")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 11
Successful recruitment and retention strategies for women health volunteers: viewpoints of the volunteers' supervisors and relevant researchers
Authors Rezakhani Moghaddam H , Allahverdipour H, Matlabi H
Received 17 July 2018
Accepted for publication 21 August 2018
Published 26 October 2018 Volume 2018:11 Pages 621—634
DOI https://doi.org/10.2147/JMDH.S180544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hamed Rezakhani Moghaddam, Hamid Allahverdipour, Hossein Matlabi
Department of Health Education and Promotion, Faculty of Health Sciences, Tabriz University of Medical Sciences, Tabriz, Iran
Background: Women health volunteers (WHVs) are a link between people and healthcare workers. Despite their key role in promoting community health, strategies are rarely designed to keep them volunteering. The aim of this research was to find successful strategies to overcome barriers to recruitment and retention of the volunteers in assigned activities.
Subjects and methods: A three-round online national Delphi technique was used to ask the opinions of Iranian health volunteers’ supervisors and the relevant researchers. At the first round, the participants were asked ten open-ended questions across four barriers: inadequate capability of the volunteers and trainers, inadequate acceptance of the volunteers, restrictive social norms, and organizational problems. At the second round, with the questionnaire consisting of closed-ended questions, the experts were asked to rank the feasibility of each strategy using a seven-point Likert scale. Items along with the feedback received from the second round were included in the third-round questionnaire. Strategies with a median of 6 or higher and with an interquartile range ≤1 were regarded to be feasible.
Results: Consensus was obtained on 100 of the 133 strategies. A mixture of improving group work, implementing motivation tactics, assessing the needs of people/WHVs, reforming policy, monitoring and evaluation of WHVs/trainers, mobilizing the community, empowering WHVs/trainers, rationalizing WHVs/trainers/ people, improving intersectional collaboration, implementing problem-based approaches, allocating proper resources, appropriate recruitment of WHVs, using social networks, and information dissemination were found to be the effective strategies to overcome the barriers to active participation.
Conclusion: The highest consensuses among experts were on implementing motivation tactics and mobilizing the community. It seems that community mobilization, incentives, and logistical supplies such as providing prizes and transportation facilities for volunteers are mechanisms that can help retain WHVs and also overcome barriers to their active participation.
Keywords: health volunteers, Delphi technique, consensus, community health, retention strategies
Introduction
The new primary healthcare approach emphasizes strengthening of social participation to promote health.1 Community participation is a process by which people are actively and effectively involved in determining issues, deciding on the factors influencing their lives, formulating and implementing policies, designing, developing and delivering services, and trying to achieve changes.2 As a consequence of these changes, an empowered and developed community can be established.3 People’s participation in diagnosing and identifying health problems leads to improvement in health service coverage, increase in community health literacy,4 social learning, increase in knowledge and skills,5 and reduction in employee absenteeism.6 Involvement of the community in health developing activities can also be done through voluntary work or community-based activities.7 Many governments strengthen their health system by using voluntary actions.8
For these reasons, in 1990, the Ministry of Health and Medical Education of Iran developed the women health volunteers (WHVs) initiative nationwide.9 Inside the program, volunteers are the people living in a geographic area covered by a health center, who are familiar with the culture and customs of the society. WHVs recruited those women who voluntarily took part in community health activities including attending training sessions, educating health issues, updating demographics, and following up the covered 50 households.10
Health volunteers contributed to disease control, public health promotion,11 oral health improvement,12 and an increase in childhood immunization as well as breastfeeding rates13 in different countries worldwide. Similarly, in Iran, the evaluation and survey of the WHV program showed that their activities contributed in improving individual and community health.5 In general, health volunteers can play an effective role in empowering the community due to ongoing communication with families and cultural, economic, and social similarities with the community members.14
Nevertheless, studies showed that the lack of transportation facilities, negative attitude of the community members toward volunteering, lack of community support, lack of effective supervision, multiple chronic difficulties, geographic limitations, literacy limitations, limitations of professional respect on behalf of health care workers to health volunteers, and inadequate training were particularly the important barriers to health volunteers’ active participation.15–18 In Iran, these challenges were mainly categorized as lack of familiarity with the program, lack of incentives, and disregarding the needs of WHVs.9 Furthermore, Vizeshfar et al determined the challenges faced by WHVs, including role confusion, ineffective training program, lack of good reputation among people, and inability to communicate with, and therefore teach, as barriers to the active participation of Iranian health volunteers.19 As a result, many health volunteers have been inactive to do their duties in recent years.20
Although various strategies have been used to overcome barriers to the active participation of health volunteers worldwide,21,22 various evidences have shown that WHVs initiatives are basically culture oriented. In this case, the intervention approach has to be based on the culture and contexts of the community in which the researchers, healthcare workers, and program supervisors have to collaborate with each other to present suitable and executable strategies.8 Therefore, the aim of this study was to identify feasible strategies to overcome perceived barriers to the active participation of WHVs utilizing national Delphi technique.
Subjects and methods
An online national three-round Delphi technique was used to identify strategies to overcome barriers to the participation of WHVs. The steps and procedure are briefly presented in Table 1.
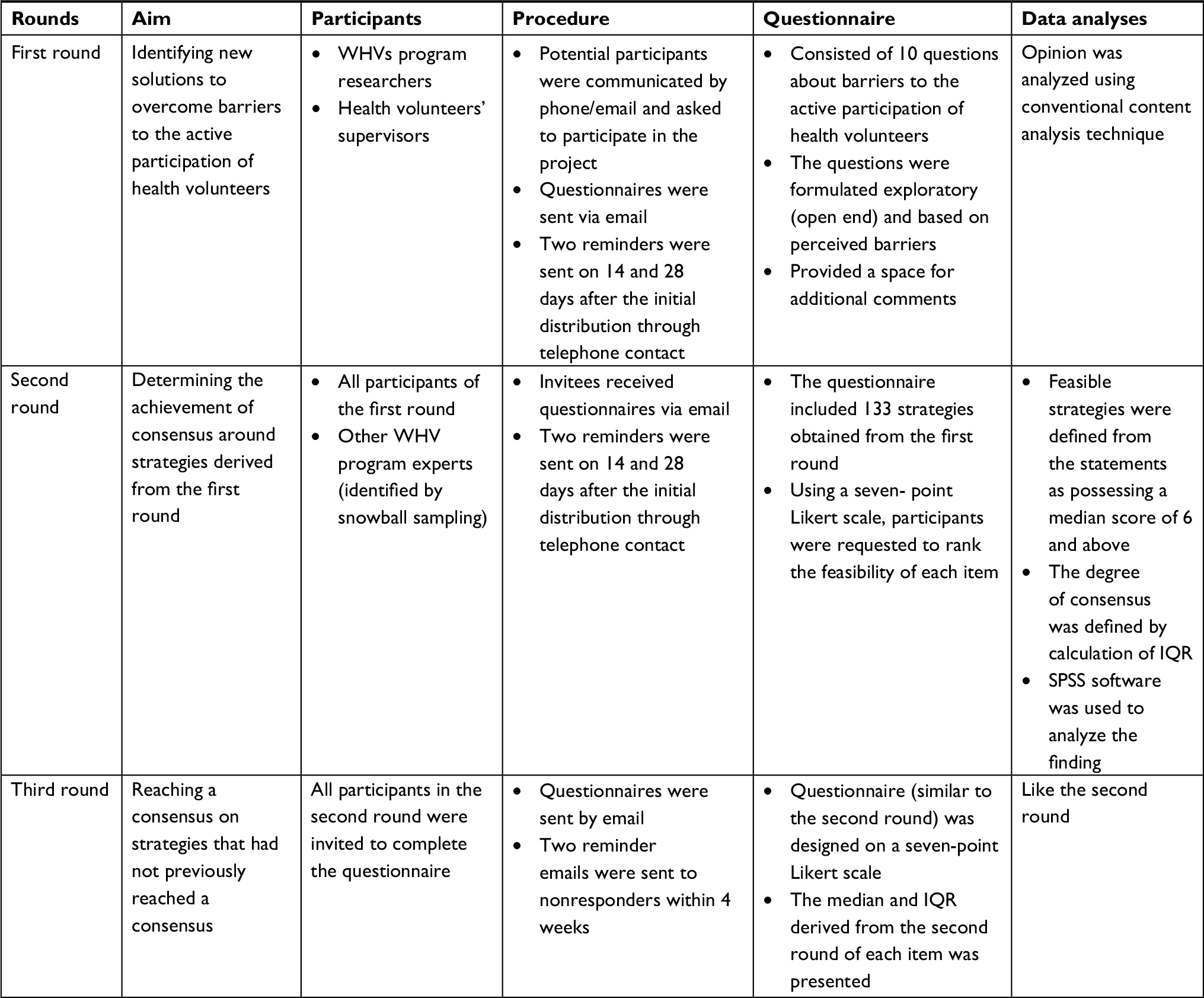 | Table 1 The methods and process of implementing the study Abbreviations: WHV, women health volunteer; IQR, interquartile range. |
Round 1
Aim
The aim of the first step was to identify prospective solutions to overcome barriers to the active participation of health volunteers.
