182/blood-2018-04-843540
5. Qualls D, Salles G. Prospects in the management of patients with follicular lymphoma beyond first-line therapy. Haematologica. 2022;107(1):19–34. doi:10.3324/haematol.2021.278717
6. Rivas-Delgado A, Magnano L, Moreno-Velázquez M, et al. Response duration and survival shorten after each relapse in patients with follicular lymphoma treated in the rituximab era. Br J Haematol. 2019;184(5):753–759. doi:10.1111/bjh.15708
7. Casulo C, Larson MC, Lunde JJ, et al. Treatment patterns and outcomes of patients with relapsed or refractory follicular lymphoma receiving three or more lines of systemic therapy (LEO CReWE): a multicentre cohort study. Lancet Haematol. 2022;9(4):e289–e300. doi:10.1016/S2352-3026(22)00033-3
8. Link BK, Day BM, Zhou X, et al. Second-line and subsequent therapy and outcomes for follicular lymphoma in the United States: data from the observational National LymphoCare Study. Br J Haematol. 2019;184(4):660–663. doi:10.1111/bjh.15149
9. Casulo C, Byrtek M, Dawson KL, et al. Early relapse of follicular lymphoma after rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone defines patients at high risk for death: an analysis from the national lymphocare study. JCO. 2015;33(23):2516–2522. doi:10.1200/JCO.2014.59.7534
10. Lansigan F, Barak I, Pitcher B, et al. The prognostic significance of PFS24 in follicular lymphoma following firstline immunotherapy: a combined analysis of 3 CALGB trials. Cancer Med. 2019;8(1):165–173. doi:10.1002/cam4.1918
11. Casulo C, Dixon JG, Le-Rademacher J, et al. Validation of POD24 as a robust early clinical end point of poor survival in FL from 5225 patients on 13 clinical trials. Blood. 2022;139(11):1684–1693. doi:10.1182/blood.2020010263
12. Fowler NH, Dickinson M, Dreyling M, et al. Tisagenlecleucel in adult relapsed or refractory follicular lymphoma: the Phase 2 ELARA trial. Nat Med. 2022;28(2):325–332. doi:10.1038/s41591-021-01622-0
13. Jacobson CA, Chavez JC, Sehgal AR, et al. Axicabtagene ciloleucel in relapsed or refractory indolent non-Hodgkin lymphoma (ZUMA-5): a single-arm, multicentre, phase 2 trial. Lancet Oncol. 2022;23(1):91–103. doi:10.1016/S1470-2045(21)00591-X
14. Smith SD, Reddy P, Sokolova A, et al. Eligibility for CAR T-cell therapy: an analysis of selection criteria and survival outcomes in chemorefractory DLBCL. Am J Hematol. 2019;94(4):E117–E116. doi:10.1002/ajh.25411
15. Perrone S, Lopedote P, Levis M, Di Rocco A, Smith SD. Management of relapsed or refractory large B-cell lymphoma in patients ineligible for CAR-T cell therapy. Expert Rev Hematol. 2022;15(3):215–232. doi:10.1080/17474086.2022.2044778
16. Loken MR, Shah VO, Dattilio KL, Civin CI. Flow cytometric analysis of human bone marrow. II. Normal B lymphocyte development. Blood. 1987;70(5):1316–1324. doi:10.1182/blood.V70.5.1316.1316
17. Sun LL, Ellerman D, Mathieu M, et al. Anti-CD20/CD3 T cell–dependent bispecific antibody for the treatment of B cell malignancies. Sci Transl Med. 2015;7(287):287ra70–287ra70. doi:10.1126/scitranslmed.aaa4802
18. Zhu M, Wu B, Brandl C, et al. Blinatumomab, a bispecific T-cell engager (BiTE(®)) for CD-19 targeted cancer immunotherapy: clinical pharmacology and its implications. Clin Pharmacokinet. 2016;55(10):1271–1288. doi:10.1007/s40262-016-0405-4
19. Ridgway JBB, Presta LG, Carter P. ‘Knobs-into-holes’ engineering of antibody CH3 domains for heavy chain heterodimerization. Protein Eng Design Select. 1996;9(7):617–621. doi:10.1093/protein/9.7.617
