")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Systematic Use of Song and Music in Dementia Care: Health Care Providers’ Experiences
Received 17 September 2019
Accepted for publication 23 January 2020
Published 11 February 2020 Volume 2020:13 Pages 143—151
DOI https://doi.org/10.2147/JMDH.S231440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Else Mari Ruberg Ekra,1 Bjørg Dale2
1Institute of Health and Nursing Science, University of Agder, Grimstad NO-4898, Norway; 2Centre of Caring Research – Southern Norway, Faculty of Health and Sport Sciences, University of Agder, Grimstad NO-4898, Norway
Correspondence: Else Mari Ruberg Ekra Email [email protected]
Background and Aim: Using song and music in a systematic way in residential dementia care may have several positive impacts on the patients, as well as the care providers. The aim of this study was to explore how health care providers experienced taking responsibility for conducting a song and music program in dementia care in nursing homes.
Methods: An explorative, qualitative study design was used. Focus groups were formed by 17 health care providers from 3 different nursing homes. These providers had experience implementing and using the “Gjenklang” (“reverberation”) song and music program especially developed for people with dementia. Focus group interviews were transcribed verbatim, and systematic text condensation was used for analysing the data.
Results: Three categories with associated subcategories emerged from the analysis process. The categories were 1) the music program increased the staff’s consciousness and awareness; 2) the music program evoked the patients’ emotions and reactions; and 3) maintaining enthusiasm over time.
Conclusion: The general opinion among the participants was that using the song and music program in a systematic and planned way had many benefits and positive impacts on the patients, as well as the staff. However, it was challenging to make it a part of the daily routine. Thus, it is important that the leaders of the units take responsibility to ensure continuity and maintain engagement among the staff over time.
Keywords: dementia, music therapy, music program, qualitative, focus group interviews, nursing homes
Introduction
The rates of dementia are rapidly growing worldwide, and it is estimated that in 35 years 140 million people will suffer from dementia.1 The same development is happening in Norway, with the prevalence of dementia in Norwegian nursing homes over 80%.1 Dementia is an inherited brain-organic syndrome characterized by reduced cognitive capacity.1 Although dementia is caused by a wide range of brain diseases, common symptoms are cognitive impairment, changes in emotions and personality, and reduced ability to function in daily life.2 Dementia might affect different parts of the brain, and will, in general, typically affect a person’s ability to solve problems, reason, speak, and remember.3
As dementia develops, it might be challenging to interact and building relationships with patients, due to deteriorating verbal communication skills.4 Therefore, it is necessary to identify other ways to building relationships with this patient group.4 One non-pharmacological intervention found to be appropriate in the treatment of both behavioural and psychological symptoms of dementia is music therapy.5–7 Music therapy is defined as a music intervention facilitated by a trained music therapist.6,8
The goal of the Norwegian Dementia Plan 20209 is to build a more dementia-friendly society. This implies, among other things, supporting the physical and mental health of persons suffering from dementia, and the facilitation of coping, belonging, and experience of meaningfulness. Person-centred care is highly emphasized,10,11 and environmental treatments, such as song and music therapy, are described as a central approach. Studies have shown that implementing song and music therapy in dementia care has positive impacts, and familiar and preferred music is found to increase the sense of environmental familiarity for people suffering from dementia.12 Further, it might enhance the person’s well-being, vitality, and feelings of joy and peace;13 reduce anxiety and depression;14 and improve cognitive functioning.15 Studies have also shown that music has a positive effect on alleviating some of the challenging behaviours caused by dementia.5,13,16 Mendes3 describes that the emotions evoked by music can help persons recall lasting memories, and even persons with severe dementia who lack language ability may be able to clap to a beat, tap their feet, or hum. However, other studies have found that people with dementia can react negatively to music. For example, Garrido et al6 found that patients with high levels of depression showed more sadness when they listened to music. Given this discrepancy, we sought to examine the implementation of a song and music program in more detail from the care providers perspective.
Music therapy is a safe and low-cost alternative intervention compared to pharmacological treatment.14,15 However, according to Myskja,13 important prerequisites are that the music is individually adapted, and that it is systematically planned and used.
Sung et al17 found that, although most healthcare professionals had a positive attitude towards using music for people with dementia, few of them used it. The main reason for that was that the health providers had limited knowledge and skills. Therefore, health professionals need to be more conscious about the possibility of music therapy to increase the patients’ quality of life,18 and they need training and guidance on how music therapy can be used systematically. It is also important to prevent or minimize problematic issues, such as lack of training and lack of individual tailoring, by taking enough time to plan the intervention.19
A song and music program, developed and introduced by music therapists, was implemented in residential dementia care in three nursing homes in Norway. Health care providers received training on implementing the song and music program from the music therapists. After the program was introduced and initiated, the care staff were responsible for continuing the program.
