")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Study of the possibility of introduction of Kazakhstan NGO-based rapid HIV testing procedures
Authors Alibayeva KO, Saparbekov MK, Baiserkin BS, Abishev AT, Tazhibaeva GH, Kasymbekova SZ
Received 22 April 2019
Accepted for publication 19 August 2019
Published 11 September 2019 Volume 2019:11 Pages 219—227
DOI https://doi.org/10.2147/HIV.S212718
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
KO Alibayeva,1 MK Saparbekov,1 BS Baiserkin,2 AT Abishev,2 GH Tazhibaeva,2 SZ Kasymbekova2
1Department of Public Health and Social Sciences, Kazakhstan School of Public Health, Kazakhstan Medical University, Almaty, Republic of Kazakhstan; 2Organization and Methodical Department, Reference Laboratory, Republican Center on Prevention and Control of AIDS, Almaty, Republic of Kazakhstan
Correspondence: KO Alibayeva
Kazakhstan’s Medical University “Kazakhstan School of Public Health”, 19A Utepov Street, Almaty 050060, Republic of Kazakhstan
Tel +7 701 778 6509
Email [email protected]
Introduction: New initiatives presented by the World Health Organization (WHO) and the Joint United Nations Program on HIV and AIDS , such as 90-90-90, test and treat, preventive treatment, and best international practices related to the introduction of rapid human immunodeficiency virus (HIV) testing in clinics, and field conditions, including self-testing, predetermined the introduction of NGO-based rapid HIV testing in the Republic of Kazakhstan nongovernmental organizations (NGOs). This work presents the results of a comprehensive study conducted about the possible introduction of NGO-based rapid HIV testing in the country. It should be noted that 32,573 HIV infections have been diagnosed in Kazakhstan (prevalence of 117.7 per 100,000 people) from 1987 to 2018. Most of these new cases are diagnosed among “key” population groups, such as people who use injectable drugs, sex workers, men who have sex with men, those who rely mainly on NGOs, and those who prefer to deal with an organization such as an NGO, which makes it possible to introduce NGO-based rapid HIV testing in Kazakhstan.
Methods: In this work, we used the following rapid HIV tests: Alere DetermineTM HIV ½ Ag/Ab Combo, Hexagon HIV 1+2, Abon HIV ½, HIV 1,2 Han Medtest, and Geenius HIV1/2 Confirmatory.
Results: The study of the rapid tests, including their diagnostic patterns, conducted in Kazakhstan shows that five rapid HIV tests completely meet the WHO’s requirements (sensitivity>99%; specificity>98%). These are Alere DetermineTM HIV ½ Ag/Ab Combo, Hexagon HIV 1+2, Abon HIV ½, HIV 1,2 Han Medtest, and Geenius HIV1/2 Confirmatory. The study of legal and social problems associated with rapid HIV testing in NGOs shows that HIV-related medical examination and counseling carried out in Kazakhstan, including those by rapid methods, are governed by corresponding laws and normative legal documents.
Conclusion: It has been established that there are social barriers that interfere with rapid HIV testing. In view of this, services associated with NGO-based rapid HIV testing shall be rendered with the use of a social and legal protection mechanism for those under examination.
Keywords: rapid HIV testing, NGO, key population groups, HIV infection, Republic of Kazakhstan
Introduction
As of January 1, 2018, 32,573 Human Immunodeficiency Virus (HIV) cases were diagnosed in Kazakhstan, among them, PLHIV (people living with HIV) were 20,841, 117.7 per 100,000 people. The highest PLHIV prevalence were observed in Pavlodar, Karaganda, Kostanay Regions, and in Astana. According to the International Bank for Reconstruction and Development (2015), the HIV epidemic in the countries of Central Asia, including Kazakhstan, is still at its “concentrated” stage where most of new HIV cases are diagnosed among “key” population groups, particularly among people who use injectable drugs (PUIDs), men who have sex with men (MSM), prisoners, sex workers (SWs), and their clients. If these current trends, such as a lack of changes in the “key” population groups’ behavior and low coverage by preventive programs, are maintained, it is expected that during 2015–2020 new HIV cases will increase by 13% and AIDS-related deaths by 32%. It is also expected that PUIDs and MSM will be 67% of all new HIV cases.1
The studies conducted outside the Republic of Kazakhstan show that among “key” population groups HIV serological status is usually associated with a behavioral model of men and women with high risks, sexual relations, and drug addiction. For example, according to S.A. Strathdee et al (2010, 2011), A. Krusi et al (2010), there are many behavioral factors that give rise to HIV among PUIDs, including a lack of access to sterile needles, syringes, a fear of becoming subject to discrimination, arrest, imprisonment, the presence of barriers preventing them from receiving testing, HIV, and drug addiction treatment services.2–4 This opinion is generally shared by other authors.5–7 The study by N. EL-Bassel et al (2013) conducted in Almaty, Kazakhstan, among 728 injecting drug users and their intimate partners convincingly shows that the HIV prevalence among women and men who are PUIDs is 28%, which is considerably higher than the HIV prevalence according to the official report on integrated HIV bio-behavioral surveillance.8 The authors note that only 10% of the participants have ever used a needle and syringe exchange program, and 25.3% have never been tested for HIV. The same situation is observed among SWs. For example, according to the US President’s Emergency Plan for AIDS Relief (PEPFAR) 2016 for Central Asia, researchers (2013–2014) used the TraC methods and showed that the HIV prevalence among SWs who had reported about their injection drug use experience in these three Central Asian countries (Kazakhstan, Kyrgyzstan, and Tajikistan) would exceed similar values among those SWs who had not practiced this type of high-risk behavior by 20 times.9 The PEPFAR experts note that, regardless of a high demand for HIV testing and counseling services, a considerable number of SWs are not regularly tested for HIV in the Central Asian regions under consideration.
