")
Back to Journals » Journal of Hepatocellular Carcinoma » Volume 6
Status of, and strategies for improving, adherence to HCC screening and surveillance
Authors Francica G, Borzio M
Received 18 January 2019
Accepted for publication 26 June 2019
Published 24 July 2019 Volume 2019:6 Pages 131—141
DOI https://doi.org/10.2147/JHC.S159269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Giampiero Francica,1 Mauro Borzio2
1Unità Operativa Ecografia ed Ecointerventistica, Pineta Grande Hospital, Castel Volturno, Italy; 2Unità Operativa Complessa Gastroenterologia ed Endoscopia Digestiva, Azienda Socio Sanitaria TerritorialeMelegnano e della Martesana, Milano, Italy
Abstract: Hepatocellular carcinoma (HCC) represents the second leading cause of cancer deaths worldwide and the main cause of death in patients with cirrhosis. Secondary prevention of HCC can be accomplished through the serial application of screening tests (ultrasound with or without alpha-fetoprotein) to detect the presence of subclinical lesions amenable to potentially curative treatment, such as surgery and ablation. The efficacy of HCC screening is accepted by hepatologists in terms of decline in cancer-specific mortality, but its translation into clinical practice is less than ideal. The effectiveness of HCC screening is hampered by several factors: failure to identify at-risk patients, failure to access care and failure to detect HCC. For each of these steps, possible improvements are discussed in order to face the changing etiology of cirrhosis and expand the screening of at-risk populations by including selected nonalcoholic fatty liver disease patients.
Keywords: cirrhosis, hepatocellular carcinoma, ultrasound, alpha-fetoprotein, screening
Introduction
Hepatocellular carcinoma (HCC) represents a leading cause of cancer mortality, being the 5th most common cancer in men and representing the second leading cause of cancer death worldwide.1,2 HCC incidence in the United States and Europe has doubled over the past two decades, and HCC is the main cause of death in patients with cirrhosis.3
Surveillance represents a typical tool for secondary prevention of cancer and entails the serial application of screening tests to detect the presence of HCC among at-risk populations before the neoplasm becomes clinically suspected or evident.
When detected at a symptomatic stage, HCC is almost invariably fatal. By this stage, the cancer is usually large and untreatable, with rapid progression and an interval from diagnosis to death of 3–6 months.4 This pattern characterized the large majority of patients in the era before the development of ultrasound (US) and computed tomography (CT) scan and is still the pattern of presentation where these techniques are either not available or not applied.
However, HCC has a prolonged subclinical growth period5–8 during which curative treatments are often possible. The principal objective of surveillance is, therefore, the detection of subclinical lesions that might be amenable to potentially curative treatment.9–11
Although the efficacy of HCC screening is accepted by hepatologists, its effectiveness, ie, the benefits achieved in real practice and broader populations, is far from ideal. This explains why nonliver scientific societies have not endorsed HCC screening due to the lack of high-quality data. The US Preventive Services Task Force has not adopted an HCC practice guideline, the American Cancer Society makes no recommendation on HCC screening12 and the National Cancer Institute found no evidence that screening decreases mortality from HCC but did find evidence that screening could result in harm.13
Another major issue is the low adherence to screening programs: in order to achieve outcome improvements in HCC, at least 34% of individuals within a cirrhosis population must undergo surveillance to capture an early-stage diagnosis rate of at least 42%.14 In real life, reported HCC surveillance rates in most observational studies in the United States and Europe are far from these values.15–18
The latest meta-analysis, including 22 studies from North and South America, Europe and Asia and 19, 511 patients with advanced fibrosis or compensated cirrhosis (Ishak score≥3), was published in 2018.19 It revealed an overall adherence rate to HCC surveillance of 52% with wide differences in compliance rates between studies: in fact, it is higher in studies from Europe than in studies from the United States and Asia (70%, 42%, 33%, respectively) and in those patients with cirrhosis compared to patients without (52% and 32%, respectively). However, in the multivariate analysis, the study design (retrospective vs prospective) turned out to be the only independent predictor accounting for differences in adherence levels. Indeed, the true real-life adherence rate was of 39% based on estimates from retrospective studies where selection bias of patients was deemed to be less relevant.
Therefore, there is a need to improve quality data on HCC screening and to recognize the levels at which the screening fails in order to introduce corrections.
HCC screening: current status
In recent years, guidelines for HCC screening and surveillance have been issued by major liver disease scientific societies in Europe, the United States and Asia.9–11 Such endorsement relies on the assumption that HCC surveillance fulfills all the pre requisites that make the screening policy cost-effective, according to WHO recommendations.
First, HCC is a common cancer that is the 5th most common cancer in the world and is the third cause of cancer-related mortality, as estimated by the WHO (globacan.iarc.fr).
Second, the risk of disease in the target population is great enough to justify the costs (Box 1). Cirrhosis is considered the most important risk factor for the development of HCC, and, therefore, cirrhotics of any etiology are the patients who may benefit most from screening surveillance. Conventionally, the risk of developing HCC refers to the incidence rate of the disease per year in the target population. Several studies of cost-efficacy or cost-utility analysis have been carried out in the last 20 years.20–29 Although these models differed in terms of the inception cohort, input values and assumptions (surveillance techniques and surveillance intervals, the follow-up after identification of HCC, rate of patients undergoing curative treatment and costs), virtually all concluded that surveillance is cost effective and enables a reduction in mortality. All these studies confirmed that the cost efficacy of surveillance is critically dependent on the annual incidence of HCC even though an absolute cut off to institute surveillance was not achieved. Averaging out these studies suggests that surveillance is effective for patients with cirrhosis if the annual incidence of HCC exceeds 1.5–2%. This threshold is currently recommended by the most important international guidelines.9,10