20. Spiess C, Merchant M, Huang A, et al. Bispecific antibodies with natural architecture produced by co-culture of bacteria expressing two distinct half-antibodies. Nat Biotechnol. 2013;31(8):753–758. doi:10.1038/nbt.2621
21. Ferl GZ, Reyes A, Sun LL, et al. A preclinical population pharmacokinetic model for anti-CD20/CD3 T-cell-dependent bispecific antibodies. Clin Transl Sci. 2018;11(3):296–304. doi:10.1111/cts.12535
22. Budde LE, Assouline S, Sehn LH, et al. Single-agent mosunetuzumab shows durable complete responses in patients with relapsed or refractory b-cell lymphomas: phase I dose-escalation study. J Clin Oncol. 2022;40(5):481–491. doi:10.1200/JCO.21.00931
23. Hosseini I, Gadkar K, Stefanich E, et al. Mitigating the risk of cytokine release syndrome in a Phase I trial of CD20/CD3 bispecific antibody mosunetuzumab in NHL: impact of translational system modeling. NPJ Syst Biol Appl. 2020;6(1):28. doi:10.1038/s41540-020-00145-7
24. Budde LE, Sehn LH, Matasar M, et al. Safety and efficacy of mosunetuzumab, a bispecific antibody, in patients with relapsed or refractory follicular lymphoma: a single-arm, multicentre, phase 2 study. Lancet Oncol. 2022;23(8):1055–1065. doi:10.1016/S1470-2045(22)00335-7
25. Bartlett N. Mosunetuzumab monotherapy demonstrates durable efficacy with a manageable safety profile in patients with relapsed/refractory follicular lymphoma who received ≥2 prior therapies: updated results from a pivotal phase II study. ASH; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper157691.html.
26. Lamure S, Dulery R, Delord M, et al. Abstract S09-02: high incidence of persistent COVID-19 among patients with lymphoma treated with B-cell depleting immunotherapy. Clin Cancer Res. 2021;27(6_Supplement):S09–02. doi:10.1158/1557-3265.COVID-19-21-S09-02
27. Patel NJ, D’Silva KM, Hsu TY, et al. Coronavirus disease 2019 outcomes among recipients of anti‐CD20 monoclonal antibodies for immune‐mediated diseases: a comparative cohort study. ACR Open Rheumatol. 2021;4(3):238–246. doi:10.1002/acr2.11386
28. Calderón-Parra J, Múñez-Rubio E, Fernández-Cruz A, et al. Incidence, clinical presentation, relapses and outcome of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in patients treated with anti-CD20 monoclonal antibodies. Clin Infect Dis. 2022;74(10):1786–1794. doi:10.1093/cid/ciab700
29. Kang C. Mosunetuzumab: first approval. Drugs. 2022;82(11):1229–1234. doi:10.1007/s40265-022-01749-5
30. Lee DW, Santomasso BD, Locke FL, et al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant. 2019;25(4):625–638. doi:10.1016/j.bbmt.2018.12.758
31. Flinn IW, Miller CB, Ardeshna KM, et al. DYNAMO: a Phase II study of duvelisib (IPI-145) in patients with refractory indolent non-Hodgkin lymphoma. JCO. 2019;37(11):912–922. doi:10.1200/JCO.18.00915
32. Fowler NH, Samaniego F, Jurczak W, et al. Umbralisib, a dual PI3Kδ/CK1ε inhibitor in patients with relapsed or refractory indolent lymphoma. J Clin Oncol. 2021;39(15):1609–1618. doi:10.1200/JCO.20.03433
33. Dreyling M, Santoro A, Mollica L, et al. Long-term safety and efficacy of the PI3K inhibitor copanlisib in patients with relapsed or refractory indolent lymphoma: 2-year follow-up of the CHRONOS-1 study. Am J Hematol. 2020;95(4):362–371. doi:10.1002/ajh.25711
34. Matasar MJ, Capra M, Özcan M, et al. Copanlisib plus rituximab versus placebo plus rituximab in patients with relapsed indolent non-Hodgkin lymphoma (CHRONOS-3): a double-blind, randomised, placebo-controlled, Phase 3 trial. Lancet Oncol. 2021;22(5):678–689. doi:10.1016/S1470-2045(21)00145-5