Participants and procedure
A list of authors of 40 scientific articles relevant to WHVs and their supervisors was provided in cooperation with the Ministry of Health and Medical Education. Based on purposive sampling, eligible participants were chosen if they had at least a couple of years of experience in the WHVs program, had at least a bachelor’s degree, and had published scholarly articles. Potential participants were contacted by phone/email and were requested to participate in the project. The questionnaire was sent via email and the participants were asked to express their ideas about how to overcome the barriers to the active participation of health volunteers. Two telephone reminders were attempted on 14 and 28 days after the initial distribution.
Questionnaire
The questionnaire items were obtained from the first phase of a qualitative study.10 Barriers to the active participation of health volunteers were categorized into “inadequate capability of the volunteers and trainers”, “inadequate acceptance of the volunteers”, “restrictive social norms”, and “organizational problems”. Also, the subthemes included “volunteers’ inadequate knowledge, trainers’ inadequate skills, inefficient communication, not taking care of the population covered by the, program, organizational distrust, unrealistic expectations and systemic confusion, escaping and denial of responsibility, lack of motivation and organizational support, and educational failure”. Based on perceived barriers, the questionnaire consisted of ten open-ended queries. Each barrier was explained, and then, the participant was asked to report at least five strategies to overcome it. The last section of the questionnaire provided a space for additional comments.
Round 2
Aim
The aim of this round was to achieve consensus among specialists on the strategies derived from the first round.
Participants and procedure
All participants of the first round were requested to take part. In addition, snowball sampling was implemented to recruit other potential experts. The received questionnaires were demanded to rate the feasibility of each strategy.
Questionnaire
A questionnaire was developed to identify existing obstacles’ solutions. Each barrier was explained first, and then, the suggested strategies were presented. Finally, the questionnaire included 133 strategies. Using a seven-point Likert scale (from 1=low feasibility to 7=high feasibility), participants were requested to score the feasibility rate for each item.
Round 3
Aim
The aim was to obtain consensus over strategies that had not been obtained previously.
Participants and procedure
All participants in the second round were invited to complete the questionnaire. Two reminder emails were sent to nonresponders within 4 weeks.
Questionnaire
Similar to the second round questionnaire, the items were designed on a seven-point Likert scale. In addition, the median and interquartile range (IQR) of each item derived from the second round were presented. Participants were asked to review their responses again and revise their opinions and judgments if needed. Finally, the experts were asked to rerate strategies based on the IQR and median score of each strategy.
Data analyses
Round 1
Data analysis was done using the conventional content analysis method. Therefore, a six-step process of thematic analysis was used.23 After collecting experts’ responses, two researchers independently reviewed the proposed responses and identified themes. Any disagreement was discussed carefully and then adjusted with other research team members’ opinions. MAXQDA v.12 software was used to manage the data.
Rounds 2 and 3
Data were analyzed by calculating the median; a median score of ≥6 indicated a “feasible” or “very feasible” strategy. The degree of consensus was defined by calculating the IQR (the distance between the 25th and the 75th percentiles). An IQR value of 1.00 indicated that 50% of all the rankings listed by the participants were located within one point on the scale and was considered as indicative of a high degree of consensus.24 We wanted to identify which group played a more important role in no-consensus items statistically. Therefore, the Mann–Whitney U test was used to compare the opinions of health volunteers’ supervisors and researchers on nonconsensus strategies applying SPSS software because the distribution was not normal. The consolidated criteria for reporting qualitative research were used in presentation of the study results.25
Ethics and consent
This study was approved by the Ethical Review Committee of the Tabriz University of Medical Sciences (IR. TBZMED; REC: 1395-1038). The participant had to fill out the online informed consent which explained the aims, reasons for doing the research, the method, and keeping responses confidential, and the procedures of the study.
Results
In order to identify feasible strategies to overcome perceived barriers to the active participation of WHVs through national Delphi technique, a total of 42 specialists including 26 health volunteers’ supervisors and 16 researchers were invited to participate in the current study. The response rates for the first, second, and third rounds were 90%, 81.57%, and 78.94%, respectively. Overall, 10 (24%) were male and 32 (76%) were female. The experts were aged 27–51 years (M=35.23, SD=6.65). Experts’ field of study included educational administration (n=6, 14%), public health (n=22, 52%), health education and health promotion (n=10, 24%), and family health (n=4, 10%).
At the first round, results of the study revealed that the 133 suggested strategies to overcome barriers to participation of WHVs were categorized into 14 themes including empowering WHVs/trainers, allocating proper resources, assessing the needs of people/WHVs, improving group work, implementing problem-based approaches, using social networks, appropriate recruitment of WHVs, implementing motivation tactics, improving intersectional collaboration, reforming policy, information dissemination, monitoring and evaluation of WHVs/trainers, rationalizing WHVs/trainers/ people, and mobilizing the community. Participants at the second and third rounds reached consensus over 81 and 100 items. In the following sections, the suggested strategies are reported through questions.
Q.1. What is needed to increase the knowledge of health volunteers?
A good consensus was gained about empowering WHVs/trainers to increase the knowledge of health volunteers. Furthermore, allocating proper resources, assessing needs of people/WHVs, and improving group work were consensually approved. No consensus was obtained on five strategies (Table 2).
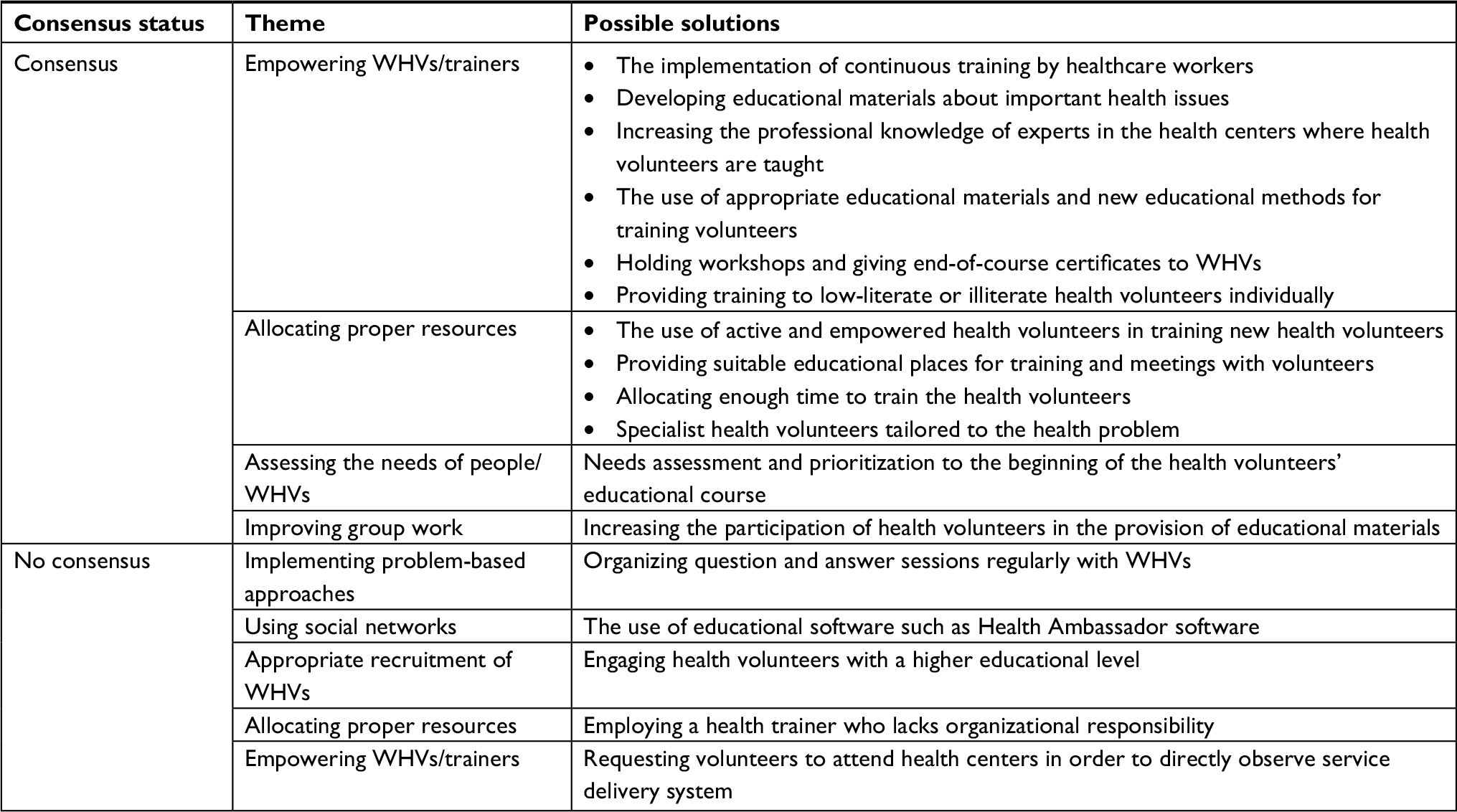 | Table 2 Strategies for inadequate knowledge of volunteers: Q.1. What is needed to increase the knowledge of health volunteers? Abbreviations: Q, question; WHV, women health volunteer. |
Q.2. What do you believe are contributors to the adequate skills of the volunteers/trainers?
