")
Back to Journals » Cancer Management and Research » Volume 11
Survival advantage and clinicopathological significance of microRNA-22 in cancers: a meta-analysis
Authors Xiang Q, Xiang Z, Dou R , Xiong B
Received 23 August 2018
Accepted for publication 23 July 2019
Published 8 October 2019 Volume 2019:11 Pages 8855—8868
DOI https://doi.org/10.2147/CMAR.S185124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Qingming Xiang,1,* Zhenxian Xiang,2,* Rongzhang Dou,2 Bin Xiong2
1Department of Radiation and Medical Oncology, Zhongnan Hospital of Wuhan University, Hubei Key Laboratory of Tumor Biological Behaviors & Hubei Cancer Clinical Study Center, Wuhan 430071, People’s Republic of China; 2Department of Oncology, Zhongnan Hospital of Wuhan University, Hubei Key Laboratory of Tumor Biological Behaviors & Hubei Cancer Clinical Study Center, Wuhan 430071, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Xiong
Department of Oncology, Zhongnan Hospital of Wuhan University, Hubei Key Laboratory of Tumor Biological Behaviors & Hubei Cancer Clinical Study Center, No. 169 Donghu Road, Wuchang District, Wuhan 430071, Hubei Province, People’s Republic of China
Tel +86 0 276 781 3152
Email [email protected]
Abstract: An increasing number of studies revealed that microRNA-22 as a biomarker may play a significant role in the cancer patients’ prognosis, but the accurate prognosis value of microRNA-22 remains somewhat controversial. Thus, we comprehensively searched the database and performed this study to explicate the accurate value of microRNA-22 in the cancer patients’ prognosis. This meta-analysis revealed that elevated expression of microRNA-22 correlated with good overall survival (OS) and disease-free survival (DFS)/progression-free survival (PFS)/recurrence-free survival (RFS) in cancers, while no significant association was found in metastasis-free survival (MFS)/distant metastasis-free survival (DMFS). Through the subgroup analysis for OS and DFS/PFS/RFS, we found that elevated expression of miR-22 significantly correlated with good prognosis in most subgroups, while it predicted a worse prognosis in nasopharyngeal carcinoma subgroup. And besides that, elevated expression of miR-22 was negatively correlated with TNM stage, lymph node metastasis, distant metastasis and recurrence, while no significant association was found between microRNA-22 expression and T stage, tumor differentiation, and lymphatic invasion. Our meta-analysis demonstrated that elevated expression of microRNA-22 predicted a good OS and DFS/PFS/RFS in cancer patients; meanwhile, its high expression also means earlier TNM stage, and lower likelihoods of lymph node metastasis, of distant metastasis and of recurrence. If we regularly monitor miR-22 expression in cancer patients, it might be useful for us to predict cancer prognosis in future clinical applications.
Keywords: hsa-miR-22, cancer, prognosis, clinicopathological, biomarker, meta-analysis
Introduction
Due to the growth of population, the deterioration of the environment and unhealthy lifestyle, cancer has become the leading cause of death worldwide for a long time, and the incidence of cancer has increased substantially in recent years.1 Despite the extensive use of surgical operations, radiotherapy, chemotherapy, hormone treatment and biological treatment, the prognosis in most cancers remains unsatisfactory.2,3 Thus, it is of great clinical value for researchers to find valuable prognosis indicators, which may help doctors promote early prognostic classification and find novel therapy strategy for cancer patients. Among them, microRNAs have been an attractive direction of research in recent years.
MicroRNAs, approximately 22–25 nucleotides in length and abundant among plants, animals and even viruses,4,5 belong to a single-stranded noncoding RNA. The sequence of most microRNAs is highly conserved, but not all. In fact, a substantial portion of microRNAs in many species is species specific.6–9 The microRNAs of animals and most plants exert their regulatory effect by base-pairing with the 3ʹ-untranslated region of target mRNA and inhibiting target gene translation to protein,10 leading to mRNA degradation or translational inhibition.5,11 Unlike animal miRNAs, some plant miRNAs can pair with genic regions that are not in 3′UTRs and direct cleavage of the target gene.12 In various kinds of tumor, the aberrantly expressed miRNAs have been observed,13 and they contribute significantly to many biological processes of the tumor, such as cellular growth, proliferation, apoptosis, development, differentiation, angiogenesis, and metastasis.14,15 Therefore, researchers hold great expectations toward microRNAs as conceivable biomarkers for cancer prognosis.
As a cancer-related microRNA located in chromosome 17 (17p13.3),16 microRNA-22 (miR-22, miRNA-22, hsa-miR-22) was one of the most frequently studied microRNAs, which has been revealed to participate in many biological processes such as cardiac remodeling, cell cycle control,17–19 proliferation, differentiation and apoptosis, and their deregulation is also a forewarning of human cancer.20 Many previous studies have demonstrated a significant association between high miR-22 expression and good prognosis in cancer patients, such as epithelial ovarian cancer (EOC),21–23 hepatocellular carcinoma (HCC),24,25 and breast cancer (BC);26–28 but some studies did not reveal significant association,29 and still others showed a negative correlation.30–32 Thus, we conducted this meta-analysis to clarify the accurate correlation between miR-22 expression and the prognosis, as well as the clinicopathological significance of cancer patients.
Method
We carried out this meta-analysis as per the guidelines of PRISMA criteria.33
Search strategy, inclusion and exclusion criteria
We carefully searched Web of Science, PubMed and Embase to identify relevant literature published until 20 June 2017; gray literature was not found during our meta-analysis. Keywords used in the search strategy were “miR-22 OR miRNA-22 OR microRNA-22 OR hsa-miR-22” (all fields) AND “cancer OR neoplasm OR carcinoma OR tumor” (all fields). We did not employ any advanced limitations during the searching period. The inclusion criteria of this study are as follows: i) the correlation between miR-22 expression levels and cancer patients’ prognosis or clinicopathological significance was studied; (ii the expression level of miR-22 was measured in tumor tissue, serum or urine; iii) the HR for prognostic outcome indicator according to miR-22 expression level either had to be reported or could be calculated from the information presented, and we described the method of analysis in the data extraction in detail;34,35 iv) when several studies used the same sample source, the most accurate and most representative one was chosen, only in this way can we avoid the overlap between cohorts. Finally, articles that fulfilled the aforementioned eligibility criteria were further excluded on the basis of following criteria: i) non-English articles, meeting letters or review articles; ii) not dichotomous variable or human studies and iii) lack of essential information.
Quality assessment
We evaluated the quality of all the articles on the basis of a critical review checklist of the Dutch Cochrane Centre, which was previously described by MOOSE.36,37 The key points of the quality assessment were as follows: i) the country and ethnic composition; ii) clear definition of cutoff value; iii) clear definition of outcome assessment; iv) the measurement method of miR-22; v) the type of cancer and vi) sufficient period of follow-up. Studies were excluded if they did not mention all the key points aforementioned.
Data extraction
The following data were carefully extracted by two investigators independently: i) publications details, including first author and publication year; ii) main characteristic of this study population, including nationality, cancer type, sample number and clinicopathological features; iii) the cutoff value and measurement method of miR-22; iv) HRs of elevated expression levels of miR-22 for overall survival (OS), recurrence-free survival (RFS), disease-free survival (DFS), progression-free survival (PFS), metastasis-free survival (MFS) and distant metastasis-free survival (DMFS) and v) if a study reported the results by both univariate and multivariate analysis, the multivariate analysis was our first choice. Because the multivariate analysis weakens the effects of confounding factors. Additionally, if only Kaplan–Meier curves are available, the methods described by Parmar et al34 and Tierney et al35 were used to calculate HR and 95% CI. The Engauge Digitizer version 9.8 was used to read Kaplan–Meier survival curves and get the data we need, and we repeated this process three times to reduce variability. To reduce reading variability, three researchers read the curves independently and disagreements were discussed among themselves.
Statistical analysis
HR and their 95% CI were used to evaluate the correlation between miR-22 high expression and cancer patients’ prognosis. Generally, a 95% CI of HR completely >1 in the forest plot suggested that elevated expression of miR-22 correlated with poor prognosis of cancer patients. If the 95% CI of HR contains one, it indicates that no significant association exists between miR-22 expression and the cancer patients’ prognosis. In addition, if the pooled HR <1 and 95% CI completely lower than one, the high expression of miR-22 predicted a good OS. We employed the Cochran Q test (significant at P<0.10) and Higgins I2 statistic (ranging from 0% to 100%)38 to test heterogeneity of this meta-analysis, which was considered statistically significant at Pheterogeneity <0.1 or I2>50%. If Pheterogeneity >0.1 and I2<50%, we ignored the influence of heterogeneity, and a fixed-effects model39 was employed to pool the overall result; otherwise, the random-effects model was employed.40 Funnel plot, Begg’s test, and Egger’s test were used to estimate the publication bias (publication bias was statistically significant for P<0.05).41 Sensitivity analysis was performed to evaluate the stability of the results and further seek out the sources of heterogeneity. A two–tailed P<0.05 was considered statistically significant.
