")
Back to Journals » Patient Preference and Adherence » Volume 17
Survey on the Impact of the COVID-19 Pandemic on Patients with Parkinson’s Disease and Their Caregivers in Japan
Authors Hattori N , Okada Y , Kawata Y, Furusawa Y , Imai T, Yoshida H, Ota M , Arai M , Shintani A , Fernandez J
Received 21 December 2022
Accepted for publication 29 March 2023
Published 8 May 2023 Volume 2023:17 Pages 1221—1235
DOI https://doi.org/10.2147/PPA.S402193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Nobutaka Hattori,1 Yoshiko Okada,2 Yayoi Kawata,3 Yoshihiko Furusawa,3 Takumi Imai,4 Hisako Yoshida,4 Mihoko Ota,3 Masaki Arai,3 Ayumi Shintani,4 Jovelle Fernandez3
1Department of Neurology, Juntendo University, Tokyo, Japan; 2Japan Parkinson Congress, Tokyo, Japan; 3Japan Medical Office, Takeda Pharmaceutical Company Limited, Tokyo, Japan; 4Department of Medical Statistics, Graduate School of Medicine, Osaka Metropolitan University, Osaka, Japan
Correspondence: Yoshihiko Furusawa, Japan Medical Office, Takeda Pharmaceutical Company Limited, 2 Chome-1-1 Nihonbashihoncho, Chuo City, Tokyo, 103-0023, Japan, Tel +81-3-3278-2111, Fax +81-3-3278-2000, Email [email protected]
Objective: The coronavirus disease 2019 (COVID-19) pandemic changed the lives of patients with Parkinson’s disease (PD) and their caregivers. This study aimed to investigate changes in patient behavior and PD symptoms and their effect on caregiver burden resulting from the COVID-19 pandemic in Japan.
Methods: This nationwide, observational, cross-sectional survey included patients with self-reported PD and caregivers (members of the Japan Parkinson’s Disease Association). The primary objective was to evaluate changes in behaviors, self-assessed PD symptoms, and caregiver burden from pre–COVID-19 (February 2020) to post–national state of emergency (August 2020 and February 2021).
Results: Responses from 1883 patients and 1382 caregivers from 7610 distributed surveys were analyzed. Mean (standard deviation) age of patients and caregivers was 71.6 (8.2) and 68.5 (11.4) years, respectively; 41.6% of patients had a Hoehn and Yahr (HY) scale of 3. Patients (> 40.0%) reported decreased frequency of going out. Most patients (> 70.0%) reported no change in treatment visit frequency, voluntary training, or rehabilitation and nursing care insurance services. Symptoms worsened for approximately 7– 30% of patients; the proportion with HY scale 4– 5 increased from pre–COVID-19 (25.2%) to February 2021 (40.1%). Aggravated symptoms included bradykinesia, walking, gait speed, depressed mood, fatigue, and apathy. Caregivers’ burden increased because of patients’ worsened symptoms and reduced time going out.
Conclusion: Control measures during infectious disease epidemics should consider that patients’ symptoms may worsen; therefore, patient and caregiver support is needed to reduce burden of care.
Keywords: Parkinson’s disease, COVID-19, questionnaire design, caregiver burden
Introduction
In late 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) led to a global pandemic of coronavirus disease 2019 (COVID-19). The infectious coronavirus leads to a severe respiratory syndrome and potentially to neurological disorders.1 Older people with comorbidities, including diabetes mellitus, cardiac failure, and respiratory disease, are at increased risk for serious COVID-19 illness. Parkinson’s disease (PD) is more prevalent in older people who are often frail and have comorbidities; therefore, elderly patients with PD could be at risk of severe COVID-19 disease.1,2
Many countries implemented lockdowns and social distancing to control the COVID-19 pandemic. These social measures may have changed the lives of patients with PD and their caregivers by reducing access to treatment and rehabilitation services. In addition, reduced socialization may also contribute to physical and mental health effects, even in noninfected patients. Patients with PD worldwide experienced worsening of motor and nonmotor symptoms during the COVID-19 pandemic, including more stress, depression, and anxiety, and less physical activity.3–12 Under nonpandemic conditions, the duration and severity of PD are predictors of caregiver burden, and psychiatric symptoms, hallucinations, and falls greatly impact caregiver quality of life.13–16 In Italy, during COVID-19 lockdown, caregiver stress and exacerbation of burden correlated with patient independence17 and nonmotor PD symptoms.18 Thus, social restrictions and psychological stress caused by COVID-19 extend to caregivers.
Japan declared a national state of emergency in April and May 2020, and people were encouraged to stay at home and social distance. In a survey conducted under this state of emergency, clinical depression and anxiety correlated with motor aspects of daily living in patients with PD.19 In a study of 100 patients with PD and their caregivers, lifestyle changes due to the COVID-19 pandemic resulted in symptom worsening, increased stress, and decreased physical activity in one-third to one-half of patients.17 For caregivers, depression, stress, and worsening of patients’ mood contributed to worse mental health.20 To date, no large study has reported COVID-19–induced behavior changes in patients with PD or their caregivers and their effects on PD symptoms in Japan.
Our large-scale survey investigated the changes in behavior and PD symptoms of patients with PD, and the effect of these changes on caregiver burden, before and after the COVID-19 pandemic in Japan.
Methods
Study Design
This was an observational, cross-sectional, paper-based survey conducted from February 2 to 26, 2021 in Japan. Paper surveys were mailed to patients with PD and their caregivers. Patients and caregivers had to provide written informed consent to participate and permit the publication and secondary use of survey results. People objectively considered incapable of giving informed consent could participate with the consent of their legal representative. Participation was voluntary, and respondents received a gift card from the survey company after survey completion. The protocol was approved by the Institutional Review Board (IRB #: 202009) in Japan. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and in compliance with the Ethical Guidelines for Medical Research Involving Human Subjects. The study was registered at the University Hospital Medical Information Network-Clinical Trials Registry (https://www.umin.ac.jp/ctr/index.htm; identification: UMIN000043167; date of registration: January 29, 2021).
Study Population
Respondents included consenting patients with PD (self-reported by patients or caregivers) and their caregivers, either of whom were members of the Japan Parkinson’s Disease Association (JPDA). Respondents were excluded if they did not provide an answer to over half of the survey questions, gave the same answer to all questions, answered after the survey period, or did not participate in the follow-up process if they had provided safety information (adverse events).
Objectives
The primary objective was to evaluate how the COVID-19 pandemic affected behaviors and PD symptoms (motor and nonmotor) in patients with PD, and caregiver burden. The secondary objectives were to determine whether perceived effects of the COVID-19 pandemic on motor and nonmotor symptoms differed between patients and caregivers, and to explore the needs and challenges of online medical care and medication instruction.
Survey Variables and Measurement Scales
The survey consisted of 29 questions for patients and 20 questions for caregivers, from which respondents could select ≥1 answer. Three confirmation questions on informed consent, who completed the survey, and patient/caregiver relationship were also included. The questionnaires were developed and delivered in Japanese (see Supplementary Methods for questionnaires in English).
