")
Back to Journals » Advances in Medical Education and Practice » Volume 11
Survey on the Quality of Care Standards in a Nursing/Midwifery Training Hospital at Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, 2019
Authors Habte T , Tsige Y, Cherie A
Received 6 May 2020
Accepted for publication 22 September 2020
Published 16 October 2020 Volume 2020:11 Pages 763—774
DOI https://doi.org/10.2147/AMEP.S260339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Teshome Habte, Yosief Tsige, Amsal Cherie
Department of Nursing, School Nursing and Midwifery, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Teshome Habte Email [email protected]
Objective: The aim of this article was to conduct a survey on the quality of care standards in nursing/midwifery training hospital of Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia.
Methods: A multiple methods design was used for the study. For the quantitative phase, 35 nurses, 35 patients, and 52 patient charts were selected by simple random sampling from eight randomly selected wards of the hospital. For the qualitative phase, purposive sampling was employed to select participants for focus group discussion and in-depth interview. Twelve instructors and 11 head nurses were recruited. The Quality Audit tool developed by Ethiopian Federal Ministry of Health was applied.
Results: It was found that the nursing and midwifery service quality standards were low and did not meet Ministry of Health standards. The chart review showed that 83% of nursing and midwifery assessments were not completed within eight hours of patient arrival, and in over half the charts (58%), there was no written evidence of compilation of data based on Gordon’s functional model. Only two wards met Standard 1 with adequate medical equipment for nursing diagnosis or intervention. Seventy-five percent of the wards had a scarcity of materials and supplies needed to provide a quality nursing service. Half the nursing stations had adequate patient visibility, and half had an organized chart filing system based on the patient’s bed number.
Conclusion: A high proportion of wards were not meeting Ministry of Health standards for nursing midwifery services. Improvement in care standards is vital to enable the hospital to function as a clinical setting for the education of health-care students. This might be achieved through ongoing attention to quality improvement and a program of in-service training regarding national care quality standards for managers, nurses, and midwives.
Keywords: quality of care, standards, nursing/midwifery, hospital
Introduction
Background Information
In the globalized context, in which science, technology and information lie within many people’s reach, the professions, and particularly nursing and midwifery, are confronted with the need to improve their work processes with a view to guaranteeing provision of high-quality care to the patients.1,2 The new health-care technologies have increased the costs of the health sector and the population’s expectations with regard to the services offered. Nevertheless, studies indicate flaws in the quality and safety of care, involving unwanted events that negatively affect the health organizations’ image.3,4 Although different countries present problems in the quality and safety of hospital care, efforts have been made to improve their efficiency and efficacy. Therefore, the World Health Organization has recommended that managers take into account the citizens’ expectations in decision-making and, since then, various studies about patient satisfaction through quality and integrated service have been conducted.5–7 As nursing and midwives are practice-oriented professions that deal with the life of individuals, it needs competency through community-based team training, and hospital-based provision of service in different settings by ongoing integration of theory and practice followed by an internship or professional practice. It is committed to the development and implementation of practice standards through ongoing acquisition, application and evaluation of relevant knowledge, skills, attitudes and judgment. The critical contribution of nurses and midwives helps to improve the outcome of the health-care service.6,8,9 Development of a problem-oriented integration document to be used as a guide for the implementation of the program considered the critical mass of patient, staff, and student, service continuity and complex nature of the academic and service activities.
The School of Nursing and Midwifery is dedicated to contributing as a center of excellence by advancing relevant, innovative and creative teaching, together with research and community services responsive to national and international demands.
Statement of the Problem
Nursing education is currently facing challenges related to the application of nursing knowledge in clinical environments and inability of students in the application of nursing procedures in clinical settings. The School of Nursing and Midwifery should represent the best means of identifying these challenges. Universities are responsible for the disseminating and transferring knowledge, as well as for providing specialized human resources. In addition, they are continually required to analyze and update their services, and to identify problems and challenges to allow them to optimize the quality of educational and nursing and midwifery service.7,10 It is clear that provision of high-quality, affordable, integrated health-care service is an increasingly difficult challenge. Due to the complexities of health-care services and systems, investigating and interpreting the use, costs, quality, accessibility, delivery, organization, financing, and outcomes of health-care services is the key to informing government officials, insurers, providers, consumers, and others making decisions about health-related issues.4,11 Currently, nursing and midwifery care are practiced based on sound scientific principles embedded in a process called the nursing process. The nursing process has been accepted by the nursing profession as a standard for providing ongoing nursing care that is adapted to individual client’s needs.2,12
The need to improve the quality of nursing and midwifery services in Tikur Anbessa Specialized Hospital is one of the major health-care items on the agenda. Involvement of academicians in clinical services is essential to improve the quality of service through the strategy of education, service, and research-based integration of nursing and midwifery activities.
Significance of the Study
Integration of nursing and midwifery service, education, and research is fundamental to the health-care reform goals of improving the quality of care for individual and the population via the efficient and effective use of resources. The increased complexity of care, growing numbers of patients with chronic disease, and exploding health-care costs heighten the need for better integration of care without increased expenditure.3,13 Very convincing evidence indicates that non-integrated service or uncoordinated care greatly increases health-care service costs, but there is still a need to identify “best practices” and describe models and interventions that achieve patient-centered, high-quality nursing and midwifery service. Therefore, assessing the quality of nursing and midwifery services at Tikur Anbessa Specialized Hospital (TASH) would be the most important variable used as baseline information for the proposed implementation process of service integration. The integration of service, education, and research activities of nurses and midwives are expected to improve the health-care service outcomes of patient at TASH and helpful to clinical exercise for teaching staff of Nursing and Midwifery Department of Addis Ababa University. In addition to these, designing nursing and midwifery service program integration building substantial support requires new evidence forms, new roles, new teams, and new practice cultures used as a good practice model for the national program in the country.
Therefore, the information obtained from this study was designed to develop a sustainable integration program through baseline information obtained from the assessment of the nursing and midwifery service is vital to determine and alleviate the potential and actual gaps and helpful to develop a comprehensive document that is required to guide a fully integrated nursing and midwifery service, education, and research at Tikur Anbessa Specialized Hospital.