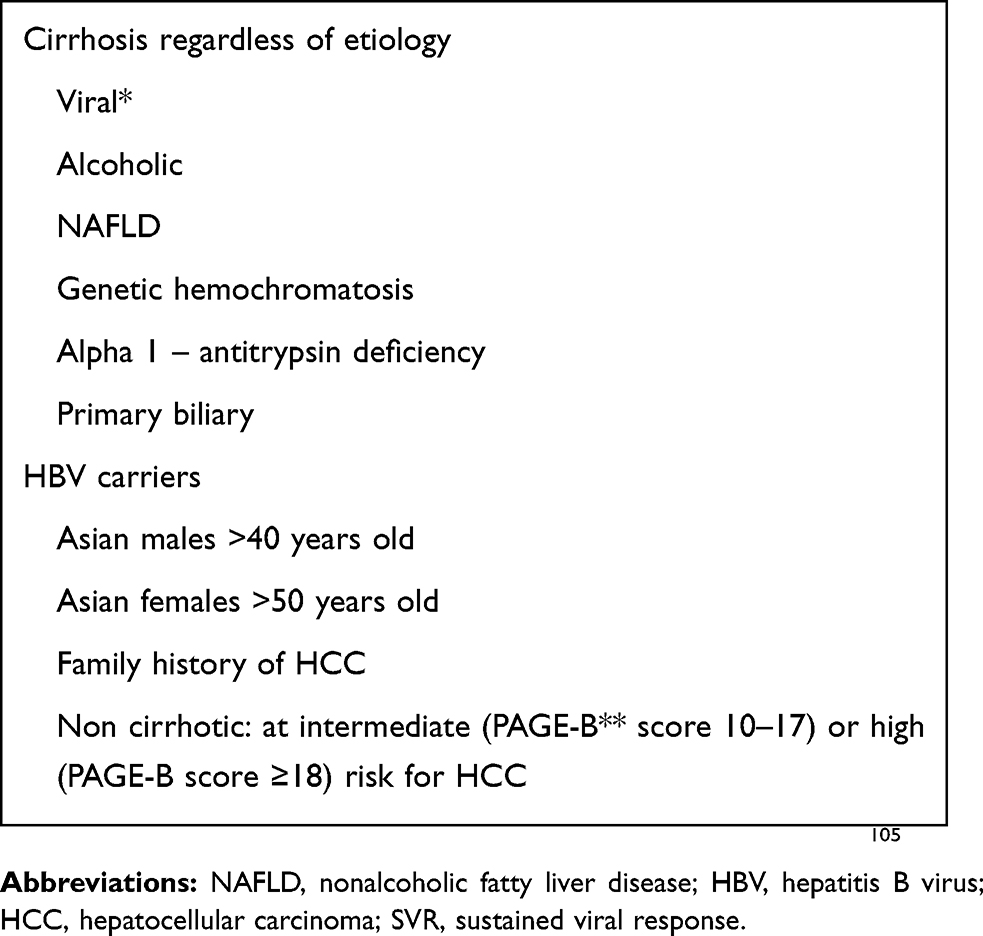 |
Box 1 Population group at high risk for HCC |
An HCC annual incidence equal to or exceeding 1.5–2% characterizes viral cirrhosis worldwide. A significant risk of cancer, although drastically reduced, still persists for both hepatitis B virus (HBV)- and hepatitis C virus (HCV)-related cirrhosis following viral suppression (HBV) or viral clearance (HCV) by direct-acting antivirals (DAA). For these reasons, both the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) recommend maintaining successfully treated patients under surveillance.9,10
An elevated risk above the threshold has been reported in cirrhosis due to genetic hemochromatosis irrespective of iron depletion.30 In patients with primary biliary cholangitis (PBC) at an advanced fibrotic stage (cirrhosis) the risk of HCC is similar to that seen in cirrhotic hepatitis C;31 hence, these patients also warrant surveillance.
For other types of liver diseases such as autoimmune, Wilson’s disease or α-1 antitrypsin deficiency, the risk of HCC is thought to be below the above mentioned threshold, and the guidelines do not recommend surveillance. In these instances, HCC incidence is thought to be increased only if cirrhosis is present. Concerns have been raised about the opportunity to offer regular surveillance to alcoholic cirrhotic patients who stopped drinking. A recent French study,32 however, showed that the incidence of HCC in alcohol-related cirrhosis is sufficient (being the lowest risk estimation in the best scenario of 1.4%) to justify performing HCC screening with regular imaging techniques, mainly US. The main problem is the high rate of noncompliant patients in this at-risk subgroup, given the large proportion of dropouts registered in the study.33
Surveillance of non alcoholic fatty liver disease (NAFLD) is still a matter of debate. The most recent epidemiological data34 provided two kinds of evidence: 1) although the risk of HCC is higher in NAFLD patients than that observed in the general clinical population without major liver disease risk factors, the absolute risk of HCC is too low to recommend universal HCC surveillance in the total NAFLD population; 2) cirrhosis is the major risk factor for HCC development in NAFLD patients, given that the risk of HCC in this subset of patients reached or exceeded the cut offs (0.8–2.3% per year) beyond which HCC surveillance becomes cost-effective.
In the NAFLD context, however, solid prospective information on the real cancer risk is still missing, and the precise indication to begin surveillance still remains unsettled.35 This conclusion also takes into account the notion that the accepted tool for screening (ie, US) is expected to under diagnose HCC at an early stage owing to the difficult assessment of severe fatty liver and/or obese patients. Moreover, first-line curative treatments (especially surgery) may be hampered in such a population where most of these patients are obese and carry concurrent cardiovascular diseases. However, it is conceivable that in the near future the population at risk for HCC will be broader due to the large number of NAFLD patients.
In non cirrhotic chronic viral hepatitis, the estimated risk of HCC is variable. In the absence of cost-efficacy modeling, expert opinion indicates that surveillance would be warranted if the annual incidence of HCC is at least 0.2%.36–38
In the HBV setting, the guidelines recommend surveillance in male patients aged >60 years, with a family history of HCC and higher levels of HBV replication.39,40 These patients carry a risk greater than the threshold as compared to the general population. Accordingly, international guidelines suggest that in non cirrhotic HBV patients, regular 6-month surveillance may not begin at baseline, but may be initiated whenever the abovementioned risk factors develop. This implies that these patients should undergo regular re assessment for entry into a surveillance program.
In the HCV setting, the incidence of HCC in F3 patients is too low to warrant regular surveillance.41 However, the exact staging of fibrosis is a challenge even at histological examination since fibrosis is a dynamic process which can either progress or regress over time. These patients should be regularly monitored with Fibroscan even if a cut off threshold to begin surveillance remains to be defined.
In summary, surveillance should be offered to patients in whom cirrhosis has etiology due to viral infection, hemochromatosis, PBC, or alcohol (with ongoing alcohol consumption). In viral cirrhosis, the risk of HCC is not totally eliminated in patients at risk after achieving sustained viral response (SVR) with both PegIFN-based and DAA-based therapies; therefore, surveillance should invariably be carried out. In HBV non cirrhotic patients, surveillance should be carried out only in the presence of additional risk factors, while in non cirrhotic HCV patients standard surveillance is not recommended unless bridging fibrosis is histologically documented. In non cirrhotic viral (HBV and HCV) chronic liver disease, transient elastography has been proposed as a useful tool to stratify the variable risk of HCC.42,43
Third, available test procedures are acceptable, safe, relatively inexpensive and offer a good balance between sensitivity (for early HCC detection) and specificity (to reduce false positive-related harm). The above-mentioned professional societies9–11 agree that US is the cornerstone of HCC screening, due to its widespread availability, low costs, lack of ionizing radiation, repeatability and acceptability by patients. However, limits of US should be considered: operator and US equipment dependency and technical limitations (coarse liver echo-texture, severe steatosis and obesity) explain why early HCC may be detected only in approximately one-third of patients with cirrhosis by using US alone.44,45 In order to increase the diagnostic performance of screening, other imaging techniques, such as CT or magnetic resonance imaging (MRI) have been proposed. However, their use in clinical practice is hampered by several limitations including the dangerously high rate of false-positive results, low availability, radiation risk, long duration of scan and, primarily, elevated costs (see the Failure to detect HCC section). Indeed, the AASL and EASL guidelines9,10 do not recommend the routine use of CT or MRI as they are not considered cost-effective for screening programs.