The highest consensus was about allocating proper resources. Other themes included implementing motivation tactics, improving group work, and empowering WHVs/trainers. However, lack of consensus was found for about five items related to implementing motivation tactics, allocating proper resources, and empowering WHVs/trainers (Table 3).
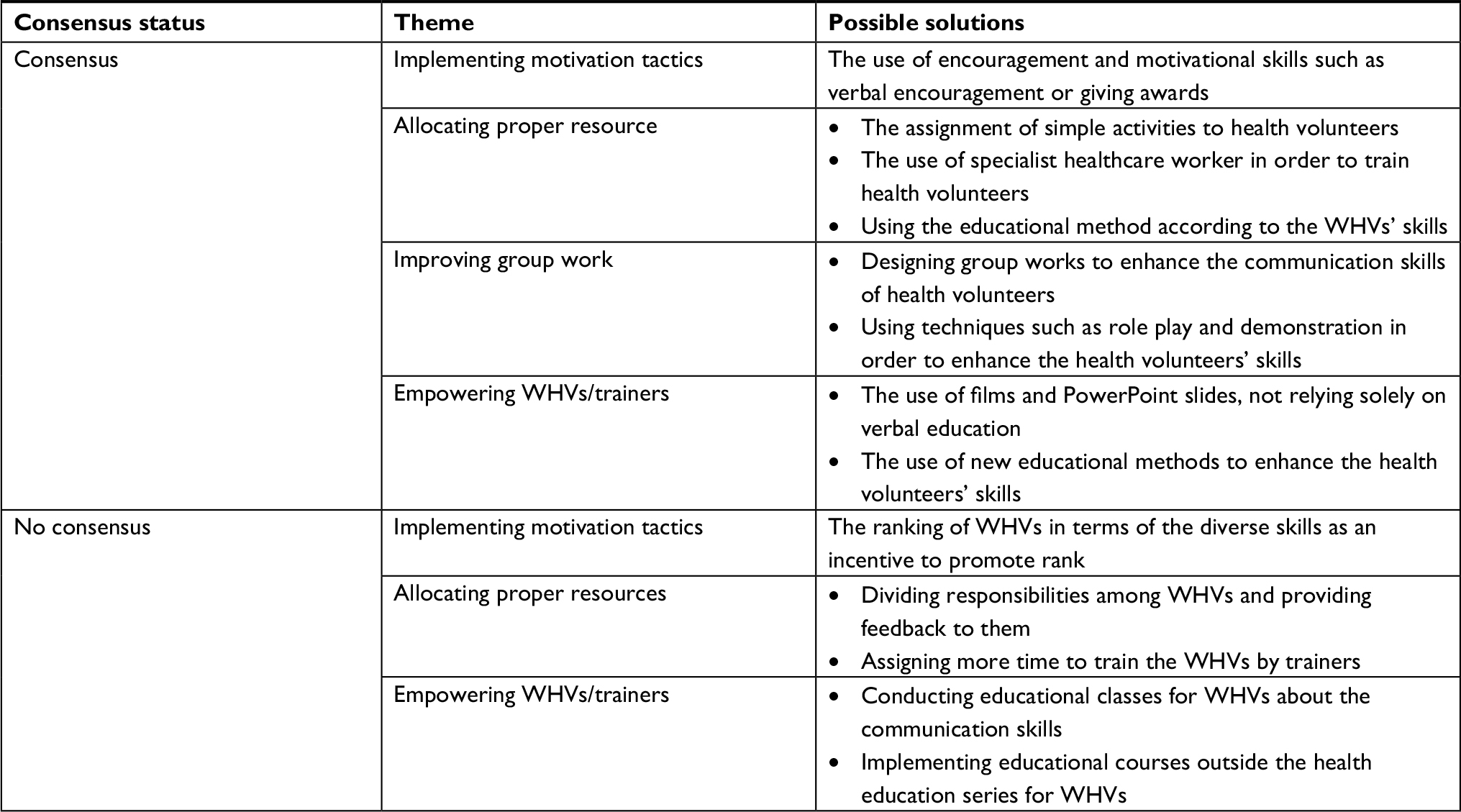 | Table 3 Strategies for inadequate skills of the volunteers/trainers: Q.2. What do you believe are contributors to the adequate skills of the volunteers/trainers? Abbreviations: Q, question; WHV, women health volunteer. |
Q.3. Which intervention approaches are needed to improve people’s cooperation with WHVs program?
Most of the panelists recommended community-based interventions to improve people’s cooperation with WHVs program, mainly with a consensus about mobilizing the community. Other consensus strategies included information dissemination, reforming policy, improving intersectional collaboration, and assessing the needs of people/WHVs. Conversely, there was no consensus over strategies related to empowering WHVs/trainers and rationalizing WHVs/trainers/people (Table 4).
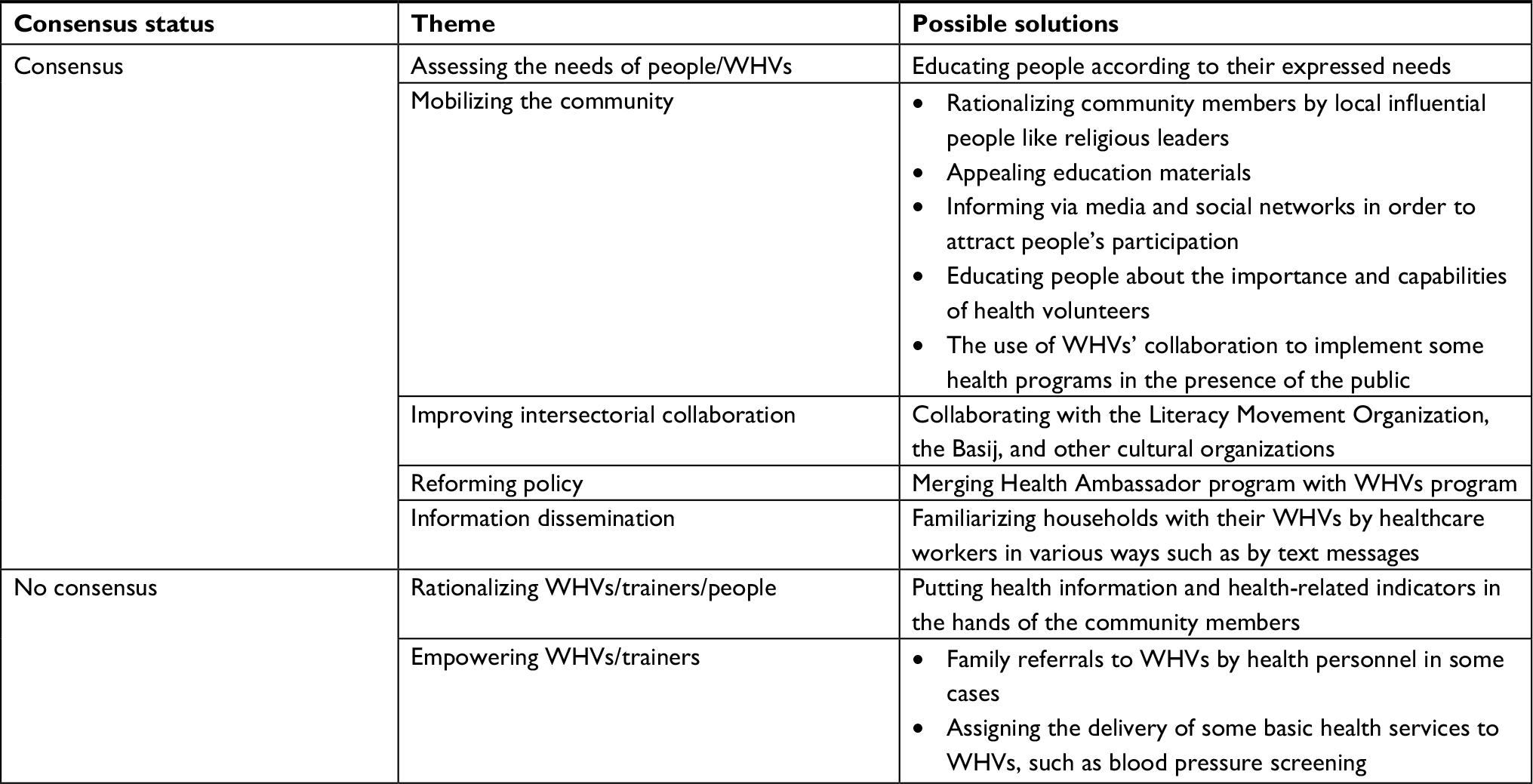 | Table 4 Strategies for not taking care of the population covered by the program: Q.3. Which intervention approaches are needed to improve people’s cooperation with WHVs program? Abbreviations: Q, question; WHV, women health volunteer. |
Q.4. What strategies may be effective on inefficient communication in WHVs program?
Consensus was obtained on the feasibility of all suggested strategies, except for empowering WHVs/trainers and allocating proper resources (Table 5).
