")
Back to Journals » International Journal of Women's Health » Volume 13
Surgical Techniques for the Prolapse of Neovagina in Women: Case Report and Review of Literature
Authors Faehnle-Schiegg I , Christmann-Schmid C
Received 17 October 2020
Accepted for publication 25 November 2020
Published 13 January 2021 Volume 2021:13 Pages 81—86
DOI https://doi.org/10.2147/IJWH.S285474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Ivo Faehnle-Schiegg, Corina Christmann-Schmid
Luzerner Kantonsspital, Frauenklinik, CH 6000 Luzern, Switzerland
Correspondence: Ivo Faehnle-Schiegg Email [email protected]
Introduction: A neovaginal prolapse is a rare condition. Only a few cases have been reported and described in literature. The surgical management is complex and depends on the initial surgical techniques for the reconstruction of a neovagina applied. We present a case of a stage IV prolapse of a sigmoid vaginal prolapse and a review of surgical procedures in literature.
Methods: We describe the case of a 41-year-old woman with a stage IV prolapse of a sigmoid neovagina who presented 20 years after the initial reconstruction due to a botryoid sarcoma of the pelvis in the childhood. The initial surgical repairs with a fixation of the apex of the sigmoid vagina to the sacral promontory with resorbable suture and consecutively in a second procedure with a polypropylene mesh failed. The interdisciplinary approach with the colorectal team which included a significant shortening of the neovagina prior to the mesh fixation led to a stable repair of the prolapse.
Conclusion: Only a few cases of women with a prolapse of a sigmoid neovagina are published. An interdisciplinary approach including a significant shortening of the neovagina and the fixation with a non-absorbable mesh was necessary to achieve a successful repair. The surgical techniques to create a sigmoid neovagina are crucial in order to perform successful later reconstructive surgery if indicated. Our experience in this case is consistent with the findings from our literature review.
Keywords: laparoscopy, sacrocolpopexy, pelvic organ prolapse, neovagina
Introduction
The use of a part of the sigmoid colon in order to form a neovagina is a valid option to create a neovagina in women with a congenital vaginal aplasia or after prior colpectomy with good anatomical and functional outcomes.1–5 Due to the low number of affected women treated with a sigmoid vagina the incidence of consecutively reported neovaginal prolapse is low.6–14 Djordjevic et al2 reported in their series a prolapse rate of 8.1%. In total some data indicate that the incidence of a neovaginal prolapse is approximately 2.3%.10
The pathophysiology of a neovaginal prolapse is still unclear. Most likely the missing integration into the pelvic floor in comparison to a natural vagina with its anterior and apical support to the pelvic side walls seems to be a reasonable explanation.10
Furthermore, sexual intercourse is a hypothetical reason for lengthening of the neovagina.9,10
To date there are no standardized techniques established to re-suspend the prolapse. Various surgical approaches ranging from vaginal mesh repair, to open or laparoscopic fixation of the neovagina with or without mesh inlay have been described.
In conclusion of the missing data and rarely reported cases in literature we present this case and a systematic review of literature.
Methods
The MEDLINE and Cochrane library databases were searched for the terms “neovagina prolapse”, “neovagina pelvic organ prolapse”, “neovagina prolapse repair”. We did not apply any restriction regarding the year of publication or language, only results in English were retrieved though. We excluded publications concerning male to female transsexual patients and publications without full text availability. From the remaining results we manually excluded those not describing specific surgical techniques in order to achieve a repair of a neovagina.
Case
A 41-year-old woman was admitted to our unit in February 2016 due to a symptomatic prolapse of a sigmoid neovagina. She suffered from a vaginal bulge, ulcerations and bleeding from the protruding area. Furthermore, she reported malodorous vaginal discharge over the last few months.
At the age of two she had a hysterectomy and radical colpectomy in order to resect a botryoid sarcoma of the pelvis. In 1995, at the age of 20, a sigmoid neovagina was formed to reconstruct a vagina. Sexual intercourse was possible with no pain and normal sensation.
The initial examination showed a vaginal prolapse with a POP-Q stage III (POP-Q values of Aa +1, Ba +2, C −6, Ap +1, Bp +2). Interestingly an outstanding long neovagina was found with a total vaginal length of at least 18cm. The ulcerations with some metaplasy were found in the exposed areas of the neovagina, the cytology showed inflammation but no suspicious cells. No other bladder dysfunction or anal incontinence was reported or objectified.
