")
Back to Journals » Cancer Management and Research » Volume 11
Stereotactic Radiotherapy for Parasagittal and Parafalcine Meningiomas: Patient Selection and Special Considerations
Authors Pinzi V , Fariselli L , Marchetti M , Scorsetti M, Navarria P
Received 7 September 2019
Accepted for publication 22 October 2019
Published 29 November 2019 Volume 2019:11 Pages 10051—10060
DOI https://doi.org/10.2147/CMAR.S187371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
V Pinzi,1 L Fariselli,1 M Marchetti,1 M Scorsetti,2 P Navarria2
1Neurosurgery Department, Radiotherapy Unit, Fondazione IRCCS Istituto Neurologico C. Besta, Milan, Italy; 2Radiotherapy and Radiosurgery Department, Humanitas Cancer Center and Research Hospital, Rozzano, Milan, Italy
Correspondence: V Pinzi
Neurosurgery Department, Radiotherapy Unit, Fondazione IRCCS Istituto Neurologico C. Besta, Via G. Celoria 11, Milan 20131, Italy
Tel +390223942312
Email [email protected]
Abstract: Treatment options for intracranial meningiomas are surgical resection alone, surgery followed by adjuvant radiation therapy (RT), or exclusive RT. Parasagittal and parafalcine meningiomas are a subgroup of meningeal disease located close to the vascular structures. Considering the frequent venous invasion, a complete resection is not possible in the majority of cases, and even if a Simpson Grade I resection can be performed, the risk of recurrence is relevant. To date, few studies are focused on parasagittal and parafalcine meningiomas. Because of their specific related issues, particular considerations on decision-making process, outcome, and toxicity follow-up are mandatory. In fact, parasagittal and parafalcine meningiomas require a clear-cut radiological assessment, as well as a tailored toxicity risk evaluation. Moreover, similarly to other meningioma sites, also for parasagittal and parafalcine ones, a standardization of local control, toxicity, and quality of life evaluation is needed in order to lead to a pooled analysis of the results. In this context, our aim was to review the literature data regarding the role of both single-session and multisession radiosurgery (RS), and stereotactic radiotherapy (SRT) for parasagittal and parafalcine meningioma management, summarizing available data on safety and efficacy. It was also discussed how RS and SRT can be performed in a setting of evolving views concerning the treatment paradigm of the parasagittal and parafalcine meningiomas.
Keywords: meningioma, parasagittal meningioma, parafalcine meningioma, stereotactic radiotherapy, radiosurgery, radiotherapy
Background
Meningiomas are the most common primary intracranial tumors in adults,1 and the parafalcine and parasagittal location account for 30% of them.2 The prognosis could be very different, based on several factors: the tumor grading, the type of surgery performed according to Simpson criteria,3,4 the presence of molecular alterations, and/or genetic syndromes.5,6 Treatment options include surgical resection, both single- and multisession radiosurgery (RS), and stereotactic radiotherapy (SRT). Notwithstanding, RS represents a valid and largely accepted option for treating intracranial meningioma,7 it is little employed in cases of parasagittal and parafalcine location compared to skull base site.7–9 The main treatment for parafalcine and parasagittal meningiomas is still surgical removal. Nevertheless, since parasagittal meningiomas often develop close to the vascular structures (eg, the superior sagittal sinus, critical bridging veins), and abut or invade venous structures, complete resection is not always achievable, and even if a Simpson grade I resection can be performed, the risk of recurrence is considerable.10–12 In these cases, RS in single- or multisession approach, as well as stereotactic radiotherapy (SRT) have been used in adjuvant setting7,11 with optimal results in terms of efficacy, and with a low incidence of toxicity.7 In addition, considering the risk of surgery-related neurological impairment, especially in the cases of elderly and frail patients, RS alone represents a valid treatment as an alternative to surgery, increasing the chances for quality of life preservation. Although these treatments represent the current standard options for meningioma patient management,13 controversies remain regarding the timing, the prescription doses, and the fractionation of RS/SRT.14 Besides, for parafalcine and parasagittal lesions, the radiation-related risk of developing edema seems to be higher than for other locations. So far, data on treatment-related symptom control and toxicity are not yet conclusive.7 From this perspective, the aim of this review was to evaluate the role of both single session and multisession RS/SRT, summarizing available data on long-term safety, and efficacy. It was also discussed how RS and SRT can be performed in a setting of evolving views concerning the treatment paradigm of the parasagittal and parafalcine meningiomas.
Methods
A PubMed search was carried out on the studies which investigated the effects of RS and SRT for parafalcine and parasagittal meningioma. The analyzed treatment was RS (high total dose of radiation delivered in 1 or few large fractions with dedicated device)15 in both exclusive and post-operative settings. We did not use any limit for outcome search strategy. Published papers, showing population data from the same Institute and the same period, were analyzed once.16,17 Studies including data for anatomical mixed population were considered not eligible for this review unless the data were reported separately.
Results
Literature data focused on RS and SRT outcomes for parasagittal and parafalcine meningiomas are very limited.8,10,18,19 Five studies were found reporting the lesion outcomes,8,16,19–21 in which only one single dose RS was employed. Only 1 study specifically addressed on fractionated RS.10 However, the population herein included was heterogeneous, and the authors did not analyze the site subgroups separately. Table 1 summarizes the analyzed RS series describing the outcomes for parasagittal and parafalcine meningiomas.
