")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Statins in High-Risk Chronic Obstructive Pulmonary Disease Outpatients: No Impact on Time to First Exacerbation and All-Cause Mortality – The STATUETTE Cohort Study
Authors Damkjær M, Håkansson K, Kallemose T , Ulrik CS , Godtfredsen N
Received 9 December 2020
Accepted for publication 7 February 2021
Published 5 March 2021 Volume 2021:16 Pages 579—589
DOI https://doi.org/10.2147/COPD.S296472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Mathias Damkjær, 1 Kjell Håkansson, 1 Thomas Kallemose, 2 Charlotte Suppli Ulrik, 1, 3 Nina Godtfredsen 1, 3
1Department of Respiratory Medicine, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark; 2Clinical Research Centre, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark; 3Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark
Correspondence: Nina Godtfredsen
Department of Respiratory Medicine, Hvidovre Hospital, Kettegård Allé 30, Hvidovre, 2650, Denmark
Email [email protected]
Background: Statins have, due to their anti-inflammatory properties, been suggested to potentially improve chronic obstructive pulmonary disease (COPD) outcomes. We aimed to investigate the effect of statins on time to first exacerbation and all-cause mortality in high-risk COPD outpatients.
Methods: All outpatients with COPD seen at the Department of Respiratory Medicine, Copenhagen University Hospital Amager and Hvidovre, Denmark in 2016 were identified and followed for 3.5 years in this retrospective, registry-based cohort study of time to first acute exacerbation of COPD (AECOPD) or death. AECOPD was defined as a rescue course of oral corticosteroid and/or hospital admission. The association was estimated using time-varying crude and multivariable Cox proportional hazard regression.
Results: The cohort comprised 950 COPD outpatients, mean (SD) age 71 (11) years, and FEV1 44% predicted (IQR 33%; 57%). The annual exacerbation rate was 0.88 (1.68) and 211 patients (22%) had a history of hospital admission for AECOPD in the 12 months prior to index date. Three hundred and ninety-three patients (41.4%) were defined as statin users, with 131 (33.3%) having filled the first prescription for statin after index date. Statin use was not associated with reduced risk of AECOPD. When stratifying for moderate and severe exacerbations in a sub-analysis in the same model, statin use did not have an increased HR for exacerbation of either severity (HR = 1.02 (95% CI 0.85to 1.24; p = 0.811) and HR = 1.07 (95% CI 0.89 to 1.29; p = 0.492) respectively). Statin use was not associated with all-cause mortality (HR 1.05 (95% CI, 0.75 to 1.47, p = 0.777)).
Conclusion: We did not find any association between statin use and risk of AECOPD or all-cause mortality. The result adds to the evidence that an aggressive approach with statin treatment upfront is not beneficial in COPD, unless prescribed according to current guidelines for cardiovascular diseases.
Keywords: chronic obstructive pulmonary disease, cardiovascular disease, exacerbations, statins, mortality
Corrigendum for this paper has been published
Plain Language Summary
What is Already Known on This Topic
- An association between statin use and reduced risk of exacerbations and mortality has been reported in observational studies. A single RCT has reported no effect of 40 mg simvastatin daily on exacerbation rate in COPD patients without CVD.
- Results from observational studies on statin therapy and COPD-related outcomes in COPD patients with concomitant CVD diverge, leaving the role of statin therapy in COPD yet to be elucidated.
What This Study Adds
- This 3.5-year retrospective cohort study including 950 patients did not find any association between statin use and reduced time to first AECOPD or risk for all-cause mortality.
- In an unselected COPD patient population, an aggressive, upfront statin therapy is not warranted in patients without CVD – however, our data suggest a continued high burden and undertreatment of CVD in COPD patients.
