")
Back to Journals » Clinical Ophthalmology » Volume 16
Systane iLux Thermal Pulsation System in the Treatment of Meibomian Gland Dysfunction: A Post-Hoc Analysis of a 12-Month, Randomized, Multicenter Study
Authors Wesley G, Bickle K, Downing J, Fisher B, Greene B, Heinrich C, Kading D, Kannarr S, Miller J, Modi S , Ludwick D, Tauber J , Yeh TN , Srinivasan S
Received 29 June 2022
Accepted for publication 14 October 2022
Published 3 November 2022 Volume 2022:16 Pages 3631—3640
DOI https://doi.org/10.2147/OPTH.S379484
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gina Wesley,1 Katherine Bickle,2 Johnathon Downing,3 Bret Fisher,4 Brennan Greene,5 Colton Heinrich,6 David Kading,7 Shane Kannarr,8 Jason Miller,9 Satish Modi,10 David Ludwick,11 Joseph Tauber,12 Thao N Yeh,13 Sruthi Srinivasan14
1Complete Eye Care of Medina, Hamel, MN, USA; 2ProCare Vision Center, Granville, OH, USA; 3East West Eye Institute, Los Angeles, CA, USA; 4Eye Center of N Florida, Panama City, FL, USA; 5The Eye Care Institute, Louisville, KY, USA; 6Clarke EyeCare Center, Wichita Falls, TX, USA; 7Specialty Eyecare Group, Bellevue, WA, USA; 8Kannarr Eye Care LLC, Pittsburg, KS, USA; 9Insight Research Clinic, Powell, OH, USA; 10Alterman, Modi & Wolter, Poughkeepsie, NY, USA; 11Ludwick Eye Center, Chambersburg, PA, USA; 12Tauber Eye Center, Kansas City, MO, USA; 13Alcon Vision, LLC, Fort Worth, TX, USA; 14Alcon Research, LLC, Johns Creek, GA, USA
Correspondence: Sruthi Srinivasan, Alcon Research, LLC, 11460 Johns Creek Parkway, Johns Creek, GA, 30097, USA, Tel +1 678 415 5315, Email [email protected]
Purpose: This study aimed to demonstrate the effectiveness of Systane iLux, a thermal pulsation device, in patients with MGD, over 12 months post-single treatment.
Methods: This is a post-hoc analysis of a previous prospective, assessor-masked, parallel-group, multicenter study (NCT03956225) that compared the effectiveness and safety of iLux with LipiFlow in subjects with MGD. The original study included subjects with meibomian gland score (MGS) ≤ 12 in lower eyelids, Impact of Dry Eye on Everyday Life-Symptom Bother (IDEEL-SB) module score > 16, and non-invasive tear break-up time (NITBUT) < 10 seconds. Subjects were randomized (1:1) to receive a single bilateral treatment of iLux or LipiFlow. In this post-hoc analysis, mean changes in MGS, NITBUT (first break-up; seconds), IDEEL-SB module score, and corneal staining, from baseline to 12 months were analyzed post-single treatment with iLux.
Results: Data from 119 patients (n=238 eyes) treated with iLux were analyzed. The mean±SD age of the subjects was 58.4± 13.4 years, with majority being female (79.0%). MGS (mean±SD) for both eyes improved significantly from baseline to 12 months (OD [baseline: 6.9± 3.69; month 12: 22.8± 11.31; change: 15.9± 11.57, p< 0.0001]; OS [baseline: 6.4± 3.66; month 12: 23.0± 11.33; change: 16.7± 11.40, p< 0.0001]). Similarly, significant improvements were observed in NITBUT (OD [baseline: 5.2± 1.97; month 12: 7.0± 3.68; change: 1.9± 3.69, p< 0.0001]; OS [baseline: 5.6± 1.96; month 12: 7.9± 4.58; change: 2.3± 4.59, p< 0.0001]) and IDEEL-SB score (p< 0.0001). Corneal staining reduced significantly from baseline to 12 months (OD [baseline: 2.1± 2.96; month 12: 0.7± 1.56; change: − 1.4± 2.65, p< 0.0001]; OS [baseline: 2.1± 2.94; month 12: 0.7± 1.44; change: − 1.4± 2.75, p< 0.0001]). Improvements in MGS, NITBUT, IDEEL-SB module score, and corneal staining were seen as early as week 2, and at months 1, 3, 6, and 9 (all p< 0.001).
Conclusion: A single treatment with iLux significantly improved clinical parameters of MGS, NITBUT, and corneal staining, and patient-reported symptom assessment with IDEEL-SB in patients with MGD over 12 months.