Objectives of the Study
General Objective
It is aimed to conduct a baseline survey of quality of care standards in a nursing/midwifery training hospital of Tikur Anbessa Specialized Hospital in Addis Ababa, Ethiopia, 2019.
Specific Objectives
- Assess the availability of necessary facilities, equipment and supplies at TASH
- Identify nursing and midwifery management functionality at TASH
- Assess the level of nursing midwifery care practice at TASH
- Verify patient-centered nursing midwifery service is given to all patients
- Explore academic staff clinical role besides conducting teaching and research activities
- Explore clinical service staff academic role besides clinical activities
Methods and Materials
Study Area
The Tikur Anbessa Specialized Hospital (TASH) is a teaching hospital of the college. TASH is the largest specialized hospital in Ethiopia, with over 700 beds, and serves as a training center for undergraduate and postgraduate medical students, dentists, nurses, midwives, pharmacists, medical laboratory technologists, radiology technologists, and others who shoulder the health problems of the community and the country at large.
In line with the mission and vision of AAU, the CHS exercises unique roles in training highly skilled health professionals at MSc, PhD, specialty, and subspecialty levels. This allows it to contribute to the expansion of quality health care, education, and research in the country. The CHS is the only institution where some specialized tertiary health care is rendered. Moreover, under the new structure of AAU, the CHS is expected to enjoy a high level of academic and administrative autonomy.8
Study Design
An institution-based descriptive cross-sectional study design using quantitative and qualitative methods was conducted.
Sampling Techniques and Sample Size Determination
Sampling Techniques
Eight from 19 wards of the inpatient department at the Black Lion Hospital, one ward from each specialty (medical, surgical, obstetrics, gynecology, ICU, oncology, orthopedics and pediatrics), were selected using simple random sampling.
Sample Size
The sample size determination of the quantitative study is depicted in Table 1. The minimum requirement of sample size for each standard was adopted from the Federal Ministry of Health, Ethiopia National Supportive Supervision and Baseline Assessment on Nursing and Midwifery Service Quality Standards audit tool.3
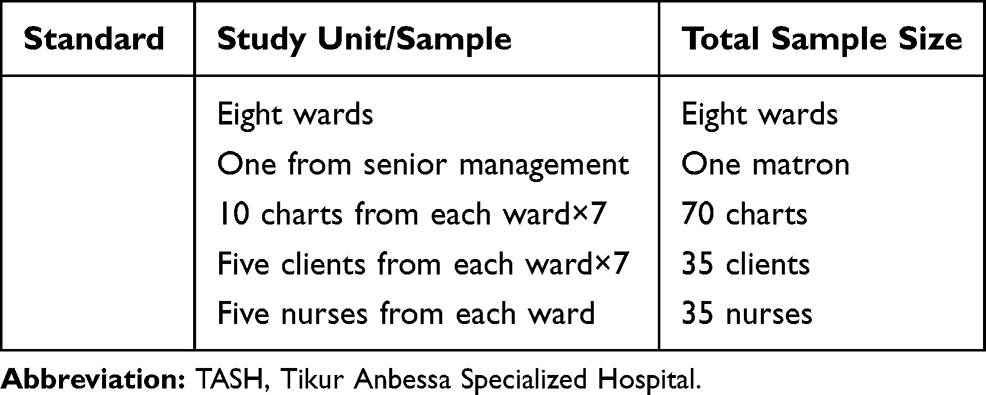 |
Table 1 Sample Size Determination of Quantitative Study Used for the Baseline Survey of Nursing and Midwifery Service, Teaching and Research Integration at TASH, 2019 |
A purposive sampling technique was used to select participants for focus group discussions (FGDs) and in-depth interviews. Twelve instructors (six senior and six junior) and 11 head nurses (five senior and six junior) were involved, along with six mangers for the in-depth interviews.
Data Collection
First quantitative data were collected from four data sources (observation, document review, client’s chart and client interview), followed by qualitative data collection through focus group discussion and in-depth interview.
Quantitative Data Collection and Measures
The quantitative data were collected using nursing and midwifery service quality audit tool adapted from the Federal Ministry of Health, Ethiopia National Supportive Supervision and Baseline Assessment on Nursing and Midwifery Service Quality Standards audit tool of FMOH3 comprising four standards:
Standard One: Facilities, equipment, and supplies needed to provide a quality nursing service containing 13 scores through observation data collection technique
Standard Two: Functional nursing midwifery management comprising 36 points using document review and matron interview
Standard Three: Quality nursing midwifery service is ensured for all patients from 225 points from chart review
Standard Four: Patient-centered nursing midwifery service is given to all patients composed of 120 points using client and nurse interview data collection technique
Qualitative Data Collection
Qualitative data were collected using focus group discussions and in-depth interview. The focus group discussion (FGD) guide with instructors consisted of eight themes: role of instructors in clinical instruction of nurse and midwife students, instructor related challenges to clinical instruction, school level challenges to clinical instruction, hospital factors affecting clinical instruction, college factors affecting clinical instruction, colleague factors affecting clinical instruction, student-related factors affecting clinical instruction and patient related factors and solutions to alleviate these problems.
FGD guide with hospital nurses comprising three themes: role of nurses in clinical instruction of nurse and midwife students, challenges to clinical instruction, and possible solutions to address the challenges.
In-depth interview with matron, head nurses, head of Department of Nursing and Midwifery, Dean School of Allied Health Sciences, Clinical Director of Black Lion Hospital and Chief Executive Director of The College of Health Sciences containing of three themes: benefits of Black Lion Hospital nursing service and department of nursing and midwifery integration, challenges of nursing service and department of nursing and midwifery integration, and remedies for the successful integration of nursing service and department of nursing and midwifery.
The discussions and interviews were moderated by principal investigators and a research assistant took field notes of each session. The FGD took, on average, 90 min to two hours and the in-depth interview from 60–90 min. Discussions and interviews were tape recorded after securing consent from the participants. Data were collected to the level of information saturation.
Data Collectors
Ten data collectors and two supervisors were involved in the data collection process.
Data Processing and Analysis
The collected data were coded, entered, and cleaned with EpiData 3.1 for the descriptive statistics such as frequencies and percentages were used to describe the responses of the quantitative data. For the qualitative responses all transcripts from FGDs and in-depth interviews was coded, transcribed verbatim, and analyzed thematically and the findings were presented with examples from the participants’ descriptions.