Result
Summary of enrolled studies
Using the searching strategy aforementioned, we found 213 articles in PubMed, 500 articles in Embase and 349 articles in Web of Science. Seven hundred and sixty articles remained after duplicates were removed. We excluded 724 articles after glancing over the title, abstract, and main figures; then 10 articles were further removed as per the evaluation of full text (Figure 1). Finally, 26 articles spanning 28 studies, which revealed the correlation between miR-22 expression and cancer patients’ prognosis or clinicopathological significance, were considered qualified for current meta-analysis. In the course of searching, no gray literature was found in these articles. The main characteristics of eligible articles were systematically summarized in Table 1. The 26 included articles covered participants from China, USA and Japan, among whom 5467 participants had OS data, 3534 had DFS/PFS/RFS/DMFS/MFS data and 846 had clinicopathological features data. Studied cancers include HCC, BC, esophageal squamous cell carcinoma, colorectal cancer (CRC), EOC, gastric cancer (GC), osteosarcoma (OST), myelodysplastic syndrome (MDS), nasopharyngeal carcinoma (NPC), renal cell carcinoma, primary plasma cell leukemia, bladder cancer and glioma. Notably, either the mean value or the median value was selected as the cutoff value in most articles.
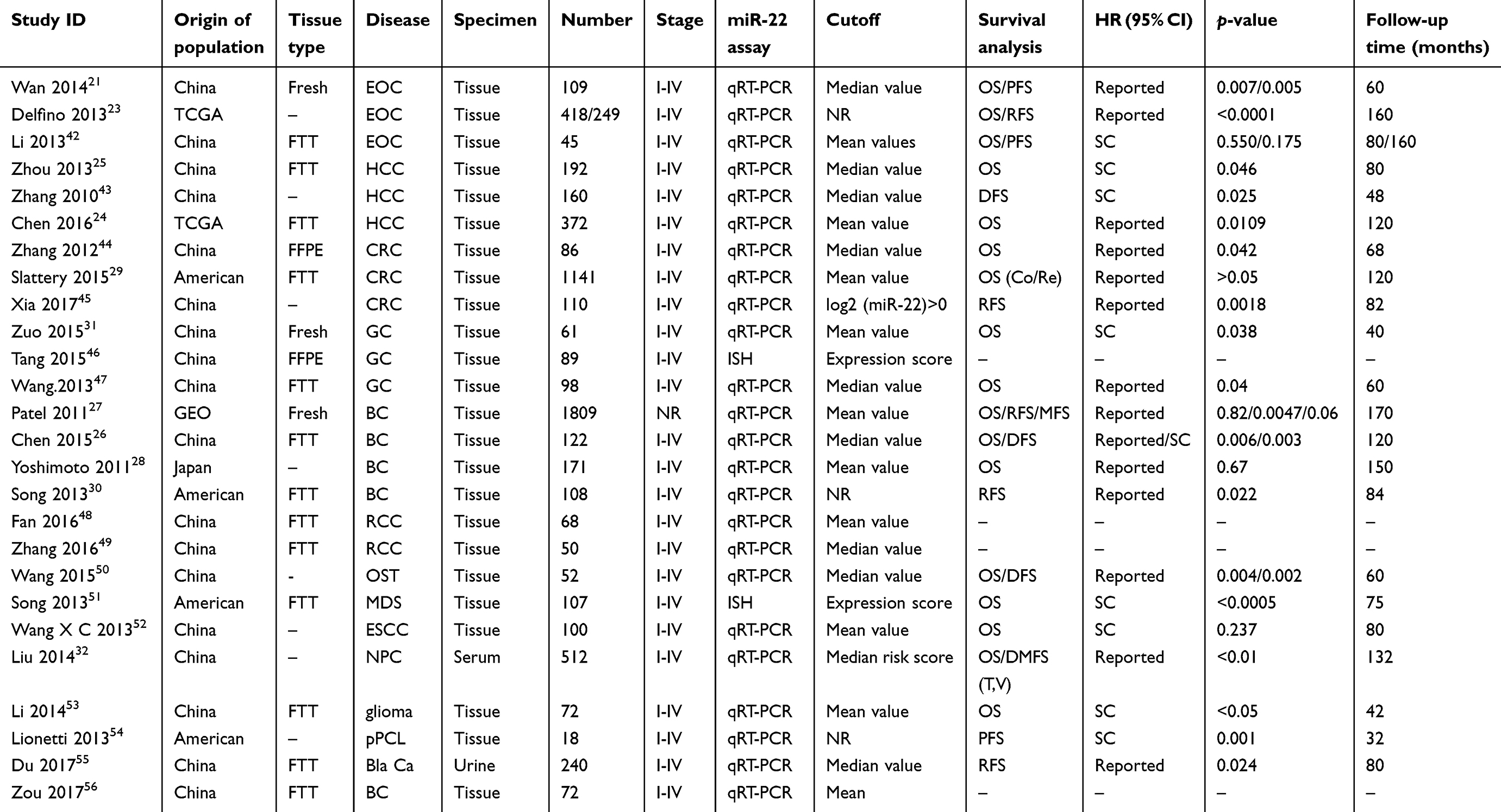 |
Table 1 Main characteristics of 26 studies after screening |
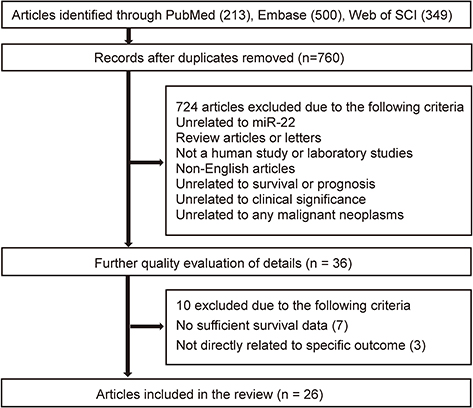 |
Figure 1 Flowchart of the study selection process. |
Relationship between miR-22 expression and OS
Due to obvious heterogeneity among the studies (I2=78.4%), which included 19 studies about OS, a random-effects model was employed to pool all HRs of OS and their 95% CIs. As revealed in Figure 2, high expression of miR-22 represents a good OS of cancer patients (HR =0.76, 95% CI: 0.62–0.92), indicating that patients with high miR-22 expression may have longer survival time.