The aim of this study was to explore how health care providers experienced taking responsibility for conducting a song and music program in dementia care in nursing homes.
The research questions were: Was the song and music program acceptable to staff? Did they feel that the program had positive impacts on the residents? How did the program influence their experience as care workers?
Materials and Methods
This study employed an explorative qualitative design. Focus groups were conducted with health care staff who had experiences in using the song and music program.
Context
The music program that was implemented was termed “Gjenklang” in Norwegian (similar to “reverberation” in English). It includes songbooks and accompanying CDs containing a repertoire of songs intended to be well known by older people in Norway, such as songs from their childhood, schooldays, youth, etc. The CDs allow patients and staff to follow the music and sing and hum in their own way. The material could be used both individually or with small groups of patients.
Guidelines on how to use the program in a conscious and systematic way together with the patients were available, and a training program developed by the music therapists was carried out for the care staff who were involved in the patient care. First, the care staff attended a treatment session run by a music therapist. Second, they were responsible for a treatment session with supervision by a music therapist, where they received feedback afterwards. The music therapists were responsible for regular follow-up. A training video was also prepared showing how a treatment session should be conducted. In addition to instructions on how to use the songbooks and CDs, the personnel were supervised on what and how to observe the patients’ responses and reactions during the treatment session, and how and what to document in retrospect. This part was considered important for using the program in a systematic way.
Participants and Recruitment
One contact person at each of the three target institutions informed the care staff about the study and was responsible for inviting and recruiting participants to the focus groups. The only inclusion criterium was that the health care provider should have experiences related to the song and music program. Efforts were made to include persons with different types of professional background, ages, length of employment in the unit, both full time and part time employed, and both permanent and temporary positions. The rationale behind this was to explore if such conditions could have an impact on the participants’ experiences.
Data Collection
Data were collected during spring and summer 2017 through three focus group interviews, one interview at each of the included nursing homes. Focus group interviews were chosen as the method that allows participants to share and discuss common experiences related to the same topic. The focus groups included five persons from nursing home A, five persons from nursing home B, and seven persons from nursing home C. The interviews were conducted at the staff’s own workplace, and they lasted between 52 and 65 mins. They were audio-recorded and subsequently transcribed verbatim.
