")
Back to Journals » Clinical Ophthalmology » Volume 13
Surgical Outcomes Of Rhegmatogenous Retinal Detachment In Young Adults Ages 18–30 Years
Authors Brown K, Yannuzzi NA, Callaway NF , Patel NA, Relhan N, Albini TA, Berrocal AM, Davis JL, Fortun JA, Smiddy WE , Sridhar J, Flynn HW Jr , Townsend JH
Received 22 April 2019
Accepted for publication 10 September 2019
Published 31 October 2019 Volume 2019:13 Pages 2135—2141
DOI https://doi.org/10.2147/OPTH.S213042
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Karen Brown, Nicolas A Yannuzzi, Natalia F Callaway, Nimesh A Patel, Nidhi Relhan, Thomas A Albini, Audina M Berrocal, Janet L Davis, Jorge A Fortun, William E Smiddy, Jayanth Sridhar, Harry W Flynn Jr, Justin H Townsend
Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Justin H Townsend
Department of Ophthalmology, Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, 900 NW 17th Street, Miami, FL 33136, USA
Tel +1305 326-6000
Fax +1305 326-6417
Email [email protected]
Purpose: The purpose of this study is to investigate associations with and surgical outcomes of rhegmatogenous retinal detachment (RRD) in young adults.
Methods: This is a retrospective consecutive case series of patients aged 18–30 years who underwent surgical repair for RRD between January 1, 2014 and December 1, 2016 at a university referral center.
Results: The current study includes 38 eyes with RRD. Documented high or moderate myopia was present in 28 (74%) eyes. Connective tissue disease was present in 3 (8%) eyes. Median pre-operative visual acuity (VA) was 20/70. Surgery was performed via scleral buckle (SB) alone in 27/38 (71%) and via combined SB and pars plana vitrectomy (SB/PPV) in 11/38 (29%) eyes. Single surgery anatomical success (SSAS) rate was 20/27 (74%) for SB and 7/11 (64%) for SB/PPV. The retina was reattached at last follow-up in 25/27 (93%) for SB and 11/11 (100%) for SB/PPV. The median postoperative VA was 20/40.
Conclusion: In the current study of young adults with RRD, the most common association was high or moderate myopia. Visual and anatomic outcomes at last follow-up were generally favorable.
Keywords: myopia, rhegmatogenous retinal detachment, RRD, young adults
Introduction
Rhegmatogenous retinal detachment (RRD) occurs in about 1 in 10,000 people per year,1 most commonly in the fourth decade or later, often in association with myopia or prior intraocular surgery. RRD in the pediatric population is less common and is often attributable to previous intraocular surgery, trauma, connective tissue disorder or myopia.2–4 While many studies have examined the associations and surgical outcomes in a broad range of adult and pediatric populations, few studies have focused on outcomes in the young adult population. The purpose of this study is to evaluate associations with and surgical outcomes of RRD in young adults.
Materials And Methods
This is a retrospective consecutive case series of patients age 18–30 who underwent primary surgical repair for RRD at Bascom Palmer Eye Institute between January 1, 2014 and December 31, 2016. Approval was obtained by the Institutional Review Board (IRB) of the University of Miami School of Medicine. Written consent was obtained from all subjects and all performed procedures were in accordance with the Declaration of Helsinki. To evaluate only spontaneous RRD without any tractional or exudative component, patients with RRD in the context of documented trauma, proliferative diabetic retinopathy, other retinal vascular disease, chorioretinal inflammatory disease or viral retinitis were excluded. Patients with limited follow-up (less than 3 months) were also excluded. Patients with prior pneumatic retinopexy or surgical repair for RRD elsewhere in the affected eye were also excluded. The current study had no prospective protocol for surgical management or technique and the surgical approach was selected at the discretion of the treating surgeon. Data recorded included concurrent connective tissue disorder, history of high myopia (defined as manifest refraction ≥6 diopters) or moderate myopia (manifest refraction >1 but <6 diopters), lens status, presence of macular hole, macular status (attached or unattached), need for reoperation and type of secondary repair, retinal reattachment at last examination, preoperative visual acuity and visual acuity at last examination, presence of proliferative vitreoretinopathy (PVR) preoperatively, and development of PVR postoperatively.