Whether adding α-fetoprotein (AFP) to US improves screening performance is a matter of debate. Conflicting results are reported in the literature, and the variable suggestions from liver disease societies across the world reflect such uncertainty: EASL guidelines9 do not recommend AFP in addition to US given its insufficient sensitivity and specificity; in contrast, AASLD10 states that is not possible to establish whether US should be coupled with AFP for HCC surveillance. A recent meta-analysis showed that, in studies comparing sensitivity for HCC with or without AFP, the pooled sensitivity of US alone was poor (63%) for early HCC and even worse in the subgroup of prospective studies (42%).46 By adding AFP measurement, a significant gain in pooled sensitivity (63%) was achieved in the subgroup of early HCCs, and this advantage of AFP was maintained in the subgroups of prospective studies (pooled sensitivity of 60%).
On the other hand, adopting AFP as a single tool for screening cannot be recommended since it is both a tumor marker and a regeneration marker. In chronic liver disease, elevated AFP serum levels may indeed simply reflect inflammation and subsequent regeneration.
Fourth, curative treatments are available to patients in whom HCC is discovered at an early stage owing to regular surveillance. Potentially curative treatments include orthotopic liver transplantation (OLT), resection and ablation and offer survival rates at 5 years ranging from 50% to 70%.9–11 In population-based series and in large prospective cohorts worldwide, the rate of patients receiving curative treatments is steadily increasing, thanks to the expansion of surveillance programs.16,47–49 Conversely, to avoid futility, this pre requisite would also imply that patients with either decompensated cirrhosis or severe co morbidities would not benefit from surveillance, and therefore they should not be offered any.50
HCC screening: limits
Although the efficacy of screening for HCC detection at an early stage has been affirmed by several studies and constitutes the basis of guidelines on HCC surveillance delivered by specialist societies, its translation into clinical practice is less than ideal.
This poor effectiveness might represent one of the reasons why HCC mortality has increased over the last two decades.51
A recent study by Moon et al52 failed to demonstrate a relationship between HCC screening and the decline in cancer-specific mortality, ie, one of the main goals of a screening program. These authors applied a matched case–control study design by selecting patients from the largest integrated health care system in the United States (Veterans Affairs): cirrhotic patients with fatal cancer (cases) were compared to those who did not die from it (controls), on the assumption that a lower adherence to screening programs in the cases should be expected. This analysis did not provide any evidence for a protective effect of specific mortality. The authors ascribed these findings to the low diagnostic performance of diagnostic tests which allow the identification only of slow-growing tumors (length bias) and/or the inadequacy of current treatments.
These results seem to reinforce those concerns raised regarding HCC surveillance which has been adopted in the United States in the absence of sufficient data to demonstrate its efficacy.53,54
In addition, potential screening-related undesired effects have recently been highlighted: in a retrospective cohort study 27.5% of patients under surveillance experienced physical harm, defined as CT or MRI scans or biopsies performed for false-positive or indeterminate surveillance findings.55 Similarly, Konerman et al56 found that 17% of 999 patients under a well-structured surveillance program had suspicious nodules without a final HCC diagnosis and experienced severe harm (eg, CT/MRI tests ≥4 or a liver biopsy). Although these two studies highlighted the potential harm mainly as multiple imaging evaluation, it should be pointed out that a detection rate of early HCC as high as 70–75%, allowing curative treatments, was reported in both papers. To date, albeit data on harm (including the not yet explored psychological and financial aspects) related to HCC screening are scanty, it seems that advantages of surveillance programs outweigh potential harm.
Indeed, benefits of well-structured surveillance programs have recently been confirmed by a prospective study57: in a large cohort of patients, the adherence to a HCC surveillance program after correction for lead-time bias played a pivotal role in the outcome of screened patients. Indeed, a timeframe <7 months was associated with a median survival twice as long as the survival observed in non compliant patients.
HCC screening: possible improvements
These conflicting results should prompt investigators and health care authorities to evaluate the topic of HCC screening limits and explore possible improvements at various levels.
Failure to identify at-risk patients
It is well known that up to 40% of patients present with HCC without having previously recognized liver disease and/or cirrhosis.58,59 In addition, the failure to recognize cirrhosis is strongly associated with advanced HCC stage at diagnosis and may be related to patient evaluation by non specialist care providers.60
In order to improve the recognition of those subjects at risk, a number of measures could be implemented:
- Increasing the use of electronic medical records to facilitate the recognition of patients with positive viral markers and the assessment of non invasive laboratory markers of liver disease and/or fibrosis such as the AST to platelet ratio index (APRI)58,61–63 in order to trigger the cascade of instrumental and/laboratory screening modalities (see below) in a larger population of patients;
- Reduce under-recognition of HCV-positive cases: Centers for Disease Control and Prevention and the US Public Health Task Force recommended one-time testing for anti-HCV for people born between the years 1945 and 1965, a period of time when the highest incidence of HCV was found.64,65 Recently, in France and the United States, universal screening for HCV has been proposed based on the assumption that it is cost-effective in terms of increased life expectancy and quality-adjusted life years, provided that early therapy is started with direct-acting Antivirals (DAA) regardless of the stage of fibrosis.66–68
- Inclusion of other subsets of patients at risk: in NAFDL/non-alcoholic steatohepatitis (NASH) patients (especially those with obesity and/or diabetes) HCC may occur in the absence of cirrhosis69 in approximately 15% of cases, and is often recognized at an advanced stage when survival times are shorter.70 These poor outcomes do not result from a greater biological aggressiveness of NAFLD-related HCC but from delayed referral to tertiary care (or specialist) centers.71 What kind of NAFLD patients at risk for HCC should undergo regular surveillance is likely to be the huge health care question over the next few years. This will occur due to a decline in HCV infection as a consequence of effective eradicative therapy and the reduction of baby boomers, who are the major reservoir of HCV. On the basis of the most recent epidemiological data,34 it seems logical to assume that at least NAFLD-related cirrhosis warrants surveillance. Alcoholic etiology of cirrhosis should be reconsidered as well in the light of recent epidemiological evidence that annual HCC incidence in this specific population is well above the threshold which makes screening programs cost-effective.32
- Education of primary care providers (PCPs): it is maintained that PCPs under-recognize chronic liver disease and cirrhosis and may have misconceptions about how best to perform surveillance (timing and/or type of screening tools) and report several barriers to implementation (eg, not being up-to-date with current guidelines, lack of reminder systems for HCC surveillance).72 It is not by chance that the adherence rate improves dramatically if patients seek hepatogastroenterologic visits.59,72,73 Therefore, efforts should be undertaken to educate PCPs regarding at-risk populations with chronic liver disease of any etiology, the correct use of screening tools and the benefit of HCC surveillance. Since PCPs are one of the main steps toward improving screening, automated reminders could also be a mean to increase their awareness of HCC screening.74 A pilot study in Italy75 showed that implementation of a training program targeting PCPs, aimed at improving the identification of cirrhotic patients living in an area with a high prevalence of disease, led to improved HCC patient survival.