In summary, the questionnaires asked about life before and after the COVID-19 pandemic. The patient questionnaire included questions about patient demographics, PD treatment and lifestyle, self-assessed PD symptoms, and PD-related information (disease duration, severity, and treatment). The caregiver questionnaire included questions about patient and caregiver demographics, caregiver lifestyle and burden, PD treatment, and patient lifestyle and PD symptoms. The use of telemedicine by telephone was defined as phone calls without video; online telemedicine included the use of video. Self-assessed symptom severity was selected from “0: No symptom” to “5: Most severe symptom”. Caregiver burden was selected from “0: No burden” to “5: Greatest burden”. Health status (fatigue, insomnia, irritability, loss of appetite, weight loss) was selected from “0: No problem” to “5: Severe problem”. See Supplementary Methods for further details and for patient and caregiver questionnaires.
Timeline
Responses for each survey question were required for February (Feb) 2020 (pre–COVID-19), August (Aug) 2020 (post–national state of emergency; referred to as post–state of emergency from here onward), and Feb 2021 (time of survey and continued pandemic conditions).
Statistical Analysis
Responses were collected, converted to electronic data, tabulated, and analyzed. The mean, standard deviation (SD), median, quartile 1 and 3 (Q1, Q3), minimum, and maximum were determined for continuous variables, and the number and percentage of responses in each category were described for categorical variables. Changes in Hoehn and Yahr (HY) scale (self-assessed) (Feb 2020–Feb 2021) were modeled using ordinal logistic regression. Change in self-assessed PD symptoms (Feb 2020–Aug 2020 and Feb 2020–Feb 2021) was categorized as “worsened”, “not changed”, and “improved”. Subgroup analyses were conducted to investigate the effects of the COVID-19 pandemic on PD symptoms. The perceived effects of the COVID-19 pandemic on symptoms between patients and caregivers and the needs/challenges of online medical care and medication instruction were explored using descriptive statistics. If no valid selection was made for any survey question, the response was handled as missing. For ordinal logistic regression, multiple imputation was performed for missing data. All analyses were conducted using R, Version 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria). See Supplementary Methods for further details.
Results
Demographic and Clinical Characteristics
Of the 7610 surveys distributed, 1950 patients with PD and 1493 caregivers responded. Responses from 1883 patients and 1382 caregivers were included in the analysis (Figure S1).
Most eligible respondents lived in Tokyo (patients: 170/1860, 9.1%; caregivers: 126/1377, 9.2%), Osaka (patients: 147/1860, 7.9%; caregivers: 105/1377, 7.6%), and Hyogo (patients: 121/1860, 6.5%; caregivers: 95/1377, 6.9%) prefectures (Figure S2). The mean (SD) age of patients and caregivers was 71.6 (8.2) years and 68.5 (11.4) years, respectively, and just over half were female. Most patients (64.0%) were unemployed and lived with their spouse (75.1%), and in most cases (82.3%) the spouse was the caregiver. Approximately half of patients had a PD diagnosis for ≥10 years, and 41.6% had a self-assessed HY scale of 3. Most patients traveled <1 hour to receive treatment and traveled by private car (64.0%; Tables 1 and S1).
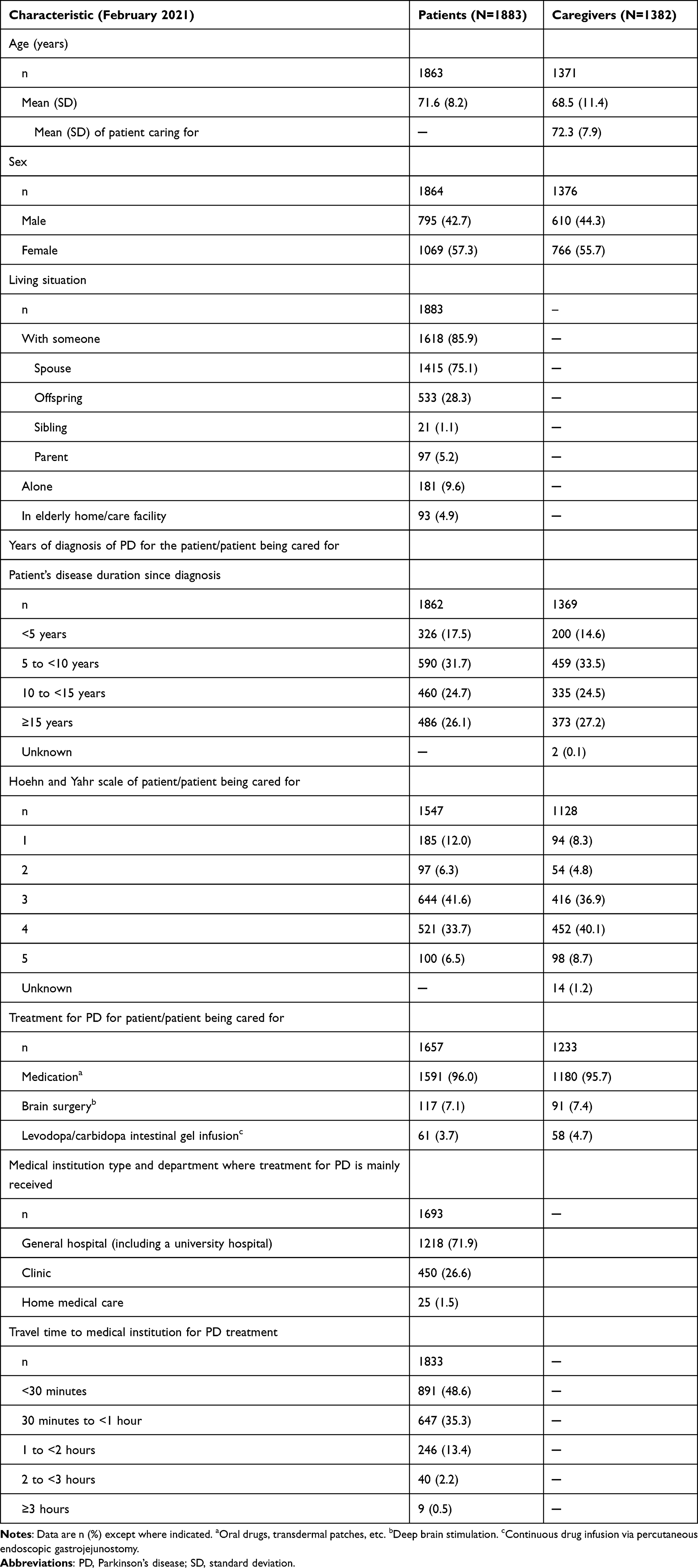 |
Table 1 Clinical Background and Demographics of Eligible Respondents at the Time of the Survey |
Behavior Changes in Patients
Frequency of Treatment Visits to a Medical Institution
The proportion of patients with a high visit frequency (1–2 visits/month) decreased from 38.3% pre–COVID-19 to 33.2% post–state of emergency (Figure 1A). The proportion of patients with a low visit frequency (<1 visit/3 months) increased from 5.6% pre–COVID-19 to 10.2% post–state of emergency and 7.8% at Feb 2021. For most patients (>70.0%), visit frequency did not change.
