")
Back to Journals » OncoTargets and Therapy » Volume 12
Stomatitis And Everolimus: A Review Of Current Literature On 8,201 Patients
Authors Arena C , Troiano G , Zhurakivska K , Nocini R , Lo Muzio L
Received 30 November 2018
Accepted for publication 23 January 2019
Published 14 November 2019 Volume 2019:12 Pages 9669—9683
DOI https://doi.org/10.2147/OTT.S195121
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Claudia Arena,1 Giuseppe Troiano,1 Khrystyna Zhurakivska,1 Riccardo Nocini,2 Lorenzo Lo Muzio1,3
1Department of Clinical and Experimental Medicine, University of Foggia, Foggia, Italy; 2Section of Otolaryngology, Department of Surgical Sciences, Dentistry, Gynecology, and Pediatrics, University of Verona, Verona, Italy; 3C.I.N.B.O. (Consorzio Interuniversitario Nazionale per la Bio-Oncologia), Chieti, Italy
Correspondence: Lorenzo Lo Muzio
Clinica Odontoiatrica, Università degli Studi di Foggia, 50 Via Rovelli, Foggia 71122, Italy
Tel +39 0881 588 090
Fax +39 0881 588081
Email [email protected]
Background: Oral toxicities, such as mucositis and stomatitis, are some of the most significant and unavoidable side effects associated with anticancer therapies. In past decades, research has focused on newer targeted agents with the aim of decreasing the rates of side effects on healthy cells. Unfortunately, even targeted anticancer therapies show significant rates of toxicity on healthy tissue. mTOR inhibitors display some adverse events, such as hyperglycemia, hyperlipidemia, hypophosphatemia, hematologic toxicities, and mucocutaneous eruption, but the most important are still stomatitis and skin rash, which are often dose-limiting side effects.
Aim: This review was performed to answer the question “What is the incidence of stomatitis in patients treated with everolimus?"
Methods: We conducted a systematic search on the PubMed and Medline online databases using a combination of MESH terms and free text: “everolimus” (MESH) AND “side effects” OR “toxicities” OR “adverse events”. Only studies fulfilling the following inclusion criteria were considered eligible for inclusion in this study: performed on human subjects, reporting on the use of everolimus (even if in combination with other drugs or ionizing radiation), written in the English language, and reporting the incidence of side effects.
Results: The analysis of literature revealed that the overall incidence of stomatitis after treatment with everolimus was 42.6% (3,493) and that of stomatitis grade G1/2 84.02% (2,935), while G3/4 was 15.97% (558).
Conclusion: Results of the analysis showed that the incidence of stomatitis of grade 1 or 2 is higher than grade 3 or 4. However, it must be taken into account that it is not possible to say if side effects are entirely due to everolimus therapy or combinations with other drugs.
Keywords: stomatitis, everolimus, mucositis, targeted therapy, oral medicine, oral pathology
Introduction
Conventional anticancer therapy does not distinguish between normal and cancer cells. The damage inflicted on normal tissue have thus hampered this therapy.1 The introduction of targeted-therapy molecules targeting specific enzymes, growth-factor receptors, and signal transducers has lowered the incidence of side effects,2 significantly influencing patient quality of life and survival rates.2mTOR is a therapeutic target for both solid and hematologic malignancies. It is part of a pathway that regulates protein biosynthesis, cell growth, and cell-cycle progression. Moreover, mTOR is the downstream effector of the PI3K–Akt–mTOR pathway, which regulates cell growth and metabolism and is involved in multiple processes.1,3–5
Rapamycin and its analogues form the first generation of mTOR inhibitors. The action of these molecules is targeting a 289 kDa serine/threonine-protein kinase that is a component of the big family of PI3Ks. Rapamycin and its analogues work by inhibiting the activity of mTORC1 through binding to FKBP12 and the establishment of a ternary complex with mTOR.6Actually, there are three available mTOR inhibitors: everolimus, temsirolimus, and ridaforolimus. Everolimus is currently used for the treatment of advanced hormone receptor–positive HER2-negative breast cancer together with exemestane, renal-cell carcinoma after failure of therapies based on sunitinib or sorafenib, progressive neuroendocrine tumors of pancreatic origin, in combination with exemestane, and subependymal giant-cell astrocytoma.
These drugs have a different spectrum of side effects compared to conventional chemotherapy. Common side effects are anemia, fatigue, hyperglycemia, hyperlipidemia, stomatitis, rash, and thrombocytopenia.5,7 The terms “oral mucositis” and “stomatitis” are both used to describe inflammation and ulceration of the oral mucosal lining due to chemotherapy or ionizing radiation. However, stomatitis associated with mTOR inhibitors should be considered a separate entity this often being designated as mTOR inhibitor–associated stomatitis (mIAS).8,9 Mouth lesions present as superficial, ovoid, well-demarcated singular or multiple ulcers with a grayish white pseudomembrane. Their size often does not exceed 0.5 cm in diameter. Lesions typically involve the nonkeratinized mucosa, like the inner aspect of the lips, the ventral and lateral surfaces of the tongue, and the soft palate. Ulcers generally develop in 5 days and usually heal spontaneously in 1 week, most frequently in the first cycle of mTOR-inhibitor therapy.10
Methods
This review was performed to answer to the question “Which is the rate of incidence of stomatitis in patients treated with everolimus?” A systematic search on the online databases PubMed and Medline was conducted using a combination of MESH terms and free-text words: “everolimus” (MESH) AND “side effects” OR “toxicities” OR “adverse events”. The authors included in this study only reports that fulfilled certain criteria: performed on human subjects, everolimus alone or in combination with other drugs/ionizing radiation, written in the English language, and providing incidence of side effects. No restrictions were applied on year of publication. Reviews, case reports, and studies in vitro or performed on animal models were excluded. Information collected comprised name of first author, year, title, number of patients enrolled, and number and grade of events recorded. In addition, data were independently extracted by two authors (CA and LLM) and checked in a joint session.
Results
Our literature search yielded 1,019 potentially relevant studies. After elimination of duplicates, titles and abstracts of 912 potentially relevant studies were screened. Of these, 731 were not considered because they did not meet the inclusion criteria. A total of 181 studies were read in full text. Of these, only 100 reported on stomatitis or oral mucositis, and 30 were excluded due to lack of data (Figure 1). Results howed that the overall incidence of stomatitis after treatment with everolimus was 42.6% (3,493), stomatitis grade G12 84.02% (2,935), and G34 15.97% (558, Table 1).