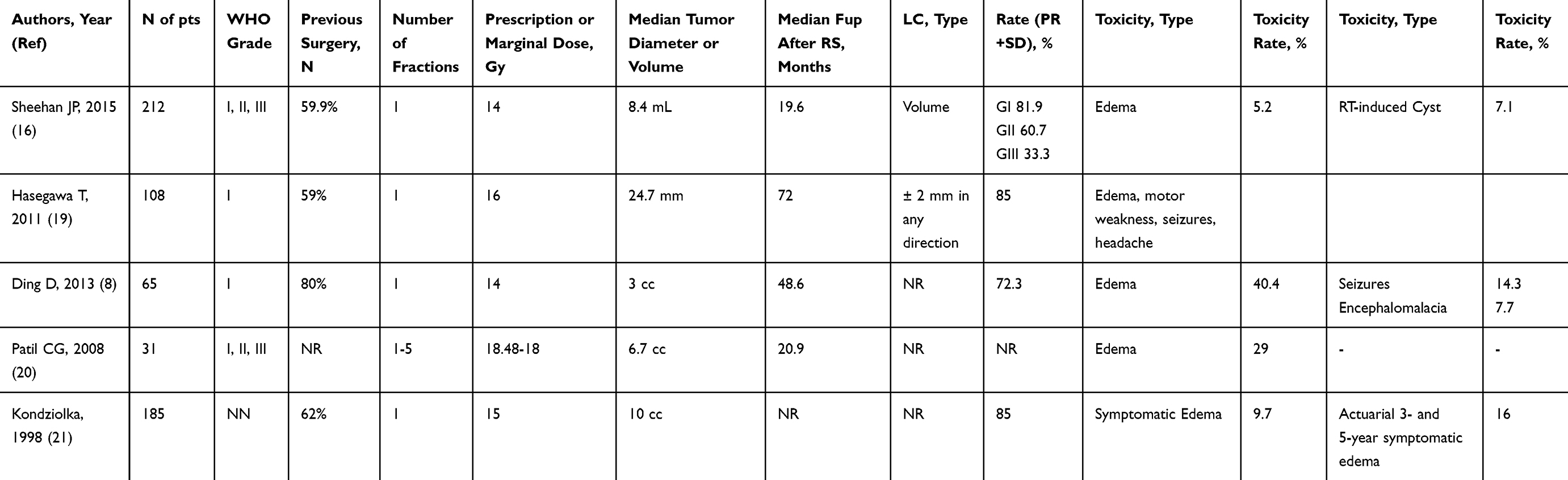 |
Table 1 Patient and Treatment Characteristics of the Analyzed Studies |
Discussion
Both parasagittal and parafalcine meningiomas present some clinical challenges. While the regional venous anatomy is important for both locations, the falcine tumors are more suitable for complete surgical resection. On the contrary, the parasagittal meningiomas are less likely amenable to be completely resected due to their adherence to the sagittal sinus. Some questions arise managing parasagittal and parafalcine meningiomas. Firstly, is the used radiological assessment complete with respect to their location anatomy? Usually, these meningiomas are radiologically approached in the same way as in other sites. Moreover, no information is provided in most of the published studies about radiological assessment for diagnosis and treatment planning. Is something missing? Secondly, is the therapeutic management similar to the entire cohort of meningiomas? Thirdly, is tumor control after treatment comparable to the results obtained with other meningioma sites? Lastly, are there any specific toxicity issues that should be more deeply considered? Is the narrative high risk to develop post-irradiation peritumoral edema truly higher than for other brain anatomical parts? Only few studies are focused on these types of meningiomas;8,16,19–21 however, distinct considerations on decision-making process, management, outcome, and toxicity follow-up are mandatory, because of their specific related issues.
Radiological Assessment
The backbone of radiation therapy is the correct assessment of radiological images. Computed tomography (CT) and magnetic resonance imaging (MRI) represent the basis of a precise and effective radiotherapy, being even pivotal for RS and SRT. Although the imaging plays a central role in the diagnosis and management of meningiomas, the studies focusing on these aspects are limited. Meningioma features are typical on CT and MRI, and images are diagnostic in 72–85% of the cases, including a sharply circumscribed lobular mass with a broad-based dural attachment.22 On basal CT, meningiomas appear as homogeneous and hyperdense extra-axial masses, and following contrast administration, they present homogeneous enhancement.23 CT images have also a key role in the identification of intratumoral calcification, expression of their slow growth rate, as well as bony changes sometimes associated with this type of tumors, such as hyperostosis, osteolysis, and pneumosinus dilatans. On MRI, meningiomas are usually hypo- to isointense relative to cerebral cortex on T1-weighted sequences, iso- to hyperintense on T2-weighted sequences, and they strongly enhance after contrast medium administration.24 MRI helps to identify the extra-axial nature of the tumor, often revealing a cerebrospinal fluid (CSF) cleft between the mass and the brain, which appears as a T2-weighted crescent. Another important feature that MRI allows is the presence of intratumoral cysts, hemorrhage, or necrosis, likely associated with more aggressive behavior of the tumor, as well as the dural tail. This latter is a sort of meningioma signature, and it is detectable on post-contrast imaging in up to 72% of the meningiomas23 and may represent reactive dural changes. However, one study found that in nearly two-thirds of dural tails there was tumor cell invasion.25 This aspect directly leads to the debate on either to treat or not also the dural tail . Similar to the dural tail, also the edema that can be associated with meningioma lesions affects the decision-making process, and radiological images are crucial in its identification and monitoring. Atypical and anaplastic meningiomas more frequently cause peritumoral edema by invading the brain. Less frequently, but not rarely, World Health Organization (WHO) grade I meningiomas present peritumoral brain edema. However, its intrinsic feature is the absence of brain invasion. The extension and how much the edema affects the surrounding tissues may influence which treatment is more appropriate. The evaluation of these aspects is essential for parafalcine and parasagittal lesions. These types of meningiomas, in fact, frequently cause peritumoral edema that can lead to symptoms, from headache to seizures. In addition to standard MRI sequences, it is important to note that thin-slice 3D views permit a precise delineation of the tumor and every nervous system part. Consequently, it allows a perfectly shaped irradiation plan. Moreover, fat-saturation sequences are particularly useful for delineation of meningioma boundaries abutting venous sinuses, enabling to discern the tumor surface from the perivascular fat and from vascular structures. Lastly, for parafalcine meningiomas likely to invade the adjacent vascular structures, CT or MR angiography can allow the recognition of displacement, encasement, and narrowing adjacent vessels, even sometimes invasion or occlusion of the dural venous sinuses, as long as proper sequences are available. Radiological imaging is fundamental not only for diagnosis and pre-treatment planning but also for post-treatment tumor control monitoring.26
Tumor Control
In the historical series of patients treated with external beam radiotherapy after partial surgical removal, postoperative irradiation showed better local control compared to surgery alone. Taylor et al27 reported an improved 10-year actuarial local control rate from 18% to 82%. Similarly, Wara et al28 showed 22% recurrence rate after subtotal resection plus radiotherapy, and 74% rate after subtotal resection alone. These results are similar to other published series, demonstrating the relevant impact of irradiation after surgical removal, even without the cutting-edge technology of current era. More recently, Ding et al published their results for parasagittal and parafalcine meningiomas after exclusive RS treatment.8 They showed a tumor control rate of 85% at 3 years, and 70% at 5 years. These results are slightly lower compared to other literature data on RS for differently located WHO G1 meningiomas.19 Taking into account the above, it must be believed that after RS cranial base lesions may have a more benign course and outcome than parafalcine and parasagittal ones. Unexpectedly, the authors found that parasagittal tumors had a higher control rate, and they conclude that this may be due to more superficial draining veins.8 