Keywords: corneal staining, meibomian gland dysfunction, meibomian gland score, tear break-up time
Introduction
Meibomian gland dysfunction (MGD), which contributes to evaporative dry eye, is the leading cause of dry eye disease.1 The prevalence estimates of MGD range from 3.5% to 69.3% and this wide variation is attributed to differences in geographic region, age distribution, and specific clinical signs used to define MGD.2 MGD is a chronic abnormality of meibomian glands and generally characterized by obstruction of terminal ducts and/or changes in glandular secretions (qualitative/quantitative).3 Epithelial hyperkeratinization and increased meibum viscosity lead to duct obstruction, cystic dilation, acinar cell atrophy, and gland dropout.4–6 As a result, tear film alteration, eye irritation, inflammation, and ocular surface disease may occur.3 MGD symptoms can have a substantial impact on patients’ quality of life.7
Treatments for MGD include: (1) eyelid hygiene (including warming/massage/expression), which is the mainstay therapy; (2) medical treatment such as antibiotics, non-steroidal and steroidal anti-inflammatory agents, hormone therapy, and treatment of Demodex infestation; (3) surgical options/procedures, such as intraductal meibomian gland probing, thermal pulsation devices, intense pulsed light therapy, and intranasal tear neurostimulation; and (4) supplements including topical lipids and oral essential fatty acid supplementation.7–10
The melting point of normal meibum ranges from 10°C to 40°C; however, this is increased in MGD and may lead to impaired spreading of meibum and increased evaporation of the tear film.11,12 Thus, the treatment of MGD generally focuses on application of external heat and pressure, which helps in melting meibum and increasing secretion.13 Although self-treatments such as warm compress and eyelid massage are the first steps in MGD treatment, patient compliance is generally low and some patients may not achieve long-lasting improvement in symptoms.13 In such cases, in-office eyelid heating therapy, such as thermal pulsation systems, are a good alternative.13 These devices apply heat at appropriate temperature and compress the meibomian glands simultaneously, to facilitate the release of contents into the tear film.14 Thermal pulsation therapies, such as LipiFlow and Systane iLux, have been reported to be highly efficient, with the effects lasting for up to 12 months.15–17
The Systane iLux MGD treatment system (Alcon, Fort Worth, TX, USA) is a handheld, thermal pulsation device.18 Two recent studies have compared Systane iLux and LipiFlow treatments in patients with MGD.17,18 Both devices were reported to significantly improve MGD signs and symptoms, over 4 weeks of treatment.18 Further, Systane iLux was reported to be non-inferior to LipiFlow in improving MGD scores, over 12 months.17 Although previous studies have evaluated Systane iLux,17–19 comprehensive monadic data describing trends in outcomes associated with Systane iLux treatment over the long-term have not been reported so far. Here, we report post-hoc analysis of a previous randomized controlled trial (NCT03956225) to demonstrate the effectiveness of Systane iLux in patients with MGD over 12 months post single treatment.
Materials and Methods
Study Design
This is a post-hoc analysis (not pre-planned) of a prospective, randomized, assessor-masked, parallel-group, multicenter, 12-month, post-approval study that evaluated the effectiveness of Systane iLux and LipiFlow in patients with MGD (NCT03956225). The study details have been published in detail previously.17 In the current post-hoc analysis, we report data on the Systane iLux treatment group from baseline to 12 months.
Study Population
Subjects aged ≥18 years, of any gender or race, with signs and symptoms of evaporative dry eye in both eyes were included. At the screening visit, subjects were required to have meibomian gland score (MGS) ≤1220 in lower eyelids, Impact of Dry Eye on Everyday Life-Symptom Bother (IDEEL-SB) module score >16, and non-invasive tear break-up time (NITBUT) <10 seconds.
Subjects with a history of intraocular/oculo-plastic surgery within the 6 months prior to screening, LipiFlow or Systane iLux treatment (in either eye) in the last 12 months, punctal plugs or punctal occlusion, meibomian gland loss >50% at screening (as indicated by meibography), uncontrolled active systemic diseases that cause dry eye, or those not on a stable dose of any dry eye or MGD medication were excluded.
Treatment
Eligible subjects from 15 sites were randomized (1:1) to receive a single bilateral treatment with either Systane iLux (TearFilm Innovations, Inc., Alcon, Fort Worth, TX, USA) or LipiFlow (Johnson & Johnson Vision, Jacksonville, FL, USA). Subjects attended a total of eight study visits: screening/baseline; treatment; and follow-up visits at 2 weeks, 1 month, 3 months, 6 months, 9 months, and 12 months. Both eyes were treated on the same day. Makeup was removed and anesthetic eye drops were instilled in both eyes before treatment with Systane iLux. The treatment time ranged from 8 to 12 minutes. Both upper and lower lids were treated: upper lid, central-nasal area; lower lid, central-nasal region; lower lid, central-temporal region.
Systane iLux MGD Treatment System
The Systane iLux MGD treatment system is a thermal pulsation, hand-held, battery-powered instrument with a disposable tip. It consists of LEDs that heat the meibum glands from 38°C to 42°C. Temperature sensors in the instrument turn off the LEDs automatically if the inner eyelid exceeds 44°C or outer eyelid exceeds 45°C. The instrument allows viewing of gland orifices and customization of pressure during heating and compression phases.13,18
Outcomes and Measures
In this post-hoc analysis, effectiveness of Systane iLux treatment was measured as mean changes in MGS, NITBUT, IDEEL-SB module score, and corneal staining from baseline to the 12-month follow-up visit (post single treatment with Systane iLux).
MGS was assessed using a Meibomian Gland Evaluator (Johnson & Johnson Vision), while viewing the lower eyelid margin through a slit-lamp biomicroscope. In each eye, a total of 15 glands of the lower lid were evaluated from the nasal, central, and temporal regions. The glands were graded on a scale of 0 to 3 based on the quality of the expressed meibomian fluid (0=no secretion, 1=inspissated, 2=cloudy, 3=clear liquid), with a maximum MGS score of 45 in each eye.16,21 NITBUT was evaluated using the OCULUS Keratograph® 5M. It was performed three times using infrared illumination. The Keratograph 5 M projects a ring pattern from a placido disc onto the tear film surface and detects a disruption automatically. NITBUT first break-up time (the first disruption in the projected placido rings) was recorded in seconds separately for each eye. The IDEEL-SB module comprises 20 questions that measure general dry eye symptoms (over the past two weeks) in patients; scores range from 0 to 100, with higher scores indicating greater bother. Corneal staining was evaluated in five corneal regions (superior, inferior, central, temporal, and nasal), using sodium fluorescein-impregnated strips. The National Eye Institute (NEI) grading scale was used; the grades ranged from 0 to 3 (0=normal, 1=mild, 2=moderate, 3=severe), with a maximum score of 15 in each eye.22
Post-Hoc Statistical Analyses
Descriptive statistics, such as means and standard deviations for continuous variables, and numbers and percentages for categorical variables, were reported for all study measures. The 95% confidence intervals (CIs) and p-values were calculated from analysis of covariance (ANCOVA), with the baseline measurement considered as a covariate for each outcome analyzed. Adjustment for multiplicity was not performed.