The focus group approach facilitated an open and fluid conversation about the participants’ experiences with the song and music program. However, a semi-structured interview guide was prepared and used to ensure that important topics and questions were discussed (Box 1).
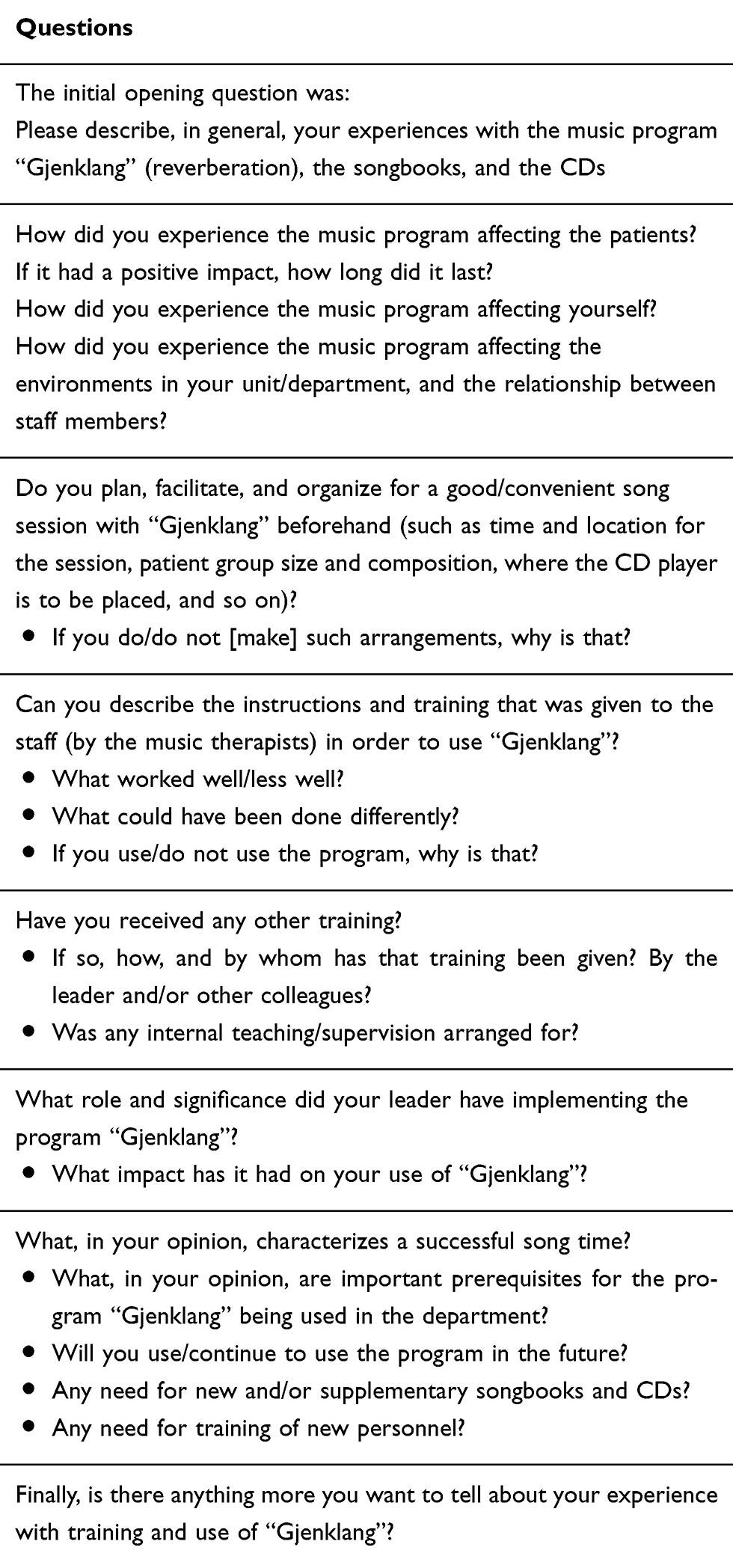 |
Box 1 Overview of the Questions in the Interview Guide |
Analysis
The data analysis was inspired by the systematic text condensation approach developed by Malterud.20 Systematic text condensation consists of four analysis steps that guided our work. In the first step, both authors read the focus group interviews independently to gain an overall impression and to identify main issues that addressed the informants’ experiences of using the song and music program. Thereafter, the authors met to discuss preliminary themes in the texts. In the second step, meaning units (MUs), that is, fragments of text containing information about the aim of the study, were identified and labelled. Subsequently, connected MUs were grouped. In the third step, systematic abstraction of the MUs was established and they were condensed to represent a decontextualized selection of units. At this stage, a first-person format was applied. In the fourth and final step, data were reconceptualized and the pieces were assembled into a whole. By synthesizing the contents of the condensates, descriptions of the findings were developed and presented as categories and sub-categories.20
Ethics
The study was guided and implemented by ethical principles for clinical research.21,22 It was approved by the Norwegian Centre for Research Data (ref. 53479). All participants were given oral and written information about the study. Confidentiality and voluntariness for participating in the study were assured, as well as the participants’ right to withdraw from the study at any time without giving any reason. Written informed consents were obtained before the interviews started.
Results
A total of 17 health care providers participated in one focus group interview each, which were conducted at their respective three workplaces. Nine of the participants were registered nurses, seven were nurse assistants, and one had a bachelor’s degree in social education. All participants were women ranging from 25 to 68 years old (M=45.6 years), and all except one were currently permanently employed in the units. On average, they had worked 11 years in the unit, ranging from 9 months to 25 years. Fourteen of them were employed more than three-quarter time, including seven with full-time positions. Eleven of the participants had at least one type of continuing education. Most had education in geriatrics, elderly care, or dementia care, but some also had supplementary education in general mental health and counselling.
The analysis of the interview texts revealed that the staff experienced using the song and music program as important. They particularly expressed pleasant surprise at how well the patients with dementia remembered the songs, how the songs evoked their memories, and how they triggered good conversations and storytelling among them. At the same time, the informants experienced challenges regarding maintenance of enthusiasm among the staff over time.
Three categories with nine corresponding subcategories emerged from the analysis of the interview texts (Table 1).
