")
Back to Journals » Clinical Interventions in Aging » Volume 17
Superoxide Dismutase and Glutathione Reductase as Indicators of Oxidative Stress Levels May Relate to Geriatric Hip Fractures’ Survival and Walking Ability: A Propensity Score Matching Study
Authors Liu M, Yang C, Chu Q, Fu X, Zhang Y, Sun G
Received 15 April 2022
Accepted for publication 30 June 2022
Published 12 July 2022 Volume 2022:17 Pages 1081—1090
DOI https://doi.org/10.2147/CIA.S370970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Mingchong Liu,1,* Chensong Yang,1,* Qining Chu,2 Xiao Fu,1 Yue Zhang,1 Guixin Sun1
1Department of Traumatic Surgery, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China; 2Emergency Trauma Center, Nanyang Second General Hospital, Nanyang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guixin Sun, Department of Traumatic Surgery, Shanghai East Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China, Tel +21-38804518, Fax +21-65983047, Email [email protected]
Background: Oxidative stress status may affect bone metabolism and regeneration. However, few studies reported whether oxidative stress could impact the outcomes of hip fractures. This study aimed to explore if superoxide dismutase and glutathione reductase, the critical antioxidant enzymes, correlated with the prognosis of hip fractures.
Methods: Patients with hip fractures were extracted from our database, and those who met the inclusion criteria were analyzed. Propensity score matching was used to reduce the influence of confounding factors, and ROC curves based on matched populations were created to determine the optimal cutoff points of SOD and GR. Then, outcomes between SOD or GR and outcomes of hip fractures were compared.
Results: Out of 301 patients enrolled in this study, 50 patients died within one year. After a 1:1 PSM, the patients with less than 1-year survival had significantly lower SOD (p = 0.026) and GR (p = 0.021) than those who were still alive at one year. Logistics analysis showed that low SOD and low GR may be independent risk factors for 6-month survival, 1-year survival, 6-month free walking ability, and 1-year free walking ability.
Conclusion: SOD and GR may be the independent risk factors for survival and walking abilities of hip fractures.
Keywords: hip fractures, oxidative stress, superoxide dismutase, glutathione reductases, prognosis
Introduction
With the aggravation of the aging society, more and more elderly people suffer from fractures.1 Hip fractures have become one of the most common and severe fractures in the old, and the incidence is increasing.2 With the deterioration of the organs and lack of regeneration ability, the elderly with hip fractures, especially those accompanied by a variety of basic diseases, may have a poor prognosis even after surgery.3 Poor bone regeneration is associated with nonunion of hip fractures, and the hip is the location that bears huge force, which results in a long stay in bed.4 Unable to get up and walk may cause severe complications, such as pneumonia, decubitus, and thrombosis, which are the main cause of death for patients with hip fractures after surgeries.5 Therefore, the potent ability of bone regeneration may accelerate the rehabilitation of hip fractures, then reduce the stay in bed and improve the survival rate and life quality.
Bone regeneration is a tightly regulated procedure that involves two types of cells: the osteoblasts and the osteoclasts. Osteoclasts play pivotal roles in bone resorption while osteoblasts involve in bone-forming. Both of them are critical in bone metabolism.6 After the fracture, the broken end of the bone may stimulate inflammation by releasing inflammatory factors and promoting the chemotactic movement of immunocytes.7 The inflammation causes cellular damage, and then free radicals, such as reactive oxygen species (ROS) and reactive nitrogen species (RNS), were accumulated, resulting in oxidative stress.8 Oxidative stress may interrupt the balance of bone metabolism and lead to abnormal bone generation, which makes patients who are suffering fractures have long bed-stay, fracture nonunion, and poor outcomes.9 Many intrinsic enzymes may neutralize oxidative stress, such as superoxide dismutase (SOD), glutathione reductases (GR), and others. These enzymes can protect DNA, enzymes, and other cell structures from the damage of oxidative stress.10
SOD are the metalloproteins, and they have a remarkable efficiency in catalyzing the dismutation of superoxide and regulating oxidative stress.11 Similarly, GR regulates oxidative stress by catalyzing the reduction of oxidized glutathione (GSSG) to GSH.12 As the two widely used intrinsic antioxidant enzymes in clinical application, SOD and GR had been proven to be biomarkers of oxidative status in many pathological and physiological processes including bone regeneration.13–16 However, how the SOD or GR correlate with outcomes of hip fracture has rarely been reported. In our study, we aimed to explore the relationships between oxidative stress and outcomes of hip fractures and identify if the levels of SOD and GR, the critical antioxidant enzymes, were associated with the survival and free walking ability of patients who underwent surgeries due to hip fracture.
Materials and Methods
Study Design and Data Collection
This study was a retrospective study using the data of patients admitted to the Department of Traumatology, Shanghai East Hospital, Tongji University, School of Medicine, Shanghai, China. The study was performed according to the Declaration of Helsinki and was approved by the Institutional Ethics Committee of East Hospital. Written informed consent was obtained from all participants enrolled in this study. All patient-related data were anonymized to ensure confidentiality.
The data of patients enrolled in this study were extracted from our database which was based on the data of all patients admitted to our department with hip fractures in recent five years. In our study, the data of patients who fulfilled the inclusion criteria and not met the exclusion criteria in the database were extracted. The inclusion criteria were set as below: (1) aged ≥50 years; (2) treated with surgeries; (3) underwent surgeries between January 2019 and February 2021. The exclusion criteria were as follows: (1) with high-energy mechanism fractures; (2) with pathological fractures; (3) with acute or severe liver diseases.
Baseline characteristics were collected and reviewed, including age, sex, height and weight, residence, the position of fracture, type of fracture, fractures history, smoking and alcoholism history, hip fracture type, polytrauma, surgical procedures, anesthesia, time from injury to surgery, electrocardiogram and chest radiograph, hemoglobin (Hb), international normalized ratio (INR), blood glucose (GLU), albumin (ALB), superoxide dismutase (SOD) and glutathione reductase (GR). Major comorbidities were reviewed and the Charlson comorbidity index (CCI) was calculated.17 The diagnosis of electrocardiogram and chest radiograph were reviewed and evaluated by the corresponding author (Dr. Sun), and those may impact the prognosis of hip fractures were considered abnormal. All the laboratory test data analyzed in our study including SOD and GR were the data of the first routine test when patients were admitted to our hospital, and all laboratory tests were conducted immediately.
