")
Back to Journals » Infection and Drug Resistance » Volume 15
Study on the Detection and Infection Distribution of Multidrug-Resistant Organisms in Different Specimens
Authors Li Z, Zhang Y, Zhang W, Zhang Y, Zhou S, Chen W, Liu Y
Received 21 May 2022
Accepted for publication 3 October 2022
Published 14 October 2022 Volume 2022:15 Pages 5945—5952
DOI https://doi.org/10.2147/IDR.S375682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Zhanjie Li,1 Ying Zhang,2 Weihong Zhang,1 Yongxiang Zhang,1 Suming Zhou,3 Wensen Chen,1 Yun Liu4,5
1Department of Infection Control, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Infection Control, Lianshui County People’s Hospital, Huaian, People’s Republic of China; 3Department of Geriatric Critical Medicine, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 4Department of Information, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 5Department of Medical Informatics, School of BioMedical Engineering and Informatics, Nanjing Medical University, Nanjing, People’s Republic of China
Correspondence: Wensen Chen, Department of Infection Control, The First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China, Tel +86-13809049855, Email [email protected] Yun Liu, Department of Information, The First Affiliated Hospital of Nanjing Medical University, No. 300 Guang Zhou Road, Nanjing, People’s Republic of China, Tel +86-18805152008, Email [email protected]
Objective: To analyze the infection and distribution of multidrug-resistant organisms (MDRO) in different clinical specimens, thereby providing a reference for clinical diagnosis and treatment and prevention and control.
Patient and Methods: 2314 strains of MDRO isolated from clinical specimens in the First Affiliated Hospital of Nanjing Medical University from January to December 2020. MDRO were collected by Information System. The detection rate of MDRO, infection rate, the proportion of infection, and detection rate of MDRO infection in different specimens were analyzed.
Results: The top three specimens in the detection rate of MDRO were BALF (60.71%), sputum (33.68%), and blood (28.79%). The top three specimens in the proportion of MDRO infection were blood (97.74), other sterile body fluids (90.35%), and BALF (90.20%). The top three specimens in the MDRO infection rate were BALF (9.75%), sputum (3.07%), and secretions (2.90%). The top three specimens in the detection rate of MDRO infection were sputum (0.63‰), other sterile body fluids (0.13‰), and secretions (0.11‰).
Conclusion: The detection and infection distribution of MDRO vary greatly in different specimens. The submission of sterile body fluids for examination should be strengthened and the standard of sample collection should be highlighted.
Keywords: different specimens, MDRO, detection rate, infection, sterile body fluids
Introduction
In the past century, antibacterial drugs have played a key role in the fight against multiple infectious diseases in humans. However, the increasingly prominent multidrug-resistant organisms (MDRO) have brought severe challenges to clinical anti-infectious therapy.1 MDRO infection not only exacerbates the suffering of patients, increases the difficulty of treatment, slows down the recovery speed, but also prolongs the length of hospital stay, increases the cost of hospital stay, and even raises the clinical mortality.2–4 Inhibiting the development of MDRO and blocking the spread of MDRO have attracted extensive attention worldwide and also become significant obstacles for clinical medical staff and management departments at all levels to improve medical quality.5,6 At present, the overall detection and infection of MDRO have been well-documented in the existing studies, but how to further promote the fine management of MDRO and achieve precise prevention and control and medication is still worth further exploration.7–9 It has been reported that compared with MDRO colonization or infection, different culture sites have a greater impact on clinical results.10 This study retrospectively analyzed the detection and infection distribution of MDRO in different specimens of a large-scale general hospital at Grade III Level A, with the aim to provide a specific reference basis for clinical diagnosis and treatment and prevention and control of nosocomial infection.
Materials and Methods
Research Objects
73,680 specimens from 158,051 inpatients in the First Affiliated Hospital of Nanjing Medical University from January to December 2020 were collected, of which 2314 strains of MDRO isolated by the clinical microbiology laboratory were selected as the research objects, including Methicillin-Resistant Staphylococcus Aureus (MRSA), Carbapenem-Resistant Enterobacteriaceae (CRE), Carbapenem-Resistant Acinetobacter Baumannii (CRAB), and Carbapenem-Resistant Pseudomonas Aeruginosa (CRPA). Duplicate strains in the same site of the same patient were eliminated.This study was approved by the hospital ethics committee and exempted from informed consent (2019-SR-075).