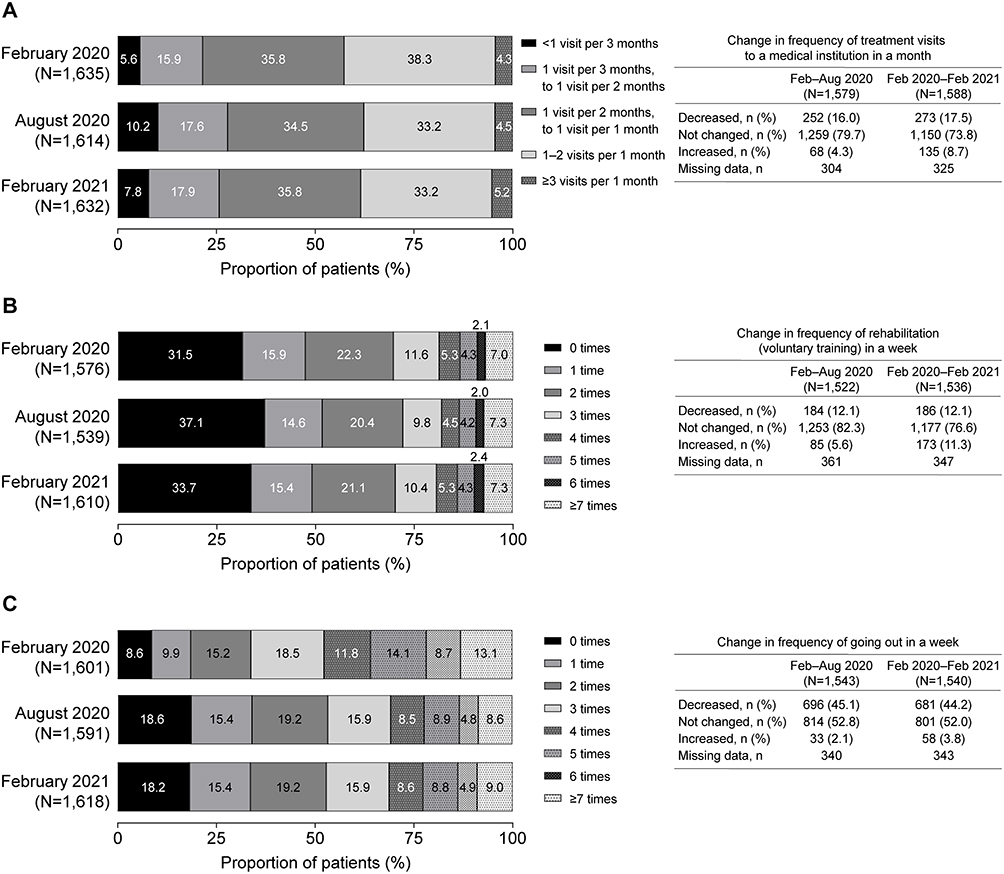 |
Figure 1 Behavior changes in patients. Change in (A) Frequency of treatment visits to a medical institution in a month, (B) Rehabilitation (voluntary training) in a week, and (C) Going out in a week among patients from pre–COVID-19 pandemic (February 2020) to post–national state of emergency (August 2020) or to the time of the survey (February 2021). Abbreviations: Aug, August; COVID-19, coronavirus disease 2019; Feb, February. |
Frequency of Rehabilitation (Voluntary Training)
Approximately one-third of patients did not undertake voluntary training pre–COVID-19 and post–state of emergency (Figure 1B). Overall, 22.3% conducted this activity 2 times/week pre–COVID-19 and 20.4–21.1% post–state of emergency, and the frequency decreased for 12.1% of patients up to Feb 2021.
Frequency of Going Out
Pre–COVID-19, most patients (66.2%) went out ≥3 times/week (Figure 1C). The frequency of going out decreased for 45.1% and 44.2% of patients post–state of emergency and up to Feb 2021, respectively.
Frequency of Rehabilitation Services and Nursing Care Insurance Services
Of patients who used rehabilitation services (excluding voluntary training), most used it 1–2 times/week (48.5%, Feb 2020; 44.4%, Aug 2020; 47.4%, Feb 2021; Figure S3). Use decreased for approximately 10% of patients post–state of emergency and up to Feb 2021. Most patients did not use nursing care insurance, bathing day care, or short-stay services, and there was minimal change in the frequency of their use.
Telemedicine Use
Most patients did not use telemedicine pre–COVID-19, post–state of emergency, and up to Feb 2021 (86.3–98.3%; Figure S4). The most common reason for not using telemedicine by Feb 2021 was “I can receive more satisfactory treatment face-to-face” (65.0%). Overall, 15.2% of patients used online telemedicine, 1.9% used the telephone, and 0.6% used both. Telemedicine use increased post–state of emergency from pre–COVID-19 (telephone: 2.0% vs 0.7%, respectively; online: 11.8% vs 1.0%, respectively).
Changes in PD Symptoms
HY Scale (Patient- and Caregiver-Assessed)
Overall, patients reported a general deterioration in HY scale, and HY scale tended to worsen for patients with milder disease versus a higher HY scale rating (Figure 2 and Table S2). There was a similar trend in the perception of severity of PD symptoms between patients and caregivers (Tables S2 and S3).
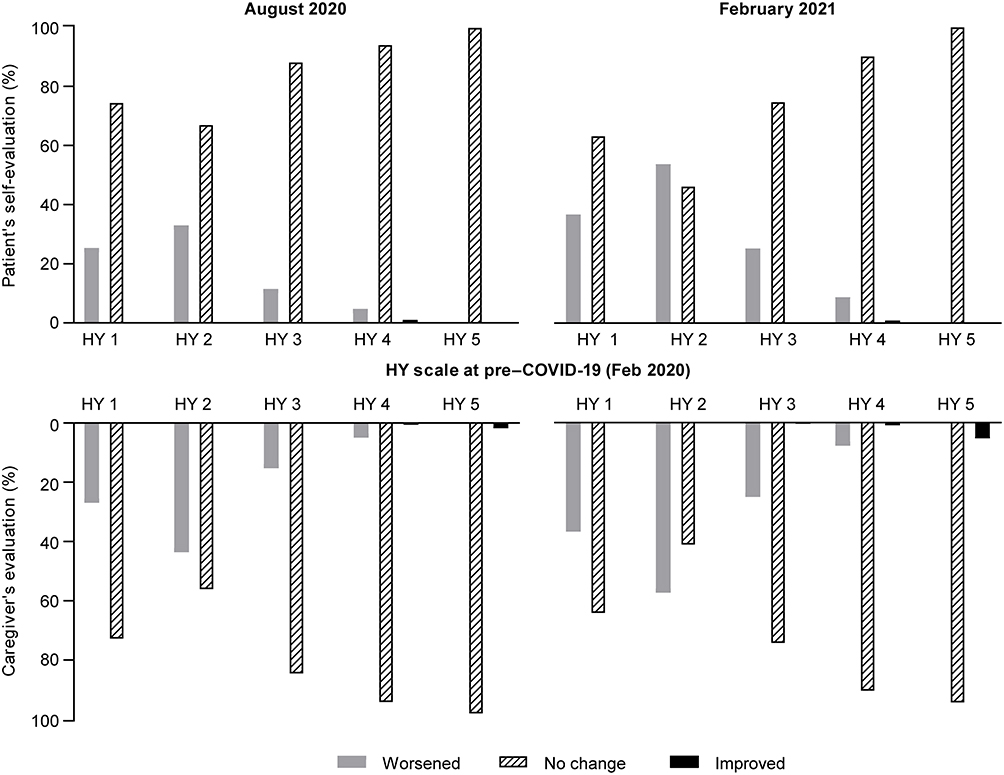 |
Figure 2 Differences between patients’ and caregivers’ perceptions of self-assessed symptom changes in Hoehn and Yahr scale. Differences from pre–COVID-19 pandemic (February 2020) to post–national state of emergency (August 2020) or to the time of the survey (February 2021). Patient perception: February 2020 to August 2020 (N=1435, missing data = 448); February 2020 to February 2021 (N=1437, missing data = 446). Caregiver perception: February 2020 to August 2020 (N=1051, missing data = 832); February 2020 to February 2021 (N=1051, missing data = 832). Abbreviations: COVID-19, coronavirus disease 2019; Feb, February; HY, Hoehn and Yahr. |
The proportion of patients with an HY scale of ≤3 was 74.8% (n=1148/1535) pre–COVID-19, 69.2% (n=1013/1464) post–state of emergency, and 59.9% (n=926/1547) up to Feb 2021. The proportion of patients with an HY scale of ≥4 was 25.2% (n=387/1535) pre–COVID-19, 30.8% (n=451/1464) post–state of emergency, and 40.1% (n=621/1547) up to Feb 2021, indicating a change to more severe PD symptoms.