Ethical Approval and Consent to Participate
Ethical approval and verbal consent were acceptable and approved by the Institutional Review Board of Department of Nursing and Midwifery, College of Health Sciences, Addis Ababa University. The objectives of the study were explained to study participants. Verbal informed consent was obtained from study participants. All collected information was kept confidential. Coding and aggregate reporting was used in data presentation to ensure anonymity.
Result and Discussions
From 19 wards of Black Lion Hospital, one ward from each specialty (medical, surgical, obstetrics, gynecology, ICU, oncology, orthopedics and pediatrics) of inpatient department, eight wards were selected using simple random sampling for quantitative data and FGD and in-depth interview employing qualitative data. Twelve instructors (six senior and six junior) and 11 head nurses (five senior and six junior) participated in the study.
Qualitative Data
Sociodemographic Characteristics of Participants
The sociodemographic characteristics of the participants shown in the Table 2 below; About 55.5% of the head nurses were female. Regarding their clinical experience, the majority (46%) of the head nurses had clinical experience of more than 10 years. The majority (73%) of the head nurses were BSc holders and only 27% of them were MSc holders. Among the instructors involved in the FGD, 58% were female and 75% had less than fvie years’ work experience in a clinical area. Regarding their educational background, about 67% the instructors had MSc degree and above.
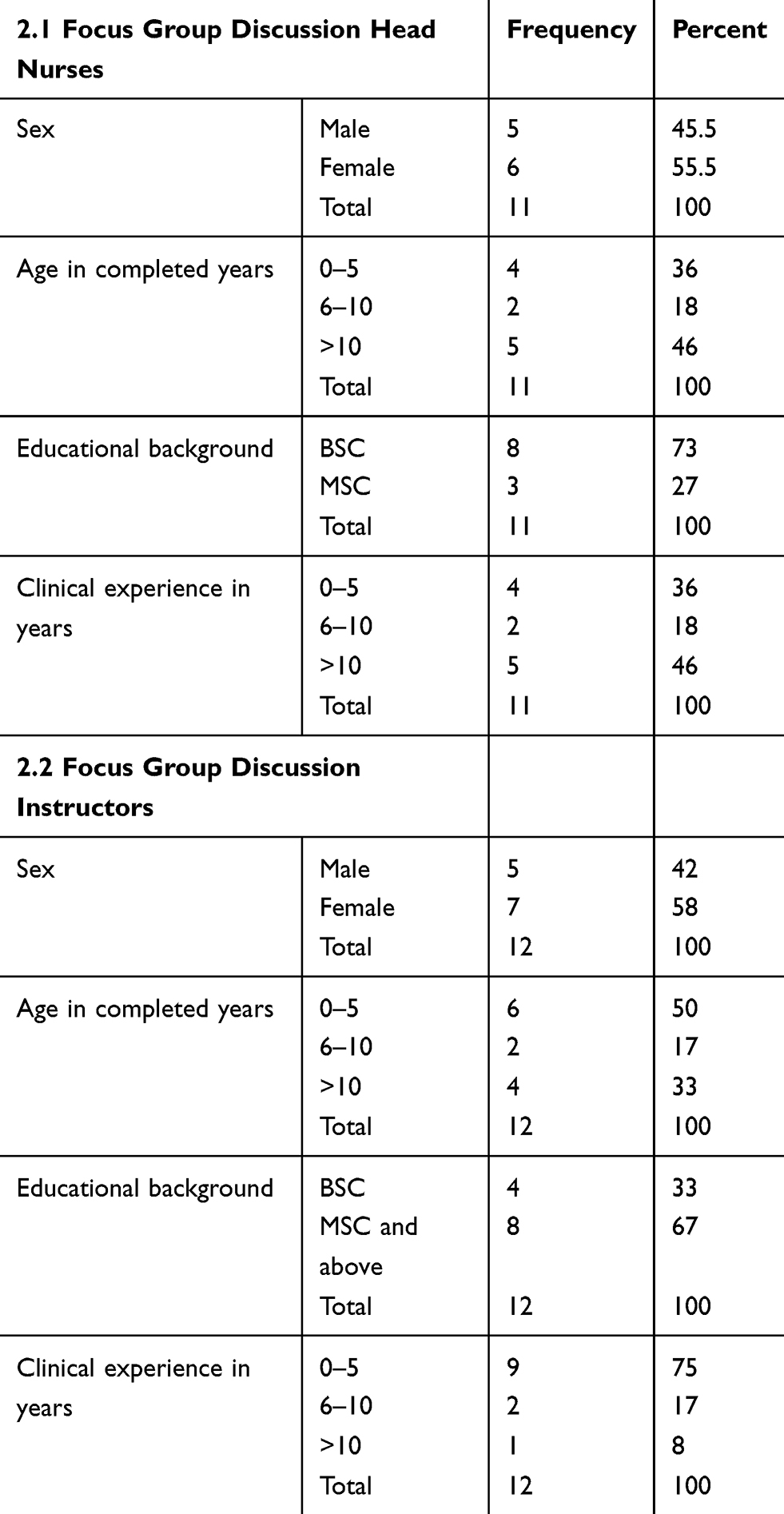 |
Table 2 Demographic Characteristics of Participants in the Focus Group Discussion Used for the Assessment of Baseline Survey for the Integration of Teaching Clinical Service Between Tikur Anbessa Specialized Hospital and School of Nursing and Midwifery, 2019 |
Quality of Nursing and Midwifery Care Provided by Ward Nurses
Participants expressed that nurses and midwives strive to render quality service. However, multilevel factors, such as factors from the management, nurses/midwives themselves, colleagues, and patients affect the delivery of effective and efficient services. Ward nurses and midwives expressed that
We want to give appropriate care to our patients but we seldom get the materials and equipment we need to give care to our clients; resource scarcity is one of the hindrances to provide quality patient care.
The other problem raised is “nurses and midwives are not given the autonomy to perform nursing and midwifery tasks and procedures; most of the tasks are overtaken by doctors. Nursing and midwifery as a profession has its own scope of practice and have independent, dependent and interdependent role.