Results
Socio-Demographic and Clinical Characteristics
Data from 119 subjects (238 eyes) were evaluated. The mean±SD age of the subjects was 58.4±13.4 years (Table 1). The majority of subjects were female (79.0%), white (86.6%), and non-Hispanic/Latino (95.8%). At baseline, the mean±SD total MGS (combined scores from both eyes) was 6.6±3.68, total NITBUT (combined values from both eyes) was 5.4±1.97 seconds, and IDEEL-SB module score was 55.8±15.93. The corneal staining score was approximately 2.1±2.9 in both eyes (Table 1).
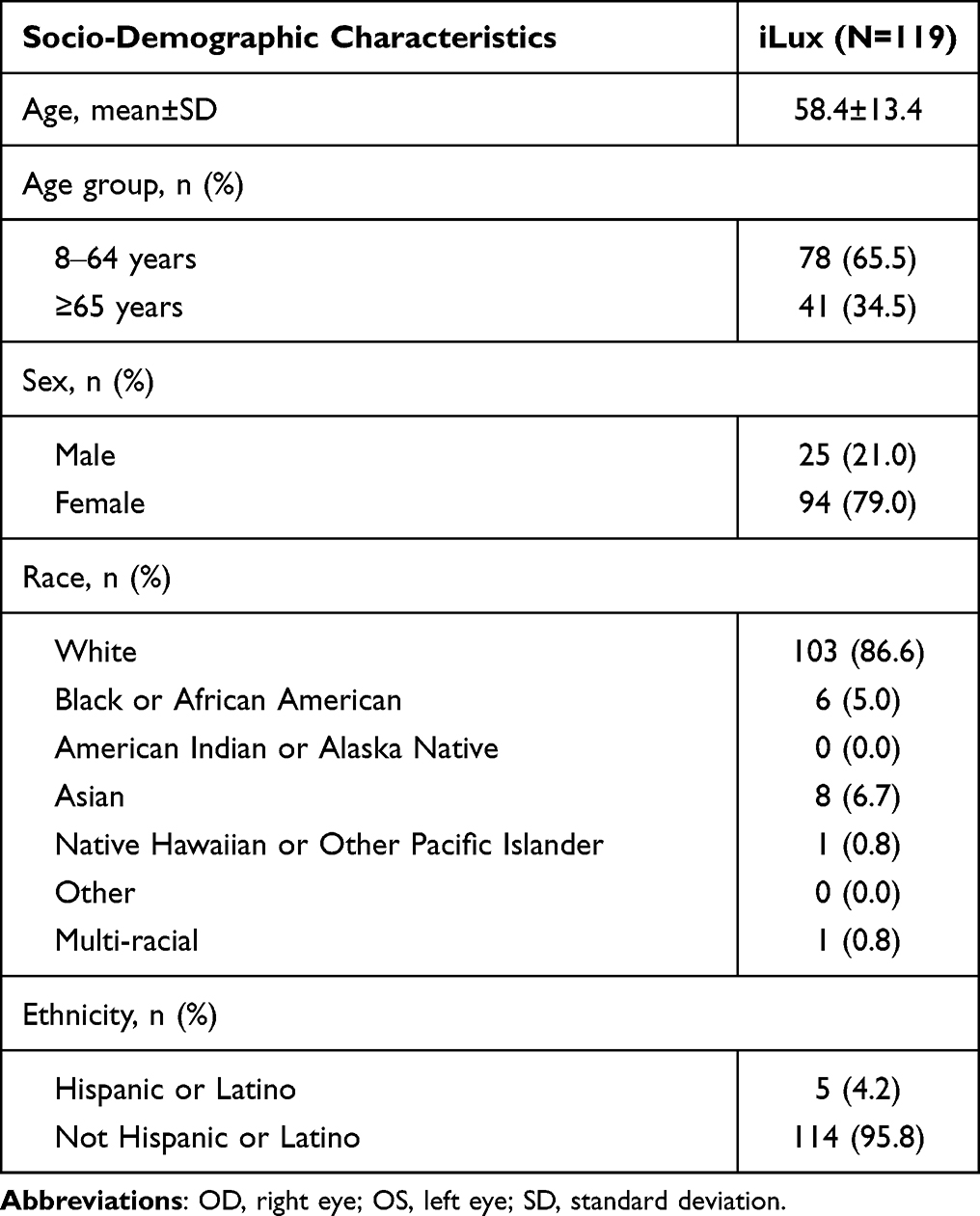 |
Table 1 Baseline Socio-Demographic and Clinical Characteristics of the Study Subjects |
Change in MGS from Baseline to 12 Months Post-Treatment
The MGS (mean±SD) for both left (OS) and right (OD) eyes improved significantly from baseline to 12 months (OD [baseline: 6.9±3.69; month 12: 22.8±11.31; change from baseline: 15.9±11.57, p<0.0001]; OS [baseline: 6.4±3.66; month 12: 23.0±11.33; change from baseline: 16.7±11.40, p<0.0001]) (Table 2). Furthermore, for both eyes, significant improvement in MGS from baseline was observed as early as week 2, as well as at month 1, month 3, month 6, and month 9 (all p<0.0001).
