")
Back to Journals » Patient Preference and Adherence » Volume 13
Status and associated factors of self-management in people living with HIV/AIDS in Liangshan area, China: a cross-sectional study
Authors Wang H, Chen AC, Wan S, Chen H
Received 1 February 2019
Accepted for publication 6 May 2019
Published 24 May 2019 Volume 2019:13 Pages 863—870
DOI https://doi.org/10.2147/PPA.S203799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Huan Wang,1 Angela Chia-Chen Chen,2 Shaoping Wan,3 Hong Chen1
1West China School of Nursing and Department of Nursing, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 2College of Nursing and Health Innovation, Arizona State University, Phoenix, AZ, USA; 3Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China
Background: HIV self-management is a lifetime and central task for people living with HIV/AIDS (PLWH). To date, there is little evidence to identify the related factors of self-management in PLWH from China.
Purpose: This study aimed to investigate the status and related factors of self-management in PLWH from the Liangshan area of Sichuan Province, China.
Patients and methods: A total of 322 PLWH were recruited from August to December 2017 in the study. Demographics characteristics and disease-related data were documented for each participant, social support was measured by the Medical Outcomes Study Social Support Survey (MOS-SSS-C), and self-management was evaluated by the HIV Self-Management Scale. Descriptive statistics analysis, independent Student’s t-test, one-way ANOVA, Spearman rank correlation, and multiple regression analysis were used to analyze the data.
Results: The total score of HIV self-management was 38.26±7.17. Significant differences in self-management scores were found among the subgroups of different education level, marital status, nation, religion, resident place, occupation, infection route, symptom, research site, and household per capita monthly income. Self-management was positively significantly correlated with social support. Multiple regression analysis identified that nation, resident place, gender, marital status, and social support were the contributors of HIV self-management.
Conclusion: The study demostrated that self-management in Yi Autonomous Prefecture was relatively low. The results indicate that the associated factors of self-management should be considered to develop effective intervention to improve the self-management of PLWH.
Keywords: self-management, self-care, HIV, HIV/AIDS, China
Introduction
The epidemic of AIDS has become a global public health issue. According to WHO,1 there were about 36.9 million people living with HIV/AIDS (PLWH) by the end of 2017, and 1.8 million people were newly-infected in 2017 worldwide. In China, about 850,000 people were currently living with HIV/AIDS up to 2018.2
With the introduction and widespread availability of highly active antiretroviral treatment (ART), the life expectancy of PLWH is gradually increasing,3,4 and AIDS is being accepted as a more manageable chronic disease.5,6 Thus, antiretroviral therapy adherence is crucial for PLWH to achieve optimal health outcomes and prevent disease progression.7–9 In additional to treatment adherence, PLWH often suffer from some other comorbidities, including cancers, diabetes mellitus, osteoporosis, cardiovascular, hepatic, pulmonary, and psychiatric disorders.10–12 These comorbidities propose additional challenges to PLWH, such as managing symptoms of different chronic illness and the interactions of these illnesses, and arranging appointments for different speciality care. Given the complexity of the tasks required to optimize health in PLWH, researchers13,14 find that self-management is important and remains challenging.
Self-management is defined as the ability of the individual, in conjunction with family, community, and healthcare professionals, to manage illness and promote health.15,16 For PLWH, self-management includes adherence to medication, self-monitoring, reduction of negative emotional states, positive social and family relationships, etc.17 Self-management is regarded as the best practice to improve clinical care and outcomes, and can also reduce burden on healthcare system resources and capacities for chronic diseases.18,19 Recent research showed self-management could directly and indirectly reduce susceptibility to worsening HIV20 and some burdensome physical comorbidities.10
This study was conducted in Liangshan, of which the morbidity of HIV was 697/100,000 by the end of 2016.21 The Liangshan area is quite unique in China for its complicated geographic position and different national culture, which lead to the birth of one of the highest prevalence areas of HIV in China. The Liangshan area is located in the southwest of China, and has been an important channel of drug transit from the Golden Triangle into Sichuan Province, China. On this basis, injection drug use is one primary infection route of HIV/AIDS in this specific area.22 Poverty also contributes to the epidemic of AIDS. Furthermore, the Liangshan area is a region with the largest number of an ethnic minority – the Yi people in China. Their different language and unique culture, like sexual culture and marriage practices, may post a higher risk for them to be infected with HIV/AIDS.23 Their casual sex includes concurrent sexual partnerships, premarital sex, and extramarital sex.24 The marriage practices, such as endogamy, means a preference for early marriage and bilateral-cross-cousin marriage.25 It is reported that the Yi people account for more than 85% of new HIV infections in the Liangshan area.26
At present, it is reported that the treatment outcome of ART for PLWH in the Liangshan area is not very satisfactory.27,28 Although antiretroviral drugs are all free for PLWH in the Liangshan area, the rate of complete virological suppression is about 55%,27,28 lower than in other provinces in China.29–31 Unsatisfactory treatment outcome is one important cause of poor quality-of-life and poor health conditions of PLWH.32,33 Adherence to ART is a major determinant of treatment outcome.34 Besides health behaviors, knowledge level about AIDS and health delivery system are also associated with treatment outcome.28 Thus, self-management and related self-management programs can work on some of these factors and improve treatment outcome. However, there were no special self-management programs oreven research on self-management in the Liangshan area. Thus, it was significant to investigate self-management in the Liangshan area.