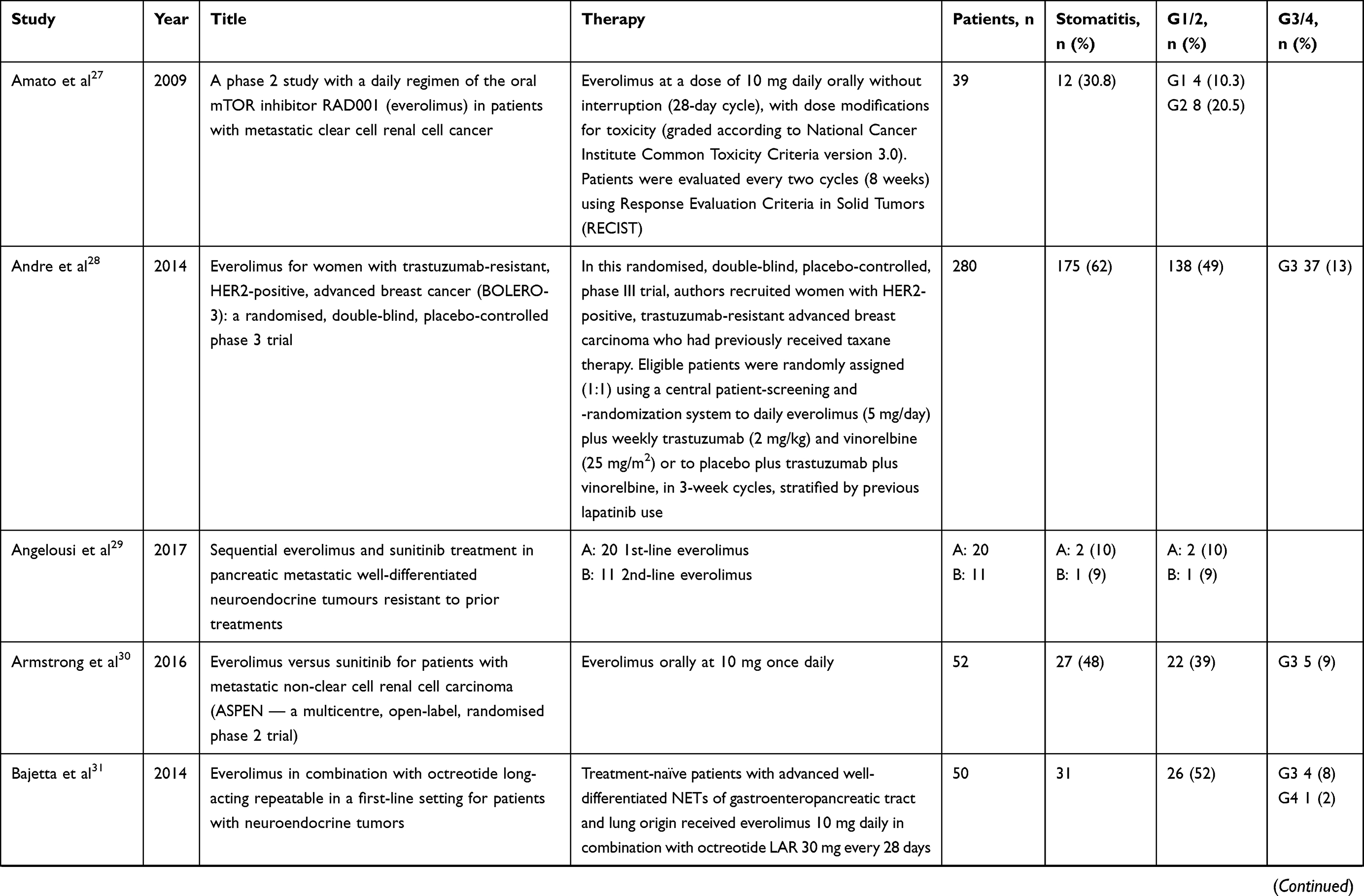 | 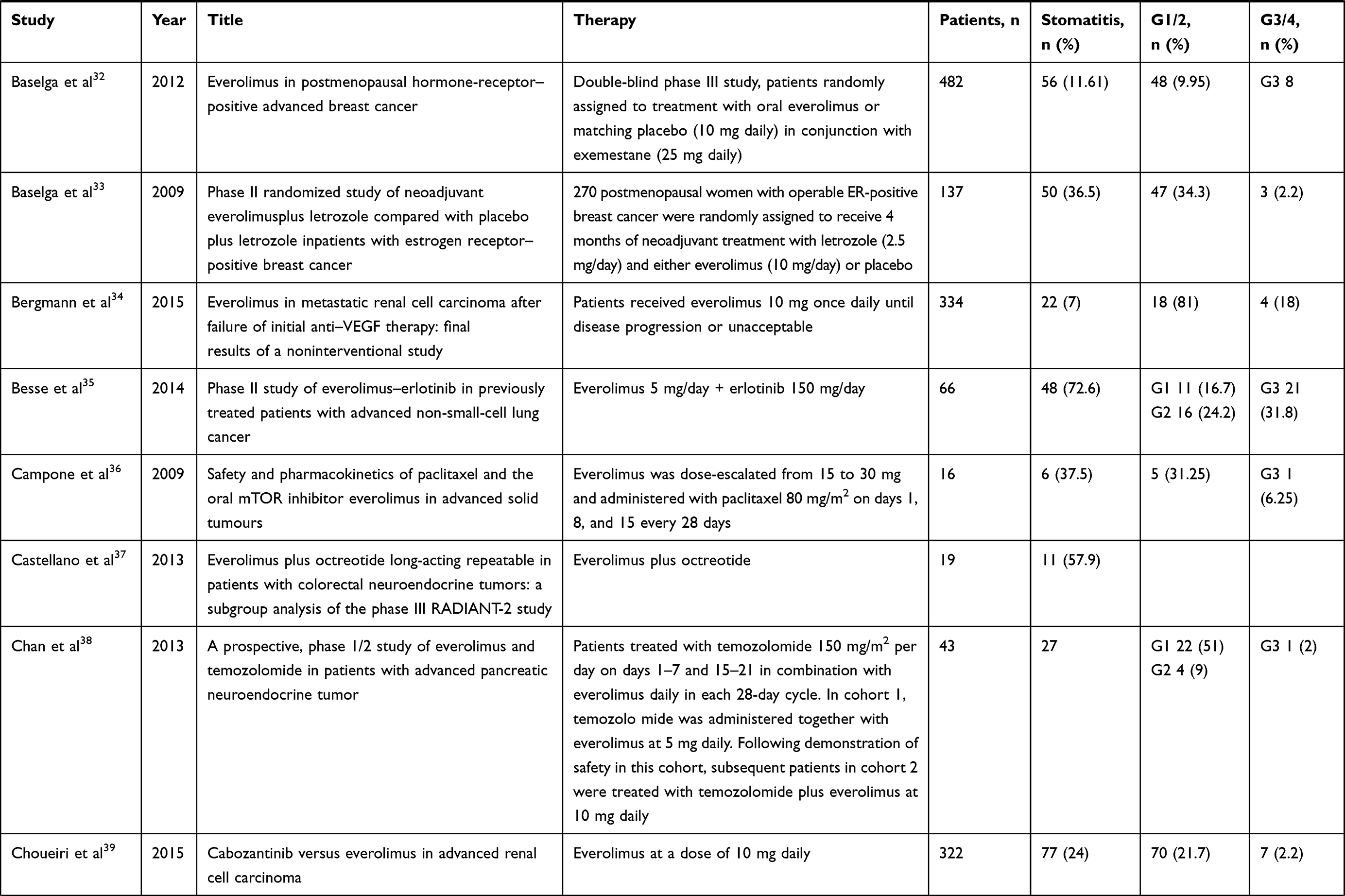 | 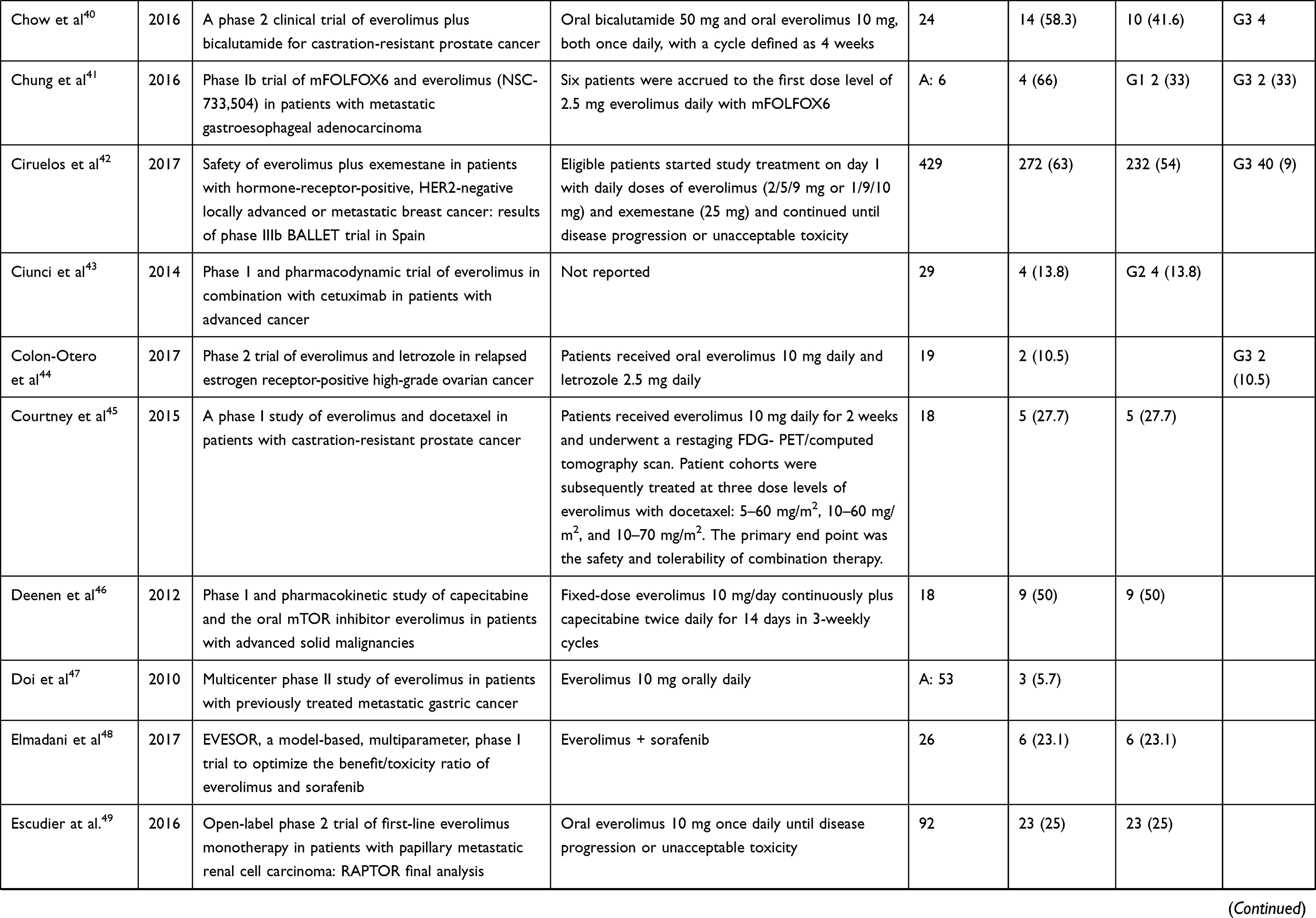 | 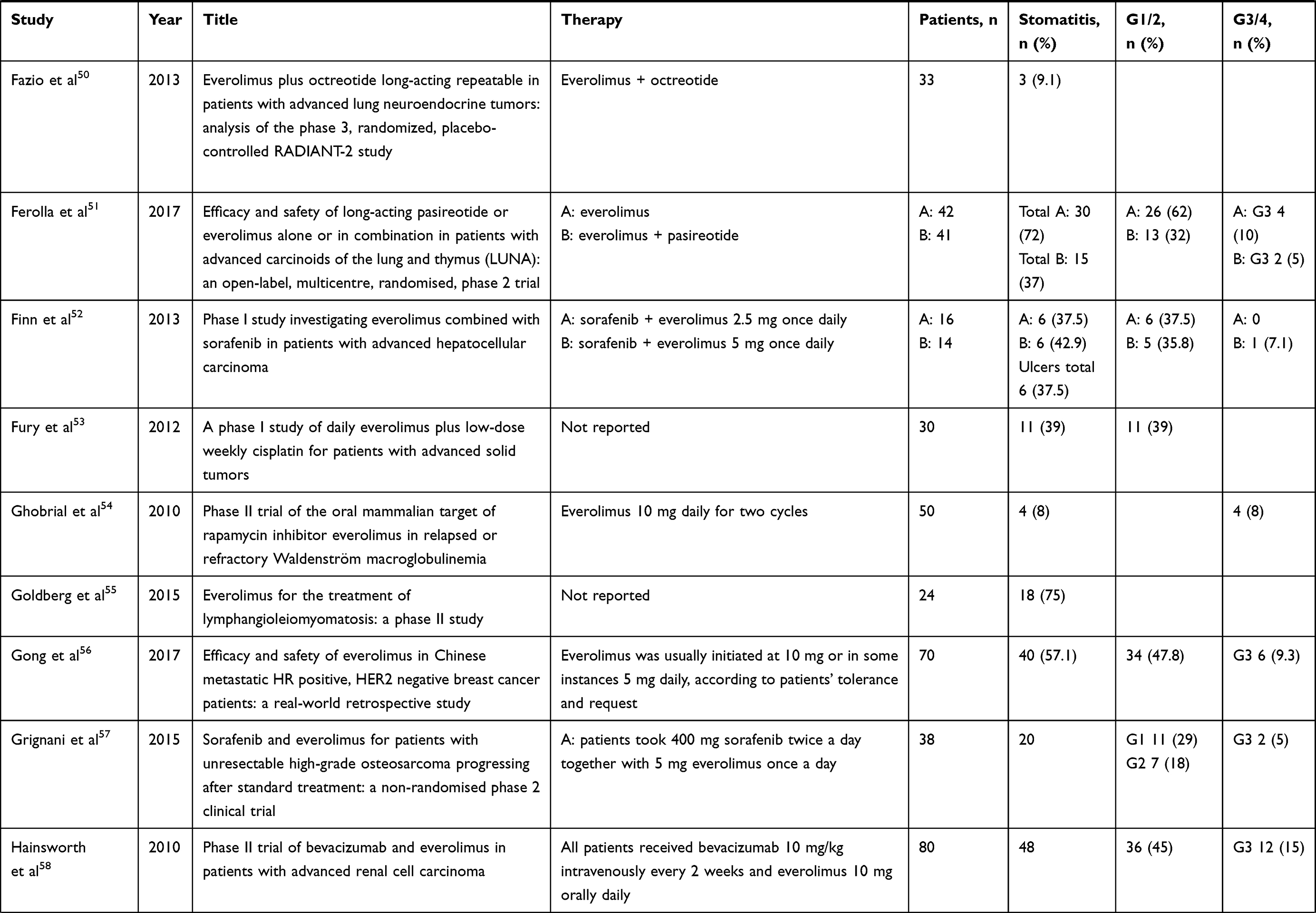 |  | 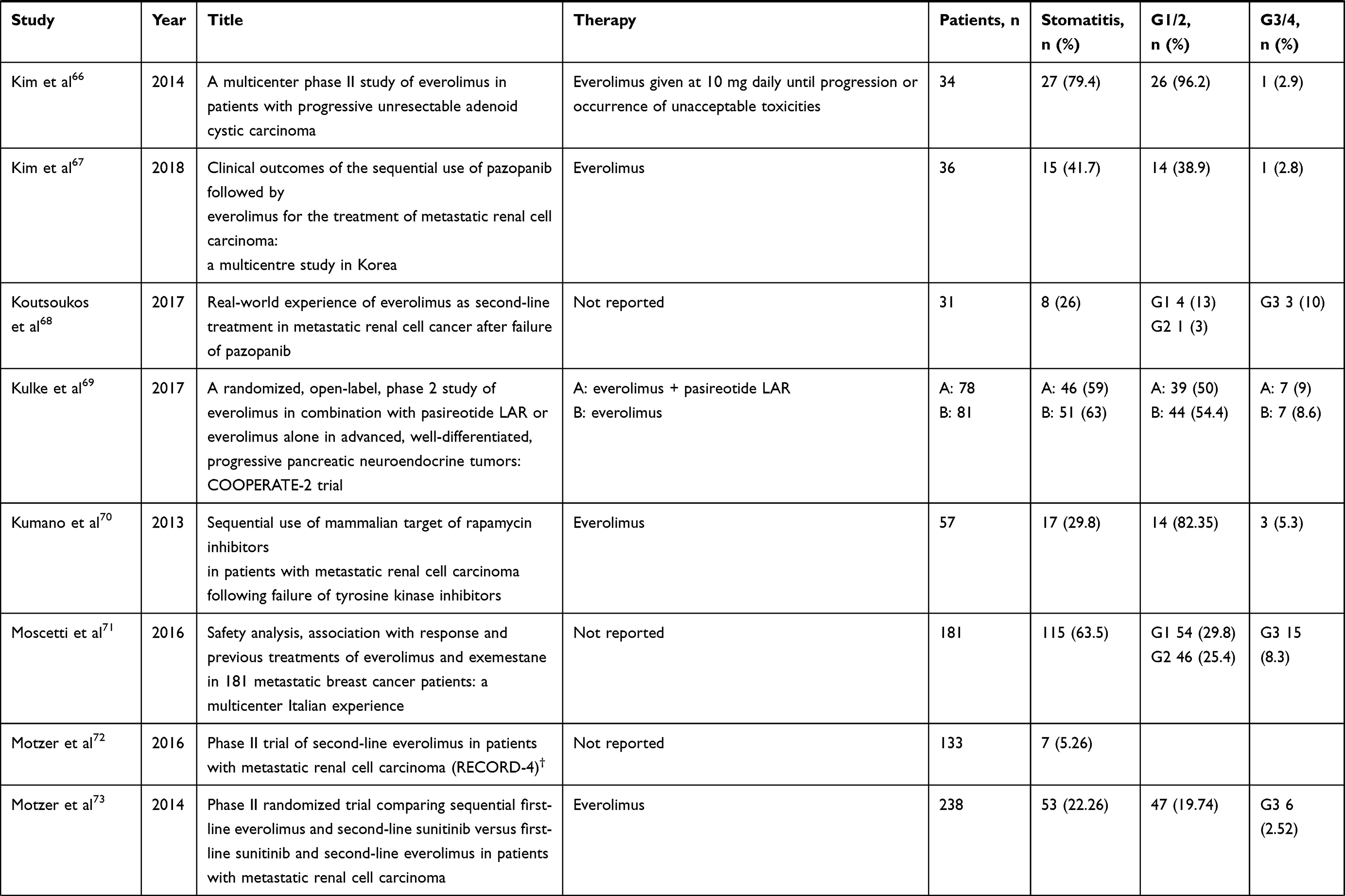 | 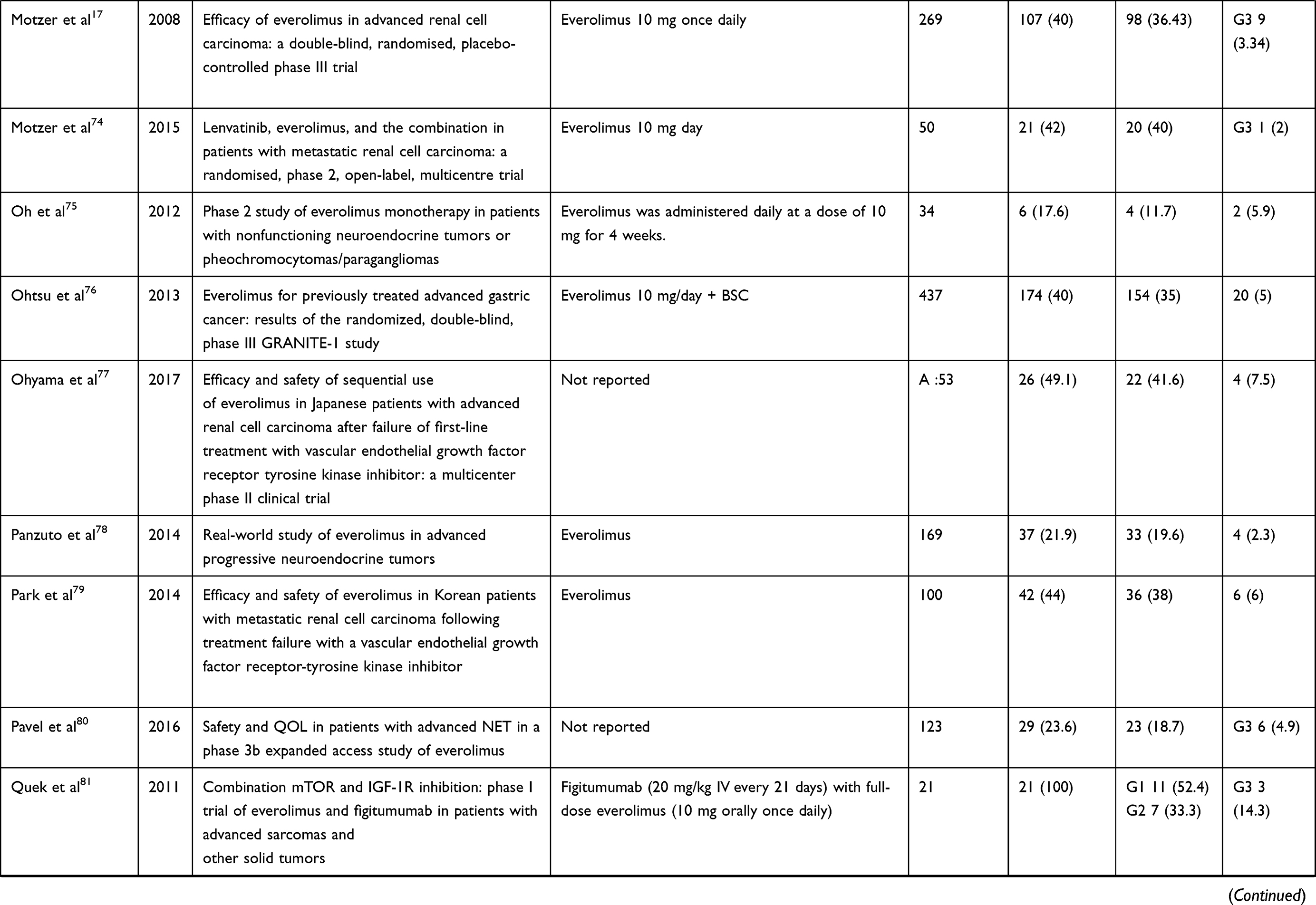 | 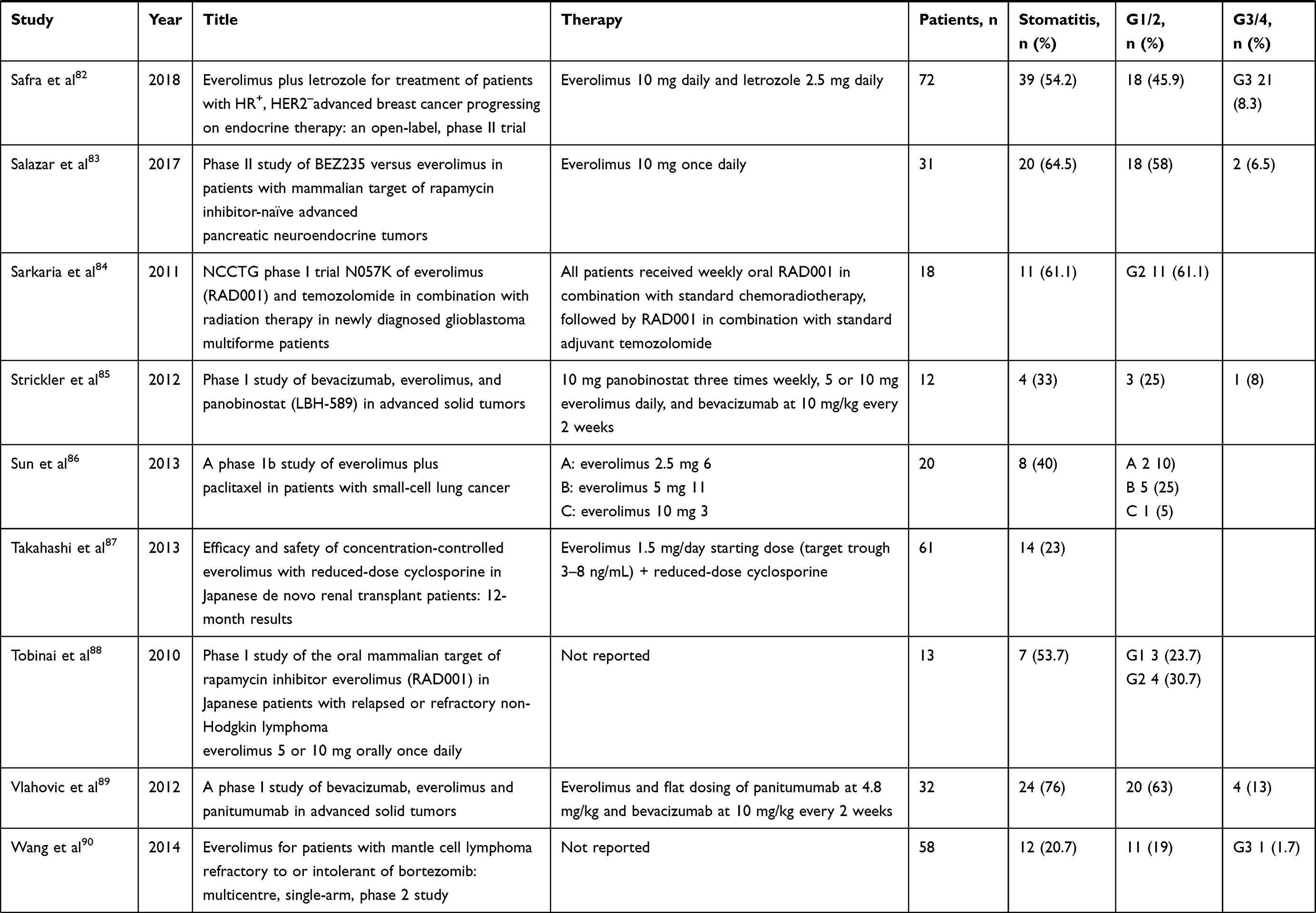 | 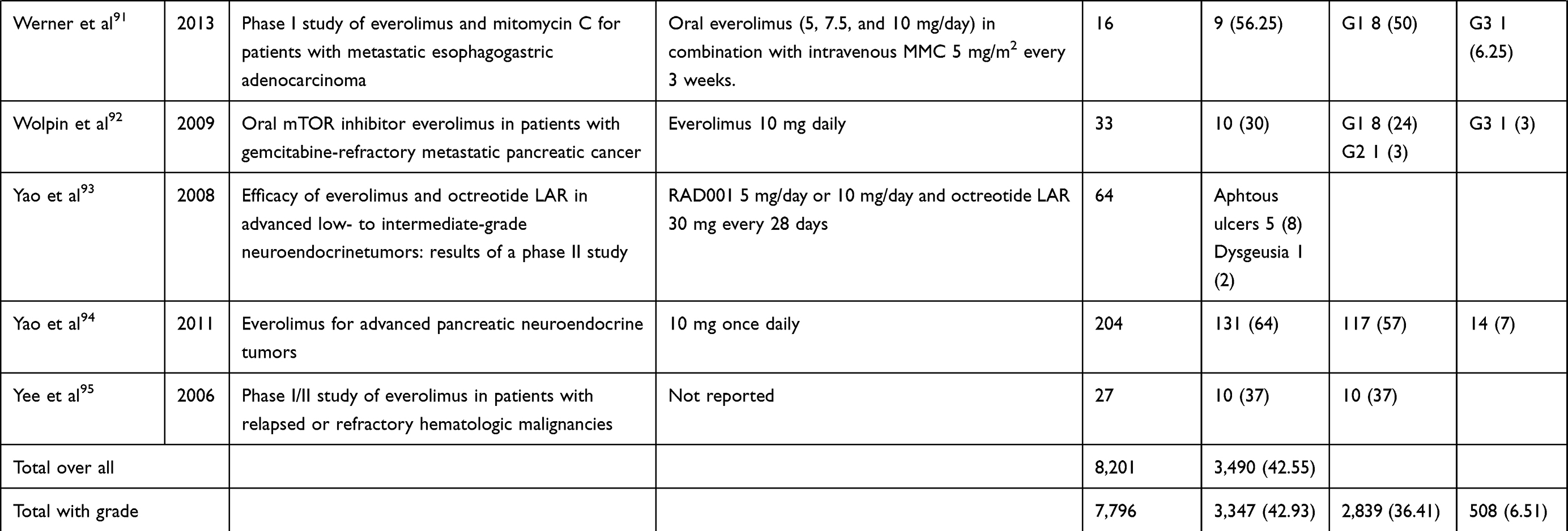 |
Table 1 Papers About Everolimus And Stomatitis |
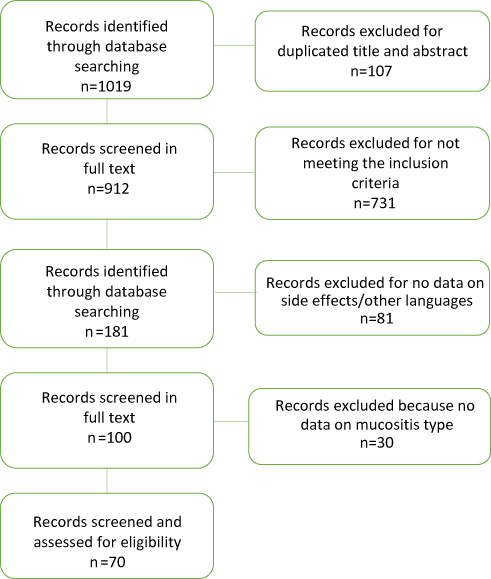 |
Figure 1 Flowchart showing the process of paper selection used in this review. |
Discussion
Targeted therapy includes those drugs that selectively inhibit a target that is mutated in malignant tissue, aiming to achieve preferential localization in the region of disease and thus an increase in local concentration. In particular, mTOR inhibitors work as signal-transduction inhibitors. Rapamycin, also named sirolimus, was the first mTOR inhibitor approved. It is an antiungal agent produced by Streptomyces hygroscopicus with immunosuppressive properties.11 However, sirolimus has been show to have poor pharmacokinetic characteristics, and