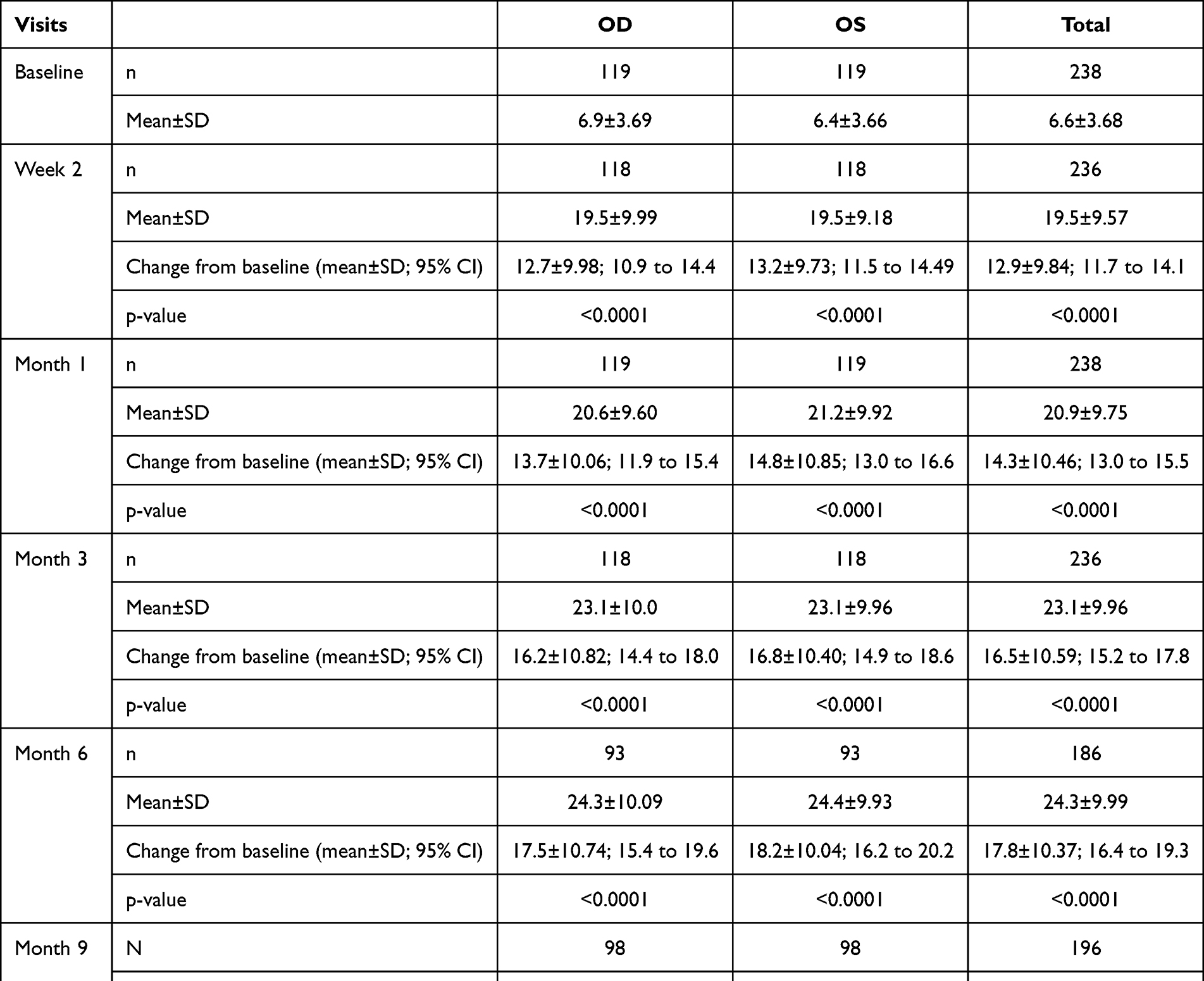 |
Table 2 Meibomian Gland Scores at Baseline and Post-Treatment Follow-Up Visits |
A similar trend was observed for the total MGS; the score improved significantly from baseline to 12 months (p<0.0001), and at all other visits post-treatment (week 2, month 1, month 3, month 6, and month 9; all p<0.0001) (Table 2).
Change in NITBUT from Baseline to 12 Months Post-Treatment
NITBUT (first break-up time; mean±SD; seconds) for both eyes improved significantly from baseline to 12 months (OD [baseline: 5.2±1.97; month 12: 7.0±3.68; change from baseline: 1.9±3.69, p<0.0001]; OS [baseline: 5.6±1.96; month 12: 7.9±4.58; change from baseline: 2.3±4.59, p<0.0001]) (Table 3). Furthermore, for both eyes, significant improvement in NITBUT from baseline was observed as early as week 2, as well as at month 1, month 3, month 6, and month 9 (all p<0.001).