There was a paucity of literature exploring how the unique and complex social, cultural, and healthcare environment in other parts of China impacted PLWH’s self-management skills and, in turn, their health outcomes. Furthermore, previous research on PLWH’s self-management used the Exercise of Self-Care Agency Scale (ESCA) or some other self-made scales to measure self-management in China.35 The ESCA was designed to measure human capabilities or dispositions about selfcare abilities,36 being short of HIV-specific items, and most self-made scales lacked the test of reliability and validity. The unvalidated scales might reduce the validity of their findings. In the study, the HIV Self-Management Scale was chosen as the measurement of self-management because it was proved to have good reliability and validity. Besides, the Medical Outcomes Study Social Support Survey (MOS-SSS) was used to measure social support, since social and family environment was important for the establishment and development of self-management.37
Given the above-mentioned considerations, the aim of the present cross-sectional study was to measure the self-management and to explore its related-factors of PLWH in the Liangshan area, China.
Materials and methods
Ethical statement
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional research committee and the guidelines of the Declaration of Helsinki. All participants provided written informed consent before investigation. The study was approved by the West China Hospital Medical Ethics Committee (Num: 20170430).
Study design and participants
The study was a cross-sectional study. We divided 17 counties (cities) of the Liangshan area into high HIV prevalence area and low HIV prevalence area according to the AIDS prevalence level first. Then Zhaojue county and Xichang city were selected as the representative research sites of high-prevalence and low-prevalence areas by random sampling, respectively. Participants were recruited from the AIDS Clinics and the Centers for Disease Control (CDC) in the two cities by convenience sampling when they received antiretroviral drugs or got health counseling between August and December 2017. The inclusion criteria were: 1) HIV diagnosis; 2) 18 years or older; and 3) able to respond to the questionnaire. Patients with mental illness or cognitive impairment were excluded from the study. A total of 334 questionnaires were collected, 12 questionnaires were discarded due to missing data on the major variables. Finally, 322 participants were included in the study (the available rate was 96.41%).
Data collection
All data were collected through questionnaire survey. First, the investigators were trained, the training content included the research purpose and procedures, the questionnaire content, filling methods, and some notes. These trained investigators explained the study purpose, procedure, potential risks and benefits, and guaranteed confidentiality and voluntary participation to participants before investigation. Each participant signed an informed consent document and completed a self-report survey containing demographic and disease-related information, the HIV Self-Management Scale, and the Medical Outcomes Study Social Support Survey (MOS-SSS). It took about 20–30 minutes to complete the survey. Each participant was compensated with ¥50 as compensation for transportation expenses.
Measures
Demographics and disease-related variables
The following variables were documented for each participant: age, gender, education level, marital status, nation, religion, resident place, occupation, household income monthly per capita (HIMPC), infection route, disease duration, having symptom or not, and research site.
Self-management
The HIV Self-Management Scale is a self-report questionnair developed by Webel et al.13 The scale consists of 20 items relating to three domains: daily self-management health practices, social support of HIV self-management, and the chronic nature of HIV self-management. Each item is scored on a 0–3 scale: 0=not applicable, 1=none of the time, 2=some of the time, and 3=all of the time. Total score of the scale is calculated by adding all items’ scores, with a higher score indicating a higher level of self-management, and possible scores range from 0–60. Each domain is scored separately by summing applicable item responses and dividing by the number of items in that domain. The internal consistency and temporal reliability for this scale were 0.72–0.86 and 0.61–0.85, respectively. We have obtained Webel’s permission to use the scale by email.