In order to correct the prolapse, an initial diagnostic laparoscopy was performed. There were significant intra-abdominal adhesions to the pelvic side walls which had to be dissected and a fully adherent cystadenoma of the left ovary had to be removed. Because of the prolonged length of the neovagina intraoperatively (18cm) the apex could be fixated directly with PDS-sutures to the anterior ligament of the sacral promontory. At this first step no mesh could be used as no peritoneum was present for the retroperitoneal closer of the mesh (Figure 1). Two months postoperatively the subjective and objective result was excellent with no prolapse to be detected.
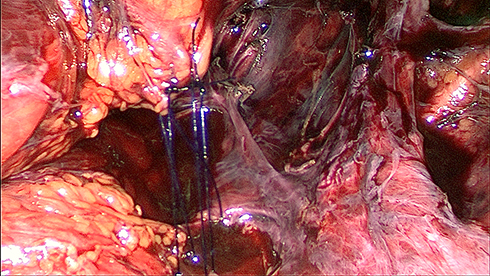 |
Figure 1 Intraoperative site during first surgery. The neovagina is attached to the promontory with PDS 2/0 sutures. After extensive dissection of adhesions there is no peritoneal coating present. |
Three months later, a recurrence of the prolapse occurred with POP-Q values of Aa +1, Ba +2, C −6, Ap 0, Ap +1. Similar symptoms including ulcerations of the protruding part occurred. The intraoperative situs initially showed, that the whole neovagina was detached from the promontory and layed at the level of the pelvic floor (Figure 2). Hence, in December 2016 a laparoscopy with sacrocolpopexy using a Ultrapro® mesh (macroporous polypropylene) was performed. The full length of the sigmoid neovagina was used for the suspension. Anteriorly the vesicovaginal and rectovaginal space could not be dissected and separated as they were obliterated from the initial surgery in the early childhood. Therefore, one strip mesh was placed over the apex (Figure 3A and B). OR-time for this procedure was 148 minutes, the blood loss was minimal.
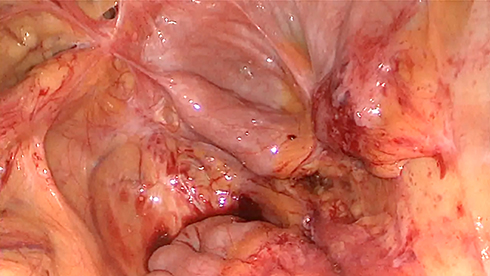 |
Figure 2 Initial intraoperative site during second surgery. The neovagina is hardly visible as it lays at the level of the pelvic floor and the former attachment to the promontory is detached completely. |
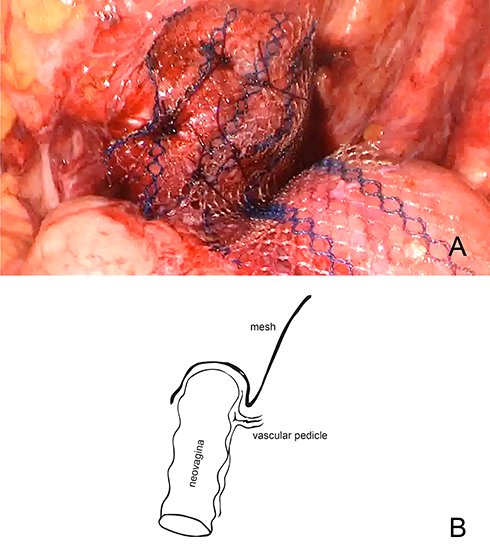 |
Figure 3 (A) During the second surgery a single mesh strip was placed over the apex of the neovagina. It was not possible to dissect the anterior compartment down to level of the bladder neck and at the posterior wall the vascular pedicle had to be spared. (B) The sketch illustrates schematically the course of the mesh and the relation of the vascular pedicle. |
However, only two months after this surgery another recurrence of the prolapse with POP-Q values of Aa 0, Ba +2, C −10, Ap −1, Bp 0 was present. The protrusion of the anterior vaginal wall led to the same problems as before. A further support with mesh was not possible in the present situation. The mesh could not be laid any further down neither anteriorly nor posteriorly as it was placed as caudal anterior as possible and because the vascular pedicle of the neovagina on the dorsal side had to be preserved (Figure 4).