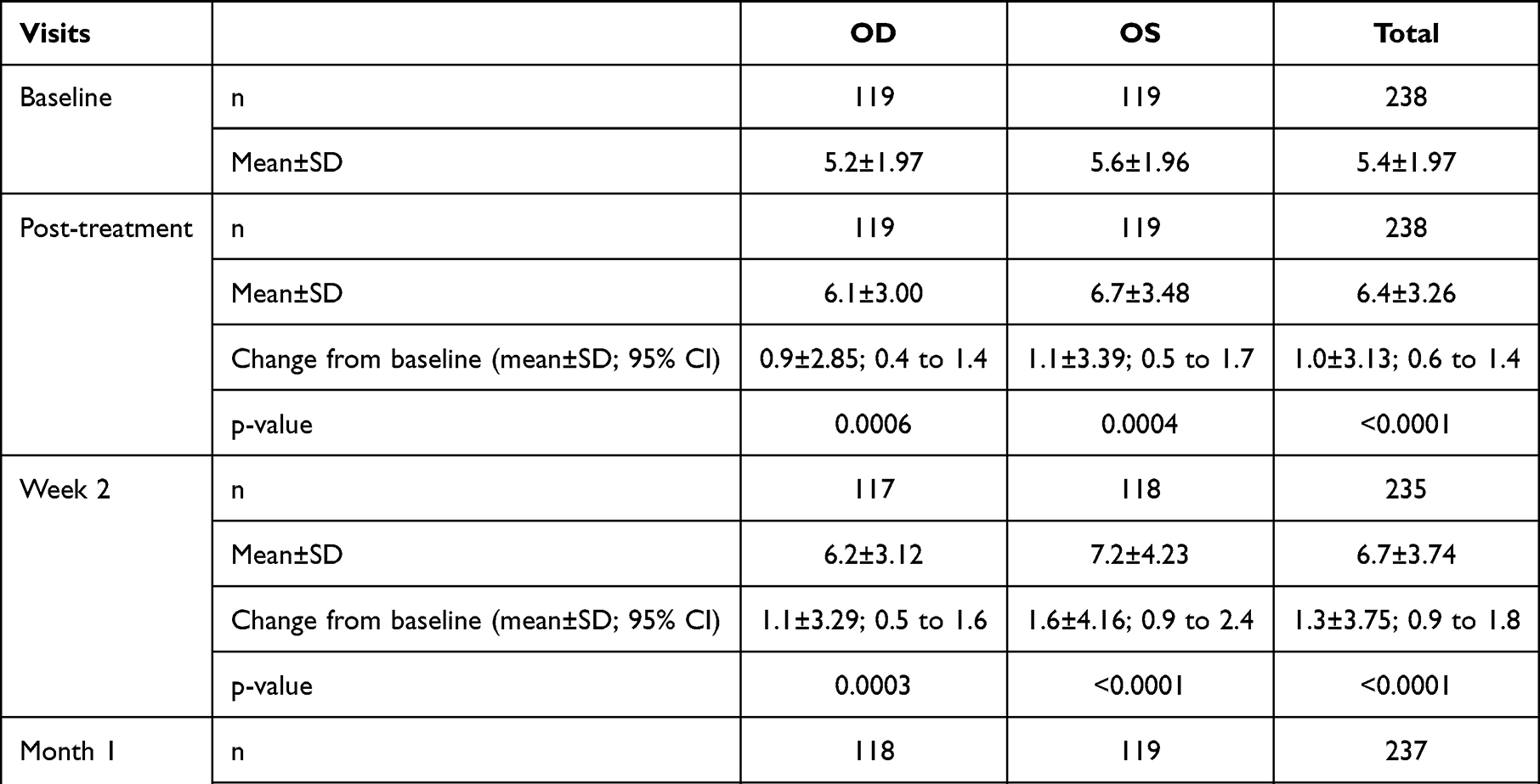 |
Table 3 Non-Invasive Tear Break-Up Time (First Break-Up Time) at Baseline and Post-Treatment Follow-Up Visits |
Similarly, the total NITBUT improved significantly from baseline to 12 months (p<0.0001); the improvement was also observed at all other visits post-treatment (week 2, month 1, month 3, month 6, and month 9; all p<0.0001) (Table 3).
Change in IDEEL-SB from Baseline to 12 Months Post-Treatment
The total IDEEL-SB score (mean±SD) improved significantly from baseline to 12 months (baseline: 55.8±15.93; month 12: 34.3±16.65; change from baseline: −21.1±16.46; p<0.0001). Significant improvement in total IDEEL-SB score from baseline was also observed at all other visits post-treatment (week 2, month 1, month 3, month 6, and month 9; all p<0.0001) (Table 4).
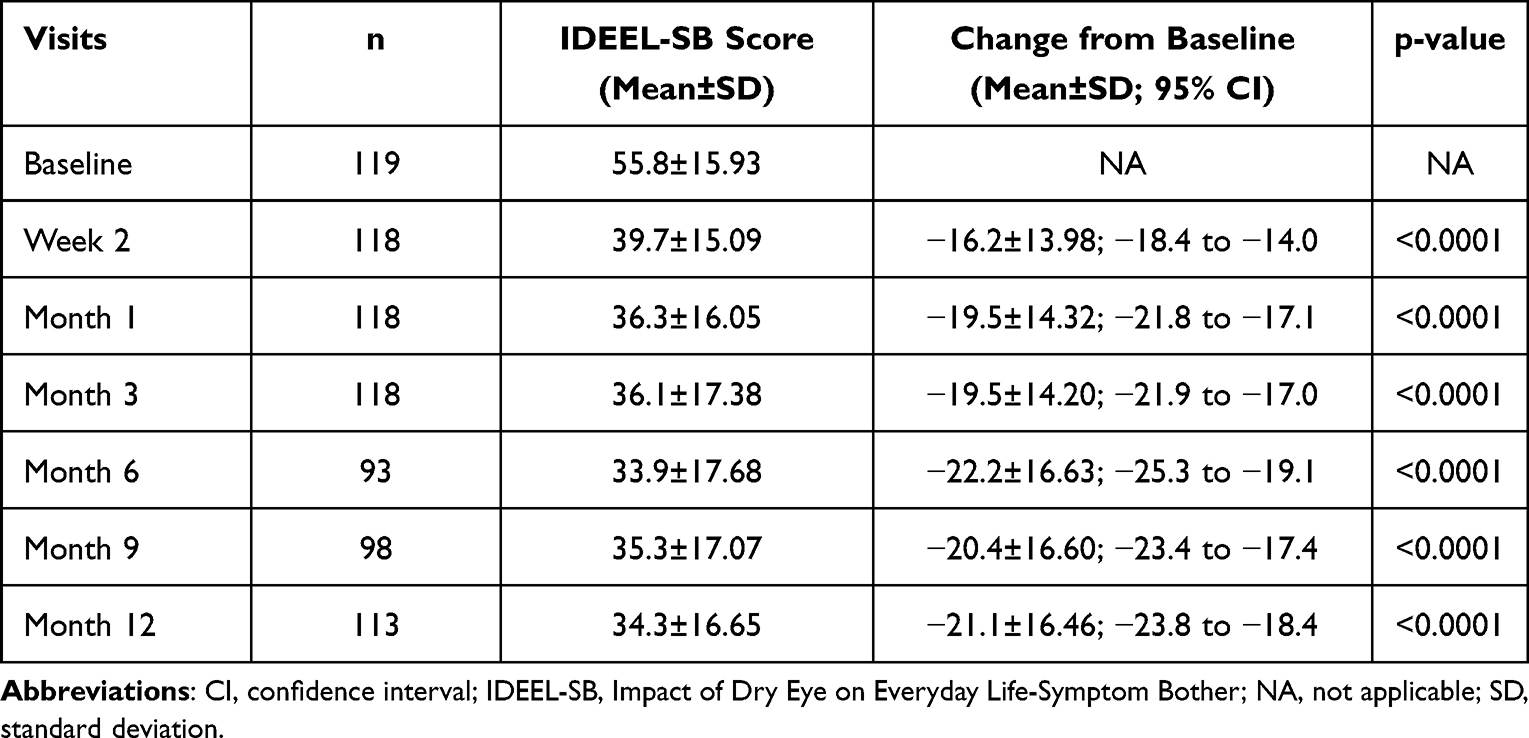 |
Table 4 Impact of Dry Eye on Everyday Life-Symptom Bother at Baseline and Post-Treatment Follow-Up Visits |
Change in Corneal Staining from Baseline to 12 Months Post-Treatment