Research Methods
The specimens submitted for examination in the whole hospital from January to December 2020 were collected by Xinglin Real-Time Nosocomial Infections System and Laboratory Information System (LIS) and divided into 6 categories according to the source of the specimens, including 1) sputum (43.96%), 2) blood (17.77%), 3) urine (15.23%), 4) secretions (pus, wound secretion, etc.)(8.32%), 5) bronchoalveolar lavage fluid (BALF)(1.92%), 6) other sterile body fluids (cerebrospinal fluid, pleural fluid, ascites, bile, etc.) (12.79%). The MDRO detection rate, MDRO infection rate, the proportion of MDRO infection, and detection rate of MDRO infection in different specimens were compared and analyzed.
Diagnostic Criteria of Infection
The diagnostic criteria of nosocomial infection adopted the Diagnostic Criteria of Nosocomial Infection (Trial) issued by the Ministry of Health in 2001.11 The judgment criteria of MDRO infection adopted the unified consensus of international experts.12
Calculation Formula
MDRO detection rate = (number of MDRO strains/number of strains corresponding to the pathogen) × 100%; MDRO infection rate = (number of MDRO infections/number of specimens submitted for examination in the same period) × 100%; the proportion of MDRO infection = (number of MDRO infection cases/number of specific MDRO cases detected in the same period) × 100%; detection rate of MDRO infection = (number of MDRO infection cases/total number of inpatients in the same period) × 1000‰.
Bacterial Identification and Antimicrobial Susceptibility Test
Bacterial identification was performed using the VITEK-2 CompactV automatic bacterial identification instrument (Bio Mérieux, France) or API identification system (Bio Mérieux, France). Kirby-Bauer method (Oxide, Japan) was used in the antimicrobial susceptibility test. The infection point of inhibition zone in the Kirby-Bauer disk diffusion test and antimicrobial susceptibility results were interpreted according to the standards formulated by the Clinical and Laboratory Standards Institute (CLSL) in 2020.13 The quality control strains (Clinical Laboratory Center of National Health and Family Planning Commission) are as follows: Escherichia coli (ATCC 25922), Klebsiella pneumoniae (ATCC 700603), Staphylococcus aureus (ATCC 25923), Acinetobacter baumannii (ATCC 19606), Pseudomonas aeruginosa (ATCC 278553), and Enterobacter cloacae (ATCC 700323).
Statistical Analysis
WPS 2019 software was used for data statistics and SPSS 23.0 software was used for data analysis. The enumeration data were expressed in frequency and percentage. Chi-square test or Fisher exact probability test was adopted for the comparisons among multiple groups. A value of P < 0.05 was indicated of statistical significance.
Results
Detection Rate of MDRO in Different Specimens
The top three specimens in the detection rate of MDRO were BALF (60.71%), sputum (33.68%), and blood (28.79%) (P < 0.001). There were significant differences in the detection rates of different MDRO in different specimens (all P < 0.001). The top three specimens in the CRAB detection rate were BALF (89.47%), other sterile body fluids (79.27%), and blood (68.63%); the top three specimens in the CRE detection rate were BALF (42.11%), blood (18.95%), and sputum (17.47%); the top three specimens in the CRPA detection rate were other sterile body fluids (39.13%), blood (38.71%), and BALF (37.50%); the top three specimens in the MRSA detection rate were other sterile body fluids (71.93%), BALF (71.43%), and sputum (63.24%). The sputum specimens and MDRO-positive sputum specimens accounted for the highest proportion of all specimens (52.32% and 60.98%). Table 1 shows the detailed information.