Nevertheless, for patients without prior treatment, thus excluding previous resection, embolization, and radiotherapy, the actuarial tumor control rate at both 3 and 5 years was 93% for parafalcine and parasagittal meningiomas.8 Hence, it would be more appropriate to explain their results hypothesizing that prior treatments negatively affect the RS efficacy. Kondziolka et al reported an overall 5-year actuarial overall tumor control rate after RS of 67% ± 8.7%, and a 5-year actuarial in-field (within the targeted lesion) tumor control rate of 85% ± 6.2%.21 Also in this study, the tumor control for lesions without previous surgery was higher. In fact, for patients who underwent RS as primary treatment, the actuarial 5-year control rate was 93.4 ± 3.7%, while for patients who had undergone previous resection the local control rate was 60% ± 10.4% (P = 0.08).2115 On the contrary, the authors did not find any correlation between previous radiation treatment and tumor control. However, on multivariate analysis, the only two factors that significantly affected the tumor control were large treatment volume (P = 0.01, hazard rate ratio [HRR] = 1.06/cc), and the presence of pre-RS neurological deficits.21 Overall, in the studies analyzed in this review, the rate of tumor control for WHO GI meningiomas was from 72.3% to 85%, with a median follow-up time from 19.6 to 72 months. Certainly, long-term results are needed to confirm the RS and SRT efficacy. Closely related to the tumor control issue is the question on how assessing the local control after RS or SRT. To properly report local control, a befitting baseline appraisal is needed. In a recently published paper, the Response Assessment in Neuro-Oncology (RANO) Working Group suggested that26 all baseline evaluations should be performed as close as possible to the treatment start, and not more than 4 weeks before the beginning of treatment. However, since for RS or SRT meningioma treatment a pre-planning MRI is mandatory, this should be the baseline for every follow-up evaluation. Moreover, it is recommended to use thin-section imaging (≤1.5 mm pixel resolution), especially for evaluating lesions <10 mm in maximal diameter and/or small changes in lesion size,26 like the WHO grade I meningiomas treated with RS or SRT. Most of the published studies on meningiomas have described disease control assessment criteria; however, there is no uniform definition. Some authors referred to linear measurements, others used modified MacDonalds criteria, and few others relied on volumetric lesion evaluation.7,16 Even when adjusted for meningioma, the MacDonalds criteria, like many of the other ones, are often misleading.29 Hence, as some authors have highlighted, we should consider the post-irradiation volumetric analysis as the most reliable method to detect slow-growing meningioma volume changes, also due to the frequently irregular contour of these lesions.7,22,26,30 Furthermore, if dural tail cannot be discerned from the main lesion, as often is the case of en plaque meningiomas and parafalcine and parasagittal ones, the lesion should be considered as nonmeasurable by 2D criteria but it can still be measured by volumetric criteria.26 In the present study, 2 out of 5 authors reported the methodology used for tumor control evaluation. How frequent the radiological follow-up should be assessed is a matter of controversy. The National Comprehensive Cancer Network suggests monitoring WHO grades I and II meningiomas at 3, 6, and 12 months after initial treatment, followed by every 6–12 months for 5 years, and then every 1–3 years (NCCN version 1.2018). Meningiomas may exhibit delayed recurrence, even after 10 to 20 years from treatment, requiring long-term monitoring. For high-risk meningiomas (WHO grade III and for any grade that are treated for recurrence), more frequent imaging may be necessary, and it may depend on symptoms, and expected risk of relapse.
Toxicity Risk
Overall, treatment-related complications have been reported in approximately 8.1% of the patients treated using RS for intracranial meningiomas,7 with a value up to 40% when symptomatic edema has been included.8,16,17,19 The main risks associated with RS, for parafalcine and parasagittal meningiomas, are those usually associated with irradiation, as well as those directly due to their location. The array of RS-related complications includes radiation necrosis, motor deficit, vascular occlusion, and peritumoral edema. Moreover, a radiation-induced venous thrombosis and occlusion may result in delayed venous infarcts.31 Peritumoral edema associated with parasagittal or parafalcine meningiomas is common, with some series proving edema in 48% of the patients.32 In our analysis, only 3 authors reported this data, showing a peritumoral edema at baseline in 0%,20 3.7%,19 and 45.3%16 of the meningiomas, respectively. Only one study reported the rate of worsened, improved, and stable edema status after RS.16 The authors found a rate of improved edema after irradiation of 26.4% and only 5.2% of worsened cases. Unexpectedly, the rate of post-RS edema in all studies varied considerably, going from 5.2%16 to 40%.8 These results are consistent with those recently published by Milano et al.33 The authors reviewed the literature data about radiation-induced edema, and they found that except for skull base lesions, the rate of post-RS edema occurred in 5% to 43% of the patients treated.33 Due to the scarcity of data, we cannot assume any correlation. However, the minimum value of the post-RS edema was not correspondent to the minimum value of tumor volume, as well as the maximum one did not correlate to the higher volume of lesions. Similarly, the delivered dose did not seem to affect the post-irradiation edema risk. Thus, as of now, it is not possible to confirm that parafalcine and parasagittal meningiomas are more prone to develop post-RS peritumoral edema, and further data are needed. The post-RS edema usually occurs in a delayed phase. Sheehan et al17 found that for parafalcine and parasagittal tumors showing initial edema progression followed by regression, the median peak edema was at 18 months (range 6–24 months) after RS. For tumors with progressive edema at the last follow-up, the median interval between RS and peak of the edema was 36 months. Kondziolka et al13 found the onset of edema at 6–8 months after RS (range 1–23 months). In a previous study focused on