")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 10
Surveying the effect of a self-care education program on severity of nausea and emesis in colorectal cancer patients under chemotherapy
Authors Karimi S, Makhsosi BR, Seyedi-Andi SJ, Behzadi M, Moghofeh Y, Mohammadinasrabadi K, Abdi A , Ahmadi P
Received 26 December 2016
Accepted for publication 14 July 2017
Published 14 August 2017 Volume 2017:10 Pages 301—307
DOI https://doi.org/10.2147/JMDH.S131111
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saba Karimi,1 Behnam Reza Makhsosi,2 Seyed Jalil Seyedi-Andi,3 Maryam Behzadi,4 Yasaman Moghofeh,5 Kourosh Mohammadinasrabadi,1 Alireza Abdi,1 Pegah Ahmadi1
1School of Nursing and Midwifery, 2Surgical Department, Imam Reza Hospital, Kermanshah University of Medical Sciences, Kermanshah, 3Social Determinants of Health Research Center, Babol University of Medical Sciences, Babol, 4Taleghani Hospital, 5Imam Khomeini Hospital, Kermanshah University of Medical Sciences, Kermanshah, Iran
Background and objective: Colorectal cancer is one of the main causes of mortality in both developed and developing countries, including Iran. One of the treatments available for colorectal cancer is chemotherapy, of which nausea and emesis are the side effects. Owing to problems in controlling the side effects, a combination of medicine and non-medicine interventions is usually used. Self-care is one of the non-medicine interventions in this regard. The present study was aimed at surveying the effect of a self-care education program on severity of nausea and emesis in colorectal cancer patients under chemotherapy.
Methods: A semi-experimental study was carried out in Imam Reza Hospital of Kermanshah, Iran. The sample group comprised 52 patients with colorectal cancer under chemotherapy. Data gathering tools included a demographics questionnaire and Morrow Assessment of Nausea and Emesis. To control intensity of nausea and emesis, a package of self-care measures including muscular progressive relaxation, music, and education on nutrition was used. Afterward, the collected data were analyzed using statistical tests such as Shapiro–Wilk test (to check normal distribution of the data), Mann–Whitney U test, Wilcoxon test, and chi-square test with the help of SPSS 20.
Results: The results showed a considerable decrease in intensity and frequency of nausea and emesis after the intervention. The p-value of Mann–Whitney U test results with regard to intensity of nausea in the experiment and control groups after the intervention was 0.029; this figure for intensity of emesis was 0.009, which indicated effectiveness of the self-care program.
Conclusion: As the results showed, using self-care program could be effective in attenuating intensity of emesis and nausea in colorectal cancer patients under chemotherapy. So, it can be concluded that the use of this program can increase the patient’s self-care ability to control vomiting and nausea, which can be considered as a complementary approach to the antiemetic medications.
Keywords: colorectal cancer, self-care, chemotherapy, nausea and emesis
Introduction
Cancer is one of the main causes of mortality in the developed and developing countries such as Iran. The disease is highly prevalent and growing in cases so that it consumes a large portion of health service resources. Along with changes in lifestyle and growth of urbanism, prevalence of some types of cancers including gastrointestinal cancer is growing.1 Colorectal cancer is the second cause of cancer-caused mortality in the USA (the third and second prevalent cancer in men and women, respectively). Moreover, gastrointestinal cancer represents 38% of all cancers and 44.4% of mortality rate; it is one of the main types of cancers in Iran, and its number was estimated to be 19,617 cases in 2009.2 Colorectal cancer is a chronic disease with symptoms such as weakness, dizziness, lack of appetite, nausea and emesis, anemia, and nutrition disorder. In addition, colorectal cancer treatment causes side effects such as nausea and emesis, alopecia, and stomatitis, all of which reduce quality of life of the patients.3 One of the common treatments for colorectal cancer is chemotherapy. Currently, this treatment is used not only as a pain killing intervention but also to treat some specific types of cancers and long-term control of some others. The treatment is one of the main measures performed in colorectal cancer centers. However, as noted earlier, chemotherapy is not free of side effects. Among these side effects, nausea and emesis are notable, which result in electrolytic disorders (potassium and sodium), malnutrition, dehydration, esophagus injuries, and tiredness. Approximately 40–80% of the patients experience nausea and emesis. Intensity of these side effects differs in different patients, and they cause notable negative effects on quality of life. Furthermore, the electrolyte side effects (hyponatremia, hypokalemia, etc.) of emesis and some consequences such as immunity system problem, physical activity disorder, cognitive