 |
Table 1 Detection Rate of MDRO in Different Specimens |
Proportion of MDRO Infection in Different Specimens
The top three specimens in the proportion of MDRO infection were blood (97.74%), other sterile body fluids (90.35%), and BALF (90.20%) (P<0.001). There were significant differences in the proportion of MDRO infection in different specimens (all P < 0.05). As shown in Table 2, the top three specimens in the proportion of CRAB infection were blood (97.14%), other sterile body fluids (93.85%), and BALF (88.24%); the top three specimens in the proportion of CRE infection were blood (100%), secretions (94.74%), and BALF (87.50%); the top three specimens in the proportion of CRPA infection were BALF (100%), other sterile body fluids (85.19%), and blood (83.33%); the top three specimens in the proportion of MRSA infection were BALF (100%), blood (100%), and other sterile body fluids (95.12%).The details are shown in Table 2
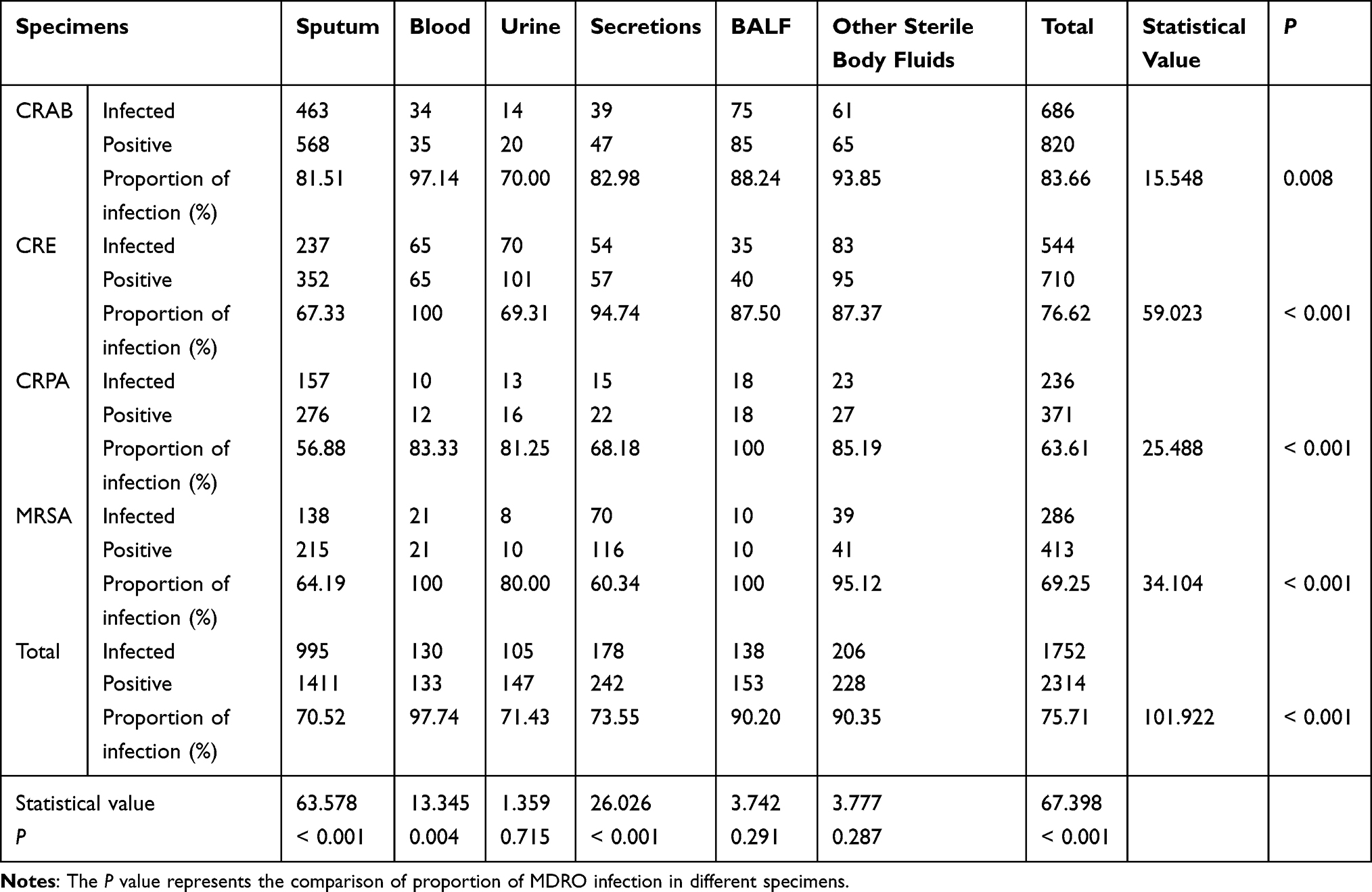 |
Table 2 Proportion of MDRO Infection in Different Specimens |
Infection Rate of MDRO in Different Specimens
The top three specimens in the MDRO infection rate were BALF (9.75%), sputum (3.07%), and secretions (2.90%) (P < 0.001). There were significant differences in the MDRO infection rate in different specimens (all P < 0.001). The top three specimens in the CRAB infection rate were BALF (5.30%), sputum (1.43%), and other sterile body fluids (0.65%); the top three specimens in the CRE infection rate were BALF (2.47%), other sterile body fluids (0.88%), and secretions (0.88%); the top three specimens in the CRPA infection rate were BALF (1.27%), sputum (0.48%), and other sterile body fluids (0.24%); the top three specimens in the MRSA infection rate were secretions (1.14%), BALF (0.71%), and sputum (0.43%). The details are shown in Table 3.