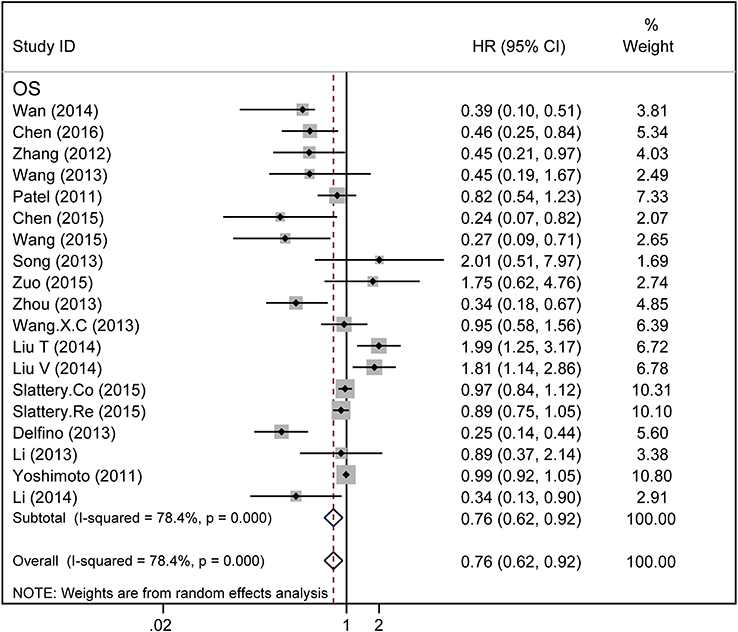 |
Figure 2 Forest plot of miR-22 expression and overall survival in various cancers. |
Afterward, subgroup analyses were performed on the basis of cancer type, the anatomical system of cancer (digestive system and reproductive system), the ethnic background of participants (Asian and Caucasian), the sample type (tissue or serum), the main pathological type (squamous cell carcinoma and adenocarcinoma), tissue preservation method (formalin-fixed paraffin-embedded, frozen tumor tissue, Fresh tissue) and the miR-22 assay method (q-PCR and ISH). As no significant heterogeneity was found among HCC (I2=0.0%), CRC (I2=49.6%) and NPC (I2=0.0%) (Figure S1B, Table 2), a fixed-effects model was employed to pool the HRs of OS. We also pooled the HRs of EOC, GC and BC via random-effects model as a result of significant heterogeneity (Figure S1A, Table 2). According to the subgroup analysis for cancer type, elevated expression of miR-22 predicted a good OS in HCC (HR =0.40, 95% CI: 0.26–0.62) and EOC (HR =0.42, 95% CI: 0.20–0.86) (Table 2); meanwhile, it predicted a worse OS in NPC (HR =1.90, 95% CI: 1.37–2.63). But the prognostic value of miR-22 for GC (HR =0.90, 95% CI: 0.24–3.39), CRC (HR =0.92, 95% CI: 0.83–1.03) and BC (HR =0.81, 95% CI: 0.54–1.22) remains unclear. In addition, we test the conclusion using TCGA data (Figure S5–S9). When grouped as per the anatomical system of cancer, as Figure 3A shows, the combined HRs of the digestive system and of the reproductive system were 0.74 (95% CI: 0.58–0.95) and 0.55 (95% CI: 0.33–0.93), respectively, indicating that miR-22 was indicator of good prognosis in the digestive system and reproductive system. In the subgroup analysis by the ethnic background of participants, there was no obvious association between elevated expression of microRNA-22 and good prognosis in the Asian group (Figure S1D, Table 2) and the Caucasian group (Figure S1C, Table 2). Among the 19 studies, 14 articles recruited patients with adenocarcinoma and three articles recruited patients with squamous cell carcinoma. Therefore, subgroup analysis was performed in adenocarcinoma and squamous cell carcinoma. The results revealed that elevated expression of miR-22 was related with good survival outcome in adenocarcinoma (HR =0.75, 95% CI: 0.61–0.92), while no significant correlation was found in squamous cell carcinoma (HR =1.52, 95% CI: 0.97–2.37) (Figure 3B, Table 2). Subgroup analysis was also carried out on the basis of sample type, namely, tissue and serum. The results suggested that increased expression of miR–22 indicated a good prognosis in tissue, while it predicted a worse OS in serum (Figure 3C, Table 2). Subgroup analysis was further performed according to the preservation method of tumor tissue, while no significant association was found in these subgroups other than FFPE (Figure S4), which indicated that miR-22 predicted a good OS in FFPE subgroup (Table 2). Additionally, we also found a significant correlation between miR–22 expression and OS in q-PCR assay subgroup, while no significant association was found in the ISH assay subgroup (Figure 3D, Table 2).
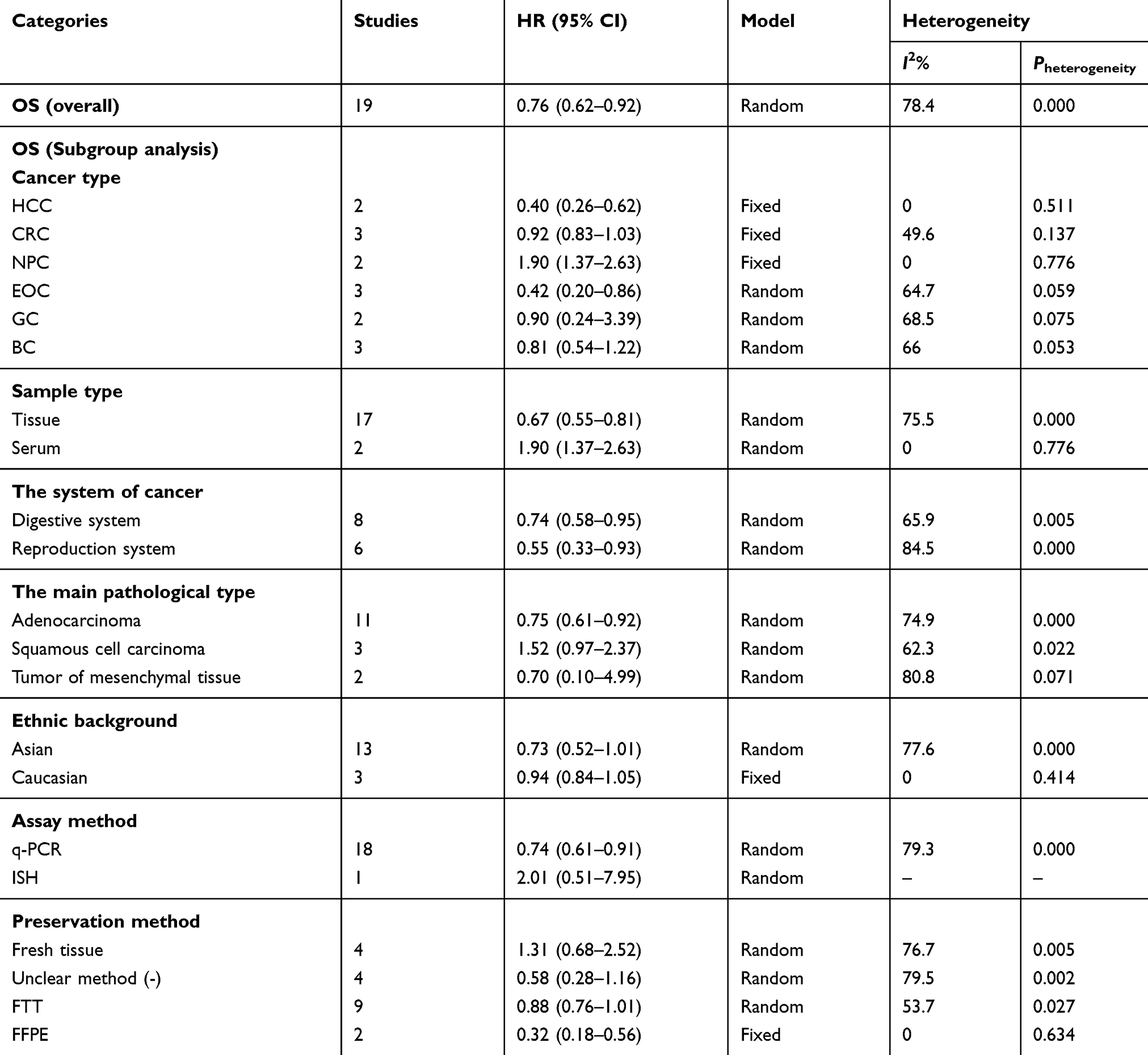 |
Table 2 Meta-analysis of overall and subgroup analysis for miR-22 expression and OS in cancers |
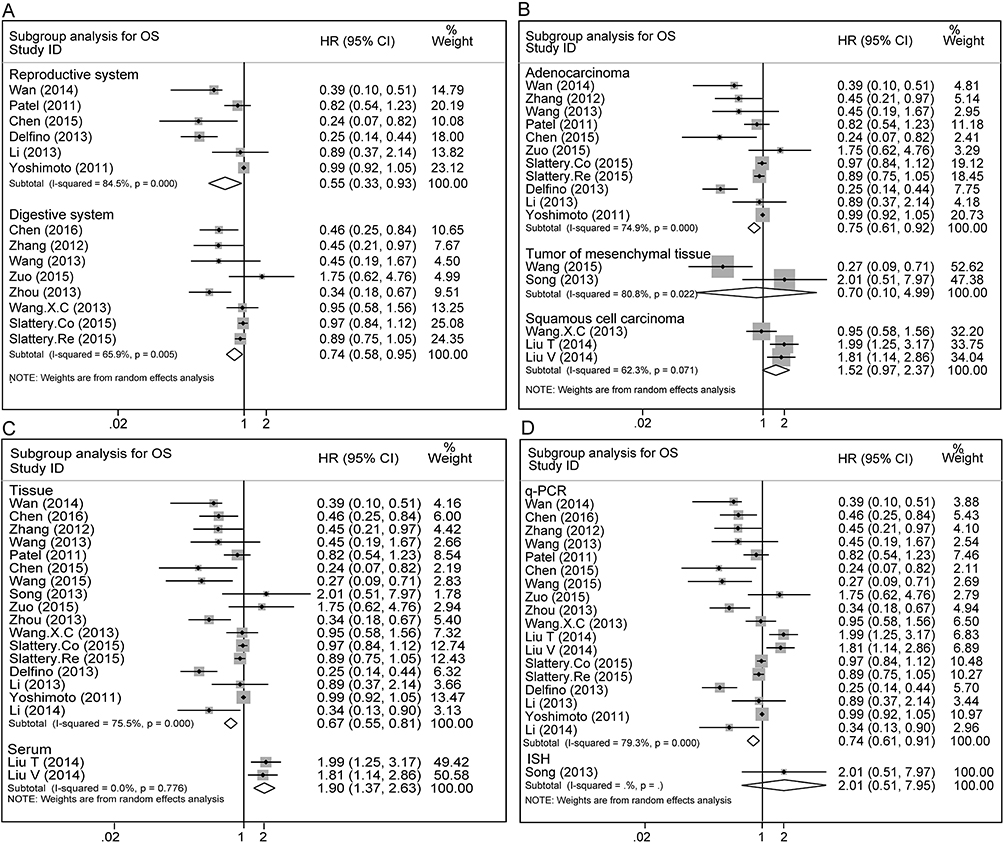 |
Figure 3 Forest plot of subgroup analysis for OS: (A) subgroup analysis for the anatomy system of cancer (digestive system and reproduction system); (B) subgroup analysis for the main pathological type of cancer; (C) subgroup analysis for different sample type (tissue or serum); (D) subgroup analysis for different assay method for miR-22 expression (q-PCR and ISH). |
The relationship between miR-22 expression and disease progression
Among the 26 articles, 12 articles, which include 14 studies and 3534 participants, investigated the correlation between miR-22 expression and PFS/RFS/DFS/DMFS/MFS; hence we performed a meta-analysis among them. Because PFS, RFS, and DFS were similar as outcome indicators, we regard the PFS, RFS, and DFS as the same outcome indicators, so that we can pool more HRs of PFS/RFS/DFS in this meta-analysis to get a more accurate result about the miR-22 expression and disease progress. We pooled the HR of PFS, DFS, and RFS by random-effects model given the significant heterogeneity (I2=79.1%). The results revealed that high expression of miR-22 indicated a longer PFS/DFS/RFS of cancer patients (HR =0.57, 95% CI: 0.37–0.87), indicating that high miR-22 expression prevented the progress and recurrence of cancer (Figure 4A, Table 3). Due to significant heterogeneity, we pooled the MFS/DMFS via random-effects model. As shown in Figure 4A, no significant correlation was found between miR-22 expression and DMFS/MFS with a pooled HR of 1.57 (0.67–3.68) (Figure 4A, Table 3).