35. Leonard JP, Trneny M, Izutsu K, et al. AUGMENT: a Phase III study of lenalidomide plus rituximab versus placebo plus rituximab in relapsed or refractory indolent lymphoma. JCO. 2019;37(14):1188–1199. doi:10.1200/JCO.19.00010
36. Andorsky DJ, Coleman M, Yacoub A, et al. MAGNIFY phase IIIb interim analysis of induction R2 followed by maintenance in relapsed/refractory indolent NHL. JCO. 2020;38(15_suppl):8046. doi:10.1200/JCO.2020.38.15_suppl.8046
37. Morschhauser F, Tilly H, Chaidos A, et al. Tazemetostat for patients with relapsed or refractory follicular lymphoma: an open-label, single-arm, multicentre, phase 2 trial. Lancet Oncol. 2020;21(11):1433–1442. doi:10.1016/S1470-2045(20)30441-1
38. Batlevi CL, Salles G, Park SI, et al. Tazemetostat in combination with lenalidomide and rituximab in patients with relapsed/refractory follicular lymphoma: phase 1b results of symphony-1. Blood. 2022;140(Supplement1):2296–2298. doi:10.1182/blood-2022-166991
39. Budde E. Subcutaneous mosunetuzumab is active with a manageable safety profile in patients (pts) with relapsed/refractory (R/R) B-cell non-Hodgkin lymphomas (B-NHLs): updated results from a phase I/II study. ASH; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper157729.html.
40. Morschhauser F, Bishton M, Eyre TA, et al. Mosunetuzumab in combination with lenalidomide has a manageable safety profile and encouraging activity in patients with relapsed/refractory follicular lymphoma: initial results from a phase Ib study. Blood. 2021;138(Supplement 1):129. doi:10.1182/blood-2021-145694
41. Nastoupil LJ, Morschhauser F, Scholz CW, et al. CELESTIMO: a phase III trial evaluating the efficacy and safety of mosunetuzumab plus lenalidomide versus rituximab plus lenalidomide in patients with relapsed or refractory follicular lymphoma who have received ≥ 1 line of systemic therapy. JCO. 2022;40(16_suppl):TPS7588–TPS7588. doi:10.1200/JCO.2022.40.16_suppl.TPS7588
42. Tilly H, Morschhauser F, Sehn LH, et al. Polatuzumab vedotin in previously untreated diffuse large B-cell lymphoma. N Engl J Med. 2022;386(4):351–363. doi:10.1056/NEJMoa2115304
43. Morschhauser F, Flinn IW, Advani R, et al. Polatuzumab vedotin or pinatuzumab vedotin plus rituximab in patients with relapsed or refractory non-Hodgkin lymphoma: final results from a phase 2 randomised study (ROMULUS). Lancet Haematol. 2019;6(5):e254–e265. doi:10.1016/S2352-3026(19)30026-2
44. Osada T, Patel SP, Hammond SA, Osada K, Morse MA, Lyerly HK. CEA/CD3-bispecific T cell-engaging (BiTE) antibody-mediated T lymphocyte cytotoxicity maximized by inhibition of both PD1 and PD-L1. Cancer Immunol Immunother. 2015;64(6):677–688. doi:10.1007/s00262-015-1671-y
45. Krupka C, Kufer P, Kischel R, et al. Blockade of the PD-1/PD-L1 axis augments lysis of AML cells by the CD33/CD3 BiTE antibody construct AMG 330: reversing a T-cell-induced immune escape mechanism. Leukemia. 2016;30(2):484–491. doi:10.1038/leu.2015.214
46. Chang CH, Wang Y, Li R, et al. Combination therapy with bispecific antibodies and PD-1 blockade enhances the antitumor potency of T cells. Cancer Res. 2017;77(19):5384–5394. doi:10.1158/0008-5472.CAN-16-3431
47. Sam J, Colombetti S, Fauti T, et al. Combination of T-cell bispecific antibodies with PD-L1 checkpoint inhibition elicits superior anti-tumor activity. Front Oncol. 2020;10. doi:10.3389/fonc.2020.575737
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.