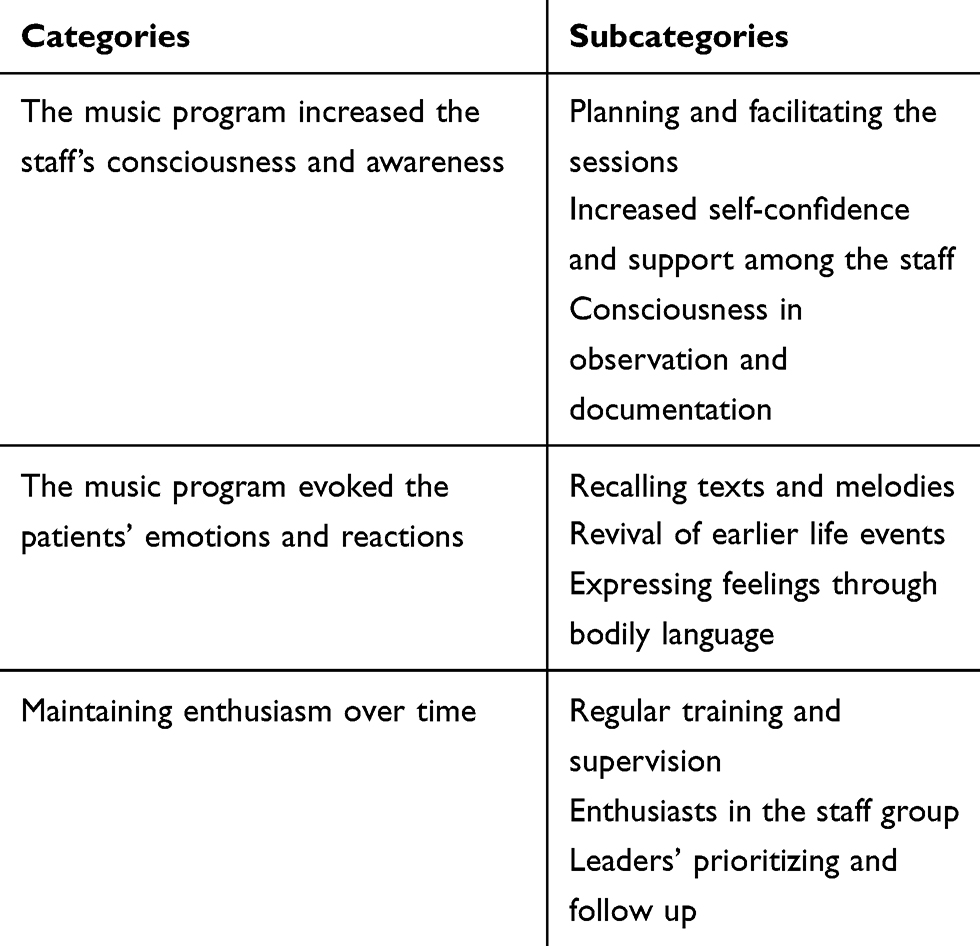 |
Table 1 Overview of the Categories and Subcategories from the Analyses |
In the following subsections, the categories and subcategories are more deeply described. Quotes from the participants are used to illustrate and complement the findings.
The Music Program Increased the Staff’s Consciousness and Awareness
The use of songs and music in a planned and systematic way was important for gaining positive impacts. When used otherwise, for example, solely as background music, the informants experienced that music could be perceived solely as noise. The informants reported that they had been more conscious and aware how they used song and music in the units. One stated that “ … we have become more aware that music could also be noisy …, instead we put on a CD and we sing together with the patients”. They also emphasized the importance of staff presence when music was played. One reported the following experience: “If they (the patients) just sit and listen to the music they easily fall asleep …, if we (the staff) disappear, they often get restless and start walking”.
Although the need for a good structure and plan was emphasized, the importance of flexibility was also underlined. They had to consider and facilitate the appropriate time, duration, frequency, and size of the patient group before offering music treatment sessions. They also described it as crucial to sit in such a way that they had eye contact with them to keep their attention. One informant described her method as follows: “it is important for me to include everyone during the sessions … I sit on a chair that has wheels … I roll to each person to make eye contact and get them to join the singing”.
It was also important to joke a little if it was natural in the situation. It was emphasized to consider that the patients were different, and their wishes and needs varied. This could be, for example, to pay attention and seat patients where they preferred to sit, or respect their preferences according to songs they knew and liked. Consequently, the song repertoire should be variable to fit everyone. Some of the informants mentioned that the selection of songs in the songbooks and CDs needed updating. They reported that the song repertoire was a bit limited due to the different patients’ preferences and backgrounds. Some of the patients were relatively young, and it was obvious that some preferred special kinds of music that were not included in the song repertoire at that time.
The song book and the CDs were a good support for those in the staff that were less experienced with singing, helping them to keep the pace and tone of the music, and the text was clear. They could use the program even if they were not a talented or experienced singer or familiar with the songs: “The program was, in a way, for everyone”. They described that they previously had needed staff who could play an instrument, but now they were less dependent on that. Being engaged and participating in the program led to an increased consciousness of the benefits of using song and music, and they sang more. In the very beginning, the staff that not were familiar with singing experienced the song sessions as challenging: “For those of us who cannot sing it was a little scary … we are not used to singing in front of people so it was a little scary”. However, this experience gradually changed: “We may have become more confident about the situation. It is no longer so embarrassing as it might be when one is not so good at singing”.