Failure to access care
Although patients’ adherence is not considered a major barrier to HCC screening, patient non compliance accounted for <10% of cases in which surveillance was not completed.73 Difficulty with the scheduling process, costs of surveillance testing and transportation difficulties may prevent access to screening especially in socio economically disadvantaged patients.76 Conversely, high levels of instruction and income, living in urban areas, and insurance coverage are all associated with more regular and effective surveillance.15,16,73
In this context, the type of health care system plays a pivotal role: wherever government health care authorities cover patient expenses and offer more screening tests and shorter screening intervals, a higher compliance to HCC surveillance is expected. This is the case of Japan, one of the few countries which carried out a national screening program.77 In contrast, in the United States different health care insurance systems exist, which explains, at least in part, the HCC screening adherence rate widely ranging between 12% and 80%.44,59,78–82 In addition, participation in screening campaigns of cirrhotic patients may be improved by mailed outreach strategies by providing information about HCC risk and the importance of semi annual surveillance, as well as direct patient telephone interviews aimed at encouraging those who did not adhere to surveillance.83 However, these strategies were not capable of either pushing surveillance rate above 30% in the enrolled population or significantly increasing the detection rate of early-stage HCC compared to standard surveillance modality (ie, HCC surveillance ordered by clinicians during any outpatient visit).
Failure to detect HCC
1. To overcome the above mentioned US limitations, CT- or MRI-based surveillance has been proposed.84,85 MRI proved the best method of surveillance for early HCC (sensitivity of 83.7%)85 but high costs, long scan times and low availability prevent the widespread use of MRI as an imaging technique for screening. An abbreviated MRI protocol (AMRI) which comprises two sequences performed approximately 20 mins after the intravenous injection of gadoxetate disodium86,87 can be performed at a lower cost in a shorter time than a complete examination, thus making it more suitable for routine HCC surveillance. In retrospective studies,86,88 AMRI has proven superior to US in diagnostic per-patient and per-lesion performance. Another AMRI protocol utilizing only T1-weighted pre contrast and dynamic post contrast images using an extracellular gadolinium contrast agent has recently been proposed.89 In this retrospective study conducted on 164 consecutive screenings, this AMRI protocol afforded examination time (7–10 mins) even shorter than an accurate US examination and showed a strong agreement with conventional MRI in categorizing newly detected lesions according to liver imaging reporting data system (LI-RADS). In addition, it is likely that AMRI would prove especially useful in the NAFLD populations where the diagnostic accuracy of US is greatly reduced.
In a recent mathematical model, bi annual contrast-enhanced AMRI showed a higher sensitivity than US and proved affordable when applied to high-risk patients, resulting in improvement of early tumor detection in a cost-effective manner.90 If these data are confirmed in controlled trials, AMRI could become a cost-effective alternative to conventional MRI for screening in cirrhosis even though scarce availability and costs of MRI remain problems to be solved.
2. AFP performance can be improved by monitoring longitudinal patterns of AFP over time: if the rate of increase of AFP and the degree of fluctuation of all AFP-values recorded within each patient are used rather than the last value of AFP, the accuracy of the test in detecting HCC among patients with hepatitis C and either advanced fibrosis or cirrhosis may increase.91,92 Several other tumor markers have been reported as good complements to AFP and have been used in clinical diagnosis, including lens culinaris agglutinin reactive AFP (AFP-L3%), des-γ-carboxy prothrombin (DCP), fucosylated biomarkers (such as Golgi protein 73 and AFP), osteopontin, glypican-3, and micro-RNAs.93–101 Albeit these biomarkers have been evaluated as potential tools for HCC screening in some studies,94,100,101 so far they have not met the clinical requirements for HCC surveillance. Prospective studies are needed to externally validate their accuracy for early detection of HCC.102
Future directions
In the era of precision medicine and limited resources, screening programs have to accomplish the difficult task of personalized surveillance according to the risk of disease since HCC risk is not uniform across all patients with the same clinical conditions such as cirrhosis owing to different etiologies.
Risk scores providing a numerical cut off for the 5- and 10-year risk of developing HCC have been proposed. These scores have been developed for hepatitis B and for hepatitis C separately, as well as for cirrhosis (of any etiology). Several risk scores have been developed for hepatitis B.40,103–105 Among them the Risk Estimation for Hepatocellular Carcinoma in chronic hepatitis B (REACH-B)40 and the Platelets, Age, Gender in chronic hepatitis B (PAGE-B)105 and their recent modifications106,107 are the most popular. The first has been developed and validated in Asian patients without cirrhosis using clinical parameters such as sex, age, serum alanine aminotransferase (ALT) concentration, HBeAg status plus HBV-DNA status.40 Accordingly, atminimum score values (0–6), the 10-year risk of having HCC is negligible (<1%), while at the value of 16 the 3-, 5-, 10-yeas risk is 15%, 32%, 64%, respectively. Recently, HBV-DNA status has been replaced by liver stiffness (as a measure of liver fibrosis) based on the assumption that HBV clearance can easily be achieved in the era of effective antiviral therapy, therefore leading to overestimation of the incidence of HCC.106
PAGE-B score was first developed in Caucasian patients with chronic hepatitis without HCC and treated with first-line oral antivirals for ≥12 months. Based on simple clinical variables (age, gender, and platelets), this score proved useful in the assessment of the 5-year risk of HCC: a high PAGE-B score (≥18) should prompt continuous and careful surveillance in that the 5-year cumulative risk of HCC is 17% in this subgroup of patients. Recently, a modified PAGE-B score by adding serum albumin levels has been validated in Asian populations.107
A risk score for HCV patients has been developed using the Hepatitis C Antiviral Long-term Treatment against Cirrhosis (HALT-C) cohort.41This model includes age, alkaline phosphatase (ALP), black race, albumin, gastroesophageal varices and platelets. The calculation is complex, and the score has not been validated so far. For these reasons, its use is not recommended.
To further refine HCC prediction, the combination of serum concentrations of three biomarkers (AFP, AFP-L3% and DCP), with patient sex and age has been proposed as a diagnostic model (GALAD),108 and preliminary clinical results seem to support a widespread use in clinical practice.109 Improvement of the GALAD score has recently been reported by adding US results (presence of a solid lesion on surveillance).110 Another risk score, the Doylestown algorithm, incorporates biomarkers (AFP and fucosylated biomarkers) and relevant clinical variables (age, gender and ALT) with ALP.111 Although promising, these clinical scores have not yet been widely approved for HCC screening.
To supplement these imperfect clinical scores, new molecular biomarkers have been explored.112,113 Several germline single-nucleotide polymorphisms in epidermal growth factor and myeloperoxidase genes have been associated with elevated HCC risk.114,115 Similarly, a prognostic 186-gene signature has been identified and validated as an HCC risk predictor in patients with chronic liver disease with different etiologies.116,117
Once again, all these molecular biomarkers are far from being in widespread use in clinical practice.
In summary, although there is evidence of the benefits of HCC surveillance in terms of improved specific cancer mortality, improving modality of, and tools for, screening is necessary in order to cope with future scenarios where the etiology of cirrhosis is changing and the population at risk is becoming larger.
Disclosure
The authors certify that they have no affiliations with, or involvement in, any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
2. Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liver diseases in the world. J Hepatol. 2019;70(1):151–171. doi:10.1016/j.jhep.2018.09.014
3. Bertuccio P, Turati F, Carioli G, et al. Global trends and predictions in hepatocellular carcinoma mortality. J Hepatol. 2017;67(2):302–309. doi:10.1016/j.jhep.2017.03.011
4. Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19(3):329–338. doi:10.1055/s-2007-1007122
5. Taouli B, Goh JS, Lu Y, et al. Growth rate of hepatocellular carcinoma: evaluation with serial computed tomography or magnetic resonance imaging. J Comput Assist Tomogr. 2005;29(4):425–429.