Main outcome measures were single surgery anatomic success (SSAS), overall anatomic success (OAS), and best-corrected visual acuity (VA) at last examination. SSAS was defined as retinal reattachment at last follow-up after only one surgery. Eyes treated with subsequent surgery for epiretinal membrane (ERM) or cataract extraction were not considered primary failures. Eyes treated with supplemental laser were not considered primary failures if they did not require additional surgery in the operating room. Eyes that underwent silicone oil (SO) removal in the setting of attached retina, without need for further surgery, were not considered primary failures and were included as single surgery operation successes. OAS was defined as retinal reattachment at last examination. Visual outcome was determined by best-corrected VA at last examination and by change in VA from preoperative VA to VA at last follow-up. Visual success was defined as an improvement in VA by 15 or more letters on the Early Treatment Diabetic Retinopathy Study (ETDRS) letter score, or with final Snellen VA of 20/40 or better.
Because the current study was retrospective in nature, details of PVR grading were not always recorded. However, details of PVR were analyzed using any recorded data from the medical record or photography. There was no prospective protocol for recording grades of PVR or for surgical management.
Statistical analysis was performed with Fisher exact testing for categorical variables and with Wilcoxon rank-sum testing for continuous variables (i.e. visual acuity). The small sample size in this study precluded covariate adjustment. Therefore, statistical analysis presented in this study is unadjusted for covariables.
Results
A computerized search of the electronic medical record between 2014 and 2016 (3 years) for all RRDs resulted in 96 patients age 18–30. Forty-one patients were excluded based on ocular history: history of trauma (34), prior retinal surgery (1), history of retinopathy of prematurity (3), sickle cell retinopathy (1), proliferative diabetic retinopathy (1), chorioretinitis (1). An additional 17 patients were excluded from outcomes analysis due to duration of follow-up for less than 3 months. Of these 17 eyes, high or moderate myopia was present in 12 eyes (71%) and macula was attached in 4 (24%). Lens status was documented in 15 eyes and all were phakic. SB was performed in 12 (71%) eyes, PPV alone in 1 (6%) eye, and combined SB/PPV in 4 (24%).
In the current study, 38 eyes met the inclusion criteria. This study includes 38 eyes from 36 patients age 18–30 years (mean age 25.0 years, SD 4.2) with spontaneous RRD. Of the 38 cases, 22 (58%) were female. All eyes were phakic. The macula was attached at presentation in 10/39 (26%) of eye. Documented high myopia (manifest refraction ≥6 diopters) or moderate myopia (manifest refraction ≥1 but <6 diopters) was present in 28/38 (74%) eyes. Diagnosed or suspected connective tissue disease was present in 3/38 patients (8%). One patient was diagnosed with Stickler syndrome, 1 patient had retinal findings suggestive of Stickler syndrome, and 1 patient had Marfanoid habitus but no formal diagnosis at the time of RD. All three patients with suspected or diagnosed connective tissue abnormality also had high myopia. The remaining patients had no identifiable systemic or ocular predisposition. Prior retinal detachment in the fellow eye was present in 6/38 (16%) cases. Prior laser retinopexy had been performed for retinal tear in 3/38 (8%) eyes. Amblyopia was present in 1/38 (3%) eyes. Patient demographics and outcomes are outlined in Figure 1A and B.