function disorder, social problems, depression, and failure to fulfill social responsibilities could happen. So, it is important, therefore, to control nausea and emesis caused by chemotherapy in colorectal cancer patients;4–6 otherwise, ~20% of the patients would refuse to continue the treatment program. To prevent nausea and emesis in these patients, serotonin, corticosteroids, and metoclopramide receiver antagonists are prescribed. Studies have reported ~50% intensive nausea and emesis even after using prophylaxis. On the other hand, these medicines are very costly and they induce their own side effects such as extrapyramidal side effects, decrease in blood pressure, headache, constipation, tiredness, dry mouth, dizziness, diarrhea, and restlessness.7 Because using antiemetic medicines induces side effects and the health system incurs heavy costs taking care of these patients, having the patients responsible for even a small part of the treatment would be of great help in improvement of quality of life of these patients. In fact, the purpose of healthcare services for chronic diseases is to preserve well-being of the patients despite the chronic disease. Taking into account that colorectal cancer is a chronic disease and the disease and its treatment cause side effects such as nausea and emesis, which decrease quality of life of the patients,8–10 it is essential to empower the patients to do self-care measures. The problems caused by colorectal cancer are chronic,11 and as shown by other studies, self-care would be of great help for chronic patients suffering from heart failure,12 myocardial infarction,13 and multiple sclerosis.14 Given the above introduction and knowing that nurses are the main members of medical teams, they can empower the patients to carry out self-care in the field of preventing and controlling nausea and emesis. Self-care as a non-pharmacological program is aimed at increasing self-care via some educational programs for the patients, through which healthcare workers try to improve the physical and mental states.15 Through this, the expenses of frequent hospitalization would be omitted and the patients would enjoy better clinical condition. Therefore, the present study was an attempt to survey effectiveness of self-care educational programs on prevention and reduction of intensity of nausea and emesis in colorectal cancer patients under chemotherapy.
Methods
Study design
The study was carried out as a semi-experimental study in radio/chemotherapy clinic, oncology ward, Imam Reza Hospital, Kermanshah (500 beds), in 2016. At the time of the study, the center hosted 366 colorectal cancer patients.
The study population comprised colorectal cancer patients hospitalized in the hospital, and the sample group size was determined based on the following formula with confidence level of 95% and test power of 90% based on similar studies.16 The obtained sample group size was equal to 24, and by assuming 10% attrition, 26 patients were selected randomly.
 |
The sample size was 52 people. For preventing the association of experimental and control group members with each other, people in even days were recruited into the experimental group and individuals whose chemotherapy was on the odd days were placed into the control group. The participants were selected through quota sampling. The inclusion criteria were age range of 18–65 years; definite diagnosis of colorectal cancer; patients with the cancer stages of I, II, and III without any metastasis receiving chemotherapy regimen (the chemotherapy protocol contains oxaliplatin platinum, 5 fluorouracil and FOLFOX) for the first time only containing cisplatin and etoposide (<50 mg);15–17 willingness to participate; being under chemotherapy; consciousness; no psychological disease record; no other disease that would cause nausea and emesis (e.g., liver/kidney failure, gastritis, acute hepatitis C, and cerebral problems); lack of metastasis; and not using antiemetic drugs. The exclusion criteria included reluctance to participate in the study and participation in other educational courses held in the center.
Data gathering tool
The data gathering tools included a demographics questionnaire and Morrow Assessment of Nausea and Emesis (MANE). The former collected information about age, gender, marital status, smoking and drinking habits, occupation, and education. The latter was designed in 1984 by Morrow, and it comprised 17 short questions to survey and evaluate nausea and emesis before, during, and after treatment and term and intensity of the problem. The questionnaire is designed based on Likert’s 7-point scale (0 = no problem to 6 = unbearable problem). The tool is a self-report tool, and the obtained scores are interpreted as 0 = no nausea and emesis, 1–2 = mild nausea and emesis, 3–4 = moderate nausea and emesis, and 5–6 = severe nausea and emesis.18 Validity and reliability of the questionnaire have been examined by several studies (r = 0.72–0.96).19,20 To examine internal consistency, Cronbach’s alpha was used (r = 0.86).