research has focused on the synthesis of analogues of rapamycin more suitable to therapy, such as everolimus, temsirolimus, and ridaforolimus. These molecules differ from sirolimus in their C-40-O positions, resulting in disparate pharmacokinetic and pharmacodynamic profiles.12 This class of drugs is typically used for the treatment of solid tumors, such as renal-cell carcinoma, breast cancer, pancreatic neuroendocrine tumors, and tuberous sclerosis complex.13–17
Unlike results obtained from reviews about mucositis caused by conventional chemotherapy, in which mucositis is often severe and the most debilitating effect for patients,18 our analysis showed that the incidence of stomatitis of grade 1 or 2 is higher than that of grade 3 or 4. These results are consistent with our previous work.19 However, it must be taken into account that it is not possible to say if side effects are entirely due to everolimus therapy or combination with other drugs. Moreover, not all the papers included in this review specified the exact therapeutic regimen. mIAS generally sets in within a few weeks of initiating everolimus therapy. Grade 3 or 4 lesions may lead to dose interruption or reduction. Interfering with patientfood intake and diminishing quality of life, this kind of toxicity may cause treatment discontinuation or interruption.20
mIAS is often evaluated using common scales employed in the evaluation of conventional oral mucositis (OMAS, 1999; NCI-CTCAE 2006, 2010). However, its clinical appearance tends to differ from conventional mucositis. A more specific mIAS scale was set by Boers-Doets and Lalla. According to this scale, lesions are evaluated depending on their duration, eg, a grade 3 lesion is an ulceration lasting >7 days.21 Management of mIAS is still widely based on education of patients on oral hygiene measures, diet modifications, and pain management.9,22 Treatments used are often based on “magic” mouthwash, composed of lidocaine gel 2% × 30 g, doxycycline suspension 50 mg/5mL × 60 mL, and sucralfate oral suspension 1,000 mg/5 mL dissolved in sodium chloride 0.9% × 2,000 mL used for 3–15 days,23 a sodium bicarbonate–based mouthwash combined with oral fluconazole,24 or a combination of dexamethasone solution 0.5 mg/mL and miconazole 2% gel.25 Another treatment is based on a combination of topical anesthetics, a magic mouthwash (composed of lidocaine, aluminum hydroxide, magnesium hydroxide, dimethicone suspension, diphenhydramine, equal parts) clobetasol gel 0.05%, dexamethasone 0.1 mg/mL, triamcinolone paste, intralesional triamcinolone, and systemic prednisone (1 mg/kg for 7 days). Management of mIAS nowadays is based on education of patients on oral hygiene measures, diet modifications, and pain management.9 Rugo et al showed evidence of the efficacy of a prophylactic use of dexamethasone mouthwash in patients treated with everolimus plus exemestane for advanced or metastatic breast cancer.26 The mouthwash was administered in combination with a prophylactic topical antifungal agent to prevent potential fungal infection.26 It still cannot be determined which lesions will self-limit and which will reduce quality of life, leading to malnutrition and dose reduction in medically necessary treatment.