MSM are one of the most important “key” population groups that is strongly affected by the HIV epidemic in Kazakhstan. Let us note that the HIV prevalence in this population category is of contradictory nature. If the official figures of Kazakhstan show that the HIV prevalence among the MSM population is 3.16%, then the work by M. Berry et al (2012) indicates that only in Almaty, Kazakhstan, the HIV prevalence reaches 20.2%.10 This wide variations information about HIV prevalence and the MSM population is most probably connected with low-quality studies, a lack of representativeness in the selection of MSM as well as stigma and discrimination existing in this population group.
Therefore, from the epidemiological point of view, there are convincing reasons why HIV/AIDS control programs to be implemented in Kazakhstan shall be particularly focused on “key” population groups.
Currently is a better word, the Joint United Nations Programme on HIV/AIDS (UNAIDS) adopted a new “90-90-90” strategy for counteraction with the spread of HIV infection.11 By 2020, according to this strategy aimed at ending the AIDS epidemic in the world, 90% of all PLHIV will know their HIV status, 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy, 90% of all people receiving antiretroviral therapy will have viral suppression. In this regard, the Republic of Kazakhstan is taking measures to improve and extend access to NGO-based rapid HIV testing and early HIV treatment among “key” population groups.
The objective of this study is to identify the possibility of introduction of NGO-based rapid HIV testing with whole blood in Kazakhstan. For this purpose, Kazakhstan’s Medical University “KSPH”, together with specialists the Republican Center on Prevention and Control of AIDS, the Kazakhstan Union of PLHIV NGO in partnership with international organizations have initiated a comprehensive study of the possibility of introduction of NGO-based rapid testing. In addition to the search of feasibility and applicability of NGO-based rapid testing methods in East Kazakhstan and Pavlodar Regions, they have organized such activities as rapid testing for PLHIV and practical training for nongovernmental organization (NGOs)’ employees. Patients with positive HIV test results are brought to the Territorial Center for Prevention and Control of AIDS in order to establish their final HIV status and receive early treatment.
Materials and methods
Materials
The following information has been used in order to analyze the facts of feasibility and applicability of NGO-based rapid HIV testing procedures:
- Best practices from different countries, world literature describing the introduction of rapid HIV testing methods into national health care systems;
- Results of our validation assessment of the quality of the five rapid tests registered in Kazakhstan and made by different manufacturing companies;
- Analytical study of the applicable legislative and normative legal documents of the Republic of Kazakhstan that govern HIV testing procedures;
- Materials of the sociological studies aimed at assessing the possible barriers interfering with Kazakhstan NGO-based rapid HIV testing.
- The laboratory part of this study was carried out during 2015–2017 with advisory, technical and financial support from the Center for Disease Control and Prevention (CDC).
Methods
Assessing the quality parameters of rapid tests
This fragment of the study was carried out within the premises of the reference laboratory of the Republican Center for Prevention and Control of AIDS.
All rapid HIV test manufacturers registered in Kazakhstan were requested to participate in this study. Only five companies agreed to take part. We validated the following rapid HIV tests:
- Alere DetermineTM HIV ½ Ag/Ab Combo;
- Hexagon HIV 1+2;
- Abon HIV ½;
- HIV 1,2 Han Medtest;
- Geenius HIV1/2 Confirmatory.
The study used two series of each test.
Two panels were created: 1) a panel of native serum samples that included 300 HIV-positive and 300 negative serum or plasma samples; and 2) a panel of titrated serum or plasma samples prepared by 4-time dilutions of 10 HIV-positive serum samples.
The samples of both panels were tested by two IFA tests:
- Genscreen Ultra HIV Ag-Ab (Bio-Rad, France) – is a fourth-generation enzyme immunoassay based on the principle of the sandwich technique for the detection of HIV antigen and of the various antibodies associated with HIV-1 and/or HIV-2 virus in human serum or plasma.
- Murex HIV Ag/Ab (Diasorin, Italy) – is an enzyme immunoassay for the simultaneous qualitative detection of HIV p24 antigen and antibodies to HIV type 1 (HIV-1 group O) and HIV type 2 (HIV-2) in human serum or plasma.
The tests were carried out in parallel. The samples not reactive in both IFA tests were considered to be negative. All ones reactive according to the results of both IFA tests were confirmed by the New Lablot immunoblot (Bio-Rad, France). The samples reactive in both IFA tests and the immunoblot were considered to be positive. Each sample of the panels was tested with the use of at least two different series of each rapid test system under study in order to assess their variability.