Corneal staining scores (mean±SD) for both eyes reduced significantly from baseline to 12 months (OD [baseline: 2.1±2.96; month 12: 0.7±1.56; change from baseline: −1.4±2.65, p<0.0001]; OS [baseline: 2.1±2.94; month 12: 0.7±1.44; change from baseline: −1.4±2.75, p<0.0001]) (Table 5). Furthermore, for both eyes, a significant reduction in corneal staining scores from baseline was observed as early as week 2, as well as at month 1, month 3, month 6, and month 9 (all p<0.0001).
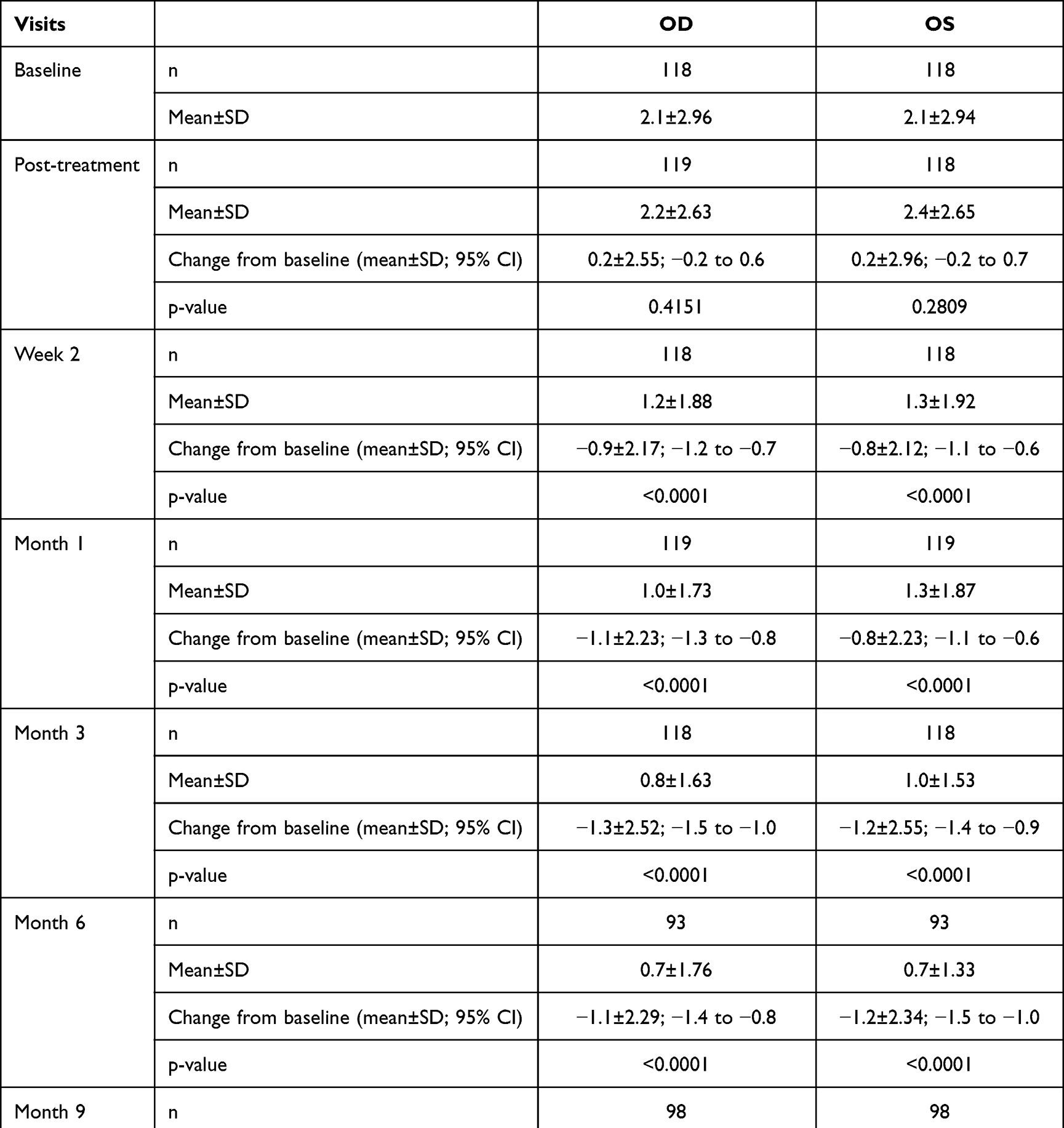 |
Table 5 Corneal Staining Scores at Baseline and Post-Treatment Follow-Up Visits |
Discussion
Thermal pulsation systems, such as Systane iLux, have been shown to substantially improve signs and symptoms of MGD up to 4 weeks after treatment.18,19 Systane iLux has been reported to be non-inferior to LipiFlow in treating MGD, post single treatment, in a 12-month randomized controlled trial.17 The current post-hoc analysis of the previous randomized trial17 was conducted to provide comprehensive monadic data on long-term Systane iLux effectiveness. Our results demonstrated that a single treatment with Systane iLux significantly improved outcomes in patients with MGD, over 12 months of follow-up. Specifically, improvements were noted in the clinical parameters of MGS, NITBUT, and corneal staining, along with patient-reported symptom assessment with the IDEEL-SB.