6. Barbara L, Benzi G, Gaiani S, et al. Natural history of small untreated hepatocellular carcinoma in cirrhosis: a multivariate analysis of prognostic factors of tumor growth rate and patient survival. Hepatology. 1992;16(1):132–137.
7. Sheu JC, Sung JL, Chen DS, et al. Growth rate of asymptomatic hepatocellular carcinoma and its clinical implications. Gastroenterology. 1985;89(2):259–266.
8. An C, Choi YA, Choi D, et al. Growth rate of early-stage hepatocellular carcinoma in patients with chronic liver disease. Clin Mol Hepatol. 2015;21(3):279–286. doi:10.3350/cmh.2015.21.3.279
9. European Association for the Study of the Liver.European Association for the Study of the Liver.EASL Clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
10. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
11. Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11(4):317–370. doi:10.1007/s12072-017-9799-9
12. American Cancer Society. Can Liver Cancer Be Found Early? Vol. 2018. Atlanta, GA: American Cancer Society; 2016.
13. National Cancer Institute. Liver (hepatocellular) cancer screening—health professional version. Available from: https://www.cancer.gov/types/liver/hp/liver-screening.
14. Mourad A, Deuffic-Burban S, Ganne-Carrié N, et al. Hepatocellular carcinoma screening in patients with compensated hepatitis C virus (HCV)-related cirrhosis aware of their HCV status improves survival: a modeling approach. Hepatology. 2014;59(4):1471–1481. doi:10.1002/hep.26944
15. Davila JA, Morgan RO, Richardson PA, Du XL, McGlynn KA, El-Serag HB. Use of surveillance for hepatocellular carcinoma among patients with cirrhosis in the United States. Hepatology. 2010;52(1):132–141. doi:10.1002/hep.23615
16. Davila JA, Henderson L, Kramer JR, et al. Utilization of surveillance for hepatocellular carcinoma among hepatitis C virus-infected veterans in the United States. Ann Intern Med. 2011;154(2):85–93.
17. Schutte K, Bornschein J, Kahl S, et al. Delayed diagnosis of HCC with chronic alcoholic liver disease. Liver Cancer. 2012;1(3–4):257–266. doi:10.1159/000343840
18. Edenvik P, Davidsdottir L, Oksanen A, Isaksson B, Hultcrantz R, Stal P. Application of hepatocellular carcinoma surveillance in a European setting. What can we learn from clinical practice? Liver Int. 2015;35(7):1862–1871. doi:10.1111/liv.12764
19. Zhao C, Jin M, Le RH, et al. Poor adherence to hepatocellular carcinoma surveillance: a systematic review and meta-analysis of a complex issue. Liver Int. 2018;38(3):503–514. doi:10.1111/liv.13555
20. Kang JY, Lee TP, Yap I, Lun KC. Analysis of cost-effectiveness of different strategies for hepatocellular carcinoma screening in hepatitis B virus carriers. J Gastroenterol Hepatol. 1992;7(5):463–482.
21. Arguedas MR, Chen VK, Eloubeidi MA, Fallon MB. Screening for hepatocellular carcinoma in patients with hepatitis C cirrhosis: a cost-utility analysis. Am J Gastroenterol. 2003;98(3):679–690.
22. Lin OS, Keeffe EB, Sanders GD, Owens DK. Cost-effectiveness of screening for hepatocellular carcinoma in patients with cirrhosis due to chronic hepatitis C. Aliment Pharmacol Ther. 2004;19(11):1159–1726. doi:10.1111/j.1365-2036.2004.01963.x
23. Andersson KL, Salomon JA, Goldie SJ, Chung RT. Cost effectiveness of alternative surveillance strategies for hepatocellular carcinoma in patients with cirrhosis. Clin Gastroenterol Hepatol. 2008;6(12):1418–1424. doi:10.1016/j.cgh.2008.08.005
24. Sarasin FP, Giostra E, Hadengue A. Cost-effectiveness of screening for detection of small hepatocellular carcinoma in western patients with child-pugh class A cirrhosis. Am J Med. 1996;101(4):422–434. doi:10.1016/S0002-9343(96)00197-0
25. Patel D, Terrault NA, Yao FY, Bass NM, Ladabaum U. Cost-effectiveness of hepatocellular carcinoma surveillance in patients with hepatitis C virus-related cirrhosis. Clin Gastroenterol Hepatol. 2005;3(1):75–84.
26. Nouso K, Tanaka H, Uematsu S, et al. Cost-effectiveness of the surveillance program of hepatocellular carcinoma depends on the medical circumstances. J Gastroenterol Hepatol. 2008;23(3):437–444. doi:10.1111/j.1440-1746.2007.05054.x
27. Cucchetti A, Trevisani F, Cescon M, et al. Cost-effectiveness of semi-annual surveillance for hepatocellular carcinoma in cirrhotic patients of the Italian liver cancer population. J Hepatol. 2012;56(5):1089–1096. doi:10.1016/j.jhep.2011.11.022
28. Thompson Coon J, Rogers G, Hewson P, et al. Surveillance of cirrhosis for hepatocellular carcinoma: a cost-utility analysis. Br J Cancer. 2008;98(7):1166–1175. doi:10.1038/sj.bjc.6604301
29. Cadier B, Bulsei J, Nahon P; for ANRS CO12 CirVir and CHANGH groups, et al. Early detection and curative treatment of hepatocellular carcinoma: a cost-effectiveness analysis in France and in the United States. Hepatology. 2017;65(4):1237–1248. doi:10.1002/hep.28961.
30. Nowak A, Giger RS, Krayenbuehl PA. Higher age at diagnosis of hemochromatosis is the strongest predictor of the occurrence of hepatocellular carcinoma in the Swiss hemochromatosis cohort: a prospective longitudinal observational study. Medicine (Baltimore). 2018;97(42):e12886. doi:10.1097/MD.0000000000012886
31. Cavazza A, Caballería L, Floreani A, et al. Incidence, risk factors, and survival of hepatocellular carcinoma in primary biliary cirrhosis: comparative analysis from two centers. Hepatology. 2009;50(4):1162–1168. doi:10.1002/hep.23095
32. Ganne-Carrié N, Chaffaut C, Bourcier V; for CIRRAL Group, et al. Estimate of hepatocellular carcinoma incidence in patients with alcoholic cirrhosis. J Hepatol. 2018;69(6):1274–1283. doi:10.1016/j.jhep.2018.07.022.