Disclosure
The authors report no conflicts of interest in this work
References
1. Gomez-Pinillos A, Ferrari AC. mTOR signaling pathway and mTOR inhibitors in cancer therapy. Hematol Oncol Clin North Am. 2012;26(3):483–505, vii. doi:10.1016/j.hoc.2012.02.014
2. Keefe DM, Bateman EH. Tumor control versus adverse events with targeted anticancer therapies. Nat Rev Clin Oncol. 2011;9(2):98–109. doi:10.1038/nrclinonc.2011.192
3. Khokhar NZ, Altman JK, Platanias LC. Emerging roles for mammalian target of rapamycin inhibitors in the treatment of solid tumors and hematological malignancies. Curr Opin Oncol. 2011;23(6):578–586. doi:10.1097/CCO.0b013e32834b892d
4. Dabney R, Devine R, Sein N, George B. New agents in renal cell carcinoma. Target Oncol. 2014;9(3):183–193. doi:10.1007/s11523-013-0303-8
5. Yuan R, Kay A, Berg WJ, Lebwohl D. Targeting tumorigenesis: development and use of mTOR inhibitors in cancer therapy. J Hematol Oncol. 2009;2:45. doi:10.1186/1756-8722-2-45
6. Meng LH, Zheng XF. Toward rapamycin analog (rapalog)-based precision cancer therapy. Acta Pharmacol Sin. 2015;36(10):1163–1169. doi:10.1038/aps.2015.68
7. Martins F, de Oliveira MA, Wang Q, et al. A review of oral toxicity associated with mTOR inhibitor therapy in cancer patients. Oral Oncol. 2013;49(4):293–298. doi:10.1016/j.oraloncology.2012.11.008
8. Sonis S, Treister N, Chawla S, Demetri G, Haluska F. Preliminary characterization of oral lesions associated with inhibitors of mammalian target of rapamycin in cancer patients. Cancer. 2010;116(1):210–215. doi:10.1002/cncr.24696
9. Boers-Doets CB, Raber-Durlacher JE, Treister NS, et al. Mammalian target of rapamycin inhibitor-associated stomatitis. Future Oncol. 2013;9(12):1883–1892. doi:10.2217/fon.13.141
10. Peterson DE, O’Shaughnessy JA, Rugo HS, et al. Oral mucosal injury caused by mammalian target of rapamycin inhibitors: emerging perspectives on pathobiology and impact on clinical practice. Cancer Med. 2016;5(8):1897–1907. doi:10.1002/cam4.2016.5.issue-8
11. Sehgal SN, Baker H, Rapamycin VC. (AY-22,989), a new antifungal antibiotic. II. Fermentation, isolation and characterization. J Antibiot (Tokyo). 1975;28(10):727–732. doi:10.7164/antibiotics.28.727
12. Liu Q, Thoreen C, Wang J, Sabatini D, Gray NS. mTOR mediated anti-cancer drug discovery. Drug Discov Today Ther Strateg. 2009;6(2):47–55. doi:10.1016/j.ddstr.2009.12.001
13. Awada A, Cardoso F, Fontaine C, et al. The oral mTOR inhibitor RAD001 (everolimus) in combination with letrozole in patients with advanced breast cancer: results of a phase I study with pharmacokinetics. Eur J Cancer. 2008;44(1):84–91. doi:10.1016/j.ejca.2007.10.003
14. Boers-Sonderen MJ, de Geus-Oei LF, Desar IM, et al. Temsirolimus and pegylated liposomal doxorubicin (PLD) combination therapy in breast, endometrial, and ovarian cancer: phase Ib results and prediction of clinical outcome with FDG-PET/CT. Target Oncol. 2014;9(4):339–347. doi:10.1007/s11523-014-0309-x
15. Hudes GR, Berkenblit A, Feingold J, Atkins MB, Rini BI, Dutcher J. Clinical trial experience with temsirolimus in patients with advanced renal cell carcinoma. Semin Oncol. 2009;36(Suppl 3):S26–S36. doi:10.1053/j.seminoncol.2009.10.013
16. Krueger DA, Care MM, Holland K, et al. Everolimus for subependymal giant-cell astrocytomas in tuberous sclerosis. N Engl J Med. 2010;363(19):1801–1811. doi:10.1056/NEJMoa1001671
17. Motzer RJ, Escudier B, Oudard S, et al. Efficacy of everolimus in advanced renal cell carcinoma: a double-blind, randomised, placebo-controlled phase III trial. Lancet. 2008;372(9637):449–456. doi:10.1016/S0140-6736(08)61039-9
18. Borbasi S, Cameron K, Quested B, Olver I, To B, Evans D. More than a sore mouth: patients’ experience of oral mucositis. Oncol Nurs Forum. 2002;29(7):1051–1057. doi:10.1188/02.ONF.1051-1057
19. Lo Muzio L, Arena C, Troiano G, Villa A. Oral stomatitis and mTOR inhibitors: a review of current evidence in 20,915 patients. Oral Dis. 2018;24(1–2):144–171. doi:10.1111/odi.12795
20. Rugo HS, Pritchard KI, Gnant M, et al. Incidence and time course of everolimus-related adverse events in postmenopausal women with hormone receptor-positive advanced breast cancer: insights from BOLERO-2. Ann Oncol. 2014;25(4):808–815. doi:10.1093/annonc/mdu009
21. Boers-Doets C, Lalla RV. The mIAS scale: a scale to measure mTOR inhibitor-associated stomatitis. Supp Care Cancer. 2013;21(Suppl):1.
22. Ji YD, Aboalela A, Villa A. Everolimus-associated stomatitis in a patient who had renal transplant. BMJ Case Rep. 2016;2016.
23. Kalogirou EM, Tosios KI, Piperi EP, Sklavounou A. mTOR inhibitor-associated stomatitis (mIAS) in three patients with cancer treated with everolimus. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;119(1):e13–e19. doi:10.1016/j.oooo.2014.08.023
24. Ferte C, Soria JC, Penel N. Dose-levels and first signs of efficacy in contemporary oncology phase 1 clinical trials. PLoS One. 2011;6(3):e16633. doi:10.1371/journal.pone.0016633
25. Nicolatou-Galitis O, Nikolaidi A, Athanassiadis I, Papadopoulou E, Sonis S. Oral ulcers in patients with advanced breast cancer receiving everolimus: a case series report on clinical presentation and management. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;116(2):e110–e116. doi:10.1016/j.oooo.2013.02.022
26. Rugo HS, Seneviratne L, Beck JT, et al.Prevention of everolimus-related stomatitis in women with hormone receptor-positive, HER2-negative metastatic breast cancer using dexamethasone mouthwash (SWISH): a single-arm, phase 2 trial. Lancet Oncol. 2017;(18):654–662. doi:10.1016/S1470-2045(17)30109-2
27. Amato RJ, Jac J, Giessinger S, Saxena S, Willis JP. A phase 2 study with a daily regimen of the oral mTOR inhibitor RAD001 (everolimus) in patients with metastatic clear cell renal cell cancer. Cancer. 2009;115(11):2438–2446. doi:10.1002/cncr.v115:11
28. Andre F, O’Regan R, Ozguroglu M, et al. Everolimus for women with trastuzumab-resistant, HER2-positive, advanced breast cancer (BOLERO-3): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet Oncol. 2014;15(6):580–591. doi:10.1016/S1470-2045(14)70138-X
29. Angelousi A, Kamp K, Kaltsatou M, O’Toole D, Kaltsas G, de Herder W. Sequential everolimus and sunitinib treatment in pancreatic metastatic well-differentiated neuroendocrine tumours resistant to prior treatments. Neuroendocrinology. 2017;105(4):394–402. doi:10.1159/000456035
30. Armstrong AJ, Halabi S, Eisen T, et al. Everolimus versus sunitinib for patients with metastatic non-clear cell renal cell carcinoma (ASPEN): a multicentre, open-label, randomised phase 2 trial. Lancet Oncol. 2016;17(3):378–388. doi:10.1016/S1470-2045(15)00515-X
31. Bajetta E, Catena L, Fazio N, et al. Everolimus in combination with octreotide long-acting repeatable in a first-line setting for patients with neuroendocrine tumors: an ITMO group study. Cancer. 2014;120(16):2457–2463. doi:10.1002/cncr.28726
32. Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med. 2012;366(6):520–529. doi:10.1056/NEJMoa1109653
33. Baselga J, Semiglazov V, van Dam P, et al. Phase II randomized study of neoadjuvant everolimus plus letrozole compared with placebo plus letrozole in patients with estrogen receptor-positive breast cancer. J Clin Oncol. 2009;27(16):2630–2637. doi:10.1200/JCO.2008.18.8391
34. Bergmann L, Kube U, Doehn C, et al. Everolimus in metastatic renal cell carcinoma after failure of initial anti-VEGF therapy: final results of a noninterventional study. BMC Cancer. 2015;15:303. doi:10.1186/s12885-015-1309-7
35. Besse B, Leighl N, Bennouna J, et al. Phase II study of everolimus-erlotinib in previously treated patients with advanced non-small-cell lung cancer. Ann Oncol. 2014;25(2):409–415. doi:10.1093/annonc/mdt536
36. Campone M, Levy V, Bourbouloux E, et al. Safety and pharmacokinetics of paclitaxel and the oral mTOR inhibitor everolimus in advanced solid tumours. Br J Cancer. 2009;100(2):315–321. doi:10.1038/sj.bjc.6604851
37. Castellano D, Bajetta E, Panneerselvam A, et al. Everolimus plus octreotide long-acting repeatable in patients with colorectal neuroendocrine tumors: a subgroup analysis of the phase III RADIANT-2 study. Oncologist. 2013;18(1):46–53. doi:10.1634/theoncologist.2012-0263
38. Chan JA, Blaszkowsky L, Stuart K, et al. A prospective, phase 1/2 study of everolimus and temozolomide in patients with advanced pancreatic neuroendocrine tumor. Cancer. 2013;119(17):3212–3218. doi:10.1002/cncr.28142
39. Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1814–1823. doi:10.1056/NEJMoa1510016
40. Chow H, Ghosh PM, deVere White R, et al. A phase 2 clinical trial of everolimus plus bicalutamide for castration-resistant prostate cancer. Cancer. 2016;122(12):1897–1904. doi:10.1002/cncr.29927
41. Chung V, Frankel P, Lim D, et al. Phase Ib trial of mFOLFOX6 and everolimus (NSC-733504) in patients with metastatic gastroesophageal adenocarcinoma. Oncology. 2016;90(6):307–312. doi:10.1159/000445297
42. Ciruelos E, Vidal M, Martinez de Duenas E, et al. Safety of everolimus plus exemestane in patients with hormone-receptor-positive, HER2-negative locally advanced or metastatic breast cancer: results of phase IIIb BALLET trial in Spain. Clin Transl Oncol. 2017.