Data analysis
When assessing the quality of the rapid tests, we used the methods specified by the WHO for similar studies.12 The sensitivity, specificity, predictive value of the positive and negative results of each rapid test were calculated on the basis of comparisons with the results of the confirming test with the use of the 2×2 table and retrospective data on the HIV prevalence among the main population groups of the Republic of Kazakhstan. Accurate 95% confidence intervals for binomial relations were calculated on the basis of Fisher’s F-distribution at the relation tending to 1.0. The variability of the testing results was considered as a relation of the quantity of samples with ambiguous interpretation of the total number of samples. In order to calculate the sensitivity and specificity of the test, we used only those samples that were identified as positive or negative when using the test considered to be “gold standard” (IFA-IFA-immunoblot). In order to assess the quality of the rapid tests under study, we used the criteria proposed by the WHO: clinical sensitivity –>99%; clinical specificity – >98%; variability of results from operator to operator – ≤5%; variability of results from series to series – ≤2%; invalid results – ≤1%.
Analyzing the legislative and regulatory acts of the Republic of Kazakhstan
In light of the forthcoming introduction of NGO-based rapid HIV testing procedures, we analyzed the following main legislative normative legal documents:
- The Constitution of the Republic of Kazakhstan (dated August 30, 1995, as amended and supplemented).
- The Code of the Republic of Kazakhstan “On the People’s Health and Healthcare System” (2009).
- Law No. 202-V dated May 16, 2014, of the Republic of Kazakhstan “On Permits and Notices”
- Order No. 508 dated June 23, 2015, of the Ministry of Health of the Republic of Kazakhstan “On the Approval of the Rules of Compulsory Confidential Medical Examination for HIV as per Clinical Indications”.
- The Law of the Republic of Kazakhstan “On Prevention of AIDS” (1994).
- Order No. 246 dated April 22, 2016, of the Ministry of Health of the Republic of Kazakhstan “On the Approval of the Rules of Voluntary Anonymous and (or) Confidential Medical Examination and Consultation of the RoK citizens and Migrants Regarding HIV Infection on a Paid Basis”.
- Order No. 115 dated February 28, 2013, “On the Introduction of Amendments to Order No. 228 dated March 9, 2004, of the Ministry of Health of the Republic of Kazakhstan “On the Approval of the Regulations on Organization of Drop-In Centres’ Activities for Injection Drug Users”
Sociological studies
The field studies of the barriers interfering with the introduction of NGO-based rapid HIV testing were conducted in the following seven regional centers of Kazakhstan: Pavlodar, Kostanay, Ust-Kamenogorsk, Temirtau, Shymkent, Almaty. The following NGOs were involved in the sociological studies: 1) “Ty ne odin”, “Gerlita” (Pavlodar), “Kuat”, “Answer” (Ust-Kamenogorsk), “Kuat” (Shymkent), “Shapagat” (Karaganda), “Pomotsch” (Kostanay).
The following assessment instruments were developed in order to collect information as per the WHO’s methods:13
1) Questionnaires for patients of the AIDS Center; the PLHIV; 2) questionnaires for clients of the HIV prevention program, i.e. PUIDs, SWs, MSM visiting “drop-in centers”, “friendly rooms”; 3) questionnaires for activists, NGOs’ employees; 4) questionnaires for interviewing experts, specialists of the AIDS Centers, NGOs; 5) informed consent forms for those participating in the study.
The following people took part in the study: 141 clients of the HIV/AIDS prevention program, including 12 patients of the AIDS centers (PLHIV); 32 experts, specialists of the AIDS centers, NGOs; two focus groups of clients of the HIV/AIDS prevention program, of 12–13 people each, were among the respondents. In total, 185 people were interviewed.
In our studies we classified the barriers interfering with rapid HIV testing as follows:
- Individual (gender, age, marital status, drug use and other high-risk practices, educational level, salary, self-stigma).
- Social (stigma, discrimination from the public)
- Structural and system-based (laws, restriction on rights for PUIDs, SWs, MSM, violations of the legal framework, health care systems).
When analyzing the results of the sociological studies, we used the following methods and statistical techniques:
- Summary analysis of questionnaires and results from the focus groups:
- statistical processing of questionnaires (coding and analysis of answers). The respondents were asked to define the extent of their consent to some statements. The answers to the questions were selected from a 5-point ordinal scale where 5 – respondents completely agree with this statement, 1 – completely disagree. An average value of points of all the answers as to a certain statement was used as an overall and ranking estimate of the answers. When selecting a characteristic of average level, Mode was calculated;
- Content analysis of interviews and results from the focus group;
Results
Results of the validation study of the rapid tests
The beginning of our studies on the introduction of rapid HIV testing in Kazakhstan was dedicated to the search of reliable rapid tests and identification of their quality parameters. It has been established that the country officially has 10 rapid HIV tests; however, they are used in practice only as preliminary tests and are regularly duplicated by traditional IFA diagnostics. The main results of our validation study of the rapid tests are presented in Table 1.
