")
Back to Journals » Vascular Health and Risk Management » Volume 16
Systemic Arterial Stiffness in New Diagnosed Idiopathic Pulmonary Arterial Hypertension Patients
Authors Radchenko GD , Zhyvylo IO, Titov EY, Sirenko YM
Received 6 September 2019
Accepted for publication 15 November 2019
Published 16 January 2020 Volume 2020:16 Pages 29—39
DOI https://doi.org/10.2147/VHRM.S230041
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Pietro Scicchitano
GD Radchenko, 1 IO Zhyvylo, 1 EY Titov, 2 Yuriy M Sirenko 1
1Secondary Hypertension Department, State Institution “National Scientific Center “Institute of Cardiology Named After acad.M.D.Strazhesko” of Ukrainian National Academy of Medical Science, Kyiv, Ukraine; 2Non-Coronary Heart Disease Department, State Institution “National Scientific Center “Institute of Cardiology Named After acad.M.D.Strazhesko” of Ukrainian National Academy of Medical Science, Kyiv, Ukraine
Correspondence: GD Radchenko
Department of Secondary Hypertension, State Institute “National Scientific Center “Institute of Cardiology n.a.acad. M.D. Strazhesko” of National Academy of Medical Science, Kyiv, Ukraine
Tel +38-0667128405
Email [email protected]
Objective: We suggested: 1) patients with idiopathic pulmonary hypertension (IPAH) have active factors which could damage not only the pulmonary but systemic arteries too as in arterial hypertensive patients; 2) if these changes were present, they might correlate with other parameters influencing on the prognosis. This study is the first attempt to use cardio-ankle vascular index (CAVI) for the evaluation of systemic arterial stiffness in patients with IPAH.
Methods: A total of 112 patients were included in the study: group 1 consisted of 45 patients with new diagnosed IPAH, group 2 included 32 patients with arterial hypertension, and in the control group were 35 healthy persons adjusted by age. Right heart catheterization, ECG, a 6-minute walk test (6MWT), echocardiography, blood pressure (BP) measurement and ambulatory BP monitoring, pulse wave elastic artery stiffness (PWVe; segment carotid-femoral arteries) and muscular artery stiffness (PWVm; segment carotid-radial arteries), CAVI, and N-terminal pro-B-type natriuretic peptide (NT-proBNP) level were provided. The Spearman correlation, a linear regression and multivariable binary logistic analysis were performed to indicate the predictors associated with PWV and CAVI.
Results: The groups were adjusted for principal characteristics influenced on arterial stiffness. IPAH patients had significantly (P< 0.001 for all) shorter 6MWT distance and higher Borg dyspnea score than the patients with arterial hypertension (systolic/diastolic BP = 146.1± 10.7/94.2± 9.8 mmHg) and the control group = 330.2± 14.6 vs 523.8± 35.3 and 560.9± 30.2 m respectively and 6.2± 1.8 vs 1.2± 2.1 and 0.9± 2.8 points. The PWVm and PWVe were the highest in hypertensive patients (10.3± 1.5 and 11.42± 1.70 m/s). The control group and IPAH did not have significant differences in aorta BP, but PWVm/PWVe values were significantly (P< 0.003/0.008) higher in IPAH patients than in the control group (8.1± 1.9/8.49± 1.92 vs 6.63± 1.34/7.29± 0.87 m/s). The CAVIs on both sides were significantly lower in the healthy subjects (5.91± 0.99/5.98± 0.87 right/left side). Patients with IPAH did not differ from the arterial hypertension patients by CAVIs in comparison with the control group (7.40± 1.32/7.22± 1.32 vs 7.19± 0.78/7.2± 1.1 PWVe) did not correlate with any parameters except uric acid. PWVm correlated with uric acid (r=0.58, P< 0.001), NT-proBNP (r=0.33, P=0.03) and male gender (r=0.37, P=0.013) at Spearman analysis, but not at multifactorial linear regression analysis. The CAVI correlated with age and parameters characterized functional capacity (6MWT distance) and right ventricle function (NT-proBNP, TAPSE) at Spearman analysis and with age and TAPSE at multifactorial linear regression analysis. At binary logistic regression analysis CAVI > 8.0 at right and/or left side had a correlation with age, 6MWT distance, TAPSE, but an independent correlation was only with age (β=1.104, P=0.008, CI 1.026– 1.189) and TAPSE (β=0.66, P=0.016, CI 0.474– 0.925).
Conclusion: In spite of equal and at normal range BP level, the age-adjusted patients with IPAH had significantly stiffer arteries than the healthy persons and they were comparable with the arterial hypertensive patients. Arterial stiffness evaluated by CAVI correlated with age and TAPSE in IPAH patients. Based on our results it is impossible to conclude the pathogenesis of arterial stiffening in IPAH patients, but the discovered changes and correlations suggest new directions for further studies, including pathogenesis and prognosis researches.
Keywords: idiopathic pulmonary arterial hypertension, systemic arterial stiffness, functional capacity, pulse wave velocity, cardio-ankle vascular index
Introduction
Idiopathic pulmonary arterial hypertension (IPAH) is one of the rare and poor prognostic diseases characterized by progressive pulmonary artery damage, increasing of pulmonary vascular resistance and pulmonary blood pressure, high level of patient’s disability and death. The etiology of this disease is unknown and prevalence ranges from 6 to 9 in a million adults.1–4 Female/male incidence ratio is 2:1 and females are significantly older.5
There are a lot of studies devoted to evaluation of the IPAH prevalence and factors associated with poor prognosis. Male gender, high right atrium pressure, low cardiac output, poor functional capacity (low WHO functional class, short 6-minute walking test (6MWT) distance, high level of natriuretic peptides) are associated with IPAH mortality.2,6 The search for new markers of poor prognosis is a perspective direction for new investigations in the field of pulmonary hypertension.
IPAH is characterized by pulmonary artery vascular damage: smooth muscle hypertrophy, vasoconstriction, plexiform remodeling, local hypercoagulability and endothelial injury. These changes are supported by inflammatory cytokines, disorders of NO synthesis and destruction.2,4,7–14
Soon et al15 demonstrated increased levels of tumor necrosis factor-α, interferon-γ and some interleukins in patients with IPAH and familial PAH compared to the control group; and the elevated level of interleukin-6 was associated with worse survival. The role of inflammation in PAH was evaluated in some other studies.16–18 Cracowski et al17 and Heresi et al18 confirmed the increased level of cytokines in PAH patients and their predictive role in prognosis. It is unclear if the inflammation is the cause of the disease or a consequence, but some publications have indicated pathological descriptions highlighting the degree of inflammation and lymphoid neogenesis in the vascular remodelling process.19,20
In some experimental researches the authors described how inflammation plays a role in the development of systemic hypertension by inducing vascular damage, renal damage, and/or abnormal central neural regulation.21–24 The Japanese observational study25 reported an increased risk of arterial hypertension development in 3,274 middle‐aged men with a high level of C reactive protein, which continued for 9 years. This risk was realized through increasing of arterial stiffness. The main conclusion of this study was that systemic inflammation may play a role in the pathogenesis of hypertension by the progression of arterial stiffness. Association of arterial stiffness with inflammation has also been highlighted in other works.26–28
Thus, the inflammation process is activated both in IPAH patients and in the systemic hypertensive patients. It is reasonable to suggest that activated cytokines and other proinflammatory substances in IPAH could damage not only the pulmonary arteries but also the systemic arteries, leading to increasing systemic arterial stiffness. In IPAH patients, the left ventricle suffers due to increased right ventricular pressure and worsening of the systemic arterial stiffness may lead to increasing left ventricular afterload and to additional worsening of its functional capacity. That is why systemic artery stiffness may be a marker of disease severity and response to treatment.