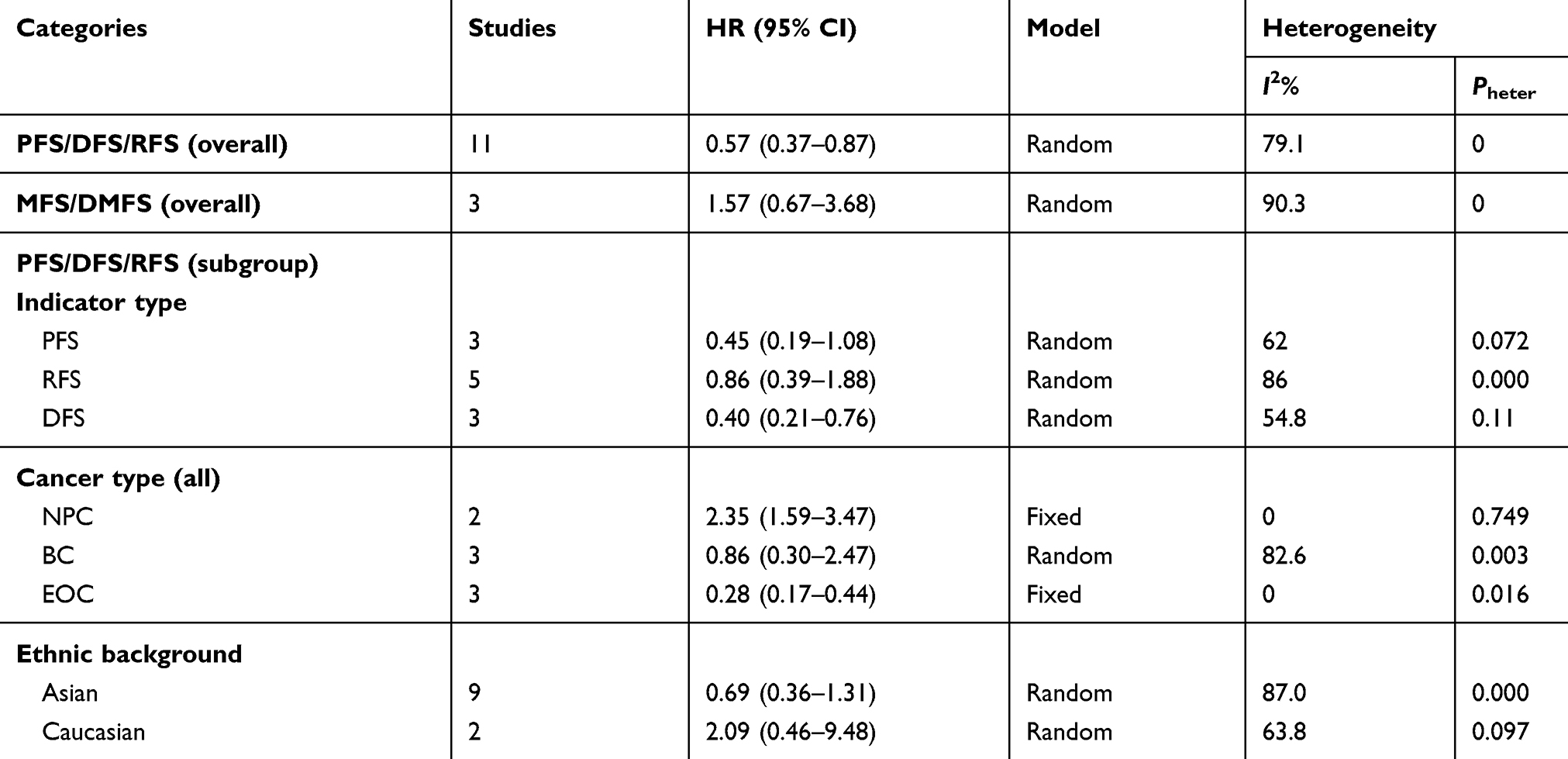 |
Table 3 Meta-analysis of overall and subgroup analysis for miR-22 expression and disease progress in cancers |
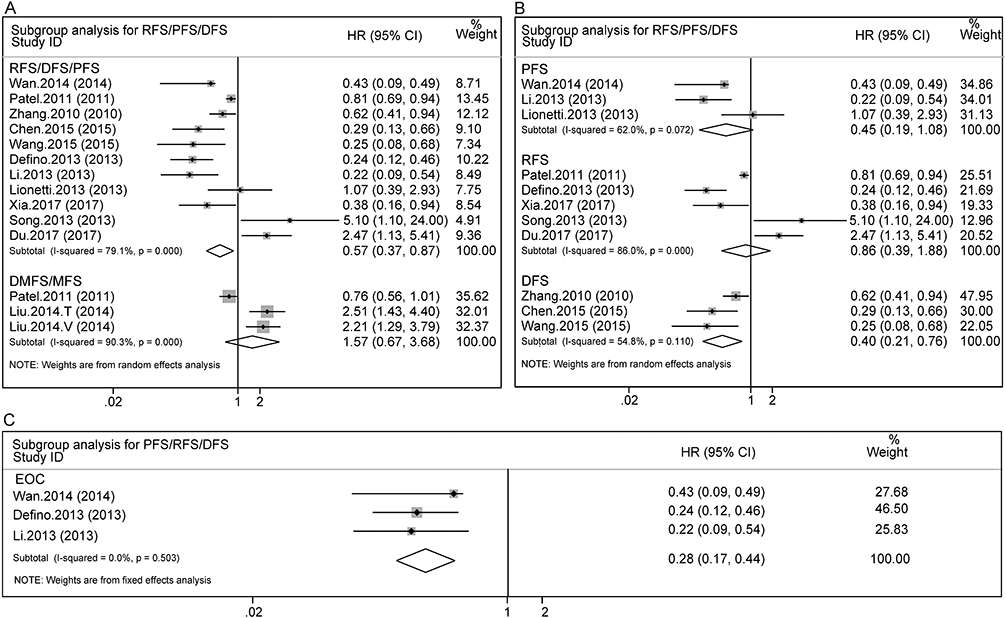 |
Figure 4 Forest plot of miR-22 expression and disease progress: (A) subgroup analysis for PFS/DFS/RFS and MFS/DMFS; (B) subgroup analysis for different indicator type (PFS, DFS, RFS); (C) subgroup analysis for PFS/DFS/RFS in EOC subgroup. |
According to subgroup analysis, on the basis of cancer type (EOC, NPC and BC), main ethnic background (Asian or Caucasian) and outcome indicator type (PFS, DFS and RFS), elevated expression of miR-22 prevented progress and recurrence in EOC patients (HR =0.28, 95% CI: 0.17–0.44) (Figure 4C, Table 3), while in BC patients (Figure S2A), Asiatic cancer patients (HR =0.69, 95% CI: 0.36–1.31) and Caucasian cancer patients (HR =2.09, 95% CI: 0.46–9.48) (Figure S2B, Table 3), the prognostic value of miR-22 remains unclear. Besides that, the results showed in Figure 4B potently indicated that elevated expression of miR-22 prolonged the cancer patients’ DFS time, but no significant association was found in PFS and RFS subgroup (Figure 4B, Table 3). In addition, we got the opposite outcome in NPC, which indicates that elevated expression of miR-22 promotes the distant metastasis of NPC patients (Figure S2C, Table 3).
