")
Back to Journals » International Journal of General Medicine » Volume 13
Subtrochanteric Femoral Fracture in a Patient with Osteopetrosis: Treated with Internal Fixation and Complicated by Intraoperative Femoral Neck Fracture
Received 2 November 2020
Accepted for publication 4 December 2020
Published 16 December 2020 Volume 2020:13 Pages 1551—1557
DOI https://doi.org/10.2147/IJGM.S289265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xing Hua,1 Zhenyu Liu,2 Xinjia Wang3
1Department of Stomatology, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, People’s Republic of China; 2Department of Orthopedics, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, People’s Republic of China; 3Department of Pediatrics, Beijing Friendship Hospital, Capital Medical University, Beijing 100050, People’s Republic of China
Correspondence: Xinjia Wang Email [email protected]
Objective: Osteopetrosis (OP) is a rare, heritable skeletal disorder that is caused by osteoclast dysfunction, leading to failure of bone resorption and increased bone density. The fragility of such dense bone may result in an increased incidence of fractures. Furthermore, surgery in patients with OP is associated with increased technical difficulty and a higher risk of complications.
Case Report: We report a case of a 20-year-old woman with autosomal dominant OP who developed a subtrochanteric femoral fracture. The fracture was treated by open reduction and internal fixation using a dynamic hip screw. Although technical difficulties were experienced and an intraoperative femoral neck fracture occurred, the surgical outcome was satisfactory. Union of the fractures was visible on radiographs obtained 12 months postoperatively. At 2 years postoperatively, the patient was completely free of any complications resulting from her injury and treatment.
Conclusion: Open reduction and internal fixation may be an effective option for fractures in patients with OP. Orthopedic surgeons should be aware that the increased density and stiffness of osteopetrotic bone increases the risks of intraoperative technical difficulties, iatrogenic fractures, and postoperative complications.
Kgeywords: osteopetrosis, autosomal dominant osteopetrosis, subtrochanteric fracture, dynamic hip screw
Introduction
Osteopetrosis (OP) is a rare, heritable skeletal disorder that was first described in 1904.1 OP is caused by osteoclast dysfunction that leads to failure of bone resorption and increased bone density2 and is characterized by hard but brittle bone with a narrow or even absent medullary canal.3 Based on the severity and pattern of inheritance, OP is divided into three types: autosomal dominant OP (ADO), autosomal recessive OP (ARO), and intermediate autosomal OP (IAO).4 The features of the three types of OP are summarized in Table 1.
 |
Table 1 Characteristics of Three Types of OP |
The fragility of such dense bone in OP may result in an increased incidence of fractures.5 Most fractures in patients with OP are treated using conservative methods, including skeletal traction and plaster fixation, due to the high risks of infection and nonunion.6 Technical challenges and complications may occur during surgery because of the hard but brittle bone structure. We report a patient with an osteopetrotic subtrochanteric fracture treated by open reduction and internal fixation with a dynamic hip screw (DHS).
Case Report
A 20-year-old woman fell while playing volleyball and incurred a subtrochanteric fracture of her right femur (Figure 1). The patient had the following typical imaging manifestations of OP: increased radiation density of the entire skeleton, absence of medullary canals, appearance of a “thick Jersey spine” or “sandwich vertebrae” caused by thickening of the vertebral endplates, and several sclerotic concentric bands (bone-within-bone) in the iliac wing (Figure 2A). Radiographs of the right knee showed no “Erlenmeyer flask” deformity of the distal femur (Figure 2B). She had no cranial and facial distortions or syndactylies of the fingers and toes, but she was short (145 cm). Laboratory examination results showed normal hematological parameters, thyroid hormone levels, and alkaline phosphatase concentration. There was no evidence of skeletal deformities, hepatosplenomegaly, or cranial nerve disturbances. The patient had no previous history of fractures, anemia, recurrent infections, or bone pain. The patient was diagnosed with ADO type II (known as Albert-Schonberg disease or marble bone disease). The X-ray examination results of her parents were normal, and they had no history of fractures. The family history of previous generations was unknown. The patient and her parents refused to undergo genetic examinations.