Follow Up and Outcomes
All patients in our database had been or were being followed up for one year. The status of patients who visited our outpatient clinic regularly was recorded by our colleagues while others were followed up via telephone. Survival time in our study was identified as the time from surgery to death caused by any disease. The patients with more than one-year survival were defined as censored data. Patients who were able to handle the daily activities without assistance were considered to have free walking abilities. Outcomes in this study were the statues of survival and free walking at 3 months, 6 months, and 1 year after surgery.
Statistical Analyses
Continuous variables were presented as mean ± standard deviation and evaluated by independent Student’s t-test for normally distributed variables, and by Wilcoxon rank-sum test for non-normally distributed data. Categorical variables were expressed as count (percent) and compared by chi-square test or Fisher’s exact test. Baseline characteristics of the patients grouped by survival status at one year were summarized and compared. Then, a 1:1 PSM (propensity score matching) with a caliper of 0.2 in R software was used to reduce the influence of confounding factors and the baseline features were also examined for populations after matching. ROC curves were established to determine the optimal cutoff points of SOD and GR according to Youden Index.
Stepwise regression was used to identify if multiple co-linear relationships existed between SOD and GR. Similarly, Spearman’s rank correlation coefficient was calculated to explore the correlation between SOD and GR. Cox analysis was used to identify the risk factors of 1-year survival, and SOD and GR in different types of variables were included. Moreover, outcomes were compared in patients divided by the levels of SOD and GR. Kaplan-Meier and Log rank tests were used for the analysis of 1-year survival. Then, Logistics regression was performed to identify the predicted value of SOD and GR for survival and free walking abilities at 6 months and 1 year after surgery. All p < 0.05 were considered statistically significant and statistical analyses were performed using SPSS version 26.0 (IBM, Armonk, NY, USA), GraphPad Prism version 8.0.1 (GraphPad Software San Diego, USA), and R software version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study Population
Out of 604 patients who underwent hip surgeries for hip fractures between January 2019 and February 2021 in our hospital, 303 patients were excluded because of the unavailable data of SOD and GR, loss of following up, and miss of the inclusion. Finally, 301 patients were analyzed (Figure 1). All the surgical procedures for the patients were carried out by the senior author (Guixin, Sun) or in the presence and supervision of him, which may reduce the impact of the operator factor. Almost all the patients with intertrochanteric fractures were treated by internal fixation (only two cases underwent arthroplasty), while patients with femoral neck fractures were treated by internal fixation or arthroplasty (Figure 1). Patients were not allowed to bear any weight for 1 week after surgery, followed by partial weight bearing, then full weight bearing at 4 weeks. All the patients were able to walk independently before surgery.
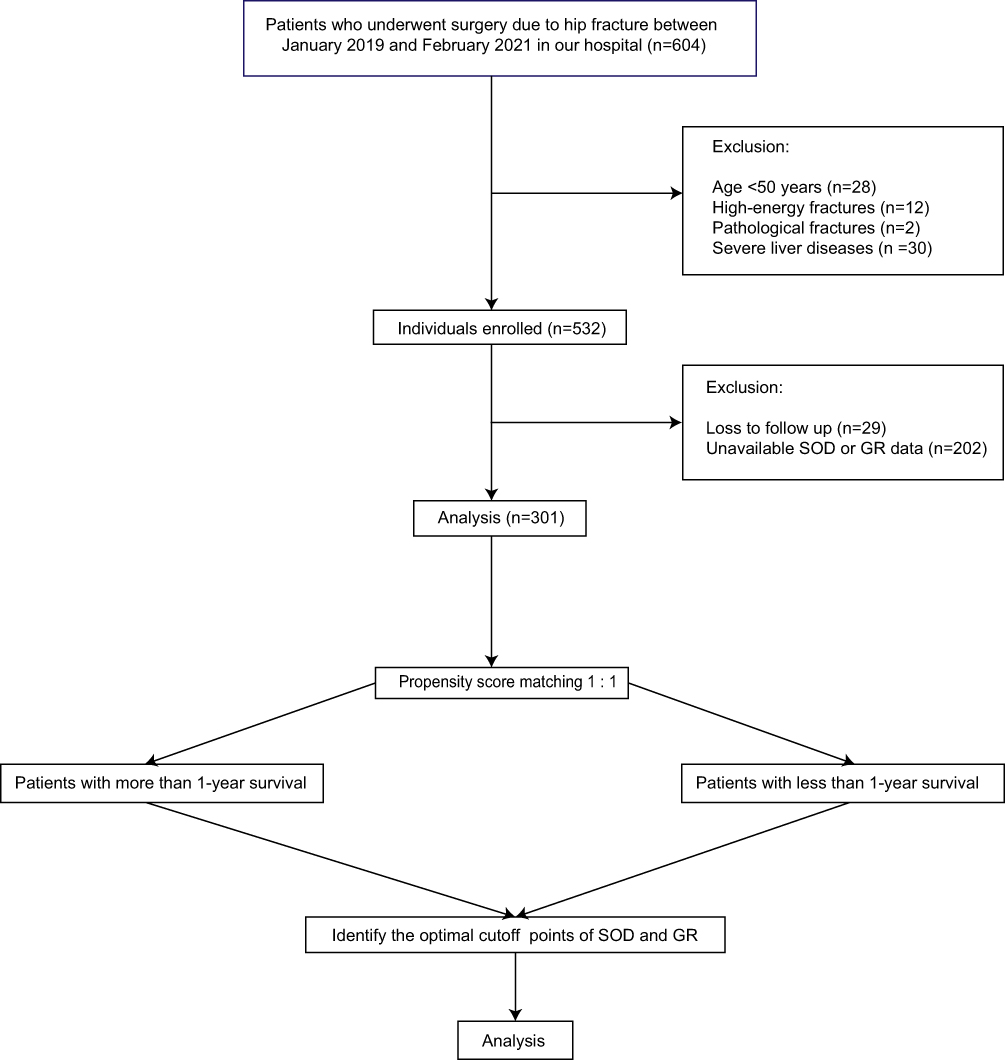 |
Figure 1 Flowcharts of our study. |
Then the baseline characteristics were compared between the patients who survived more than one year and less than one year as shown in Table 1. Baseline features of patients grouped by type of surgery were also summarized in Supplementary Table 1. Many factors that may affect the outcomes of the patients were significantly different in the groups divided by 1-year survival (Table 1), so PSM was used to reduce the bias of the covariables.