Ordinal logistic regression analysis showed that frequency of going out (1-day decrease/week), age (10-year increase), HY scale at Feb 2020, PD duration since diagnosis, and living situation were significantly associated with the deterioration in HY scale from pre–COVID-19 to Feb 2021, and changes in the frequency of rehabilitation services (1-time decrease/week) were significantly associated with improvement in HY scale (Table 2).
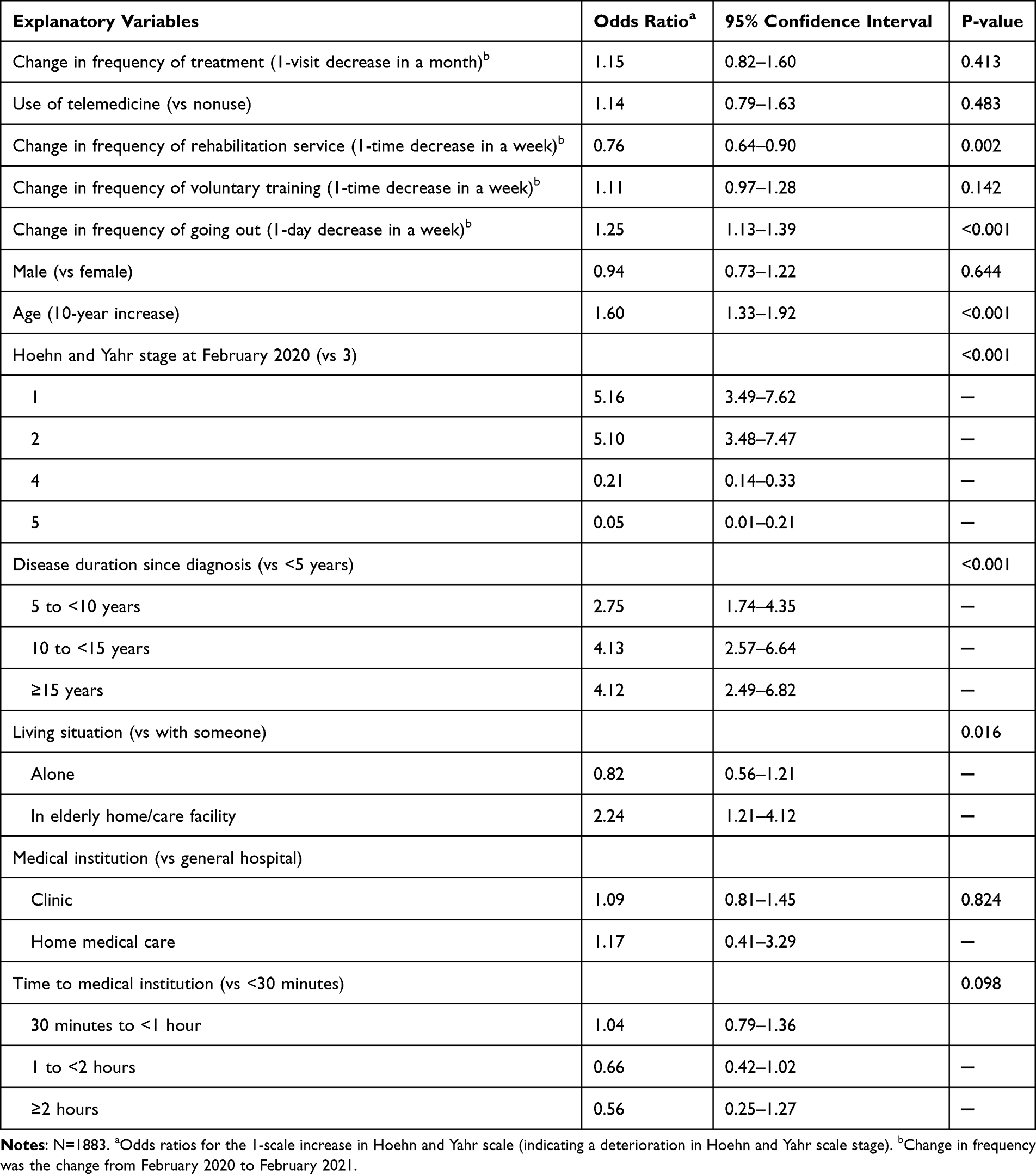 |
Table 2 Ordinal Logistic Regression Analysis of Change in Hoehn and Yahr Scale |
Motor and Nonmotor Symptoms
The proportion of patients with more severe self-assessed symptoms increased over time, with motor and nonmotor symptoms worsening in approximately 7–30% of patients pre–COVID-19 to post–state of emergency and up to Feb 2021 (Figure 3). Similar trends were observed for patient- and caregiver-reported changes in severity for motor and nonmotor symptoms (Figures 3 and S5).