parasagittal meningioma, the authors21 reported for both 3- and 5-year actuarial rate of symptomatic edema a value of 16% ± 3.8%. The symptoms occurred at 1 to 23 months after RS. Cai et al evaluated the risk factors of post-RS peritumoral edema for intracranial meningiomas of any location, and they found that the median time of new or worsening edema appearance was 4 months, but the at-risk period reported was within 48 months.34 In our study, the time of edema onset was 121 to 2416 months. Nevertheless, two studies did not report this data. In this context, despite the data being sparse, it should be considered that the post-RS monitoring would be more appropriate if 3 or 2 radiological exams per year were conducted for at least 3 years after treatment. A better understanding of the risk factors related to the edema post-RS would lead to a tailored treatment and follow-up. Numerous factors have been called into question. In a recently published review33 focused on all meningoma locations, the parasagittal one was found as a risk factor for radiation-induced edema. The series analyzed in the present study8,16,1,20,21 reported as risk factors the tumor volume, preexisting edema, preexisting neurological deficits, tumor–brain contact area, parasagittal and midline parasinus site, both fewer prior treatment and no previous resection, and high radiation doses. However, no one has been confirmed, and a well-conducted comparison among parasagittal, parafalcine, and other meningiomas is unavailable.35 All data on peritumoral edema of the analyzed studies are summarized in Table 2. Sheehan et al analyzed the factors related to the post-RS edema in parafalcine and parasagittal meningiomas.17 They found as risk factors a tumor volume > 10 cc, the presence of venous sinus compression or invasion, the parasagittal site, and a high maximal and marginal dose. Patil et al20 analyzed the risk of RS-related edema in the parasagittal meningiomas compared to other supratentorial locations. They found that patients with parasagittal meningiomas were 4.1 times more likely to develop symptomatic edema after RS (hazard ratio, 4.1; 95% confidence interval, 1.5–11.5; P 0.0076).20 However, the 6-, 12-, 18-, and 24-month actuarial rates of symptomatic edema development were significantly greater for patients with parasagittal meningiomas compared to non-parasagittal ones (17.8 versus 1.3%, 25.4 versus 5.8%, 35.2 versus 7.8%, and 35.2 versus 10.9%, respectively; P 0.0038, log-rank test).20 Notably, the authors also analyzed all midline parasinus tumors, including parasagittal, falcine, and pineal tumors. They found that midline parasinus meningiomas were 4.7 times more likely to develop symptomatic edema than non-midline supratentorial tumors (hazard ratio, 4.7; 95% confidence interval, 1.5–14.7; P = 0.0083).20 This implies that the risk factor may be the midline location instead of the solely parasagittal and parafalcine ones. All authors reported an almost complete resolution of the post-irradiation edema. A better knowledge of the edema development mechanism would help in identifying which supposed risk factors really affect the post-RS outcome. Nevertheless, the data on edema onset and evolution are insufficient. Cai et al hypothesized that damage to the tumor–brain contact interface is a key for the development of post-irradiation edema.34 The cause of post-RS edema in meningioma seems to be vasogenic rather than cytotoxic.36,37 Some authors reported that electronic microscopy analysis showed that in the white matter with edema, extracellular fluid increased, but the blood–brain barrier was not damaged, whereas meningioma revealed hyperpermeability of blood vessels. These findings suggest that the edema fluid may be produced by the meningioma tissue.38 Meanwhile, Salpietro et al37 were able to identify cortical penetration by CT evaluation and hypothesized a correlation between the disruption of the cerebral cortex and severity of the edema. Moreover, the disruption of leptomeninges and cerebral cortex can be directly correlated with the growth of tumors. In short, the lesion volume would be a cause of peritumoral edema. On the other hand, other authors did not find any correlation between tumor volume and post-irradiation edema20,37 but found tumor–brain contact interface area as strong predictor for the occurrence of post-irradiation edema.37 However, the exact pathophysiology of edema formation after irradiation remains unclear but some theories have been evaluated. The cerebrovascular impairment, the disruption of the blood–brain barrier, and the radiation-induced damage to microglia, and astrocytes may be correlated with the edema formation.38 Also the arachnoid layer disruption caused by close tumor/brain contact might lead to protein secretion generating a cascade effect up to edema formation.39 Some other authors reported different molecular factors as mediators implicated in edema induction, including inflammatory cytokines, angiogenesis factors (VEGF), hypoxia-related factors (HIF-1), cyclooxygenases, and markers of glial activation.39,40 In particular, VEGF-A that is an important member of a family of signaling molecules is expressed by meningioma stromal and endothelial cells in the presence of hypoxia.41,42 Moreover, some studies have suggested that VEGF may be secreted by meningiomas cells,41 and upregulation of VEGF has been observed in meningiomas, and it has been correlated with edema formation.39,41 This would imply the possibility to adopt an anti-VEGF therapy to overcome the post-irradiation edema, adding a valid alternative for symptomatic edema management. In fact, to reduce the peritumoral edema associated with meningiomas, corticosteroids represent the most used therapy. In the analyzed studies, almost all patients resolved the edema, the majority with the corticosteroid administration. Regarding the toxicity topic, it is noteworthy that the major limitation in RS toxicity includes a heterogeneity in the definition of adverse events, challenge in discriminating volume changes, and lack of adherence to the international toxicity grading systems.7 Despite being premature to draw any definitive conclusion, there is a favorable trend in a reported lower risk to develop post-irradiation edema when RS is delivered in multisession setting.10,43 This could broaden the patient selection for SRT or RS in treating parafalcine and parasagittal meningiomas.