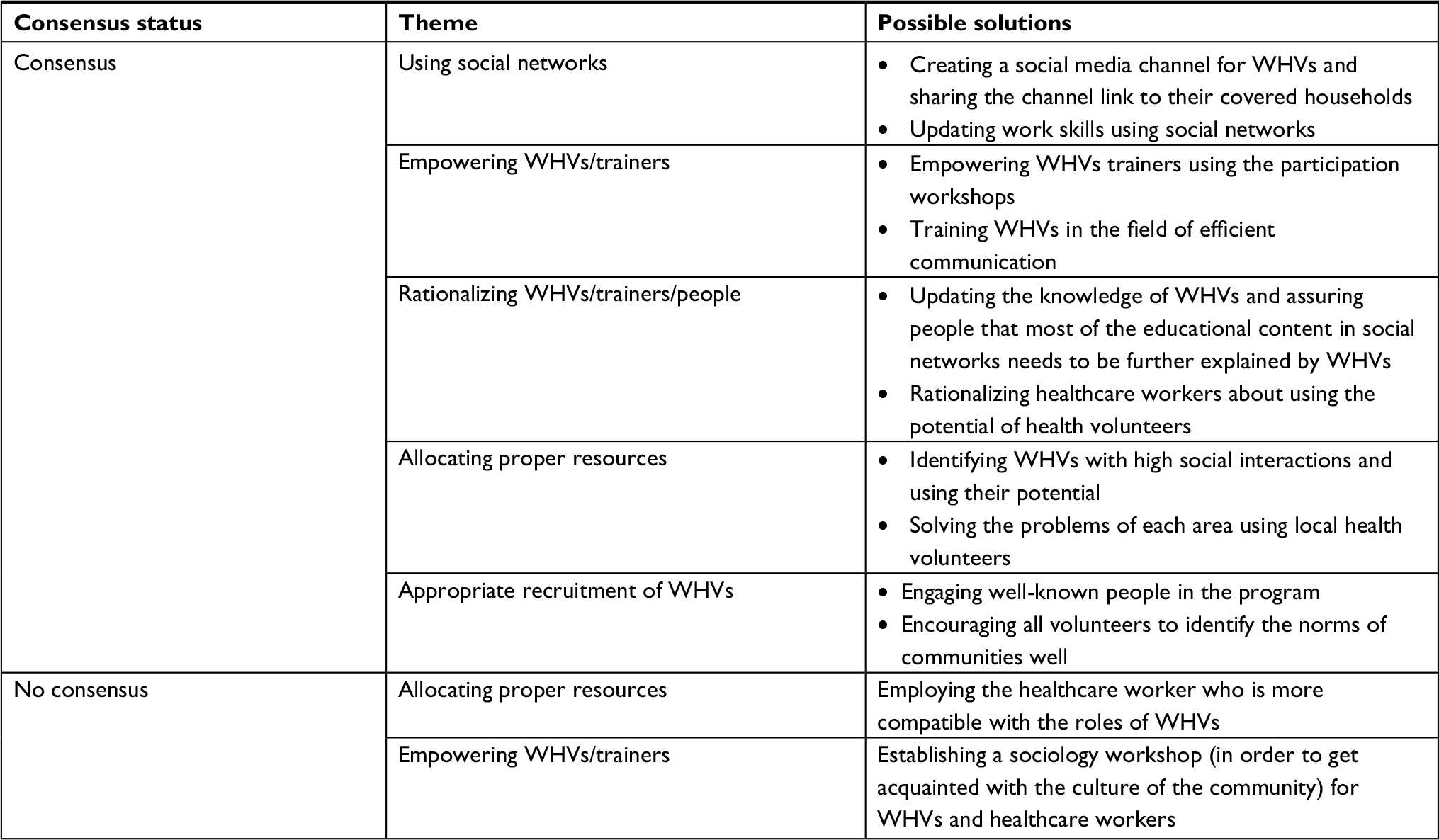 | Table 5 Strategies for inefficient communication: Q.4. What strategies may be effective on inefficient communication in WHVs program? Abbreviations: Q, question; WHV, women health volunteer. |
Q.5. How could social norms be better to improve the active participation of WHVs?
Most panelists agreed on the use of interventions associated with mobilizing the community, problems’ attentiveness, allocating proper resources, rationalizing WHVs/trainers/people, and reforming policy to overcome social norms barriers. Two strategies related to mobilizing the community and rationalizing WHVs/trainers/people had median scores of 5 and were not regarded to be feasible (Table 6).
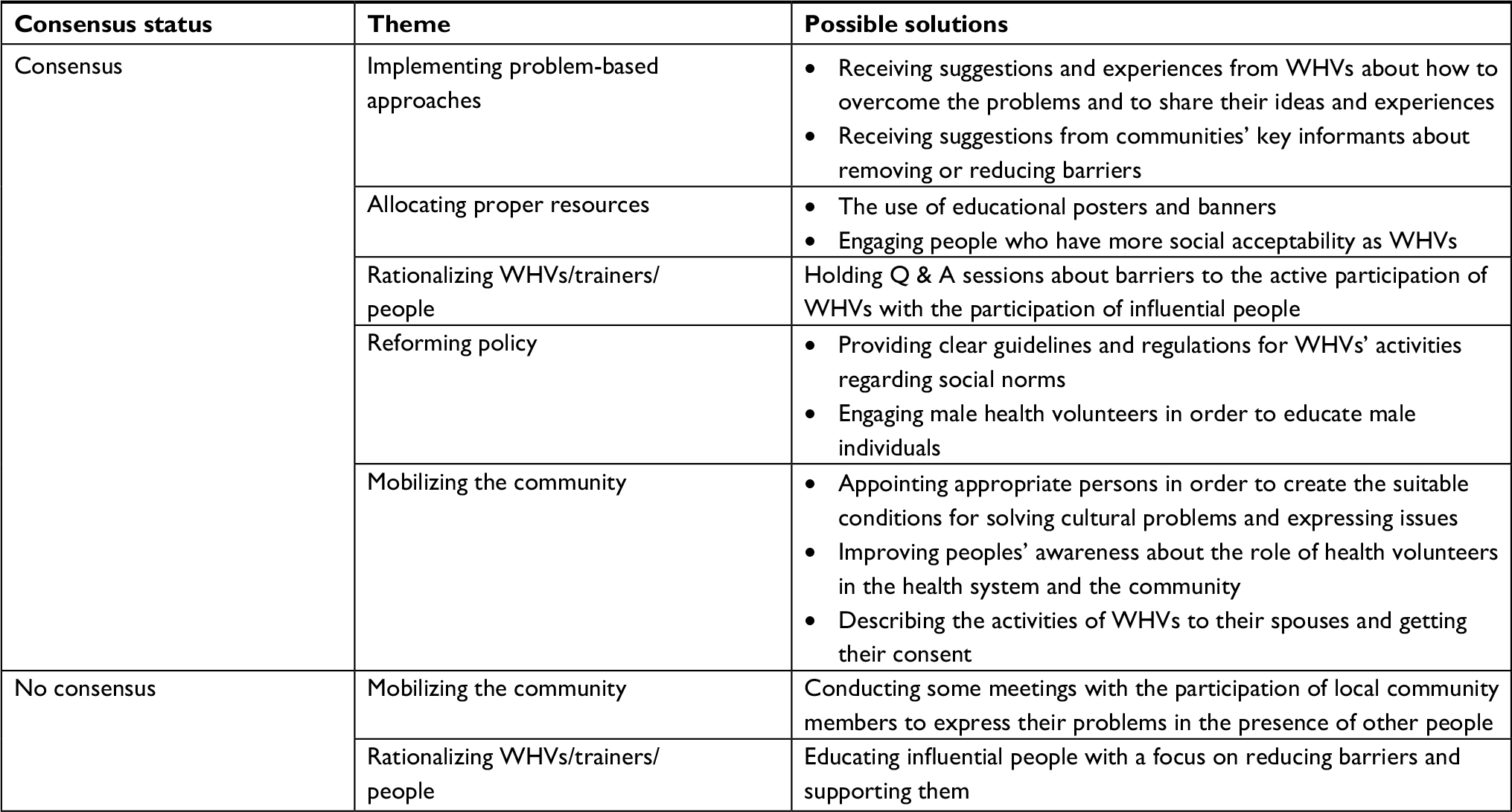 | Table 6 Strategies for restrictive social norms: Q.5. How could social norms be better to improve the active participation of WHVs? Abbreviations: Q, question; Q & A, question and answer; WHV, women health volunteer. |
Q.6. Which interventions are needed to reduce organizational distrust?
Experts agreed that the executive interventions should include reforming policy, improving intersectional collaboration, empowering WHVs/trainers, and allocating proper resources. Three strategies were disagreed for being feasible in reducing organizational distrust. These items were categorized as appropriate recruitment of WHVs, reforming policy, and monitoring and evaluation of WHVs/trainers (Table 7).