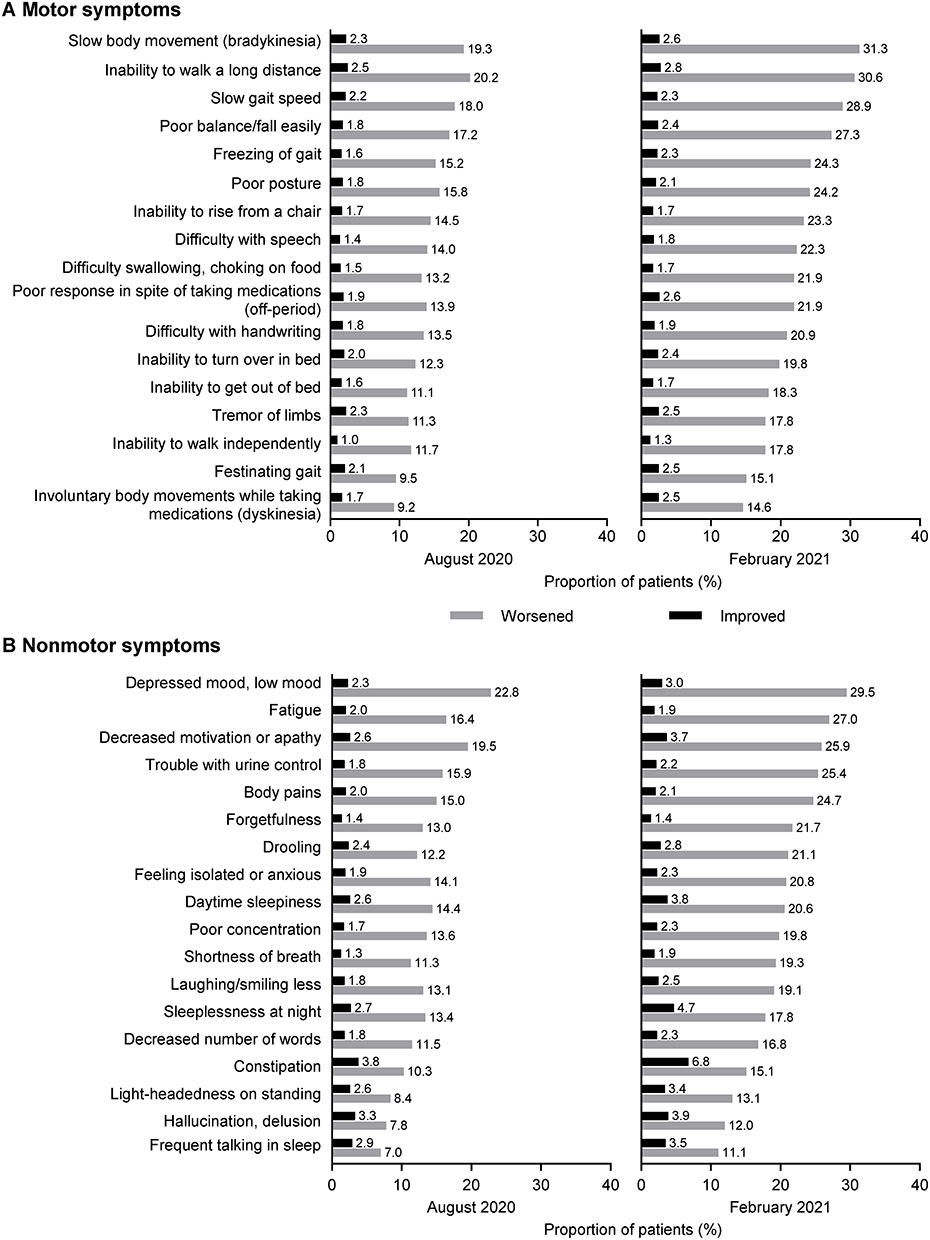 |
Figure 3 Changes in self-assessed motor and nonmotor symptoms. Change in severity of (A) Motor and (B) Nonmotor symptoms in patients from pre–COVID-19 pandemic (February 2020) to post–national state of emergency (August 2020) or to the time of the survey (February 2021). Abbreviation: COVID-19, coronavirus disease 2019. |
In a subgroup analysis, changes in PD symptoms tended to differ with HY scale, disease duration, and living situation; no clear trend was observed with sex and age (Figure S6). Compared with their respective subgroups, worsening of motor symptoms was greater in patients with an HY scale of 1–3 and disease duration <15 years. Worsening of nonmotor symptoms was greater in patients living alone or in an elderly home or care facility.
Changes in Caregiver Burden
An increase in daily caregiver hours pre–COVID-19 to Aug 2020 and up to Feb 2021 was reported by 16.8% and 22.9% of caregivers, respectively (Figure 4). Median (Q1–Q3) hours for patient care increased from 1.00 (0.0–4.0) pre–COVID-19 to 2.0 (0.0–5.0) in Feb 2021. The burden increased for 31.2% of caregivers up to Feb 2021 (Table S4). Of the 432 of 1382 caregivers who reported increased burden, 385 provided reasons, which were mainly aggravation of the patient’s symptoms (44.2%) and patients went out less frequently, requiring caregivers to spend more hours at home (43.9%). Approximately 40% of caregivers and their patients went out less frequently post–state of emergency and up to Feb 2021 (Figure S7). The most commonly reported changes in PD symptoms that contributed to increased caregiver burden were poor balance/fall easily (40.6%) and slow body movement (39.0%; Figure S7). Caregivers’ health status tended to not change over time, but caregivers were particularly troubled by fatigue and frustration (Table 3).
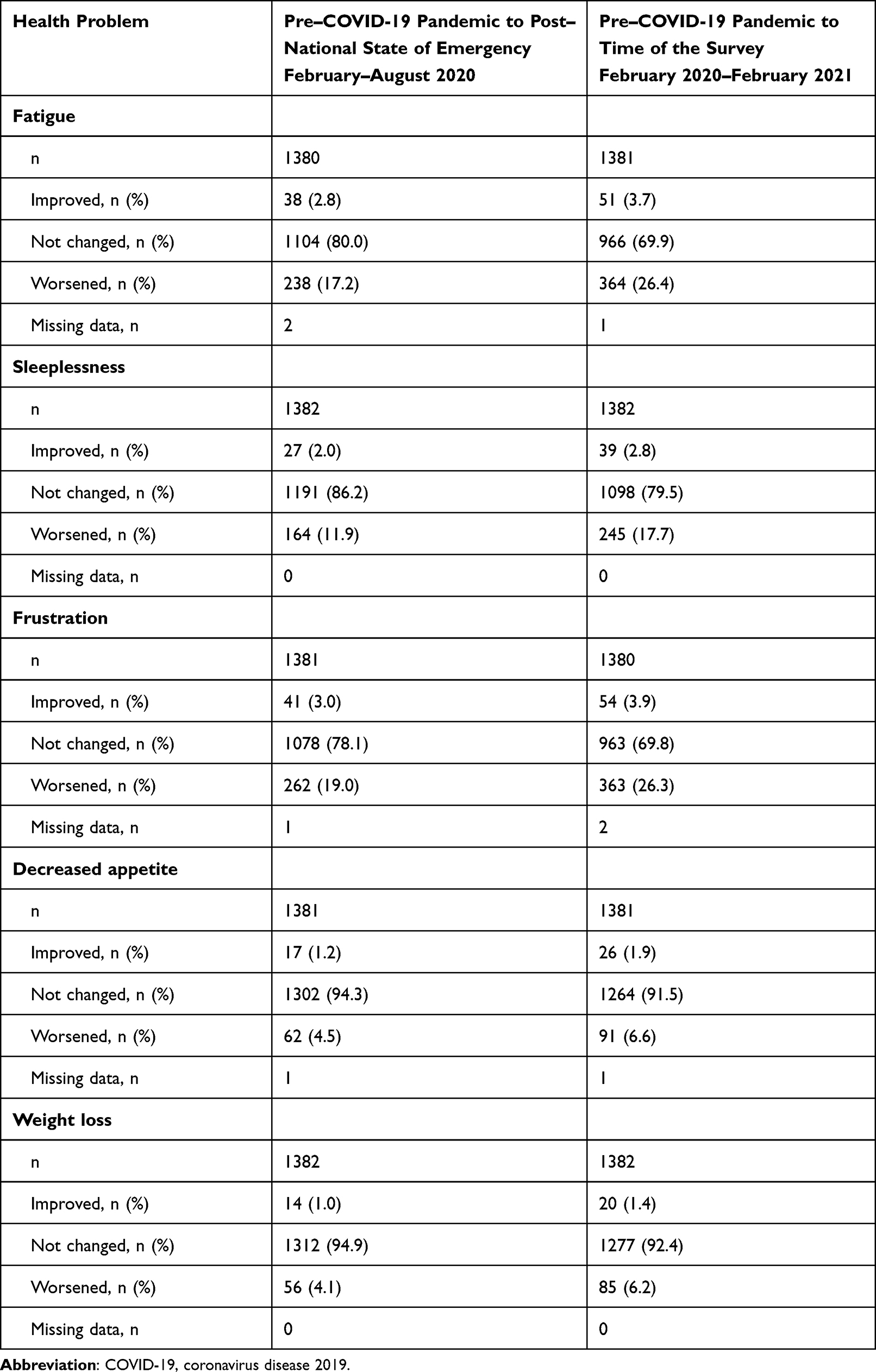 |
Table 3 Changes in Caregivers’ Health Status |
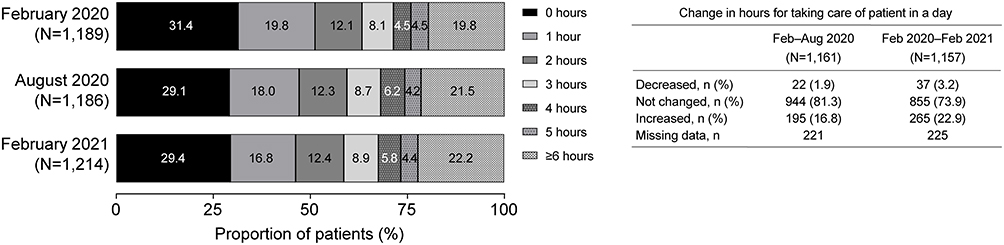 |
Figure 4 Changes in caregiver burden. Changes in daily caregiver hours from pre–COVID-19 pandemic (February 2020) to post–national state of emergency (August 2020) or to the time of the survey (February 2021). Abbreviations: Aug, August; COVID-19, coronavirus disease 2019; Feb, February. |
Discussion
This novel, large-scale observational survey investigated patient behavior and PD symptoms, and caregiver burden and health status, before and after the COVID-19 pandemic in Japan. Most patients (>70.0%) reported no change in their behavior during the pandemic, except for going out, for which >40.0% reported a decrease in frequency, indicating that unnecessary and nonurgent going out decreased during the pandemic. In contrast, the decrease in frequency of necessary activities, such as treatment visits to a medical institution, was small (≤17.5%). Symptoms worsened for approximately 7–30% of patients, and HY scale tended to worsen in patients with milder disease. A similar trend in perceived changes in patient behavior and symptoms was observed between patients and caregivers. Burden of care increased in approximately one-third of caregivers, largely due to patients going out less and worsened PD symptoms. These results suggest that social restrictions during the COVID-19 pandemic contributed to worsening PD symptoms and caregiver burden.