However, because of power imbalance nurses are expending most of their time on the dependent role. Attitude towards team work is very low”. Skill gap and lack of up-to-date knowledge is the other factor for poor quality nursing care
Some of the nurses and midwives are not adequately prepared during their nursing and midwifery training. There is skill gap and no on the job or off job training is given and also there is no professional development scheme.
They also described that “there is work overload and patient to nurse ratio is high”. They also pinpointed that the effort of the management to motivate nurses and midwives is very low.
There is no recognition, appreciation and opportunity for growth. There is no equal and fair treatment. Nursing is not seen as a profession. There is a perception that some professions are taken as superior and nursing and midwifery as inferior.
Ward Nurses and Midwives Perception About Clinical Teaching of Student Nurses and Midwives
Four-level factors were raised about challenges of clinical teaching of student nurses and midwives. The first factor raised is ward nurses and midwive’s perception about clinical teaching. There are mixed and differing views among nurses and midwives about clinical teaching of student nurses and midwives. Some of the nurses and midwives say “It is our duty to teach students. It is written in our job description”. Others say “Our responsibility is to our patients not to students”. Even those who said it is our duty to teach students said
We show them only the way when we have time. We give priority to our patients. There is work overload; as a result, we don’t have time to teach students. We say them participate yourself. If they are interested and active let them see what we are doing.
They emphasized that
Ward nurse’s role in clinical instruction is not clearly defined, and there is no guideline. Even when students are assigned to our ward, they don’t come with the course objectives because of this we don’t know the area to be emphasized.
The second factor pinpointed is teacher related.
They said the prime responsibility of teaching students lies on the teacher. However, we seldom see teachers disposing this responsibility. Apart from assigning students and sometimes taking attendance (head counting) the teachers are not following their students regularly; they don’t do the clinical teaching. Teachers are not stationed in the service area. It seems that some of the teachers themselves lack the practical skill, there is skill gap.
The third point raised by ward nurses and midwives about challenges of clinical instruction is the student-related factor.
Students are not oriented about the profession and internalized the profession as a result some of them are not eager to learn and some others don’t have interest about the profession. It is good if the Ministry of Education assigns students based on their interest and the school should continuously work on helping students to internalize the professional culture and increase their commitment by being role model and inculcate the expected knowledge, attitude and skill.
The fourth challenge to clinical teaching accentuated by ward nurses and midwives is the factor related to management.
We don’t have adequate resource to teach students. Let alone to students there is resource scarcity to give patient care. In addition, the number of students assigned to the hospital is beyond its capacity. Our hospital receives students from different teaching Institutions from Addis Ababa and all over Ethiopia. The student’s number is more than the patients. There is patient fatigue. The cases we have will not be adequate to this large number of students.
Perception Towards the Benefit of School of Nursing and Midwifery and Tikur Anbessa Specialized Hospital Nursing and Midwifery Service Integration
Ward nurses and midwives, instructors, and mangers underlined the importance of integration to the provision of quality of service rendered to patients, nurses and midwives working in the hospital, school of nursing, and midwifery instructors and the college at large.
They highlighted that “Integration facilitates the correlation of teaching, service and research; it gives chance to teachers to be involved in the service of the hospital”. They said
all benefit from the synergy of the integration, there will be knowledge transfer from the school to service and from service to school. Integration of the hospital and the school human and material resource help improvements in the quality of service, patient satisfaction, improved patient outcome including length of hospital stay, and service standard.
They also emphasized
the integration helps to establish clear communication and good relationship between the hospital and the school. Furthermore, integration promotes Evidence Based Practice and facilitation of problem-solving research.
Teacher’s Perception About Clinical Teaching of Student Nurses and Midwives
The teachers said one of the challenges to clinical teaching is student’s dormitory and hospital proximity. “The student’s residence is far from the hospital. Much of student’s practical time is wasted through transportation. Students arrive late and leave early”.
Problem with the teaching environment was raised as a challenge for teachers to teach their students in the clinical area. Some of the teachers said
the environment is not receptive to students and conducive for clinical teaching. There is unwelcoming reception by departments in the hospital especially Doctors
Another challenge expressed is organization, timely planning and delivery of courses. There must be proper horizontal and vertical organization of courses and early planning and selection of student’s practical placement. Schedules should not be distributed at the eleventh hour. The practical assignment should also consider teacher's time and workload (sometimes, instructors are assigned two different health care institutions at a time to coach students in their clinical practice, for example, an instructor is assigned at St Paul hospital to supervise for MSc trainees as well as assigned at Black lion hospital with BSc students in addition to theoretical session). There should be fair distribution of workload. The school and the hospital should plan together student’s clinical placement and clinical teaching. Formulation of clinical instruction guideline is essential to have consistent clinical teaching”.
The attitude of teachers toward their profession and clinical instruction are the factors underscored by the discussants.
Teachers should be role model to their students. Some of the teachers don’t have a positive feeling about their profession. Some of them think practical teaching is not their responsibility. Some lack the clinical skill to teach their students. Some of the teachers give more attention to outside work they don’t have time to teach their students in the clinical area.
Challenges from School of Nursing and Midwifery and Tikur Anbessa Specialized Hospital Nursing and Midwifery Service Integration
The challenges expressed from the School of Nursing and Midwifery and Tikur Anbessa Specialized Hospital Nursing and Midwifery service integration are:
- Workload
- Attitude of ward nurses, midwives, and instructors towards integration
- Readiness of the School of Nursing and Midwifery and Tikur Anbessa Specialized Hospital Nursing and Midwifery towards integration
- Managerial commitment and resource availability for the integration.
Types of Integration
For successful integration, higher performance and sustainability of integration, functional and structural integration is proposed by discussants and interviewees.
Quantitative Data
The quantitative finding of this baseline survey is summarized according to the four nursing and midwifery service quality standards.
Standard 1
Standard one is about facilities, equipment’s, and supplies needed to provide a quality nursing/midwifery service. It has three quality statements with eight quality measures. Seven of the quality measures are for the first statement and two are for the second and third statements (one for each). As depicted in Table 3, of the eight wards visited during the assessment, half of them have nursing stations that have visibility of patients and of circulation paths, have organized and efficient chart filing systems on a shelf and central or room cabinet for medication store based on the patient bed number. Seven of eight wards have dressing room with locker and only two wards have medical equipment for nursing diagnosis or intervention use.