Significant improvements in MGS and NITBUT from baseline were seen in both eyes as early as 2 weeks and the effects were sustained for 12 months. These results are similar to previous studies that reported improvement in MGS and tear break-up time over 4 weeks.18,19 The improvement of approximately 16 points in MGS in the current analysis (at 12 months) was similar to the improvement observed in the Tauber et al study (17 points, at 4 weeks) and the Schanzlin et al study (14 points, at 4 weeks).18,19 Further, the improvement of approximately 2 seconds in NITBUT in the current analysis (at 12 months) was similar to the tear break-up time (TBUT) improvement observed in the Tauber et al study (3 seconds, at 4 weeks) but lower than the Schanzlin et al study (4.5 seconds, at 4 weeks); however, the comparisons may be limited due to the differences in NITBUT versus invasive TBUT.18,19 Our study findings demonstrate that the trends in outcomes associated with Systane iLux extend beyond 4 weeks and are sustained over 12 months.
For the patient-reported outcome measure of symptoms with the IDEEL-SB questionnaire, a difference of 12 points is considered to be clinically significant.23 The current analysis revealed a substantial decrease in IDEEL-SB scores from baseline to week 2 and up to month 12, ranging from 16- to 22-point reduction; these results indicate a clinically meaningful reduction. The improvement in subjective symptom scores in our study is similar to previous studies that reported improvement in Ocular Surface Disease Index (OSDI) and Standard Patient Evaluation of Eye Dryness (SPEED) scores.18,19 Further, in our analysis, corneal staining reduced significantly from baseline to 12 months in both eyes, similar to previous studies,18,19 indicating improvements in ocular surface with a single treatment of Systane iLux.
In the current analysis, the effectiveness of Systane iLux was observed early, even at 2 weeks after treatment; this suggests potential benefits of Systane iLux in patients requiring quick relief, such as those with severe dry eye disease or those planning cataract or refractive surgeries.19 MGD treatments that stabilize the tear film rapidly and improve ocular surface health may help with providing accurate keratometry measurements and pre-surgical planning.19,24
MGD signs and symptoms improvement observed in this study indicate that subjects with MGD may have gland obstruction and/or altered meibum composition that prevents meibum secretion into the tear film. Systane iLux facilitates melting of meibum and improves secretion onto the ocular surface by applying heat and pressure simultaneously to the eyelids.18 Thus, Systane iLux treatment may be more convenient and time-efficient than eyelid heating devices that require a separate step of manual meibomian gland expression.19
In summary, the results of the post-hoc analysis demonstrate that a single treatment with Systane iLux is effective in improving signs and symptoms of MGD over 12 months.
The current analysis had a few limitations. As this was only an assessor-masked study, there could have been a potential bias in unmasked results on the IDEEL-SB questionnaire. The subjective symptom scores (IDEEL-SB) may have been influenced by the better eye and/or worse eye. However, this influence might have been minimal since the objective assessments of MGS, NITBUT, and corneal staining were similar for both left and right eyes. Further, since the subjects were not stratified based on baseline symptom severity, effects of Systane iLux across varying disease severity was not assessed. At-home therapies, such as warm compresses and artificial tears, were not monitored, which may have impacted the results. Further, since this post-hoc analysis evaluated the effectiveness of only Systane iLux over 12 months, any control group comparison was not made.
Conclusion
This post-hoc analysis demonstrated that Systane iLux is effective in improving signs and symptoms of MGD over 12 months after a single treatment. Improvement in MGS, NITBUT, corneal staining scores, and IDEEL scores were observed as early as 2 weeks and sustained over 12 months.
Data Sharing Statement
Due to varying rights of individuals and contractual rights of parties involved, Alcon does not make a practice of sharing datasets.
Acknowledgments
Writing, editorial support, and formatting assistance was provided by Veeri Rajendra Babu, PhD, and Sudha Korwar, PhD, Indegene Pvt. Ltd., Bangalore, India, which was contracted and funded by Alcon. This paper was presented at the American Optometric Association (AOA) Optometry’s Meeting® 2022 as a poster presentation with interim findings. The poster’s abstract was published on the AOA website.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Alcon Research, LLC.
