")
Back to Journals » OncoTargets and Therapy » Volume 14
Surgical Resection of Pancreatic Hepatoid Carcinoma Followed by Combined Transarterial Chemoembolization and Immunotherapy: A Case Report
Authors He J, Zhao Q, Liu Q, Li F, He L, Liu M, Yan X
Received 8 June 2021
Accepted for publication 24 July 2021
Published 26 August 2021 Volume 2021:14 Pages 4575—4578
DOI https://doi.org/10.2147/OTT.S323811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Arseniy Yuzhalin
Jintong He,1 Qinying Zhao,2 Qiang Liu,1 Fei Li,1 Long He,1 Mengyi Liu,1 Xiong Yan1
1Department of Hepatobiliary Surgery, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Endocrinology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Correspondence: Xiong Yan
Department of Hepatobiliary Surgery, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Street, Yuzhong District, Chongqing, 400016, People’s Republic of China
Tel/Fax +86 23 89011491
Email [email protected]
Abstract: Pancreatic hepatoid carcinoma (HC) is a heterogeneous tumor with high degree of malignancy and poor prognosis, which display cytological and/or structural features of focal hepatocellular carcinoma (HCC). For the low incidence and atypical clinical symptoms, it is possible to be diagnosed as pancreatic cancer before operation, and mainly depending on the pathological examination. To the best of our knowledge, surgery combined with radiotherapy and chemotherapy is the common treatment of pancreatic HC. However, the curative effect and prognosis is poor. We report a case of 44-year-old woman with pancreatic HC treated with PD-1 receptor inhibitor and transarterial chemoembolization, whose clinical symptoms and laboratory indexes are significantly improved after treatment.
Keywords: pancreatic hepatoid carcinoma, surgical resection, transarterial chemoembolization, immunotherapy, case report
Introduction
Hepatoid carcinoma (HC) refers to an extra hepatic neoplasm which is characterized by its morphological and functional similarities to hepatocellular carcinoma (HCC).1 Most patients have elevated serum AFP and frequent vascular invasion, and are prone to liver and/or lymph node metastasis. HC usually occurs in the stomach, but can also occur in the ovaries, lungs, pancreas, uterus, gallbladder, bladder and other organs.2 Pancreatic HC, an extremely rare and easily overlooked tumor in clinical, is mainly diagnosed by postoperative pathological examination.3 At present, surgery combined with radiotherapy and chemotherapy is the common treatment of pancreatic HC, but the curative effect and prognosis is poor. We reported a pancreatic HC, discussed the challenges associated with the diagnosis and management of this rare tumor, and proposed a new method of the remarkable treatment.
Case Presentation
A 44-year-old woman, presented with 1-year history of dull pain in the left upper abdomen and aggravated with vomiting for 7 days, was admitted to our hospital in July 2020.The symptoms were not associated with eating and could be slightly relieved after curling position. Physical examination results showed a hard mass (7.0 × 6.0 cm) was found under the xiphoid in the upper abdomen with poor mobility and no tenderness.
The laboratory examination of tumor markers revealed CA 12–5 66.3 U/mL, CA 19–9 8.8 U/m, CA 72–4 1.5 U/m, CEA 0.9 ng/mL, AFP 77481.0 ng/mL, AFP-L3 10297.50 ng/mL. Blood test, liver and kidney function test, blood lipase and amylase test, coagulation test, fecal occult blood and hepatitis B test were normal. Abdominal enhanced CT revealed a heterogeneous soft tissue mass (7.6 × 7.3 cm) with nodular calcification in the splenogastric space, which showed an unclear boundary among the gastric wall, the caudal dorsal pancreas, and the splenic curvature of colon. Puncture biopsy of abdominal tumor revealed malignant tumor cell.
During the operation, a solid mass (about 12 × 15 × 10 cm) was found in the tail of the pancreatic body with complete capsule and hard texture, which was closed to the splenic body, the great curvature of posterior gastric wall, and the splenic flexion of colon. Eventually, we completely resected the tumor, spleen and splenic curvature of colon and performed them biopsy. Postoperative pathological examination showed the poorly differentiated carcinoma in pancreas (Figure 1). Immunohistochemical analysis: AFP (+), HC sectional (+), Arginase (-), CK7 (-), CK8 sectional (+), CK18 (+), CK19 sectional (+), CgA (-), CD56 (-), Syn (-), CK20 (-), CK5/6 (-), CDX-2 (-), P40 (-), CD34 vascular (+). Combined with the results of morphology and immunohistochemistry, the diagnosis of pancreatic HC was confirmed. After the operation, the AFP and AFP-L was detected decreased apace, AFP decreased to 22860.0 ng/mL and AFP-L decreased to 3385.00 ng/mL, respectively.