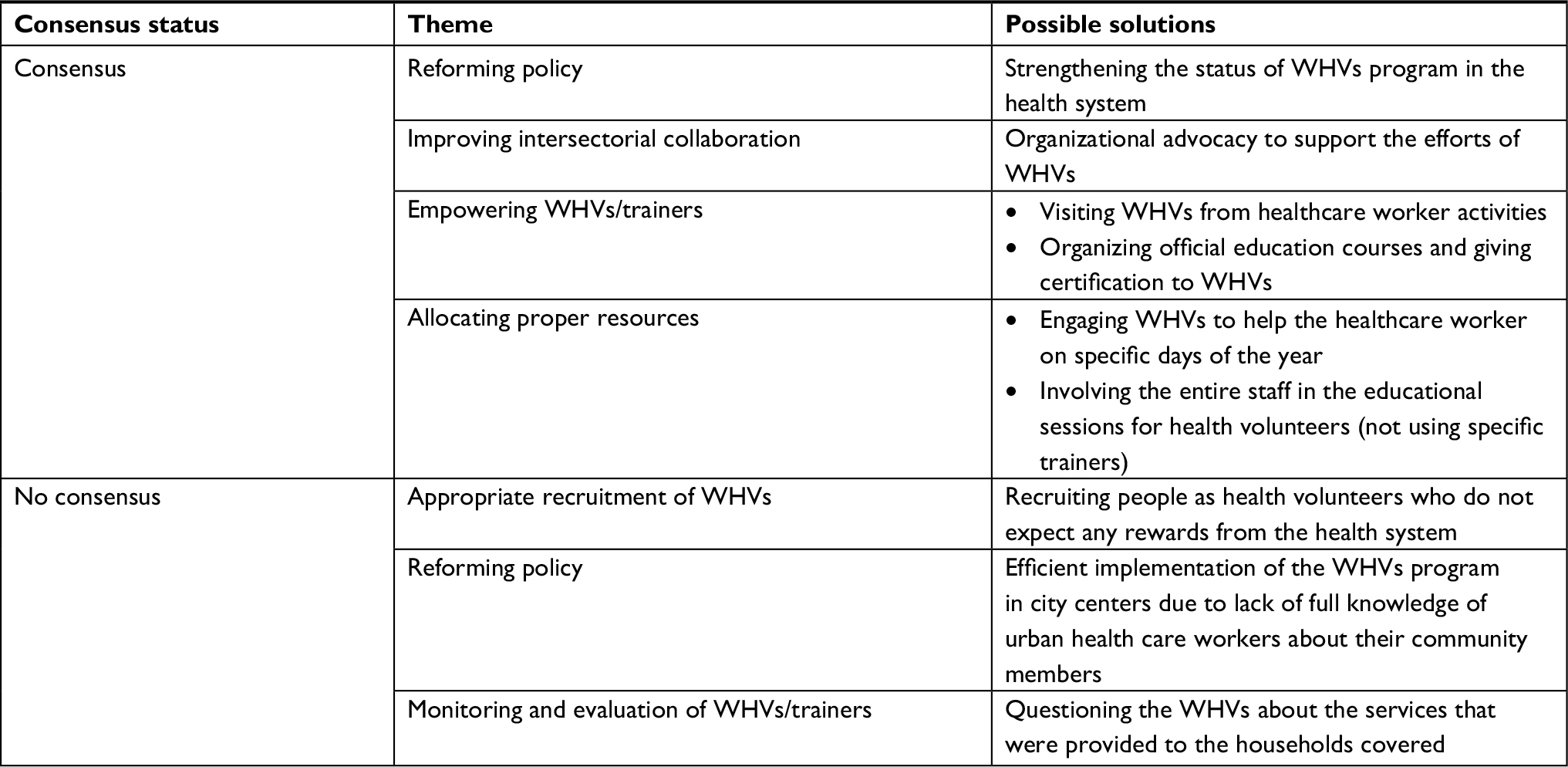 | Table 7 Strategies for organizational distrust: Q.6. Which interventions are needed to reduce organizational distrust? Abbreviations: Q, question; WHV, women health volunteer. |
Q.7. Which intervention approaches to reduce systemic confusion are most likely to succeed?
A high consensus was achieved on reforming policy. In addition, the five items that emphasized the implementation of short-/medium-term strategies included implementing problem-based approaches, rationalizing WHVs/trainers/people, information dissemination, assessing the needs of people/WHVs, and allocating proper resources. However, no consensus was obtained on three strategies related to rationalizing WHVs/trainers/people, reforming policy, and allocating proper resources as intervention approaches to reduce systemic confusion (Table 8).
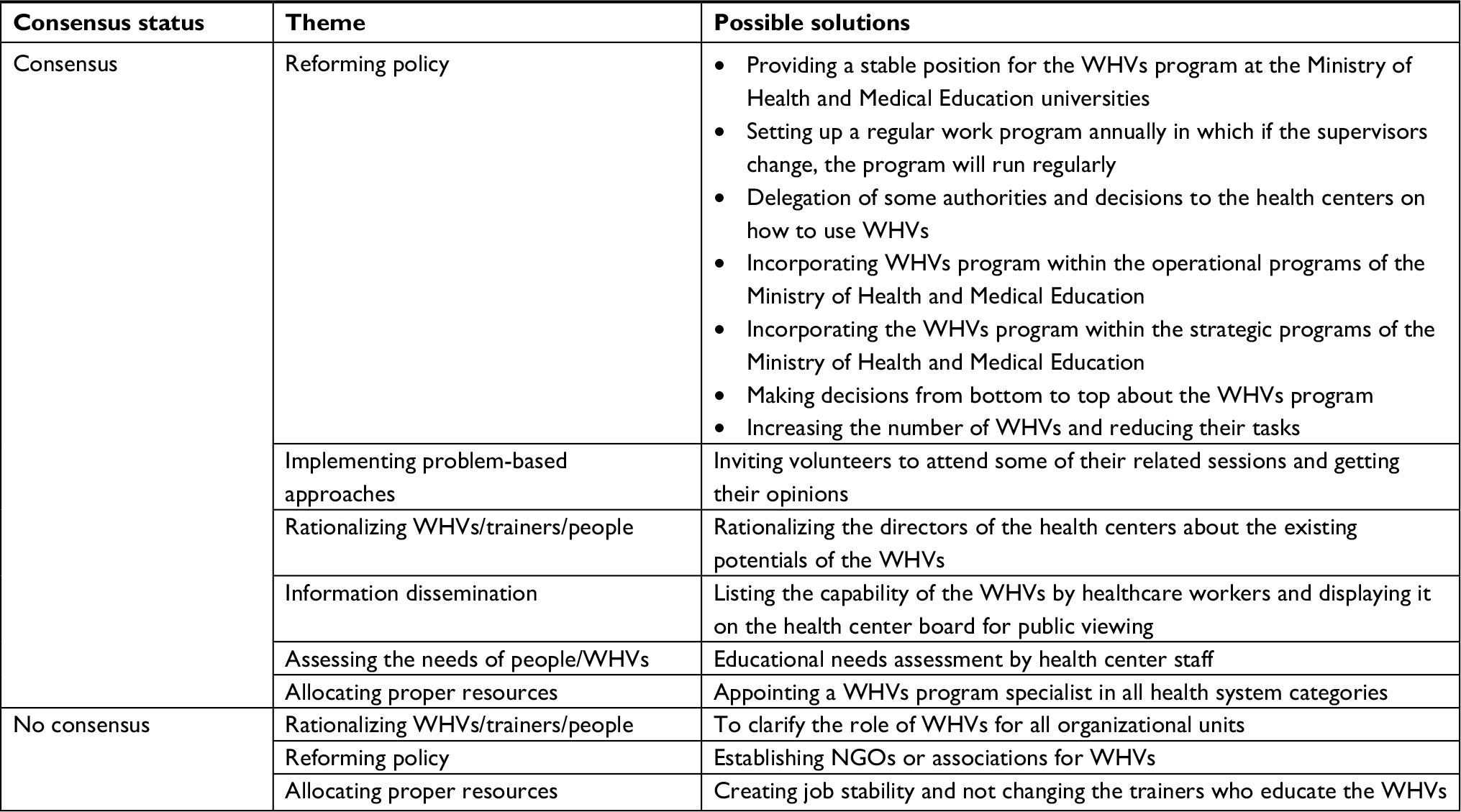 | Table 8 Strategies for unrealistic expectations and systemic confusion: Q.7. Which intervention approaches to reduce systemic confusion are most likely to succeed? Abbreviations: Q, question; NGO, nongovernmental organization; WHV, women health volunteer. |
Q.8. What can be done to overcome escaping and denial of responsibility problem?
Strategies were located in rationalizing WHVs/trainers/people, reforming policy, using social networks, allocating proper resources, and improving intersectional collaboration. The consensus was not achieved on four suggested factors to resolve escaping and denial of responsibility (Table 9).
 | Table 9 Strategies for escaping and denial of responsibility: Q.8. What can be done to overcome escaping and denial of responsibility problem? Abbreviations: Q, question; WHV, women health volunteer. |
Q.9. Which intervention approaches are needed to improve the motivation of health volunteers and their supervisors?