Social support
The original Medical Outcomes Study Social Support Survey (MOS-SSS) was developed by Sherbourne and Stewart in 1991.38 The Chinese version of MOS-SSS (MOS-SSS-C)39 was used in this study to assess social support. The scale consists of 19 items divided into four subscales: tangible support, informational and emotional support, positive social interaction, and affectionate support. Each item is scored on a 5-point Likert scale to indicate how often each kind of support was available to the participants if they need it. The score for scales is computed by averaging across items and then transformed so that the score ranges from 0–100, so that a higher score indicates more availability of different supports. An additional item is used to measure the number of close relatives/friends of participants. The test–re-test reliability of the Chinese version was 0.77 and the Cronbach’s alpha reliability coefficient was 0.889 .
Statistical methods
Data were inputed by two researchers through EpiData 3.1, and all statistics analyses were performed by using SPSS 22.0. P<0.05 was considered statistically significant. Descriptive statistics analysis was performed by mean±standard deviation (SD), frequency, and constituent ratio, as appropriate. independent Student’s t-test, and one-way ANOVA were used to examine the self-management of PLWH with different demographic characteristics and disease characteristics. The relationship between metrological variables and self-management was analyzed by Spearman rank correlation analysis. A multiple linear regression analysis was conducted to explore the associated factors of self-management in PLWH. The criterion of variable entering equation was P<0.05, and the criterion of draining out of equation was P>0.1.
Results
Sociodemographic
Demographic characteristics of participants and the self-management in different groups were presented in Table 1. The mean age of the participants was 39.22±9.59 years, most of them were Yi nationality (n=246, 76.4%), and 52.2% (n=168) were illiterate. The majority of patients were married (n=215, 66.8%). Most of the PLWH lived in rural areas (n=270, 83.9%), were living on farm land(n=243, 75.5%), and most of them had a low household income monthly per capita (HIMPC) of about 0–499 yuan (n=250, 77.6%). The social support score was 54.21±18.68.
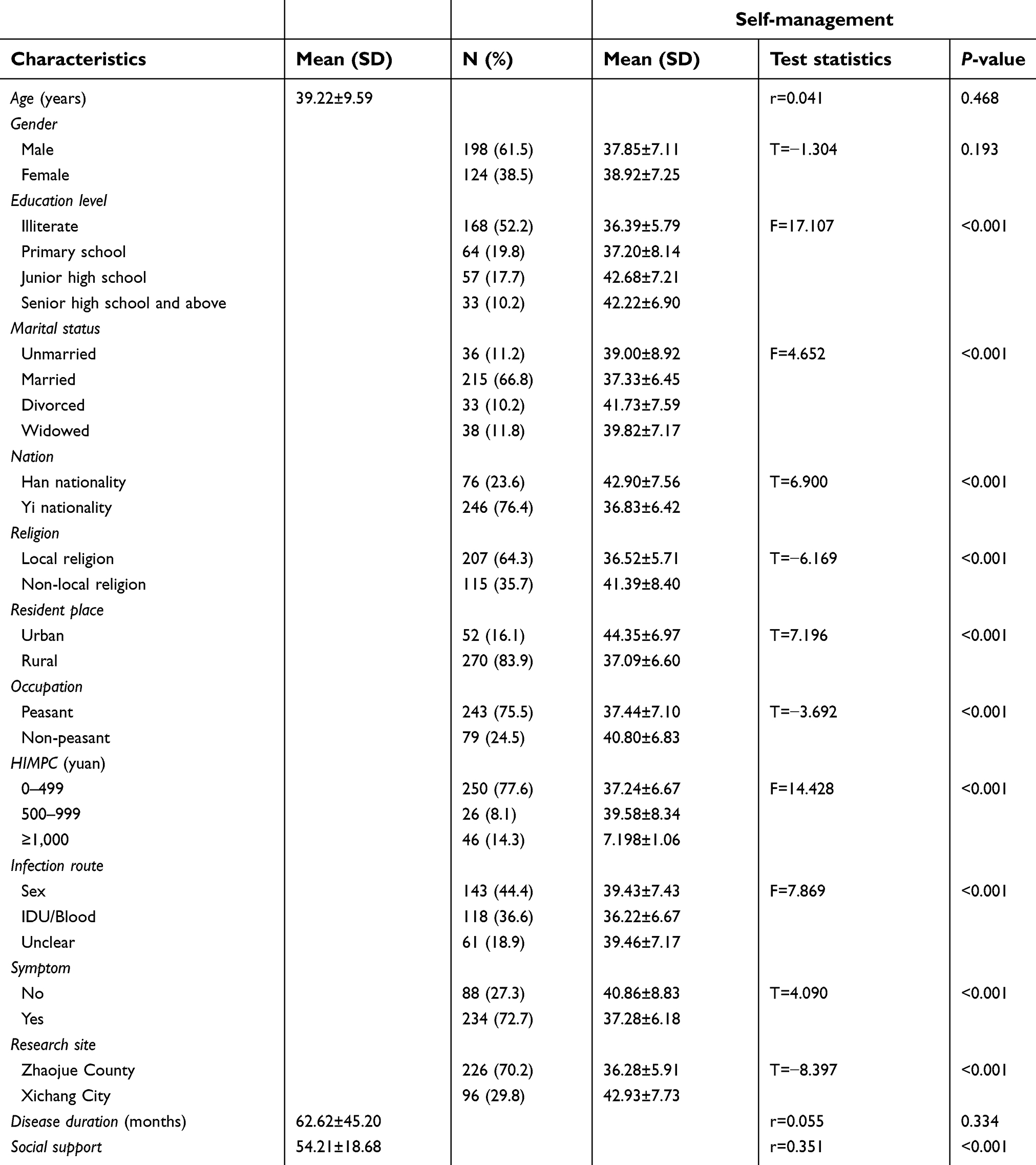 | Table 1 Demographic characteristics of people living with HIV and univariate analysis of self-management (N=322) |
Self-management
The total self-management score was 38.26±7.17, and the mean level of self-management was 1.91±0.36. Self-management scores varied by domains: the mean daily self-management health practices score was 1.80±0.42; the mean social support domain of the HIV self-management scale was 1.47±0.63, and the mean chronic nature of HIV score was 2.46±0.43.