Background
Chronic obstructive pulmonary disease (COPD) and cardiovascular disease (CVD) are two of the world’s leading causes of morbidity and mortality,1 with a large unmet need for more efficient treatments for COPD beyond smoking cessation, rehabilitation and controller therapy with primarily long-acting bronchodilators and inhaled corticosteroids to alter disease prognosis.2–4
In terms of pathophysiology, there is a well-established association between COPD and CVD, where inflammation-driven pulmonary and vascular damage caused by chronic exposure to tobacco smoke accounts for a major part of the common link between the two diseases. It has also been suggested though that COPD may be an individual risk factor for CVD, but this assumption remains disputed.5–7 Regardless, COPD patients have more than two-fold increase in the odds of having CVD, relative to COPD-free patients.8 Due to their close association and common risk factors, it has been hypothesized that some conventional therapies used to treat CVD could have a potential role in the treatment of COPD, especially in those with concomitant CVD. Furthermore, CVD in COPD is assumed to be systematically underdiagnosed due to the overlapping symptoms between the two diseases.6 However, presently, no compelling evidence has emerged that could warrant an aggressive and upfront approach to preventive statin treatment in COPD patients for COPD-related outcomes.6
While statins are mainly known for their plasma cholesterol-lowering effects through 3-hydroxy-3-methyl-glutaryl-coenzyme A-reductase inhibition, studies have shown pleiotropic effects, including anti-inflammatory actions capable of significantly lowering C-reactive protein (CRP) and interleukin-6 (IL-6) in COPD patients.9 A subset of COPD patients have elevated levels of systemic inflammation, and it has been suggested that this population might have the most benefit of statin treatment for COPD-related outcomes, due to the inflammatory components of both COPD and CVD.10,11
A recent meta-analysis investigating the role of statins in the treatment of COPD show a discordance between observational and randomized clinical trials (RCT).12 While observational studies have shown promising results with reduced exacerbations and mortality in COPD patients, RCTs fail to show an effect.9 However, many studies focus on COPD patients without concurrent CVD and often using short (<365 days) follow-up time.9 Considering the high CVD burden in COPD, it can be argued that the populations in these studies are not representative of real-world COPD populations where CVD comorbidity is exceedingly common. As such, both observational and RCT studies are needed to elucidate the effect of statin treatment on COPD in real-world settings.
In the present study, we aimed to examine the associations between statin use, time to exacerbation and all-cause mortality over 3.5 years in an unselected population of high-risk COPD outpatients followed at a university hospital.
Methods
Study Design and Setting
The present study is a retrospective cohort study using data from medical journals and a nationwide medication registry. It included patients from a single center using a fixed time follow-up interval.
The study was conducted at the Respiratory Outpatient Clinic, Copenhagen University Hospital Amager and Hvidovre, Hvidovre, Denmark. Patients with an active COPD diagnosis (confirmed by spirometry and assessment by a respiratory specialist) with a scheduled visit during 2016 were included and followed from date of routine visit (index date) to August 2019 or to date of death. All Danish citizens are covered by a national public health insurance with free access to healthcare.
Ethics
Study approvals were given by the Danish Patient Safety Authority (ref. 3–3013-3198/1) and the Greater Capital Region of Copenhagen’s Data Safety Board (ref. P-2019-674).
Data Collection
Data were collected using unique, national Danish civil registration numbers13 to combine individual electronic patient records with vital status, laboratory- and dispensed prescription data.
Hospital admissions, disease severity, comorbidities and routine visit assessment data, such as pulmonary function tests, was accessed using the electronic patient journal system Sundhedsplatformen (Epic Inc., USA). Dispensed prescription data from January 2014 to August 2019 was supplied by the Danish National Health Service Prescription Registry (DNPR).14 Medication status for statin-, inhaler- and other therapies were based on ATC-codes, as described in Appendix 1.
Definitions
Exposure to statin was defined as a dispensed statin prescription according to three categories:
- Persistent user: dispensed prescription of a statin up to 4 months (121 days) before index date.
- New user: dispensed prescription of a statin after index date and before end of follow-up date.