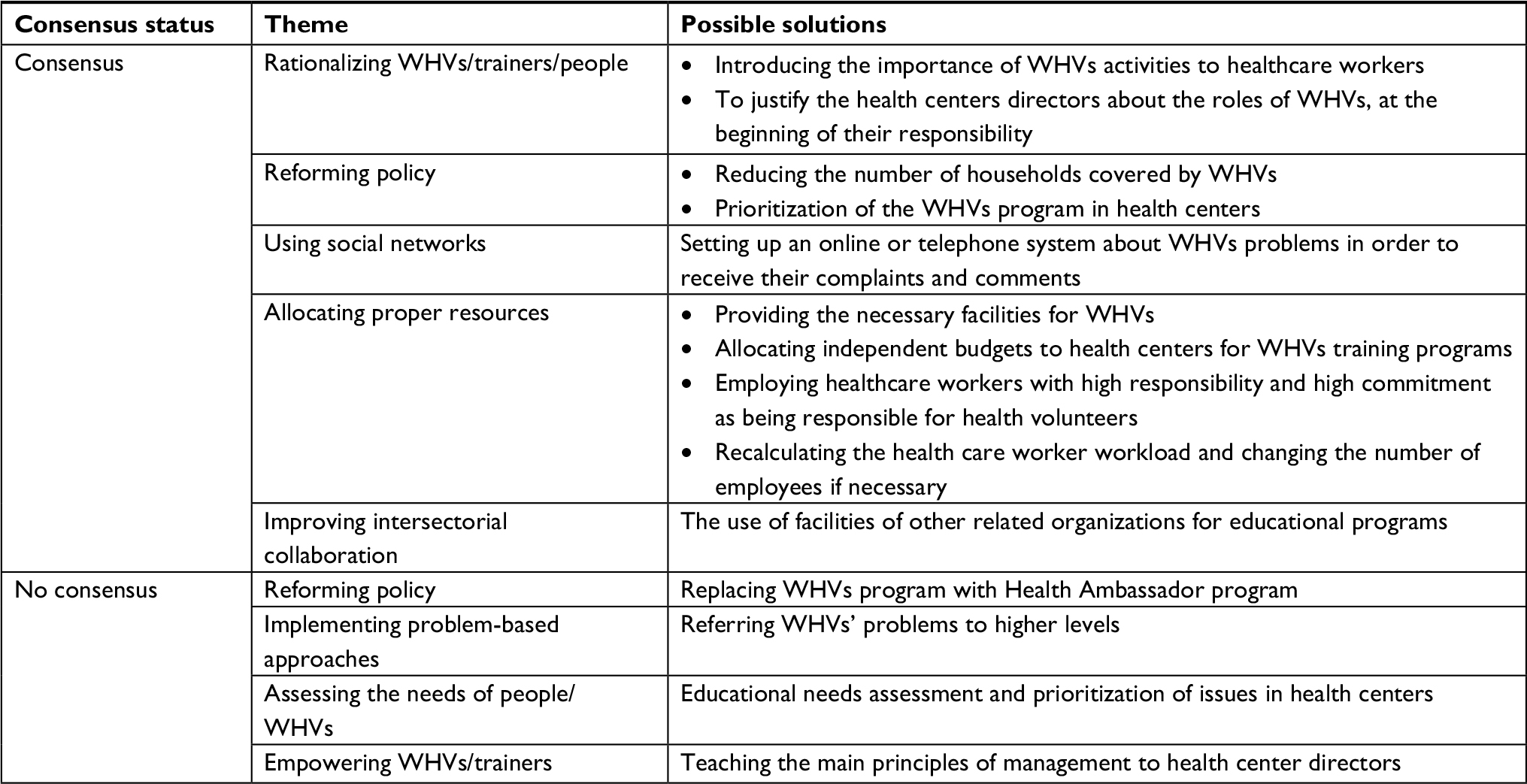
The highest consensuses were obtained on implementing motivation tactics, so that all but one of the eight recommendations was ranked as “very feasible”. Three other consensus strategies were related to implementing problem-based approaches and improving intersectional collaboration. However, no consensus was obtained on rationalizing WHVs/trainers/people as an appropriate intervention approach to improve the motivation of health volunteers and their supervisors (Table 10).
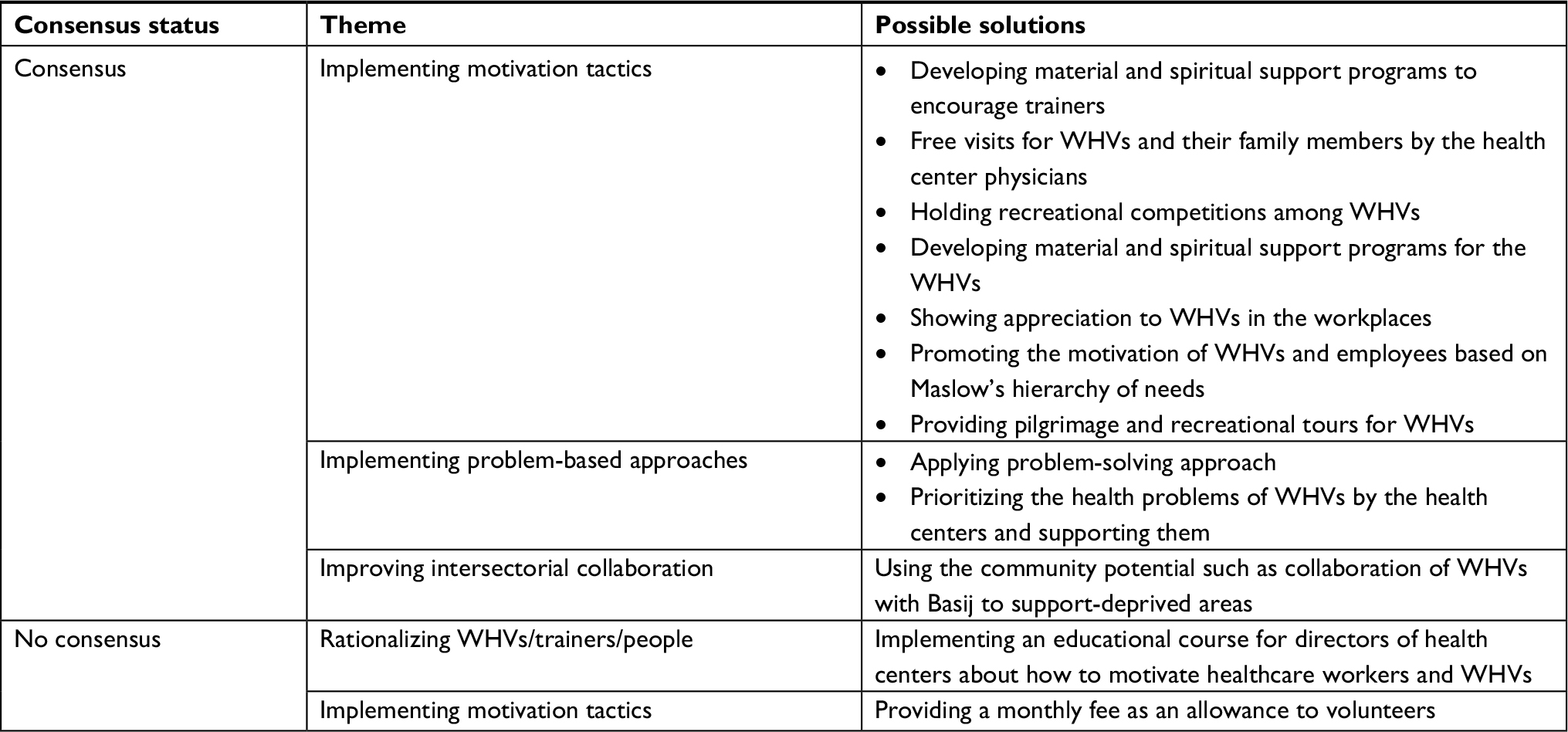 | Table 10 Strategies for lack of motivation and organizational support: Q.9. Which intervention approaches are needed to improve the motivation of health volunteers and their supervisors? Abbreviations: Q, question; WHV, women health volunteer. |
Q.10. How can we overcome educational failure?
Consensus was obtained over empowering WHVs/trainers, improving group work, allocating proper resources, reforming policy, mobilizing the community, monitoring and evaluation of WHVs/trainers, and using social networks. There was no consensus over the two suggested strategies in the theme of allocating proper resources. There was no consensus over reforming policy and empowering WHVs/trainers as the strategies to overcome educational failure (Table 11).