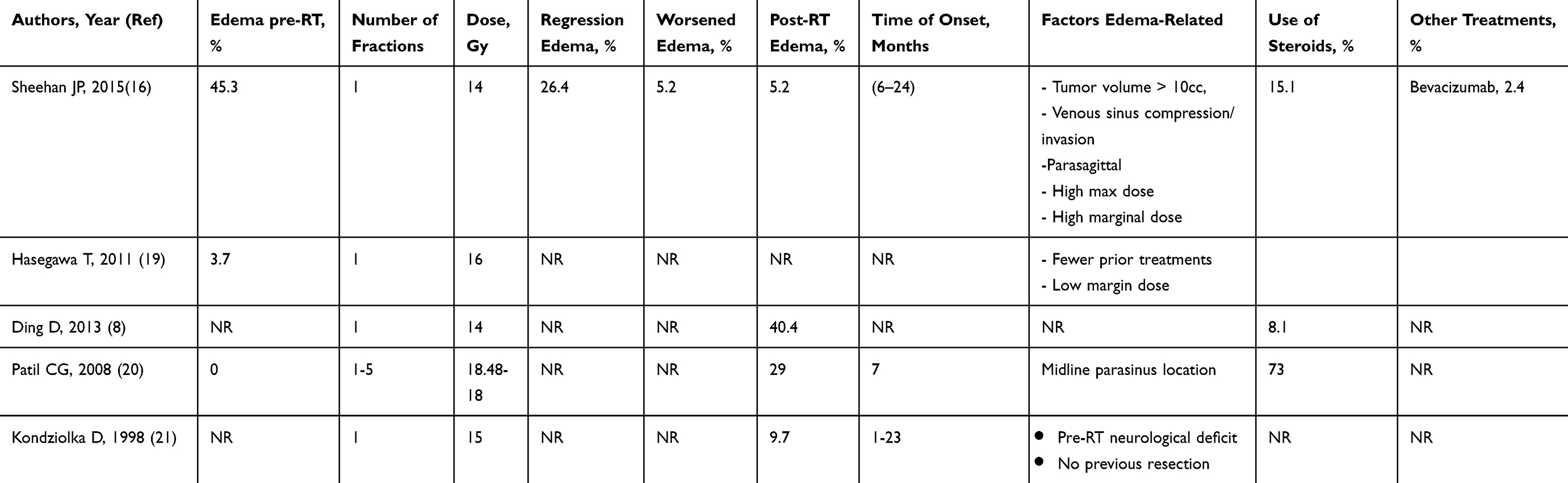 |
Table 2 Radiation-Induced Edema Characteristics of the Analyzed Studies |
Quality of Life
Another important aspect in the decision-making process for treating intracranial meningiomas, is patients quality of life (QoL). Only few studies have reported data about QoL after treatments for meningiomas.44–49 Only one study is focused on RS and parasagittal meningiomas, although the tests used for analysis were not detailed, and the primary endpoint was not QoL but ability to employment and functional status.21 However, it is crucial to highlight this topic to which we should pay attention in every clinical evaluation. Recently, a large cohort analysis has been published.44 The authors focused on QoL outcomes of 291 meningioma patients treated with surgical resection. Their results showed considerable limitations in QoL for more than 120 months after surgery, reporting impairment in cognitive, emotional, and social functions, as well as suffering significant fatigue and sleep disturbance.44 On the other hand, other studies showed an improved QoL after surgical resection.45,46 Some studies demonstrate an amelioration of patients QoL and neurocognitive function following treatments (surgery, radiotherapy or combination of them), on the contrary others show a persistence of neurocognitive deficits for many years after therapies.46,47 In addition, some studies reported the brain tumor diagnosis, although benign, as a source of concern for the patients, strongly conditioning the QoL. Several authors highlighted a continued fear of tumor progression, or a perceived cognitive dysfunction, which may not always be reflected by objective testing.44,47 A recent published systematic review, focused on the relevance and comprehensiveness of the questionnaires used in meningioma research, found that the existing questionnaires (the general and brain tumor modules “Functional Assessment of Cancer Therapy” FACT-G and FACT-Br, and the SF-3630–33) do not cover all the relevant issues for patients with meningioma diagnosis.50 Kondziolka et al21 analyzed a large population of parasagittal meningiomas treated with RS. They found a decrease in functional status after RS in only 3 out of 33 employed patients (9%) and in 7 out of 77 unemployed patients (9%). Out of 57 patients with neurological deficits before RS, 7 improved (12%), 30 remained neurologically stable (53%), and 8 (14%) experienced neurological decline. Interestingly, among patients who had no neurological deficits at the time of RS (n = 53), 44 remained stable (83%), 6 experienced neurological decline (11%), and 3 underwent additional treatment (6%).21 As suggested by Nassiri et al,44 fatigue management, cognitive rehabilitation, and psychological and sleep management support are usually not offered but should be part of a multidisciplinary program. The lack of a validated, specific, and largely employed instrument for QoL evaluation in meningiomas44 precludes drawing any conclusion, but at the same time identifies an issue that needs to be addressed in the future.
Special Considerations: Cornerstones and Controversial Issues
An increase in tumor size > 10% is significantly associated with the development of clinical symptoms, even for small size tumors.51 It turns out the importance of frequent follow-up imaging especially in the first years from treatment. Preexisting peritumoral edema has a high chance (around 77%) of deteriorating after RS. Thus, in this case, or when the lesion has a large meningioma–brain contact interface, the RS treatment may increase the risk to develop symptomatic edema. A multidisciplinary approach should be advocated to the best decision for treating those patients, taking into account surgery, surgery followed by RS, multisession RS or SRT. The inclusion of dural tail in RS targeting and planning is a debated issue. Many parasagittal and parafalcine meningiomas have an extensive dural tail, which is generally not targeted with the aim to minimize the treatment volume. Some authors clearly suggest including the neoplastic dural base to the tumor excision.21 However, to date, no consolidate evidences are available about this topic, and more studies are needed to understand whether the dural tail inclusion could further decrease the long-term recurrence rate. As for the mechanism leading to the post-RS edema development, the reasons for different responses to radiation therapy and the effective dose for treating different types of meningiomas are not well known. Unfortunately, there is a lack of preclinical research on meningioma.52,53 Given that the response to radiotherapy depends not only on irradiation features but also on tumor radiosensitivity, a more focused radiobiological research is advocated.53 Addressing this issue could provide crucial information on the index of proliferation and neurobiological characteristics associated with the molecular pathways that regulate the apoptotic response of tissue, cellular, and genetic post-irradiation damage.52 With regard to the management of these tumors, some authors suggest be planned RS within a few months if a larger lesion with mass effect has been resected.18 Due to the high recurrence rate reported, even when an apparently total resection is obtained, a multidisciplinary approach is mandatory for parafalcine and parasagittal meningiomas. This concern is also related to the risk of neurological sequelae when an aggressive surgery is done.54 RS and SRT should always be taken into account as exclusive or adjuvant therapy when these meningiomas are in charge, sharing with patients all pros and cons of treatments. Additionally, the standardization of the assessment methods is very relevant in enabling comparison of the results between literature studies.7,55 In fact, the lack of a validated, specific, and largely employed instrument for edema evaluation, tumor control report, and QoL in meningiomas44 precludes drawing any conclusion but represent an unmet need that should be thoroughly addressed in future studies.