The modern pharmacological treatment of IPAH includes drugs which have the following mechanism of action: improving endothelial function in pulmonary arteries. Initially some pulmonary hypertension remedies were proposed for arterial hypertension or coronary heart disease treatment because of their influence on the systemic arteries. Later their much more prominent effects on pulmonary arteries were found. Although antihypertensive therapy did not demonstrate the proven positive impact in pulmonary hypertensive patients, except for calcium channel blockers in vasoreactive patients, it could improve the systemic arterial stiffness.
In the literature we were able to find some observations devoted to evaluation of the pulmonary artery resistance,11,12,29–32 but only a few of them studied the systemic arterial stiffness.33–35 Before planning this study we hypothesized the following: 1) patients with IPAH have active factors in circulation which could damage not only the pulmonary but systemic arteries too as in arterial hypertensive patients; 2) if these changes are present, they might correlate with other parameters influencing on the prognosis. That is why we evaluated systemic arterial stiffness measured as carotid-femoral pulse wave velocity (PWVe), carotid-radial PWV (PWVm) and cardio-ankle vascular index (CAVI) in IPAH patients and compared the results with those in the matched arterial hypertensive patients and the healthy people. Also we assessed the association of arterial stiffness parameters with the main factors of poor prognosis.
PWVe is accepted as the gold standard for evaluation of aorta arterial stiffness and could be taken into consideration for the cardiovascular risk stratification (target organ damage) in arterial hypertensive patients;4 but it depends highly on the blood pressure (BP) level, because blood pressure exerts on the arterial wall. It has been demonstrated that the measured stiffness was increased with a rise in loading pressure without any structural change.36 Besides this, PWVe depends on other factors like breathing movements (lower during inspiration than during expiration).37 The CAVI is a less BP-dependent characteristic of arterial stiffness.37–41 This study is the first attempt to use CAVI for evaluation of the systemic arterial stiffness in patients with IPAH.
Patients and Methods
Patients
In the Ukrainian referral center 112 patients were included in the study: group 1 consisted of 45 patients with newly diagnosed IPAH, group 2 included 32 patients with arterial hypertension, and in the control group were 35 healthy persons adjusted by age. Pulmonary hypertension was confirmed by right heart catheterization (RHC), mean pulmonary arterial pressure (mPAP) ≥ 25 mm Hg, pulmonary vascular resistance (PVR) ≥ 240 dynes*s/cm5 and pulmonary artery wedge pressure (PAWP) ≤ 15 mmHg at rest.4 The first RHC was performed in our referral center within the previous 12 months. The diagnosis of IPAH was established after exclusion of all other reasons for pulmonary hypertension, except heritable pulmonary hypertension (in Ukraine it is not possible to provide genetic analysis for these kinds of patients). We used the local standard examination protocol based on ESC-2015 guidelines on diagnosis and treatment of pulmonary hypertension.4 Considering specific age and gender characteristics of the patients in the IPAH group, we recruited patients adjusted for demographic features in the arterial hypertension group from our department database. The sample selection was done automatically after implementation of filter criteria: age < 65 years, newly diagnosed arterial hypertension, not taking antihypertensive treatment in previous month, and presence of arterial stiffness parameters. Patients with diseases having an influence on arterial stiffness (diabetes mellitus, chronic kidney disease, ischemic heart disease, and peripheral vascular disease, history of stroke or systemic rheumatic diseases) were excluded. The control group included age-adjusted healthy persons who were examined at our department but had no diseases assessed as influencing on arterial stiffness were found.
All patients were included in the study after signing an informed consent form for personal data process. The protocol of our study was approved by the local ethics committee of the State Institution “National Scientific Center “Institute of Cardiology named after academician M.D.Strazhesko” of Ukrainian National Academy of Medical Science (Kyiv, Ukraine). The study was based on the tenets of the Declaration of Helsinki.
Methods
Systolic (SBP) and diastolic (DBP) arterial blood pressure (BP) were measured three times by Omron M-10 (Omron Healthcare Co., Ltd., Kyoto, Japan) in a sitting position after 10 minutes of rest in accordance with ESH-2018 guidelines.42 The mean of the three measurements was included in the database. Heart rate (HR) was evaluated after the second BP measurement. Body mass and height were evaluated with SECA 220 (Seca GmbH & Co, Hamburg, Germany). For exclusion or confirmation of the systemic arterial hypertension, ambulatory blood pressure monitoring (ABPM) was done by using device ABPM-04 (Meditech, Budapest, Hungary).
A 6-minute walking test (6MWT) was conducted twice in accordance with the American Thoracic Society guidelines43,44 and the best result was included in the database. HR, BP, oxygen saturation (SaO2) and dyspnea score (Borg Dyspnoea Score) were registered before and just after the test.
Transthoracic echocardiography (EchoCG) was conducted by the same specialists using standard measurements (Artida, Toshiba, Tokio, Japan) in accordance with joint American Society of Echocardiography and European Association of Cardiovascular Imaging recommendations.45 The evaluation process included both ventricle and atrium size, ejection fraction (LVEF) and diastolic function of left ventricle, stroke volume, pulmonary velocity values, tricuspid annular plane systolic excursion (TAPSE), tricuspid regurgitation velocity, calculated systolic pulmonary BP (SPBP), and dimensions of the inferior vena cava.
In the systemic hypertensive patients and in the control group the systemic vascular resistance (SVR) was calculated as:

Mean arterial pressure was calculated by using the formula: [(systolic BP)/3 + 2 × (diastolic BP)/3]. Cardiac output was calculated as stroke volume * heart rate. SVR for IPAH patients was calculated after direct hemodynamic measurements of cardiac output and mean right atrium pressure during RHC.
PWV and central BP were assessed by using SphygmoCor (AtCor Medical Pty Ltd., Sydney, Australia). Sensors were placed at the right common carotid artery, right femoral artery and right radial artery. The impulses were enhanced to draw out a curve of the pulse wave of the carotid artery and the femoral artery (or radial artery) after the detection, registration, and computer processing. The distance between sensors was measured by a centimeter ribbon. The time of delay between the onset of the two pulse waves was automatically measured and the PWV was calculated (the distance divided by the delay time). For the evaluation of the elastic artery stiffness (PWVe), a segment from the carotid artery to the femoral artery was used, and for the assessment of muscular artery stiffness (PWVm), a segment from the carotid artery to the radial artery was used. The normal value of the PWVe is considered < 10 m/s.42 The aorta blood pressure and augmentation index (Aix) adjusted for HR 75 per 1 minute (Aix@75) measurements were performed with a Sphygmocor-PVx device too.