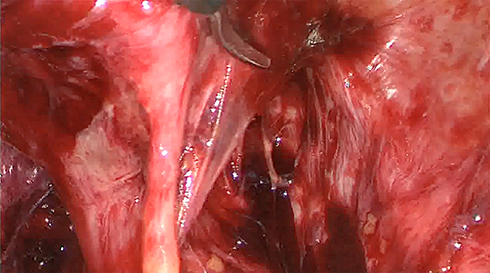 |
Figure 4 Vascular pedicle. Anteriorly the neovagina is visible. The strand deriving from the posterior wall corresponds to the vascular pedicle. |
Thus, in an interdisciplinary collaboration with our colleagues from the department of colorectal surgery we performed a median laparotomy.
At this step we saw that the actual neovaginal length was as long as 33 centimeters with a significant kinking at the level of 18 centimeters. The neovagina was dissected including the dorsal vascular pedicle. The apical part of the neovagina was resected using a Medtronic EndoGIA® 60 stapler, the previously implanted mesh was removed and the shortened neovagina was fixated with an Ultrapro® mesh (macroporous polypropylene) to the sacral promontory. This surgical procedure took 276 minutes with an estimated blood loss of 500mL.
Finally a sufficient and entire correction of the prolapse could be achieved. To date, no recurrence occurred and the patient did not report any significant symptoms. POP-Q was Aa −3, Ba −3, C −11, Ap −3, Bp −3.
Results
We identified 31 publications. Three papers concerning male-to-female transsexual patients were excluded. Further, we excluded two abstracts without full text availability. From the resulting 26 results, we manually excluded all contributions not describing surgical techniques. Finally, 18 full text publications could be included in our literature review (Figure 5). An overview of the results is listed in Table 1.
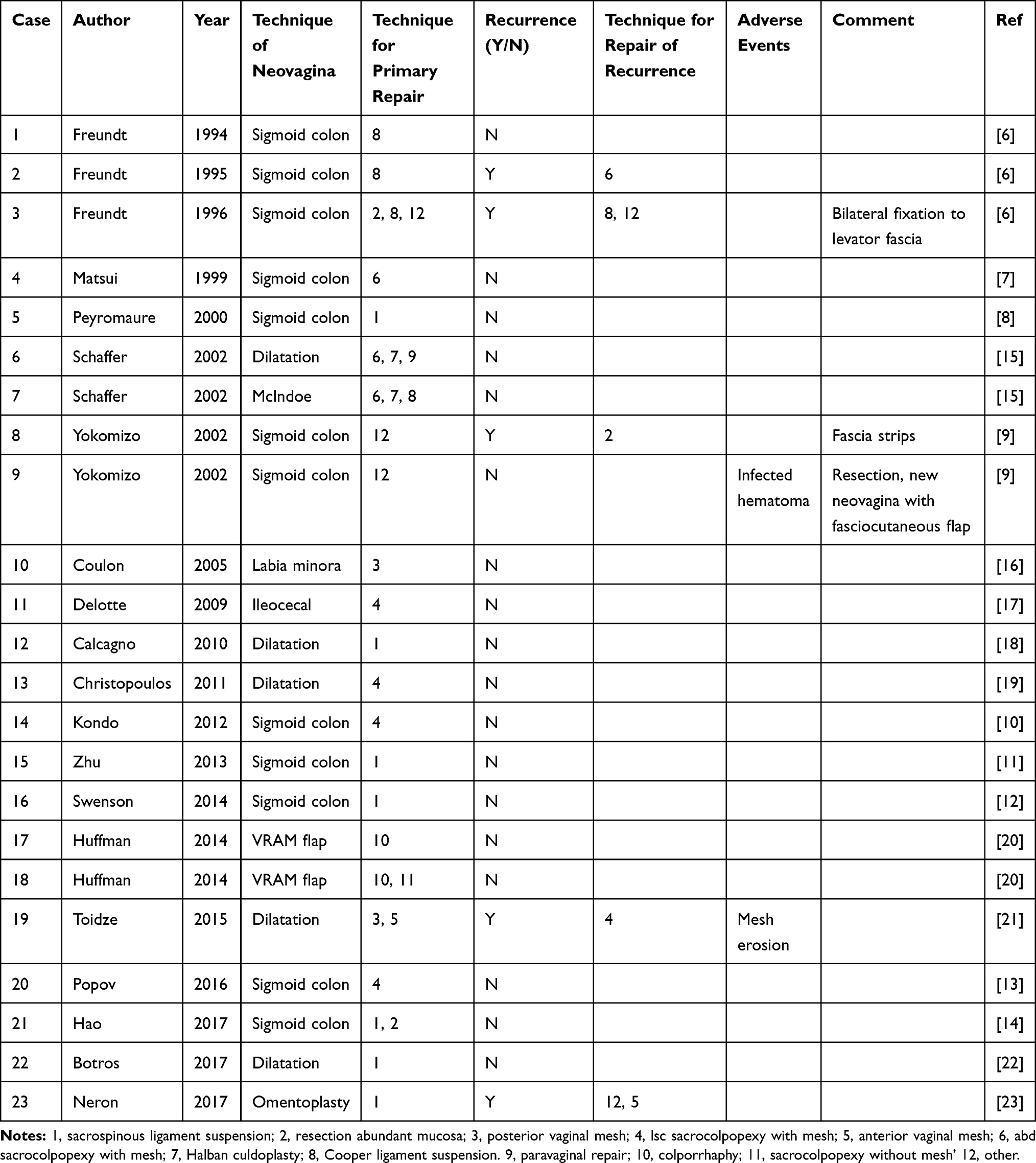 |
Table 1 Synopsis of surgical techniques for prolapse repair in the reported cases from the literature review |
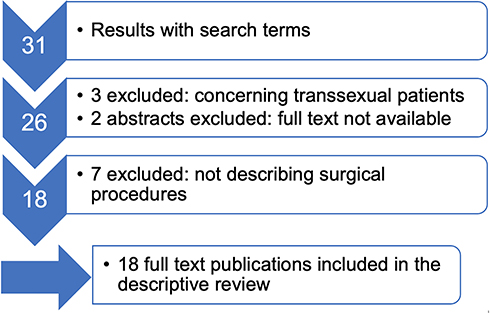 |
Figure 5 Procedure of literature selection with corresponding numbers of publications. |