33. D’Amico G, Bataller R. Need for surveillance of hepatocellular carcinoma in patients with alcoholic cirrhosis. J Hepatol. 2018;69(6):1219–1220. doi:10.1016/j.jhep.2018.09.027
34. Kanwal F, Kramer JR, Mapakshi S, et al. Risk of hepatocellular cancer in patients with non-alcoholic fatty liver disease. Gastroenterology. 2018;155(6):1828–1837. doi:10.1053/j.gastro.2018.08.024
35. Kolly P, Dufour JF. Surveillance for hepatocellular carcinoma in patients with NASH. Diagnostics. 2016;6(2):E22. doi:10.3390/diagnostics6020022
36. Sherman M. Surveillance for hepatocellular carcinoma. Best Pract Res Clin Gastroenterol. 2014;28(5):783–793. doi:10.1016/j.bpg.2014.08.008
37. Wong VW-S, Janssen HLA. Can we use HCC risk scores to individualize surveillance in chronic hepatitis B infection? J Hepatol. 2015;63(3):722–732. doi:10.1016/j.jhep.2015.05.019
38. Diaz-Gonzalez A, Forner A. Surveillance for hepatocellular carcinoma. Best Pract Res Clin Gastroenterol.2016;30(6):1001–1010. doi:10.1016/j.bpg.2016.04.007
39. Chen CJ, Yang HI, Iloeje UH. Hepatitis B virus DNA levels and outcomes in chronic hepatitis B. Hepatology. 2009;49(5 suppl):S72–S84. doi:10.1002/hep.22884
40. Yang HI, Yuen MF, Chan HL, et al. Risk estimation for hepatocellular carcinoma in chronic hepatitis B (REACH B): development and validation of a predictive score. Lancet Oncol. 2011;12(6):568–574. doi:10.1016/S1470-2045(11)70150-4
41. Lok AS, Seeff LB, Morgan TR, et al. Incidence of hepatocellular carcinoma and associated risk factors in hepatitis C-related advanced liver disease. Gastroenterology. 2009;136(1):138–148. doi:10.1053/j.gastro.2008.09.014
42. Masuzaki R, Tateishi R, Yoshida H, et al. Prospective risk assessment for hepatocellular carcinoma development in patients with chronic hepatitis C by transient elastography. Hepatology. 2009;49(6):1954–1961. doi:10.1002/hep.22870
43. Kim MN, Kim SU, Kim BK, et al. Increased risk of hepatocellular carcinoma in chronic hepatitis B patients with transient elastography-defined subclinical cirrhosis. Hepatology. 2015;61(6):1851–1859. doi:10.1002/hep.27735
44. Singal AG, Conjeevaram HS, Volk ML, et al. Effectiveness of hepatocellular carcinoma surveillance in patients with cirrhosis. Cancer Epidemiol Biomarkers Prev. 2012;21(5):793–799. doi:10.1158/1055-9965.EPI-11-1005
45. Del Poggio P, Olmi S, Ciccarese F, et al. Factors that affect efficacy of ultrasound surveillance for early stage hepatocellular carcinoma in patients with cirrhosis. Clin Gastroenterol Hepatol. 2014;12(11):1927–1933. doi:10.1016/j.cgh.2014.02.025
46. Tzartzeva K, Obi J, Rich NE, et al. Surveillance imaging and alpha fetoprotein for early detection of hepatocellular carcinoma in patients with cirrhosis: a meta-analysis. Gastroenterology. 2018;154(6):1706–1718. doi:10.1053/j.gastro.2018.01.064
47. Cucchetti A, Trevisani F, Pecorelli A, et al. Estimation of lead-time bias and its impact on the outcome of surveillance for the early diagnosis of hepatocellular carcinoma. J Hepatol. 2014;61(2):333–341. doi:10.1016/j.jhep.2014.03.037
48. Serper M, Taddei TH, Mehta R, et al. Association of provider specialty and multidisciplinary care with hepatocellular carcinoma treatment and mortality. Gastroenterology. 2017;152(8):1954–1964. doi:10.1053/j.gastro.2017.02.040
49. Borzio M, Dionigi E, Rossini A, et al. Trend of improving prognosis of hepatocellular carcinoma in clinical practice. An Italian In-Field Experience Dig Dis Sci. 2015;60(5):1465–1473. doi:10.1007/s10620-014-3427-5
50. Trevisani F, Santi V, Gramenzi A, et al. Surveillance for early diagnosis of hepatocellular carcinoma: is it effective in intermediate/advanced cirrhosis? Am J Gastroenterol. 2007;102(11):2448–2457. doi:10.1111/j.1572-0241.2007.01395.x
51. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2018. [Epub ahead of print]. doi:10.1002/ijc.31937
52. Moon AM, Weiss NS, Beste LA, et al. No association between screening for hepatocellular carcinoma and reduced cancer-related mortality in patients with cirrhosis. Gastroenterology. 2018;155(4):1128–1139. doi:10.1053/j.gastro.2018.06.079
53. Kelley MJ. Surveillance for hepatocellular carcinoma. Ann Intern Med. 2011;155(4):274. author reply 275. doi:10.7326/0003-4819-155-4-201108160-00016
54. Lederle FA, Pocha C. Screening for liver cancer: the rush to judgment. Ann Intern Med. 2012;156(5):387–389. doi:10.7326/0003-4819-156-3-201202070-00006
55. Atiq O, Tiro J, Yopp AC, et al. An assessment of benefits and harms of hepatocellular carcinoma surveillance in patients with cirrhosis. Hepatology. 2017;65(4):1196–1205. doi:10.1002/hep.28895
56. Konerman MA, Verma A, Zhao B, Singal AG, Lok AS, Parikh ND. Frequency and outcomes of abnormal imaging in patients with cirrhosis enrolled in a hepatocellular Carcinoma surveillance program. Liver Transpl. 2019;25(3):369–379. doi:10.1002/lt.25398
57. Costentin CE, Layese R, Bourcier V, et al. Compliance with hepatocellular carcinoma surveillance guidelines associated with increased lead-time adjusted survival of patients with compensated viral cirrhosis: a multi-center cohort study. Gastroenterology. 2018;155(2):431–442. doi:10.1053/j.gastro.2018.04.027
58. Stravitz RT, Heuman DM, Chand N, et al. Surveillance for hepatocellular carcinoma in patients with cirrhosis improves outcome. Am J Med. 2008;121(12):119–126. doi:10.1016/j.amjmed.2007.09.020
59. Singal AG, Yopp A, Gupta S, et al. Failure rates in the hepatocellular carcinoma surveillance process. Cancer Prev Res. 2012;5(9):1124–1130. doi:10.1158/1940-6207.CAPR-12-0046
60. Walker M, El-Serag HB, Sada Y, et al. Cirrhosis is under-recognised in patients subsequently diagnosed with hepatocellular cancer. Aliment Pharmacol Ther. 2016;43(5):621–630. doi:10.1111/apt.13505
61. Kramer JR, Davila JA, Miller ED, Richardson P, Giordano TP, El-Serag HB. The validity of viral hepatitis and chronic liver disease diagnoses in veterans affairs administrative databases. Aliment Pharmacol Ther. 2008;27(3):274–282. doi:10.1111/j.1365-2036.2007.03572.x
62. Lin ZH, Xin YN, Dong QJ, et al. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysis. Hepatology. 2011;53(3):726–736. doi:10.1002/hep.24105
63. Nehra M, Ma Y, Clark CB, Amarasingham R, Rockey DC, Singal AG. Use of administrative claims data for identifying patients with cirrhosis. J Clin Gastroenterol. 2013;47(5):e50–e54. doi:10.1097/MCG.0b013e3182688d2f
64. Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, Ward JW. Hepatitis C virus testing of persons born during 1945–1965: recommendations from the Centers for Disease Control and Prevention. Ann Intern Med. 2012;157(11):817–822. doi:10.7326/0003-4819-157-9-201211060-00529
65. Moyer VA. U.S. preventive services task force. Screening for hepatitis C virus infection in adults: U.S. preventive services task force recommendation statement. Ann Intern Med. 2013;159(5):349–357. doi:10.7326/0003-4819-159-5-201309030-00672
66. Deuffic-Burban S, Huneau A, Verleene A, et al. Assessing the cost-effectiveness of hepatitis C screening strategies in France. J Hepatol. 2018;69(4):785–792. doi:10.1016/j.jhep.2018.05.027
67. Rein DB, Wittenborn JS, Dougherty MC. The cost-effectiveness of a one-time hepatitis C virus antibody test followed by treatment for all Americans ages 18 and older as compared to current testing recommendations in the United States. J Hepatol. 2017;66:S405. doi:10.1016/S0168-8278(17)31168-6
68. Barocas JA, Tasillo A, Eftekhari Yazdi G, et al. Population level outcomes and cost-effectiveness of expanding the recommendation for age-based hepatitis C testing in the United States. Clin Infect Dis. 2018;67(4):549–556. doi:10.1093/cid/ciy098
69. Leung C, Yeoh SW, Patrick D, et al. Characteristics of hepatocellular carcinoma in cirrhotic and non-cirrhotic non-alcoholic fatty liver disease. World J Gastroenterol. 2015;21(4):1189–1196. doi:10.3748/wjg.v21.i10.2937
70. Giannini EG, Marabotto E, Savarino V, Italian Liver Cancer (ITALICA) Group, et al.. Hepatocellular carcinoma in patients with cryptogenic cirrhosis. Clin Gastroenterol Hepatol. 2009;7(5):580–585.