Relationships between study variables and self-management
The relationships between self-management and variables are presented in Table 1. The results of inter-group comparison and Spearman correlation analysis showed that nation (T=6.900, P<0.001), religion (T=−6.169, P<0.001), education level (F=17.107, P<0.001), marital status (F=4.652, P<0.001), HIMPC (F=14.428, P<0.001), resident place (T=7.196, P<0.001), occupation (T=−3.692, P<0.001), infection route (F=7.869, P<0.001), symptom (T=4.090, P<0.001), research site (T=−8.397, P<0.001), and social support (r=0.351, P<0.001) were significantly associated with self-management among PLWH.
Regression analyses of self-management
Table 2 outlinesthe results of a multiple linear regression model examining the relationships between demographics, social support, and HIV self-management. Being a female PLWH (B=1.456, P=0.044, 95% CI=0.038–2.873), better social support (B=0.127, P<0.001, 95% CI=0.091–0.164), and being divorced (B=4.021, P=0.006, 95% CI=1.153–6.889) or widowed (B=3.262, P=0.029, 95% CI=0.341–6.184) had statistically significant positive associations with self-management. We also observed that the Yi (B=−2.757, P=0.006, 95% CI=−4.735–0.779) and rural residents (B=−3.538, P=0.004, 95% CI=−5.915–1.162) got a lower self-management score.
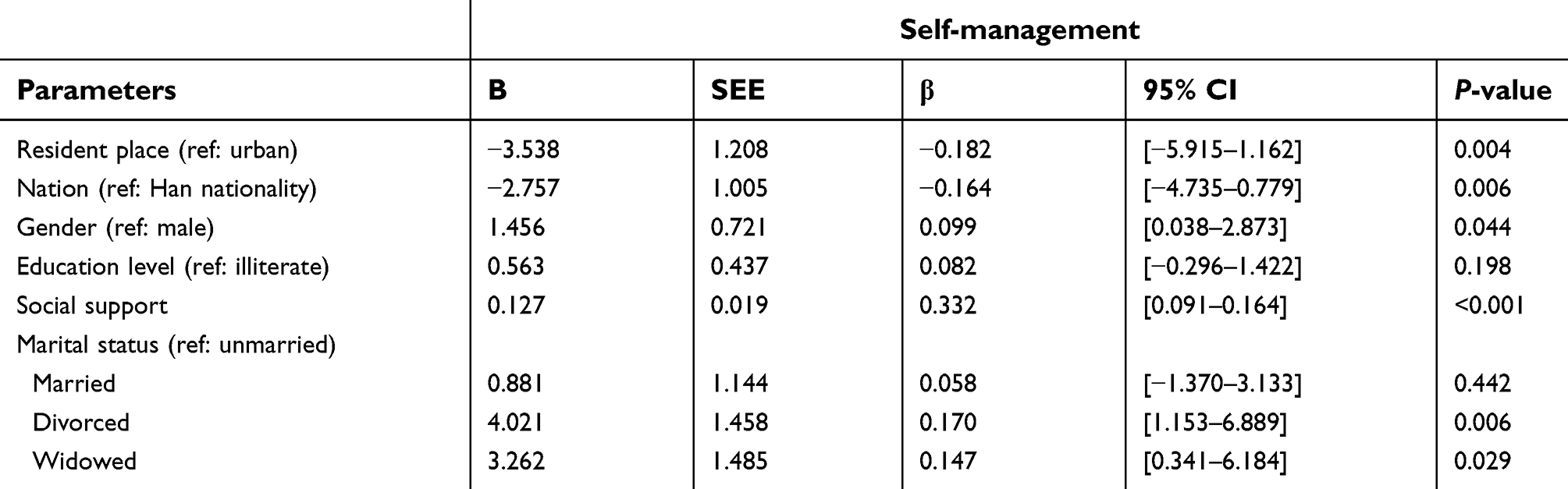 | Table 2 Multiple linear regression on self-management of people living with HIV |
Discussion
In our study, the mean level of total HIV self-management in PLWH was 1.91±0.36. Webel et al20 reported a higher score of self-management (2.64±0.43) of women in the US. Kim et al40 found the score of self-management of outpatients at general hospitals was 2.00±0.49 in Korea, which was also higher than that in our study. Chronic disease self-management programs have been developed for decades in developed countries such as the US and South Korea and has been applied to AIDS patients.41,42 The implementation of these intervention projects could effectively improve the self-management ability of PLWH. However, the research on self-management of AIDS patients has been carried out late in China, and there is still a lack of self-management intervention program for PLWH in the Liangshan area. The difference reminds our government that we should speed up the implementation of the HIV self-management program in Liangshan, in order to improve the self-management ability of PLWH.
Of the three domains, the social support domain of the HIV self-management scale had the lowest score of 1.47±0.63. The low score indicated that PLWH in the Liangshan area received less support from others and organizations since this domain includes concepts of social influence, social support, and collaboration with healthcare professionals.13 Thisresult could also be proved by the low score of social support in PLWH (54.21±18.68). This score was significantly lower than that of a report from Hong Kong in which authors reported a social support score of 60.82±25.74 among the study participants.43
We detected that better social support was benificial for improving self-management. Better social support was proved to be correlated with better psychosocial adjustment, and could enhance self-management.44 The stress-buffering hypothesis offered a good theoretical explanation for such positive effects.45 This hypothesis assumed that social support could exert a buffering effect that alleviates an individual’s reaction to the adverse impacts of chronic illness. Above all, it is essential to establish a more complete family and social support system of PLWH considering the lack of social support.