Disclosure
GW is a consultant for Alcon, Aerie, Allergan, Bausch, BioTissue, CooperVision, Johnson & Johnson, OcuSoft, Optovue, Orasis, and Tarsus Medical. CH is an educational consultant for Valley Contax and reports grants from Alcon during the conduct of the study. SM and BF are consultants for Alcon. JT and JM were paid as clinical investigators with a research grant from Alcon. DK was paid as a researcher for Alcon and reports payment for research from Specialty Eyecare Group and Johnson & Johnson. KB reports compensation as an investigator for this study by Alcon. JD, BG, and DL have no financial interests to disclose. SK has received speaking, consulting and research fees from AbbVie, Alcon, Bausch and Lomb, Essilor, Johnson & Johnson, Kala, Sun, Osmotica, Tear Care, and Vision Source. SK is also an investigator in a study for Alcon on thermal pulsation for meibomian gland disease. SS and TNY are employees of Alcon. The authors report no other conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Schaumberg DA, Nichols JJ, Papas EB, Tong L, Uchino M, Nichols KK. The international workshop on meibomian gland dysfunction: report of the subcommittee on the epidemiology of, and associated risk factors for, MGD. Investig Ophthalmol Vis Sci. 2011;52(4):1994–2005. doi:10.1167/iovs.10-6997e
3. Daniel nelson J, Shimazaki J, Benitez-del-Castillo JM, et al. The international workshop on meibomian gland dysfunction: report of the definition and classification subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):1930–1937. doi:10.1167/iovs.10-6997b
4. Chhadva P, Goldhardt R, Galor A. Meibomian gland disease. Ophthalmology. 2017;124(11):S20–S26. doi:10.1016/j.ophtha.2017.05.031
5. Liu S, Richards SM, Lo K, Hatton M, Fay A, Sullivan DA. Changes in gene expression in human meibomian gland dysfunction. Investig Opthalmology Vis Sci. 2011;52(5):2727. doi:10.1167/iovs.10-6482
6. Baudouin C, Messmer EM, Aragona P, et al. Revisiting the vicious circle of dry eye disease: a focus on the pathophysiology of meibomian gland dysfunction. Br J Ophthalmol. 2016;100(3):300–306. doi:10.1136/bjophthalmol-2015-307415
7. Sabeti S, Kheirkhah A, Yin J, Dana R. Management of meibomian gland dysfunction: a review. Surv Ophthalmol. 2020;65(2):205–217. doi:10.1016/j.survophthal.2019.08.007
8. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Investig Ophthalmol Vis Sci. 2011;52(4):2050–2064. doi:10.1167/iovs.10-6997g
9. Maskin SL. Intraductal meibomian gland probing relieves symptoms of obstructive meibomian gland dysfunction. Cornea. 2010;29(10):1145–1152. doi:10.1097/ICO.0b013e3181d836f3
10. Greiner JV. A single LipiFlow® thermal pulsation system treatment improves meibomian gland function and reduces dry eye symptoms for 9 months. Curr Eye Res. 2012;37(4):272–278. doi:10.3109/02713683.2011.631721
11. Butovich IA, Lu H, McMahon A, et al. Biophysical and morphological evaluation of human normal and dry eye meibum using hot stage polarized light microscopy. Investig Opthalmology Vis Sci. 2014;55(1):87. doi:10.1167/iovs.13-13355
12. Willcox MDP, Argüeso P, Georgiev GA, et al. TFOS DEWS II tear film report. Ocul Surf. 2017;15(3):366–403. doi:10.1016/j.jtos.2017.03.006
13. Beining M, Magno M, Moschowits E, et al. In-office thermal systems for the treatment of dry eye disease. Surv Ophthalmol. 2022;67:1405–1418. doi:10.1016/j.survophthal.2022.02.007
14. Valencia-Nieto L, Novo-Diez A, Blanco-Vázquez M, López-Miguel A. Therapeutic instruments targeting meibomian gland dysfunction. Ophthalmol Ther. 2020;9(4):797–807. doi:10.1007/s40123-020-00304-3
15. Greiner JV. Long-term (12-month) Improvement in meibomian gland function and reduced dry eye symptoms with a single thermal pulsation treatment. Clin Exp Ophthalmol. 2013;41(6):524–530. doi:10.1111/ceo.12033
16. Blackie CA, Coleman CA, Holland EJ. The sustained effect (12 months) of a single-dose vectored thermal pulsation procedure for meibomian gland dysfunction and evaporative dry eye. Clin Ophthalmol. 2016;10:1385–1396. doi:10.2147/OPTH.S109663
17. Wesley G, Bickle K, Downing J, et al. Comparison of two thermal pulsation systems in the treatment of meibomian gland dysfunction. Optom Vis Sci. 2022;99:323–332. doi:10.1097/OPX.0000000000001892
18. Tauber J, Owen J, Bloomenstein M, Hovanesian J, Bullimore MA. Comparison of the iLUX and the lipiflow for the treatment of meibomian gland dysfunction and symptoms: a randomized clinical trial. Clin Ophthalmol. 2020;14:405–418. doi:10.2147/OPTH.S234008
19. Schanzlin D, Owen JP, Klein S, Yeh TN, Merchea MM, Bullimore MA. Efficacy of the systane iLux thermal pulsation system for the treatment of meibomian gland dysfunction after 1 week and 1 month. Eye Contact Lens Sci Clin Pract. 2021. doi:10.1097/ICL.0000000000000847
20. Korb DR, Blackie CA, Paul LE, Solomon JD. Distribution of meibomian glands yielding liquid secretion by section of the lower lid. Invest Ophthalmol Vis Sci. 2008;49(13):85.
21. Lane SS, Dubiner HB, Epstein RJ, et al. A new system, the LipiFlow, for the treatment of meibomian gland dysfunction. Cornea. 2012;31(4):396–404. doi:10.1097/ICO.0b013e318239aaea
22. Lemp MA. Report of the national eye institute/industry workshop on clinical trials in dry eyes. CLAO J. 1995;21(4):221–232.
23. Fairchild CJ, Chalmers RL, Begley CG. Clinically important difference in dry eye: change in IDEEL-symptom bother. Optom Vis Sci. 2008;85(8):29–34. doi:10.1097/OPX.0b013e3181824e0d
24. Matossian C. Impact of thermal pulsation treatment on astigmatism management and outcomes in meibomian gland dysfunction patients undergoing cataract surgery. Clin Ophthalmol. 2020;14:2283–2289. doi:10.2147/OPTH.S263046
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.