71. Piscaglia F, Svegliati-Baroni G, Barchetti A; HCC-NAFLD Italian Study Group, et al. Clinical patterns of hepatocellular carcinoma in nonalcoholic fatty liver disease: a multicenter prospective study. Hepatology. 2016;63(3):827–838. doi:10.1002/hep.28368.
72. Dalton-Fitzgerald E, Tiro J, Kandunoori P, Halm EA, Yopp A, Singal AG. Practice patterns and attitudes of primary care providers and barriers to surveillance of hepatocellular carcinoma in patients with cirrhosis. Clin Gastroenterol Hepatol. 2015;13(4):791–798. doi:10.1016/j.cgh.2014.06.031
73. Singal AG, Li X, Tiro J, et al. Racial, social, and clinical determinants of hepatocellular carcinoma surveillance. Am J Med. 2015;128(1):
74. Beste LA, Ioannou GN, Yang Y, Chang MF, Ross D, Dominitz JA. Improved surveillance for hepatocellular carcinoma with a primary care-oriented clinical reminder. Clin Gastroenterol Hepatol. 2015;13(1):172–179. doi:10.1016/j.cgh.2014.04.033
75. Del Poggio P, Olmi S, Ciccarese F, et al. A training program for primary care physicians improves the effectiveness of ultrasound surveillance of hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2015;27(9):1103–1108. doi:10.1097/MEG.0000000000000404
76. Farvardin S, Patel J, Khambaty M, et al. Patient-reported barriers are associated with lower hepatocellular carcinoma surveillance rates in patients with cirrhosis. Hepatology. 2017;65(3):875–884. doi:10.1002/hep.28770
77. Zhao C, Nguyen MH. Hepatocellular carcinoma screening and surveillance: practice guidelines and real-life practice. J Clin Gastroenterol. 2016;50(2):120–133. doi:10.1097/MCG.0000000000000446
78. Wong CR, Garcia RT, Trinh HN, et al. Adherence to screening for hepatocellular carcinoma among patients with cirrhosis or chronic hepatitis B in a community setting. Dig Dis Sci. 2009;54(12):2712–2721. doi:10.1007/s10620-009-1015-x
79. Sarkar M, Shvachko VA, Ready JB, et al. Characteristics and management of patients with chronic hepatitis B in an integrated care setting. Dig Dis Sci. 2014;59(9):2100–2108. doi:10.1007/s10620-014-3142-2
80. Ly CL, Wong LL. Ethnicity as a predictive factor for hepatocellular carcinoma screening among patients in Hawaii. Ethn Dis. 2014;24(3):376–381.
81. Palmer LB, Kappelman MD, Sandler RS, Hayashi PH. Surveillance for hepatocellular carcinoma in a Medicaid cirrhotic population. J Clin Gastroenterol. 2013;47(8):713–718. doi:10.1097/MCG.0b013e318286fd97
82. Tran SA, Le A, Zhao C, et al. Rate of hepatocellular carcinoma surveillance remains low for a large, real-life cohort of patients with hepatitis C cirrhosis. BMJ Open Gastroenterol. 2018;5(1):e000192. doi:10.1136/bmjgast-2017-000192
83. Singal AG, Tiro JA, Murphy CC, et al. Mailed outreach invitations significantly improve hcc surveillance rates in patients with cirrhosis: a randomized clinical trial. Hepatology. 2019;69(1):121–130. doi:10.1002/hep.30129
84. Pocha C, Dieperink E, McMaken KA, Knott A, Thuras P, Ho SB. Surveillance for hepatocellular cancer with ultrasonography vs computed tomography—a randomised study. Aliment Pharmacol Ther. 2013;38(3):303–312. doi:10.1111/apt.2013.38.issue-3
85. Kim SY, An J, Lim YS, et al. MRI with liver-specific contrast for surveillance of patients with cirrhosis at high risk of hepatocellular carcinoma. JAMA Oncol. 2017;3(4):456–463. doi:10.1001/jamaoncol.2016.3147
86. Marks RM, Ryan A, Heba ER, et al. Diagnostic per-patient accuracy of an abbreviated hepatobiliary phase gadoxetic acid-enhanced MRI for hepatocellular carcinoma surveillance. AJR Am J Roentgenol. 2015;204(3):527–535. doi:10.2214/AJR.14.12986
87. Besa C, Lewis S, Pandharipande PV, et al. Hepatocellular carcinoma detection: diagnostic performance of a simulated abbreviated MRI protocol combining diffusion- weighted and T1-weighted imaging at the delayed phase post gadoxetic acid.Abdom Radiol. 2017;42(1):179–190. doi:10.1007/s00261-017-1139-y
88. Tillman BG, Gorman JD, Hru JM, et al. Diagnostic per-lesion performance of a simulated gadoxetate disodium-enhanced abbreviated MRI protocol for hepatocellular carcinoma screening. Clin Radiol. 2018;73(5):485–493. doi:10.1016/j.crad.2017.11.013
89. Lee JY, Huo EJ, Weinstein S, et al. Evaluation of an abbreviated screening MRI protocol for patients at risk for hepatocellular carcinoma. Abdom Radiol. 2018;43(7):1627–1633. doi:10.1007/s00261-017-1339-5
90. Goossens N, Singal AG, King LY, et al. Cost-effectiveness of risk score-stratified hepatocellular carcinoma screening in patients with cirrhosis. Clin Transl Gastroenterol. 2017;8(6):e101. doi:10.1038/ctg.2017.26
91. Lee E, Edward S, Singal AG, Lavieri MS, Volk M. Improving screening for hepatocellular carcinoma by incorporating data on levels of alpha-fetoprotein, over time. Clin Gastroenterol Hepatol. 2013;11(4):437–440. doi:10.1016/j.cgh.2012.11.029
92. Tayob N, Lok AS, Do KA, Feng Z. Improved detection of hepatocellular carcinoma by using a longitudinal alpha-fetoprotein screening algorithm. Clin Gastroenterol Hepatol. 2016;14(3):469–475. doi:10.1016/j.cgh.2015.07.049
93. Lok AS, Sterling RK, Everhart JE, et al. Des-gamma-carboxy prothrombin and alphafetoprotein as biomarkers for the early detection of hepatocellular carcinoma. Gastroenterology. 2010;138(2):