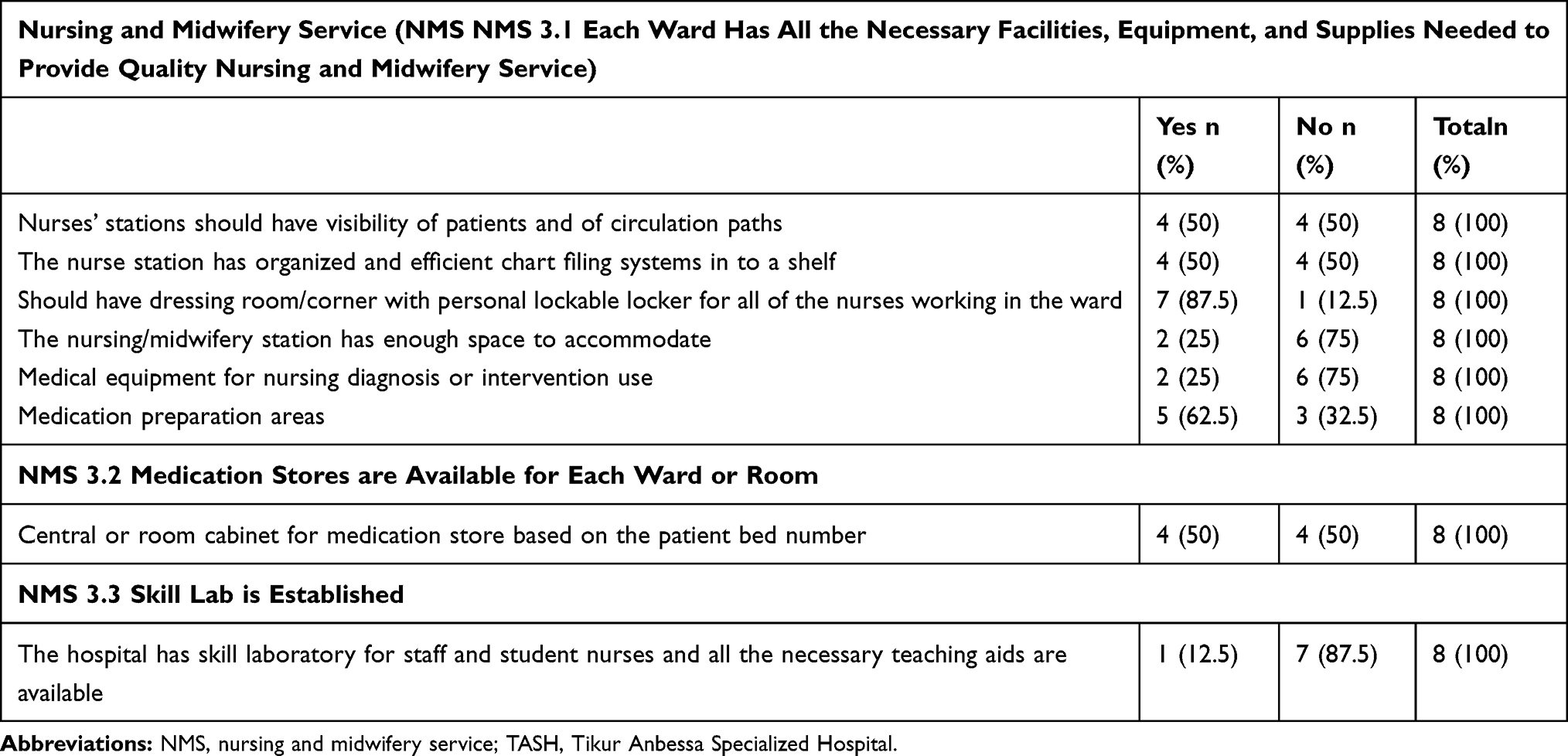 |
Table 3 Availability of All the Necessary Facilities, Equipment, and Supplies Needed to Provide Quality Nursing and Midwifery Service at TASH, June 2019 |
Standard 2
Standard 2 is about functionality of the nursing and midwifery service management, which comprise two quality statements with four quality measures for each. The two quality statements entail eight and 28 points, respectively, making a score of 36 points for the standard. As shown in Table 4, the hospital obtained 50% for the first quality measure which is about the functionality of nursing and midwifery management. Even if the matron/nurse midwifery director of the hospital is a member of the SMT, she is not regularly participating in an SMT meeting and regular refreshment training was not offered for all staffs, at least quarterly. However, the hospital conduct quality improvement projects identified nursing midwifery service quality gaps with a score of 93% assigned for the quality statement.