We found that self-management of the Yi was worse than the Han. This result could be partly explained by the language barrier of the Yi, which restricted them access to medical support and information support.46 At present, the overall cultural level of the Yi nationality is lower than that of the Han nationality.46 Since we have known that people with a higher education level can better acquire self-management knowledge,47 the education level may be one explanation for thisdifference. In addition, the propaganda material of AIDS in the Liangshan area was commonly in Chinese. Yi people might have some difficulties in understanding Chinese, which would affect their acquisition of AIDS-related knowledge, thus affecting their self-management ability.
We observed that PLWH living in rural areas had worse self-management than those living in urban. A previous study48 showed that financial problems was one of the frequently noted barriers to impede self-management. The economic level in Liangshan is relatively backward, especially in rural areas,46 which may be one of the reasons for the result. In addition, the poor development of medical and healthcare systems in rural areas led to the lack of disease-related health education.46 In Liangshan, the government has set up an AIDS management center for each county or district to manage and provide services for PLWH. However, the inconvenient transportation makes it difficult for rural residents to access resources provided by the government and medical institution.49 Therefore, how to enable PLWH in rural areas to enjoy better medical services and support is an important issue to be addressed by the government.
Our study showed that divorced or widowed PLWH had better self-management than the unmarried. A possible explanation for the result was that most of the PLWH in our study were Yi people, and the special sexual culture of Yi. It is not a rare phenomenon that Yi people have more than one sexual partner. Therefore, the Yi unmarried have few fixed partners and they can get little support from their partners, leading to worse self-management. Besides, people unmarried are less restrained by their family, so they are more likely to be addicted to drug use and other bad behaviors. However, we didn’t find that married PLWH had better self-management than the unmarried. This was in disagreement with Mak et al,50 who reported marriage was good for self-management, because marriage was the main form of family support, and a stable marriage could provide material and spiritual support for each other. One possible reason for our result was that married PLWH were affected by their various duties, including daily house chores, raising children, providing care, and financial support. These traditional family roles could make them stressful and give them less time to do daily self-management tasks.51
We also observed that females had better self-management than males. Previous studies have reported that women’s poor self-management was mainly due to the demanding social roles (wife, mother, employee), poverty, homelessness, and inadequate access to healthcare, powerlessness, racism, sexism, and classism.51–53 One possible reason for thisinconsistent result was that the rate of illicit drug use in men was higher than women in the Liangshan area.54 Substance abuse behaviors in HIV disease are known to reduce patients’ self-control, complicate HIV/AIDS care, and negatively impact disease outcomes.55
At present, the Chinese government has launched various policies to provide medical, economic, and educational support for PLWH and their family members. For example, the Comprehensive AIDS Response Program (China CARES) has effectively improved social support of PLWH by relieving their mental pressure and rising their awareness of HIV/AIDS.56 In addition, the Precise Poverty Alleviation Policy, a new idea of poverty alleviation, could improve the economic conditions.