Some described a sense of coping and self-esteem among the staff, related to the contribution of doing something valuable for the patients in addition to their own experiences of managing the program. Some of the care workers also reported a sense of increased community and team spirit in the staff. Although it could sometimes be resource-intensive to implement the program systematically, some believed that it could also be resource-saving because of the impact it had on patients, as well as releasing resources for other tasks.
The staff members had been taught and trained in how to observe the patients during and after the song sessions. In addition, they were instructed on what they should observe and how to document their observations in the patients’ care plan. Many expressed that they perceived this part of the project as important, but very time consuming. Some found it challenging to both sing and do observation simultaneously. Further, even when they observed the patients, they found it difficult to find the “correct” words when documenting it in the patient’s care plan. The informants also described that they were more eager to document in the initial phase of the project when it was newly introduced. After some while, documentation was less prioritized because of other care tasks that they perceived to be more important. In summary, the staff members’ consciousness of documentation was increased, but it was nevertheless not prioritized for various reasons.
The Music Program Evoked the Patients’ Emotions and Reactions
The informants described that the music program made a difference for many of the patients, they recalled and recognized texts and melodies, and the songs evoked memories. Some patients were in a way caught up by the song and music, and suddenly they started to sing. This could happen even though the patients had little or no language ability. One informant said “One of our patients has begun to lose language and cannot speak whole sentences … I was so surprised. She did all the verses, they just rolled out, verse after verse”.
Another informant said:
People are actually living up. So, with people who have dementia, I think it’s special. So, there were many of them that I thought would not sing at all, and who suddenly woke up and were attending (hmm), it was very nice to experience.
Some of the informants had the impression that the songs and the music represented something that the patients could still cope with, which gave them a sense of mastery. They discovered things and events they had long forgotten because it was “far behind”. It was often found that the patients knew the song texts and melodies better than the staff did. One said:
I liked to look at one of the patients and sing after her. Then you get a special contact … for you are sort of more at an equal level in that setting, and you just see that glimpse in the patient’s eyes and get eye contact, you feel like you’re doing something together.
Often the song and music awakened memories of the patients’ earlier lives, such as their childhood and school days, and this was the start of good conversations and storytelling. The song could trigger smiles and laughter, as well as tears and sad memories because they recalled the losses they had experienced. Regardless of reactions, pausing between the songs to allow for discussion and recollection was considered to be as important as the song itself: “… there are a lot of memories with those songs … when they hear the songs, some memories come up … almost like a treasure chest that is open”.
One of the informants said:
We sang a lullaby. And then she (the patient) told that her mother sang that lullaby to her every night when she went to bed. She got tears in her eyes and started to cry because she thought of her mother. Others also started telling about their mothers.
Another reported the following experience:
If we do a song about school … then we stop after a verse. Then, for example, they begin to tell about their first day at school, … about having a school bag. They remember these things, everything, what the teacher was called, their way to school … what clothes they were wearing, their food … It is amazing that they have preserved so much.
Sometimes they experienced that patients expressed emotions through their body language by clapping their hands, tapping their feet, and even dancing with the music. Most residents became, in general, calmer during and after the song sessions, stopping restless wandering or unwanted outward behaviour: “Then you can observe changes and that they are just happy, you see it on their face or body … tilting their legs and like that”.
Decreased need for sedatives was also observed. However, there were also patients who became uneasy and angry. Not everybody loved music, some patients did not manage to sit still for a long time, and some patients became frustrated when they could not remember the songs.
The good atmosphere that the songs and music created, and the patient’s reactions and responses, were experienced as motivational for the staff: “It gives a very good feeling; … it is very nice when you have such a good time together … It gives something to the patients and to the staff as well”.
Further, they experienced making a positive contribution to the patients: “ … you feel happy when you go home after work … you feel that you have contributed, that you have actually accomplished something and that they are doing well”.
Maintaining Enthusiasm Over Time
It was a general impression that the informants had experienced several benefits of using the song program, but they also reported that the engagement and motivation were clearly highest in the initial phase of the project. At that time, the music therapists were often present in the units. They had a close follow-up on teaching and supervising the staff and performing song sessions with the patients and staff.
One participant said:
They (the music therapists) had a singing session … and I have never sung so loud before, … so incredibly inspiring … I saw how they used themselves and how the responses were … after a while I dared to try it myself.