CAVI was measured by Sphygmomanometer and Sphygmograph VaSera-1500N (Fukuda, Tokio, Japan) by a standard method.39 CAVI was calculated after acquiring the distance from the level of the aortic valve (brachial level) to the measuring point (the ankle) and the time delay between the closing of the aortic valve to the detected change in arterial pressure wave at the set point.46 Information for CAVI computation includes PWV, SBP and DBP as well as arterial pulse waveforms. It could be obtained through the electrocardiogram, cardiac phonogram, and the pressure cuffs on the testing subject at the reference points. According to the manufacturer’s instructions, a CAVI < 8.0 is supposed to be normal, 8.0–9.0 = “borderline”, > 9.0 is considered as suspected arteriosclerosis.39,47 The CAVI assessments were provided before the first RHC was done.
During the RHC we evaluated the right atrial, the right ventricular, the pulmonary artery and the wedge pressures. The thermodilution method was used to determine the cardiac output and calculate the stroke volume, the cardiac index (CI), and the indexed pulmonary vascular resistance (PVR). In all pulmonary hypertensive patients the vasoreactivity test with inhaled iloprost was conducted in accordance with ESC-2015 guidelines.4 Patients with positive tests were excluded from the study.
The biochemical analyses were provided by an automatic photometer (Cormay Livia Chemistry Analyzer, Lublin, Poland). The kidney function was estimated according to the results of the glomerular filtration rate (GFR) calculated by the EPI formula from serum creatinine concentration. N-terminal pro-B-type natriuretic peptide (NT-proBNP) level was also assessed by electrochemiluminescence immunoassay (ECLIA) method (NT pro-BNP, Roche, Germany) with a Roche modular analytics E170 immunoassay analyzer.
The baseline study procedures were conducted in naïve patients without therapy. Further, IPAH patients were prescribed sildenafil or inhalation iloprost or their combination (the only specific drugs available in Ukraine at the time of study). The patients with arterial hypertension started to take antihypertensive drugs according to ESC/ESH-2018 guidelines.
Statistical Methods
Variables are presented as mean ± standard deviation (SD) or as a percentage. All statistical calculations were performed using the Statistical Package for Social Sciences version 13.0 (SPSS Inc, Chicago, IL, USA). The Student’s t-test of mean values was used for comparisons between the two groups and chi-square analysis was provided for categorical variables. The Spearman correlation coefficients were calculated between the systemic artery stiffness parameters and the main IPAH patient characteristics. Significant variables on the Spearman correlation were used in multivariable linear regression analysis (Backward stepwise method) for the evaluation of independent predictors correlated with PWVe, PWVm and CAVI. The univariate and multivariable binary logistic analyses were performed to indicate the parameters associated with abnormal CAVI level (> 8). All the tests were two-tailed. The data were considered significant at p < 0.05.
Results
Baseline patient characteristics are presented in Table 1. The groups were adjusted by the main characteristics influencing on arterial stiffness: age, gender, body mass index and serum glucose level. The prevalence of smoking history did not differ significantly between the groups. In comparison with the IPAH and control groups the patients with arterial hypertension had a higher level of total cholesterol, but its mean value was within the normal range. The office SBP, DBP and pulse blood pressure (PBP) levels were significantly higher in the arterial hypertensive patients, than in IPAH and the control group. The HR was significantly higher in IPAH patients than in the hypertensive and control group patients. The PBP level was significantly lower in IPAH patients than in the healthy persons. The GFR-EPI was the highest in healthy adults. In the IPAH group 4 (8.9%) patients had mPAP 25–44 mmHg, 21 (46.7%) had mPAP 45–64 mmHg, and 20 (44.4%) had mPAP ≥ 65 mmHg. Fifteen (33.3%) IPAH patients presented with WHO functional class I–II, 26 (57.8%) with WHO functional class III and 4 (8.9%) with WHO functional class IV. IPAH patients had significantly shorter 6MWT distance and higher Borg dyspnea scores than the patients with arterial hypertension and the control group. Also they had lower TAPSE and a higher eccentricity index. SVR in IPAH patients was significantly lower than in the hypertensive patients, but significantly higher than in the control group.
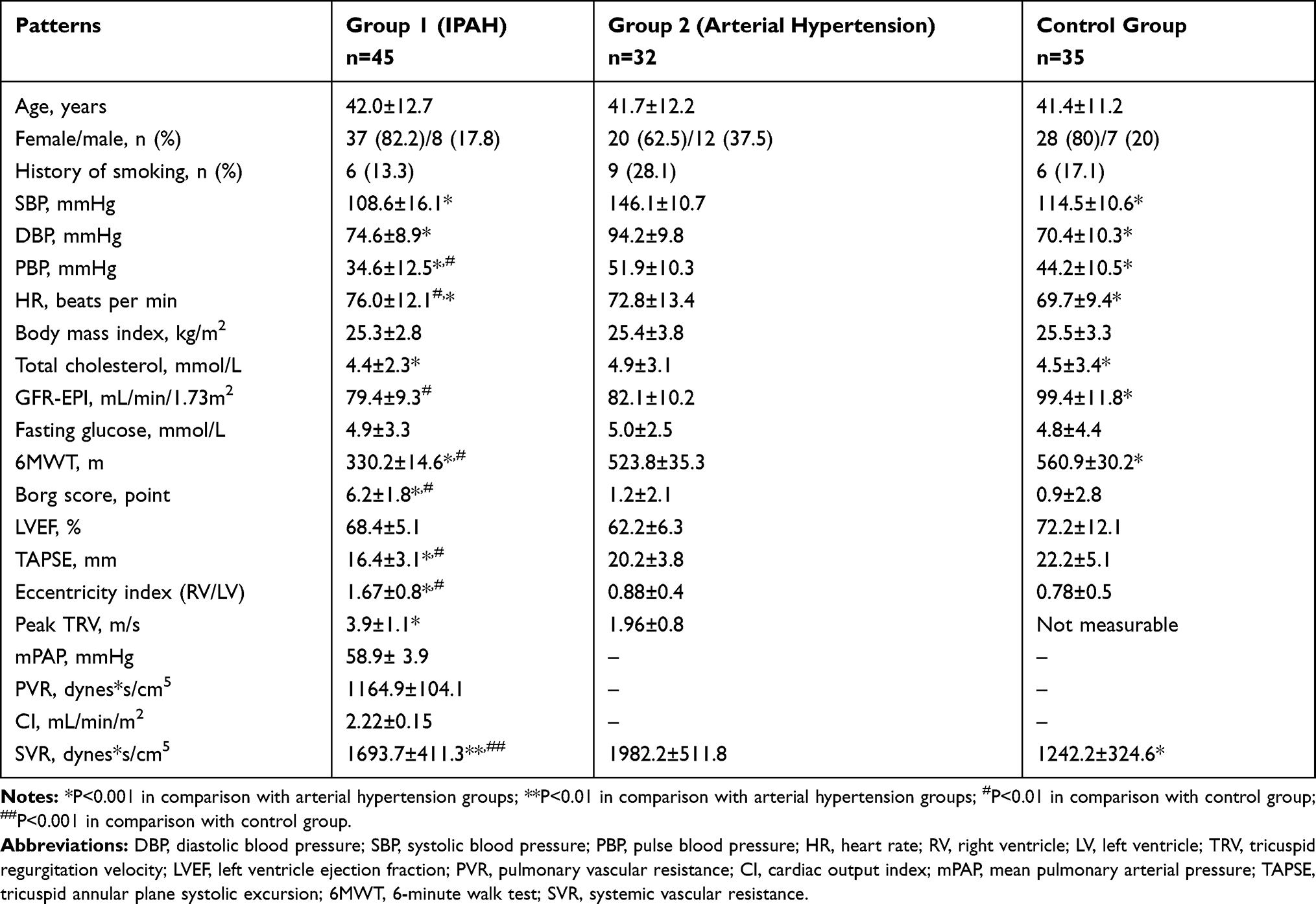 |
Table 1 Patients' Characteristics in Groups (M±SD), n (%) |
Aortic SBP and arterial stiffness characteristics in the groups are presented in Table 2. As it was expected the central blood pressure, AIx, PWVm and PWVe were the highest in the hypertensive patients. After adjusting for HR groups did not differ by AIx@75. The control group and IPAH did not have significant differences in mean aorta SBP, AIx and AIx@75, but PWVm and PWVe values were significantly higher in IPAH patients, than in the control group. The CAVIs on both sides were significantly lower in the healthy subjects. Patients with IPAH did not differ from the arterial hypertension patients by CAVIs: 40% (n=18) of IPAH patients had CAVI > 8.0 on the right and/or left side.