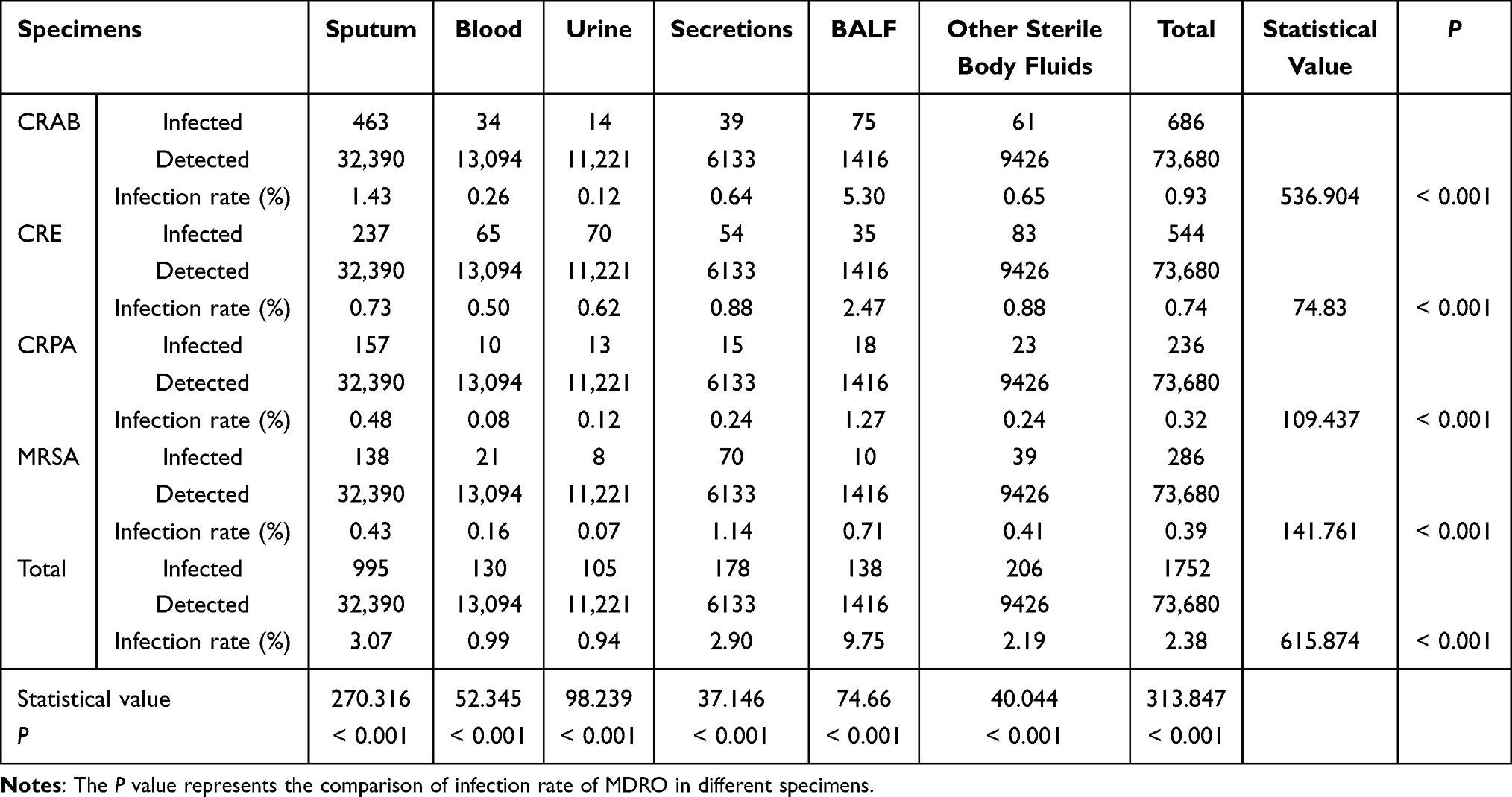 |
Table 3 Infection Rate of MDRO in Different Specimens |
Detection Rate of MDRO Infection in Different Specimens
The top three specimens in the detection rate of MDRO infection were sputum (0.63‰), other sterile body fluids (0.13‰), and secretions (0.11‰) (P < 0.001). There were significant differences in the detection rate of MDRO infection in different specimens (all P < 0.001). As shown in Table 4, the top three specimens in the detection rate of CRAB infection were sputum (2.93‰), BALF (0.48‰), and other sterile body fluids (0.39‰); the top three specimens in the detection rate of CRE infection were sputum (1.50‰), other sterile body fluids (0.53‰), and urine (0.44‰); the top three specimens in the detection rate of CRPA infection were sputum (0.99‰), other sterile body fluids (0.15‰), and BALF (0.11‰); the top three specimens in the detection rate of MRSA infection were sputum (0.87‰), other sterile body fluids (0.25‰), and blood (0.13‰).The details are shown in Table 4.