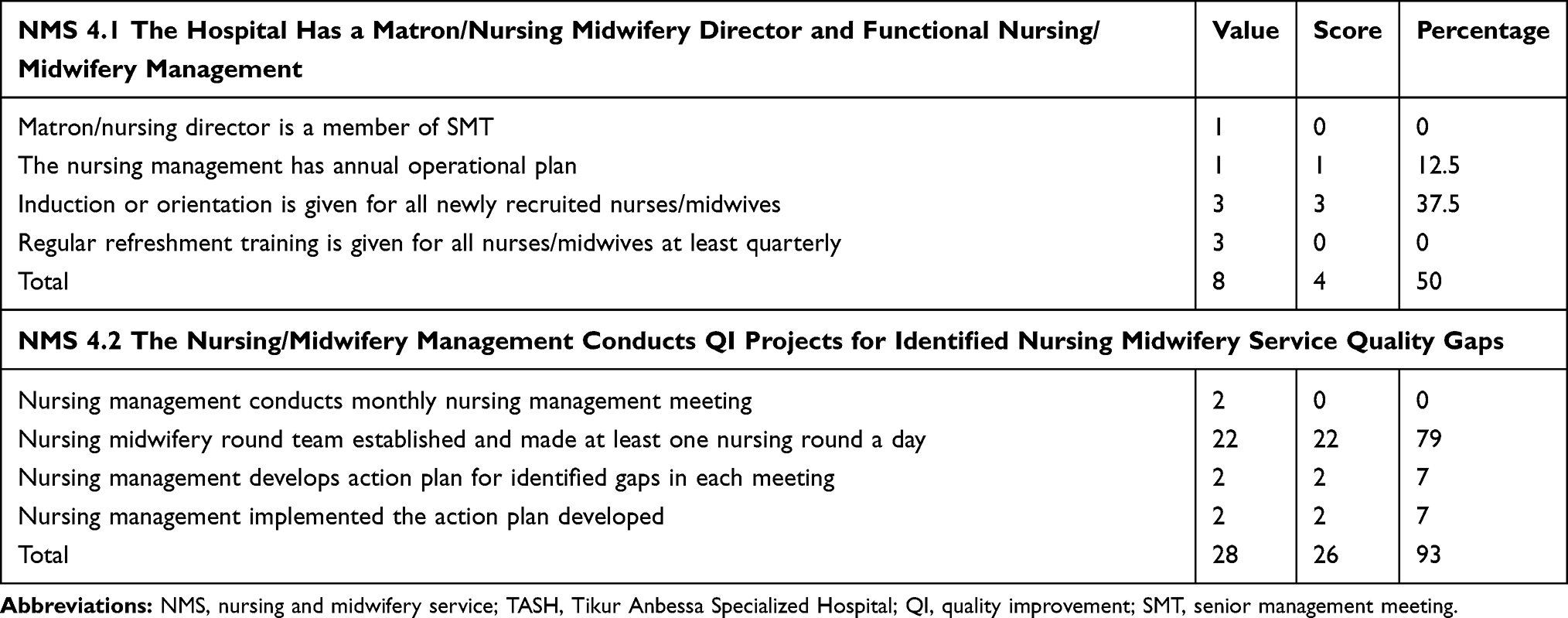 |
Table 4 Functionality of the Nursing and Midwifery Service Management at TASH, June 2019 |
Standard 3
Standard 3 is about provision of quality nursing/midwifery service for all patients using nursing process as an approach. It entails five quality statements with 22 quality measures. Fifty-two patient charts were randomly selected from even wards for the assessment of this standard.
Comprehensive nursing and midwifery assessments are not done for all patients admitted to the hospital as shown in Table 5. There is no written evidence of a compilation of data (57.7%); the majority (82.7%) of nursing and midwifery assessments were not completed within eight hours of patient arrival. Furthermore, all entries in the nursing process are not legible, dated, timed and signed (69.2%).
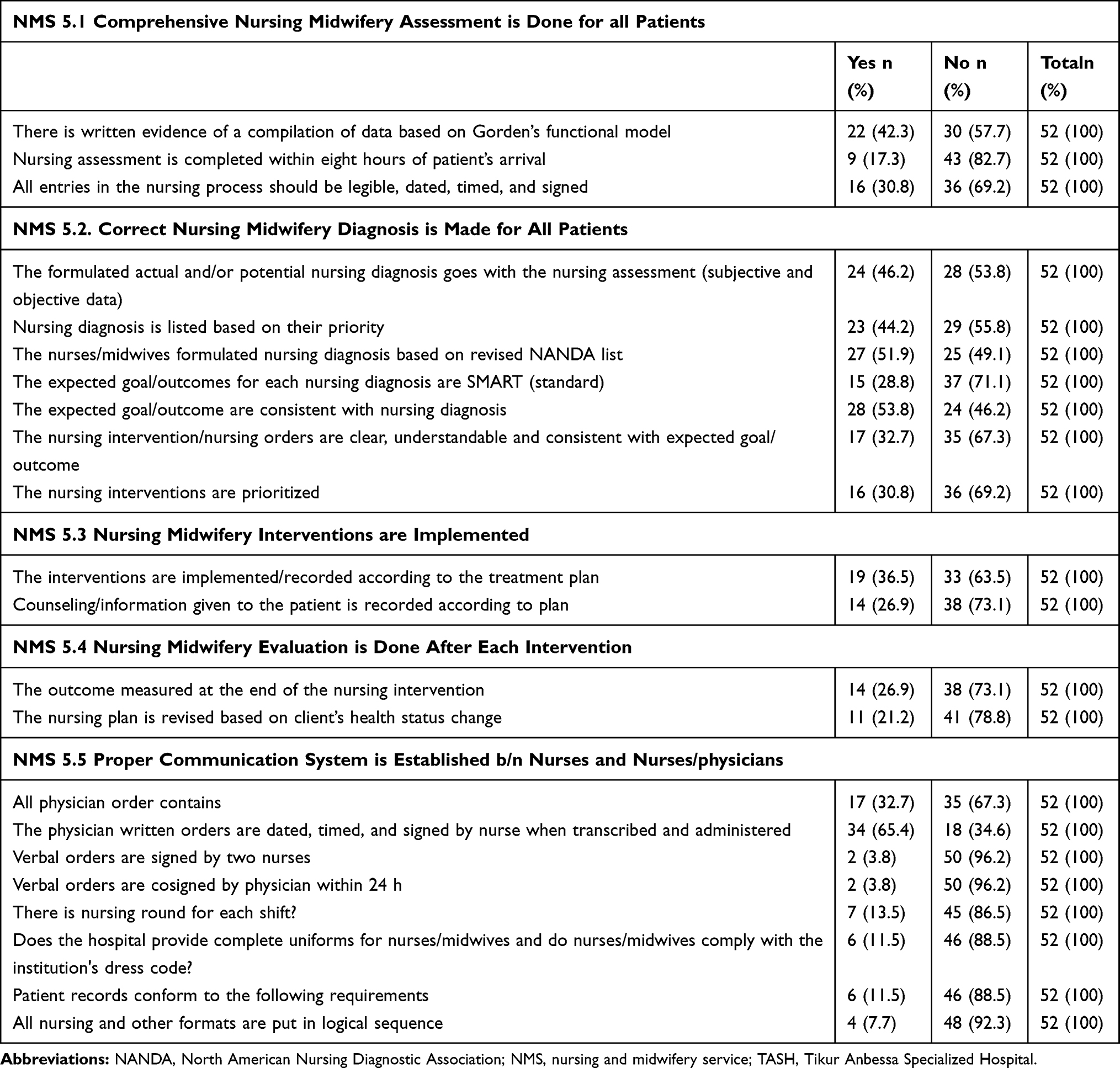 |
Table 5 Provision of Quality Nursing and Midwifery Service to All Patients at TASH, June 2019 |
Regarding formulation of correct nursing diagnosis, this survey revealed that most of the quality measures set for this quality statement are below the expected standard. For example, establishment of goal or outcome for each nursing diagnosis are not meeting the standard (71.1%), the nursing interventions are not prioritized (69.2%), and the nursing intervention/nursing orders are not clear, understandable, and consistent with expected goal/outcome (67.3%). With regard to implementation of nursing and midwifery interventions, counseling/information given to the patient is not recorded according to plan and interventions are not implemented/recorded according to the treatment plan (63 and 73%, respectively). This survey also revealed that nursing and midwifery evaluation after each intervention is not done. The outcome is not measured at the end of the nursing intervention and the nursing plan is not revised based on clients’ health status change (73 and 78%, respectively).