94. Marrero JA, Feng Z, Wang Y, et al. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma. Gastroenterology. 2009;137(1):110–118. doi:10.1053/j.gastro.2009.04.005
95. Aoyagi Y, Isemura M, Suzuki Y, et al. Fucosylated alpha-fetoprotein as marker of early hepatocellular carcinoma. Lancet. 1985;2(8468):1353–1354. doi:10.1016/S0140-6736(85)92643-1
96. Wang M, Sanda M, Comunale MA, et al. Changes in the glycosylation of kininogen and the development of a Kininogen-based algorithm for the early detection of HCC. Cancer Epidemiol Biomarkers Prev. 2017;26(5):795–803. doi:10.1158/1055-9965.EPI-16-0974
97. Mao Y, Yang H, Xu H, et al. Golgi protein 73 (GOLPH2) is a valuable serum marker for hepatocellular carcinoma. Gut. 2010;59(12):1687–1693. doi:10.1136/gut.2010.214916
98. Shang S, Plymoth A, Ge S, et al. Identification of osteopontin as a novel marker for early hepatocellular carcinoma. Hepatology. 2012;55(2):483–490. doi:10.1002/hep.24703
99. Lin X-J, Chong Y, Guo Z-W, et al. A serum microRNA classifier for early detection of hepatocellular carcinoma: a multicentre, retrospective, longitudinal biomarker identification study with a nested case-control study. Lancet Oncol. 2015;16(7):804–815. doi:10.1016/S1470-2045(15)00048-0
100. Li B, Li B, Guo T, et al. Artificial neural network models for early diagnosis of hepatocellular carcinoma using serum levels of α-fetoprotein, α-fetoprotein-L3, des-γ-carboxy prothrombin, and Golgi protein 73. Oncotarget. 2017;8(46):80521–80530. doi:10.18632/oncotarget.19298
101. Choi J, Kim GA, Han S, Lee W, Chun S, Lim YS. Longitudinal assessment of three serum biomarkers to detect very early stage hepatocellular carcinoma. Hepatology. 2019;69(5):1983–1994. doi:10.1002/hep.30233
102. Yang JD, Patel T. Early detection of hepatocellular carcinoma: expanding the utility of circulating tumor markers. Hepatology. 2019;69(5):1855–1857. doi:10.1002/hep.30468
103. Yuen MF, Tanaka D, Fong YT, et al. Independent risk factors and predictive score for the development of hepatocellular carcinoma in chronic hepatitis B. J Hepatology. 2009;50(1):80–88. doi:10.1016/j.jhep.2008.07.023
104. Wong VW, Chan SL, Mo F, et al. Clinical scoring system to predict hepatocellular carcinoma in chronic hepatitis B carriers. J Clin Oncol. 2010;28(10):1660–1665. doi:10.1200/JCO.2009.26.2675
105. Papatheorodidis G, Dalekos G, Sypsa V, et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasian with chronic hepatitis B on 5-year antiviral therapy. J Hepatol. 2016;64(4):800–806. doi:10.1016/j.jhep.2015.11.035
106. Lee HW, Yoo EJ, Kim BK, et al. Prediction of development of liver-related events by transient elastography in hepatitis B patients with complete virological response on antiviral therapy. Am J Gastroenterol. 2014;109:1241–2499. doi:10.1038/ajg.2014.157
107. Kim JH, Kim YD, Lee M, et al. Modified PAGE-B score predicts the risk of hepatocellular carcinoma in Asians with chronic hepatitis B on antiviral therapy. J Hepatol. 2018;69(5):1066–1073. doi:10.1016/j.jhep.2018.07.018
108. Johnson PJ, Pirrie SJ, Cox TF, et al. The detection of hepatocellular carcinoma using a prospectively developed and validated model based on serological biomarkers. Cancer Epidemiol Biomarkers Prev. 2014;23(1):144–153. doi:10.1158/1055-9965.EPI-13-0870
109. Best J, Bilgi H, Heider D, et al. The GALAD scoring algorithm based on AFP, AFP-L3, and DCP significantly improves detection of BCLC early stage hepatocellular carcinoma. Z Gastroenterol. 2016;54(12):1296–1305. doi:10.1055/s-0042-119529
110. Yang JD, Addissie BD, Mara KC, et al. GALAD score for hepatocellular carcinoma detection in comparison to liver ultrasound and proposal of GALADUS score. Cancer Epidemiol Biomarkers Prev. 2018:
111. Wang M, Devarajan K, Singal AG, et al. The Doylestown algorithm: a test to improve the performance of AFP in the detection of hepatocellular carcinoma. Cancer Prev Res (Phila). 2016;9(2):172–179. doi:10.1158/1940-6207.CAPR-15-0186
112. Goossens N, Sun X, Hoshida Y. Molecular classification of hepatocellular carcinoma: potential therapeutic implications. Hepat Oncol. 2015;2(4):371–379. doi:10.2217/hep.15.26
113. Goossens N, Bian CB, Hoshida Y. Tailored algorithms for hepatocellular carcinoma surveillance: is one-size-fits-all strategy outdated? Curr Hepatol Rep. 2017;16(1):64–71. doi:10.1007/s11901-017-0336-z
114. Tanabe KK, Lemoine A, Finkelstein DM, et al. Epidermal growth factor gene functional polymorphism and the risk of hepatocellular carcinoma in patients with cirrhosis. JAMA. 2008;299(1):53–60. doi:10.1001/jama.2007.65
115. Abu Dayyeh BK, Yang M, Fuchs BC, et al. A functional polymorphism in the epidermal growth factor gene is associated with risk for hepatocellular carcinoma. Gastroenterology. 2011;141(1):141–149. doi:10.1053/j.gastro.2011.03.045
116. Hoshida Y, Villanueva A, Sangiovanni A, et al. Prognostic gene expression signature for patients with hepatitis C-related early-stage cirrhosis. Gastroenterology. 2013;144(5):1024–1030. doi:10.1053/j.gastro.2013.01.021
117. King LY, Canasto-Chibuque C, Johnson KB, et al. A genomic and clinical prognostic index for hepatitis C-related early-stage cirrhosis that predicts clinical deterioration. Gut. 2015;64(8):1296–1302. doi:10.1136/gutjnl-2014-307862
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.