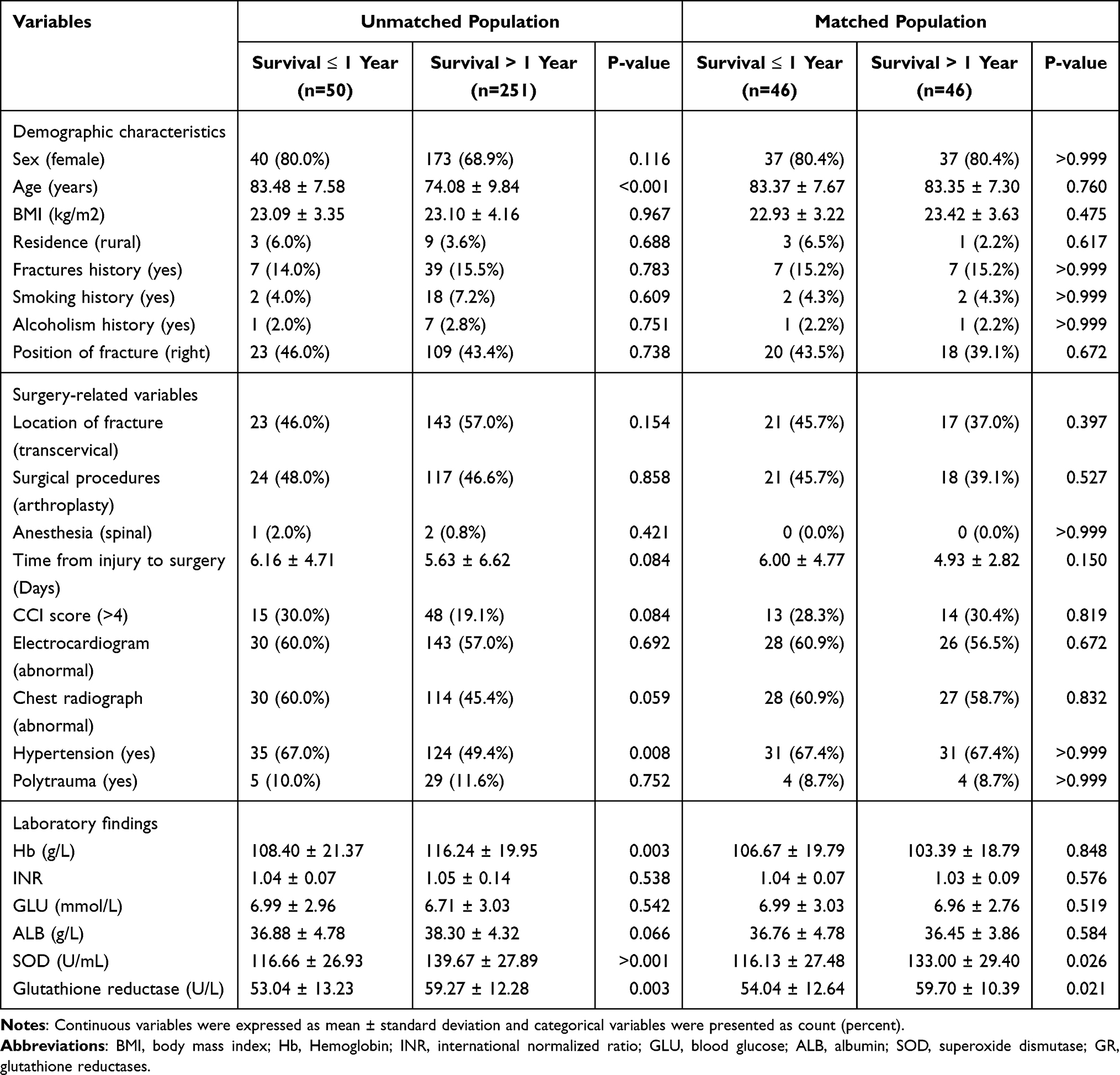 |
Table 1 Baseline Characteristics of Patients Grouped by the Status of 1-Year Survival for Unmatched and PSM Population |
PSM and Identification of Optimal Cutoff Points of SOD and GR
After PSM, there was no significant difference in covariables between the two groups (Table 1). As shown in the Figure 2A and B, in the PSM population, the levels of SOD of patients with more than 1-year survival were significantly higher than those with less than 1-year survival (p = 0.026, Figure 2A), as well as GR (p = 0.021, Figure 2B). To determine the most suitable cutoff points SOD and GR, ROC curves in the matched patients were established for SOD (area under the ROC curve, 0.635; p = 0.026; Figure 2C) and GR (area under the ROC curve, 0.640; p = 0.021; Figure 2D). According to Youden Index, the cutoff points of SOD and GR were 112.5 U/mL and 52.5 U/L, respectively. The patients with more than SOD levels of 112.5 U/mL were identified as high SOD while others as low SOD. Similarly, patients were also labeled as high GR and low GR according to GR of 52.5 U/L.