Sensitivity analysis
The sensitivity analysis was performed among the OS and PFS/RFS/DFS, which was used to test the stability of our results. The result remained similar when any single article in the current study was removed each time, which reflects the limited influence of any single study on the overall pooled result. The pooled HRs for OS ranged from 0.70 (95% CI: 0.55–0.91) after removing the study of Yoshimoto28 to 0.83 (95% CI: 0.69–0.99) after removing the study Delfino23 (Figure 5A, Table S1), and the pooled HRs of PRS/RFS/DFS ranged from 0.48 (95% CI: 0.32–0.74) to 0.63 (95% CI: 0.41–0.96) (Figure 5B, Table S2), both of which indicate that the pooled results for OS and PFS/DFS/RFS are stable. We also employ the sensitivity analysis to seek out the source of heterogeneity further. The result revealed that the heterogeneity for OS or PFS/RFS/DFS did not change significantly, no matter which article was removed (Table S1, Table S2).
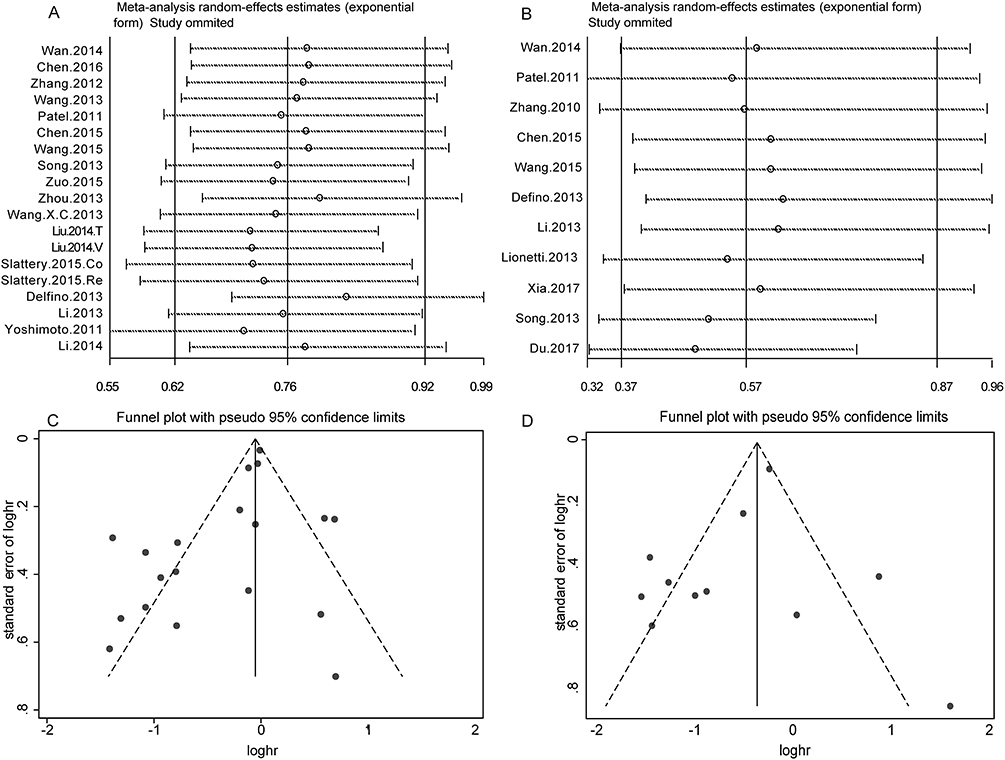 |
Figure 5 Forest plot of miR-22 expression and clinicopathological features. (A) subgroup analysis for miR-22 expression and TNM stage; (B) subgroup analysis for miR-22 high expression and lymph node metastasis; (C) subgroup analysis for miR-22 high expression and distant metastasis; (D) subgroup analysis for miR-22 high expression and recurrence. |
miR-22 expression and clinicopathological characteristics
Ten articles were considered eligible in this analysis, among which nine studies were used to evaluate the correlation between the high expression of miR-22 and TNM stage. Nine out of 10 studies investigated the relationship between the expression of miR-22 and lymph node metastasis, and the combined RRs were 0.48 (95% CI: 0.34–0.67, I2=72.9%) and 0.55 (95% CI: 0.40–0.77, I2=72.1%), respectively, which indicates that the elevated expression of miR-22 was negatively related to TNM stage (Figure 6A, Table 4), as well as lymph node metastasis (Figure 6B, Table 4). We also revealed that increased expression of miR-22 was negatively related to distant metastasis (Figure 6C, Table 4) and recurrence (Figure 6D, Table 4), while no significant association was found between elevated expression of miR-22 and tumor tissue differentiation (Figure S3, Table 4), T stage (Figure S3, Table 4) and lymphatic invasion (Figure S3, Table 4).
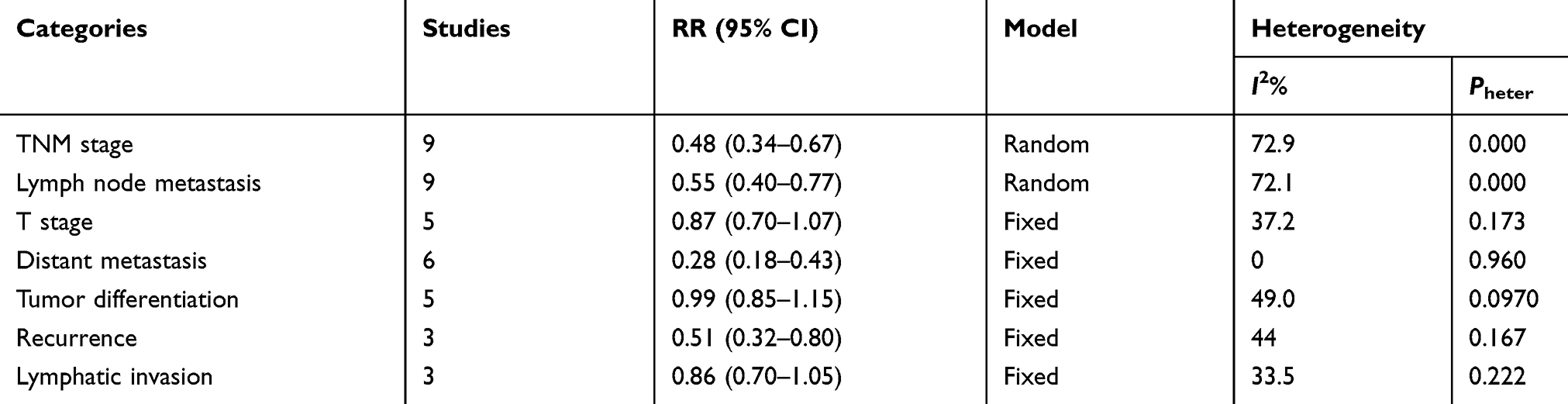 |
Table 4 Meta-analysis of miR-22 high expression and clinicopathological features |
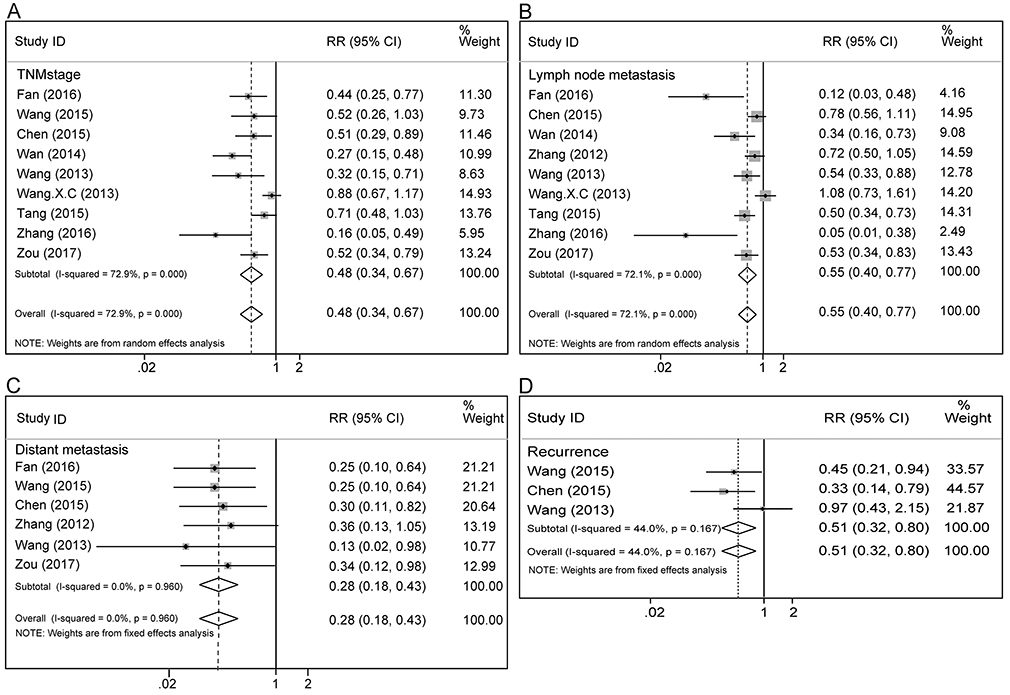 |
Figure 6 Sensitivity analysis and publication bias analysis under a specific model. (A), sensitivity analysis for overall survival; (B) sensitivity analysis for disease progress (PFS/RFS/DFS); (C) funnel plot of publication bias for OS; (D) funnel plot of publication bias for disease progress (PFS/RFS/DFS). |
Assessment of publication bias
We assessed the publication bias of the enrolled studies via Funnel plot, Begg’s test and Egger’s test. The Funnel plot of OS and PFS/DFS/RFS was revealed in Figure 5C and D. The p-values of Begg ’s test and Egger’s test for OS were 0.294 and 0.053; meanwhile, for PFS/RFS/DFS, they are 0.876 and 0.320. Collectively, no significant publication bias exists in this meta-analysis.