 |
Figure 1 X-ray examination results of the pelvis showed a right subtrochanteric femoral fracture and osteosclerosis of the pelvis with bone-within-bone appearance in the iliac wing and obliteration of the femoral medullary canal. |
 |
Figure 2 Anteroposterior radiograph of the lumbar spine (A) showed the appearance of a “rugger jersey spine ”caused by thickening of vertebral endplates. Anteroposterior radiograph of right knee (B) showed no “Erlenmeyer flask” deformity of the distal femur. |
As access to the intramedullary canal may not have been possible in this patient, we chose to use a DHS instead of intramedullary nailing. The procedure was technically challenging. The patient was placed in the supine position on a fracture traction table under general anesthesia. The fracture was reduced under fluoroscopic visualization. New sharp drill bits were used, as blunt drill bits were more likely to break. Saline was continuously applied to help keep the drill bit cool to prevent bone necrosis and drill bit breakage. It took 30 minutes to create the hole and insert a guidewire for the lag screw. Reaming along the guidewire was also difficult and time-consuming. The sclerotic bone produced excessive resistance to tapping. During the tapping process, the surgeon felt a sudden cracking sensation through the handle. A femoral neck fracture was detected by fluoroscopy. The nondisplaced fracture was located in the middle of the femoral neck, and the lag screw provided adequate stable fixation and compression. Therefore, we decided to proceed with the original surgery plan. Subsequently, the lag and plate were attached (Figure 3A and B). During the surgery, a cortical screw and six drill bits were broken, and a few guidewires were bent.
 |
Figure 3 Postoperative radiographs of the pelvis (A, B) showed the right subtrochanteric femoral fracture with a dynamic hip screw and fracture of the right femoral neck. |
The patient was instructed to carry out active hip and knee joint training from the first postoperative day and used crutches to walk without placing weight on the affected limb for 7 days postoperatively. The patient had obtained 90° active hip flexion at 3 weeks postoperatively. She was discharged on crutches and instructed not to bear weight on the affected limb until the fracture had healed. Routine postoperative clinical and radiological follow-up examinations were performed. At 12 months postoperatively, there was complete healing of the fractures on X-ray examination, and the patient was allowed to commence full weightbearing (Figure 4A and B). At 2 years postoperatively, the patient was pain-free with full range of motion of the hip and had returned to work.
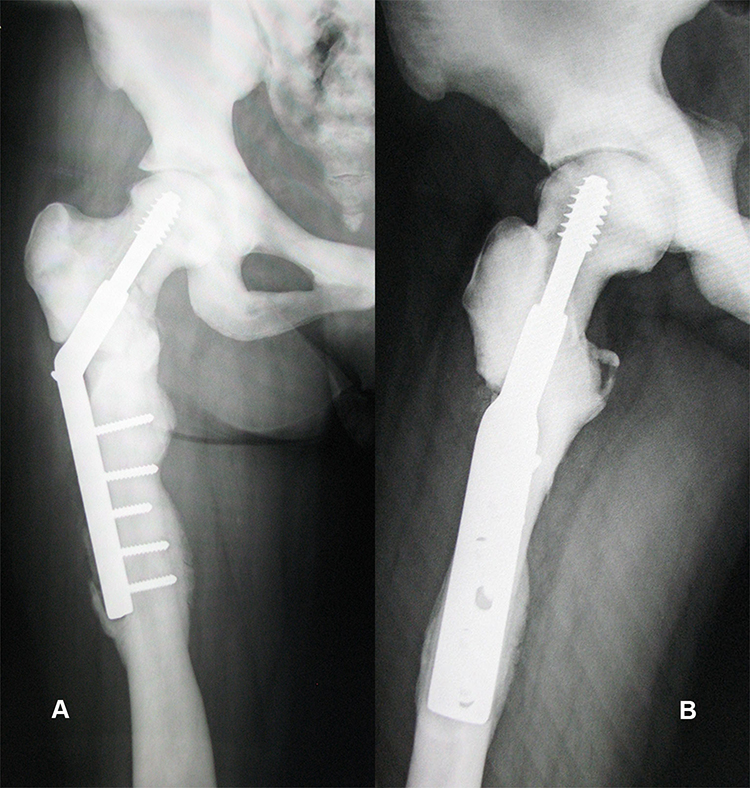 |
Figure 4 The X-ray examination results (A, B) showed complete healing of the subtrochanteric fracture and femoral neck fracture 2 years after surgery. |
Discussion
OP is a rare congenital bone disorder that makes the bones abnormally dense and prone to fractures, as defective osteoclast function and failure of proper reabsorption results in sclerotic bones.7 OP is categorized clinically into three primary types: ADO, ARO, and IAO. All types of OP are usually diagnosed based on radiographic features found in a skeletal survey.8 ADO is the most common type of OP and used to be subdivided into type I and type II.9 Type I is no longer used in the classification of OP,3 while type II, which is also called Albert-Schonberg disease or marble bone disease, is identified by the classic vertebral endplate sclerosis (“sandwich” vertebrae appearance) and basal skull involvement.10 ADO type II is the most common form of OP seen in adulthood, with an incidence of 1 in 20,000.11 Patients with ADO type II generally have a normal life expectancy but experience a multitude of orthopedic complications, including mandibular osteomyelitis, fractures, hip osteoarthritis, and facial nerve palsy.5 In addition, ADO type II tends to skip a generation.12 The genetic penetrance of ADO is estimated to be 75%.13 The parents of patients with OP should be carefully evaluated and may be unaffected due to gonadal mosaicism.14 In our case, the X-ray examination results of the patient’s parents were negative. However, the patient and her parents refused to undergo genetic examinations.