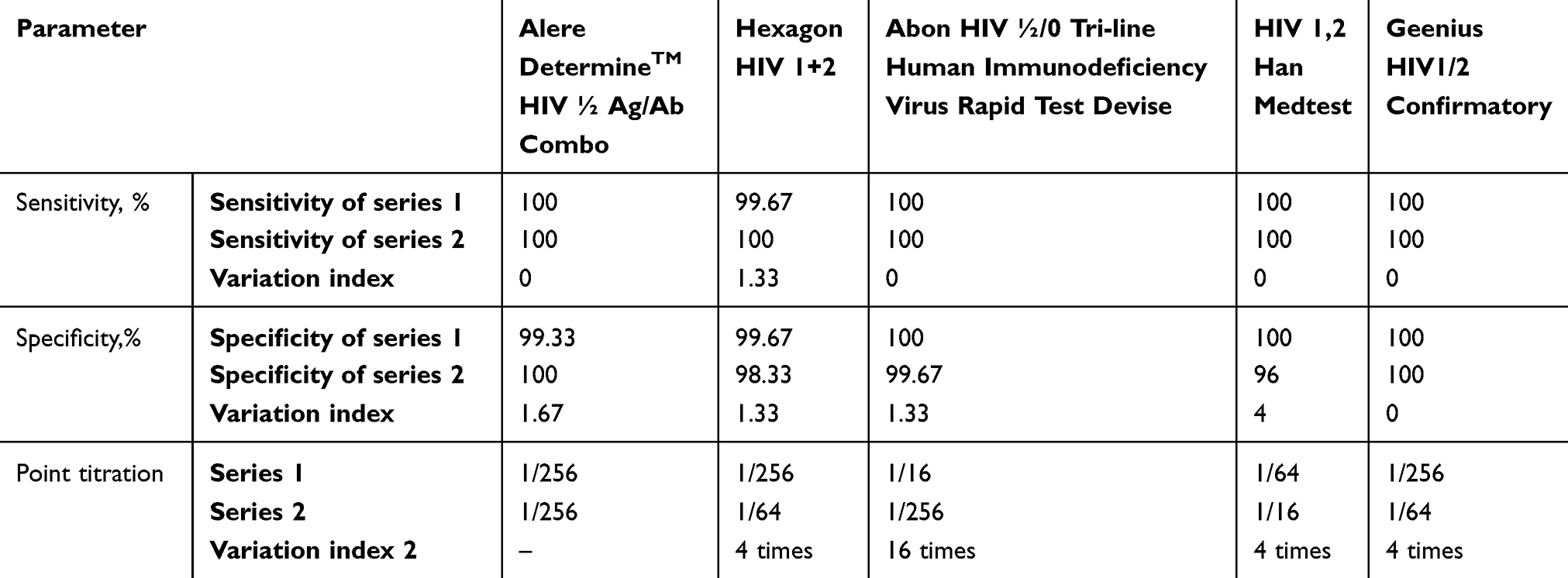 |
Table 1 Main quality parameters of the approved tests and the commercial value of the tests presented in Kazakhstan |
All the rapid tests under study (Alere DetermineTM HIV ½ Ag/Ab Combo; Hexagon HIV 1+2; Abon HIV ½; HIV 1,2 Han Medtest; Geenius HIV1/2 Confirmatory) on the panel of the native blood serum samples correspond to the WHO’s recommendations as to such quality parameters as sensitivity and specificity (sensitivity>99%, specificity>98%). It should be noted that the first series of the 1,2 Han Medtest HIV rapid test made in Kazakhstan show very high sensitivity and specificity values (100% and 100%). However, the second series of the same test was characterized by low specificity (96%), less than permitted by the WHO. However, it is demonstrated that the local manufacturer can create diagnostic test systems of modern level but, at the same time, has to make efforts aimed at standardizing a production process. Therefore, such rapid tests as Alere DetermineTM HIV- ½ Ag/Ab Combo, Hexagon HIV 1+2 и Abon HIV ½ that are used to detect HIV infection can be currently used in Kazakhstan on an equal basis with such traditional HIV diagnosis method as IFA.
Results of the study of the legislative and regulatory acts of the Republic of Kazakhstan
We studied the legal and social problems associated with the forthcoming introduction of Kazakhstan NGO-based rapid HIV testing procedures.
Based on the analytical study of the legislative and regulatory documents of Kazakhstan, orders of the Ministry of Health of the RoK, we established that medical HIV testing conditions in Kazakhstan are governed by authorized state bodies, i.e. the AIDS Center. At the same time, according to Law No. 202-V dated May 16, 2014, of the Republic of Kazakhstan “On Permits and Notices”, private and nonprofit organizations are allowed to carry out HIV testing procedures. According to this Law of the Republic of Kazakhstan, any legal entity or natural person, including NGOs, having a corresponding license is entitled to carry out testing by any methods as this Law stipulates no restrictions on diagnostic methods and materials.
Thus, all rapid tests, both blood and saliva ones, can be used in NGOs’ activities if there are corresponding licenses. In our opinion, a way out of this situation is to obtain licenses for NGO-based rapid HIV testing and related medical activities.
Results of the sociological studies
The main objective of these sociological studies was to identify possible individual, social, and structural barriers interfering with the introduction of NGO-based rapid HIV testing procedures in the country. Within this study, we classified the questioning and interviewing results according to the following two categories: 1) clients of HIV/AIDS prevention programs, patients of AIDS centers (141 respondents); 2) experts, employees of AIDS centers, NGOs (32 respondents).