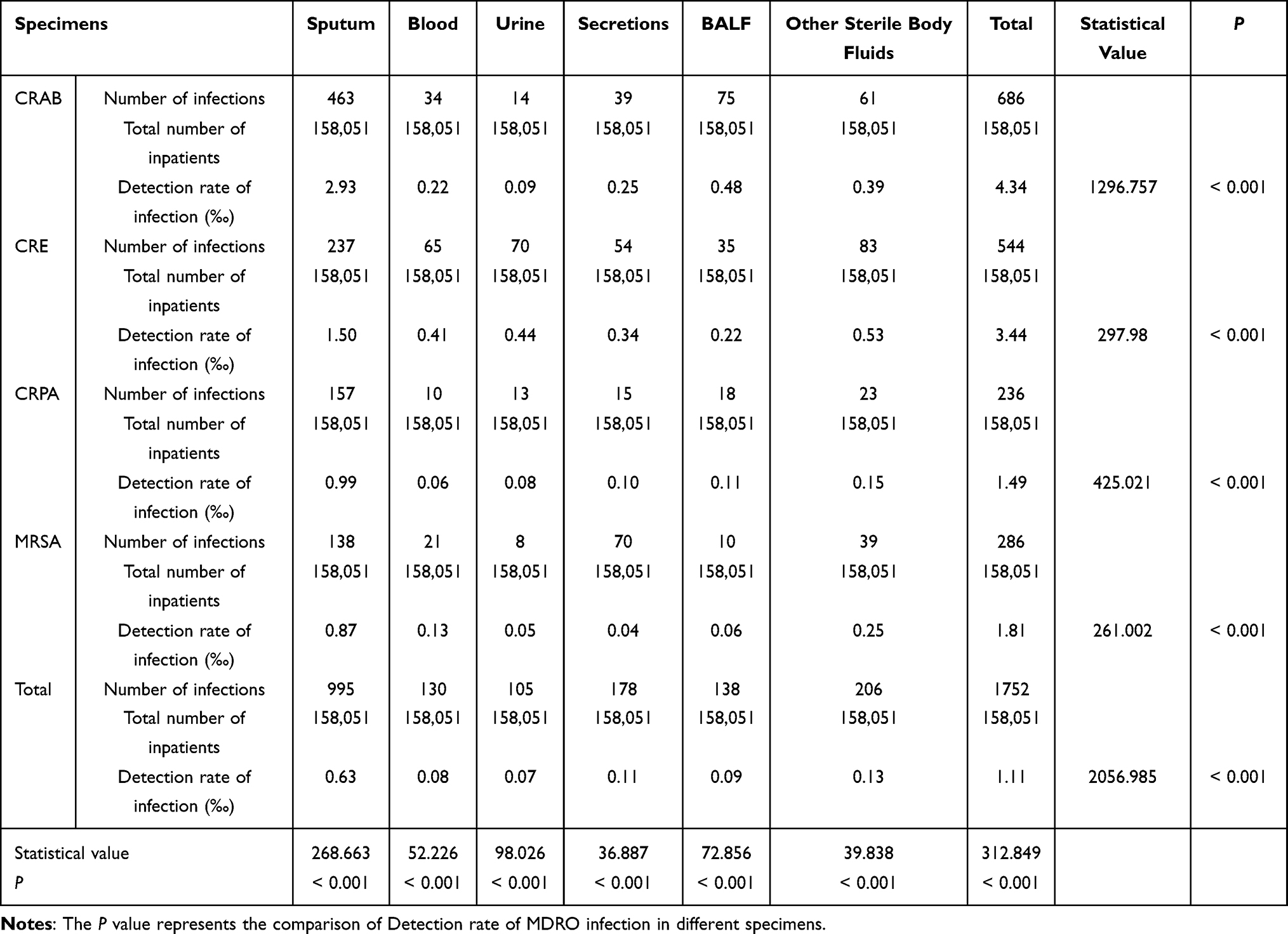 |
Table 4 Detection Rate of MDRO Infection in Different Specimens |
Discussion
This study demonstrated that the detection rate of MDRO in BALF specimens (60.71%) was the highest, nearly twice higher than that in sputum specimens (33.68%). The specimens with the highest detection rates of four kinds of MDRO were mainly sterile body fluids including BALF, blood, and other sterile body fluids, which was basically consistent with the data in the China Antimicrobial Resistance Surveillance System (CARSS).14,15 The detection rates of CRAB, CRE, CRPA, and MRSA in BALF specimens in our hospital were 89.47%, 42.11%, 37.50%, and 71.43% respectively, which were higher than 80.4%, 21.5% (CRKP, Carbapenem-resistant Klebsiella Pneumoniae), 26.5%, and 37.9% recorded in CARSS in 2019. The possible reason may be that CARSS members are national medical institutions at Grade II and above, while our hospital is at Grade III Level A with the strongest comprehensive strength in Jiangsu Province. Hence, the average critical degree of patients in our hospital is higher and more invasive operations are involved. Meanwhile, it also reflects that the detection rate of MDRO is underestimated due to the low proportion of sterile body fluids submitted for examination, which needs further attention. Moreover, the detection rate of MDRO in urine specimens (11.08%) was the lowest, which was similar to the results of Howard-Anderson et al.10 The proportion of infection can better reflect the proportion of pathogen infection in different specimens, and pathogenic bacteria are the pathogens that need to be found mostly in the process of clinical diagnosis and treatment to guide the use of antibiotics. This study showed that the top three specimens in the proportion of MDRO infection were all sterile body fluids (blood, other sterile body fluids, and BALF), with the proportion of infection over 90%, which was much higher than that of other specimens (70.25–73.55%), implying the higher