- Nonuser: no statin prescriptions between index date and end of follow-up date.
Outcomes were defined as following:
- All-cause mortality was defined as categorial yes or no during the follow-up period.
- Acute exacerbation (AECOPD) was defined as a composite outcome of:
- Moderate exacerbation: defined by time to first dispensed prescription of an oral glucocorticoid with short term use defined as filling a maximum of 20 tablets of 25 mg in one day with or without concurrent antibiotics.
- Severe exacerbation: defined as time to first hospital admission for AECOPD (≥24 hours) based on ICD-10 DJ46 and administration of systemic corticosteroids.
The first occurring event was chosen as the date of the composite outcome. This definition has been validated15 and used in other observational studies.16
COPD disease severity as defined by the Global Initiative for Obstructive Lung Disease (GOLD) 2020 guidelines.17 CVD was defined as active or previous ICD-10 codes corresponding to acute coronary syndrome (I24.9), chronic ischemic heart disease (I25), diabetes mellitus type 1 or 2 (E10, E11) or stroke (I64). Baseline inhalation medication treatment was based on dispensed prescription data 4 months prior to index date.
Statistical Analyses
Descriptive statistics were used to present continuous variables by either median (Interquartile Range (IQR)) or mean (Standard Deviation (SD)). Categorical variables were presented as counts (%). Missing values were presented as an absolute number for each variable according to groups. No sample size calculations were done prior to the study.
Crude (statin use only) and multivariable (statin use and confounders) Cox proportional hazard regressions were used to estimate the association of statin use with time to exacerbation and time to death. Given the possible change in statin use during follow-up, statin use was included as a time varying covariate in the models. Estimates are presented as hazard ratios (HRs) with 95% confidence intervals (CI’s). In the Cox regression for exacerbations, death was considered a competing endpoint, therefore risk time was censored at the time of death. Proportional assumption was evaluated by the Schoenfeld residuals; if violated modifications to the Cox model was made by stratifying the hazard by the violating adjusted variables.
In multivariable analysis, possible confounders were age, sex, body mass index (BMI), heart failure, smoking status and GOLD-severity. Inclusion of these were determined by evaluating the change in statin use HR between models with and without the specific confounder, if sufficient change was introduced the variable was included as a confounder. Additional models with interaction between statin use and CVD and inhaled corticosteroids (ICS) were done. Furthermore, a sub-analysis with the same multivariable analysis model but with moderate and severe exacerbations as single outcome variables.
Immortal time bias was addressed by a Mantel Byar design.18 Accordingly, the analysis was adjusted for the unexposed time (“immortal time”) in the “New user” statin category avoiding a potential false increase in survival time attributed to the fact that the patients must have been alive to receive a statin medication and bias in exacerbation outcome associated with death in the fixed follow-up period (see Figure 1).