Data gathering
Before commencing the study, it was approved by the ethics committee of research deputy affiliated to Kermanshah University of Medical Sciences in Kermanshah, Iran. Then, for data collection, the authors referred to oncology ward and chemotherapy clinic of Imam Reza Hospital. In all, 52 patients who met the inclusion criteria were selected at first and categorized into control and experiment groups. The participants were briefed about the purposes of the study, and a written letter of consent was obtained from each participant. Education stage was performed in the oncology ward of the hospital. At first, the demographics questionnaire and MANE were filled out by the participants in both groups. Then, severity of nausea and emesis of the patients and the educational needs were determined. Afterward, the education was started based on spiritual condition and literacy of the patients. The education was a 12-session course, and the educational tools included pamphlet, brochure, picture, and video. Self-care education to attenuate the severity of nausea and emesis from different aspects included self-care training about regimen before and after chemotherapy (e.g., using frequent meals of small portion, using mashed food without stimulants, using cold food, using rich carbohydrate and low-fat regimen such as roasted bread, cookies, yoghurt, juice, cooked cereals, soft peeled fruits, juicy melon, banana, and other natural fruit juices) for colorectal cancer. In order to train patients, we divided the experimental group into two groups of 13 people. For each group, six sessions of training were designed. Training was done to reduce the patient’s nausea and vomiting before starting chemotherapy. These six sessions took place within 2 months, and the duration of each session was 45–60 minutes.
Lack of awareness of colorectal cancer and self-care benefits
At the first session, we first described the nature of colorectal cancer in order to provide patients with information about their illness. In this session, in order to improve patient motivation to self-care, there are some benefits to self-care, such as improving the patient’s quality of life, reducing the severity of the illness, having autonomy in doing things, adapting to his or her own circumstances, being active in his or her affairs, and the presence in the community for patients is explained. In the second session, patients were provided with explanations about the causes of nausea and vomiting and the importance of preventing or reducing the incidence of this problem. In the third session, recommendations were given to patients about the importance of high-calorie diet, proteinuria, and high protein, as well as the type of diet before and after chemotherapy. A nutritional checklist was used to track nutrition during the period. In the fourth session, an appropriate posture during chemotherapy was given to reduce the severity of nausea and the use of ice to reduce the severity of nausea and vomiting in patients was described. In the fifth session, training in methods of diversion (music therapy, talking with family or friends, watching TV, reading a book) during chemotherapy or whenever a patient experiences nausea and vomiting was given. In the sixth session, progressive muscle relaxation was taught to patients (in which the patient begins to contract and release his muscles from the sole of the foot, and the contraction lasts for 10 seconds) to reduce the severity of nausea and vomiting, as well as to create mental relaxation for the training of patients we gave.15
In addition, the patients were warned not to use fat-rich, fried, and spicy foods. Before chemotherapy, the patients were recommended to use ginger, given its antiemetic effects; in addition, it was recommended to eat more slowly in a calm environment.21 Muscular progressive relaxation technique including relaxation and contraction of the muscles from the forehead to the feet was also trained. The patients were asked to think of distracting thoughts, listen to others’ dialog/music, and watch TV after initiation of chemotherapy medicine injections.22 After the intervention course, the participants filled out the questionnaire once more. The collected data were analyzed with the help of SPSS using Shapiro–Wilk test (to check normal distribution of data), Mann–Whitney U test, Wilcoxon test, and chi-square test.
Findings
As the results showed, the average age of the participants in the control and experiment groups were 53 ± 6.89 and 52.5 ± 7.07 years, respectively; married and male participants constituted 78.84% (41) and 57.69% (30) of the sample group, respectively. Results of independent t-test (p = 0.62, f = 0.011) showed that there was no significant difference between the two groups with regard to age. Majority of the participants did not have high school diploma (38.46%) and were workers (34.61%). Table 1 lists demographics of the participants. Chi-square test showed no significant difference between the participants with regard to gender, marital status, smoking and drinking habits, education, and occupation. Normal distribution of the data was tested using Shapiro–Wilk test, and non-parametric tests were used for data analyses.