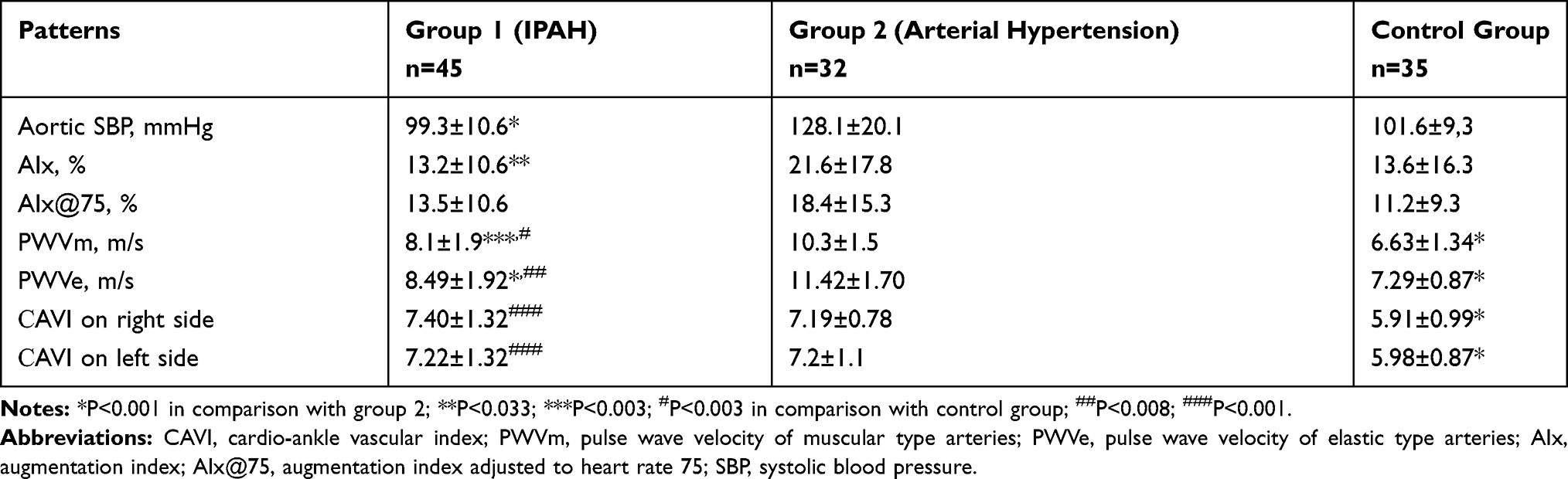 |
Table 2 Central Blood Pressure and Arterial Stiffness Characteristics in Groups (M±SD) |
Thus, in spite of the equal and at normal range blood pressure level, the age-adjusted patients with pulmonary hypertension had significantly stiffer arteries than healthy persons and they were comparable with the arterial hypertensive patients by CAVI.
In the group of IPAH patients we provided the correlation analysis between arterial stiffness and other possible prognostic parameters. Results are presented in Table 3. PWVe did not correlate with any parameters except uric acid. The patient functional state, biomarker level, EchoCG, and RHC values did not have associations with aorta stiffness. PWVm correlated with uric acid (r=0.58, P<0.001), NT-proBNP (r=0.33, P=0.03) and male gender (r=0.37, P=0.013) at Spearman analysis, but after the conducted multifactorial linear regression analysis only an association with uric acid preserved significance. The CAVI correlated with age and parameters characterizing of functional capacity (6MWT distance) and right ventricle function (NT-proBNP, TAPSE) at Spearman analysis and with age and TAPSE at multifactorial linear regression analysis. We did not find significant correlations between SVR, PVR and CAVI. Only for SVR and PWVm was the correlation coefficient 0.22, but P=0.07.