We should still make further efforts to improve self-management of PLWH. First, strengthen the publicity of AIDS, adding self-management-related content, to train PLWH in the skills that they need to care for themselves. Second, providing more service and support for special groups of PLWH, such as the Yi and drug abusers.
There were limitations in our study that should be acknowledged. First, most of the Yi peoples enrolled in our study native language was Yi language. Although the investigators, who were proficient in Chinese and Yi language, could assist the participants in understanding and completing the questionnaires, a misunderstanding about the questionnaire was still possible. Thus, there were possibilities of measurement bias to consider when interpreting the data. Second, we could not determine the exact causality between self-management and related influential factors due to the cross-sectional design. Therefore, there is a need for continuing longitudinal research and muticenter studies to confirm our findings and explore its causality.
Conclusion
In conclusion, the self-management of PLWH in the Yi autonomous area was relatively poor, which deservesmore attention. The resident place, gender, marital status, nation, and social support are significantly associated with self-management. So it is vitally important to implement policy inclination to the Liangshan prefecture, and provide more support and services for PLWH considering the unique local culture and self-management related factors.
Acknowledgments
The authors gratefully appreciate the support of the investigators and all the participants.
Disclosure
All authors declare that they have no conflicts of interest to report in this work. The abstract of this paper was presented at the 8th world Conference on Asia Pacific STD and Infectious Disease Congress; “Status and associated factors of self-management in people living with HIV/AIDS in Yi Autonomous Prefecture of Liangshan, China” as a conference talk with interim findings.
References
1.
2.
3. Thompson MA, Aberg JA, Cahn P, et al. Antiretroviral treatment of adult HIV infection: 2010 recommendations of the International AIDS Society-USA panel. JAMA. 2010;304(3):399–405.
4. Ford N, Calmy A, Mills EJ. The first decade of antiretroviral therapy in Africa. Global Health. 2011;7(1):33–33. doi:10.1186/1744-8603-7-33
5. Mitchell CG, Linsk NL. A multidimensional conceptual framework for understanding HIV/AIDS as a chronic long-term illness. Soc Work. 2004;49(3):469–477. doi:10.1093/sw/49.3.469
6. Beaudin CL, Chambre SM. HIV/AIDS as a chronic disease: emergence from the plague model. Am Behav Sci. 1996;39(6):684–706. doi:10.1177/0002764296039006006
7. Nozaki I, Dube C, Kakimoto K, Yamada N, Simpungwe JB. Social factors affecting art adherence in rural settings in zambia. AIDS Care. 2011;23(7):831–838. doi:10.1080/09540121.2010.542121
8. Amico KR, Harman JJ, Johnson BT. Efficacy of antiretroviral therapy adherence interventions: a research synthesis of trials, 1996 to 2004. J Acquir Immune Defic Syndr. 2006;41(3):285–297. doi:10.1097/01.qai.0000197870.99196.ea
9. Bangsberg DR, Perry S, Charlebois ED, Clark RA, Moss A. Nonadherence to highly active antiretroviral therapy predicts progression to aids. AIDS. 2001;15(9):1181–1183.
10. Smith CJ, Ryom L, Weber R, et al. Trends in underlying causes of death in people with HIV from 1999 to 2011 (D:A:D): a multicohort collaboration. Lancet. 2014;384(9939):241–248. doi:10.1016/S0140-6736(14)60604-8
11. Triant VA, Lee H, Hadigan C, Grinspoon SK. Increased acute myocardial infarction rates and cardiovascular risk factors among patients with human immunodeficiency virus disease. J Clin Endocrinol Metab. 2007;92(7):2506–2512. doi:10.1210/jc.2006-2190
12. Phillips A, Neaton J, Lundgren J. The role of hiv in serious diseases other than aids. AIDS. 2008;22(18):2409–2418. doi:10.1097/QAD.0b013e3283174636
13. Webel AR, Asher A, Cuca Y, et al. Measuring HIV self-management in women living with HIV/AIDS: a psychometric evaluation study of the HIV Self-management Scale. J Acquir Immune Defic Syndr. 2012;60(3):e72–e81. doi:10.1097/QAI.0b013e318250f011
14. Bodenheimer T, Lorig K, Holman H, et al. Patient self-management of chronic disease in primary care. JAMA. 2002;288(19):2469–2475. doi:10.1001/jama.288.19.2469