The music therapists were, in general, experienced as good role models and created enthusiasm among the staff. Hence, many of the informants wanted the music therapists to continue a regular follow-up over time to maintain their commitment: “The best would been to have a music therapist present regularly, and preferably every day”.
According to the informants, having some enthusiasts among staff was an important factor in maintaining the commitment and motivation to continue using the song program:
The most important thing is that those who use the program pass on how good the effect was … the more positive you see that it is with the patients, the more you want to use it.
Another informant said “Getting the whole staff involved can be a challenge. Good structures and personnel who are good role models to invite and motivate colleagues can contribute to increased use”. They also expressed the importance of enthusiastic leaders to maintain engagement: “… there must be someone who ‘burns’ for it … you must have such leaders who are driving forces to keep it active”. Busy working days, various issues related to daily patient care, or new projects and care tasks often draw attention away from the song and music program.
Discussion
The aim of this study was to explore how health care providers experienced taking responsibility for conducting a song and music program in dementia care in nursing homes. Music therapy is highlighted, in several studies, to have promising impacts on quality of life and well-being in persons with dementia.2,11,23,24 This impression was also supported by the informants in the current study, although certain aspects were emphasized as important for it to be an appropriate tool. This will be further elaborated below.
It was a general opinion among the participants that the song and music program achieve positive impacts when used in a systematic, conscious, and planned way. If used only as background music, for example, by having the TV and radio constantly on, the informants had previously experienced that the music could have a negative effect on residents. It could be perceived as disturbing and make the patients more anxious and restless. Studies have shown that non-personalized music might increase anxiety and depression in patients with dementia.6,25 It was vital to organize active song sessions in groups with staff present all the time. Several strategies related to music therapy are described, and distinction is often made between a receptive approach (listening to music) and an active approach (i.e., participating).26 In a randomized controlled trial, Cho2 compared the effect of three different approaches to music therapy with persons with dementia living in a nursing home. One group participated in active singing, one group only listened to music, and one group watched TV with staff present. She found significantly increased quality of life and decreased negative behaviour in the active singing group only and suggested that some of the explanations might be the physical impact (the persons’ physical movement while singing), the interpersonal activity, and the ability to participate in a meaningful activity. Similar findings have been found in other studies.6,25
People with dementia are as varied as people without it, and they have their own backgrounds, histories, and preferences. Music is found to be closely associated with each person’s identity, history, and earlier life events, which are often linked to a particular type of music.5 Therefore, it seemed to be crucial that the songs and music were adapted to the participants in the groups. Music therapy in group settings is found to be beneficial for persons with dementia.25 However, studies have also shown that when the song/music is pre-recorded it may be less beneficial because it is difficult to account for each group member’s personal music taste.25 In addition, because the music taste and preferences may vary a lot between individuals, the composition of group members appears to be important. It is important for the staff to balance their attention towards the group as a whole and at the same time see the patients as individuals. Another individual aspect to consider when the group sessions are planned is that of temporality, such as to assess the patient’s daily condition and what time of day it is most appropriate for performing the song session. To succeed when implementing an intervention like this, it is crucial that the patients’ needs are met.19
The informants in our study expressed that it was startling how much the patients could recall the lyrics and tunes of the songs, even though they had partly or completely lacked verbal language for a long time. In addition to singing along, their responses to the music by means of feet tapping, hand clapping, humming, and dancing are in line with what has been found in other studies.5,11 Thus, their body language clearly expressed emotional reactions, such as joy. Music can help persons with dementia to improve their mood and increase their attentiveness,5 at least immediately and in the short term.
Combining music and reminiscence therapy might be a fruitful intervention, particularly when combined with conversation and storytelling.27 Our informants narrated several episodes where patients had described experiences from their past lives in detail, often from their childhood. In fact, some of them claimed that the talks and storytelling related to the memories evoked by a song or music were as important as the song and music itself. Some informants compared it to opening a treasure box full of memories, something that Mendes3 describes as “unlocking” a person with dementia through song and music. It was therefore considered very important to stop the music when it felt right and natural to allow time and space for conversation. Matthews28 claims that music therapy may stimulate the patients to achieve a state where they can connect, both with their memories from the past, and with the people around them. However, the reminiscence effect of song and music therapy might also evoke sad memories, as was found in the current study.