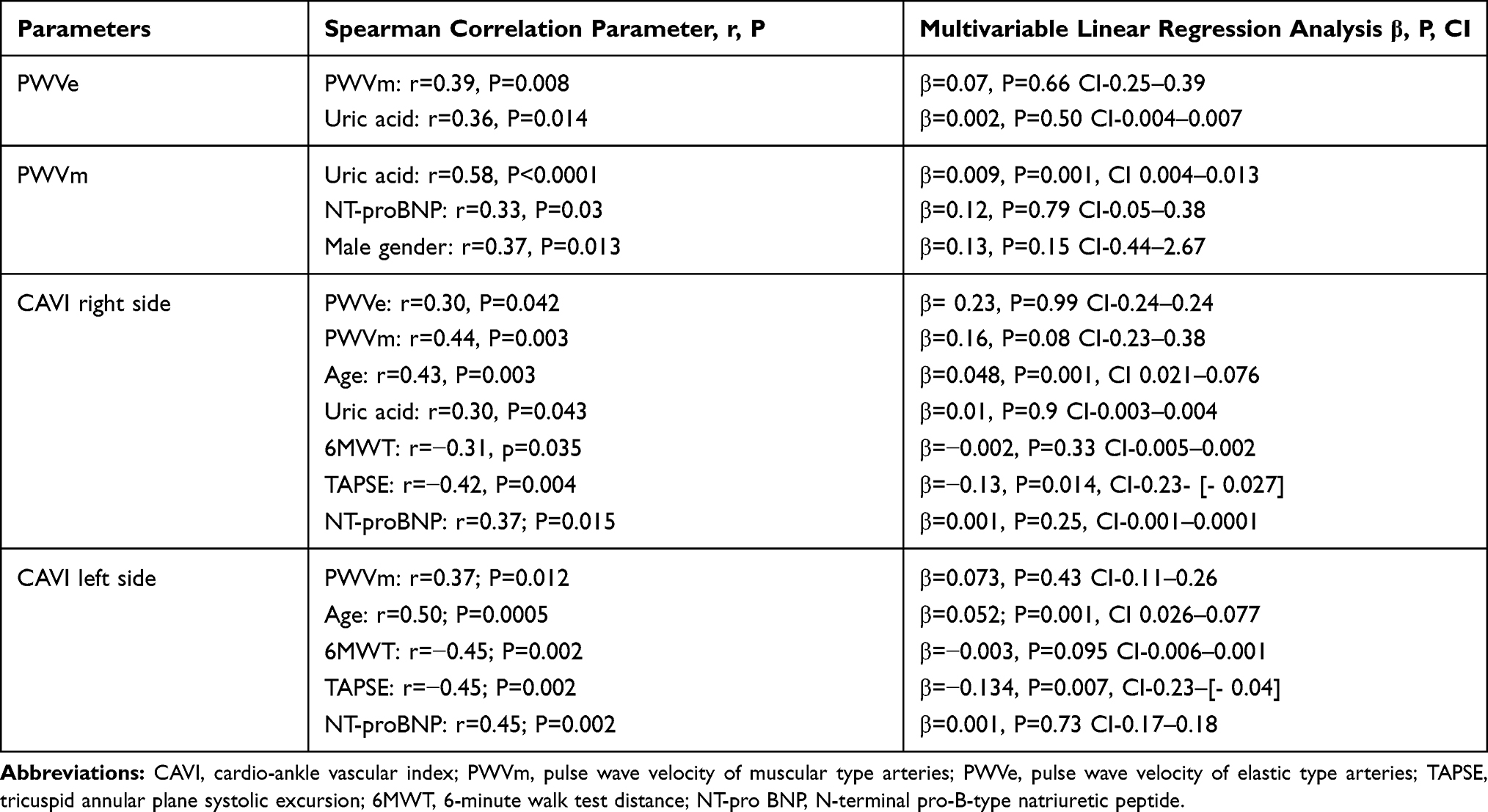 |
Table 3 Significant Correlation Between Arterial Stiffness and Other Parameters in Idiopathic Pulmonary Arterial Hypertension Patients |
We evaluated the association between abnormal values of CAVI (> 8.0) on the right and/or left side and other parameters in patients with IPAH (Table 4) by the binary logistic regression analysis. We found the same associations: CAVI > 8.0 with age, 6MWT distance, TAPSE, but independent correlations were only with age (β=1.104, P=0.008, CI 1.026–1.189) and TAPSE (β=0.66, P=0.016, CI 0.474–0.925).
 |
Table 4 Parameters Correlated Significantly with CAVI > 8.0 (Binary Logistic Analysis) |
Discussion
Arterial stiffness is a well-known risk factor for cardiovascular event development and the secondary target point for pharmacological treatment. In the meta-analysis of Vlachopoulos et al48 it was demonstrated that a 1 m/s rise of PWV value increases cardiovascular risk by more than 10%. The predictive role of PWV has been confirmed in patients with arterial hypertension, diabetes mellitus, chronic kidney diseases, coronary heart diseases and in the general population.49–57 Kaess et al58 presented the very interesting and convincing data about a causal role of arterial stiffness in the development of arterial hypertension: the higher level of PWV preceded and correlated with an increased risk of hypertension.
Artery endothelial dysfunction is one of the main factors associated with pulmonary hypertension development4,10,14–16,31 as well as systemic hypertension development.24–28,59 And it is reasonable to assume that patients with both diseases could have changes in the systemic and pulmonary artery circulation systems. But the degree of damages in different circulation systems might be different in dependency of the disease: more in systemic circulation at arterial hypertension or more in pulmonary circulation at IPAH. It was confirmed by our study in which the patients with IPAH had significantly higher PWVe and PWVm than in healthy persons, but lower than in the arterial hypertension patients, and this was confirmed by other studies too. Chamorro et al34 demonstrated that the patients with pulmonary arterial hypertension had reduced flow-mediated dilation of the brachial artery (10.6±3.9 and 7.5±6.3, respectively; p< 0.05) and higher PWVe (8.4±2.5 and 7.3 ± 1.6 m/s, respectively; p < 0.05) in comparison with the matched health subjects. The first parameter reflects endothelial dysfunction, the other one reflects systemic arterial stiffness. In our study, mean PWVe values were very similar to those in Chamorro et al's study for IPAH patients (8.49±1.92 m/s) and healthy adults (7.29±0.87 m/s). Sznajder et al33 evaluated systemic arterial stiffness in chronic thromboembolic pulmonary hypertension (CTEPH) and the control group patients were adjusted by age, gender, and concomitant diseases. They found significantly higher levels of PWVe in CTEPH patients (10.3 ± 2.5 vs 9 ± 1.3 m/s, p < 0.05). The mean PWVe value in CTEPH patients was higher than in our IPAH patients that could be explained by more advanced age in CTEPH patients (69 ± 10 vs 42.0±1.9 years old).
We used not only PWV but also CAVI for the evaluation of artery stiffness and found that the mean CAVI values in IPAH patients did not differ significantly from those in the systemic hypertensive patients, in spite of our expectations of getting higher values for the systemic hypertension patients. It could be explained by the fact that CAVI is a less blood pressure dependent marker of arterial stiffness than PWVe or PWVm.40,41,60 The formula for its calculation is:
CAVI = a[(2ρ/ΔP) ⋅ In(SBP/DBP) ⋅ PWV2] + b,
where a and b are scale conversion constants, PWV = pulse wave velocity from valve orifice to ankle, SBP = systolic blood pressure; DBP = diastolic blood pressure; ΔP = change in blood pressure; ρ = blood density.38 Blood pressure is measured in a supine position automatically. This formula helps to minimize the influence of the “functional” component of arterial stiffness, when blood extends on the arterial wall at high pressure. Bergel reported that the measured stiffness could increase with the increment of loading pressure without any structural change.36 That is why IPAH and the systemic hypertension patients differed by PWVm and PWVe, on which higher blood pressure could influence. The real arterial stiffness (structure) assessed by CAVIs was similar in both groups.
It should be taken into consideration that our systemic arterial hypertensive patients were young and with just newly diagnosed disease. The deep structural changes were less prominent and comparable with IPAH patients in which disease was newly diagnosed too. We could assume in future that the long lasting arterial hypertension will lead to more advanced systemic arterial stiffness worsening. But at the beginning of their disease the patients with systemic and pulmonary hypertension have the same artery structure changes that could reflect the similar pathogenic mechanisms.