Discussion
Alteration of biological markers in serum or tissues plays an important role in predicting the cancer patients’ prognosis, and so great efforts have been made to establish reliable and convincing prognosis biomarkers for cancer patients, through which we can provide doctors useful information and guide clinical precision medicine. During the last decade, accumulating studies have revealed that miRNAs are novel biomarkers involved in cancer patients’ tumorigenesis and progression, acting as an oncogene or tumor-suppressive gene.57,58 Moreover, some studies have shown that miRNAs bear a special expression profile in cancerous tissues, and they can be precisely detected by qRT-PCR in paraffin-embedded, frozen, formalin-fixed tissues and serum samples.59 Compared with mRNA, microRNAs are more stable and easily detected by qRT-PCR. Among them, miR-22 is one of the most frequently studied microRNAs in cancer patients, which was revealed to be aberrantly expressed in various tumors including BC,28 GC,47 CRC,29 HCC,25 ovarian carcinoma42 and others. Therefore, we conduct this meta-analysis to evaluate the association between high expression of miR-22 and the OS as well as clinicopathological significance of cancer patients.
The current meta-analysis, for the first time, evaluated the correlation between elevated expression of miR-22 and cancer patients’ prognosis, progress and clinicopathological significance in various tumors. In our study, high expression of miR-22 predicted a good OS (HR =0.76, 95% CI: 0.62–0.92) (Figure 2, Table 2) and PFS/RFS/DFS (HR =0.57, 95% CI: 0.37–0.87) (Figure 4A, Table 3) for cancer patients, while no significant correlation was found between the expression of miR-22 and MFS/DMFS (Figure 4A, Table 3). Afterward, we performed the subgroup analysis of OS to attempt to explain the sources of heterogeneity and find out the specific relationship between miR-22 expression and the OS of cancer type, sample type, the anatomical system of cancer, main pathologic type, main ethnic background and assay method (q-PCR and ISH). Cancer type’s subgroup analysis showed that increased expression of miR-22 predicts a good OS in HCC (Figure S1B, Table 2) patients and EOC patients (Figure S1A, Table 2); meanwhile, no obvious association was found between miR-22 high expression and prognosis in GC patients (Figure S1A, Table 2), CRC patients (Figure S1B, Table 2) and BC patients (Figure S1A, Table 2). However, 512 participants in NPC (namely serum subgroup) showed an opposite outcome (Figure S1B, Table 2), which indicates that miR-22 high expression might shorten the OS time and promote the distant metastasis of NPC patients. Perhaps that overexpression of miR-22 might downregulate a tumor-suppressor gene or other genes involved in cell differentiation, hence promoting tumorigenesis by stimulating tumor proliferation, angiogenesis and invasion.60 As was shown in Figure S5–S9, we test the conclusion of cancer type’s subgroup analysis in TCGA data. However, we found some inconsistent even opposite conclusions. We found most patients in TCGA are Caucasians, while most patients in our research are Asians, so it is reasonable for us to get these conclusions. Through the subgroup analysis of OS, we could find that elevated expression of miR-22 predicted a good OS in the digestive system subgroup, reproduction system subgroup, adenocarcinoma subgroup, q-PCR subgroup, FFPE subgroup and tissue subgroup, and no significant association was found in other subgroups of OS (Table 2). In the subgroup analysis of PRS/RFS/DFS, high expression of miR-22 might predict a good DFS (Figure 4B), which suggested that the miR-22 high expression prolongs the DFS time of cancer patients, while no significant association was found in RFS and PFS subgroup (Figure 4B). Additionally, in subgroup analysis based on the characteristics of the individual studies, we observed statistically significant outcomes in the PFS/DFS/RFS of EOC subgroup (Figure 4C), with pooled HRs of 0.28 (95% CI: 0.17–0.44); no significant association was found between miR-22 high expression and PFS/RFS/DFS in BC patients (Figure S2A), Asiatic cancer patients (Figure S2B) subgroup and Caucasian cancer patients subgroup (Figure S2B).
Through the subgroup analysis, the heterogeneity of some subgroup remains large still, so the subgroup analysis could not account for the sources of heterogeneity completely. According to the subgroup analysis, the heterogeneity of OS might derive from the different characteristics of the studies, such as cancer type, sample type, the anatomical system of cancer, main pathological type, main ethnic background, as well as the cutoff value of the miR-22 expression. For example, when we stratified them according to cancer type and sample type, heterogeneity became insignificant in CRC,and disappeared in serum samples, in HCC subgroup, as well as in NPC subgroup (Table 2). The heterogeneity was also reduced when the DFS/RFS/PFS studies were classified by the indicator type and main ethnic subgroup, through which we can partly explain the source of heterogeneity for PFS/RFS/DFS (Table 3). According to the sensitivity analysis of OS (Figure 5A, Table S1) and PFS/RFS/DFS (Figure 5B, Table S2), no single study significantly influenced the pooled results, which indicates that the outcome for prognosis and disease progress are stable. Additionally, the sensitivity analysis also suggested that no single study significantly influences the heterogeneity of OS and PFS/RFS/DFS (Table S1, Table S2).
Furthermore, we analyzed the correlation between miR-22 expression and clinicopathological characteristics of cancer patients. As shown in Table 4, elevated expression of miR-22 was negatively correlated with TNM stage (Figure 6A), lymph node metastasis (Figure 6B), distant metastasis (Figure 6C) and recurrence (Figure 6D). The results indicate that cancer patients with higher expression level of microRNA-22 means lower likelihoods of lymph node metastasis, of distant metastasis and of recurrence. miR-22 is also negatively correlated with TNM stage (Figure 6A), which indicates that miR-22 high expression means earlier TNM stage. In addition, there was no significant association between high expression of microRNA-22 and T stage (RR =0.87, 95% CI: 0.71–1.07), tumor differentiation (HR =0.99, 95% CI: 0.85–1.15) and lymphatic invasion (RR =0.86, 95% CI: 0.70–1.05) (Figure S3).