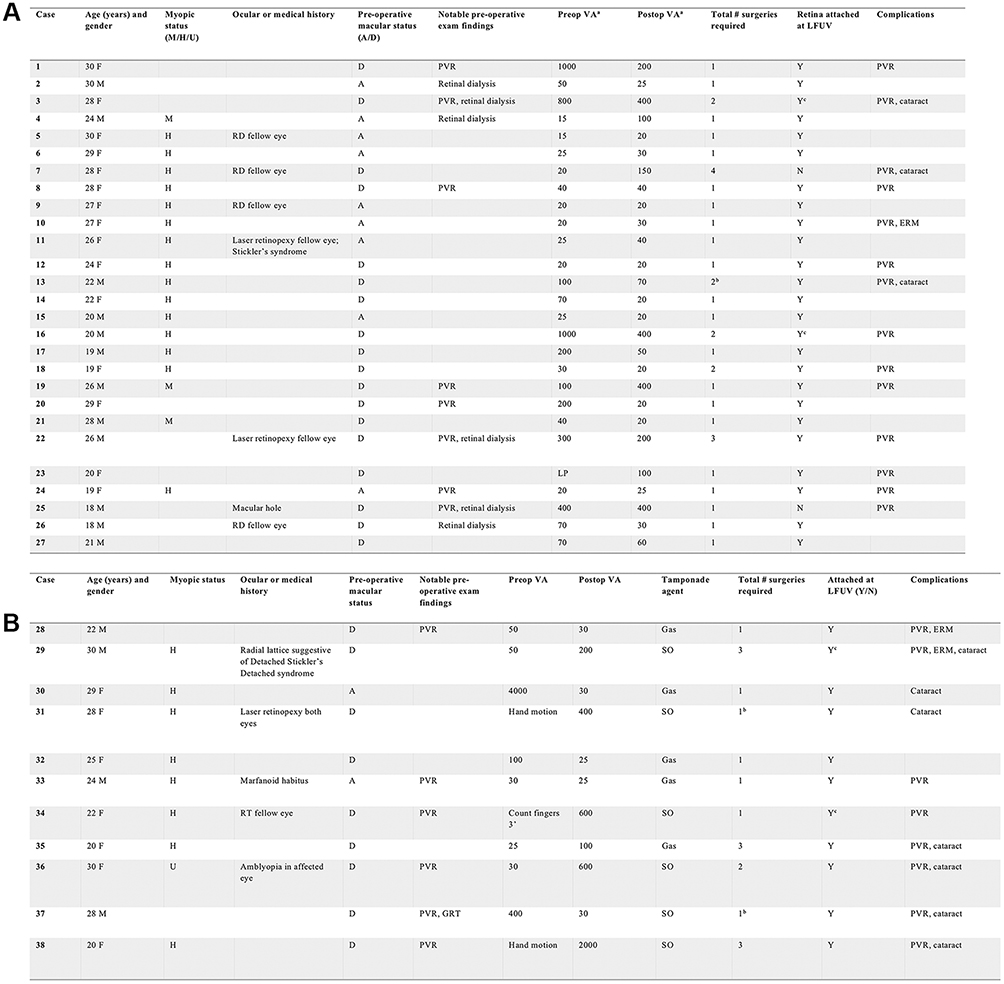 |
Figure 1 (A) Demographics and outcomes of eyes that underwent primary SB for RRD. (B) Demographics and outcomes of eyes that underwent primary SB/PPV for RRD. |
Surgery was performed via scleral buckle (SB) alone in 27/38 (71%) and via combined SB and pars plana vitrectomy (SB/PPV) 11/38 (29%) of cases. All scleral buckles used were encircling scleral buckles. A radial element was used in addition to encircling buckle in one eye in the SB group (case 23). No patients underwent primary PPV alone. For patients who underwent SB/PPV, 5/11 (45%) received gas tamponade (either SF6 or C3F8) and 6/11 (55%) received silicone oil (SO) tamponade. All cases were repaired by one of 16 vitreoretinal faculty at the Bascom Palmer Eye Institute.
At least one retinal break was identified in 34/38 (89%) eyes. In the absence of documented ocular trauma, giant retinal tear was identified in 1/38 (3%) eye and retinal dialysis was identified in 6/38 (16%) eyes. The SSAS in eyes with dialysis was 3/6 (50%) and overall anatomic success (OAS) was 5/6 (83%) due to persistent-localized subretinal fluid in one patient that did not require reoperation after primary repair. Median postoperative Snellen VA in patients with retinal dialysis was 20/141 (LogMAR 0.80).
Overall mean follow-up was 19.1 months (SD 10.6 months). Mean follow-up in the primary SB group and primary SB/PPV group was 18.3 months (SD 11.3 months) and 20.9 months (SD 8.6 months), respectively.