Genetic mutations are believed to be the cause of OP.15 Mutations in T cell immune regulator 1 (TCIRG1), chloride channel 7 (CLCN7), osteopetrosis-associated transmembrane protein 1, sorting nexin 10, and pleckstrin homology and RUN domain containing M1 lead to osteoclast-rich ARO, in which the osteoclasts are abundant but have severely impaired resorptive function.16 More than 50% of ARO cases are caused by mutations in the TCIRG1 gene.11 TCIRG1-mutated osteoclasts have a defective ruffled border and significantly reduced resorptive activity.17 Mutations in the CLCN7 gene are associated with ARO and ADO type II.18 CLCN7 is essential for bone remodeling, and mutations of the CLCN7 gene make the bone brittle.16 Mutations in TNFSF11 (also known as RANKL) and its receptor TNFRSF11A (also known as RANK) lead to osteoclast-poor ARO.19 IAO is attributed to hypomorphic mutations in the NF-κB essential regulator gene.11,20 The development of genetic technology has led to the discovery of new genes associated with OP, and the genetics of OP warrants further study.
Due to the high density and brittleness of the bones in OP, surgical interventions lead to a high incidence of complications; therefore, most fractures in patients with OP are treated conservatively. However, surgical treatment may be a better choice for patients in pursuit of an active life. Intramedullary nailing is effective for subtrochanteric fractures in patients without OP. However, patients with OP have a narrow or even completely absent medullary canal, which makes surgery challenging. Various osteosynthesis techniques and implants have been reported, each with its own advantages and disadvantages. Table 2 summarizes the published cases describing the surgical treatment of subtrochanteric femoral fractures in patients with OP between 2010 and 2020. In our case, internal fixation with a DHS obtained a satisfactory surgical outcome.
 |
Table 2 Summary of the Published Cases Describing the Surgical Treatment of Subtrochanteric Femoral Fractures in Patients with OP (2010–2020) |
Patients with OP have a poor bone blood supply and relative osteopenia, which are associated with increased risks of infection and osteomyelitis.35 An infection rate of 12% was reported in a case series of patients with OP.36 Furthermore, the increased density and stiffness of osteopetrotic bone makes it susceptible to drill bit breakages and iatrogenic fractures, as in our case. Therefore, it is crucial to have a detailed presurgical plan when treating fractures in patients with OP. Surgeons should be aware that an increased number of drills, batteries, and some other osteosynthesis implants must be obtained for the surgery. The processes of drilling, reaming, and implantation into dense brittle bone are challenging and exhausting, and extra care and caution are required. In our case, the fracture was located in the middle of the femoral neck, and the lag screw was able to apply enough stable fixation and compression. Another problem encountered when treating fractures in patients with OP is delayed union or nonunion. Histologically, the bone callus that develops after fracture in patients with OP is apparently normal in the early stages, but there is no Haversian organization in the mature callus.37 Fractures take more time to heal in patients with OP than in the general population. The mean time to fracture union in one study of nine patients with OP was 8.3 months (7 to 12).38 In our case, the fracture was healed at 12 months postoperatively and there was no sign of infection.
Conclusion
Open reduction and internal fixation may be an effective option for treating fractures in patients with OP. Orthopedic surgeons should be aware that the increased density and stiffness of osteopetrotic bone increases the risks of intraoperative technical difficulties, iatrogenic fractures, and postoperative complications.
Abbreviations
OP, osteopetrosis; ADO, autosomal dominant osteopetrosis; ARO, autosomal recessive osteopetrosis; IAO, intermediate autosomal osteopetrosis; DHS, dynamic hip screw.
Data Sharing Statement
Please contact the corresponding author for data requests.