In our study, PWVe did not correlate with parameters of IPAH, but only with PWVm and uric acid level at Spearman analysis, but it was not significant at the multivariable linear regression analysis. PWVm correlated significantly with the uric acid level, NT-proBNP and male gender at Spearman analysis and only with the uric acid level at multifactorial linear regression analysis. It contradicts the data from other studies. Chamorro et al34 demonstrated that the flow-mediated dilation was not associated with pulmonary hypertension severity, while PWVe correlated with DLCO (r=−0.27; p<0.05), PaO2 (r=−0.41; p<0.01), the 6MWT distance (r=−0.34; p<0.05) and functional class. Thus, the authors concluded that the patients with pulmonary arterial hypertension had altered vascular function in the systemic arteries and, considering the relationship between PWV and pulmonary hypertension severity, systemic arterial stiffness might serve as a marker of the disease severity and response to a treatment. Sznajder et al33 found the elevated PWVe was associated with older age, higher pulmonary vascular resistance and lower oxygen saturation in CTEPH.
We did not find correlations between SVR, PVR and parameters of arterial stiffness (these data are present in the Supplementary Table), there was just a tendency towards an association between SVR and PWVm (r=0.22, P=0.07). But the patients with IPAH had a significantly higher level of SVR than the healthy persons. That could be explained by an activation of the sympathetic system as the answer to left ventricular stroke volume decreasing in IPAH patients. Sympathetic activity may lead to peripheral vascular constriction and centralization of the circulation. This constriction could be associated with increasing SVR. Some recent studies demonstrated positive relations between SVR and PWVe,61,62 but we did not find any studies assessing correlation between CAVI and SVR, especially in the pulmonary hypertensive patients. In some studies the relation between SVR and PWVe was weak and more prominent for AIx.63,64 They concluded that SVR and PWVe could reflect the relationship between distal and proximal parts of the arterial tree. That is why in our study we did not find any significant correlation between SVR and the aorta stiffness parameters (PWVe, CAVI), but there was a tendency towards an association with the distal artery stiffness parameter (PWVm).
Independent correlations of PWVe and PWVm with uric acid were demonstrated in the Framingham Heart Study for the younger Caucasian population.65 The authors explained this by the proliferative and proinflammatory actions of uric acid through inducing monocyte chemoattractant protein-1 and cyclooxygenase-266,67 and increasing tumor necrosis factor-α production.68 But in the Framingham Heart Study, PWVe was associated also with age, history of hypertension, glucose level, blood pressure level, male gender that was not confirmed in our IPAH population and, partly, could be explained by the smaller size of our group (45 vs 4257 persons).
CAVI, unlike PWVe and PWVm, correlated with age, as was expected, and some specific for IPAH population parameters: 6MWT distance, TAPSE and NT-proBNP. It also had an association with PWVe and, especially, with PWVm. PWVm and CAVI are both dependent on smooth muscle tone.60,69 Multivariable linear regression and binary logistic analysis demonstrated independent correlation only between age, TAPSE value and CAVI. We could not find any other studies in which CAVI was used for evaluation of arterial stiffness in IPAH patients. That is why we do not have the possibility to compare our data with other author findings. It is easy to explain an association between CAVI and age, however it is hard to interpret relations between TAPSE and CAVI. TAPSE is a parameter of the global right ventricle function and characterized by the apex-to-base shortening.70,71 TAPSE correlated with the right ventricle ejection fraction and prognosis in the pulmonary hypertension patients.72,73 Association of TAPSE and CAVI might reflect two parallel processes in IPAH patients: worsening of arterial stiffness and right ventricle function. Both are connected with structural changes including under proinflammation cytokine influence. The causal relations are hard to explain. We need to provide more studies with a larger IPAH population and prospective evaluation of prognostic significance of the arterial stiffness parameters.
Limitations of the Study
This is just one center cross-sectional study which included a relatively small group of patients with newly diagnosed IPAH. We did not analyze the time from the first presentation of the symptoms, but in our country where there are some obstacles in the diagnostic process (sometimes 2–3 years passed till a patient would be referred to a specialized center); all of that could be much different for each patient and could have influence on the arterial stiffness worsening level. However, we compare IPAH patient data with the newly diagnosed systemic hypertensive patients, which also could have different times from the disease start. And the fact that these two different populations of the patients had comparable systemic artery stiffness is noteworthy. The observations were not blinded, but for arterial stiffness evaluation the semi-automatic devices were used and the influence of the investigator seemed to be negligible. Based on our results it is impossible to conclude on the pathogenesis of arterial stiffening in IPAH patients, but the discovered changes and correlations suggest the new directions for further studies, including pathogenesis and prognosis researches.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173(9):1023–1030. doi:10.1164/rccm.200510-1668OC
2. Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122(2):156–163. doi:10.1161/CIRCULATIONAHA.109.911818
3. Farber HW, Loscalzo J. Pulmonary arterial hypertension. N Engl J Med. 2004;351:1655–1665. doi:10.1056/NEJMra035488
4. Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension: the Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. doi:10.1093/eurheartj/ehv317
5. Peacock AJ, Murphy NF, McMurray JJ, Caballero L, Stewart S. An epidemiological study of pulmonary arterial hypertension. Eur Respir J. 2007;30(1):104–109. doi:10.1183/09031936.00092306
6. Miyamoto S, Nagaya N, Satoh T, et al. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension: comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2000;161:487–492. doi:10.1164/ajrccm.161.2.9906015
7. Versari D, Daghini E, Virdis A, et al. Endothelium-dependent contractions and endothelial dysfunction in human hypertension. Br J Pharmacol. 2009;157:527–536. doi:10.1111/j.1476-5381.2009.00240.x