The summary survey results in case of clients of HIV/AIDS prevention programs – PLHIV (in total, 141 people interviewed) are presented in Tables 2 and 3.
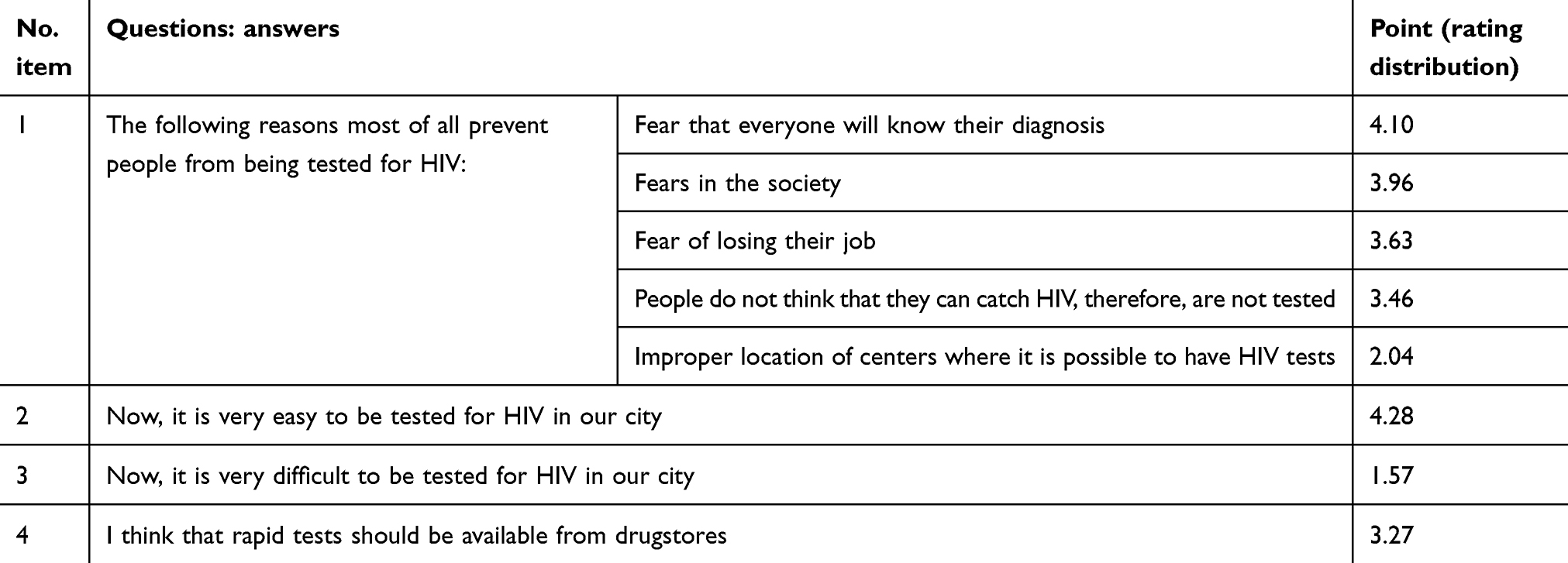 |
Table 2 Summary survey results for clients of HIV/AIDS prevention programs, PLHIV (in total, 141 people interviewed) |
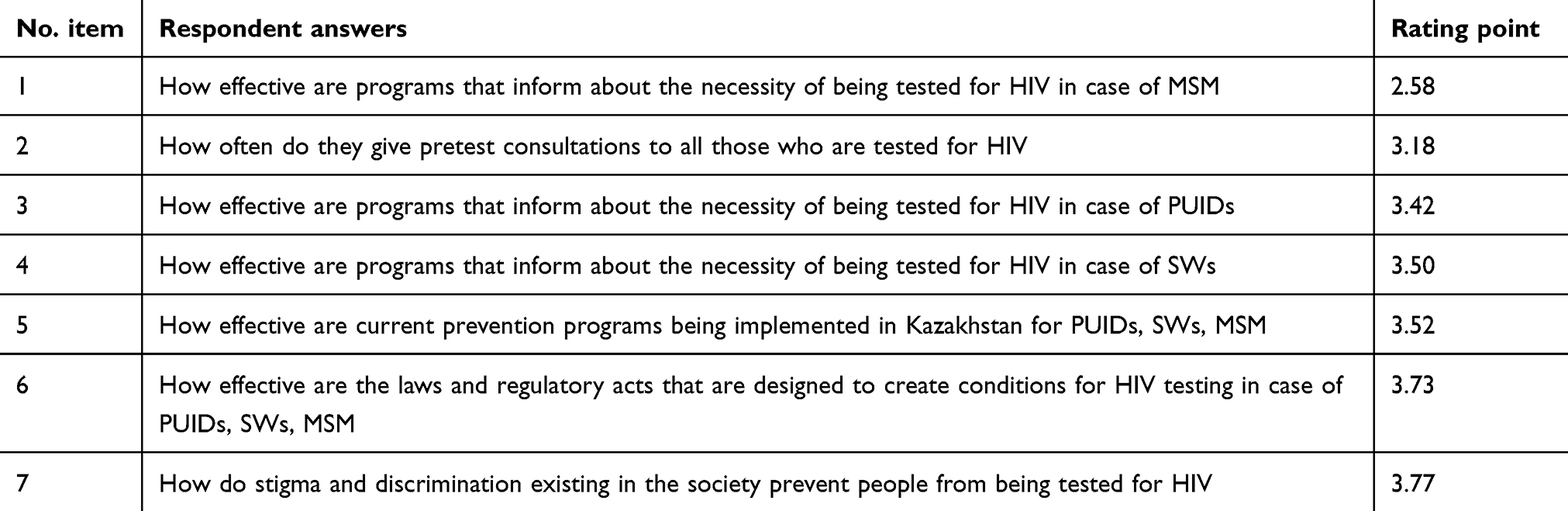 |
Table 3 Rating distribution of the respondents’ answers (from the answers with a low average point to the answers with the highest point) |
Table 2 shows that the main barrier preventing people from being tested for HIV is: “fear that everyone will know their diagnosis”, an average point amounted to 4.10 (mode) as per the 5-point scale. The second place is taken by “fears in the society”, an average point of 3.96 (mode-5). Then, “fear of losing their job”, a point of 3.63 (mode-5). Further, “people do not think that they can catch HIV, therefore, are not tested”, an average point of 3.40 (mode-5). Such statement as “improper location of centers where it is possible to have HIV tests” is not statistically significant, 2.04 (mode-1).