43. Ciunci CA, Perini RF, Avadhani AN, et al. Phase 1 and pharmacodynamic trial of everolimus in combination with cetuximab in patients with advanced cancer. Cancer. 2014;120(1):77–85. doi:10.1002/cncr.28294
44. Colon-Otero G, Weroha SJ, Foster NR, et al. Phase 2 trial of everolimus and letrozole in relapsed estrogen receptor-positive high-grade ovarian cancers. Gynecol Oncol. 2017;146(1):64–68. doi:10.1016/j.ygyno.2017.04.020
45. Courtney KD, Manola JB, Elfiky AA, et al. A phase I study of everolimus and docetaxel in patients with castration-resistant prostate cancer. Clin Genitourin Cancer. 2015;13(2):113–123. doi:10.1016/j.clgc.2014.08.007
46. Deenen MJ, Klumpen HJ, Richel DJ, et al. Phase I and pharmacokinetic study of capecitabine and the oral mTOR inhibitor everolimus in patients with advanced solid malignancies. Invest New Drugs. 2012;30(4):1557–1565. doi:10.1007/s10637-011-9723-4
47. Doi T, Muro K, Boku N, et al. Multicenter phase II study of everolimus in patients with previously treated metastatic gastric cancer. J Clin Oncol. 2010;28(11):1904–1910. doi:10.1200/JCO.2009.26.2923
48. El-Madani M, Colomban O, Tod M, et al. EVESOR, a model-based, multiparameter, Phase I trial to optimize the benefit/toxicity ratio of everolimus and sorafenib. Future Oncol. 2017;13(8):679–693. doi:10.2217/fon-2016-0357
49. Escudier B, Molinie V, Bracarda S, et al. Open-label phase 2 trial of first-line everolimus monotherapy in patients with papillary metastatic renal cell carcinoma: RAPTOR final analysis. Eur J Cancer. 2016;69:226–235. doi:10.1016/j.ejca.2016.08.004
50. Fazio N, Granberg D, Grossman A, et al. Everolimus plus octreotide long-acting repeatable in patients with advanced lung neuroendocrine tumors: analysis of the phase 3, randomized, placebo-controlled RADIANT-2 study. Chest. 2013;143(4):955–962. doi:10.1378/chest.12-1108
51. Ferolla P, Brizzi MP, Meyer T, et al. Efficacy and safety of long-acting pasireotide or everolimus alone or in combination in patients with advanced carcinoids of the lung and thymus (LUNA): an open-label, multicentre, randomised, phase 2 trial. Lancet Oncol. 2017;18(12):1652–1664. doi:10.1016/S1470-2045(17)30681-2
52. Finn RS, Poon RT, Yau T, et al. Phase I study investigating everolimus combined with sorafenib in patients with advanced hepatocellular carcinoma. J Hepatol. 2013;59(6):1271–1277. doi:10.1016/j.jhep.2013.07.029
53. Fury MG, Sherman E, Haque S, et al. A phase I study of daily everolimus plus low-dose weekly cisplatin for patients with advanced solid tumors. Cancer Chemother Pharmacol. 2012;69(3):591–598. doi:10.1007/s00280-011-1734-5
54. Ghobrial IM, Gertz M, Laplant B, et al. Phase II trial of the oral mammalian target of rapamycin inhibitor everolimus in relapsed or refractory Waldenstrom macroglobulinemia. J Clin Oncol. 2010;28(8):1408–1414. doi:10.1200/JCO.2009.24.0994
55. Goldberg HJ, Harari S, Cottin V, et al. Everolimus for the treatment of lymphangioleiomyomatosis: a phase II study. Eur Respir J. 2015;46(3):783–794. doi:10.1183/09031936.00210714
56. Gong C, Zhao Y, Wang B, et al. Efficacy and safety of everolimus in Chinese metastatic HR positive, HER2 negative breast cancer patients: a real-world retrospective study. Oncotarget. 2017;8(35):59810–59822. doi:10.18632/oncotarget.v8i35
57. Grignani G, Palmerini E, Ferraresi V, et al. Sorafenib and everolimus for patients with unresectable high-grade osteosarcoma progressing after standard treatment: a non-randomised phase 2 clinical trial. Lancet Oncol. 2015;16(1):98–107. doi:10.1016/S1470-2045(14)71136-2
58. Hainsworth JD, Spigel DR, Burris HA
59. Hatano T, Chikaraishi K, Inaba H, Endo K, Egawa S. Outcomes of everolimus treatment for renal angiomyolipoma associated with tuberous sclerosis complex: A single institution experience in Japan. Int J Urol. 2016;23(10):833–838. doi:10.1111/iju.2016.23.issue-10
60. Hatano T, Atsuta M, Inaba H, Endo K, Egawa S. Effect of everolimus treatment for renal angiomyolipoma associated with tuberous sclerosis complex: an evaluation based on tumor density. Int J Clin Oncol. 2017.