Glance Over Patient Selection
Taking into account that surgical removal is still the current standard treatment for these meningiomas, RS or SRT may be offered as an alternative to surgery in all parafalcine and parasagittal meningiomas that do not have a very large volume or do not show extensive peritumoral edema. However, some crucial issues should be pointed out before jumping too far. Referring back to the questions arisen in the first part of the discussion, our patient selection should begin with a proper radiological assessment. Thin-slice T1- and T2-weighted, and fat-saturation sequences of MRI should be required for pre-treatment evaluation. Moreover, for parafalcine meningiomas likely invading the adjacent vascular structures, CT or MR angiography could be obtained for better recognition of displacement, encasement, and narrowing adjacent vessels, even sometimes invasion or occlusion of the dural venous sinuses. The therapeutic management of these meningiomas certainly shares with the entire cohort of intracranial meningiomas most of the main aspects. First of all, the current standard approach that is still surgical removal. Secondly, the eventual alternative treatment that is irradiation by means of the modern cutting-edge technology, tallowing to deliver extremely precise, and therefore, safe radiotherapy. It should be clear that in the patient selection process, a multidisciplinary guidance is mandatory. Radiologists, surgeons, and radiation oncologists should share data, patient’s medical history, and also points of view before jumping too far into strict clinical decisions. Mainly, for parafalcine and parasagittal meningiomas, a shorter wait-and-scan approach could be appropriate due to the high risk of damage and occlusion of vessels and the high risk of edema development. Moreover, these lesions are frequently difficult to be completely removed, and if a partial surgical approach is planned, an adjuvant RS or SRT should be programmed based on the history of each patients. In cases of slow-growing lesions, a short to moderate follow-up (2 to 3 MRI per year) can be scheduled before confirming whether irradiation is needed. On the other hand, in cases of lesions with more rapid growing pattern, the radiation treatment should be planned in advance. This can provide a safe and effective approach and can allow patients to better deal with all difficulties tied to the psychological, functional, and medical issues related to the therapies. Notwithstanding that the literature data are insufficient for drawing any definitive conclusion, in cases of large lesions that cannot be completely excised, or when the peritumoral edema is negligible, RS and SRT can be evaluated as alternative therapeutic option to surgical removal.. In addition, also for elderly and frail patients and for those who are not comfortable with surgery, RS and SRT represent valid alternative options.
Conclusions
Taking into account all these data, comments, and suggestions, the resulting conclusions are that SRT and RS could be more widely applied for parafalcine and parasagittal meningiomas. Microsurgery remains the mainstay treatment for large intracranial meningiomas, in cases of presence of motor or sensory deficit, or in patients failed to previous RS, with the objective to control tumor growth. Although, it should be kept in mind that these meningiomas are associated with relatively higher rates of recurrence, and increased risk of injury to major venous channels, compared to meningiomas located elsewhere.54 In fact in these cases, irradiation by means of single session RS, multisession RS or SRT represents a viable option in both exclusive and adjuvant settings. For tumors >3 cm in maximum diameter, the indication for resection or RS should be debated. Certainly, if the goal is to improve symptoms related to the mass effect or rapidly reduce the peritumoral edema, the surgical removal represents the optimal therapeutic choice. Also subtotal resection followed by RS is a reasonable approach for these cases, especially when injury to critical venous structures is likely.8 However, RS and SRT showed excellent results in terms of tumor control and toxicity also when applied as exclusive treatmentIn fact, multisession RS or SRT can represent a valid option for large lesions, or for those with a wide peritumoral edema, in order to reduce the risk of sequelae. Undoubtedly more studies focused on this subgroup of meningiomas are needed, since the unique peculiarity due to their location, anatomy connection, and the resulting implication on planning RS. The delivery of multisession RS and SRT could represent a new paradigm for these lesions, possibly allowing to overcome the proper limitation of the single session RS.
Acknowledgment
The authors thank Ms Ann Marie Graham for English language editing.