In the course of the assessment of the study results, we studied the following question put forward to the respondents: “how are HIV/AIDS prevention programs implemented in NGOs for “key” population groups (PUIDs, SWs, MSM)?”
Table 3 presents the summary results obtained from questioning experts, employees of NGOs. In total, 32 people were interviewed.
Table 3 shows that an average point of the effectiveness of implementation of prevention programs among “key” population groups (PUIDs, SWs, MSM) amounts to 3.50 (mode-3). The effectiveness of the program that informs about the necessity of having a rapid HIV test for PUIDs, SWs amounts on average to 3.46 (mode-4). According to the respondents, the programs that inform about the necessity of being tested for HIV in case of MSM are the least effective – a point of 2.58 (mode-3). The questionnaire survey shows that stigma and discrimination are serious barriers preventing NGOs from carrying out rapid HIV testing (an average point of 3.77).
As a result of the conducted sociological study, we identified the most significant barriers that interfere with NGO-based rapid HIV testing procedures and are of individual, social, structural, and systematic nature:
- Marital status, drug use and other high-risk practices, educational level, and salary;
- Stigma and discrimination from the public and “self-stigmatization” of PLHIV;
- ”misunderstanding” of one’s own HIV infection;
- Poor communication between health/social workers and patients;
- Shortage of state funds for HIV/AIDS prevention programs;
- Unstable monetary support for NGOs.
For the purpose of introducing Kazakhstan NGO-based rapid HIV testing, we recommend the following:
- NGOs that have financial and technical resources shall obtain licenses for rapid HIV testing and related activities.
- Making amendments to regulatory documents: NGOs’ articles of incorporation – for the purpose of governing organizations’ activities; to Order No. 115 dated February 28, 2013, of the MoH of the RoK. – making amendments to the Regulations on organization of Drop-In Centers’ activities in the context of rapid HIV testing; to the existing orders of the Ministry of Health of the RoK – for the purpose of governing health and sanitary rules and norms related to NGOs’ premises, etc.
- Developing an algorithm of rapid HIV testing for NGOs’ employees.
- Training NGOs’ employees to carry out high-quality rapid HIV testing.
- Training health and social workers in order to carry out high-quality rapid HIV testing and counseling before and after testing.
Discussion
The results of this conducted study supported by the epidemiological data on the HIV infection situation and the analysis of the WHO’s latest program documents confirm the necessity of introducing NGO-based rapid HIV testing in Kazakhstan in order to resolve problems related to the population’s access to services. In our opinion, one of the starting points on which the effectiveness of the country’s HIV epidemic counteraction system depends is to reach the first goal of the UNAIDS strategy “90% of all PLHIV will know their HIV status”. In this regard, the WHO’s 2015 initiative “Test and Treat” (providing antiretroviral therapy to all PLHIV, irrespective of the number of CD4 cells) takes on particular importance. Unfortunately, our country is witnessing serious and critical problems in the field of rendering of HIV care and support services. This is shown by the information from the Republican Center for Prevention and Control of AIDS: 1) about 30% of PLHIV do not know their status; 2) the coverage of “key” population groups by prevention programs remains to be low (for example, only 38.6% of PUIDs were covered by prevention programs in 2015); the coverage of PLHIV by antiretroviral therapy is also low (only 11% of 111,000 PLHIV are involved in treatment).14,15
In recent years, it has been convincingly established that HIV-positive patients receiving antiretroviral therapy become less infectious, the probability of their sexual HIV transmission risk decreases. The modern HIV/AIDS control strategy is also based on the wide use of antiretroviral drugs for medical and preventive purposes: “Prevention Treatment”.16 In the Republic of Kazakhstan, in order to ensure the second component of the UNAIDS 90-90-90 strategy, they revise clinical protocols according to the WHO’s recommendations, increase purchases of antiretroviral drugs by using the state’s and international foundations’ financial resources.
