")
Back to Journals » Clinical Optometry » Volume 11
Sub-Foveal Choroidal Thickness In Healthy Nepalese Population
Authors Gyawali P , Kharel Sitaula R , Kharal A , Bhusal A, Paudel M, Joshi SN
Received 24 June 2019
Accepted for publication 17 October 2019
Published 15 November 2019 Volume 2019:11 Pages 145—149
DOI https://doi.org/10.2147/OPTO.S220615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Parash Gyawali, Ranju Kharel Sitaula, Anish Kharal, Asmita Bhusal, Manisha Paudel, Sagun Narayan Joshi
BP Koirala Lions Centre for Ophthalmic Studies, Maharajgunj Medical Campus, Institute of Medicine, Kathmandu, Nepal
Correspondence: Parash Gyawali
BP Koirala Lions Centre for Ophthalmic Studies, Maharajgunj Medical Campus, Institute of Medicine, Kathmandu, Nepal
Tel +97 798 4006 9980
Email [email protected]
Purpose: This study was conducted primarily to measure sub-foveal choroidal thickness (SFCT) in healthy Nepalese population. Also, the correlation of SFCT with age, inter-eye difference of SFCT, inter-gender variation and inter-ethnic variation of SFCT was observed.
Materials and methods: A cross-sectional, hospital based study in 162 participants (324 eyes) of six ethnic groups (Brahmin, Chhetri, Newar, Tamang, Muslim, and Gurung) was conducted. The mean age of participants was 37.37 ± 15.02 years. All the participants underwent SFCT measurement using Spectral Domain Optical Coherence Tomography (Spectralis HRA+OCT, Heidelberg Engineering, Germany) with the help of in-built caliber. Age, inter-gender, inter-eye and inter-ethnic differences in SFCT were recorded and analyzed.
Results: The average SFCT of right eye (RE) and left eye (LE) was 307.98 ± 74.64 μm and 312.63 ± 76.90 μm respectively, with average SFCT of 310.31 ± 75.70 μm for both eyes. SFCT of only the RE was selected for further calculation due to insignificant inter-eye difference of SFCT (p = 0.128). There was a significant negative correlation of SFCT with age (r = −0.705, p = 0.01). A regression analysis showed thinning of SFCT by 3.50 ± 0.278 μm per year. In another context, SFCT of male and female was 305.49 ± 79.72 μm and 313.55 ± 70.76 μm respectively. However, there was no significant inter-gender difference (p = 0.51). Similarly, inter-ethnic variations of SFCT was also statistically non -significant (p = 0.74).
Conclusion: SFCT was negatively correlated with the age of participants, implying a decrease in choroidal thickness (CT) with an increase in age. Age can be considered as an important factor in the measurement of SFCT. Gender and ethnic groups did not have a significant role in the measurement and comparison of SFCT.
Keywords: sub-foveal choroidal thickness, enhanced depth imaging, optical coherence tomography, OCT, spectral domain, SD
Introduction
Choroid is a highly vascular middle layer sandwiched between inner retinal layer and outer scleral layer of the eye. Choroid is of paramount importance to retinal and visual function as it is the source of vascular supply to retinal pigment epithelial cells and the outer retina. Sub-foveal choroidal thickness (SFCT) is found to vary with age, sex, axial length, refractive error1 and is also affected by diurnal variation.2 Knowledge about choroidal thickness (CT) could be of important clinical guide in the diagnosis, management and in monitoring of certain disease progression.
In 2008, Margolis and Spaide3 first investigated CT using enhanced depth imaging spectral domain optical coherence tomography (EDI SD-OCT) technique. EDI SD-OCT is a non-invasive novel technique which enables us to acquire “optical biopsy” of the posterior segment in vivo which further allows to make qualitative and quantitative analysis of posterior segment structure, like choroid. On the basis of histologic examination, CT ranges from 170 to 220 μm4 However, recent advances in technologies, enhanced depth imaging using a Heidelberg system, have shown an approximate SFCT of 300 μm in healthy volunteers3
The aim of this study was to determine a baseline normative data of SFCT in the healthy Nepalese population and observe its correlation with age. Also, Inter-ethnic, inter-gender and inter-eye difference of SFCT were also observed.
