")
Back to Journals » Clinical Epidemiology » Volume 12
Stroke in Heart Failure
Authors Essa H, Sankaranarayanan R, Lip GYH
Received 4 July 2020
Accepted for publication 15 October 2020
Published 5 November 2020 Volume 2020:12 Pages 1245—1247
DOI https://doi.org/10.2147/CLEP.S270702
Checked for plagiarism Yes
Editor who approved publication: Professor Henrik Sørensen
Hani Essa, 1 Rajiv Sankaranarayanan, 1, 2 Gregory YH Lip 1, 3
1Liverpool Centre for Cardiovascular Science, University of Liverpool, Liverpool Heart & Chest Hospital, Liverpool, UK; 2Liverpool University Hospitals NHS Foundation Trust, Liverpool, UK; 3Aalborg Thrombosis Research Unit, Department of Clinical Medicine, Aalborg University, Aalborg, Denmark
Correspondence: Gregory YH Lip Email [email protected]
Hippocrates, the father of medicine, first recognised stroke 2400 years ago after noting that occlusion of the carotid arteries caused loss of consciousness.1 In the twenty-first century, stroke is ranked as the second leading cause of death with an estimated mortality of around 5.5 million in 2016.2 Additionally, over 50% of stroke survivors suffer chronic disability.3 Heart failure (HF) is a global cause of morbidity and mortality with an estimated 40 million cases in 2015.4 Long-term multi-system complications of HF (Figure 1) and multimorbid disease interactions are of increasing importance and demand a multidisciplinary approach. The prevalence of both stroke and HF is expected to increase due to an ageing population.5,6 It has thus far proven difficult to elucidate the strength of the association between HF and stroke. This is due to the presence of many confounding factors in previous studies including but not limited to small sample sizes, heterogeneous study cohorts, differing definitions of stroke, multiple confounding factors and a short duration of follow up.7–12 The Framingham Study showed that HF was associated with a two to three times higher risk of stroke.13 However, patients with HF also have several co-morbidities which on their own have a propensity to cause ischaemic stroke, such as atrial fibrillation (AF), hypertension, ischaemic heart disease and diabetes.8,14 Lip et al, demonstrated that patients without AF or prior stroke in the study had a hazard ratio of 2.3 (95% Confidence interval (CI) 1.8–3.0) for ischemic stroke in patients with vs without incident heart failure.8 Abdul-Rahim et al reported that a clinical trial population of patients with HF with AF had a higher average annual incidence rate of stroke compared with patients with HF and without AF (1.6% vs 1.2%).15
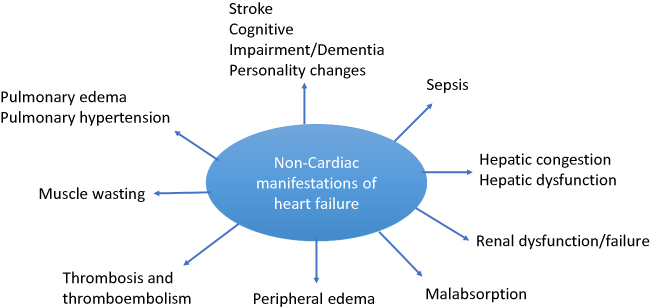 |
Figure 1 Non-cardiac complications of heart failure. |
The presumed aetiology of stroke in HF is likely to be secondary to augmentation of the Virchow’s triad: prothrombotic factors, endothelial injury and left ventricular thrombus formation with subsequent cerebral embolism.16,17 These vascular alterations are observed in both HF with reduced ejection fraction (HFrEF) as well as in HF with preserved ejection fraction (HFpEF). Prognostically, patients who suffer stroke and have HF as an existing comorbidity appear to have much greater rates of mortality. In this case, HF appears to add insult to injury.18,19
There have been several attempts to quantify the risk of stroke in HF with mixed results. A 2015 study looking at the CHA2DS2-VASc scoring system (a validated tool for AF patients) found that whilst the scoring system had a modest predictive accuracy in this cohort, the clinical utility itself was yet unclear.20 More recent data from a 2017 retrospective study has suggested that the CHA2DS2-VASc scoring system has similar validity in both an AF and a non-AF HF cohort of patients.9 The prevention of stroke in this cohort is also unclear, with data from a meta-analysis of 4 randomized control trials with a total of 3681 patients comparing warfarin to aspirin demonstrating no difference in mortality. However, warfarin conferred a lower stroke risk at the cost of a higher bleeding risk.21
In this issue, Tai and colleagues attempt to shed further light on the topic of the long-term risk of stroke and poststroke adverse outcomes in a HF population. There were 2 separate datasets studied:
- Study 1–20,072 adults aged ≥30 years newly diagnosed with HF extracted from the Taiwan national health insurance programme between 2000 and 2005. This group was compared against a cohort of 80,288 non-HF patients matched based on age and sex. Both groups had no history of stroke.