The literature analysis shows that many states currently use in their health care practices low-cost rapid tests that allow medical workers to carry out testing at the level of clinics, communities, and under field conditions. For example, according to J. Wilton (2015), L. Broekaert, and L. Challocombe (2015), rapid testing with the use of blood and gingival tests is the first and most important step in the treatment of HIV-infected patients.17,18 Based on the representative materials of Canada and using the literature review method, the authors presented a wide range of evidence in favor of the advantages of rapid HIV testing. The WHO’s recommendations also indicate the high effectiveness and quality of rapid tests.19 All these things are particularly important for this country in the context of introduction of NGO-based rapid HIV testing.
The results of the conducted validation study show that it is impossible to develop a national algorithm of HIV diagnosis without the study of such important diagnostic characteristics as sensitivity and specificity through the example of Kazakhstan blood serum samples.
Let us note one more important point: when selecting rapid tests, except for the study of documents related to their safety, quality, and effectiveness, made by a manufacturing company, it is necessary to study on the panels of native blood serum samples that include Kazakhstan HIV-positive and negative samples and diagnostic characteristics of this rapid system. It is desirable to carry out this procedure in independent laboratories.
An important moment of the studies was to identify the barriers associated with the forthcoming introduction of NGO-based rapid HIV testing. Here, we consider that the promising ideology of our studies aimed at assessing the barriers interfering with the introduction of NGO-based rapid HIV testing in the country is to create a well-informed and permanent forum in order to inform, hold political debates and reform the legislation for a deeper and better understanding of the HIV epidemic and related matters, with participation of all political trends, including NGOs. In our opinion, a good example for the Republic of Kazakhstan is a report by the Global Commission on HIV and the Law and other documents from international organizations that contain data and analyses of public health care spheres, human rights and laws, and also recommendations to legislators, high-ranking politicians, civil society, partners and representatives of the private sector who take part in the development of HIV/AIDS control measures.20,21
Main restrictions during the conducted study
The study is based on the results of the field studies in seven regional cities of Kazakhstan. With extrapolation for the whole country, it is necessary to consider that the administrative territories of the Republic of Kazakhstan are different in relation to their HIV/AIDS situation and socioeconomic development.
This study was mainly of qualitative nature.
In view of limited resources, this study does not include people who refuse to be tested for HIV. Besides, MSM and SWs were not interviewed consistently.
When developing the idea, program strategy and design of this, work, we were guided by the scientific research methods laid out in Elizabet DePoy and Laura N. Gitlin.22
The statistical analysis of the results of this study was carried out with the use of traditional biostatistics methods and the SPSS program (Statistical Package for Social Science).23
Conclusion
The outcome of the conducted studies is to create a database about the possibility of introduction of NGO-based rapid HIV testing in the Republic of Kazakhstan. We obtained the diagnostic characteristics of the five rapid tests that completely meet the WHO’s requirements and can be used in the conditions of the Republic of Kazakhstan for NGO-based rapid HIV testing procedures. It has been established that the country’s services system associated with rapid HIV testing shall be organized so that those under examination are provided with a reliable and affordable socio-legal protection mechanism. At the same time, it is recommended to develop a national plan aimed at decreasing stigma and discrimination and designed to organize purposeful activities with the population, medical community, and NGOs.
Ethical approval
This study is approved by the Local Ethics Commission of Kazakhstan Medical University “Higher School of Public Health” (Protocol No. IRB-A086 dated September 29, 2017).
Acknowledgments
The authors express gratitude to all people who rendered invaluable assistance in conducting the study and preparing this article: Michael Favorov, Marina Pak (Center for Disease Control and Prevention, USA), Alexander Goliusov, Otilia Skutelnichuk, Alia Bokazhanova (UNAIDS, Kazakhstan), Denis Kamaldinov (an independent consulting group, Russia) as well as NGO activists and employees who took part in the study. An abstract “Social aspects of the rapid HIV testing procedure among nongovernmental organizations in Kazakhstan” was published in “Abstracts” in Journal of Community and Health Education; ISSN: 2161-071, Volume 8 (https://doi.org/10.4172/2161-0711-C4-042; Joint Event on 3rd World Congress on Medical Sociology and Public HealtH & International Conference on Public health and Epidemic diseases).
Disclosure
The authors declare that they have no conflicts of interest regarding this paper.
References
1. Optimizing Investments in Kazakhstan’s HIV Response. Washington DC: The World Bank 1818; 2015:48. Available from: https://elibrary.worldbank.org/doi/abs/10.1596/24965. Accessed August 29, 2019. doi.org/10.1596/24965
2. Strathdee SA, Hallett TB, Bobrova N, et al. HIV and risk environment for injecting drug users: the past, present, and future. Lancet. 2010;376(9737):268–284. Available from: https://www.ncbi.nlm.nih.gov/pubmed/20650523. Accessed August 29, 2019.
3. Strathdee SA, Lozada R, Martinez G, et al. Social and structural factors associated with HIV infection among female sex workers who inject drugs in the Mexico-US border region. PLoS One. 2011;6(4):e19048. pmid:21541349. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5029427/. Accessed August 29, 2019.