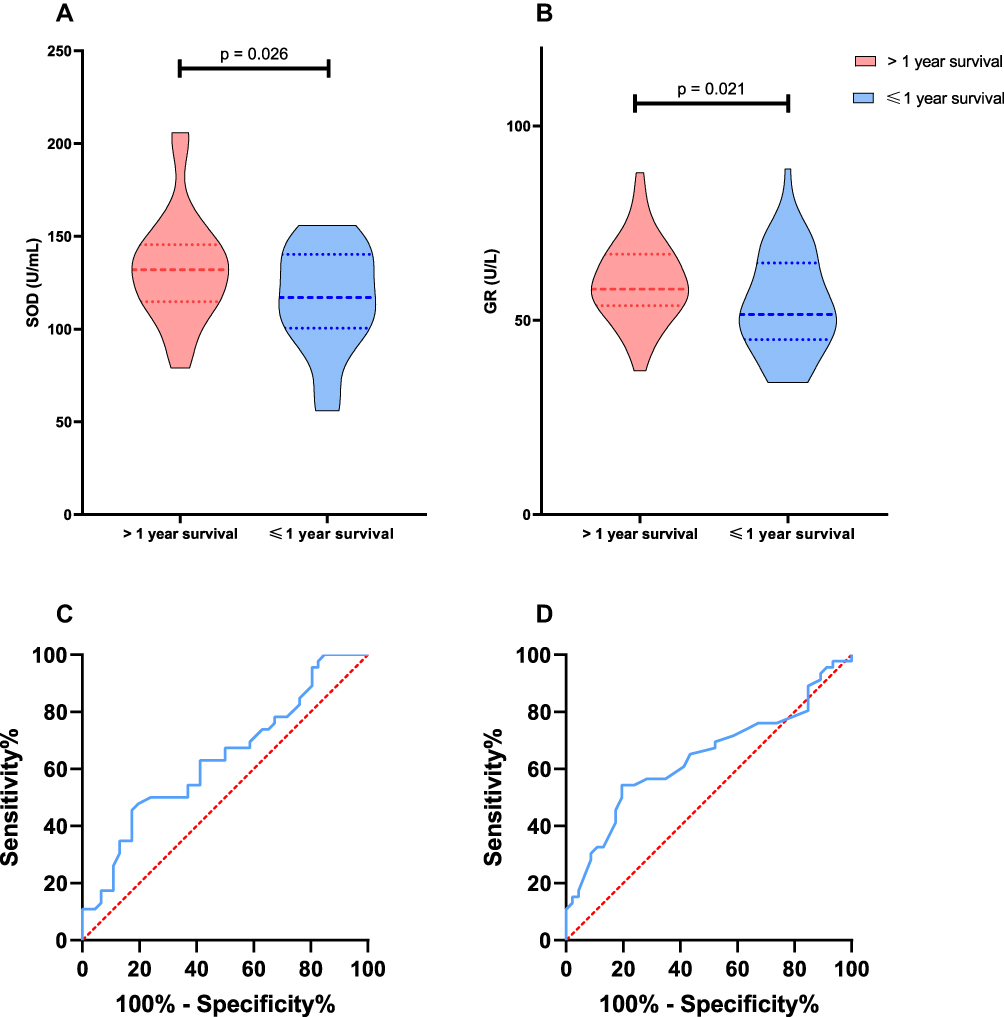 |
Figure 2 Serum levels of SOD and GR in the patients with Hip fracture after surgery grouped by one-year survival (A and B), and ROC curves of SOD and GR for one-year survival (C and D). (A and B) The patients who survived more than one year had significantly higher SOD levels (p = 0.026) than those who survived less than one year in the PSM population, as well as GR (p = 0.021); (C and D) Both SOD (AUROC: 0.635) and GR (AUROC: 0.640) were able to predict the 1-year survival according to the ROC curves. |
SOD and GR Were Risk Factors for Survival
Stepwise Regression showed that the tolerance between SOD and GR was 0.998 and the VIF (variance inflation factor) was 1.002, which suggested that there might be no multiple co-linear relationships between SOD and GR. Spearman correlation coefficient between SOD and GR was 0.045, which meant there was no significant correlation between SOD and GR. Four models were established based on Cox regression: Model 1 and Model 3 were adjusted for age, type of fracture, hypertension, Hb, CCI score, sex, time from injury to surgery, and ALB, while Model 2 and Model 4 were fully adjusted. Continuous SOD and GR were analyzed in Model 1 and Model 2 and grouped SOD and GR were included in Model 3 and Model 4. Model 1 and Model 3 were direct entry models while Model 2 and Model 4 were conditional stepwise forward models. As shown in Table 2, patients with higher SOD and GR may have decreased death risk. Patients with low SOD (≤112.5 U/mL) showed a 196.5% increase in death risk (HR = 2.965, CI: 1.605–5.476) in Model 3 and 169.0% (HR = 2.690, CI: 1.480–4.890) in Model 4. Similarly, death risk rose by 199.1% for patients with low GR in Model 3 (HR = 2.991, CI: 1.671–5.355) and 173.6% in Model 4 (HR = 2.736, CI: 1.563–4.792). The predictive value of all four models was measured and represented by C indices, and all models showed great prediction power (C indices: 0.832 for model 1; 0.822 for model 2; 0.831 for model 3; 0.821 for model 4; Supplementary Table 2). Survival probability between groups divided by different levels of SOD and GR was proved to be significantly different (For SOD groups: p < 0.001; For GR groups: p = 0.006). The patients with high SOD had significantly high survival probabilities than those with low SOD, as well as GR (Figure 3).