Overall, we could find the description of 23 cases in women with a prolapse of a neovagina. Most of the women had a neovagina formed by sigmoid colon (12/23), further techniques were clearly more seldom used. In five cases dilatation was performed, for the other cases various different techniques were used to form the neovagina. In order to repair the prolapse a sacrospinous ligament suspension was the most common technique (6/23), in four cases a sacrocolpopexy with mesh was successful. In four cases a suspension to the Cooper ligament was performed, in two women resulting in recurrence of the prolapse, though. Further resection of abundant mucosa was necessary in three cases, always combined with at least one other surgical technique. In two women a vaginal mesh was used, in one case resulting in mesh erosion. For the other cases various techniques were used.
Discussion
To our knowledge we describe the twenty-fourth case of prolapse repair surgery in a neovagina. Only 12 other cases of women with a sigmoid neovagina are described. There is no consensus on the standard surgical treatment options. Sacrospinal ligament suspension is the most often used technique. Further techniques described in more than one case were sacrocolpopexy with mesh, suspension to the Cooper ligament and resection of abundant mucosa.
Our case showed that several complex aspects have to be considered when a neovaginal sigmoid prolapse occurs. In our patient various surgical attempts were necessary in order to successfully correct the neovaginal prolapse. Our experience is consistent with the literature we have found.
In our first attempt we initially decided for a sacrocolpopexy with mesh. As the neovagina of the patient was very long, the fixation to the sacrospinous ligament would probably not have offered enough suspension to the upper part of the neovagina. Intraoperatively we realized that the length of the vagina was much longer than preoperatively stated (33cm instead of 18cm). In addition, we found multiple adhesions intra-abdominally. As we assumed, that the blood vessel supply from the sigmoid arteries2 was one reason for the abundant length and therefore did not attempt to resect the cranial part. We then decided to suspend the neovagina directly to the promontory with PDS sutures and without the use of a mesh.