Ethics Approval and Consent to Participate
The study was approved by the ethics committee of Beijing Friendship Hospital. The patient provided written informed consent to have the case details and any accompanying images published. This study was conducted in accordance with the latest version of the Declaration of Helsinki. Each subject was ensured anonymity, which was maintained by using subject-specific numeric codes on all records, including registration cards.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Stark Z, Savarirayan R. Osteopetrosis. Orphanet J Rare Dis. 2009;4(1):5. doi:10.1186/1750-1172-4-5
2. Pang Q, Chi Y, Zhao Z, et al. Novel mutations of CLCN7 cause autosomal dominant osteopetrosis type II (ADO-II) and intermediate autosomal recessive osteopetrosis (IARO) in Chinese patients. Osteoporos Int. 2016;27(3):1047–1055. doi:10.1007/s00198-015-3320-x
3. Paccou J, Michou L, Kolta S, et al. High bone mass in adults. Joint Bone Spine. 2018;85(6):693–699. doi:10.1016/j.jbspin.2018.01.007
4. Wu CC, Econs MJ, DiMeglio LA, et al. Diagnosis and Management of Osteopetrosis: consensus Guidelines From the Osteopetrosis Working Group. J Clin Endocrinol Metab. 2017;102(9):3111–3123. doi:10.1210/jc.2017-01127
5. Palagano E. Genetics of Osteopetrosis. Curr Osteoporos Rep. 2018;16(1):13–25.
6. Rathod AK, Dhake RP, Borde MD. Traumatic multiple cervical spine injuries in a patient with osteopetrosis and its management. Eur Spine J. 2017;26(Suppl 1):229–235.
7. Bacon S, Crowley R. Developments in rare bone diseases and mineral disorders. Ther Adv Chronic Dis. 2018;9(1):51–60. doi:10.1177/2040622317739538
8. Beaton CD, Rivera L, Echegaray G, et al. Bilateral Posterior-Stabilized Total Knee Arthroplasty in a Patient With Osteopetrosis and Literature Review. Arthroplast Today. 2020;6(4):866–871. doi:10.1016/j.artd.2020.09.016
9. Bollerslev J, Mosekilde L. Autosomal dominant osteopetrosis. Clin Orthop Relat Res. 1993;294:45–51. doi:10.1097/00003086-199309000-00006
10. Bollerslev J, Andersen PJ. Fracture patterns in two types of autosomal-dominant osteopetrosis. Acta Orthop Scand. 1989;60(1):110–112. doi:10.3109/17453678909150106
11. Penna S, Capo V, Palagano E, et al. One Disease, Many Genes: implications for the Treatment of Osteopetroses. Front Endocrinol (Lausanne). 2019;10:85. doi:10.3389/fendo.2019.00085
12. Armstrong DG, Newfield JT, Gillespie R. Orthopedic management of osteopetrosis: results of a survey and review of the literature. J Pediatr Orthop. 1999;19(1):122–132. doi:10.1097/01241398-199901000-00026
13. Johnston CJ, Lavy N, Lord T, et al. Osteopetrosis. A clinical, genetic, metabolic, and morphologic study of the dominantly inherited. Benign Med. 1968;47(2):149–167. doi:10.1097/00005792-196803000-00004
14. Ladd LM, Imel EA, Niziolek PJ, et al. Radiographic imaging, densitometry and disease severity in Autosomal dominant osteopetrosis type 2. Skeletal Radiol. 2020. doi:10.1007/s00256-020-03625-3
15. Xue JY, Ikegawa S, Guo L. Genetic disorders associated with the RANKL/OPG/RANK pathway. J Bone Miner Metab. 2020.
16. Bug DS, Barkhatov IM, Gudozhnikova YV, et al. Identification and Characterization of a Novel CLCN7 Variant Associated with Osteopetrosis. Genes. 2020;11(11):11. doi:10.3390/genes11111242
17. Capo V, Penna S, Merelli I. et al. Expanded circulating hematopoietic stem/progenitor cells as novel cell source for the treatment of TCIRG1 osteopetrosis. Haematologica;2020.
18. Chorin O, et al. Transcriptome sequencing identifies a noncoding, deep intronic variant in CLCN7 causing autosomal recessive osteopetrosis. Mol Genet Genomic Med. 2020;e1405.