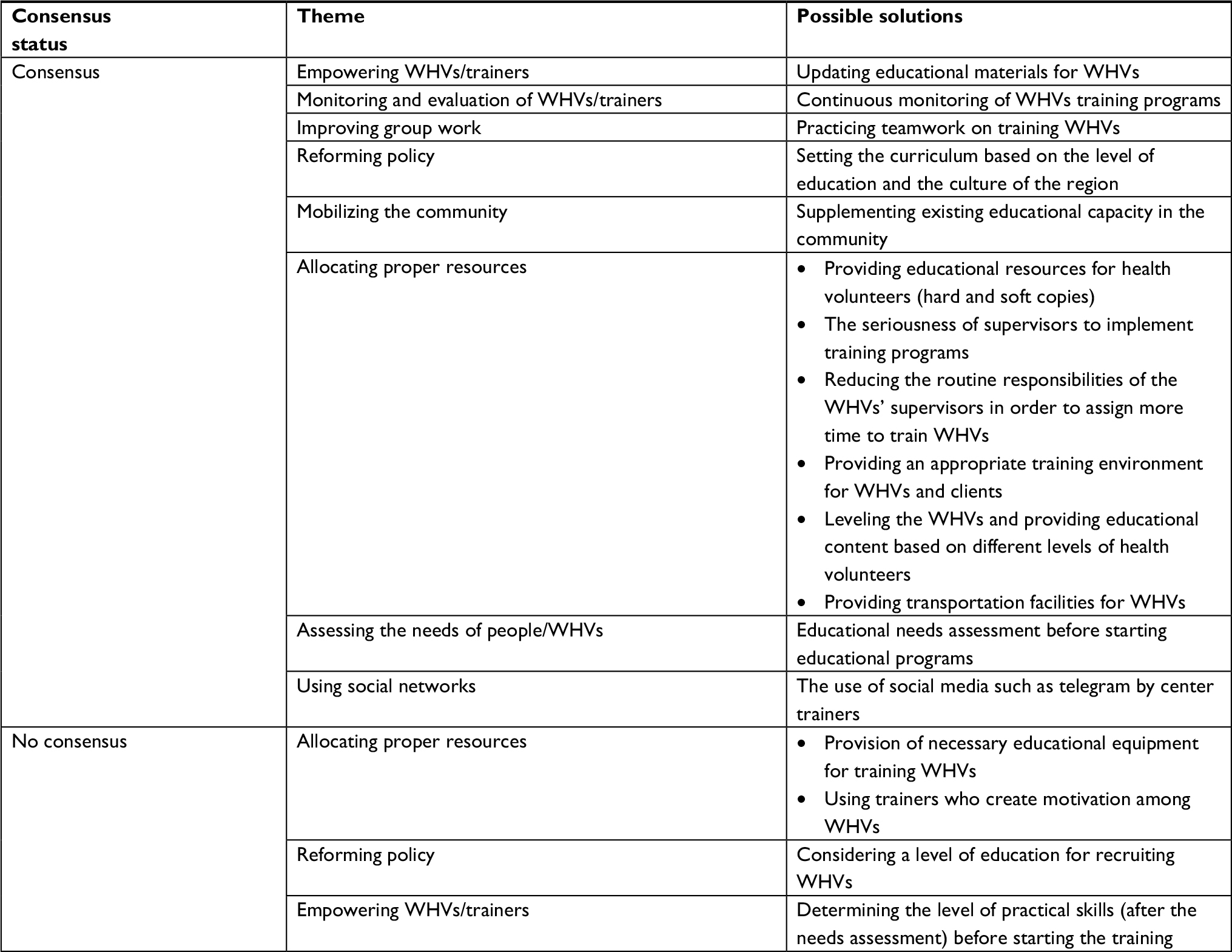 | Table 11 Strategies for educational failure: Q.10. How can we overcome educational failure? Abbreviations: Q, question; WHV, women health volunteer. |
Differences between researchers and health volunteer’s supervisors
Overall, no consensus was reached for about 33 items of the strategies to overcome barriers to the active participation of health volunteers. Opinions between the two groups of participants were compared using the Mann–Whitney U test. A statistically significant difference was found only among four strategies (Table 12). In all four strategies, researchers had a significantly higher median rank, except “establishing nongovernmental organizations or associations for WHVs”.
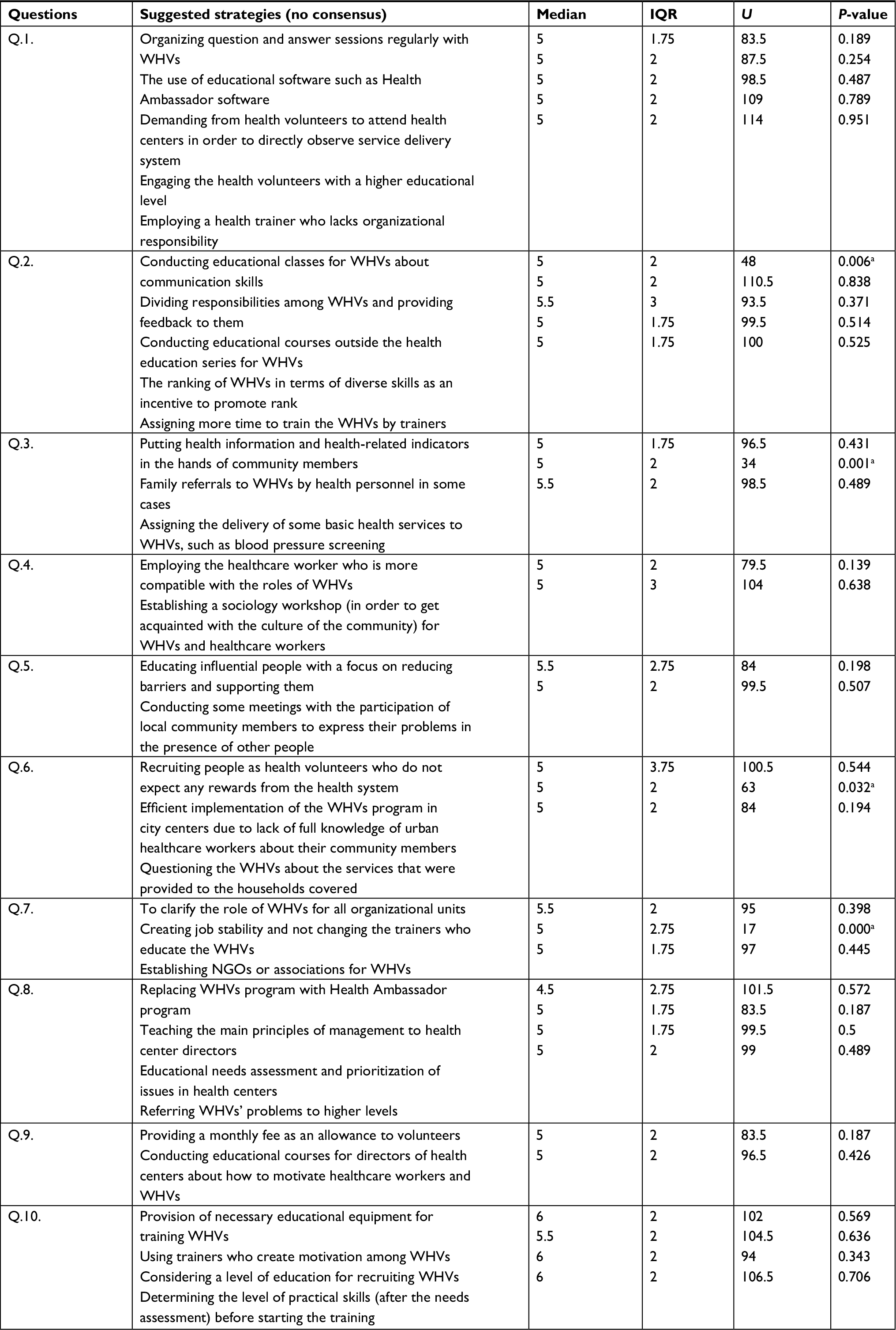 | Table 12 Mann–Whitney U test comparing groups (WHVs’ supervisors and researchers) around no consensus strategies Note: aStatistically significant (P<0.05). Abbreviations: IQR, interquartile range; NGO, non-governmental organization; Q, question; WHV, women health volunteer. |
Discussion
In the current national Delphi study, strategies to overcome barriers to the active participation of WHVs were investigated. Results revealed the views of WHVs’ supervisors and researchers. In the first round, 133 strategies emerged, using a consensus level of 70%. The consensus was obtained over 81 items at round 2 and 100 strategies at round 3.
In all questions, the use of educational methods was emphasized as the strategy to overcome barriers to WHVs’ active participation. These results were in line with many other studies.11,26,27 For example, Correia believes that education is effective in developing skills and increasing participation as well as empowering the WHVs/trainers of people in the society.28 Education contributes to better understanding of active social participation by creating participation knowledge among people.29 Moreover, studies have shown that training health care workers will improve their performance through the following three mechanisms: critical awareness about health service performance, acquiring the ability to carry out changes, and improving knowledge and skills.21,30
Among educational methods, the highest consensus was for the face-to-face training. This may be due to the more interactional nature of these training methods. Due to the fact that the availability of space and facilities are prerequisites for achieving the unit’s definition of problems and learning from each other,31 it can be said that social participation requires direct training. Therefore, more the health volunteers interact with each other at the time of training, their active participation increases.
Although motivating factors to join voluntary programs are very important,32 as our findings suggest, there was no consensus over the strategy of regular wages such as monthly payments as a motivational factor. These findings are in line with many studies in this area. For instance, Glenton et al believed that wages may be a threat to the sustainability of the female community health volunteer initiatives.22 The WHVs program may lose its voluntary nature by regular wages, and women join the program in order to receive wages. Therefore, it is likely that other intentions for participation (such as learning and developing individual skills) will be overshadowed by the regular wages.33 Nevertheless, the WHO guidelines considered payment as an essential strategy for sustainability of voluntary programs in the long term.33.34 It seems that facilities such as free visits and recreational camps may be alternatives for regular wages, upon which the experts in this study had consensus.