- Study 2–480,604 adults aged ≥30 hospitalized for stroke with and without HF between 2002 and 2009. In this cohort were 30,532 patients with a prior diagnosis of HF.
From their analysis, several important points of discussion emerge in study 1. Firstly, in the HF cohort, stroke risk was significantly higher (hazard ratio (HR) 2.32, 95% CI 2.21–2.43). Secondly, this increased risk of stroke was independent of age and medical background. Thirdly, the association between increased stroke risk was seen throughout the follow-up period when patients who developed stroke in the first 12 months (HR 1.72, 95% CI 1.63–1.81) after the onset of HF were excluded. In study 2, the main finding is that in the HF cohort there was a higher risk of poststroke pneumonia (Odds ratio (OR) 1.31, 95% CI 1.24–1.38), sepsis (OR 1.25, 95% CI 1.17–1.35), intensive care admission (OR 1.47, 95% CI 1.41–1.54), and overall mortality during the hospitalisation (OR 1.44, 95% CI 1.31–1.59).
Tai et al’s study benefits from a large sample size and long duration of follow-up lending credible evidence to two emerging consensuses. Mainly, that HF is a strong risk factor for stroke and that stroke with underlying HF is much worse prognostically. The results reported are consistent with multiple previous studies.7–11 Furthermore, this study demonstrates that stroke risk persists and does not normalise after 6 months, a finding that has previously been shown.8 Several limitations, most of which are acknowledged by the authors, must be considered when interpreting this data. First, this is a retrospective observational study and therefore open to unknown confounding factors which may explain these findings; second, misclassification is common in data that relies on coding for diagnosis; third, the population studied is a mainly homogenous Taiwanese population, therefore these findings may not necessarily be replicated in other ethnicities.
In conclusion, the researchers’ findings highlight the complex nature of the link between HF and stroke and its negative prognostic implications, reflecting earlier study results and solidifying this link. Going forward, important future areas that need to be researched include 1) identification and validation of an appropriate scoring system for stroke risk in HF to highlight low and high-risk patients, and 2) identification of appropriate prophylactic treatment to help reduce the stroke burden in this cohort.
Disclosure
Professor Lip reports consultancy and speaker fees from Bayer, Bayer/Janssen, BMS/Pfizer, Biotronik, Medtronic, Boehringer Ingelheim, Microlife, Roche, and Daiichi-Sankyo outside the submitted work. Dr Sankaranarayanan reports speaker fees from Novartis, Astra Zeneca, Vyfor, BMS/Pfizer and research grants from Biotronik UK, British Heart Foundation outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Engelhardt E. Apoplexy, cerebrovascular disease, and stroke: historical evolution of terms and definitions. Dement Neuropsychol. 2017;11(4):449–453. doi:10.1590/1980-57642016dn11-040016
2. Collaborators GN. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2019;18(5):459–480.
3. Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367(9524):1747–1757. doi:10.1016/S0140-6736(06)68770-9