15. Richard AA, Shea K. Delineation of self-care and associated concepts. J Nurs Scholarsh. 2011;43(3):255–264.
16. Lorig KR, Holman HR. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1–7. doi:10.1207/S15324796ABM2601_01
17. Swendeman D, Ingram BL, Rotheramborus MJ. Common elements in self-management of HIV and other chronic illnesses: an integrative framework. AIDS Care. 2009;21(10):1321–1334. doi:10.1080/09540120802385579
18. Bourbeau J, Nault D, Dangtan T. Self-management and behaviour modification in COPD. Patient Educ Couns. 2004;52(3):271–277. doi:10.1016/S0738-3991(03)00102-2
19. Fishwick D, D’Souza W, Beasley R. The asthma self-management plan system of care: what does it mean, how is it done, does it work, what models are available, what do patients want and who needs it? Patient Educ Couns. 1997;32(12 Suppl):S21–S33. doi:10.1016/S0738-3991(97)00093-1
20. Webel AR, Cuca Y, Okonsky JG, et al. The impact of social context on self-management in women living with HIV. Soc Sci Med. 2013;87:147–154. doi:10.1016/j.socscimed.2013.03.037
21.
22. Mo-Se DE, Wang Z, Deng F, Zhang JH, Gong YH, Yan ZM. Analysis of epidemiological characteristics and countermeasure of AIDS in Liangshan state. Modern Prev Med. 2008;35(4):630–631.
23. Yang SJ, Luo M, Zhang SH, Yao YN, Wang QX, Liao Q. Overview on culture and customs related to AIDS epidemic and prevention among Yi people in Liangshan. Chin J AIDS STD. 2017;23(3):101–104.
24. Yang Y, Luan RS, Liu P, Wu CL, Zhou Y, Chen W. Casual sex and concurrent sexual partnerships among young people from an yi community with a high prevalence of hiv in China. Asian J Androl. 2012;14(5):758–765. doi:10.1038/aja.2012.25
25. Guo ZT. When politics meet marriage: changes in marriage practices among migrated yi cadres in Liangshan, China. In: Decimo F, Gribaldo A, editors. Boundaries Within: Nation, Kinship and Identity among Migrants and Minorities. Cham: Springer; 2017:181–198. Online.
26. Yang SJ, Wang QX, Yang C, et al. HIV-related high-risk behaviours and factors maternal AIDS sentinel surveillance in Liangshan prefecture, 2011–2015. Modern Prev Med. 2017;44(13):
27. Bian SC, Chen XR, Chen MG, Xiao L. Accepted HAART patients viral result of Liangshan Yi autonomous prefecture from 2011 to 2015. J Prev Med Inf. 2018;34(7):944–947.
28. Xu JL. Effects and Associated Factors of HIV/AIDS Antiretroviral Therapy in the Key Area of Liangshan Prefecture. Beijing: Chinese Center for Disease Control and Prevention; 2018.
29. Yang WJ, Fan PY, Liang Y, et al. Analysis on HIV suppression effect after initiating antiretroviral treatment and related factors among AIDS patients in Henan province during 2008 and 2013. Chin J Prew Med. 2015;49(1):13–20.
30. Dou ZH, Zhang FJ, Zhao Y, et al. Progress on China’s national free antiretroviral therapy strategy in 2002–2014. Chin J Epidemiol. 2015;36(12):1345–1350.
31. Zheng W, Tang H, Da Q, Peng GP. Effect of antiviral treatment of AIDS in Hubei Province (2011–2015). J Pub Health Prev Med. 2017;28(5):37–41.
32. He D, Pu J, Xu YZ, et al. Investigation on social support and quality of life among pregnant women with HIV infection in different areas of Liangshan Yi Autonomous Prefecture. Matern Child Health Care China. 2017;32(20):5079–5081.
33. Meng YJ, Li NX, Chen JH, Song YC, Qian ZS. Using the SF-36 to assess the quality of life of people living with HIV in Sichuan. J Sichaun Univ (Med Sci Edi). 2007;38(3):471–474.