Disclosure
M Marchetti reports grants and personal fees from accuracy europe and from AB Medica, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Pinzi V, Caldiera V, Schembri L, Cerniauskaite M, Fariselli L. Spontaneous resolution of visual loss due to optic pathway meningioma: a case report and a review of the literature. Brain Injury. 2016;30(2):225–229. doi:10.3109/02699052.2015.1089600
2. Pettersson-Segerlind J, Orrego A, Lönn S, Mathiesen T. Long- term 25-year follow-up of surgically treated parasagittal meningiomas. World Neurosurg. 2011;76:564–571. doi:10.1016/j.wneu.2011.05.015
3. Simpson D. The recurrence of intracranial meningiomas after surgical treatment. J Neurol Neurosurg Psychiatry. 1957;20(1):22–39. doi:10.1136/jnnp.20.1.22
4. Gousias K, Schramm J, Simon M. The Simpson grading revisited: aggressive surgery and its place in modern meningioma management. J Neurosurg. 2016;125(3):551–560. doi:10.3171/2015.9.JNS15754
5. Linsler S, Kraeme D, Driess C, et al. Molecular biological determinations of meningioma progression and recurrence. PLoS One. 2014;9(4):e94987. doi:10.1371/journal.pone.0094987
6. Suppiah S, Nassiri F, Bi WL, et al. Molecular and translational advances in meningiomas. Neuro Oncol. 2019;21(Supplement_1):i4–i17. doi:10.1093/neuonc/noy178
7. Pinzi V, Biagioli E, Roberto A, et al. I Floriani I. Radiosurgery for intracranial meningiomas: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2017;113:122–134. doi:10.1016/j.critrevonc.2017.03.005
8. Ding D, Xu Z, McNeill IT, Yen CP, Sheehan JP. Radiosurgery for parasagittal and parafalcine meningiomas. J Neurosurg. 2013;119(4):871–877. doi:10.3171/2013.6.JNS13110
9. Starke RM, Williams BJ, Hiles C, Nguyen JH, Elsharkawy MY, Sheehan JP. Gamma knife surgery for skull base meningiomas. J Neurosurg. 2012;116:588–597. doi:10.3171/2011.11.JNS11530
10. Girvigian MR, Chen JC, Rahimian J, Miller MJ, Tome M. Comparison of early complications for patients with convexity and parasagittal meningiomas treated with either stereo- tactic radiosurgery or fractionated stereotactic radiotherapy. Neurosurgery. 2008;62(5 Suppl):A19–A28. doi:10.1227/01.neu.0000325933.34154.cb
11. Eichberg DG, Casabella AM, Menaker SA, Shah AH, Komotar RJ. Parasagittal and parafalcine meningiomas: integral strategy for optimizing safety and retrospective review of a single surgeon series. Br J Neurosurg. 2019. doi:10.1080/02688697.2019.1635988
12. Mahmood A, Qureshi NH, Malik GM. Intracranial meningiomas: analysis of recurrence after surgical treatment. Acta Neurochir (Wien). 1994;126:53–58. doi:10.1007/BF01476410
13. Kondziolka D, Mathieu D, Lunsford LD, et al. Radiosurgery as definitive management of intracranial meningiomas. Neurosurgery. 2008;62:53–60. doi:10.1227/01.NEU.0000311061.72626.0D
14. Marcus HJ, Price SJ, Wilby M, Santarius T, Kirollos RW. Radiotherapy as an adjuvant in the management of intracranial meningiomas: are we practising evidence-based medicine? Br J Neurosurg. 2008;22(4):520–528. doi:10.1080/02688690802308687
15. Barnett GH, Linskey ME, Adler JR, et al. Stereotactic radiosurgery? An organized neurosurgery-sanctioned definition. J Neurosurg. 2007;106(1):1–5. doi:10.3171/jns.2007.106.1.1
16. Sheehan JP, Cohen-Inbar O, Ruangkanchanasetr R, et al. Post-radiosurgical edema associated with parasagittal and parafalcine meningiomas: a multicenter study. J Neurooncol. 2015;125(2):317–324. doi:10.1007/s11060-015-1911-1
17. Sheehan JP, Lee CC, Xu Z, Przybylowski CL, Melmer PD, Schlesinger D. Edema following Gamma Knife radiosurgery for parasagittal and parafalcine meningiomas. J Neurosurg. 2015;123(5):1287–1293. doi:10.3171/2014.12.JNS142159
18. Kondziolka D. Radiosurgery for parasagittal and parafalcine meningiomas. J Neurosurg. 2013;119(4):869–870. doi:10.3171/2013.3.JNS13574
19. Hasegawa T, Kida Y, Yoshimoto M, Iizuka H, Ishii D, Yoshida K. Gamma Knife surgery for convexity, parasagittal, and falcine meningioma. Clinical articles. J Neurosurg. 2011;114:1392–1398. doi:10.3171/2010.11.JNS10112
20. Patil CG, Hoang S, Borchers DJ
21. Kondziolka D, Flickinger JC, Perez B. Judicious resection and/or radiosurgery for parasagittal meningiomas: outcomes from a multicenter review. Neurosurgery. 1998;43(3):405–414. doi:10.1097/00006123-199809000-00001
22. Huang RY, Bi WL, Griffith B, et al. Imaging and diagnostic advances for intracranial meningiomas. Neuro Oncol. 2019;21(Supplement_1):i44–i61. doi:10.1093/neuonc/noy143
23. O’Leary S, Adams WM, Parrish RW, Mukonoweshuro W. Atypical imaging appearances of intracranial meningiomas. Clin Radiol. 2007;62(1):10–17. doi:10.1016/j.crad.2006.09.009
24. Amrazi B, Shiroishi MS, Liu CS. Advanced imaging of intracranial meningiomas. Neurosurg Clin N Am. 2016;27(2):137–143. doi:10.1016/j.nec.2015.11.004
25. Wen M, Jung S, Moon KS, et al. Immunohistochemical pro le of the dural tail in intracranial meningiomas. Acta Neurochir (Wien). 2014;156(12):2263–2273. doi:10.1007/s00701-014-2216-4
26. Huang RY, Bi WL, Weller M, et al. Proposed response assessment and endpoints for meningioma clinical trials: report from the response assessment in Neuro-Oncology Working Group. Neuro Oncol. 2019;21(1):26–36. doi:10.1093/neuonc/noy137
27. Taylor BW, Marcus RB, Friedman WA, Ballinger WE, Million RR. The meningioma controversy: postoperative radiation therapy. Int J Radiat Oncol Biol Phys. 1988;5:299–304. doi:10.1016/S0360-3016(98)90008-6
28. Turgut M, Ozcan OE, Benli K, et al. Factors affecting morbidity and mortality following surgical intervention in patients with intracranial me ningioma. Aust N Z J Surg. 1996;66:144–150. doi:10.1111/j.1445-2197.1996.tb01143.x
29. Quant EC, Wen PY. Response assessment in neuro-oncology. Curr Oncol Rep. 2011;13(1):50–56. doi:10.1007/s11912-010-0143-y