Social isolation is associated with disease severity and poor quality of life in patients with PD.21 In this study, the frequency of medical treatment and services, such as rehabilitation and nursing care, did not change much. However, nearly half of respondents went out less, suggesting that unnecessary and nonurgent going out decreased. A shift from a low (HY 1–2) to a higher HY scale was observed in patients with PD, indicating a change from mild to more severe disease during the pandemic. However, patients may readily transition from lower (mild disease) to higher HY values.22 Regression analysis showed a significant association between decreased frequency of going out and HY scale deterioration; however, it is unclear if this was the cause or a consequence of the observed HY scale change. Increasing age, long disease duration since diagnosis, and living situation were also significantly associated with HY scale deterioration.
In Japan, online medical care had been provided before the COVID-19 pandemic; however, in response to the pandemic, in April 2020 the Ministry of Health, Labour and Welfare in Japan relaxed restrictions on telemedicine consultations and allowed insurance payment for telemedicine services.23 Interestingly, in this study, the frequency of medical treatment visits did not change much during the pandemic and, although telemedicine consultations were permitted, there appeared to be hesitancy with their uptake. Considering that most patients with PD visit a hospital relatively infrequently for treatment (ie, 1–2 times/month or every 2 months), it is reasonable that the frequency of treatment visits did not change during the pandemic. In addition, in this study, patients indicated a preference for face-to-face visits, with only a small proportion (11.8%) using online telemedicine services during the pandemic. Similarly, only 9.0% of patients with PD in the Tochigi prefecture in Japan implemented online care during the pandemic.20 This is in contrast to the high acceptance of telemedicine observed in surveys of people with PD across the United States (US), where telehealth use increased from 9.7% before to 63.5% during the pandemic,24 and in Fukuoka, Japan, during the state of emergency, where 60.2% of patients indicated that they would be inclined to use telemedicine.25 Furthermore, in a global survey on telemedicine use during March and April 2020, all forms of telemedicine for movement disorders increased globally,26 and in a Japanese study of patients with neurological disease during the pandemic, patients with PD tended to prefer telemedicine more than those without PD.27 Differences in the uptake of telemedicine may be attributed to the lack of facilities to conduct online medical care, cultural differences, insufficient reimbursement of costs by insurance,26 difficulty in obtaining reimbursement of costs, and regional differences in the number of people infected with SARS-CoV-2. Overall, the results of our study suggest that patients with PD in Japan are typically engaged with their routine treatment visits to a medical institution and have low affinity for online medical care.
In a single-center survey investigating the impact of the COVID-19 pandemic on PD in Japan, worsening of tremor, rigidity, gait, postural stability, cognition, mood, and sleep was reported by approximately 30–40% of patients and caregivers; <25% of patients reported a worsening of bradykinesia.20 Furthermore, many patients reported increased stress and decreased physical activity during the pandemic.20 In our study, approximately 7–30% of patients reported worsening of PD symptoms from before the COVID-19 pandemic to the time of this study. The most aggravated symptoms included bradykinesia, ability to walk long distances, slow gait speed, depressed mood, fatigue, and decreased motivation or apathy. Deterioration in PD symptoms during the COVID-19 pandemic has been observed in other countries. In the US, in an online study of >5000 patients with PD, 43% and 52% of patients not diagnosed with COVID-19 reported worsening of their motor and nonmotor symptoms, respectively.6 In India, a study of 100 patients with PD indicated that 11% of patients experienced aggravation of their PD symptoms, and 4% had problems with medical visits and drug supply during the pandemic.3 In Italy, in a study of spontaneous communications from patients with PD to a medical clinic, and a questionnaire survey study in patients with PD receiving deep brain stimulation, worsening of subjective motor and/or psychiatric symptoms during the COVID-19 lockdown were reported.4,28 In Iran, a cross-sectional survey indicated that 25.5% of patients with PD experienced severe anxiety after the COVID-19 outbreak,29 and in Egypt, a telephone survey showed that during the pandemic, patients with PD had more stress, depression, and anxiety, less physical activity, and lower quality of life than matched controls without PD.5 Furthermore, social restrictions and psychological stress caused by the pandemic exacerbate nonmotor symptoms, including anxiety/depression,7–9,12,19,20 cognitive function,10 and pain.11
In PD, caregiver burden is dependent on patient factors,30 in particular nonmotor symptoms such as sleep problems and autonomic dysfunction.15,16,31 A US study reported increased caregiver strain and stress since the COVID-19 pandemic began. The societal effects of the pandemic, loss of caretaking services, and increased time taking care of the patient all contributed to increased caregiver burden.32 Patient and caregiver quality of life is closely linked, with caregivers reporting deterioration in their health as a result of caregiving and increased burden with increased patient disability, in particular depression, hallucination or confusion, and falls.13 A single-center survey in Japan also reported the negative impact of COVID-19 on caregivers’ quality of life, with depression, stress, and worsening of patients’ mood being key factors.20 In our study, caregiver burden increased with the COVID-19 pandemic. Time spent on patient care increased for approximately 20% of caregivers, and up to 31.2% of caregivers stated that their burden of care had increased. Increased caregiver time at home due to patients going out less and increased burden due to worsening of patient PD symptoms were the main factors that contributed to increased caregiver burden.