In our meta-analysis, elevated expression of miR-22 suggested a good prognosis of cancer patients in most subgroup, but we can also find inconsistent even opposite outcome in some subgroups (NPC subgroup, serum subgroup, squamous cell carcinoma subgroup and so on). As is known to all, miR-22 acts as oncogene or antioncogene which largely depends on their corresponding target gene. If the target gene of miR-22 involved in the process of tumor suppressor, through binding to the mRNA of target gene at the 3ʹ-untranslated region, miR-22 may lead to the mRNA of target gene degradation or translational repression11,61 and act as oncogenes.62 Otherwise, miR-22 act as antioncogene62 In this meta-analysis, most articles suggested that miR-22 act as antioncogene and their elevated expression predicted a good OS.21,23–26,50,53 Whereas a few studies reported inconsistent results,31,32 indicating miR-22 maybe an oncogene in some specific type of cancer. This is mainly because miR-22 regulates different target genes in different types of cancer (Table S3), thus resulting in the different prognostic value in different cancer types. In these subgroups, in which miR-22 acts as an oncogene, the result affected most by NPC. Perhaps that miR-22 target some specific oncogene, although further research needs to be performed. In addition, because of the limit of language, the result of Asian and Caucasian becomes less persuasive (lose non-English study in Asian). So it is reasonable for us to get these conclusions, but we should treat these results cautiously in some specific types of cancer; only in this way can we get more accurate result.
Although meta-analysis is robust, several limits still persist in this meta-analysis. First, the miR-22 expression data in global populations are not available for us, making it impossible for us to set a standard cutoff value, which leads to the inconsistent cutoff value of miR-22 and makes our conclusion less persuasive. Second, miR-22 expression was detected most in tumor tissue (23 studies) but little in serum (two studies) and urine (one study), which was more easily accepted and monitored by patients than tissue. Third, this meta-analysis exists relatively large heterogeneity, which was likely because of the different characteristics of studies (cancer type, sample type, the anatomical system of cancer, the main ethnic background and main pathological type),measurement method and the cutoff value of miRNA-22 expression. Fourth, some data were extracted from survival curves, which might be less accurate than calculated via raw data. Finally, a panel of miRNAs may have stronger predictive value for prognosis than a single miRNA, which should be cheaper and have higher sensitivity and specificity.
In our meta-analysis, neither Begg’s test nor Egger’s test showed significant evidence of publication bias (0.294 and 0.053 for OS; meanwhile, it is 0.876 and 0.320 for PFS/RFS/DFS); publication bias might still exist because the tendency for journals to publish positive results could also make certain bias. Language bias might exist because the studies retrieved in our study were limited in English.
Despite the limits described above, our study clearly demonstrated that elevated expression of miR-22 predicted a good OS, clinicopathological features and PFS/RFS/DFS in cancer patients. To better understand and apply the effect of miR-22 in cancer, more multicenter clinical investigations should be conducted before the application of miR-22 in predicting prognosis of some specific type of cancers.
Abbreviations
miR-22, microRNA-22; T, training set; V, validation set; NR, not reported; Co, colon set; Re, rectal set; “-”, not mention; ISH, in situ hybridization; SC, survival curve; OS, overall survival; PFS, progress free survival; DFS, disease-free survival; RFS, recurrence-free survival; MFS, metastasis-free survival; DMFS, distant metastasis-free survival; mth, month; TCGA, The Cancer Genome Atlas; GEO, Gene Expression Omnibus; BC, breast cancer; EOC, Epithelial ovarian cancer; CRC colorectal carcinoma; HCC, hepatocellular carcinoma; NPC, nasopharyngeal carcinoma; GC, gastric cancer; OST, osteosarcoma; MDS, myelodysplastic syndrome; ESCC, esophageal squamous cell carcinoma; pPCL, primary plasma cell leukemia; RCC, renal cell carcinoma; Bla Ca, bladder cancer; FFPE, formalin-fixed paraffin-embedded; FTT, frozen tumor tissue; “-”, not mentioned.
Acknowledgment
The analysis was supported by National Natural Science Foundation of China (Grant No. 81572874). We would like to acknowledge Sze Ka Lun, Ziming Xiang, Gao Tan, Bin Xiong, Liang Zheng, Shuyi Wang, Zewei Yan, Chunxiao Zhang and Kun Zou for their technical assistance and rational suggestion.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflict of interest in this work.
References
1. Bray F, Ren JS, Masuyer E, Ferlay J. Global estimates of cancer prevalence for 27 sites in the adult population in 2008. Int J Cancer. 2013;132(5):1133–1145. doi:10.1002/ijc.27711
2. Dai J, Tang K, Xiao W, et al. Prognostic significance of C-reactive protein in urological cancers: a systematic review and meta-analysis. Asian Pac J Cancer Prev. 2014;15(8):3369–3375. doi:10.7314/apjcp.2014.15.8.3369
3. Zeng R, Duan L, Kong Y, et al. Clinicopathological and prognostic role of MMP-9 in esophageal squamous cell carcinoma: a meta-analysis. Chin J Cancer Res. 2013;25(6):637–645. doi:10.3978/j.issn.1000-9604.2013.11.03
4. Carthew RW, Sontheimer EJ. Origins and mechanisms of miRNAs and siRNAs. Cell. 2009;136(4):642–655. doi:10.1016/j.cell.2009.01.035
5. Lee RC, Feinbaum RL, Ambros V, The C. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell. 1993;75(5):843–854. doi:10.1016/0092-8674(93)90529-y
6. Hu HY, He L, Fominykh K, et al. Evolution of the human-specific microRNA miR-941. Nat Commun. 2012;3:1145. doi:10.1038/ncomms2146
7. Zhan S, Merlin C, Boore JL, Reppert SM. The monarch butterfly genome yields insights into long-distance migration. Cell. 2011;147(5):1171–1185. doi:10.1016/j.cell.2011.09.052
8. Fu Y, Yang Y, Zhang H, et al. The genome of the Hi5 germ cell line from Trichoplusia ni, an agricultural pest and novel model for small RNA biology. Elife. 2018;7. doi:10.7554/eLife.42270
9. Landgraf P, Rusu M, Sheridan R, et al. A mammalian microRNA expression atlas based on small RNA library sequencing. Cell. 2007;129(7):1401–1414. doi:10.1016/j.cell.2007.04.040
10. Filipowicz W, Bhattacharyya SN, Sonenberg N. Mechanisms of post-transcriptional regulation by microRNAs: are the answers in sight? Nat Rev Genet. 2008;9(2):102–114. doi:10.1038/nrg2290
11. Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell. 2004;116(2):281–297. doi:10.1016/s0092-8674(04)00045-5
12. Zhang B, Pan X, Cobb GP, Anderson TA. Plant microRNA: a small regulatory molecule with big impact. Dev Biol. 2006;289(1):3–16. doi:10.1016/j.ydbio.2005.10.036
13. Guz M, Rivero-Muller A, Okon E, et al. MicroRNAs-role in lung cancer. Dis Markers. 2014;2014:218169. doi:10.1155/2014/594093
14. Ling H, Fabbri M, Calin GA. MicroRNAs and other non-coding RNAs as targets for anticancer drug development. Nat Rev Drug Discov. 2013;12(11):847–865. doi:10.1038/nrd4140
15. Bouyssou JM, Manier S, Huynh D, Issa S, Roccaro AM, Ghobrial IM. Regulation of microRNAs in cancer metastasis. Biochim Biophys Acta. 2014;1845(2):255–265. doi:10.1016/j.bbcan.2014.02.002
16. Gurha P, Abreu-Goodger C, Wang T, et al. Targeted deletion of microRNA-22 promotes stress-induced cardiac dilation and contractile dysfunction. Circulation. 2012;125(22):2751–2761. doi:10.1161/CIRCULATIONAHA.111.044354
17. Berenguer J, Herrera A, Vuolo L, et al. MicroRNA 22 regulates cell cycle length in cerebellar granular neuron precursors. Mol Cell Biol. 2013;33(14):2706–2717. doi:10.1128/MCB.00338-13
18. Choong ML, Yang HH, McNiece I. MicroRNA expression profiling during human cord blood-derived CD34 cell erythropoiesis. Exp Hematol. 2007;35(4):551–564. doi:10.1016/j.exphem.2006.12.002
19. Huang ZP, Wang DZ. miR-22 in cardiac remodeling and disease. Trends Cardiovasc Med. 2014;24(7):267–272. doi:10.1016/j.tcm.2014.07.005
20. Song SJ, Pandolfi PP. miR-22 in tumorigenesis. Cell Cycle. 2014;13(1):11–12. doi:10.4161/cc.27027
21. Wan WN, Zhang YQ, Wang XM, et al. Down-regulated miR-22 as predictive biomarkers for prognosis of epithelial ovarian cancer. Diagn Pathol. 2014;9. doi:10.1186/s13000-014-0178-8
22. Li J, Liang SH, Yu HL, Zhang J, Ma DA, Lu X. An inhibitory effect of miR-22 on cell migration and invasion in ovarian cancer. Gynecol Oncol. 2010;119(3):543–548. doi:10.1016/j.ygyno.2010.08.034
23. Delfino KR, Rodriguez-Zas SL. Transcription factor-microRNA-target gene networks associated with ovarian cancer survival and recurrence. PLoS One. 2013;8(3):e58608. doi:10.1371/journal.pone.0058608
24. Chen M, Hu W, Xiong CL, et al. miR-22 targets YWHAZ to inhibit metastasis of hepatocellular carcinoma and its down-regulation predicts a poor survival. Oncotarget. 2016;7(49):80751–80764. doi:10.18632/oncotarget.13037
25. Zhou L, He JT, Zhang YD. MicroRNA-22 expression in hepatocellular carcinoma and its correlation with ezrin protein. J Int Med Res. 2013;41(4):1009–1016. doi:10.1177/0300060513484436
26. Chen B, Tang H, Liu X, et al. miR-22 as a prognostic factor targets glucose transporter protein type 1 in breast cancer. Cancer Lett. 2015;356(2Pt B):410–417. doi:10.1016/j.canlet.2014.09.028
27. Patel JB, Appaiah HN, Burnett RM, et al. Control of EVI-1 oncogene expression in metastatic breast cancer cells through microRNA miR-22. Oncogene. 2011;30(11):1290–1301. doi:10.1038/onc.2010.510
28. Yoshimoto N, Toyama T, Takahashi S, et al. Distinct expressions of microRNAs that directly target estrogen receptor alpha in human breast cancer. Breast Cancer Res Tr. 2011;130(1):331–339. doi:10.1007/s10549-011-1672-2
29. Slattery ML, Herrick JS, Mullany LE, et al. An evaluation and replication of miRNAs with disease stage and colorectal cancer-specific mortality. Int J Cancer. 2015;137(2):428–438. doi:10.1002/ijc.29384
30. Song SJ, Ito K, Ala U, et al. The oncogenic microRNA miR-22 targets the TET2 tumor suppressor to promote hematopoietic stem cell self-renewal and transformation. Cell Stem Cell. 2013;13(1):87–101. doi:10.1016/j.stem.2013.06.003
31. Zuo QF, Cao LY, Yu T, et al. MicroRNA-22 inhibits tumor growth and metastasis in gastric cancer by directly targeting MMP14 and Snail. Cell Death Dis. 2015;6:e2000. doi:10.1038/cddis.2015.297
32. Liu N, Cui RX, Sun Y, et al. A four-miRNA signature identified from genome-wide serum miRNA profiling predicts survival in patients with nasopharyngeal carcinoma. Int J Cancer. 2014;134(6):1359–1368. doi:10.1002/ijc.28468
33. Moher D. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement (vol 8, pg 336, 2010). Int J Surg. 2010;8(8):658. doi:10.1016/j.ijsu.2010.07.299
34. Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998;17(24):2815–2834.
35. Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials. 2007;8. doi:10.1186/1745-6215-8-16
36. Stroup DF, Berlin JA, Morton SC, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. Jama. 2000;283(15):2008–2012. doi:10.1001/jama.283.15.2008
37. Hong L, Han Y, Yang J, et al. Prognostic value of epidermal growth factor receptor in patients with gastric cancer: a meta-analysis. Gene. 2013;529(1):69–72. doi:10.1016/j.gene.2013.07.106
38. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
39. Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22(4):719–748.
40. DerSimonian R, Laird N. Meta-analysis in clinical trials revisited. Contemp Clin Trials. 2015;45(Pt A):139–145. doi:10.1016/j.cct.2015.09.002
41. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
42. Li X, Lu Y, Chen YX, Lu WG, Xie X. MicroRNA profile of paclitaxel-resistant serous ovarian carcinoma based on formalin-fixed paraffin-embedded samples. BMC Cancer. 2013;13. doi:10.1186/1471-2407-13-216
43. Zhang J, Yang Y, Yang T, et al. microRNA-22, downregulated in hepatocellular carcinoma and correlated with prognosis, suppresses cell proliferation and tumourigenicity. British Journal of Cancer. 2010;103(8):1215-1220.doi: 10.1038/sj.bjc.6605895
44. Zhang GJ, Xia SS, Tian HP, Liu ZL, Zhou T. Clinical significance of miR-22 expression in patients with colorectal cancer. Medical Oncology. 2012;29(5):3108-3112.doi: 10.1007/s12032-012-0233-9
45. Xia SS, Zhang GJ, Liu ZL, et al. MicroRNA-22 suppresses the growth, migration and invasion of colorectal cancer cells through a Sp1 negative feedback loop. Oncotarget. 2017;8(22):36266-36278.doi: 10.18632/oncotarget.16742
46. Tang Y, Liu X, Su B, et al. microRNA-22 acts as a metastasis suppressor by targeting metadherin in gastric cancer. Mol Med Rep. 2015;11(1):454-460.doi: 10.3892/mmr.2014.2682
47. Wang W, Li F, Zhang Y, Tu Y, Yang Q, Gao X. Reduced expression of miR-22 in gastric cancer is related to clinicopathologic characteristics or patient prognosis. Diagn Pathol. 2013;8:102. doi:10.1186/1746-1596-8-102
48. Fan W, Huang J, Xiao H, Liang Z. MicroRNA-22 is downregulated in clear cell renal cell carcinoma, and inhibits cell growth, migration and invasion by targeting PTEN. Mol Med Rep. 2016;13(6):4800-4806.doi: 10.3892/mmr.2016.5101
49. Zhang S, Zhang D, Yi C, Wang Y, Wang H, Wang J. MicroRNA-22 functions as a tumor suppressor by targeting SIRT1 in renal cell carcinoma. Oncol Rep. 2016;35(1):559-567.doi: 10.3892/or.2015.4333
50. Wang G, Shen N, Cheng L, Lin J, Li K. Downregulation of miR-22 acts as an unfavorable prognostic biomarker in osteosarcoma. Tumour Biol. 2015;36(10):7891–7895. doi:10.1007/s13277-015-3379-1
51. Song SJ, Poliseno L, Song MS, Ala U, Webster K, Ng C, Beringer G, Brikbak NJ, Yuan X, Cantley LC, Richardson AL, Pandolfi PP. MicroRNA-Antagonism Regulates Breast Cancer Stemness and Metastasis via TET-Family-Dependent Chromatin Remodeling. Cell 2013;154:311-24.doi:10.1016/j.cell.2013.06.026
52. Wang XC, Zhang ZB, Wang YY, et al. Increased miRNA-22 expression sensitizes esophageal squamous cell carcinoma to irradiation. J Radiat Res. 2013;54(3):401-408.doi:10.1093/jrr/rrs113
53. Li R, Wang J, Yang S. miR-22 inhibited glioma cells proliferation by targeting MTDH. China Oncol. 2014;24(6):401–406.
54. Lionetti M, Musto P, Di Martino MT, et al. Biological and clinical relevance of miRNA expression signatures in primary plasma cell leukemia. Clin Cancer Res. 2013;19(12):3130-3142. doi:10.1158/1078-0432.CCR-12-2043
55. Du L, Jiang X, Duan W, et al. Cell-free microRNA expression signatures in urine serve as novel noninvasive biomarkers for diagnosis and recurrence prediction of bladder cancer. Oncotarget. 2017. doi:10.18632/oncotarget.16586
56. Zou Q, Tang Q, Pan Y, et al. MicroRNA-22 inhibits cell growth and metastasis in breast cancer via targeting of SIRT1. Exp Ther Med. 2017;14(2):1009-1016. doi:10.3892/etm.2017.4590
57. Zhang BH, Pan XP, Cobb GP, Anderson TA. microRNAs as oncogenes and tumor suppressors. Dev Biol. 2007;302(1):1–12. doi:10.1016/j.ydbio.2006.08.028
58. Kent OA, Mendell JT. A small piece in the cancer puzzle: microRNAs as tumor suppressors and oncogenes. Oncogene. 2006;25(46):6188–6196. doi:10.1038/sj.onc.1209913
59. Kim DJ, Linnstaedt S, Palma J, et al. Plasma components affect accuracy of circulating cancer-related microRNA quantitation. J Mol Diagn. 2012;14(1):71–80. doi:10.1016/j.jmoldx.2011.09.002
60. Miska EA. How microRNAs control cell division, differentiation and death. Curr Opin Genet Dev. 2005;15(5):563–568. doi:10.1016/j.gde.2005.08.005
61. Zheng H, Li P, Kwok JG, et al. Alcohol and hepatitis virus-dysregulated lncRNAs as potential biomarkers for hepatocellular carcinoma. Oncotarget. 2018;9(1):224–235. doi:10.18632/oncotarget.22921
62. Shenouda SK, Alahari SK. MicroRNA function in cancer: oncogene or a tumor suppressor? Cancer Metastasis Rev. 2009;28(3–4):369–378. doi:10.1007/s10555-009-9188-5
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.