4. Krusi A, Wood E, Montaner J, Kerr T. Social and structural determinants of HAART access and adherence among injection drug users. Int J Drug Policy. 2010; 15:4–9. doi:10.1016/j.drugpo.2009.08.003
5. Simmons J, McMahon JM. Barriers to drug treatment for IDU couples: the need for couple-based approaches. J Addict Dis. 2012;31(3):242–257. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4204204/. Accessed August 29, 2019.
6. Walsh N, Maher L. HIV and HCV among people who inject drugs in Central Asia. Drug Alcohol Depend. 2013;132:S37–S40. Available from: https://www.ncbi.nlm.nih.gov/pubmed/23906997. Accessed August 29, 2019.
7. Boltaev A, El-Bassel N, Deryabina A, et al. The scaling up of HIV prevention for people who inject drugs in Central Asia: a review of structural challenges and ways forward. Drug Alcohol Depend. 2013; (in press). Available from:. https://www.ncbi.nlm.nih.gov/pubmed/24103128. Accessed August 29, 2019.
8. El-Bassel N, Gilbert L, Terlikbayeva A, et al. HIV among injection drug users and their intimate partners in Almaty, Kazakhstan. AIDS Behav. 2013. (epub ahead of print). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5859567/. Accessed August 29, 2019.
9. Central Asia PEPFAR Regional Operation Plan (ROP) 2016 Strategy Direction Summary. Washington; 2016: 69. Available from: http://www.pepfar.gov/documents/organization/2376118.pdf. Accessed August 29, 2019
10. Berry M, Wirtz AL, Janayeva A, et al. Risk factors for HIV and unprotected anal intercourse among men who have sex with men (MSM) in Almaty, Kazakhstan. PLoS One. 2012;7:e43071. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0043071. Accessed August 29, 2019.
11. “90-90-90”. Ambitious Treatment Targets: Writing the Final Chapter of the AIDS Epidemic a Discussion Paper. Geneva: Joint United Nations Program on HIV/AIDS; 2014. Available from: http://www.unaids.org/en/resourses/documents/2014/90-90-90.
12. HIV Assays: Operational Characteristics Report 16 Rapid Assays. Geneva: WHO; 2009:45. Available from: https://www.who.int/diagnostics_laboratory/publications/Report16_final.pdf. Accessed August 29, 2019.
13. Baggaley R. Tools for Evaluating HIV Voluntary Counselling and Testing. UNAIDS; 2000:55. Available from: http://www.unaids.org. Accessed August 29, 2019.
14. DePoy E, Gitlin LN. Introduction to Research. Understanding and Applying Multiple Strategies.
15. Abhaya Indrayan “Medical Biostatistics.
16. Yu GL, Elizareva AV, Kaspirova AA. I Drugie, “obzor Ehpidemiologicheskoj Situacii Po VICH-infekcii I Rezul’taty Ehpidemiologicheskogo Nadzora (DEHN) V Respublike Kazahstan Za 2013–2015gg”. Almaty: Izdatelstvo “Respublikanskij centr po profilaktike i bor’be so SPID”; 2016:261.
17. Kasymbekova S. “Antiretrovirusnaya therapia”, Kazahstanskii nauchno-popularny zhurnal o medicine i farmaci, Almaty [Antiretroviral therapy, Kazakhstan science popular journal about medicine and pharmacy, Almaty]. Akademia zdorovya.kz; 2017:41–42. Available from: www.academzdrav.kz. Russian.
18. Guideline on When to Start Antiretroviral Therapy and on Pre-exposure Prophylaxis for HIV. Copenhagen, Denmark: WHO Regional Office for Europe; 2015. Available from: https://www.who.int/hiv/pub/guidelines/earlyrelease-arv/en. Accessed August 29, 2019.
19. Wilton J. The State of HIV Testing in Canada: A Systematic Review, CATIE-Canada’s Source for HIV and Hepatitis C Information. Spring 2015, Available from: https://www.catie.ca/en/pif/spring-2015/state-hiv-testing-canada-systematic-review. Accessed August 29, 2019.
20. Broeckaert L, Challacombe L. Rapid Point-of-Care HIV Testing: A Review of the Evidence; 2015. Available from: http://www.catie.ca/en/pif/spring-2015/rapid-point-care-hiv-testing-review-evidence. Accessed August 29, 2019.
21. WHO “HIV RAPID Diagnostic Tests for Self-testing. 3rd Edition”, HIV-Rapid Diagnostic-tests for self testing-Landscape-Report 3rd-Edition-July-2017.pdf. Available from: http://unitaid.en/assets. Accessed August 29, 2019
22. Global Commission on HIV and the Law - UNDP; July 2012. Available from: https://www.undp.org/content/dam/undp/library/HIV-AIDS/Governance%20of%20HIV%20Responses/Commissions%20report%20final-EN.pdf. Accessed August 29, 2019.
23. Analysis of Legislation. Related to LGBT right and HIV in Eastern Europe and Central Asia, Tallin, Estonia; 2016. http://ecom.ngo/old/LAWS. Accessed August 29, 2019.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.