Materials And Methods
A cross-sectional study was conducted at B.P. Koirala Lions Center for Ophthalmic Studies (BPKLCOS), a tertiary level eye center in Kathmandu, Nepal between October 2017 and September 2018. The study was approved by the Institutional Review Committee (IRC) at the Institute of Medicine (IOM), Tribhuvan University. This study was done as per the declaration of Helsinki. Written informed consent was obtained from all the participants and for the participants below 18 years of age, parents or a legal guardian provided consent prior to the study. A purposive sampling technique was used as a sampling method. A detailed medical and ophthalmic history including information on systemic disease, ocular trauma, and ocular surgery were recorded. Only healthy subjects were enrolled for the study. Healthy subjects were defined as subjects having no systemic diseases or ocular pathological conditions that might alter the CT.
Axial length was measured using non-contact partial coherence interferometry (IOL master, Zeiss 500). CT scanning was done at sub-foveal region using Spectralis-spectral domain optical coherence tomography (Heidelberg Engineering) with software version 6.0. Sections each composed of the 100 averaged scans using eye tracking were obtained in a 5°× 30° rectangle encompassing the macula and optic nerve. The horizontal section going directly through the center of the fovea was used for the measurement of CT. SFCT in the enhanced images was measured as the perpendicular distance between the outer portion of the hyper-reflective line corresponding to the RPE (automatically detected by the instrument) to hypo-reflective line or margin corresponding to the chorio-scleral junction (Figure 1). The measurement of SFCT was made manually by a single experienced grader. All images were taken at routine clinic time (9 a.m. to 12 a.m.), to avoid possible diurnal variations in CT5
Participants with best corrected visual acuity of 20/20 or better, normal slit-lamp biomicroscopy and funduscopy, and having well-defined chorioscleral junction were enrolled in the study. Hyperopic or myopic participants having refractive error of more than 1D were excluded.
As per the census of Nepal 2011, 168 types of ethnic groups are found in Nepal. In our study, participants from Brahmin, Chhetri, Newar, Tamang, Gurung, and Muslim ethnic groups were selected, which were greater in numbers of hospital records. Participants of these ethnic groups were age and sex matched.
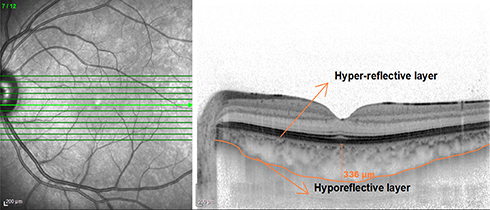 |
Figure 1 EDI-OCT scan of a healthy 24-year-old male showing normal CT with labeled RPE-Bruch’s membrane junction (hyper-reflective layer) and chorio-scleral junction (hyporeflective layer). |
All data are expressed as mean ± standard deviation (SD). Pearson’s correlation test and regression analysis were used to observe the association between SFCT and age. An independent t-test was used to compare SFCT between male and female group. The inter-eye difference of SFCT was measured using a paired t-test. The inter-ethnic difference of SFCT was calculated using a one way analysis of variance (ANOVA). P value of <0.05 was considered statistically significant, with a confidence interval (CI) of 95%.
Results
One hundred and sixty-two normal subjects (324 eyes) were included in the study, out of which 100 were female and 62 were male. The average age of subjects was 37.37 ± 15.02 years (range 17 to 79 years), with 36.17 ± 15.66 years and 35.96 ± 14.22 years in male and female respectively. There was no statistically significant age difference between two genders (p = 0.75). The Brahmin ethnic group represented 32.1% of total sample size, Chhetri represented 25.9%, Tamang 11.7%, Gurung 11.1%, Newar 9.9%, and Muslim 9.3%. The mean age and SFCT of the different ethnic groups is shown in Table 2. There was no significant age difference between different ethnic groups (p = 0.379).