Single surgery anatomical success (SSAS) rate for SB alone was 20/27 (74%) and for SB/PPV was 7/11 (64%) (p=0.43). For eyes that underwent primary SB, retinal redetachment occurred in 7/27 (26%) eyes. Localized persistent subretinal fluid occurred in 1 eye and did not require additional surgery within the follow-up period. Of the remaining 6 eyes with retinal redetachment, secondary repair was performed with PPV/SOI in 4 patients and PPV/gas in 2 patients. The average number of operations performed in patients with retinal redetachment after primary SB was 1.3 (range 0–3). For eyes that underwent primary SB/PPV, retinal redetachment occurred in 4 eyes. All eyes with retinal redetachment in this group underwent repeat PPV/SOI. The average number of reoperations performed in patients with retinal redetachment after primary SB/PPV was 2.0 (range 1–3). Of note, 2 eyes that underwent primary SB/PPV/SO underwent SOR in the setting of retinal reattachment, without subsequent redetachment in the follow-up period and were included as single surgery anatomic successes (cases 34 and 37). A third eye that underwent SB/PPV/SO remained attached under oil at last follow-up (case 34).
Overall retinal reattachment rate at the last follow-up visit was 36/38 (95%). OAS for eyes that underwent primary SB and primary SB/PPV was 25/27 (93%) and 11/11 (100%), respectively. Two eyes in the primary SB group (cases 3 and 16) and 2 eyes in the primary SB/PPV group (cases 29 and 34) had SO in place at the last follow-up and retina was attached under SO. Surgical outcomes data are presented in Figure 2.
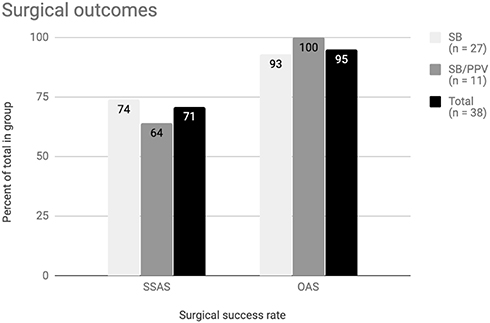 |
Figure 2 Surgical outcomes. Single surgery anatomical success (SSAS) rate for all eyes was 27/38 (71%). SSAS for SB alone was 20/27 (74%) and for SB/PPV was 7/11 (64%) (p=0.43). Overall anatomic success (OAS) rate at the last follow-up visit was 36/38 (95%). OAS for eyes that underwent primary SB and primary SB/PPV was 25/27 (93%) and 11/11 (100%), respectively. |
Proliferative vitreoretinopathy (PVR) was noted preoperatively in 15/38 (39%) eyes. PVR grade C was noted preoperatively in 11/38 (29%) eyes. Of eyes that underwent primary SB alone, 7/27 (26%) had PVR grade C preoperatively. Of eyes that underwent primary SB/PPV, 4/11 (36%) had PVR grade C preoperatively (p=0.70). PVR developed postoperatively in an additional 8 patients who did not have documented PVR preoperatively. Overall, PVR developed in 15/27 patients who underwent primary SB and 8/11 patients who underwent primary SB/PPV (p=0.47). All primary repair failures occurred in the setting of PVR development.
In the current study, median preoperative Snellen VA was 20/70 (median LogMAR VA 0.54, mean LogMAR 0.82, SD 0.86). The macula was attached in 9/27 (33%) eyes that underwent primary SB and 1/11 eyes that underwent primary SB/PPV (p=0.23). For eyes that underwent primary SB, median preoperative Snellen VA was 20/50 (LogMAR 0.40) and preoperative VA was 20/200 or better in 21/27 (78%) eyes. For eyes that underwent primary SB/PPV, median preoperative Snellen VA was 20/400 (LogMAR 1.30, p=0.02) and preoperative VA was 20/200 or better in 5/11 (45%) eyes.