61. Hurvitz SA, Dalenc F, Campone M, et al. A phase 2 study of everolimus combined with trastuzumab and paclitaxel in patients with HER2-overexpressing advanced breast cancer that progressed during prior trastuzumab and taxane therapy. Breast Cancer Res Treat. 2013;141(3):437–446. doi:10.1007/s10549-013-2689-5
62. Jerusalem G, Mariani G, Ciruelos EM, et al. Safety of everolimus plus exemestane in patients with hormone-receptor-positive, HER2-negative locally advanced or metastatic breast cancer progressing on prior non-steroidal aromatase inhibitors: primary results of a phase IIIb, open-label, single-arm, expanded-access multicenter trial (BALLET). Ann Oncol. 2016;27(9):1719–1725. doi:10.1093/annonc/mdw249
63. Jovanovic B, Mayer IA, Mayer EL, et al. A randomized Phase II neoadjuvant study of cisplatin, paclitaxel with or without everolimus in patients with stage II/III Triple-Negative Breast Cancer (TNBC): responses and long-term outcome correlated with increased frequency of DNA damage response gene mutations, TNBC subtype, AR status, and Ki67. Clin Cancer Res. 2017;23(15):4035–4045. doi:10.1158/1078-0432.CCR-16-3055
64. Jozwiak S, Kotulska K, Berkowitz N, Brechenmacher T, Franz DN. Safety of everolimus in patients younger than 3 years of age: results from EXIST-1, a randomized, controlled clinical trial. J Pediatr. 2016;172:151–155 e151. doi:10.1016/j.jpeds.2016.01.027
65. Kato R, Obara W, Matsuura T, Kato Y, Iwasaki K, Fujioka T. Efficacy of everolimus in patients with advanced renal cell carcinoma refractory or intolerant to VEGFR-TKIs and safety compared with prior VEGFR-TKI treatment. Jpn J Clin Oncol. 2014;44(5):479–485. doi:10.1093/jjco/hyu018
66. Kim DW, Oh DY, Shin SH, et al. A multicenter phase II study of everolimus in patients with progressive unresectable adenoid cystic carcinoma. BMC Cancer. 2014;14:795. doi:10.1186/1471-2407-14-795
67. Kim JH, Lee W, Kim TN, Nam JK, Kim TH, Lee KS. Clinical outcomes of the sequential use of pazopanib followed by everolimus for the treatment of metastatic renal cell carcinoma: A multicentre study in Korea. Can Urol Assoc J. 2018;12(1):E15–E20. doi:10.5489/cuaj.4644
68. Koutsoukos K, Bamias A, Tzannis K, et al. Real-world experience of everolimus as second-line treatment in metastatic renal cell cancer after failure of pazopanib. Onco Targets Ther. 2017;10:4885–4893. doi:10.2147/OTT
69. Kulke MH, Ruszniewski P, Van Cutsem E, et al. A randomized, open-label, phase 2 study of everolimus in combination with pasireotide LAR or everolimus alone in advanced, well-differentiated, progressive pancreatic neuroendocrine tumors: COOPERATE-2 trial. Ann Oncol. 2017;28(6):1309–1315. doi:10.1093/annonc/mdx078
70. Kumano M, Miyake H, Harada K, Fujisawa M. Sequential use of mammalian target of rapamycin inhibitors in patients with metastatic renal cell carcinoma following failure of tyrosine kinase inhibitors. Med Oncol. 2013;30(4):745. doi:10.1007/s12032-013-0745-y
71. Moscetti L, Vici P, Gamucci T, et al. Safety analysis, association with response and previous treatments of everolimus and exemestane in 181 metastatic breast cancer patients: a multicenter Italian experience. Breast. 2016;29:96–101. doi:10.1016/j.breast.2016.07.005
72. Motzer RJ, Alyasova A, Ye D, et al. Phase II trial of second-line everolimus in patients with metastatic renal cell carcinoma (RECORD-4). Ann Oncol. 2016;27(3):441–448. doi:10.1093/annonc/mdv612
73. Motzer RJ, Barrios CH, Kim TM, et al. Phase II randomized trial comparing sequential first-line everolimus and second-line sunitinib versus first-line sunitinib and second-line everolimus in patients with metastatic renal cell carcinoma. J Clin Oncol. 2014;32(25):2765–2772. doi:10.1200/JCO.2013.54.6911
74. Motzer RJ, Hutson TE, Glen H, et al. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. Lancet Oncol. 2015;16(15):1473–1482. doi:10.1016/S1470-2045(15)00290-9
75. Oh DY, Kim TW, Park YS, et al. Phase 2 study of everolimus monotherapy in patients with nonfunctioning neuroendocrine tumors or pheochromocytomas/paragangliomas. Cancer. 2012;118(24):6162–6170. doi:10.1002/cncr.27675
76. Ohtsu A, Ajani JA, Bai YX, et al. Everolimus for previously treated advanced gastric cancer: results of the randomized, double-blind, phase III GRANITE-1 study. J Clin Oncol. 2013;31(31):3935–3943. doi:10.1200/JCO.2012.48.3552
77. Ohyama K, Matsumoto Y, Amamizu H, et al. Association of coronary perivascular adipose tissue inflammation and drug-eluting stent-induced coronary hyperconstricting responses in pigs: (18)F-fluorodeoxyglucose positron emission tomography imaging study. Arterioscler Thromb Vasc Biol. 2017;37(9):1757–1764. doi:10.1161/ATVBAHA.117.309843
78. Panzuto F, Rinzivillo M, Fazio N, et al. Real-world study of everolimus in advanced progressive neuroendocrine tumors. Oncologist. 2014;19(9):966–974. doi:10.1634/theoncologist.2014-0037
79. Park K, Lee JL, Ahn JH, et al. Efficacy and safety of everolimus in korean patients with metastatic renal cell carcinoma following treatment failure with a vascular endothelial growth factor receptor-tyrosine kinase inhibitor. Cancer Res Treat. 2014;46(4):339–347. doi:10.4143/crt.2013.154
80. Pavel M, Unger N, Borbath I, et al. Safety and QOL in patients with advanced NET in a Phase 3b expanded access study of everolimus. Target Oncol. 2016;11(5):667–675. doi:10.1007/s11523-016-0440-y
81. Quek R, Wang Q, Morgan JA, et al. Combination mTOR and IGF-1R inhibition: phase I trial of everolimus and figitumumab in patients with advanced sarcomas and other solid tumors. Clin Cancer Res. 2011;17(4):871–879. doi:10.1158/1078-0432.CCR-10-2621
82. Safra T, Kaufman B, Kadouri L, et al. Everolimus plus letrozole for treatment of patients with HR(+), HER2(-) advanced breast cancer progressing on endocrine therapy: an open-label, Phase II trial. Clin Breast Cancer. 2017.
83. Salazar R, Garcia-Carbonero R, Libutti SK, et al. Phase II study of BEZ235 versus Everolimus in patients with mammalian target of rapamycin inhibitor-naive advanced pancreatic neuroendocrine tumors. Oncologist. 2017.
84. Sarkaria JN, Galanis E, Wu W, et al. North Central Cancer Treatment Group Phase I trial N057K of everolimus (RAD001) and temozolomide in combination with radiation therapy in patients with newly diagnosed glioblastoma multiforme. Int J Radiat Oncol Biol Phys. 2011;81(2):468–475. doi:10.1016/j.ijrobp.2010.05.064
85. Strickler JH, Starodub AN, Jia J, et al. Phase I study of bevacizumab, everolimus, and panobinostat (LBH-589) in advanced solid tumors. Cancer Chemother Pharmacol. 2012;70(2):251–258. doi:10.1007/s00280-012-1911-1
86. Sun JM, Kim JR, Do IG, et al. A phase-1b study of everolimus plus paclitaxel in patients with small-cell lung cancer. Br J Cancer. 2013;109(6):1482–1487. doi:10.1038/bjc.2013.467
87. Takahashi K, Uchida K, Yoshimura N, et al. Efficacy and safety of concentration-controlled everolimus with reduced-dose cyclosporine in Japanese de novo renal transplant patients: 12-month results. Transplant Res. 2013;2(1):14. doi:10.1186/2047-1440-2-14
88. Tobinai K, Ogura M, Maruyama D, et al. Phase I study of the oral mammalian target of rapamycin inhibitor everolimus (RAD001) in Japanese patients with relapsed or refractory non-Hodgkin lymphoma. Int J Hematol. 2010;92(4):563–570. doi:10.1007/s12185-010-0707-5
89. Vlahovic G, Meadows KL, Uronis HE, et al. A phase I study of bevacizumab, everolimus and panitumumab in advanced solid tumors. Cancer Chemother Pharmacol. 2012;70(1):95–102. doi:10.1007/s00280-012-1889-8
90. Wang M, Popplewell LL, Collins RH
91. Werner D, Atmaca A, Pauligk C, Pustowka A, Jager E, Al-Batran SE. Phase I study of everolimus and mitomycin C for patients with metastatic esophagogastric adenocarcinoma. Cancer Med. 2013;2(3):325–333. doi:10.1002/cam4.77
92. Wolpin BM, Hezel AF, Abrams T, et al. Oral mTOR inhibitor everolimus in patients with gemcitabine-refractory metastatic pancreatic cancer. J Clin Oncol. 2009;27(2):193–198. doi:10.1200/JCO.2008.18.9514
93. Yao JC, Phan AT, Chang DZ, et al. Efficacy of RAD001 (everolimus) and octreotide LAR in advanced low- to intermediate-grade neuroendocrine tumors: results of a phase II study. J Clin Oncol. 2008;26(26):4311–4318. doi:10.1200/JCO.2008.16.7858
94. Yao JC, Shah MH, Ito T, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med. 2011;364(6):514–523. doi:10.1056/NEJMoa1009290
95. Yee KW, Zeng Z, Konopleva M, et al. Phase I/II study of the mammalian target of rapamycin inhibitor everolimus (RAD001) in patients with relapsed or refractory hematologic malignancies. Clin Cancer Res. 2006;12(17):5165–5173. doi:10.1158/1078-0432.CCR-06-0764
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.