An overall impression reported by the staff was that they experienced the program as a good tool for providing daily care to people with dementia, particularly for those less experienced with singing. They underscored, nevertheless, the importance of regularly use – both to maintain their own motivation and to maintain the positive impact it had on the patients. When used regularly, the staff became more familiar and relaxed in the song sessions. Further, in accordance with our findings, the relational connectedness and social aspects associated with song sessions have been highlighted.29 Some informants expressed that the power relationship between the staff and the patients was equalized, because the staff members had something they could learn from the patients. It can be experienced as a meaningful and mutually engaging social interaction.3
Although the general experiences and opinions between the staff members participating in this study were that systematic use of song and music in dementia care had many positive impacts, they also reported that the engagement and enthusiasm were greatest in the initial phase. Many felt that the eagerness decreased after a while, especially after the music therapists were no longer present in the unit. Sung et al17 explored nursing staff’s attitudes and use of music for older people with dementia in long-term care facilities, and they concluded that the staff lacked enough formal training. Thus, it appears as vital that the music therapists are regularly present in the unit, most preferably every day, to maintain engagement, perform training, and follow-up with the staff. Further, it was also highlighted that a decisive prerequisite to maintaining good routines to implement the program on a regular basis was the leaders’ willingness to prioritize and facilitate it during busy working days.
It might also be challenging for staff to regularly arrange for song sessions in addition to all the other care duties and workload in the unit. The informants also complained about the requirement to document in writing what they observed in patients during the group sessions. Burdensome paperwork was found to be one of the challenges reported by the staff participating in a corresponding study.19
Methodological Limitations and Recommendations
This study focused on the health care providers’ experiences of using a song and music program in dementia care. Thus, information about the patients’ subjective experiences was limited to how the informants perceived and interpreted them. New studies should be conducted that explore patients’ own perceptions more directly, as well as examine how such an intervention might impact their behaviour and well-being in both the long and short term. Further, the focus group interviews were conducted only once, and the positions of the informants varied greatly. For instance, it varied greatly how much experience they had gained with the program, and whether they had participated or not in the music therapists’ training in using the program. It could, therefore, be appropriate to repeat the interviews after some while.
Analyses of findings in qualitative research are highly dependent on the authors’ views, preconceptions, and interpretations. Therefore, one should be careful and not generalize the findings beyond the actual context and study participants. Nevertheless, our results were well in line with those found in other similar studies.
Conclusions and Clinical Implications
The overall thrust of the findings in this study was that health care providers had mostly positive experiences of using song and music in residential dementia care. Consequently, such interventions could also be recommended in a similar context in dementia care. It was, however, emphasized that it had to be carried out in a systematic and planned manner; otherwise, the music could be perceived as noisy and disturbing to the patients and thus have an opposite impact. Therefore, it seems crucial that the care staff is sufficiently trained to use such programs in ways that benefits the patients. The positive experiences that were observed were that the patients seemed to recall an unexpectedly amount of a song’s lyrics and melodies, and that many of them expressed emotions and narrated personal stories as the songs were sung and played. Further, the relational power of the song and music was highlighted, both between the staff and the patients and within the patient group. One of the challenges that was expressed was to make the program a part of the regular routine in the unit and to maintain staff engagement over time. At the same time, they perceived there was a need for more training, supervision, and follow-up, especially for those newly hired and for temporary staff. It was also underscored that the leaders in the units should take responsibility for maintaining the music program.
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Engedal K, Haugen PK. Demens – Sykdommer, Diagnostikk Og Behandling (In Norwegian: Dementia – Diseases, Diagnostics and Treatment). Tønsberg: Forlaget Aldring og helse – akademisk; 2018.
2. Cho HK. The effects of music therapy-singing group on quality of life and affect of persons with dementia: a randomized controlled trial. Front Med. 2018;5:279. doi:10.3389/fmed.2018.00279
3. Mendes A. “Unlocking” people with dementia through the use of music therapy. Nurs Resident Care (NRC). 2015;17(9):512–514. doi:10.12968/nrec.2015.17.9.512
4. Lykkeslett E, Gjengedal E, Skrondal T, Storjord M-B. Sensory stimulation. A way of creating mutual relations in dementia care. Int J Qual Stud Health Well-Being. 2014;9:23888. doi:10.3402/qhw.v9.23888
5. McDermott O, Orrell M, Ridder HM. The importance of music for people with dementia: the perspectives of people with dementia, family carers, staff and music therapists. Aging Ment Health. 2014;18:706–716. doi:10.1080/13607863.2013.875124
6. Garrido S, Stevens CJ, Chang E, Dunne L. Music and dementia: individual differences in response to personalized playlists. J Alzheimers D. 2018;64(3):933–941. doi:10.3233/JAD-180084
7. Garrido S, Stevens CJ, Chang E, Dunne L. Musical features and affective responses to personalized playlists in people with probable dementia. Am J Alzheimers Dis Other Demen. 2019;34(4):247–253. doi:10.1177/1533317518808011
8. Garrido S, Dunne L, Perz J, Chang E, Stevens CJ. The use of music in aged care facilities: A mixed-methods study. J Health Psych. 2018;1–14. doi:10.1177/1359105318758861
9. Ministry of Health and Care Services. Dementia plan 2020. A more dementia-friendly society. 2016. Available from: https://www.regjeringen.no/en/dokumenter/dementia-plan-2020/id2465117/.