8. Bradley AM, Leopold JA. Emerging concepts in the molecular basis of pulmonary arterial hypertension: part II: neurohormonal signaling contributes to the pulmonary vascular and right ventricular pathophenotype of pulmonary arterial hypertension. Circulation. 2015;131:2079–2091. doi:10.1161/CIRCULATIONAHA.114.006980
9. Dzau V. The cardiovascular continuum and renin-angiotensin-aldosterone system blockade. J Hypertens. 2005;23(1):9–17. doi:10.1097/01.hjh.0000165623.72310.dd
10. Thenappan T, Ormiston M, Ryan J, Archer S. Pulmonary arterial hypertension: pathogenesis and clinical management. BMJ. 2018;360:5492. doi:10.1136/bmj.j5492
11. Sanz J, Kariisa M, Dellegrottaglie S, et al. Evaluation of pulmonary artery stiffness in pulmonary hypertension with cardiac magnetic resonance. JACC Cardiovasc Imaging. 2009;2(3):286–295. doi:10.1016/j.jcmg.2008.08.007
12. Sun W, Chan SY. Pulmonary arterial stiffness: an early and pervasive driver of pulmonary arterial hypertension. Front Med. 2018;5:204. doi:10.3389/fmed.2018.00204
13. Hassoun P. Inflammation in pulmonary arterial hypertension: is it time to quell the fire? Eur Respir J. 2014;43:685–688. doi:10.1183/09031936.00006014
14. Anwar A, Ruffenach G, Mahajan A, Eghbali M, Umar S. Novel biomarkers for pulmonary arterial hypertension. Respir Res. 2016;17:88. doi:10.1186/s12931-016-0396-6
15. Soon E, Holmes AM, Treacy CM, et al. Elevated levels of inflammatory cytokines predict survival in idiopathic and familial pulmonary arterial hypertension. Circulation. 2010;122:920–927. doi:10.1161/CIRCULATIONAHA.109.933762
16. Voelkel NF, Gomez-Arroyo J, Abbate A, Bogaard H, Nicolls M. Pathobiology of pulmonary arterial hypertension and right ventricular failure. Eur Respir J. 2012;40:1555–1565. doi:10.1183/09031936.00046612
17. Cracowski JL, Chabot F, Labarère J, et al. Proinflammatory cytokine levels are linked to death in pulmonary arterial hypertension. Eur Respir J. 2014;43:915–917. doi:10.1183/09031936.00151313
18. Heresi GA, Aytekin M, Hammel JP, Wang S, Chatterjee S, Dweik R. Plasma interleukin-6 adds prognostic information in pulmonary arterial hypertension. Eur Respir J. 2014;43:912–914. doi:10.1183/09031936.00164713
19. Perros F, Dorfmuller P, Montani D, et al. Pulmonary lymphoid neogenesis in idiopathic pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;185:311–321. doi:10.1164/rccm.201105-0927OC
20. Stacher E, Graham BB, Hunt JM, et al. Modern age pathology of pulmonary arterial hypertension. Am J Respir Crit Care Med. 2012;186:261–272. doi:10.1164/rccm.201201-0164OC
21. Rodríguez‐Iturbe B, Pons H, Quiroz Y, Lanaspa MA, Johnson RJ. Autoimmunity in the pathogenesis of hypertension. Nat Rev Nephrol. 2014;10:56–62. doi:10.1038/nrneph.2013.248
22. Caillon A, Schiffrin EL. Role of inflammation and immunity in hypertension: recent epidemiological, laboratory, and clinical evidence. Curr Hypertens Rep. 2016;18:21. doi:10.1007/s11906-016-0628-7
23. McMaster WG, Kirabo A, Madhur MS, Harrison DG. Inflammation, immunity, and hypertensive end‐organ damage. Circ Res. 2015;116:1022–1033. doi:10.1161/CIRCRESAHA.116.303697
24. Chen TH, Gona P, Sutherland PA, et al. Long‐term C‐reactive protein variability and prediction of metabolic risk. Am J Med. 2009;122:53–61. doi:10.1016/j.amjmed.2008.08.023
25. Tomiyama H, Shiina K, Matsumoto‐Nakano C, et al. The contribution of inflammation to the development of hypertension mediated by increased arterial stiffness. J Am Heart Assoc. 2017;6:e005729. doi:10.1161/JAHA.117.005729
26. Mozos I, Malainer C, Horbańczuk J, et al. Inflammatory markers for arterial stiffness in cardiovascular diseases. Front Immunol. 2017;8:1058. doi:10.3389/fimmu.2017.01058
27. Mahmud A, Feely J. Arterial stiffness is related to systemic inflammation in essential hypertension. Hypertension. 2005;46:1118–1122. doi:10.1161/01.HYP.0000185463.27209.b0
28. Arnold N, Gori T, Schnabel R, et al. Relation between arterial stiffness and markers of inflammation and hemostasis – data from the population-based Gutenberg health study. Sci Rep. 2017;7:6346. doi:10.1038/s41598-017-06175-2
29. Forouzan O, Dinges E, Runo JR, et al. Exercise-induced changes in pulmonary artery stiffness in pulmonary hypertension. Front Physiol. 2019;10:269. doi:10.3389/fphys.2019.00269
30. Gupta A, Sharifov O, Lloyd S, et al. Novel noninvasive assessment of pulmonary arterial stiffness using velocity transfer function. J Am Heart Assoc. 2018;7:1–28. doi:10.1161/JAHA.118.009459
31. Tan W, Madhavan K, Hunter KS, Park D, Stenmark KR. Vascular stiffening in pulmonary hypertension: cause or consequence? (2013 Grover Conference series). Pulm Circ. 2014;4(4):560–580. doi:10.1086/677370
32. Thenappan T, Prins K, Pritzker M, Scandurra J, Volmers K, Weir E. The critical role of pulmonary arterial compliance in pulmonary hypertension. Ann Am Thorac Soc. 2016;13(2):276–284. doi:10.1513/AnnalsATS.201509-599FR
33. Sznajder M, Dzikowska-Diduch O, Kurnicka K, et al. Increased systemic arterial stiffness in patients with chronic thromboembolic pulmonary hypertension. Cardiol J. 2018;7:e009459. doi:10.5603/CJ.a2018.0109
34. Chamorro N, Del Pozo R, García-Lucio J, et al. Peripheral arterial stiffness and endothelial dysfunction in pulmonary arterial hypertension. Eur Respir J. 2015;46:PA2452. doi:10.1183/13993003.congress-2015.PA2452
35. Alanis-Sanchez G, De La Cruz-rodriguez K, Ramos-Becerra C, et al. Association of carotid stiffness parameters with pulmonary function in patients with systemic sclerosis and pulmonary hypertension. J Hypertens. 2017;35(e–Supplement 2):e252. doi:10.1097/01.hjh.0000523735.17372.a0
36. Bergel DH. The static elastic properties of the arterial wall. J Physiol. 1961;156(3):445–457. doi:10.1113/jphysiol.1961.sp006686
37. Asmar R. Arterial Stiffness and Pulse Wave Velocity: Clinical Applications. Amsterdam, The Netherlands: Elsevier; 1999.
38. Shirai K, Utino J, Otsuka K, Takata M. A novel blood pressure-independent arterial wall stiffness parameter; cardio-ankle vascular index (CAVI). J Atheroscler Thromb. 2006;13:101–107. doi:10.5551/jat.13.101
39. Cheuk-Kwan S. Cardio-ankle vascular index (CAVI) as an indicator of arterial stiffness integrated. Blood Pressure Control. 2013;6:27–38. doi:10.2147/IBPC.S34423
40. Miyoshi T, Ito H. Assessment of arterial stiffness using the cardio-ankle vascular index. Pulse (Basel). 2016;4(1):11–23. doi:10.1159/000445214
41. Asmar R. Principles and usefulness of the cardio-ankle vascular index (CAVI): a new global arterial stiffness index. Eur Heart J Suppl. 2017;19(Supplement B):B4–B10. doi:10.1093/eurheartj/suw058
42. 2018 ESC/ESH Guidelines for the management of arterial hypertension. The task force for the management of arterial hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension. Eur Heart J. 2018;00:1–98. doi:10.1093/eurheartj/ehy339
43. Guyatt G, Sullivan M, Thompson P, et al. The 6-minute walk: a new measure of exercise capacity in subjects with chronic heart failure. Can Med Assoc J. 1985;132(919–923):PMC1345899.
44. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six minute walk test. Am J Respir Crit Care Med. 2002;166:111–117. doi:10.1164/ajrccm.166.1.at1102
45. Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiography. 2015;28:1–39. doi:10.1016/j.echo.2014.10.003
46. Yambe T, Yoshizawa M, Saijo Y, et al. Brachio-ankle pulse wave velocity and cardio-ankle vascular index (CAVI). Biomed Pharmacother. 2004;58(Suppl 1):S95–S98. doi:10.1016/S0753-3322(04)80015-5
47. Fukuda-Denshi Company L, Tokyo, Japan. Available from: https://fukuda.com/wp-content/uploads/2017/03/VS-1500N_Catalog_8P.pdfl.
48. Vlachopoulos C, Aznaouridis K, Stefanadis C. Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol. 2010;55(13):1318–1327. doi:10.1016/j.jacc.2009.10.061
49. Blacher J, Guerin A, Pannier B, Marchais S, Safar M, London G. Impact of aortic stiffness on survival in end-stage renal disease. Circulation. 1999;99:2434–2439. doi:10.1161/01.CIR.99.18.2434
50. Safar H, Mourad -J-J, Safar M, Blacher J. Aortic pulse wave velocity, an independent marker of cardiovascular risk. Arch Mal Cœur. 2002;95:1215–1218.
51. Boutouyrie P, Tropeano AI, Asmar R, et al. Aortic stiffness is an independent predictor of primary coronary events in hypertensive patients: a longitudinal study. Hypertension. 2002;39:10–15. doi:10.1161/hy0102.099031
52. Cruickshank K, Riste L, Anderson S, et al. Aortic pulse-wave velocity and its relationship to mortality in diabetes and glucose intolerance: an integrated index of vascular function? Circulation. 2002;106:2085–2090. doi:10.1161/01.CIR.0000033824.02722.F7
53. Mitchell GF, Hwang SJ, Vasan RS, et al. Arterial stiffness and cardiovascular events: the Framingham Heart Study. Circulation. 2010;121(4):505–511. doi:10.1161/CIRCULATIONAHA.109.886655
54. Guerin AP, Blacher J, Pannier B, Marchais SJ, Safar ME, London GM. Impact of aortic stiffness attenuation on survival of patients in end-stage renal failure. Circulation. 2001;103:987–992. doi:10.1161/01.CIR.103.7.987
55. DeLoach S, Townsend R. Vascular stiffness: its measurement and significance for epidemiologic and outcome studies. Clin J Am Soc Nephrol. 2008;3(1):184–192. doi:10.2215/CJN.03340807
56. Pannier B, Guerin AP, Marchais SJ, Safar ME, London GM. Stiffness of capacitive and conduit arteries: prognostic significance for end-stage renal disease patients. Hypertension. 2005;45:592–596. doi:10.1161/01.HYP.0000159190.71253.c3
57. Bonarjee VVS. Arterial stiffness: a prognostic marker in coronary heart disease. Available methods and clinical application. Front Cardiovasc Med. 2018;5:64. doi:10.3389/fcvm.2018.00064
58. Kaess BM, Rong J, Larson MG, et al. Aortic stiffness, blood pressure progression, and incident hypertension. JAMA. 2012;308(9):875–881. doi:10.1001/2012.jama.10503
59. Beevers G, Lip G, O’Brien E. The pathophysiology of hypertension. BMJ. 2001;322:912. doi:10.1136/bmj.322.7291.912
60. Shirai K. Analysis of vascular function using the cardio-ankle vascular index (CAVI). Hypertens Res. 2011;34:684–685. doi:10.1038/hr.2011.40
61. Obata Y, Mizogami M, Singh S, et al. The effects of hemodynamic changes on pulse wave velocity in cardiothoracic surgical patients. Biomed Res Int. 2016;2016:Article ID 9640457. doi:10.1155/2016/9640457
62. Wilenius M, Tikkakoski A, Tahvanainen A, et al. Central wave reflection is associated with peripheral arterial resistance in addition to arterial stiffness in subjects without antihypertensive medication. BMC Cardiovasc Disord. 2016;16:131. doi:10.1186/s12872-016-0303-6
63. Greene ES, Gerson JI, Arterial pulse wave velocity: a limited index of systemic vascular resistance during normotensive anesthesia in dogs. J Clin Monit. 1985;4:219–226. doi:10.1007/BF02832814
64. Ghosh A, Dharmarajan A, Swain P, Das D, Verma P, Tripathy P. Impact of cardiovascular factors on pulse wave velocity and total vascular resistance in different age group patients with cardiovascular disorders. Curr Aging Sci. 2018;11:261–268. doi:10.2174/1874609812666190226151
65. Mehta T, Nuccio E, McFann K, Madero M, Sarnak M, Jalal D. Association of uric acid with vascular stiffness in the Framingham Heart Study. Am J Hypertens. 2015;28(7):877–883. doi:10.1093/ajh/hpu253
66. Kanellis J, Watanabe S, Li JH, et al. Uric acid stimulates monocyte chemoattractant protein-1 production in vascular smooth muscle cells via mitogen-activated protein kinase and cyclooxygenase-2. Hypertension. 2003;41:1287–1293. doi:10.1161/01.HYP.0000072820.07472.3B
67. Kang DH, Nakagawa T, Feng L, et al. A role for uric acid in the progression of renal disease. J Am Soc Nephrol. 2002;13:2888–2897. doi:10.1097/01.asn.0000034910.58454.fd
68. Netea MG, Kullberg BJ, Blok WL, Netea RT, van der Meer JW. The role of hyperuricemia in the increased cytokine production after lipopolysaccharide challenge in neutropenic mice. Blood. 1997;89:577–582. doi:10.1182/blood.V89.2.577
69. Shirai K, Song M, Suzuki J, et al. Contradictory effects of beta1- and alpha1- aderenergic receptor blockers on cardio-ankle vascular stiffness index (CAVI) – CAVI independent of blood pressure. J Atheroscler Thromb. 2011;18(1):49–55. doi:10.5551/jat.3582
70. Alam M, Wardell J, Andersson E, Samad BA, Nordlander R. Characteristics of mitral and tricuspid annular velocities determined by pulsed wave Doppler tissue imaging in healthy subjects. J Am Soc Echocardiogr. 1999;12:618–628. doi:10.1053/je.1999.v12.a99246
71. O M U, E E C, Ueti Ade A, de Lima-filho EC, Nogueira EA. Assessment of right ventricular function with Doppler echocardiographic indices derived from tricuspid annular motion: comparison with radionuclide angiography. Heart. 2002;88:244–248. doi:10.1136/heart.88.3.244
72. Kaul S, Tei C, Hopkins JM, Shah PM. Assessment of right ventricular function using two-dimensional echocardiography. Am Heart J. 1984;107:526–531. doi:10.1016/0002-8703(84)90095-4
73. Forfia P, Fisher M, Mathai S, et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med. 2006;174:1034–1041. doi:10.1164/rccm.200604-547OC
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.