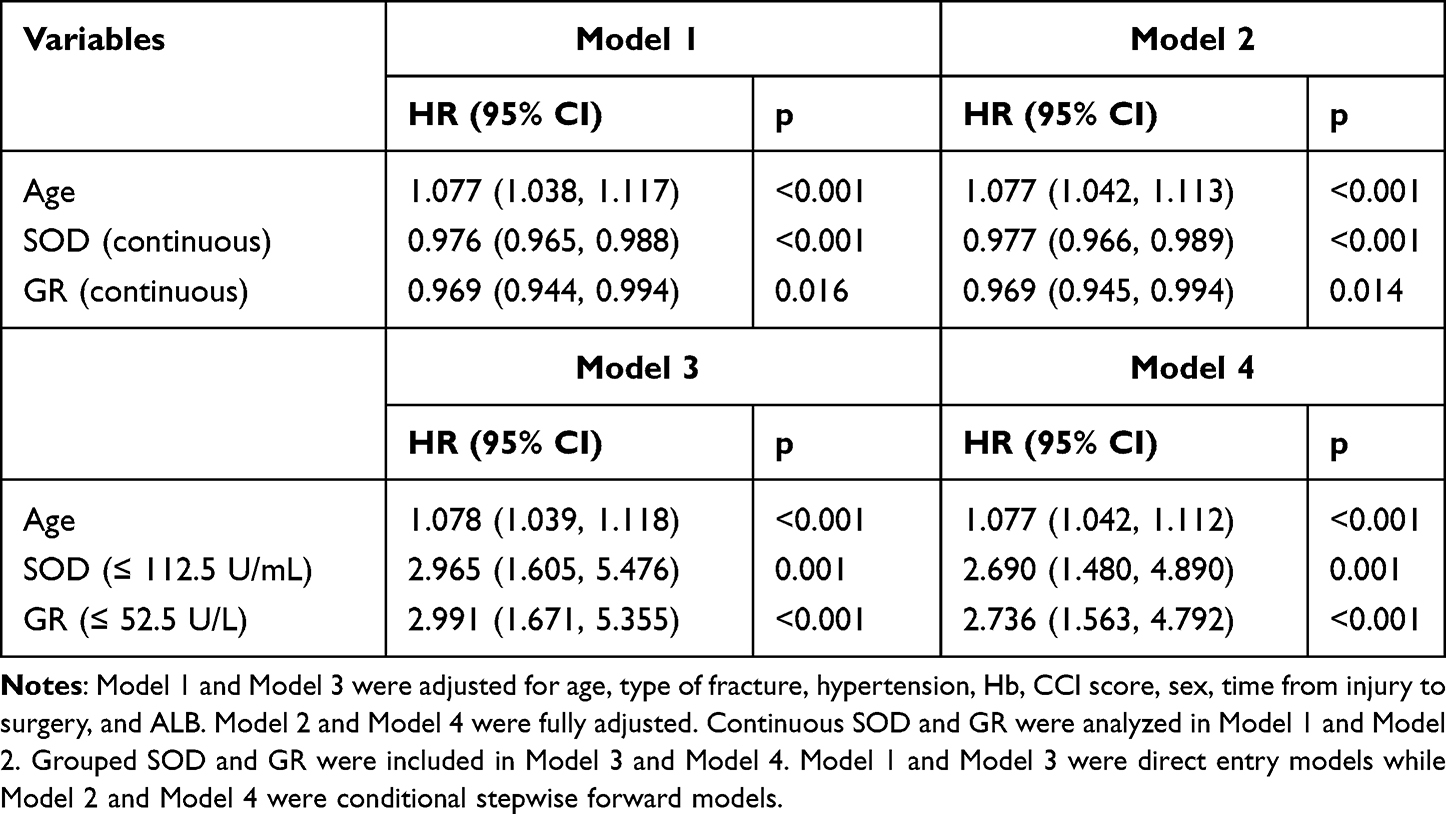 |
Table 2 Cox Regression Analyses of 1-Year Survival Adjusted for Different Factors |
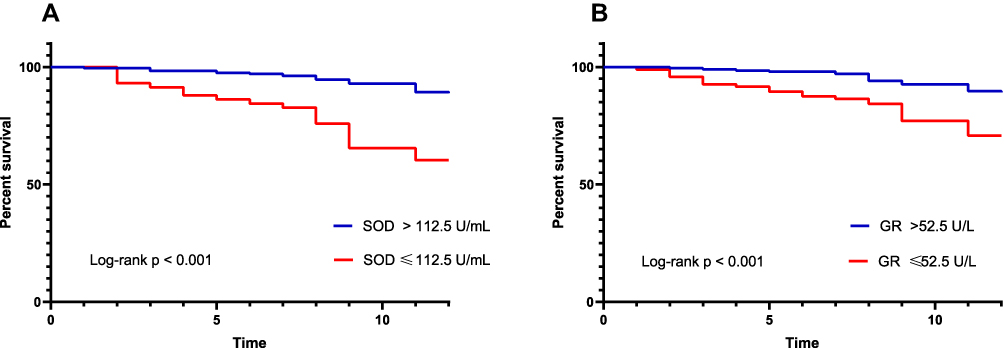 |
Figure 3 Kaplan–Meier analyses of one-year survival based on optimal serum levels of SOD (112.5 U/mL) and GR (52.5 U/L). (A) Kaplan–Meier analysis showed that SOD values of 112.5 U/mL significantly differentiated patients who died within one year and survived more than one year (p < 0.001), (B) SOD values of 52.5 U/L significantly differentiated patients who died within one year and survived more than one year (p < 0.001). |
Outcomes
Then, outcomes were compared between high SOD groups and low SOD groups, as well as between high GR groups and low GR groups, respectively. Patients in the high SOD group have significantly more favorable survival and walking abilities at 3 months, 6 months, and one year than patients in the low SOD group. Likewise, patients with high levels of GR showed a significantly higher survival rate and free walking ability rate at 3 months, 6 months, and 1 year compared with those with low levels of GR (Table 3). Outcomes of patients with intertrochanteric fractures and femoral neck fractures were also summarized in Supplementary Table 1. To further prove the prognosis value of SOD and GR, logistics models fully adjusted for survival and free walking ability at 6 months and 1 year were established by conditional stepwise forward methods and the results are shown in Table 4. As shown in Table 4, low SOD and low GR may be independent risk factors for 6-month survival, 1-year survival, 1-year free walking ability, and 1-year free walking ability (Table 4).