This nationwide study was strengthened by the large sample size for patients (>1800) and caregivers (>1300). Furthermore, this study investigated the change in individual symptoms rather than using a specific scale that may not identify all changes across the spectrum of PD symptoms. However, our results should be interpreted with the following limitations. First, patient symptoms and HY scale were self-assessed and may not align with physicians’ assessments and, because data were collected retrospectively, there may be recall bias. However, patient and caregiver perceptions of changes in symptoms were aligned, suggesting that the effect of recall bias was not large. Furthermore, because patient and caregiver answers were well matched, a formal matching analysis using groups of matched patients and caregivers was not conducted. Second, the questionnaires were not validated; however, they were created by an author (Y.O.) who is a patient with PD and designed for respondents to easily answer and comprehensively clarify patients’ subjective symptoms and conditions. Third, owing to the nature of cross-sectional surveys, any causal relationships are hypothetical and need to be interpreted with caution; specifically, changes in PD symptom severity due to disease progression33 cannot be dissociated from changes caused by the pandemic. Fourth, multiple factors may have contributed to selection bias. Although participation in the survey was voluntary, data were more likely to be collected from more cooperative respondents, and because patients with severe disease tend to be unable to participate in questionnaires, data were more likely to be collected from patients with mild disease. Finally, the study is not representative of all patients with PD in Japan, because not all patients with PD in Japan are JPDA members and because the survey recovery rate was relatively low (25.6% for patients; 19.6% for caregivers) compared with other surveys targeting the same populations (32.9–48.0% for patients34–36; 27.6% for caregivers36).
Conclusion
The COVID-19 pandemic changed patients’ behaviors, in particular the frequency of going out, worsening of motor and nonmotor symptoms, and deterioration in self-assessed HY scale. Increased time spent at home by caregivers and patients and worsened PD symptoms were likely to have increased caregiver burden. For future emergency control measures, such as those imposed for infectious disease epidemics, it is important that treatment, procedures, and policy consider the possibility that patients’ symptoms may worsen. Therefore, support for both patients and caregivers to reduce the burden of long-term care should be considered.
Abbreviations
COVID-19, coronavirus disease 2019; HY, Hoehn and Yahr; JPDA, Japan Parkinson’s Disease Association; PD, Parkinson’s disease; Q, quartile; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SD, standard deviation; US, United States.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Patients and caregivers were required to provide written informed consent to participate in the survey and to permit the publication of survey results and the secondary use of study results. The protocol was approved by the Medical Corporation, Takahashi Clinic, clinical trial examination committee, Institutional Review Board (IRB #: 202009) in Japan. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki and in compliance with the Ethical Guidelines for Medical Research Involving Human Subjects.
Acknowledgments
The authors would like to thank all study participants. Medical writing assistance was provided by Prudence Stanford, PhD, CMPP, and Yuriko Kikuchi-Rech, PhD, of ProScribe – Envision Pharma Group, and was funded by Takeda Pharmaceutical Company Limited. ProScribe’s services complied with international guidelines for Good Publication Practice (GPP3).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, or analysis and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the report has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Takeda Pharmaceutical Company Limited. Support with the survey design and survey implementation was provided by the Japan Parkinson’s Disease Association and Qlife, and both were funded by Takeda Pharmaceutical Company Limited. The Japan Parkinson’s Disease Association also provided support with contacting patients. Takeda Pharmaceutical Company Limited was involved in the study design, data collection, and preparation of the manuscript.
Disclosure
NH reports consulting fees from AbbVie Inc., Eisai Co., Ltd., FP Pharmaceutical Corporation, GlaxoSmithKline K.K., Hisamitsu Pharmaceutical Co., Inc., Kyowa Kirin Co., Ltd., Meiji Seika Pharma Co., Ltd., Ono Pharmaceutical Co., Ltd, Otsuka Pharmaceutical Co., Ltd., and Sumitomo Dainippon Pharma Co. Ltd.; lecture fees from Daiichi Sankyo Company, Limited, Eisai Co., Ltd., Eli Lilly Japan K.K., FP Pharmaceutical Corporation, GlaxoSmithKline K.K., Kyowa Kirin Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Nihon Medi-Physics Co., Ltd., MSD K.K., Nippon Boehringer Ingelheim Co., Ltd., Novartis Pharma K.K., Otsuka Pharmaceutical Co., Ltd., Pfizer Japan Inc., Sumitomo Dainippon Pharma Co. Ltd., Takeda Pharmaceutical Company Limited, and Tsumura & Co.; honoraria from AbbVie Inc., FP Pharmaceutical Corporation, Kyowa Kirin Co., Ltd., and Novartis Pharma K.K.; research support from Otsuka Pharmaceutical Co., Ltd.; and grants from Astellas Pharma Inc., Boehringer Ingelheim Co., Ltd., Boston Scientific Corporation, Eisai Co., Ltd., GlaxoSmithKline K.K., Kyowa Kirin Co., Ltd., Medtronic Japan Co., Ltd., Nippon Kissei Pharmaceutical Co., Ltd, Novartis Pharma K.K., Otsuka Pharmaceutical Co., Ltd., Pfizer Japan Inc., Sumitomo Dainippon Pharma Co. Ltd., and Takeda Pharmaceutical Company Limited outside the submitted work. YO reports payment or honoraria from Kyowa Kirin Co., Ltd. YK, YF, MO, and MA are employees of Takeda Pharmaceutical Company Limited. TI reports payment or honoraria from JCR Pharmaceuticals Co., Ltd. and Kyowa Kirin Co., Ltd. HY reports honoraria from Kyowa Kirin Co., Ltd. AS reports consulting fees and payment or honoraria from Kyowa Kirin Co., Ltd. and Takeda Pharmaceutical Company Limited. JF is a former employee of Takeda Pharmaceutical Company Limited and GlaxoSmithKline, and owns restricted stocks of GlaxoSmithKline and Takeda Pharmaceutical Company Limited.
References
1. Ferini-Strambi L, Salsone M. COVID-19 and neurological disorders: are neurodegenerative or neuroimmunological diseases more vulnerable? J Neurol. 2021;268(2):409–419. doi:10.1007/s00415-020-10070-8
2. Bhidayasiri R, Virameteekul S, Kim JM, Pal PK, Chung SJ. COVID-19: an early review of its global impact and considerations for Parkinson’s disease patient care. J Mov Disord. 2020;13(2):105–114. doi:10.14802/jmd.20042
3. Prasad S, Holla VV, Neeraja K, et al. Parkinson’s disease and COVID-19: perceptions and implications in patients and caregivers. Mov Disord. 2020;35(6):912–914. doi:10.1002/mds.28088
4. Schirinzi T, Cerroni R, Di Lazzaro G, et al. Self-reported needs of patients with Parkinson’s disease during COVID-19 emergency in Italy. Neurol Sci. 2020;41(6):1373–1375. doi:10.1007/s10072-020-04442-1
5. Shalash A, Roushdy T, Essam M, et al. Mental health, physical activity, and quality of life in Parkinson’s disease during COVID-19 pandemic. Mov Disord. 2020;35(7):1097–1099. doi:10.1002/mds.28134
6. Brown EG, Chahine LM, Goldman SM, et al. The effect of the COVID-19 pandemic on people with Parkinson’s disease. J Parkinsons Dis. 2020;10(4):1365–1377. doi:10.3233/JPD-202249
7. Helmich RC, Bloem BR. The impact of the COVID-19 pandemic on Parkinson’s disease: hidden sorrows and emerging opportunities. J Parkinsons Dis. 2020;10(2):351–354. doi:10.3233/JPD-202038
8. Kumar N, Gupta R, Kumar H, et al. Impact of home confinement during COVID-19 pandemic on Parkinson’s disease. Parkinsonism Relat Disord. 2020;80:32–34. doi:10.1016/j.parkreldis.2020.09.003
9. Zipprich HM, Teschner U, Witte OW, Schönenberg A, Prell T. Knowledge, attitudes, practices, and burden during the COVID-19 pandemic in people with Parkinson’s disease in Germany. J Clin Med. 2020;9(6):1643. doi:10.3390/jcm9061643
10. Palermo G, Tommasini L, Baldacci F, Del Prete E, Siciliano G, Ceravolo R. Impact of coronavirus disease 2019 pandemic on cognition in Parkinson’s disease. Mov Disord. 2020;35(10):1717–1718.