diagnostic and guiding values of sterile body fluids in clinical diagnosis and treatment. Early identification of pathogenic bacteria is an important reference for the transformation from empirical medication to targeted treatment, and optimizing antibacterial drug therapy can reduce the risk of bacterial resistance.16 Barnes et al17 have found a correlation between bacterial resistance and antimicrobial usage in intensive care settings.18 Up to 50% of the course of antibacterial drug therapy may be inappropriate, and even a modest reduction in the usage of antibiotics can reduce the transmission of MDRO.
Moreover, this study demonstrated that sputum specimens accounted for 52.32% (4189/8006) of the total specimens and the number of MDRO infections accounted for 60.98% (1411/2314), more than the sum of other specimens, which were consistent with the data in the CARSS.19 The most common specimens for etiological examination of lower respiratory tract infection are sputum and BALF specimens. Sputum specimens are easy to be contaminated by oral colonization bacteria, but under normal circumstances, the alveoli are sterile. BALF specimens are the alveolar surface liquid collected after lavage of the pulmonary segment and subpulmonary segment by bronchoscope.20 Compared with sputum specimens, BALF specimens have higher sensitivity and specificity in the diagnosis of lower respiratory tract infection, less possibility of contamination, and a higher bacterial isolation rate. Compared with sputum, BALF specimens have higher sensitivity and specificity for the diagnosis of lower respiratory tract infection, less possibility of contamination, and high bacterial isolation rate, and their bacterial drug sensitivity results have greater significance in guiding the anti-infective treatment of the lower respiratory tract,14,21 which suggests that more sterile body fluid specimens such as BALF and blood should be sent for examination to identify pathogens early to guide the rational use of antibiotics.