The overall median Snellen VA at last examination was 20/40 (median LogMAR 0.30, mean LogMAR 0.55, SD 0.56). Visual success, defined as Snellen VA 20/40 or better or an improvement by 15 or more letters (ETDRS), was achieved in 29/38 (76%) of all patients and overall median change in LogMAR VA was −0.18, or an improvement of 9 letters on the EDTRS letter score. Postoperative Snellen VA was significantly better in eyes with macula attached preoperatively compared to eyes with macula detachment (p=0.01). Median postoperative Snellen VA for eyes that underwent primary SB was 20/40 (LogMAR 0.30) and postoperative VA was 20/200 or better in 23/27 (85%) eyes. Visual success was achieved in 20/27 (74%) and median change in LogMAR VA was −0.10, or an improvement of 5 letters on the EDTRS letter score. For the primary SB/PPV group, median postoperative Snellen VA was 20/100 (LogMAR 0.70, p=0.05) and postoperative VA was 20/200 or better in 7/11 (64%) eyes. Visual success was achieved in 9/11 (82%) and median change in LogMAR VA was −0.35, or 18 letters on the EDTRS letter score. Visual acuity outcomes are presented in Figure 3.
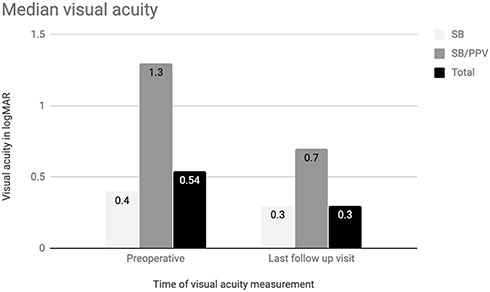 |
Figure 3 Visual acuity outcomes. Median preoperative Snellen VA was 20/70 (median LogMAR VA 0.54, mean LogMAR 0.82, SD 0.86). For eyes that underwent primary SB, median preoperative Snellen VA was 20/50 (LogMAR 0.40). For eyes that underwent primary SB/PPV, median preoperative Snellen VA was 20/400 (LogMAR 1.30, p=0.02). The overall median Snellen VA at last examination was 20/40 (median LogMAR 0.30, mean LogMAR 0.55, SD 0.56). Median postoperative Snellen VA for eyes that underwent primary SB was 20/40 (LogMAR 0.30). For the primary SB/PPV group, median postoperative Snellen VA was 20/100 (LogMAR 0.70, p=0.05). |
Cataract extraction was performed subsequent to primary repair in 3/27 (11%) eyes that underwent primary SB and in 7/11 (64%) of eyes that underwent primary SB/PPV (p=0.002). In all eyes in the SB group that underwent subsequent cataract extraction, secondary PPV had been performed with silicone oil due to recurrent detachment.
Discussion
In the current study, the majority of patients were repaired with SB alone (71%), and final anatomic reattachment rate was 95%. The predominance of SB alone as the primary treatment choice in this study is consistent with treatment modalities reported in patients with RRD in this age group. In a recent retrospective review of RRD repair in 512 patients, primary SB was the most common means of repair in patients aged 21–40 years (15/23 (65%) SB, 8/23 (35%) primary PPV alone), with primary PPV alone more common in patients aged 40 years or older.5 In a recent review of RRD repair in 3403 eyes in the United Kingdom National Health Services, a considerably lower average age was reported in patients who were repaired with SB alone (39.2 years) compared to PPV (62.6 years) or combined SB/PPV (58.4).6 The use of SB for primary repair in younger patients may reflect the lack of posterior vitreous detachment (PVD) and the phakic lens status, with an effort to preserve accommodation given the higher incidence of cataract development in phakic eyes that undergo initial PPV.7 PPV alone was not considered due to the age of the patients and the lack of PVD in this age group. The incidence of interim cataract extraction between time of primary repair and last clinical visit was significantly higher in the SB/PPV group (7/11 (64%)) compared to the SB group (3/27 (11%)) (p=0.002). All eyes that underwent primary SB and subsequent cataract extraction had also undergone secondary PPV with SO for recurrent detachment.