10. Manthorpe J, Kritika S. Person-centered dementia care: current perspectives. Clin Interv Aging. 2016;11:1733–1740. doi:10.2147/CIA.S104618
11. Ihara ES, Tompkins CJ, Inoue M, Sonneman S. Results from a person-centered music intervention for individuals living with dementia. Geriatr Gerontol Int. 2018;19:30–34. doi:10.1111/ggi.13563
12. Cuddy LL, Duffin J. Music, memory and Alzheimer’s disease: is music recognition spared in dementia and how can it be assessed? Med Hypotheses. 2005;64(2):229–235. doi:10.1016/j.mehy.2004.09.005
13. Myskja A (2012). Integrated music in nursing homes – an approach to dementia care. PhD thesis, The Grieg Academy, Department of Music, University of Bergen.
14. Ray KD, Mittelman MS. Music therapy: a nonpharmacological approach to the care of agitation and depressive symptoms for nursing home residents with dementia. Dementia. 2017;16(6):689–710. doi:10.1177/1471301215613779
15. Blackburn R, Bradshaw T. Music therapy for service users with dementia: a critical review of the literature. J Psychiatr Ment Health Nurs. 2014;21:879–888. doi:10.1111/jpm.12165
16. Marmstål Hammar L, Emami A, Engström G, Götell E. Communicating through caregiver singing during morning care situations in dementia care. Scand J Caring Sci. 2011;25:160–168. doi:10.1111/j.1471-6712.2010.00806.x
17. Sung H-C, Lee W-L, Chang S-M, Smith GD. Exploring nursing staff’s attitudes and use of music for older people with dementia in long-term care facilities. J Clin Nurs. 2011;20:1776–1783. doi:10.1111/j.1365-2702.2010.03633.x
18. Strøm BS, Ytrehus S, Grov E-K. Sensory stimulation for persons with dementia: a review of the literature. J Clin Nurs. 2016;25:1805–1834. doi:10.1111/jocn.13169
19. Parland P, Cutler C, Innes A. The challenges of implementing and evaluating a pilot music and movement intervention for people with dementia: innovative practice. Dementia. 2017;16(8):1064–1068. doi:10.1177/1471301216642342
20. Malterud K. Systematic text condensation: A strategy for qualitative analysis. Scand J Publ Health. 2012;40:795–805. doi:10.1177/1403494812465030
21. Declaration of Helsinki.
22. Beauchamp TL, Childress JF. Principles of Biomedical Ethics.
23. Fusar-Poli L, Bieleninik L, Brondino N, Chen X-J, Gold C. The effect of music therapy on cognitive functions in patients with dementia: a systematic review and meta-analysis. Aging Ment Health. 2018;22(9):1103–1112. doi:10.1080/13607863.2017.1348474
24. Spiro N, Farrant CL, Pavlicevic M. Between practice, policy and politics: music therapy and the dementia strategy, 2009. Dementia. 2017;16(3):259–281. doi:10.1177/1471301215585465
25. Garriodo S, Dunne L, Chang E, Perz J, Haertsch SCJ. The use of music playlists for people with dementia: a critical synthesis. J Alzheimer’s Dis. 2017;60(3):1129–1142. doi:10.3233/JAD-170612
26. Pavlicevic M, Tsiris G, Wood S, et al. The ‘ripple effect’: towards researching improvisational music therapy in dementia care homes. Dementia. 2015;14(5):659–679. doi:10.1177/1471301213514419
27. Istvandity L. Combining music and reminiscence therapy interventions for wellbeing in elderly populations: a systematic review. Complement Ther Clin Pract. 2017;28:18–25. doi:10.1016/j.ctcp.2017.03.003
28. Matthews S. Dementia and the power of music therapy. Bioethics. 2015;29(8):573–579. doi:10.1111/bioe.12148
29. Tuckett A, Hodgkinson B, Rouillon L, Balil-Lazoya T, Parker D. What carers and family said about music therapy on behaviours of older people with dementia in residential aged care. Int J Older People Nurs. 2014;10(2):146–157. doi:10.1111/opn.12071
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.