In terms of the infection rate of MDRO, BALF specimens still ranked first (9.75%), followed by sputum specimens (3.07%) and secretion specimens (2.90%). The detection rate of infection in sputum specimens ranked first (0.63 ‰), which was related to the highest proportion of respiratory tract infection in all infections. At the same time, it also indicates that sputum specimens have great value in the diagnosis of infection as long as standardized collection and examination can be guaranteed.22 In addition, the collection of sputum specimens is relatively convenient and has wide application and operability in practical work. A domestic status survey23 has pointed out that in 2010, 63.10% of the clinical microbiology laboratory in hospitals conducted sputum smear microscopic examination of sputum culture and in 2015, 87.17% of the clinical microbiology laboratory carried out this project. In 2015, 88.34% of sputum smear reports described the ratio of white blood cell count (WBC) to epithelial cells and the morphology of pathogens, and 62.58% described the phagocytosis of WBC. It not only reflects the progress in laboratory quality control of sputum specimens but also embodies the importance of standardized collection and examination.
This research involves a retrospective design, and there are still some limitations. Firstly, this study spans only 1 year and needs to include a longer period of study subjects to be more convincing.Secondly, this study included microbiological specimens from all inpatients, but did not distinguish between ICU (Intensive Care Unit) and non-ICU inpatients and could not precisely capture their differences.In the future, we will expand the study period and further investigate the detection and infection of MDRO in different specimens among different departments.
Conclusion
To sum up, there are significant differences in the detection and infection distribution of MDRO in different specimens. The detection rate and infection rate of MDRO in sterile body fluids are relatively high, which has greater clinical guiding value. Moreover, sputum specimens and other non-sterile specimens collected and examined in a standardized manner also have certain reference significance. Hence, the examination of sterile body fluids should be strengthened and the standard of sample collection should be highlighted. It also provides reference for the antimicrobial drug management team to effectively guide the rational application of antimicrobial drugs, curb the spread of drug-resistant bacteria, and ensure medical safety.
Abbreviation
MDRO, Multidrug-resistant organisms; MRSA, Methicillin-Resistant Staphylococcus Aureus; CRE, Carbapenem-Resistant Enterobacteriaceae; CRPA, Carbapenem-Resistant Pseudomonas Aeruginosa; LIS, Laboratory Information System; CLSL, Clinical and Laboratory Standards Institute; WBC, White blood cell count; CRKP, Carbapenem-resistant Klebsiella Pneumoniae; ICU, Intensive Care Unit.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethical Statement
We carried out this study according to the revised Declaration of Helsinki, and this study was approved by the hospital ethics committee and exempted from informed consent (2019-SR-075).Because the study was retrospective and the study followed only the drug resistance of the specimens and did not involve other information about the patients, the ethical application for exemption from informed consent was passed.
Acknowledgment
We would like to acknowledge the reviewers for their helpful comments on this paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Zhanjie Li and Ying Zhang are co-first authors.
Funding
This work was supported by the industry prospecting and common key technology key projects of Jiangsu Province Science and Technology Department (grant No. BE2020721), Project of Evidence-Based Evaluation and Demonstration Base Construction of Infection Control Measures in Medical Institutions of the Health Development Research Center of the National Health Commission (2020-53) and the Clinical Capability Improvement Project of Jiangsu Province Hospital (JSPH-MB-2020-10); Nanjing Life and Health Technology Special Project ”Cooperative research, development and transformation of active intelligent health management platform for diabetes mellitus” (202205053);Industrial chain collaborative innovation Project of Ministry of Industry and Information Technology ”Multi-modal medical data intelligent management software for the new generation of information technology” (TC210804V);The Industrial and Information Industry Transformation and Upgrading Special Fund of Jiangsu Province in 2021 (Grant no. [2021]92)) ;The Key Project of Smart Jiangsu in 2020 (Grant no. [2021]1) ;Jiangsu Province Engineering Research Center of Big Data Application in Chronic Disease and Intelligent Health Service (Grant no.[2020]1460).The funders had an important role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Mücke MM, Mayer A, Kessel J, et al. Quinolone and multidrug resistance predicts failure of antibiotic prophylaxis of spontaneous bacterial peritonitis. Clin Infect Dis. 2020;70(9):1916–1924. doi:10.1093/cid/ciz540
2. Kronenfeld N, Zilberman-Itskovich S, Lazarovitch T, et al. The impact of improper empirical usage of antipseudomonals on admission to an acute care hospital. J Glob Antimicrob Resist. 2020;22:5–8. doi:10.1016/j.jgar.2019.12.013
3. Chen YY, Wu PF, Chen CS, Chen IH, Huang WT, Wang FD. Trends in microbial profile of burn patients following an event of dust explosion at a tertiary medical center. BMC Infect Dis. 2020;20(1):193. doi:10.1186/s12879-020-4920-4
4. Wang L, Huang X, Zhou J, et al. Predicting the occurrence of multidrug-resistant organism colonization or infection in ICU patients: development and validation of a novel multivariate prediction model. Antimicrob Resist Infect Control. 2020;9(1):66. doi:10.1186/s13756-020-00726-5
5. Octaria R, Chan A, Wolford H, et al. Web-based interactive tool to identify facilities at risk of receiving patients with multidrug-resistant organisms. Emerg Infect Dis. 2020;26(9):2046–2053. doi:10.3201/eid2609.191691
6. Chen HY, Jean SS, Lee YL, et al. Carbapenem-resistant enterobacterales in long-term care facilities: a global and narrative review. Front Cell Infect Microbiol. 2021;11:601968. doi:10.3389/fcimb.2021.601968
7. Li ZJ, Wang KW, Liu B, et al. The distribution and source of MRDOs infection: a retrospective study in 8 ICUs, 2013–2019. Infect Drug Resist. 2021;14:4983–4991. doi:10.2147/IDR.S332196
8. Zang F, Zhang YX, Liu B. Distribution and sources of elderly intensive care unit patients with multidrug-resistant organisms infections. Chin J Nosocomiol. 2020;30(06):866–871.