Retinal dialysis was noted in 6/38 (16%) eyes despite no reported history of trauma. This may suggest a remote history of or unrecognized trauma in these patients. However, idiopathic, nontraumatic retinal dialysis has been reported to occur in young adult eyes, potentially attributable to a developmental abnormality of the retinal periphery or vitreous base.8
SSAS was lower in the current study (71%) compared to some recent studies reporting SSAS for all age groups. The United Kingdom Health Services review reports an SSAS of 87% for patients treated with SB and 86% for patients treated with combined SB/PPV. Haugstad et al report similar SSAS rates with primary SB and SB/PPV repair (86% and 87%, respectively). The lower SSAS may reflect the greater incidence of high myopia in the current study, although myopia incidence is not reported in either of these studies for comparison, or an inherent difference in the vitreoretinal interface of patients who develop retinal detachment at younger ages when compared to all age groups. A recent retrospective review of primary RRD repair by Mansouri et al in 2010 reported redetachment rate of 25% in patients with high myopia.9 In a recent retrospective review of recurrent retinal detachment following RRD repair for highly myopic eyes (defined as manifest refraction range −14 to −29 diopters), a lower number of adjunctive procedures was reported in eyes with recurrence following primary SB compared to eyes with recurrence following primary PPV.10 The current study demonstrated a similar trend, with lower average number of reoperations required in the SB group (1.3) compared to SB/PPV (1.8), although this may be reflective of SB/PPV surgical approach being chosen for more significant or complex detachment. There was no significant difference between the presence of myopia between the SB and SB/PPV groups (p=0.45) or between the SSAS rates between eyes with and without myopia (P=1.00). There was also no statistically significant difference between SSAS rate between the SB and combined SB/PPV groups (p=0.43).
All recurrent retinal detachments occurred in the setting of PVR. Preoperative PVR grade C was present in 26% of patients who underwent primary SB and in 38% of the patients who underwent SB/PPV. This incidence is higher than the 5–12% rate reported in prior literature in larger retinal detachment series.11–13 Overall rate of PVR development (noted preoperatively or postoperatively) was 61% (23/38) (56% in SB only group, 75% in SB/PPV group, p=0.47). This correlates more closely with previously noted rates of PVR development (20–60%) in the pediatric population.3–5,14 This may be attributable to the chronicity of retinal detachment, and indicates the challenge of retinal detachment management in the young adult population. Additional analysis with a larger sample size may allow further identification of an association between PVR and recurrent detachment in this age group.
In the current study, overall anatomic success was 95%, consistent with overall reattachment rates in recent literature.5 Prior retinal detachment in the fellow eye was present in 13% of cases, slightly higher than observed rates of 2–10% in the adult population15 and likely reflective of the presence of high myopia in the current study.16
In the current study, preoperative visual acuity was significantly better in the SB group compared to the SB/PPV group (p=0.02), reflective of the macular status of the SB group (9/27 (33%) attached) compared to the SB/PPV group (2/11 (18%) attached). There was a trend toward visual improvement in both groups postoperatively, with no statistically significant difference in postoperative visual acuity between the two groups (p=0.05). Variable complexity of the RRD and the presence of silicone oil at the last follow-up in some patients limit a definitive visual acuity analysis.
This study is limited by its retrospective design and lack of a standardized protocol for surgery and for postoperative refraction. In addition, limited follow-up resulted in exclusion of some patients from the study, which is likely due in part to the institution as a referral center, with many patients obtaining follow-up at remote locations. A further limitation of the study includes the small sample size, with the study underpowered to detect any difference in outcomes between the two surgical approaches implemented or between different demographics.
In this retrospective review of RRD repair in young adult patients, the most common association was high or moderate myopia (74%). The correlation between RRD in the setting of high myopia and younger age has been reported16 and is supported by the current study. There was no documented predisposing factor in 26% of patients. Visual and anatomic outcomes were favorable, with visual success achieved in 76% of eyes and anatomic success achieved in 95% of eyes.
Acknowledgment
The abstract of this paper was presented in July 2019 at the American Society of Retina Specialists (ASRS) annual meeting as a poster presentation with interim findings. The poster’s abstract was published in “Posters” in the ASRS website: https://www.docwirenews.com/conference-coverage/asrs2019/surgical-outcomes-of-rhegmatogenous-retinal-detachment-in-young-adults/. The abstract of this paper was presented in September 2018 at the Retina Society annual meeting as a podium presentation with interim findings.