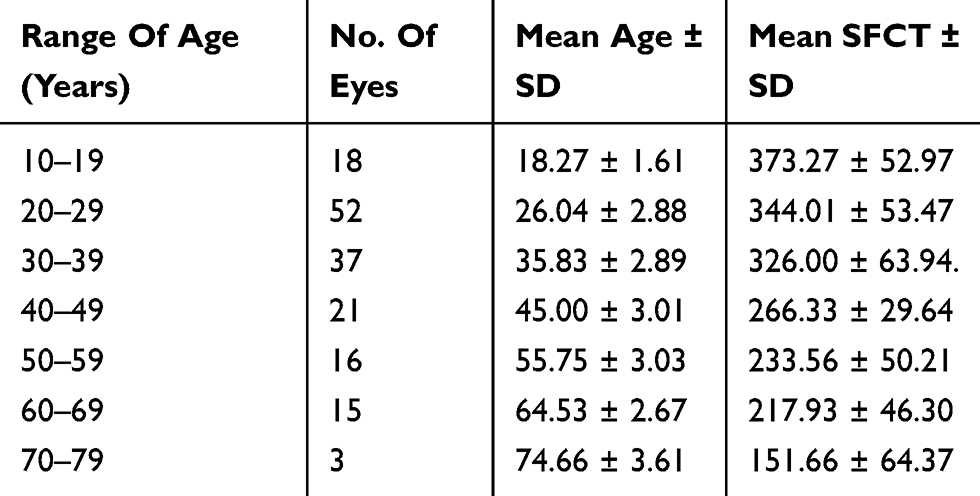 |
Table 1 Mean Age And Mean SFCT (RE) Of Participants In Different Age Groups |
 |
Table 2 Mean Age And Mean SFCT In Different Ethnic Groups |
The Mean Spherical Equivalent (MSE) refractive error in right eye (RE) and left eye (LE) was (0.89 ± 0.53) D and (0.94 ± 0.52) D respectively. The average axial length of both eyes was 23.51 ± 0.61 mm. SFCT of RE was 307.98 ± 74.64 µm (Figure 2) and that of LE was 312.63 ± 76.90 µm. In comparison, there was no statistically significant inter-eye difference of SFCT (p = 0.128). According to gender, SFCT in males and females was 305.49 ± 79.72 µm and 313.55 ± 70.76 µm respectively. Inter-gender differences of SFCT also had a statistically insignificant value (p = 0.51). The inter-ethnic variation of SFCT was also statistically non-significant (p = 0.74).
Hence, only data from RE were analyzed in relation to age, sex and ethnicity. On stratifying the cohort of participants into age groups of 10 years (Table 1), SFCT was found to be the highest in the age group 10–19 years with a value of 373.27 ± 53.35 µm, and minimum in the age group 70–79 years with a value of 151.66± 64.37 µm. SFCT was found to be negatively correlated with age (r = −0.705, p = 0.01) (Figure 3). Regression analysis showed thinning of SFCT by 3.50 ± 0.278 µm per year.
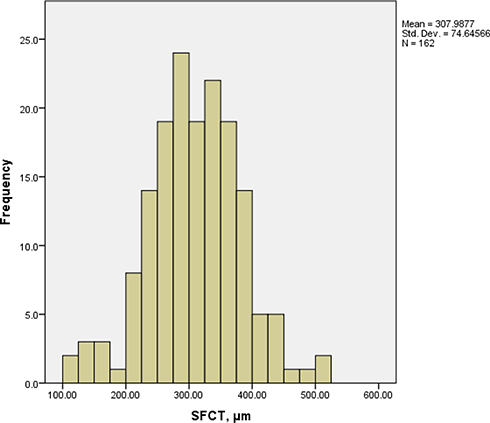 |
Figure 2 Histogram showing SFCT of the participants (RE only). |
 |
Figure 3 Scatter plot showing negative correlation between SFCT (RE) and Age (r = −0.705). |
Discussion
The choroidal layer is involved in the pathogenesis of different kinds of ocular diseases in the posterior segment of the human eye. Knowledge about CT is of utmost importance in the diagnosis and management of certain chorioretinal pathological conditions. The mean SFCT of the Nepalese population was found to be closer to the reported SFCT thickness of Singapore population6 (375.15 ± 6.58 µm), Japanese population7 (354 ± 111µm) and Spanish population8 (257.4 6 ± 99.3 µm). Reports by Chhablani et al9 from the Indian population measured SFCT o 216.4 ± 30.03 μm using Cirrus high definition (HD-OCT). These discrepancies between the findings of the Nepalese and Indian population might be due to racial differences and the use of different imaging devices (Cirrus high definition (HD) OCT, Carl Zeiss Meditec, Inc., Dublin, CA, USA. software Version 5.0.0.326). We used Heidelberg Spectralis OCT (Heidelberg, Germany) for choroidal imaging.
In the Nepalese population, SFCT showed strong negative correlation with age (r = −0.705, p = 0.001). A simple linear regression analysis showed thinning of SFCT by 3.50. ± 0.218 µm per year. This finding is closer to the data reported by Tuncer et al10 from Turkey which showed thinning of SFCT by 3.14 µm per year. However, Flores-Moreno et al8 reported thinning of SFCT by 2.6 µm per year. The thinning of SFCT with advancing age supports the idea of histologic studies, which showed a decrease in the vascular density and the diameter of capillary vessels in relation to age.11 It is hypothesized that, this very age related thinning of SFCT might account for various age related chorioretinal pathologies.