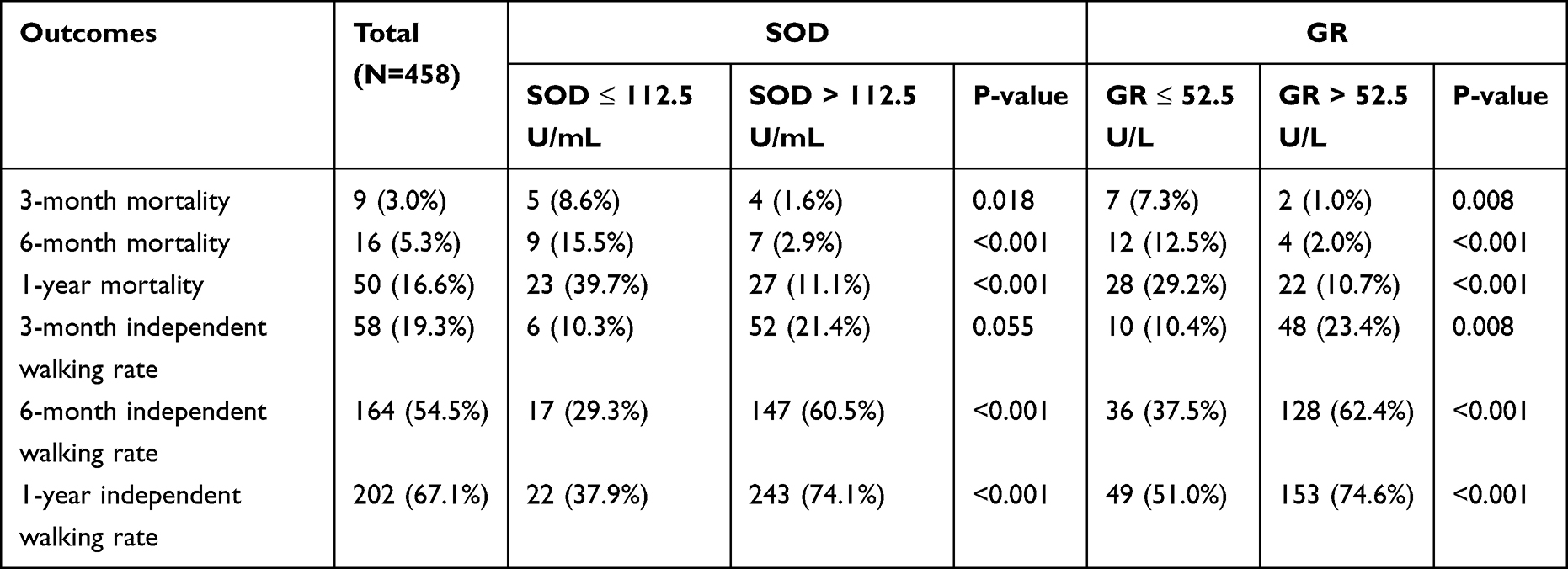 |
Table 3 Comparison of Outcomes of All Patients in Our Study |
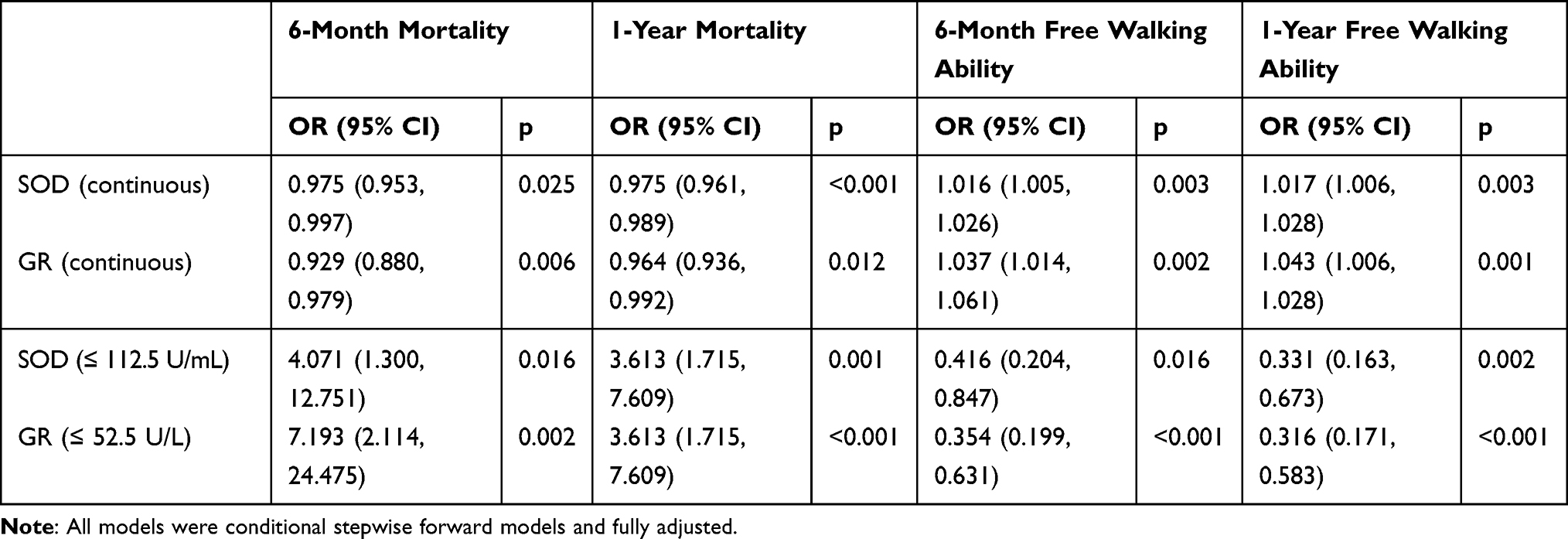 |
Table 4 Logistics Regression for Mortalities at 6 Months and 1 Year and Free Walking Abilities at 6 Months and 1 Year |
Discussion
In this study, we found that the patients with high SOD or GR may have a more favorable prognosis than those with low SOD or GR. In clinical practice, the predictive value of SOD and GR could be used for elderly patients. As we all know, many factors may impact the outcomes of patients with hip fractures, so PSM was performed to reduce the bias caused by co-factors, such as age, sex, fracture types, and as shown in Table 1, all basic features between groups did not differ significantly. The cutoff points according to the ROC curve in the population after PSM may have a better predictive value. GR may rise in the patients with severe liver disease, so the patients with severe liver disease were excluded to remove the impact of liver disease.18 Cox analyses also showed that SOD and GR, whether in continuous form or grouped form, were all associated with survival. The patients with higher SOD or GR seem to have less death risk. This result was also proved in logistics analysis.