The resorbable suture did not provide sufficient fixation of the otherwise barely suspended neovagina. We therefore planned the use of a non-resorbable mesh in our second attempt. The mesh placement worked well. Nevertheless, a second recurrence of the prolapse occurred. We analyzed two possible causes for the recurrence: i) the prolonged length of the neovagina, and ii) the lesser tension for the suspension of the dorsal part of the sigmoid neovaginal wall because of the need to spare the vascular pedicle. An abundant length of a neovagina is indeed described in several publications as well as the resection of abundant mucosa. According to the cases found in our literature review, mucosal resection was always combined with some other surgical procedure in order to achieve a sufficient suspension.6,9,14
Finally, in our third attempt an interdisciplinary approach was necessary which addressed primarily the length of the neovagina. The shortening of the apical part in combination with the suspension with a non-absorbable mesh was the successful approach to correct the recurrent prolapse. With this procedure the additional resection of abundant vaginal length was possible and the accompanying mesh fixation was now successful.
In compliance with the findings from our literature review we experienced several key points.
- There are various techniques to form a neovagina, the use of sigmoid colon is the most frequent applied technique. With this procedure a vascular pedicle has to be spared. It is important to know about the technique of forming a neovagina before performing surgery for prolapse as the vessel supply has to be preserved.
- It can be difficult to repair a prolapse of a neovagina. Several cases of recurrence are described. It might be necessary to combine more than one technique in order to achieve the goal. In particular the resection of an abundant part of the neovagina has been described to be necessary in part, we experienced this as well in our case. The evaluation of the length and width of the neovagina preoperatively is notably important.
- Fixation to the sacrospinous ligament and sacrocolpopexy with mesh are the two most frequent used techniques described. We finally succeeded with an abdominal mesh suspension. Alike the situation in suspension of a natural vagina, within the little number of cases the abdominal meshes was not associated with adverse events whereas in two cases with the use of vaginal meshes in one case an erosion arose.
- A neovagina accounts for some additional complexity for surgical repair of a prolapse. According to our experience and our literature review we suggest a multidisciplinary approach involving at minimum an urogynecologic and a colorectal surgeon.
Ethics Committee Approval
Ethics Committee approval was obtained and is filed under No 2016-01676. Written informed consent was obtained from the patient for publication of this article and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Karim RB, Hage JJ, Dekker JJML, Schoot CMH. Evolution of the methods of neovaginoplasty for vaginal aplasia. Eur J Obstet Gynecol Reprod Biol. 1995;58(1):19–27. doi:10.1016/0028-2243(94)01954-6
2. Djordjevic ML, Stanojevic DS, Bizic MR. Rectosigmoid vaginoplasty: clinical experience and outcomes in 86 cases. J Sex Med. 2011;8(12):3487–3494. doi:10.1111/j.1743-6109.2011.02494.x
3. Lima M, Ruggeri G, Randi B, et al. Vaginal replacement in the pediatric age group: a 34-year experience of intestinal vaginoplasty in children and young girls. J Pediatr Surg. 2010;45(10):2087–2091. doi:10.1016/j.jpedsurg.2010.05.016
4. Gatti C, Del Rossi C, Lombardi L, Caravaggi F, Casolari E, Casadio G. Sexuality and psychosocial functioning in young women after colovaginoplasty. J Urol. 2010;184(4S):1799–1803. doi:10.1016/j.juro.2010.03.078
5. Copeland LJ, Hancock KC, Gershenson DM, Stringer CA, Atkinson EN, Edwards CL. Gracilis myocutaneous vaginal reconstruction concurrent with total pelvic exenteration. Am J Obstet Gynecol. 1989;160(5):1095–1101. doi:10.1016/0002-9378(89)90168-3
6. Freundt I, Toolenaar TA, Jeekel H, Drogendijk AC, Huikeshoven FJ. Prolapse of the sigmoid neovagina: report of three cases. Obstet Gynecol. 1994;83(5 Pt 2):876–879.
7. Matsui H, Seki K, Sekiya S. Prolapse of the neovagina in Mayer-Rokitansky-Kuster-Hauser syndrome. A case report. J Reprod Med. 1999;44(6):548–550.
8. Peyromaure M, Villet R, Jung JL, Szwarc G. [Prolapse of neovagina after anterior pelvic exenteration for urethral cancer]. Progres En Urol J Assoc Francaise Urol Soc Francaise Urol. 2000;10(3):456–460. French.