Many strategies that were identified in the present study can be generally categorized as improving group work, implementing motivation tactics, assessing the needs of people/WHVs, reforming policy, monitoring and evaluation of WHVs/trainers, mobilizing the community, empowering WHVs/trainers, rationalizing WHVs/trainers/ people, improving intersectional collaboration, implementing problem-based approaches, allocating proper resources, appropriate recruitment of WHVs, using social networks, and information dissemination. These themes may be used to carry out an effective comprehensive intervention to increase the active participation of health volunteers. The current study was the first research to explain the feasible strategies for increasing the active participation of health volunteers in Iran. The explanation of feasible strategies helps improve the performance of health volunteers and increases their active participation.35 It also contributes to the establishment of trust between health volunteers and people.36 These feasible strategies can be used in policymaking and planning management by policymakers and health volunteer program managers.22
Implications
The current study presented a set of possible strategies to overcome barriers to the active participation of health volunteers. In future studies, researchers may test these strategies experimentally using a multilevel approach to improve the participation of health volunteers. The findings of this study can provide a framework for health program policymakers. The studied factors should be considered by policymakers in designing and developing WHVs program.
Limitations
The findings only reflected Iranian volunteers’ supervisors and relevant researchers’ opinions and did not include researchers from other countries and healthcare authorities’ recommendations. Due to multiple responsibilities, Iranian experts were not able to check their emails and researchers had to follow through the phone, which was time-consuming. It may be better if questionnaires are completed in print format by Iranian experts.
Conclusion
The findings of this study revealed those strategies that can be implemented mainly in the short or medium term. The strategies were at different levels of individual, community, organizational, and policy. A multifaceted approach should be used to improve the participation of health volunteers. In addition to motivational factors, factors such as allocating proper resources, empowering WHVs/trainers, and mobilizing the community should be also considered.
Acknowledgments
This study was supported by the Tabriz University of Medical Sciences (grant number 1001970- 25/01/2017). We appreciate the Deputy Vice-chancellor for Research and Technology, Mr Alizadeh, and Mr Ahadi for their valuable support. We are also very grateful to the facilitators and participants for their assistance in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
Rifkin SB. Lessons from community participation in health programs: a review of the post Alma-Ata experience. Int Health. 2009;1(1):31–36. | ||
World Health Organization. Community participation in local health and sustainable development: approaches and techniques. WHO Regional Office for Europe, Copenhagen; 2002. Available from: http://www.euro.who.int/__data/assets/pdf_file/0013/101065/E78652.pdf. Accessed December 29, 2017. | ||
Heritage Z, Dooris M. Community participation and empowering WHVs/trainers in healthy cities. Health Promot Int. 2009;l(1):i45–i55. | ||
Chaulagai CN. Urban community health volunteers. World Health Forum. 1993;14(1):16–19. | ||
Behdjat H, Rifkin SB, Tarin E, Sheikh MR. A new role for women health volunteers in urban Islamic Republic of Iran. East Mediterr Health J. 2009;15(5):1164–1173. | ||
Parks KM, Steelman LA. Organizational wellness programs: a meta-analysis. J Occup Health Psychol. 2008;13(1):58–68. | ||
Sein UT. Health volunteers: third workforce for health-for-all movement. Reg Health Forum. 2006;10(1):38–48. | ||
Kok MC, Dieleman M, Taegtmeyer M, et al. Which intervention design factors influence performance of community health workers in low- and middle-income countries? A systematic review. Health Policy Plan. 2015;30(9):1207–1227. | ||
Alami A, Nedjat S, Majdzadeh R, Rahimi Foroushani A, Hoseini SJ, Malekafzali H. Factors influencing women’s willingness to volunteer in the healthcare system: evidence from the Islamic Republic of Iran. East Mediterr Health J. 2013;19(4):348–355. | ||
Rezakhani Moghaddam H, Allahverdipour H, Matlabi H. Barriers to women’s participation: experiences of volunteers and community healthcare authorities. Soc Work Public Health. 2018;33(4):237–249. | ||
Bhutta ZA, Lassi ZS, Pariyo G, Huicho L. Global experience of community health workers for delivery of health related millennium development goals: a systematic review, country case studies, and recommendations for integration into national health systems. Global Health Workforce Alliance. 2010;1(249):61–65. | ||
Vichayanrat T, Steckler A, Tanasugarn C, Lexomboon D. The evaluation of a multi-level oral health intervention to improve oral health practices among caregivers of preschool children. Southeast Asian J Trop Med Public Health. 2012;43(2):526–528. | ||
Bennet C, Wamalwa D. Report on the Midterm Evaluation of the Busia Child Survival Project (BCSP). African Medical and Research Foundation (AMREF), United States Agency for International Development (USAID); 2008. Available from: https://www.oecd.org/countries/kenya/42278868.pdf. Accessed July 1, 2018. | ||
Campbell C, Gibbs A, Maimane S, Nair Y. Hearing community voices: grassroots perceptions of an intervention to support health volunteers in South Africa. SAHARA J. 2008;5(4):162–177. | ||
Schwarz D, Sharma R, Bashyal C, et al. Strengthening Nepal’s Female Community Health Volunteer network: a qualitative study of experiences at two years. BMC Health Serv Res. 2014;14(1):473. | ||
Swechhya B, Kamaraj R. Female Community Health Volunteers Program in Nepal: perceptions, attitudes and experiences on volunteerism among female community health volunteers. Int J Interdiscip Multidiscip Stud. 2014;1(5):9–15. | ||
Jeffries M, Mathieson A, Kennedy A, et al. Participation in voluntary and community organisations in the United Kingdom and the influences on the self-management of long-term conditions. Health Soc Care Community. 2015;23(3):252–261. | ||
Chatio S, Akweongo P. Retention and sustainability of community-based health volunteers’ activities: a qualitative study in rural Northern Ghana. PLoS One. 2017;12(3):e0174002. | ||
Vizeshfar F, Momennasab M, Yektatalab S, Iman MT. Challenges faced by health volunteers in comprehensive health centers in the southwest of Iran: a qualitative content analysis. J Med Life. 2018;11(1):62–68. | ||
Bayati A, Ghanbari F, Rahzani K. The process of communication cut of health communicators from health communication head quarters. J Urmia Nurs Midwifery Fac. 2012;10(4):20–28. | ||
Lewin S, Dick J, Zwarenstein M, Lombard CJ. Staff training and ambulatory tuberculosis treatment outcomes: a cluster randomized controlled trial in South Africa. Bull World Health Organ. 2005;83(4):250–259. | ||
Glenton C, Colvin CJ, Carlsen B, et al. Barriers and facilitators to the implementation of lay health worker programs to improve access to maternal and child health: qualitative evidence synthesis. Cochrane Database Syst Rev. 2013;10(10). | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
Rayens MK, Hahn EJ. Building consensus using the policy Delphi method. Policy Polit Nurs Pract. 2000;1(4):308–315. | ||
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. | ||
Lehmann U, Sanders D. Community health workers: what do we know about them? The state of the evidence on programs, activities, costs and impact on health outcomes of using community health workers. Geneva: WHO. 2007:1–42. | ||
Hermann K, van Damme W, Pariyo GW, et al. Community health workers for ART in sub-Saharan Africa: learning from experience – capitalizing on new opportunities. Hum Resour Health. 2009;7(1):31–33. | ||
Correia AMR. Information literacy for an active and effective citizenship. In White Paper prepared for UNESCO, the US National Commission on Libraries and Information Science, and the National Forum on Information Literacy, for use at the Information Literacy Meeting of Experts, Prague, and The Czech Republic; 2002. Available from: https://pdfs.semanticscholar.org/a0e6/7eab49d5e6e01fe49270a15018088949ab6a.pdf?_ga=2.78589204.1408992692.1517987637-1961287143.1503955051. Accessed January 7, 2018. | ||
Singhal A. Facilitating community participation through communication; 2001. Available from: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.468.2748&rep=rep1&type=pdf. Accessed April 21, 2018. | ||
Onyango-Ouma W, Laisser R, Mbilima M, et al. An evaluation of Health Workers for Change in seven settings: a useful management and health system development tool. Health Policy Plan. 2001;16(Suppl 1):24–32. | ||
Draper AK, Hewitt G, Rifkin S. Chasing the dragon: developing indicators for the assessment of community participation in health programmes. Soc Sci Med. 2010;71(6):1102–1109. | ||
Akintola O. What motivates people to volunteer? The case of volunteer AIDS caregivers in faith-based organizations in KwaZulu-Natal, South Africa. Health Policy Plan. 2011;26(1):53–62. | ||
World Health Organization. Scaling Up, Saving Lives: Task Force for Scaling Up Education and Training for Health Workers. Switzerland: Global Health Workforce Alliance – World Health Organization; 2008. Available from: http://www.who.int/workforcealliance/documents/Global_Health_Final_Report.pdf. Accessed 9 July, 2018. | ||
World Health Organization. Task Shifting: Rational Redistribution of Tasks among Health Workforce Teams: Global Recommendations and Guidelines. Geneva: WHO; 2007. Available from: http://apps.who.int/iris/bitstream/10665/43821/1/9789241596312_eng.pdf. Accessed June 14, 2018. | ||
Kok MC, Kane SS, Tulloch O, et al. How does context influence performance of community health workers in low- and middle-income countries? Evidence from the literature. Health Res Policy Syst. 2015;13(1):13–14. | ||
Lunsford SS, Fatta K, Stover KE, Shrestha R. Supporting close-to-community providers through a community health system approach: case examples from Ethiopia and Tanzania. Hum Resour Health. 2015;13(1):12–13. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.