Establishment of proper communication between nurses and nurses and physicians is an important parameter for provision of quality nursing and midwifery service to the patient. However, this survey reveals a gap in this regard. For instance, there is no practice of writing up and signing verbal orders by two nurses and cosigning by physician within 24 h (96.2%). Furthermore, all nursing and other formats are not put in logical sequence (92.3%), patient records do not conform to the necessary requirements (88.5%), and there is no nursing round for each shift (86.5%).
Standard 4
Standard 4 is about provision of patient-centered nursing/midwifery service to all patients. It comprises three quality statements with 12 quality measures. A total of 70 randomly selected study subjects (35 patients and 35 nurses) were interviewed for this standard.
As depicted in Table 6 below, most of the patients responded that all patients are involved in the plan of care. Accordingly, the majority of them replied that there is a system to involve all patients when changes to nursing and midwifery services are proposed and all patients are provided with information about arrangements for first contact (65.7% and 62.9%, respectively). Furthermore, a large proportion of the patients responded that all patients were approached with dignity and respect, addressed by name, and encouraged to ask questions. With regard to this quality measure, the majority of the patients responded that they were introduced with the name of the nurse during treatment sessions (77.1%), they were given a chance to ask questions (77.1), staffs are polite and considerate (71.4%), and all patients are given all the privacy they need (65.4%).
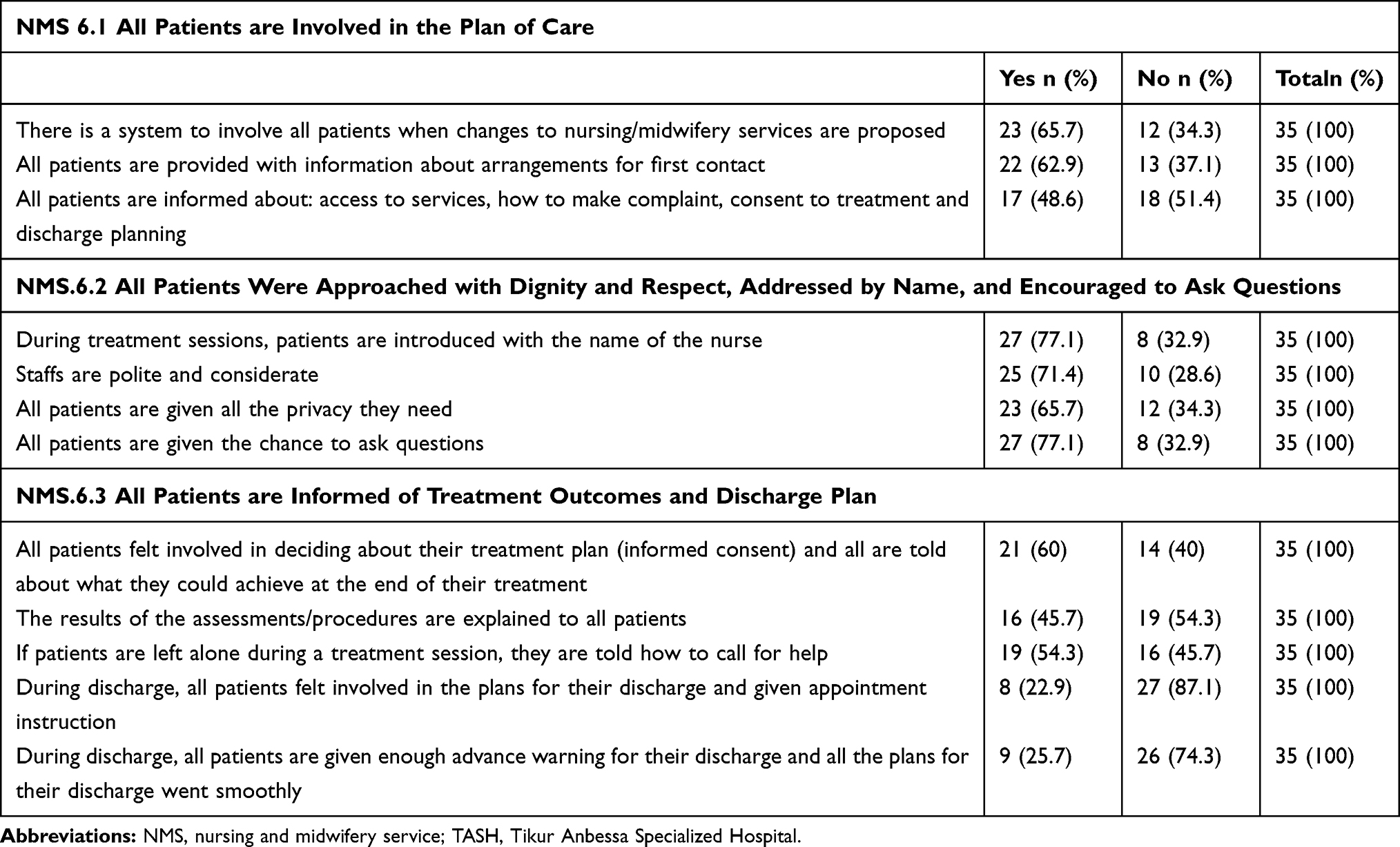 |
Table 6 Patients’ Response to Provision of Patient-centered Nursing/Midwifery Service to All Patients at TASH, June 2019 |
Regarding being informed of treatment outcomes and discharge plan, the majority (87.1%) of the patients did not feel involved in the plans for their discharge and given appointment instruction. Furthermore, most of the patients (74.3%) responded that they were not given enough advance warning of their discharge and plans for their discharge did not go smoothly.