19. Villa A, Guerrini MM, Cassani B, et al. Infantile malignant, autosomal recessive osteopetrosis: the rich and the poor. Calcif Tissue Int. 2009;84(1):1–12. doi:10.1007/s00223-008-9196-4
20. Miot C, Imai K, Imai C, et al. Hematopoietic stem cell transplantation in 29 patients hemizygous for hypomorphic IKBKG/NEMO mutations. Blood. 2017;130(12):1456–1467. doi:10.1182/blood-2017-03-771600
21. Golden RD, Rodriguez EK. Management of subtrochanteric femur fractures with internal fixation and recombinant human bone morphogenetic protein-7 in a patient with osteopetrosis: a case report. J Med Case Rep. 2010;4(1):142. doi:10.1186/1752-1947-4-142
22. Amit S, et al. Fixation of Subtrochanteric Fractures in Two Patients with Osteopetrosis Using a Distal Femoral Locking Compression Plate of the Contralateral Side. Eur J Trauma Emerg Surg. 2010;36(3):263–269. doi:10.1007/s00068-009-8237-7
23. Sonohata M, Mawatari M, Hotokebuchi T, et al. Bipolar hip arthroplasty for subtrochanteric femoral nonunion in an adult with autosomal dominant osteopetrosis type II. J Orthop Sci. 2011;16(5):652–655. doi:10.1007/s00776-011-0069-8
24. Kumar D, Jain VK, lal H, et al. Metachronous bilateral subtrochanteric fracture of femur in an osteopetrotic bone: A case report with technical note. J Clin Orthop Trauma. 2012;3(2):103–106. doi:10.1016/j.jcot.2012.09.007
25. Kumbaraci M, et al. Treatment of bilateral simultaneous subtrochanteric femur fractures with proximal femoral nail antirotation (PFNA) in a patient with osteopetrosis: case report and review of the literature. J Orthop Sci. 2013;18(3):486–489.
26. Sen RK, et al. Simple reproducible technique in treatment for osteopetrotic fractures. Musculoskelet Surg. 2013;97(2):117–121. doi:10.1007/s12306-012-0222-3
27. Aslan A, et al. Surgical treatment of osteopetrosis-related femoral fractures: two case reports and literature review. Case Rep Orthop. 2014;2014:891963.
28. Seyfettinoglu F, Tuhanioglu U, Ogur HU, et al. Proximal femoral fracture surgery in a patient with osteopetrosis tarda: complications and treatment strategy. Int Med Case Rep J. 2016;9:347–351. doi:10.2147/IMCRJ.S114710
29. Huang J, et al. Successful open reduction and internal fixation for displaced femoral fracture in a patient with osteopetrosis: case report and lessons learned. Medicine. 2017;96(33):e7777. doi:10.1097/MD.0000000000007777
30. Matsuo T, Lee SY, Iwakura T, et al. Locking plate osteosynthesis for a femoral fracture and subsequent nonunion in a patient with osteopetrosis. Int J Surg Case Rep. 2018;51:395–399. doi:10.1016/j.ijscr.2018.09.013
31. Hasan O, Pathan AZ, Naqi H, et al. Inheritance patterns, challenges, and outcomes of fracture management in osteopetrosis patients. CASE series and review of pertinent literature. Ann Med Surg. 2018;36:191–198. doi:10.1016/j.amsu.2018.10.038
32. Chawla A, Kwek E. Fractures in patients with osteopetrosis, insights from a single institution. Int Orthop. 2019;43(6):1297–1302. doi:10.1007/s00264-018-4167-5
33. Hiyama S, Takahashi T, Matsumura T, et al. Open reduction and internal fixation using a locking compression plate as treatment for subtrochanteric fracture in two patients with osteopetrosis. Injury. 2020;51(2):565–569. doi:10.1016/j.injury.2019.11.032
34. Kim J, Park YC, Moon H-S, et al. Intramedullary nailing for subtrochanteric fracture in autosomal dominant Type II osteopetrosis: case report of 2 patients. Medicine. 2020;99(32):e21648. doi:10.1097/MD.0000000000021648
35. Agrawal A, Maniar A, Maniar R. Bilateral Girdlestone Procedure as a Treatment Modality in a Case of Complicated Adult-Onset Osteopetrosis: A Case Report. JBJS Case Connect. 2019;9(4):e0179. doi:10.2106/JBJS.CC.18.00179
36. Birmingham P, McHale KA. Case reports: treatment of subtrochanteric and ipsilateral femoral neck fractures in an adult with osteopetrosis. Clin Orthop Relat Res. 2008;466(8):2002–2008. doi:10.1007/s11999-008-0256-x
37. De Palma L, et al. Fracture callus in osteopetrosis. Clin Orthop Relat Res. 1994;308:85–89.
38. Yigit S, Arslan H, Akar MS, et al. Mid-term outcomes of surgical treatment in fractures in patients with osteopetrosis. Bone Joint J. 2020;102-B(8):1082–1087. doi:10.1302/0301-620X.102B8.BJJ-2020-0431.R1
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.