9. Li ZJ, Liu B, Li HF, et al. Study on distribution and source of multi-drug resistant bacteria infection in ICUs. Chin J Nosocomiol. 2019;29(08):1166–1171.
10. Howard-Anderson JR, Adams C, Dube WC, et al. Poor outcomes in both infection and colonization with carbapenem-resistant Enterobacterales. Infect Control Hosp Epidemiol. 2022;2:1–7.
11. HMo C. Diagnostic criteria for nosocomial infection (Trial). Chin Med J. 2001;2001(5):61–67.
12. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
13. (CLSI) Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing.
14. China Antimicrobial Resistance Surveillance System. Antimicrobial resistance of bacteria from bronchoalveolar lavage fluid: a surveillance report from china antimicrobial resistance surveillance system in 2014–2019. Chin J Infect Control. 2021;20(01):61–69.
15. Committee of Expert on Rational Drug Use of the National Health Commission. China antimicrobial resistance surveillance system, national bacterial drug resistance surveillance report in 2020; 2020. Available from: http://www.carss.cn/Report/Details?aId=808.
16. Bassetti S, Tschudin-Sutter S, Egli A, Osthoff M. Optimizing antibiotic therapies to reduce the risk of bacterial resistance. Eur J Intern Med. 2022;22:00039–00045.
17. Barnes SL, Rock C, Harris AD, Cosgrove SE, Morgan DJ, Thom KA. The impact of reducing antibiotics on the transmission of multidrug-resistant organisms. Infect Control Hospital Epidemiol. 2017;38(06):663. doi:10.1017/ice.2017.34
18. Baditoiu L, Axente C, Lungeanu D, et al. Intensive care antibiotic consumption and resistance patterns: a cross-correlation analysis. Ann Clin Microbiol Antimicrob. 2017;16(1):71. doi:10.1186/s12941-017-0251-8
19. China Antimicrobial Resistance Surveillance System. Antimicrobial resistance of bacteria: a surveillance report from China Antimicrobial Resistance Surveillance System in 2014–2019. Chin J Infect Control. 2021;20(01):15–31.
20. Wei LH, Cui YL, Zhang HJ, et al. Distribution and drug resistance of bacteria isolated from bronchoalveolar lavage fluid in 74 hospitals of Gansu Province. Chin J Nosocomiol. 2021;31(22):3402–3406.
21. Zhang Z, Tian L, Chen ZJ. Distribution and antimicrobial resistance of pathogens causing lower respiratory tract infection in patients in a hospital, 2013–2015. Chin J Infect Control. 2017;16(6):516–520.
22. Respiratory Committee of Chinese Research Hospital Society, Expert Opinion Compilation Group on etiological diagnosis of adult respiratory infectious diseases. Expert opinion on the etiological diagnosis of adult respiratory infectious diseases. Chin J Tuberc Respir Dis. 2020;43(09):757–764.
23. Xu Y, Yang H, Chen LY, et al. Current situation of Chinese clinical microbiological laboratories participating in the management of healthcare-associated infection and antimicrobial use. Chin J Infect Control. 2019;18(02):120–126.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.