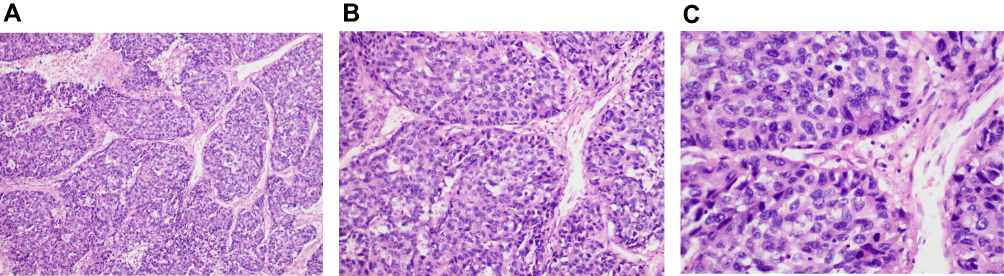 |
Figure 1 Biopsy specimen for tumor lesions. Notes: Microscopic morphology of pancreatic hepatoid carcinoma. (A) at low power view, the poorly differentiated neoplasm, which showed hepatoid differentiation, had abundant sinusoids and cord-like or nest-like arrangement of tumor cells; (B) at medium power view, the tumor cells had abundant cytoplasm, large and hyperchromatic nuclei, and frequent mitosis; (C) higher magnification of the poorly differentiated carcinoma demonstrating probable evidence of hepatoid differentiation of tumor cells. |
Considering the poor prognosis of surgery combined with radiotherapy and chemotherapy for treating the pancreatic HC, we performed the gene detection to seek the targeted gene for immunotherapy. The results showed that CDKN2A and CDKN2B were mutated. To the best of our knowledge, the mutation of CDKN2A tumor suppressor gene leads to the downstream CDK4/6 activation; PD-L1 (+), CPS=15. Thus, the patient was treated with the PD-1 inhibitor (Carrilizumab) and transcatheter arterial chemoembolization (Raltitrexed 4mg and Doxorubicin Hydrochloride Liposome Injection) 3 weeks as a course of treatment. The symptoms were significantly improved and no obvious tendency of tumor recurrence was found in repeated re-examinations. During the follow-up to March 2021, the patient is still asymptomatic alive. Her AFP decreased significantly to 24.4ng/mL and AFP-L3 decreased to 2.25ng/mL.
Discussion
HC is a rare and highly invasive malignant tumor, which derives from stomach, colon, esophagus, gallbladder, uterus, bladder, pancreas, ovary, fallopian tube and other organs.3,4 Pancreatic HC is an extremely uncommon subtype of HC which is characterized by its morphological and functional similarities to HCC.1 For the nonspecific symptoms including abdominal mass, nausea, vomiting, abdominal distension, and abdominal pain, it is easily diagnosed as pancreatic cancer. A majority (91.6%) of patients with pancreatic HC are associated with elevated AFP.5 Therefore, it is necessary to distinguish the pancreatic HC from the pancreatic cancer, the metastatic HCC, and the gynecological tumors. In this case, CT imaging features and symptoms were similar to the pancreatic cancer, except for the normal CA199. Although AFP was remarkably increased, hepatitis, liver space occupying lesions or gynecological tumors were not found. Eventually, the resection of pancreatic body and tail, splenic flexion, spleen and colon, and the liver were performed. The resected tissues were detected by pathological examination. The results confirmed that it was pancreatic HC.
Some studies have proposed that the pancreas and liver are originated from the same endoderm region and share the same primitive pluripotent stem cells.6 In the process of carcinogenesis, the genes that control hepatocyte differentiation in pancreatic stem cells are activated resulting in differentiation of pancreatic stem cells into HCC and secretion of normal hepatocytes or HCC products.7 Nowadays, dynamic monitoring of AFP and its heterogeneity are often utilized to diagnose pancreatic HC and evaluate its curative effect and prognosis. However, a recent study demonstrated that pancreatic cancer with large volume of serum and tissue AFP might not undergo hepatoid differentiation,8 which could lead to the misdiagnosis of pancreatic HC. To identify HCC, Hep-Par1 antibody, a specific marker presenting on mitochondria, is considered more sensitive than AFP. Its sensitivity and specificity can reach 83.7% and 96.7%,9 which may become a specific indicator for AFP-negative HC.