SOD and GR are pivotal antioxidant enzymes that could defend our cells from the damage of oxidative stress. Many factors, including fractures, may result in increased oxidative damage via inflammatory pathways and so on, which may consume the efficiency of the antioxidant defense system.7,10 Therefore, we believe that the patients with high SOD or GR may have strong abilities to defend their bones from oxidative stress, and then are more likely to have a more satisfactory rehabilitation. Many studies had shown how the status of oxidative stress impacts bone remolding and bone healing. As we mentioned above, there are two types of cells involve the bone remolding: osteoblasts and osteoclasts. The oxidative stress affects bone metabolism by regulating the balance between osteoblasts and osteoclasts: oxidative stress could increase osteoclastogenesis and apoptosis of osteoblast and osteocyte, and decrease the activity of osteoblast and differentiation to the osteoblast cell lineage.19 It is proved that antioxidants can reduce the expression of the receptor activator of NF-kB ligand (RANKL) and increase the expression of osteoprotegerin,20 and osteoclastogenesis can be upregulated by increased RANKL and decreased osteoprotegerin.21 Animal studies have shown that oxidative stress induced by H2O2 can reduce osteoblast differentiation and decrease differentiation markers.22
Many population studies had suggested that populations with potent antioxidant status may have a better bone mass density (BMD) than those with oxidative stress status.23 In a recent study, the serum levels of RANKL, OPG, and 8-hydroxy-2-deoxyguanosine as the marker of oxidative stress were measured to explore the implication of oxidative stress in bone metabolism based on the populations of healthy people and patients with osteoporosis, and the positive and independent correlation between increased oxidative stress markers and the subgroup of osteoporosis was found.24 A study conducted in Japan showed that the markers of oxidative stress may predict hip fractures.25 However, if the oxidative markers can predict the outcomes of hip fractures has not been reported. Therefore, in our study, SOD and GR, as critical antioxidant enzymes, were used to explore whether patients with potent antioxidant status can have a favorable survival and walking ability.
There are some limitations to our study. First, as a retrospective single-center study, this study contended with the missing follow-up and unavailable data of SOD and GR. Next, the values of SOD and GR were extracted from the first laboratory test when patients were admitted to our department. The serum levels of SOD and GR may fluctuate, which may cause bias in our results. However, we believe the data of patients at the first time may better show the daily situation. Moreover, the types of fracture were divided into intertrochanteric fractures and femoral neck fractures instead of more strict classification such as OTA/AO classification. Lastly, there may be some potential co-factors that we did not include in our analysis. We believe our study may also indicate the relationship between SOD or GR and outcomes of hip fractures despite the limitations we mentioned above.
Low levels of SOD or GR may indicate poor antioxidant status and predict poor outcomes, so we may hypothesize that neutralizing oxidative stress may provide a better prognosis for our patients with hip fractures. Decreasing oxidative stress and increasing antioxidant ability may face the potent prospect of clinical application for improving the outcomes of hip fractures. Many studies based on animal models had reported the potential novel treatment of fractures by regulating the oxidative status. Ilyas et al developed a new biomaterial based on amorphous silicon oxynitride. This fracture healing material may release Si+4, which may enhance SOD and then stimulate osteogenesis.26 Many studies also reported the potential efficiency of SOD mimic in antioxidation.27,28 Many population studies showed that the patients with a higher intake of antioxidant nutrients may face a lower risk of hip fractures.29,30 Consistently, it was also reported that antioxidant vitamin E or C supplements may be associated with decreased bone resorption in nonsmoking postmenopausal women.31 However, few had demonstrated an effect of supplemental antioxidants on the prognosis of hip fractures. We look forward to proving the hypothesis through experimental population studies with a high level of evidence.
Conclusion
SOD and GR may be the independent risk factors for survival and walking abilities of hip fractures.
Data Sharing Statement
The data is unavailable because of the concern for patient privacy.
Ethics Approval and Informed Consent
This study was an observational study using the data of patients admitted to the Department of Traumatology, Shanghai East Hospital, Tongji University, School of Medicine, Shanghai, China. The study was performed according to the Declaration of Helsinki and was approved by the Institutional Ethics Committee of East Hospital. Written informed consent was obtained from all participants enrolled in this study.
Consent for Publication
We declare that all authors have seen and approved the final version of the manuscript being submitted and that all authors have confirmed that the details of any images, videos, recordings, etc can be published.
Funding
National Natural Science Foundation of China (Grant/Award Number:81971169). Shanghai Science and Technology Commission (Grant/Award Number: 20Y11901800).
Disclosure
The authors declare that no conflicts of interest exist in this work.
References
1. Groff H, Kheir MM, George J, Azboy I, Higuera CA, Parvizi J. Causes of in-hospital mortality after Hip fractures in the elderly. Hip Int. 2020;30(2):204–209. doi:10.1177/1120700019835160
2. Veronese N, Maggi S. Epidemiology and social costs of Hip fracture. Injury. 2018;49(8):1458–1460. doi:10.1016/j.injury.2018.04.015
3. Chiang MH, Huang YY, Kuo YJ, et al. Prognostic factors for mortality, activity of daily living, and quality of life in Taiwanese older patients within 1 year following hip fracture surgery. J Pers Med. 2022;12(1):102. doi:10.3390/jpm12010102
4. Simpson CR, Kelly HM, Murphy CM. Synergistic use of biomaterials and licensed therapeutics to manipulate bone remodelling and promote non-union fracture repair. Adv Drug Deliv Rev. 2020;160:212–233. doi:10.1016/j.addr.2020.10.011
5. Rohold CK, Lauritzen JB, Jørgensen HL. Causes of death among 93.637 Hip fracture patients- data based on the Danish National Registry of causes of death [published online ahead of print, 2021 Sep 30]. Eur J Trauma Emerg Surg. 2021. doi:10.1007/s00068-021-01791-0
6. Balogh E, Paragh G, Jeney V. Influence of iron on bone homeostasis. Pharmaceuticals. 2018;11(4):107. doi:10.3390/ph11040107
7. Terkawi MA, Matsumae G, Shimizu T, Takahashi D, Kadoya K, Iwasaki N. Interplay between Inflammation and pathological bone resorption: insights into recent mechanisms and pathways in related diseases for future perspectives. Int J Mol Sci. 2022;23(3):1786. doi:10.3390/ijms23031786
8. Jitca G, Osz BE, Tero-Vescan A, et al. Positive aspects of oxidative stress at different levels of the human body: a review. Antioxidants. 2022;11(3):572. doi:10.3390/antiox11030572
9. Cerqueni G, Scalzone A, Licini C, Gentile P, Mattioli-Belmonte M. Insights into oxidative stress in bone tissue and novel challenges for biomaterials. Mater Sci Eng C. 2021;130:112433.