34. Knobel H, Guelar A, Carmona A, et al. Virologic outcome and predictors of virologic failure of highly active antiretroviral therapy containing protease inhibitors. AIDS Patient Care STDS. 2001;15(4):193–199. doi:10.1089/10872910151133729
35. Chen X, Chen XY. Self-care agency of AIDS patients undergoing anti-virus treatment and its influencing factors. J Nurs (China). 2014;21(2):1–4.
36. Wang XH, Laffrey SC. Preliminary development and testing of instruments to measure self-care agency and social support of women in taiwan. Kaohsiung J Med Sci. 2000;16(9):459–467.
37. Luo Y, Sun RJ, Fan D. Prospect of self-management in HIV infected-person and AIDS patients. Nurs J Chin PLA. 2009;26(8B):
38. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32(6):705–714. doi:10.1016/0277-9536(91)90150-B
39. Li H. Psychometric Measurement of the Simplified Chinese Medical Outcomes Study Social Support Survey (MOS-SSS-C) and Its Application in HIV/AIDS Patients. Changsha: Central South University; 2012.
40. Kim GS, Chu SH, Park Y, et al. Psychometric properties of the Korean version of the HIV self-management scale in patients with HIV. J Korean Acad Nurs. 2015;45(3):439–448. doi:10.4040/jkan.2015.45.3.439
41. Gifford AL, Laurent DD, Gonzales VM, et al. Pilot randomized trial of education to improve self-management skills of men with symptomatic HIV/AIDS. J Acquir Immune Defic Syndr Hum Retrovirol. 1998;18(2):136–144.
42. Su HK, Chang HY. Efficacy of chronic disease self-management program in older Korean adults with low and high health literacy. Asian Nurs Res (Korean Soc Nurs Sci). 2015;9(1):42–46.
43. Yu DS, Lee DT, Woo J. Psychometric testing of the Chinese version of the medical outcomes study social support survey (MOS-SSS-C). Res Nurs Health. 2010;27:135–143. doi:10.1002/nur.20008
44. Cuijpers P. Mortality and depressive symptoms in inhabitants of residential homes. Int J Geriatr Psychiatry. 2001;16(2):131–138. doi:10.1002/1099-1166(200102)16:2<131::AID-GPS 283>3.0.CO;2-W
45. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
46. Zhu CH, Zhou YB, Song XX, Jiang QW. ReView on the influence factors of AIDS epidemic and control in Liangshan Prefecture Sichuan Province of China. Fudan Univ J Med Sci. 2015;42(5):675–679.
47. Millard T, Elliott J, Girdler S. Self-management education programs for people living with HIV/AIDS: a systematic review. AIDS Patient Care STDS. 2013;27(2):103–113. doi:10.1089/apc.2012.0294
48. Jerant AF, Mmv F-F, Moore M. Patients’ perceived barriers to active self-management of chronic conditions. Patient Educ Couns. 2005;57(3):300–307. doi:10.1016/j.pec.2004.08.004
49. Fraser HS, Jazayeri D, Nevil P, et al. An information system and medical record to support HIV treatment in rural Haiti. BMJ. 2004;329(7475):1142–1146. doi:10.1136/bmj.329.7475.1142
50. Mak WW, Cheung RY, Law RW, et al. Examining attribution model of self-stigma on social support and psychological well-being among people with HIV+/AIDS. Soc Sci Med. 2007;64(8):1549–1559. doi:10.1016/j.socscimed.2006.09.027
51. Webel AR, Higgins PA. The relationship between social roles and self-management behavior in women living with HIV/AIDS. Womens Health Issues. 2012;22(1):e27–e33. doi:10.1016/j.whi.2011.05.010
52. Zaidi SA. Gender perspectives and quality of care in underdeveloped countries: disease, gender and contextuality. Soc Sci Med. 1996;43(5):721–730.
53. Arrivillaga M, Ross M, Useche B, et al. Social position, gender role, and treatment adherence among Colombian women living with HIV/AIDS: social determinants of health approach. Rev Panam Salud Publica. 2009;26(6):502–510.
54. Gong YH, Wang QX, Nan L, et al. Analysis of HIV infection among rural population aged 15 to 60 in Liangshan Prefecture, Sichuan Province. Chin J Dis Control Prev. 2014;18(12):1132–1135.
55. Brion JM, Rose CD, Nicholas PK, et al. Unhealthy substance-use behaviors as symptom-related self-care in persons with HIV/AIDS. Nurs Health Sci. 2011;13(1):16–26. doi:10.1111/j.1442-2018.2011.00645.x
56. Han M, Chen Q, Hao Y, et al. Design and implementation of a China comprehensive AIDS response programme (China CARES). 2003–08. Int J Epidemiol. 2010;39(Suppl 2):S47–S55. doi:10.1093/ije/dyq212
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.