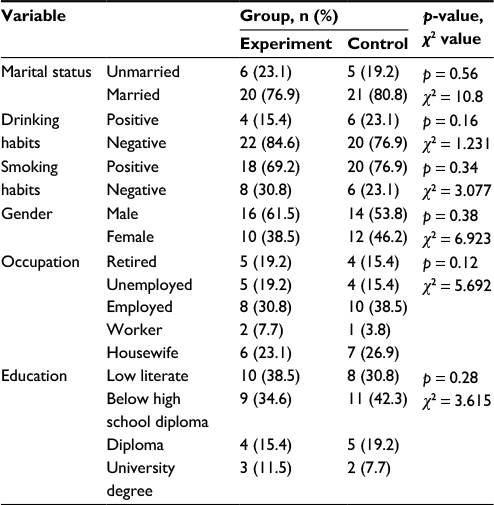 | Table 1 Definite and relative frequency distributions of the participants based on the demographics of the experiment and control groups |
Tables 2 and 3 list severity of nausea and emesis before and after self-care measures. Mean severity of nausea decreased from 3.07 ± 1.91 (moderate level) before the intervention to 1.5 ± 1.52 (trivial level) after the intervention in the experiment group. Wilcoxon test showed a significant decrease in the severity of nausea in the experiment group (p < 0.001); while no such significant decrease was observed in the control group before and after the intervention (p = 0.57).
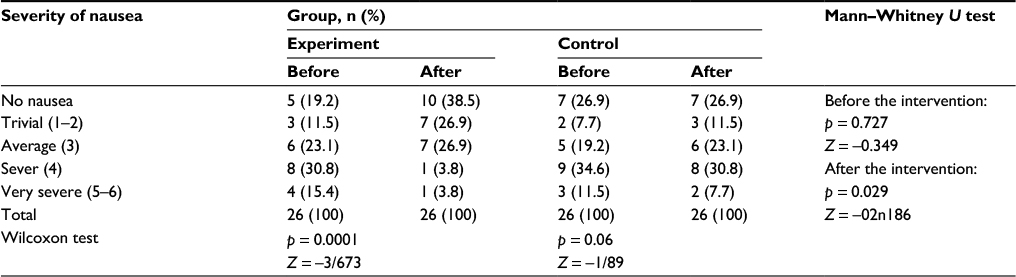 | Table 2 Comparison of relative and definite frequencies of severity of nausea before and after the intervention in control and experiment groups |
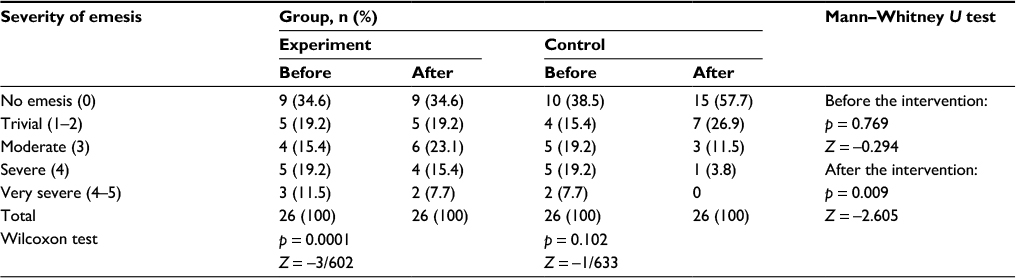 | Table 3 Comparison of relative and definite frequencies of emesis before and after the intervention in the control and experiment groups |
As to severity of emesis, mean severity of emesis in the experiment group decreased from 2.11 ± 1.96 to 0.76 ± 1.17 after the intervention. Wilcoxon test showed a significant difference in the severity of emesis in the experiment group (p < 0.001), while no such difference was observed in the control group (p = 0.33). The Mann–Whitney test showed a significant decrease in severity of emesis in the experiment group (p = 0.023), and it confirmed effectiveness of self-care measures in reducing severity of emesis in the experiment group (p = 0.003; Table 4).