The early treatment of pancreatic HC is based on surgical resection, and the radiotherapy and chemotherapy are recognized as the mainstay of treatment when tumor metastasis occurs. Unfortunately, these patients have a high risk of postoperative metastasis and death compared with the common pancreatic and metastatic liver cancer. In addition, a study indicated that AFP-producing pancreatic cancer cells were less sensitive to 5-fluorouracil and gemcitabine by conducted vitro experiments.10 Since pancreatic HC was similar to HCC, researchers speculated that whether targeted drugs (such as PD-1 inhibitors) for HCC can be used for immunotherapy.11 In the present case, we performed the gene detection, and subsequently Carrilizumab combined with TACE therapy was used on August 13. After the first-round treatment, AFP decreased to 8012.0 ng/mL and AFP-L3 decreased to 1462.75 ng/m. The upper abdominal symptoms of the patients were significantly relieved. After the three-round treatment, the levels of AFP and AFP-L3 returned to the normal range. Until December 2020, the levels of AFP and AFP-L3 were still in the normal range (AFP decreased to 24.4ng/mL and AFP-L3 decreased to 2.25ng/mL). No sign of tumor recurrence was found from the abdominal enhanced CT.
Treatment, as in this case, is the first published reports of pancreatic HC treated with PD-1 receptor inhibitor and TACE. Although it is a preliminary exploration, this case still suggests that the use of PD-1 receptor inhibitor combined with TACE can effectively improve the prognosis of patients with pancreatic HC. Additionally, a healthy lifestyle is need to be established. The blood test, liver and kidney function test, AFP and AFP-L3 test, and abdominal CT are regularly performed to evaluate the patient’s condition.
Conclusion
In summary, we speculated that the characteristic of pancreatic HC may be similar to that of HCC. According to the results of pathological examination, immunohistochemistry and gene examination, PD-1 receptor inhibitor combined with TACE can be used to prolong the survival time and improve the quality of life, which opens potential treatment options for this poorly responsive pancreatic HC.
Data Sharing Statement
The data sets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The written informed consent of the patient was obtained for the publication of this case report and any identifying information and images. Institutional approval was not required to publish the case details.
Acknowledgments
We thank the First Affiliated Hospital of Chongqing Medical University for their support towards publishing this article.
Funding
The authors report no funding in this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Majumder S, Dasanu C. Hepatoid variant of pancreatic cancer: insights from a case and literature review. J Pancreas. 2013;14(4):442–445.
2. Huang J, Zhu R, Wu R, Li R, Yao N, Deng S. Hepatoid adenocarcinoma of the renal pelvis in a 59-year-old male with nephrolithiasis: case report and review of the literature. Curr Probl Cancer. 2019;43(5):471–476. doi:10.1016/j.currproblcancer.2018.12.007
3. Ishikura H, Fukasawa Y, Ogasawara K, Natori T, Aizawa M. An AFP-producing gastric carcinoma with features of hepatic differentiation. A case report. Cancer. 1985;56(4):840–848.
4. Yorita K, Sasaki S, Kawada A, et al. Hepatoid adenocarcinoma of the extrahepatic bile duct in a patient with polysplenia syndrome. Intern Med. 2017;56(4):401–407. doi:10.2169/internalmedicine.56.7526
5. Friedman P, Lai JP. Liver metastasis of urothelial carcinoma with hepatoid features: an unusual morphological finding. Anticancer Res. 2017;37(2):801. doi:10.21873/anticanres.11380
6. Pellini F, Vasquez J, Carilli A. Metastatic hepatoid carcinoma of the pancreas: first description of treatment with capecitabine and temozolomide. Am J Med Sci. 2017;353(6):610. doi:10.1016/j.amjms.2016.12.006
7. Zhuang L, Meng Z. An analysis of 28 cases of pancreatic carcinoma with elevated serum alpha-fetoprotein reported in the medical literature. Chin J Hepatobiliary Surg. 2013;19(6):420–424.
8. Veerankutty FH, Yeldho V, Ali TS, Venugopal B, Manoj KS, Vidhya C. Hepatoid carcinoma of the pancreas combined with serous cystadenoma: a case report and review of the literature. Hepatobiliary Surg Nutr. 2015;4(005):354–362.
9. Cong W, Tan L, Zhang S, et al. Immunohistochemical spectrum in the detection and differentiation of intrahepatic neoplasms. Chin J Oncol. 2002;24(006):553–556.
10. Sasaki N, Ishii T, Kamimura R, et al. Alpha-fetoprotein-producing pancreatic cancer cells possess cancer stem cell characteristics. Cancer Lett. 2011;308(2):152–161. doi:10.1016/j.canlet.2011.04.023
11. Petrelli F, Ghilardi M, Colombo S, et al. A rare case of metastatic pancreatic hepatoid carcinoma treated with sorafenib. J Gastrointest Cancer. 2012;43(1):97–102. doi:10.1007/s12029-011-9264-2
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.