4. Collaborators GDaIIaP. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602.
5. Heidenreich PA, Albert NM, Allen LA, et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6(3):606–619. doi:10.1161/HHF.0b013e318291329a
6. Ovbiagele B, Goldstein LB, Higashida RT, et al. Forecasting the future of stroke in the United States: a policy statement from the American Heart Association and American Stroke Association. Stroke. 2013;44(8):2361–2375. doi:10.1161/STR.0b013e31829734f2
7. Witt BJ, Brown RD, Jacobsen SJ, et al. Ischemic stroke after heart failure: a community-based study. Am Heart J. 2006;152(1):102–109. doi:10.1016/j.ahj.2005.10.018
8. Lip GY, Rasmussen LH, Skjøth F, Overvad K, Larsen TB. Stroke and mortality in patients with incident heart failure: the Diet, Cancer and Health (DCH) cohort study. BMJ Open. 2012;2(4):4. doi:10.1136/bmjopen-2012-000975
9. Kang SH, Kim J, Park JJ, et al. Risk of stroke in congestive heart failure with and without atrial fibrillation. Int J Cardiol. 2017;248:182–187. doi:10.1016/j.ijcard.2017.07.056
10. Hays AG, Sacco RL, Rundek T, et al. Left ventricular systolic dysfunction and the risk of ischemic stroke in a multiethnic population. Stroke. 2006;37(7):1715–1719. doi:10.1161/01.STR.0000227121.34717.40
11. Berger JS, Peterson E, LalibertÉ F, et al. Risk of ischemic stroke in patients newly diagnosed with heart failure: focus on patients without atrial fibrillation. J Card Fail. 2019;25(6):436–447. doi:10.1016/j.cardfail.2018.03.012
12. Agarwal M, Apostolakis S, Lane DA, Lip GY. The impact of heart failure and left ventricular dysfunction in predicting stroke, thromboembolism, and mortality in atrial fibrillation patients: a systematic review. Clin Ther. 2014;36(9):1135–1144. doi:10.1016/j.clinthera.2014.07.015
13. Kannel WB, Wolf PA, Verter J. Manifestations of coronary disease predisposing to stroke. The Framingham study. JAMA. 1983;250(21):2942–2946. doi:10.1001/jama.1983.03340210040022
14. Alberts VP, Bos MJ, Koudstaal P, et al. Heart failure and the risk of stroke: the Rotterdam Study. Eur J Epidemiol. 2010;25(11):807–812. doi:10.1007/s10654-010-9520-y
15. Abdul-Rahim AH, Perez AC, Fulton RL, et al. Risk of stroke in chronic heart failure patients without atrial fibrillation: analysis of the Controlled Rosuvastatin in Multinational trial heart failure (CORONA) and the Gruppo Italiano per lo Studio della Sopravvivenza nell’Insufficienza Cardiaca-Heart Failure (GISSI-HF) trials. Circulation. 2015;131(17):1486–1494.
16. Lip GY, Gibbs CR. Does heart failure confer a hypercoagulable state? Virchow’s triad revisited. J Am Coll Cardiol. 1999;33(5):1424–1426.
17. Kalaria VG, Passannante MR, Shah T, Modi K, Weisse AB. Effect of mitral regurgitation on left ventricular thrombus formation in dilated cardiomyopathy. Am Heart J. 1998;135(2):215–220. doi:10.1016/S0002-8703(98)70084-5
18. Appelros P, Nydevik I, Viitanen M. Poor outcome after first-ever stroke: predictors for death, dependency, and recurrent stroke within the first year. Stroke. 2003;34(1):122–126. doi:10.1161/01.STR.0000047852.05842.3C
19. Divani AA, Vazquez G, Asadollahi M, Qureshi AI, Pullicino P. Nationwide frequency and association of heart failure on stroke outcomes in the United States. J Card Fail. 2009;15(1):11–16. doi:10.1016/j.cardfail.2008.09.001
20. Melgaard L, Gorst-Rasmussen A, Lane DA, Rasmussen LH, Larsen TB, Lip GY. Assessment of the CHA2DS2-VASc score in predicting ischemic stroke, thromboembolism, and death in patients with heart failure with and without atrial fibrillation. JAMA. 2015;314(10):1030–1038. doi:10.1001/jama.2015.10725
21. Kumar G, Goyal MK. Warfarin versus aspirin for prevention of stroke in heart failure: a meta-analysis of randomized controlled clinical trials. J Stroke Cerebrovasc Dis. 2013;22(8):1279–1287. doi:10.1016/j.jstrokecerebrovasdis.2012.09.015
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.