According to the assessment finding in standard 4 it reveals that most of the nurses responded that all patients are involved in the plan of care. Accordingly, the majority of them replied that there is a system to involve all patients when changes to nursing and midwifery services are proposed and all patients are provided with information about arrangements for first contact (65.7% and 77.1%, respectively). Furthermore, a large proportion of the nurses responded that all patients were approached with dignity and respect, addressed by name and encouraged to ask questions. With regard to this quality measure, the majority of the nurses responded that staffs are polite and considerate (100%), patients were given a chance to ask questions (88.6), patients were introduced with the name of the nurse during treatment sessions (65.7%), and all patients are given all the privacy they need (65.7%).
Regarding informing all patients about treatment outcomes and discharge plan, the majority (65.7%) of the nurses responded that all patients felt involved in the plans for their discharge and given appointment instruction. Furthermore, most of the patients (65.7%) responded that they were given enough advance warning for their discharge and plans for their discharge did not go smoothly.
Strength and Limitation of the Study
The strength of the institutional-based study was that both quantitative and qualitative methods were employed to triangulate the results. Conversely, the limitation was that limited research was conducted in this regard and the results were difficult to compare.
Conclusion and Recommendations
Conclusion
The following conclusions are drawn based on the facts that are observed in the results:
- Skill and knowledge gap of instructors and ward nurses and midwives
- Lack of professional autonomy
- Low attitude towards teamwork
- Work overload and patient to nurse ratio is high
- Lack of recognition, appreciation, and unfair treatment among professionals
- Lack of clearly defined nurse’s/midwives’ role in clinical instruction and guideline
- The hospital is lacking the necessary equipment and supplies to provide quality nursing care (Standard 1)
- The hospital is not ensuring a quality nursing midwifery service for all patients (standard 3).
Recommendations
- Introduction of structural and functional integration model
- Help the two entities and employees within to own the integration through continuous discussion and communication
- Provide continuous training to address skill gap of instructors, ward nurses, and midwives
- Giving autonomy to nurses and midwives to exercise their profession
- Give recognition, appreciation and opportunity for growth and fair and equal treatment.
- Management commitment is vital for success of the integration
- Consideration of workload and fair assignment of responsibility
- Incorporate nursing care practice standards in pre-service curricula.
The following factors should be considered for successful integration, higher performance, and sustainability.
Strategy of the Integration
Pilot test the integration in four selected wards: medical, surgical, obstetrics and gynecology and pediatrics.
Abbreviations
AAU, Addis Ababa University; CHS, College of Health Sciences; NANDA, North American Nursing Diagnostic Association; NMS, nursing and midwifery service; TASH, Tikur Anbessa Specialized Hospital.
Availability of Data Materials
All relevant data are included within the manuscript. If it is necessary, it is possible to contact the corresponding author to get additional material.
Ethical Approval and Consent to Participate
Ethical approval and clearance were obtained from Institutional Review Board of Department of Nursing and Midwifery, College of Health Sciences, Addis Ababa University. The objectives of the study were explained to study participants. Verbal informed consent was obtained from study participants. All collected information was kept confidential. Coding and aggregate reporting was used in data presentation to ensure anonymity.
Acknowledgments
The author would like to thank to all respondents who took their time and participated in the focus group discussion and in-depth interview, particularly to Addis Ababa University College of Health Sciences, chief academic director for the direction given to proceed and willing to provide unreserved support when need arises. We also greatly appreciate the dean of the school of nursing and midwifery for his continuous support and encouragement throughout this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding for this study was made possible through grants offered by Addis Ababa University, College of Health Sciences and Tikur Anbessa Specialized Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. World Alliance for Patient Safety. Summary of the Evidence on Patient Safety: Implications for Research. The Research Priority Setting Working Group of the World Alliance for Patient Safety. Geneva: World Health Organization; 2008.
2. Co-ovadia MY. Identification and evaluation of patient satisfaction determinants in medical service delivery systems within the South African private health care industry; University of Pretori. 2010.
3. FMOH, National Supportive. Supervision and Baseline Assessment on Nursing and Midwifery Service Quality Standards. Addis Ababa, Ethiopia; 2016.
4. FMOH, Nursing Care. Practice Standards: A Reference Manual for Nurses and Health Care Managers in Ethiopia. Addis Ababa, Ethiopia; 2011.
5. Robinson K. Care coordination: a priority for health reform. Policy Policies Nurs Pract. 2010;11(4):266–274. doi:10.1177/1527154410396572
6. American Academy of Nursing. Raise the Voice: Transforming America’s Health Care System Through Nursing Solutions. 2012.
7. Wachter RM, Pronovost SP, Shekelle P. Strategies to Improve Patient Safety: the Evidence Base Matures. Ann Intern Med. 2013;158(5 Part 1):350–352. doi:10.7326/0003-4819-158-5-201303050-00010
8. Addis Ababa university website; 2018. Available from: http://www.aau.edu.et/services/hospital/background-of-college-of-health-sciences/2018.
9. Smith R. Nurses Lack Compassion NHS Admits. The Telegraph; 2012.
10. Aiken L, Rafferty AM, Sermeus W. Caring nurses hit by a quality storm. Nurse Stand. 2014;28(35):22–25. doi:10.7748/ns2014.04.28.35.22.s26
11. Gummer B. Nursing Associate Role Offers New Route into Nursing. UK: Department of Health; 2016.
12. Aiken LH, Clarke SP, Cheung RB, Sloane DM. Silber JH Educational levels of hospital nurses and surgical patient mortality 2003. JAMA. 2003;290:1617–1623.
13. Yakusheva O, Lindrooth R, Weiss M. Economic evaluation of the 80% baccalaureate nurse workforce recommendation: a patient-level analysis. Med Care. 2014;52(10):864–869. doi:10.1097/MLR.0000000000000189
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.