30. Zeidman LA, Ankenbrandt WJ, Du H, Paleologos N, Vick NA. Growth rate of non-operated meningiomas. J Neurol. 2008;255(6):891–895. doi:10.1007/s00415-008-0801-2
31. Conti A, Pontoriero A, Salamone I, et al. Protecting venous structures during radiosur- gery for parasagittal meningiomas. Neurosurg Focus. 2009;27(5):E11. doi:10.3171/2009.8.FOCUS09-157
32. Osawa T, Tosaka M, Nagaishi M, Yoshimoto Y. Factors affecting peritumoral brain edema in meningioma: special histological subtypes with prominently extensive edema. J Neurooncol. 2013;111:49–57. doi:10.1007/s11060-012-0989-y
33. Milano MT, Sharma M, Soltys SG, et al. Radiation-induced edema after single-fraction or multifraction stereotactic radiosurgery for meningioma: a critical review. Int J Radiat Oncol Biol Phys. 2018;101(2):344–357. doi:10.1016/j.ijrobp.2018.03.026
34. Cai R, Barnett GH, Novak E, Chao ST, Suh JH. Principal risk of peritumoral edema after stereotactic radiosurgery for intracranial meningioma is tumor-brain contact interface area. Neurosurgery. 2010;66:513–522. doi:10.1227/01.NEU.0000365366.53337.88
35. Chang JH, Chang JW, Choi JY, Park YG, Chung SS. Complications after gamma knife radiosurgery for benign meningiomas. J Neurol Neurosurg Psychiatry. 2003;74:226–230. doi:10.1136/jnnp.74.2.226
36. Bitzer M, Topka H, Morgalla M, Friese S, Wockel L, Voigt K. Tumor-related venous obstruction and development of peritumoral brain edema in meningiomas. Neurosurgery. 1998;42(4):730–737. doi:10.1097/00006123-199804000-00026
37. Salpietro FM, Alafaci C, Lucerna S, Iacopino DG, Todaro C, Tomasello F. Peritumoral edema in meningiomas: microsurgical observations of different brain tumor inter- faces related to computed tomography. Neurosurgery. 1994;35(4):638–642. doi:10.1227/00006123-199410000-00009
38. Papadopoulos MC, Saadoun S, Binder DK, et al. Molecular mechanisms of brain tumor edema. Neuroscience. 2004;129:1011–1020. doi:10.1016/j.neuroscience.2004.05.044
39. Hou J, Kshettry VR, Selman WR, Bambakidis NC. Peritumoral brain edema in intracranial meningiomas: the emergence of vascular endothelial growth factor-directed therapy. Neurosurg Focus. 2013;35(6):E2. doi:10.3171/2013.8.FOCUS13301
40. Kan P, Liu JK, Wendland MM, Shrieve D, Jensen RL. Peritumoral edema after stereotactic radiosurgery for intracranial meningiomas and molecular factors that predict its development. J Neurooncol. 2007;83(1):33–38. doi:10.1007/s11060-006-9294-y
41. Ding YS, Wang HD, Tang K, et al. Expression of vascular endothelial growth factor in human meningiomas and peritumoral brain areas. Ann Clin Lab Sci. 2008;38:344–351.
42. Stevens JM, Ruiz JS, Kendall BE. Observations on peritumoral oedema in menin- gioma. Part II. Mechanisms of oedema production. Neuroradiology. 1983;25(3):125–131. doi:10.1007/BF00455731
43. Unger KR, Lominska CE, Chanyasulkit J, et al. Risk factors for posttreatment edema in patients treated with stereotactic radiosurgery for meningiomas. Neurosurgery. 2012;70:639–645. doi:10.1227/NEU.0b013e3182351ae7
44. Nassiri F, Price B, Shehab A, et al. Life after surgical resection of a meningioma: a prospective cross-sectional study evaluating health-related quality of life. Neuro Oncol. 2019;21(Supplement_1):i32–i43. doi:10.1093/neuonc/noy152
45. Jakola AS, Gulati M, Gulati S, Solheim O. The in uence of surgery on quality of life in patients with intracranial meningiomas: a prospective study. J Neurooncol. 2012;110(1):137–144. doi:10.1007/s11060-012-0947-8
46. Meskal I, Gehring K, Rutten GJ, Sitskoorn MM. Cognitive functioning in meningioma patients: a systematic review. J Neurooncol. 2016;128(2):195–205. doi:10.1007/s11060-016-2115-z
47. Kangas M, Williams JR, Smee R. The association between post- traumatic stress and health-related quality of life in adults treated for a benign meningioma. Appl Res Qual Life. 2012;7(2):163–182. doi:10.1007/s11482-011-9159-1
48. Williams T, Brechin D, Muncer S, Mukerji N, Evans S, Anderson N. Meningioma and mood: exploring the potential for meningioma to affect psychological distress before and after surgical removal. Br J Neurosurg. 2019. doi:10.1080/02688697.2019.1571163
49. Goebel S, Mehdorn HM. Development of anxiety and depression in patients with benign intracranial meningiomas: a prospective long term study. Support Care Cancer. 2013;21:1365–1372. doi:10.1007/s00520-012-1675-5
50. Zamanipoor Najafabadi AH, Peeters MCM, Lobatto DJ, et al. Health-related quality of life of cranial WHO grade I meningioma patients: are current questionnaires relevant? Acta Neurochir (Wien). 2017;159(11):2149–2159. doi:10.1007/s00701-017-3332-8
51. Sughrue ME, Rutkowski MJ, Aranda D, Barani IJ, McDermott MW, Parsa AT. Treatment decision making based on the published nat- ural history and growth rate of small meningiomas. J Neurosurg. 2010;113(5):1036–1042. doi:10.3171/2010.3.JNS091966
52. Pinzi V, Bisogno I, Ciusani E, et al. In vitro assessment of radiobiology of meningioma: a pilot study. J Neurosci Meth. 2019;311:288–294. doi:10.1016/j.jneumeth.2018.11.003
53. Pinzi V, Bisogno I, Prada F, Ciusani E, Fariselli L. Radiotherapy of meningioma: a treatment in need of radiobiological research. Int J Radiat Biol. 2018;94(7):621–627. doi:10.1080/09553002.2018.1478157
54. Giombini S, Solero CL, Lasio G, Morello G Immediate and late outcome of operations for Parasagittal and falx meningiomas. Report of 342 cases. Surg Neurol 1984; 21:427–435. doi:10.1016/0090-3019(84)90446-4
55. Rogers L, Barani I, Chamberlain M, et al. Meningiomas: knowledge base, treatment outcomes, and uncertainties. A RANO review. J Neurosurg. 2015;122(1):4–23. doi:10.3171/2014.7.JNS131644
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.