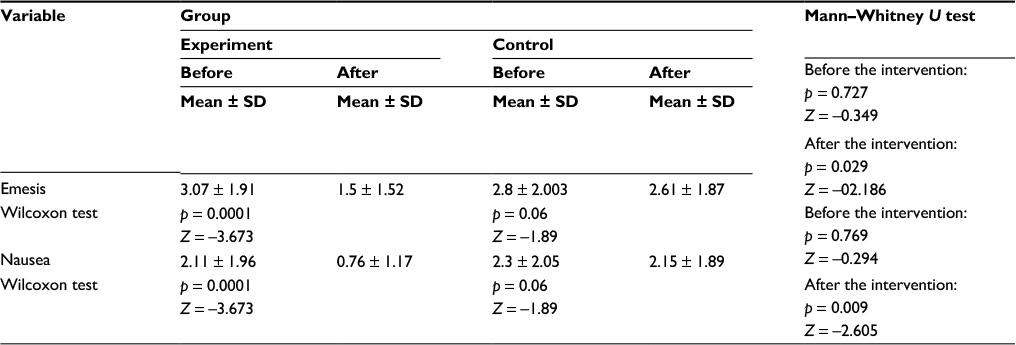 | Table 4 Comparison of severity of nausea and emesis before and after the intervention in the control and experiment groups |
Discussion
The results of the study showed that severity of nausea and emesis of the patients in the experiment group before and after the intervention was significantly different. Mean score of severity of nausea and emesis in the experiment group showed a significant decrease after the intervention compared with the control group. To reduce severity of nausea and emesis, muscular progressive relaxation technique was trained to the patients in the experiment group as a self-care measure. Since nausea and emesis after chemotherapy has both pharmacologic and psychological roots, the technique could have been effective through sequential relaxation of muscles along with deep breaths, which in turn leads to decrease in the anxiety and the stress caused by chemotherapy. The patients were asked to control and reduce severity of nausea and emesis by performing this technique before, during, and after chemotherapy. Consistently Bakhshi et al,23 Molassiotis,24 Arakawa,25 and Tipton et al26 reported that using this technique resulted in decrease in severity of nausea and emesis in chemotherapy patients.
Another self-care measure was distracting the mind by listening to music before, during, and after the chemotherapy. Music influences physical and mental–spiritual side effects of chemotherapy, restores calm, improves mood and quality of life, creates a sense of healthiness, and improves immunity system response. Consistently, Karagozoglu et al27 and Vanbockstael et al28 noted that music was effective on reducing severity of nausea and emesis in the patients under chemotherapy.
One of the main elements of the self-care education was training about nutrition. A list of dry, carbohydrate-rich, protein-rich, and vitamin-rich foods was recommended to the participants. Our results in this regard are consistent with Karimi et al29 who examined effectiveness of Orem’s self-care model on clinical condition of colorectal cancer patients. In addition, the patients were asked to use ginger before, during, and after chemotherapy. As a medicinal herb, ginger is known as a treatment for nausea and emesis without any specific side effect. Ginger candy was recommended to the participants;30 using ginger to control nausea and emesis of chemotherapy patients suffering from colorectal cancer has also been reported by Ghanbari et al.31
Taking into account that colorectal cancer is a chronic disease and the disease and the chemotherapy both cause side effects (e.g., nausea and emesis) that influence both physical and psychological health of the patients, having self-care skills is of great help in improving health condition of the patients. One of the key theories toward promotion of self-care in chronic patients is Orem’s self-care theory, also known as lack of self-care nursing theory, which is a key part of nursing knowledge. The structure of this theory comprised six key concepts (namely, self-care, asking for therapeutic self-care, decrease in self-care, nursing factor, nursing system, and an environment factor). Self-care model is the foundation of clinical work in nursing services. Orem argued that by taking care of themselves, people preserve their life and well-being. It appears that the patient feels more health and well-being when they do self-care.4–9 According to Orem, every person needs self-care and has to meet his/her need to preserve his/her health and well-being. This set of needs is known as self-care demand, and eliminating these needs requires increased self-care in each person. One’s ability to do self-care depends on age, income, growth stage of life, life experiences, cultural/social awareness, hygiene, and available resources. These factors are considered as the external variables. Orem’s self-care concepts clearly state that the adults have internal motivations of self-care. Therefore, they are expected to do self-care, health, and well-being improvement activities. According to this theory, nurses play a synergic role by facilitating self-care behaviors and capabilities. Self-care function is especially important in adults facing chronic changes.29
Given the abovementioned statements and since nurses are the main members of medical team, they can transfer responsibilities of self-care to the patients through educating them. Increase in self-care capabilities of the patients reduces the costs of frequent hospitalizations on one hand and improves clinical condition of the patients on the other hand.