9. Yokomizo R, Murakami T, Naitou H, Yamada A. Treatment for prolapse of the sigmoid neovagina in Mayer- Rokitansky-Kuster-Hauser syndrome. Obstet Gynecol. 2002;100(5):3.
10. Kondo W, Ribeiro R, Tsumanuma FK, Zomer MT. Laparoscopic promontofixation for the treatment of recurrent sigmoid neovaginal prolapse: case report and systematic review of the literature. J Minim Invasive Gynecol. 2012;19(2):176–182. doi:10.1016/j.jmig.2011.12.012
11. Zhu L, Chen N, Lang J. Vault prolapse of sigmoid neovagina 26 years after vaginoplasty in Mayer-Rokitansky-Küster-Hauser syndrome: a case report. Int Urogynecol J. 2013;24(1):179–180. doi:10.1007/s00192-012-1755-6
12. Swenson CW, DeLancey JO, Schimpf MO. Left-sided sacrospinous ligament suspension for treating recurrent sigmoid neovagina prolapse. Int Urogynecol J. 2014;25(11):1593–1595. doi:10.1007/s00192-014-2415-9
13. Popov A, Gumina D, Mironenko K, et al. Laparoscopic sacrocolpopexy in a patient with vault prolapse of the sigmoid stump. Int Urogynecol J. 2016;27(2):315–316. doi:10.1007/s00192-015-2766-x
14. Hao Z, Yang S. Neovaginal prolapse treated with sacrospinous ligament suspension: a case report and review of the literature. J Pediatr Adolesc Gynecol. 2017;30(4):505–507. doi:10.1016/j.jpag.2016.12.005
15. Schaffer J, Fabricant C, Carr BR. Vaginal vault prolapse after nonsurgical and surgical treatment of MAAdullerian agenesis. Obstet Gynecol. 2002;99(5 Pt 2):947–949. doi:10.1016/s0029-7844(02)01969-5
16. Coulon C, Orazi G, Nayama M, Cosson M. Prolapse of neovagina created with labia minora: a case report. Int Urogynecol J Pelvic Floor Dysfunct. 2005;16(5):409–411. doi:10.1007/s00192-004-1262-5
17. Delotte J, Ferron G, Lim YKT, Querleu D. First laparoscopic repair of neovaginal prolapse following ileocecal reconstruction after resection of vaginal carcinoma. J Laparoendosc Adv Surg Tech. 2009;19(1):67–69. doi:10.1089/lap.2008.0098
18. Calcagno M, Pastore M, Bellati F, et al. Early prolapse of a neovagina created with self-dilatation and treated with sacrospinous ligament suspension in a patient with Mayer-Rokitansky-Küster-Hauser syndrome: a case report. Fertil Steril. 2010;93(1):
19. Christopoulos P, Cutner A, Vashisht A, Creighton SM. Laparoscopic sacrocolpopexy to treat prolapse of the neovagina created by vaginal dilation in Rokitansky syndrome. J Pediatr Adolesc Gynecol. 2011;24(2):e33–e34. doi:10.1016/j.jpag.2010.09.004
20. Huffman LB, Randolph LK, McCann GA, et al. Options for repair of rectus abdominis myocutaneous perineal/vaginal flap prolapse: a case series. Gynecol Oncol Case Rep. 2014;7:1–3. doi:10.1016/j.gynor.2013.10.001
21. Toidze TV, Echols KT, Caraballo R. A novel approach to recurrent vaginal vault prolapse in a patient with müllerian agenesis. Female Pelvic Med Reconstr Surg. 2015;21(3):e33–e35. doi:10.1097/SPV.0000000000000168
22. Botros C, Iyer S, Tran AM, Goldberg RP. Vaginal vault prolapse in a patient with Mayer-Rokitansky-Küster-Hauser syndrome: a video case presentation. Int Urogynecol J. 2017;28(11):1747–1749. doi:10.1007/s00192-017-3325-4
23. Neron M, Ferron G, Vieille P, Letouzey V, Fatton B, de Tayrac R. Treatment of neovaginal prolapse: case report and systematic review of the literature. Int Urogynecol J. 2017;28(1):41–47. doi:10.1007/s00192-016-3009-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.