Disclosure
Thomas A Albini reports personal fees from Genentech, personal fees from Allergan, personal fees from Novartis, personal fees from Eyepoint, personal fees from Clearside, personal fees from Santen, personal fees from Bausch + Lomb, outside the submitted work. Jayanth Sridhar reports personal fees from Alcon, personal fees from Alimera Science, personal fees from Thrombogenics, outside the submitted work. Harry W Flynn Jr reports grants from National Institutes of Health (NIH), Bethesda, Maryland, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Mitry D, Charteris DG, Fleck BW, et al. The epidemiology of rhegmatogenous retinal detachment: geographical variation and clinical associations. Br J Ophthalmol. 2010;94(6):678–684. doi:10.1136/bjo.2009.157727
2. Gonzales CR, Singh S, Yu F, et al. Pediatric rhegmatogenous retinal detachment: clinical features and surgical outcomes. Retina. 2008;28(6):847–852. doi:10.1097/IAE.0b013e3181679f79
3. Soheilian M, Ramezani A, Malihi M, et al. Clinical features and surgical outcomes of pediatric rhegmatogenous retinal detachment. Retina. 2008;29(4):545–551. doi:10.1097/IAE.0b013e318194fd1a
4. Read SP, Aziz HA, Kuriyan A, et al. Retinal detachment surgery in a pediatric population: visual and anatomic outcomes. Retina. 2018;38(7):1393–1402. doi:10.1097/IAE.0000000000001725
5. Haugstad M, Moosmayer S, Bragadottir R. Primary rhegmatogenous retinal detachment – surgical methods and anatomical outcome. Acta Ophthalmol. 2017;95(3):247–251. doi:10.1111/aos.13295
6. Jackson T, Donachie P, Sallam A, Sparrow JM, Johnston RL. United Kingdom national ophthalmology database study of vitreoretinal surgery: report 3, retinal detachment. Ophthalmology. 2014;121(3):643–648. doi:10.1016/j.ophtha.2013.07.015
7. Schaal S, Sherman MP, Barr CC, Kaplan HJ. Primary retinal detachment repair: comparison of 1-year outcomes of four surgical techniques. Retina. 2011;31(8):1500–1504. doi:10.1097/IAE.0b013e31820d3f55
8. Kinyoun JL, Knoblock WH. Idiopathic retinal dialysis. Retina. 1984;4(1):9–14. doi:10.1097/00006982-198400410-00003
9. Mansouri A, Almony A, Shah GK, Blinder KJ, Sharma S. Recurrent retinal detachment: does initial treatment matter? Br J Ophthalmol. 2010;94(10):1344–1347. doi:10.1136/bjo.2009.175968
10. Ripandelli G, Rosso T, Scarinci F, Stirpe M. Encircling scleral buckling with inferior indentation for recurrent retinal detachment in highly myopic eyes. Retina. 2015;35(3):416–422. doi:10.1097/IAE.0000000000000389
11. Sadaka A, Giuliari GP. Proliferative vitreoretinopathy: current and emerging treatments. Clin Ophthalmol. 2012;6:1325–1333. doi:10.2147/OPTH.S27896
12. Kwon OW, Song JH, Roh MI. Retinal detachment and proliferative vitreoretinopathy. Dev Ophthalmol. 2016;55:154–162. doi:10.1159/000438972
13. Joeres S, Kirchhof B, Joussen AM. PVR as a complication of rhegmantogenous retinal detachement: a solved problem? Br J Ophthalmol. 2006;90(6):796–797. doi:10.1136/bjo.2005.088856
14. Soliman M, Macky T. Pediatric rhegmantogenous retinal detachment. Int Ophthalmol Clin. 2011;51(1):147–171. doi:10.1097/IIO.0b013e31820099c5
15. Steel D. Retinal detachment. BMJ Clin Evidence. 2014;2014.
16. Orihara T, Hirota K, Yokota R, et al. Clinical characteristics of rhegmatogenous retinal detachment in highly myopic and phakic eyes. Nihon Ganka Gakkai Zasshi. 2016;120(5):382–389.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.