11. van der Heide A, Meinders MJ, Bloem BR, Helmich RC. The impact of the COVID-19 pandemic on psychological distress, physical activity, and symptom severity in Parkinson’s disease. J Parkinsons Dis. 2020;10(4):1355–1364. doi:10.3233/JPD-202251
12. Hanff AM, Pauly C, Pauly L, et al. Unmet needs of people with Parkinson’s disease and their caregivers during COVID-19-related confinement: an explorative secondary data analysis. Front Neurol. 2021;11:615172. doi:10.3389/fneur.2020.615172
13. Schrag A, Hovris A, Morley D, Quinn N, Jahanshahi M. Caregiver-burden in Parkinson’s disease is closely associated with psychiatric symptoms, falls, and disability. Parkinsonism Relat Disord. 2006;12(1):35–41. doi:10.1016/j.parkreldis.2005.06.011
14. Martínez-Martín P, Forjaz MJ, Frades-Payo B, et al. Caregiver burden in Parkinson’s disease. Mov Disord. 2007;22(7):924–931; quiz 1060. doi:10.1002/mds.21355
15. von Eichel H, Heine J, Wegner F, et al. Neuropsychiatric symptoms in Parkinson’s disease patients are associated with reduced health-related quality of life and increased caregiver burden. Brain Sci. 2022;12(1):89. doi:10.3390/brainsci12010089
16. Klietz M, Schnur T, Drexel S, et al. Association of motor and cognitive symptoms with health-related quality of life and caregiver burden in a German cohort of advanced Parkinson’s disease patients. Parkinsons Dis. 2020;2020:5184084. doi:10.1155/2020/5184084
17. De Micco R, Siciliano M, Sant’Elia V, et al. Correlates of psychological distress in patients with Parkinson’s disease during the COVID-19 outbreak. Mov Disord Clin Pract. 2020;8(1):60–68. doi:10.1002/mdc3.13108
18. Oppo V, Serra G, Fenu G, et al. Parkinson’s disease symptoms have a distinct impact on caregivers’ and patients’ stress: a study assessing the consequences of the COVID-19 lockdown. Mov Disord Clin Pract. 2020;7(7):865–867. doi:10.1002/mdc3.13030
19. Kitani-Morii F, Kasai T, Horiguchi G, et al. Risk factors for neuropsychiatric symptoms in patients with Parkinson’s disease during COVID-19 pandemic in Japan. PLoS One. 2021;16(1):e0245864. doi:10.1371/journal.pone.0245864
20. Suzuki K, Numao A, Komagamine T, et al. Impact of the COVID-19 pandemic on the quality of life of patients with Parkinson’s disease and their caregivers: a single-center survey in Tochigi prefecture. J Parkinsons Dis. 2021;11(3):1047–1056. doi:10.3233/JPD-212560
21. Subramanian I, Farahnik J, Mischley LK. Synergy of pandemics-social isolation is associated with worsened Parkinson severity and quality of life. NPJ Parkinsons Dis. 2020;6(1):28. doi:10.1038/s41531-020-00128-9
22. Terwee CB, Bot SD, de Boer MR, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. 2007;60(1):34–42. doi:10.1016/j.jclinepi.2006.03.012
23. Ministry of Health, Labour and Welfare. Administrative notice: temporary and exceptional online medical examination under COVID-19 pandemic [In Japanese]. Available from: https://www.mhlw.go.jp/content/000620995.pdf.
24. Feeney MP, Xu Y, Surface M, et al. The impact of COVID-19 and social distancing on people with Parkinson’s disease: a survey study. NPJ Parkinsons Dis. 2021;7(1):10. doi:10.1038/s41531-020-00153-8
25. Kurihara K, Nagaki K, Inoue K, et al. Attitudes toward telemedicine of patients with Parkinson’s disease during the COVID-19 pandemic. Neurol Clin Neurosci. 2021;9(1):77–82. doi:10.1111/ncn3.12465
26. Hassan A, Mari Z, Gatto EM, et al. Global survey on telemedicine utilization for movement disorders during the COVID-19 pandemic. Mov Disord. 2020;35(10):1701–1711. doi:10.1002/mds.28284
27. Osada T, Deguchi I, Arai N, et al. Needs for online care of Parkinson’s patients in the Covid-19 epidemic [In Japanese].
28. Piano C, Bove F, Tufo T, et al. Effects of COVID-19 lockdown on movement disorders patients with deep brain stimulation: a multicenter survey. Front Neurol. 2020;11:616550. doi:10.3389/fneur.2020.616550
29. Salari M, Zali A, Ashrafi F, et al. Incidence of anxiety in Parkinson’s disease during the coronavirus disease (COVID-19) pandemic. Mov Disord. 2020;35(7):1095–1096. doi:10.1002/mds.28116
30. Lo Monaco MR, Di Stasio E, Ricciardi D, et al. What about the caregiver? A journey into Parkinson’s disease following the burden tracks. Aging Clin Exp Res. 2021;33(4):991–996. doi:10.1007/s40520-020-01600-5
31. Grün D, Pieri V, Vaillant M, Diederich NJ. Contributory factors to caregiver burden in Parkinson disease. J Am Med Dir Assoc. 2016;17(7):626–632. doi:10.1016/j.jamda.2016.03.004
32. Macchi ZA, Ayele R, Dini M, et al. Lessons from the COVID-19 pandemic for improving outpatient neuropalliative care: a qualitative study of patient and caregiver perspectives. Palliat Med. 2021;35(7):1258–1266. doi:10.1177/02692163211017383
33. Yoritaka A, Shimo Y, Hatano T, Hattori N. Motor/nonmotor symptoms and progression in patients with Parkinson’s disease: prevalence and risks in a longitudinal study. Parkinsons Dis. 2020;2020:2735361. doi:10.1155/2020/2735361
34. Fujimoto K, Murata M, Hattori N, Kondo T. Patients’ perspective on Parkinson disease therapies: results of a large-scale survey in Japan [In Japanese]. Brain Nerve. 2011;63(3):255–265.
35. Tsugawa J, Onozawa R, Fukae J, Mishima T, Fujioka S, Tsuboi Y. Impact of insufficient drug efficacy of antiparkinson agents on patient’s quality of life: a cross-sectional study. BMC Neurol. 2015;15:105. doi:10.1186/s12883-015-0360-y
36. Onozawa R, Tsugawa J, Tsuboi Y, Fukae J, Mishima T, Fujioka S. The impact of early morning off in Parkinson’s disease on patient quality of life and caregiver burden. J Neurol Sci. 2016;364:1–5. doi:10.1016/j.jns.2016.02.066
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.