10. Yang K, Cao F, Xue Y, Tao L, Zhu Y. Three classes of antioxidant defense systems and the development of postmenopausal osteoporosis. Front Physiol. 2022;13:840293. doi:10.3389/fphys.2022.840293
11. Wang Y, Branicky R, Noë A, Hekimi S. Superoxide dismutases: dual roles in controlling ROS damage and regulating ROS signaling. J Cell Biol. 2018;217(6):1915–1928. doi:10.1083/jcb.201708007
12. Lai Y, Li M, Liao X, Zou L. Smartphone-assisted colorimetric detection of glutathione and glutathione reductase activity in human serum and mouse liver using Hemin/G-Quadruplex DNAzyme. Molecules. 2021;26(16):5016. doi:10.3390/molecules26165016
13. Zhou Q, Zhu L, Zhang D, et al. Oxidative stress-related biomarkers in postmenopausal osteoporosis: a systematic review and meta-analyses. Dis Markers. 2016;2016:7067984. doi:10.1155/2016/7067984
14. Zhao F, Guo L, Wang X, Zhang Y. Correlation of oxidative stress-related biomarkers with postmenopausal osteoporosis: a systematic review and meta-analysis. Arch Osteoporos. 2021;16(1):4. doi:10.1007/s11657-020-00854-w
15. De Geest B, Mishra M. Role of Oxidative Stress in Diabetic Cardiomyopathy. Antioxidants. 2022;11(4):784. doi:10.3390/antiox11040784
16. Lyall R, Nikoloski Z, Gechev T. Comparative analysis of ROS network genes in extremophile eukaryotes. Int J Mol Sci. 2020;21(23):9131. doi:10.3390/ijms21239131
17. Nakajo K, Abe S, Oda I, et al. Impact of the Charlson comorbidity index on the treatment strategy and survival in elderly patients after non-curative endoscopic submucosal dissection for esophageal squamous cell carcinoma: a multicenter retrospective study. J Gastroenterol. 2019;54(10):871–880. doi:10.1007/s00535-019-01583-9
18. Prigge JR, Coppo L, Martin SS, et al. Hepatocyte hyperproliferation upon liver-specific co-disruption of thioredoxin-1, thioredoxin reductase-1, and glutathione reductase. Cell Rep. 2017;19(13):2771–2781. doi:10.1016/j.celrep.2017.06.019
19. Kimball JS, Johnson JP, Carlson DA. Oxidative Stress and Osteoporosis. J Bone Joint Surg Am. 2021;103(15):1451–1461. doi:10.2106/JBJS.20.00989
20. Zhang J, Lazarenko OP, Kang J, et al. Feeding blueberry diets to young rats dose-dependently inhibits bone resorption through suppression of RANKL in stromal cells. PLoS One. 2013;8(8):e70438. doi:10.1371/journal.pone.0070438
21. Fontani F, Marcucci G, Iantomasi T, Brandi ML, Vincenzini MT. Glutathione, N-acetylcysteine and lipoic acid down-regulate starvation-induced apoptosis, RANKL/OPG ratio and sclerostin in osteocytes: involvement of JNK and ERK1/2 signalling. Calcif Tissue Int. 2015;96(4):335–346. doi:10.1007/s00223-015-9961-0
22. Bai XC, Lu D, Bai J, et al. Oxidative stress inhibits osteoblastic differentiation of bone cells by ERK and NF-kappaB. Biochem Biophys Res Commun. 2004;314(1):197–207. doi:10.1016/j.bbrc.2003.12.073
23. Sendur OF, Turan Y, Tastaban E, Serter M. Antioxidant status in patients with osteoporosis: a controlled study. Joint Bone Spine. 2009;76(5):514–518. doi:10.1016/j.jbspin.2009.02.005
24. Cervellati C, Romani A, Cremonini E, et al. Higher urinary levels of 8-Hydroxy-2’-deoxyguanosine are associated with a worse RANKL/OPG ratio in postmenopausal women with osteopenia. Oxid Med Cell Longev. 2016;2016:6038798. doi:10.1155/2016/6038798
25. Yang S, Feskanich D, Willett WC, Eliassen AH, Wu T. Association between global biomarkers of oxidative stress and Hip fracture in postmenopausal women: a prospective study. J Bone Miner Res. 2014;29(12):2577–2583. doi:10.1002/jbmr.2302
26. Ilyas A, Odatsu T, Shah A, et al. Amorphous silica: a new antioxidant role for rapid critical-sized bone defect healing. Adv Healthc Mater. 2016;5(17):2199–2213. doi:10.1002/adhm.201600203
27. Li L, Tovmasyan A, Sheng H, et al. Fe Porphyrin-based SOD Mimic and redox-active compound, (OH)FeTnHex-2-PyP4+, in a Rodent Ischemic Stroke (MCAO) model: efficacy and pharmacokinetics as compared to its Mn Analogue, (H2O)MnTnHex-2-PyP5+. Antioxidants. 2020;9(6):467. doi:10.3390/antiox9060467
28. Mathieu E, Bernard AS, Quévrain E, et al. Intracellular location matters: rationalization of the anti-inflammatory activity of a manganese(ii) superoxide dismutase mimic complex. Chem Commun. 2020;56(57):7885–7888. doi:10.1039/D0CC03398G
29. Hantikainen E, Grotta A, Ye W, et al. Prospective study of dietary Non Enzymatic Antioxidant Capacity on the risk of Hip fracture in the elderly. Bone. 2016;90:31–36. doi:10.1016/j.bone.2016.05.006
30. Sun LL, Li BL, Xie HL, et al. Associations between the dietary intake of antioxidant nutrients and the risk of Hip fracture in elderly Chinese: a case-control study. Br J Nutr. 2014;112(10):1706–1714. doi:10.1017/S0007114514002773
31. Pasco JA, Henry MJ, Wilkinson LK, Nicholson GC, Schneider HG, Kotowicz MA. Antioxidant vitamin supplements and markers of bone turnover in a community sample of nonsmoking women. J Womens Health. 2006;15(3):295–300. doi:10.1089/jwh.2006.15.295
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.