Conclusion
The results showed effectiveness of self-care measures on decrease in severity of nausea and emesis. Therefore, by educating these interventions to the health team members, patients under chemotherapy, and family members and by motivating them to implement self-care measure during the course of treatment, the patients would enjoy a great decrease in the severity of nausea and emesis they experience. Consequently, health condition, recovery, and clinical condition of the colorectal cancer patients under chemotherapy can be improved through self-care education. The education will also be effective on reducing the costs of health services.
Limitations
Some variables were beyond our control such as spiritual and mental specifications of the participants, financial condition of the patients, and different motivation and interest level of the participants.
Acknowledgments
This paper is based on the research plan approved by Research and Technology Department of Kermanshah University of Medical Sciences under No. 4144, and it was approved by ethics committee of research deputy affiliated to Kermanshah University of Medical Sciences. The authors wish to thank the university for the financial support and also all the participants and personnel of Imam Reza Hospital of Kermanshah for their valuable cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
Mousavi SM, Gouya MM, Ramazani R, Davanlou M, Hajsadeghi N, Seddighi Z. Cancer incidence and mortality in Iran. Ann Oncol. 2009;20(3):556–563. | ||
Salehi Z, Miri M, Aminian K, Mansour-Ghanaei F. Helicobacter pylori infection and colorectal cancer in Guilan province of Iran. Ann Biol Res. 2011;2:32–39. | ||
Billiard M. Fatigue et troubles du sommeil chez les patients atteints de cancer colorectal. [Fatigue and sleep disorders in patients with colorectal cancer]. J Pathol Biol. 2013;61(5):83–87. French. | ||
Jansen L, Koch L, Brenner H, Arndt V. Quality of life among long-term (≥5 years) colorectal cancer survivors – systematic review. Eur J Cancer. 2010;46(16):2879–2888. | ||
Grant M, McMullen CK, Altschuler A, et al. Gender differences in quality of life among long-term colorectal cancer survivors with ostomies. Oncol Nurs Forum. 2011;38(5):587–596. | ||
Krouse RS, Herrinton LJ, Grant M, et al. Health-related quality of life among long-term rectal cancer survivors with an ostomy: manifestations by sex. J Clini Oncol. 2009;27(28):4664–4670. | ||
Ogata Y, Takeuchi M, Ishibashi N, et al. Efficacy of Elental on prevention for chemotherapy-induced oral mucositis in colorectal cancer patients. Gan To Kagaku Ryoho. 2012;39(4):583–587. | ||
Campos de Carvalho E, Martins FT, dos Santos CB. A pilot study of a relaxation technique for management of nausea and vomiting in patients receiving cancer chemotherapy. Cancer Nurs. 2007;30(2):163–167. | ||
Baker PD, Ellett ML. Measuring nausea and vomiting in adolescents: a feasibility study. Gastroenterol Nurs. 2007;30(1):18–28. | ||
Gray NM, Hall SJ, Browne S, et al. Modifiable and fixed factors predicting quality of life in people with colorectal cancer. Br J Cancer. 2011;104:1697–1703. | ||
Piamjariyakul U, Williams PD, Prapakorn S, et al. Cancer therapy-related symptoms and self-care in Thailand. Eur J Oncol Nurs. 2010;14:387–394. | ||
Abootalebi G, Vosooghi N, Mohammad Nejad E, Namadi M, Akbari Kaji M. Study of the self-care agency in patients with heart failure. Iran J Crit Care Nurs. 2012;4(1):203–208. | ||
Mohammadpor A, Rahmati Sharghi N, Khosravan S, Alami A. Investigating the level of self-care and supportive educative needs of patients with myocardial infarction, based on Orem’s model. J Res Health. 2013;3(4):489–496. | ||