Though SFCT of the LE in our study was slightly greater than that of the RE, the inter-eye difference of SFCT was not statistically significant (p = 0.128). The finding is in accordance with the findings of Spaide et al.3 Also, SFCT was found to be slightly less in males than in females, however, the inter-gender difference was not statistically significant (p = 0.51). SFCT of the Muslim ethnic group was highest, followed by Gurung, Tamang, Chhetri, Newar, and Brahmin, but the difference of mean SFCT was not statistically significant (p = 0.74). Similar findings with statistically non-significant differences of SFCT were reported by Karapetyan et al12 among ethnic groups of whites, Africans and Asians.
There is no availability of data regarding the SFCT of the different ethnic groups of Nepal against which we could compare our findings. The potential limitations of this study include a small sample size which may not be enough to represent the entire Nepalese population and manual measurement of SFCT. Any further studies that will address the limitations of this study will bring more insights in understanding the SFCT of the Nepalese population.
Conclusion
The SFCT reported from this study is comparable to the data reported from other parts of the country. Further, our findings are in accordance with previous studies in demonstrating that SFCT decreases with increasing age. Nepalese male have thinner choroid than female. There is no significant inter-ethnic difference of SFCT in the healthy Nepalese population. The normative data of CT of the healthy Nepalese population reported from this study will be the baseline data to conduct future studies on the affected Nepalese population.
Acknowledgment
We would like to show our gratitude to Dr. Nabin Paudel, Centre for Eye Research, Technological University Dublin for sharing his pearls of wisdom during the course of this research. It was a privilege and great honour to receive his invaluable suggestions.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Barteselli G, Chhablani J, El‑Emam S, et al. Choroidal volume variations with age, axial length, and sex in healthy subjects: a three‑dimensional analysis. Ophthalmology. 2012;119:2572–2578.
2. Tan CS, Ouyang Y, Ruiz H, Sadda SR. Diurnal variation of Choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53:261–266. doi:10.1167/iovs.11-8782
3. Spaide RF, Koizumi H, Pozonni MC. Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol. 2008;146:496–500. doi:10.1016/j.ajo.2008.05.032
4. Guyer D, Schachat A, Green W. The Choroid: Structural Considerations. Retina.
5. Usui S, Ikuno Y, Akiba M, et al. Circadian changes in subfoveal choroidal thickness and the relationship with circulatory factors in healthy subjects. Invest Ophthalmol Vis Sci. 2012;53(4):2300–2307. doi:10.1167/iovs.11-8383
6. Gupta P, Saw S-M, Carol Y, et al. Choroidal thickness and high myopia: acase–control study of young Chinese men in Singapore. Acta Ophthalmol. 2015;93:e585–e592. doi:10.1111/aos.12631
7. Ikuno Y, Kawaguchi K, Nouchi T, Yasuno Y. Choroidal Thickness in Healthy Japanese Subjects.
8. Flores-Moreno I, Lugo F, Duker JS, Ruiz-Moreno JM. The relationship between axial length and choroidal thickness in eyes with high myopia. Am J Ophthalmol. 2013;155:314–319. doi:10.1016/j.ajo.2012.07.015
9. Chhablani J, Srinivasa Rao P, Venkata A, et al. Choroidal thickness profile in healthy Indian subjects. Indian J Ophthalmol. 2014;62:1060–1063. doi:10.4103/0301-4738.146711
10. Tuncer I, Karahan E, Zengin MO, Atalay E, Polat N. Choroidal thickness in relation to sex, age, refractive error, and axial length in healthy Turkish subjects. Int Ophthalmol. 2014. doi:10.1007/s10792-014-9962-4
11. Ramrattan RS, van der Schaft TL, Mooy CM, et al. Morphometric analysis of Bruch’s membrane, the choriocapillaris, and the choroid in aging. Invest Ophthalmol Vis Sci. 1994;35:2857–2864.
12. Karapetyan A, Ouyang P, Tang LS, Gemilyan M. Choroidal thickness in relation to ethnicity measured using enhanced depth imaging optical coherence tomography. Retina. 2016;36:82–90. doi:10.1097/IAE.0000000000000654
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.