Masoudi R, Mohammadi I, Ahmadi F, Hasanpour-Dehkordi A. The effect of self-care program education based on Orem’s theory on mental aspect of quality of life in multiple sclerosis patients. Iran J Nurs. 2009;22(60):53–64. | ||
Karimi S, Vanaki Z, Bashiri H, Hassani SA. The effects of Orem’s self-care model on the nutrition status and fatigue of colorectal cancer patients. J Nurs Midwifery Sci. 2016;3(3):1–10. | ||
Yeh CH, Chien LC, Chiang YC, Lin SW, Huang CK, Ren D. Reduction in nausea and vomiting in children undergoing cancer chemotherapy by either appropriate or sham auricular acupuncture points with standard care. J Altern Complement Med. 2012;18(4):334–340. | ||
Lalla RV, Saunders DP, Peterson DE. Chemotherapy or radiation-induced oral mucositis. Dent Clin North Am. 2014;58(2):341–349. | ||
Morrow GR. A patient report measure for the quantification of chemotherapy induced nausea and emesis: psychometric properties of the Morrow assessment of nausea and emesis (MANE). Br J Cancer Suppl. 1992;19:S72–S74. | ||
Raghavendra RM, Nagarathna R, Nagendra HR, et al. Effect of an integrated yoga programme on chemotherapy – induced nausea and emesis in breast cancer patients. Eur J Cancer Care (Engl). 2007;16(6):462–474. | ||
Chan CW, Cheng KK, Lam LW, Li CK, Chik KW, Cheung JS. Psycho-educational intervention for chemotherapy–associated nausea and vomiting in paediatric oncology patients: a pilot study. Hong Kong Med J. 2008;14(5 suppl):32–35. | ||
Luisi FA, Petrilli AS, Tanaka C, Caran EM. Contribution to the treatment of nausea and emesis induced by chemotherapy in children and adolescents with osteosarcoma. Sao Paulo Med J. 2006;124(2):61–65. | ||
Ebrahimi SM, Parsa-Yekta Z, Sedighi S. Ginger effects on control of chemotherapy induced nausea and vomiting. Tehran Univ Med J. 2013;71(6):395–403. | ||
Bakhshi M, Memarian R, Azad Fallah P. The effect of progressive muscle relaxation on the dosage of antiemetic drugs in cancer patients undergoing chemotherapy. Horiz Med Sci. 2009;15(3):5–12. | ||
Molassiotis A. A pilot study of the use of progressive muscle relaxation training in the management of post chemotherapy nausea and vomiting. Eur J Cancer Care. 2008;9:230–234. | ||
Arakawa S. Relaxation to reduce nausea, vomiting and anxiety induced by chemotherapy in Japanese patients. Cancer Nurs J. 1997;20:343–348. | ||
Tipton JM, Mc Daniel RW, Barbour L, et al. Putting evidence into practice: evidence-based interventions to prevent, manage, and treat chemotherapy-induced nausea and vomiting. Clin J Oncol Nurs. 2007;11(1):69–78. | ||
Karagozoglu S, Tekyasar F, Alp Yilmaz F. Effects of music therapy and guided visual imagery on chemotherapy-induced anxiety and nausea–vomiting. J Clin Nurs. 2013;22(1):39–50. | ||
Vanbockstael J, Coquan E, Gouerant S, Allouache C, Galais MP. How to improve the prevention of chemotherapy-induced nausea and vomiting? The French NAVI study. Support Care Cancer. 2016;24(3):1131–1138. | ||
Karimi S, Vanaki Z, Bashiri H. The Effect of Self-Care Plan Based on Orem’s Self-Care Model on Clinical Improvement in Patients with Gastrointestinal Cancer. Tehran: Theses Skilled Nursing, School of Medicine, Tarbiat Modarres University; 2014. | ||
Palatty PL, Haniadka R, Valder B, Arora R, Shrinath M. Ginger in the prevention of nausea and vomiting: a review. Crit Rev Food Sci Nutr. 2013;53(7):659–669. | ||
Ghanbari A, Montazeri AS, Niknami M, Atrkar Roshan Z, Sobhani A, Najafi B. [Effect of adding ginger to routine treatment on the intensity of chemotherapy-induced nausea and vomiting in cancer patients who referred to Razi Hospital, Rasht]. J Ardabil Univ Med Sci. 2010;10(4):352–361. (Full text in Persian). |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.