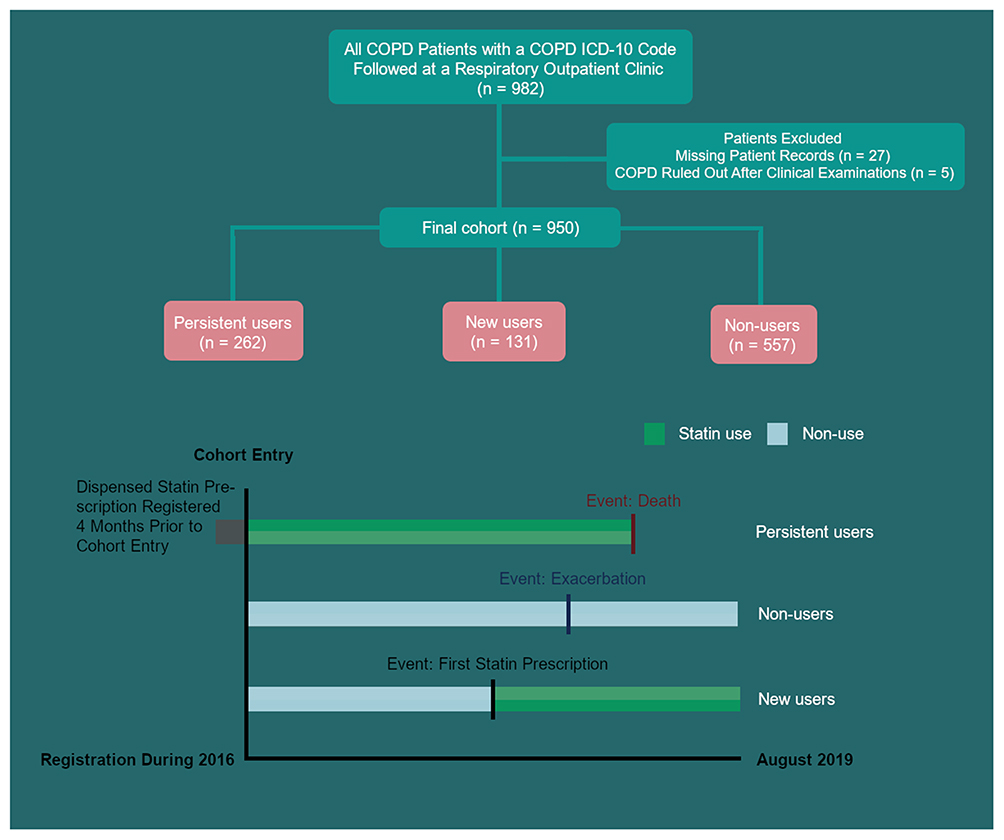 |
Figure 1 Schematic overview of study design and Mantel-Byar approach to immortal-time bias in a retrospective cohort of 950 COPD outpatients followed for 3.5 years. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Missing values were replaced with multiple imputations using multivariate imputation by chained equations on all data with 1000 imputations with a missing at random assumption. Loss to follow-up was not addressed due to a low number of missing journals. All analysis was performed using R (The R Foundation, Vienna, AU) version 4.0.2, with multivariate imputation done using the mice package19 with a significance level of  .
.
Results
A total of 982 patients were screened for eligibility, with 950 fulfilling all inclusion criteria and having patient records available (Figure 1). Of the included patients, 47% were male, and the mean age was 71 years (11). Of the patients, 26.0% were current smokers and 70.0% were ex-smokers, with overall median pack-years being 43 (IQR 30; 51). GOLD 2020 B and D were the most common disease severity classifications (34% and 36%, respectively) and the median FEV1pred was 44% (IQR 33; 57) (Table 1).
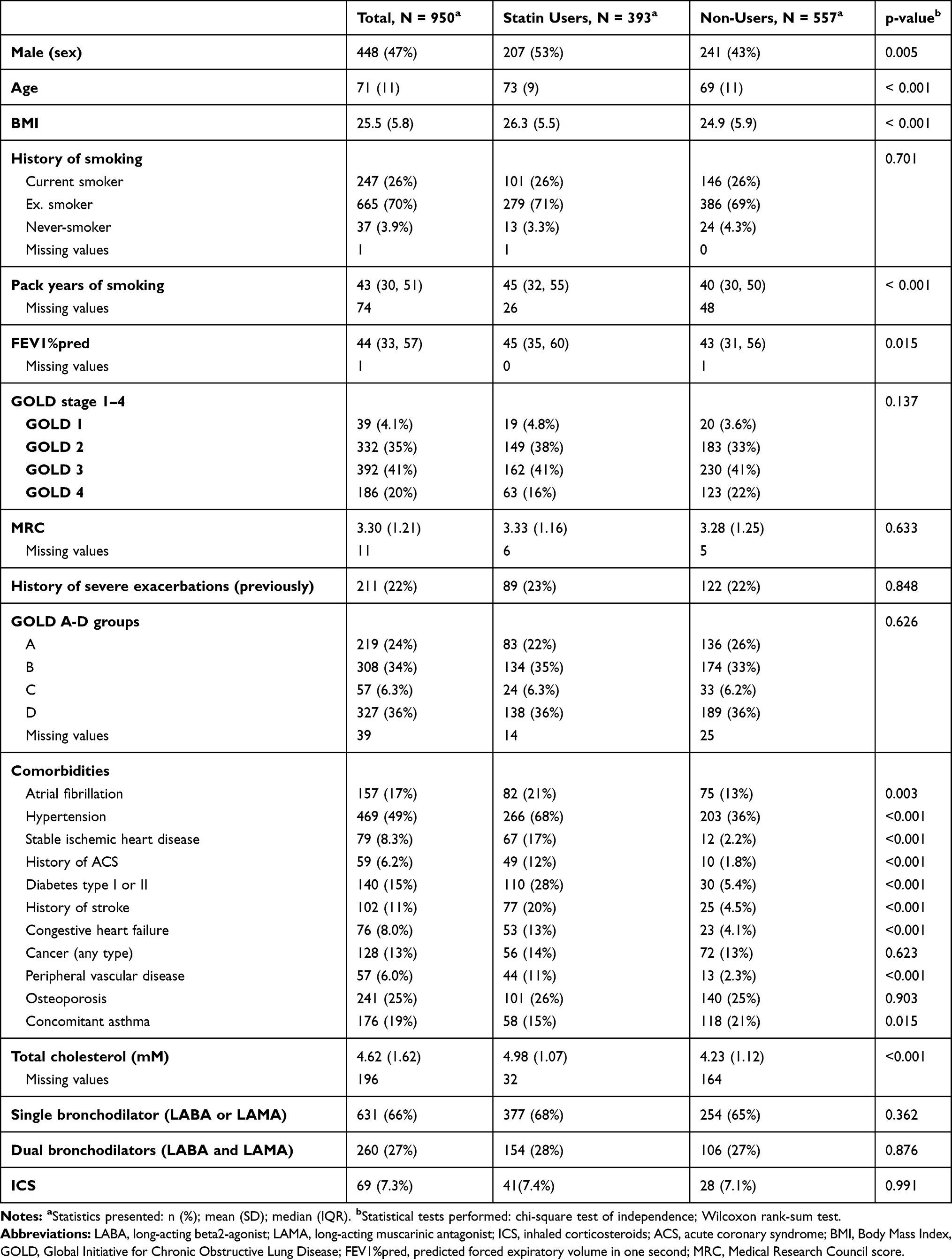 |
Table 1 Demographics of 950 COPD Patients, Divided by Statin Treatment Status, at an University Hospital Outpatient Clinic |
Between statin users and non-users, users had slightly higher median FEV1pred (45% (IQR 35; 60) vs 43 (IQR 31; 56), p = 0.015). No difference in GOLD classification, Medical Research Council (MRC)-scores, 12-month exacerbation history, smoking status nor maintenance COPD-therapy were found between statin users and non-users (Table 1). Out of 393 statin users, 131 (33.3%) were defined as “New users” and thereby received a statin medication after index date. The two most used statins were simvastatin (n = 211 (54.9%)) and atorvastatin (n = 149 (38.8%)) respectively.
In terms of comorbidity, 299 (31.5%) patients had one or more diseases classified as CVD in the present study, of whom 232 (77,6%) had dispensed a statin prescription in the study period. No differences in non-CVD comorbidities such as cancer and osteoporosis were found between the groups, while CVD diagnoses were more prevalent in patients receiving statins (Table 1). Furthermore, mean total cholesterol was significantly lower in statin users (4.23 (SD 1.12) vs 4.98 (SD 1.07), p <0.001) (Table 2) and 268 patients had a cholesterol level >5 mM, of which only 78 (29.1%) received a statin medication.
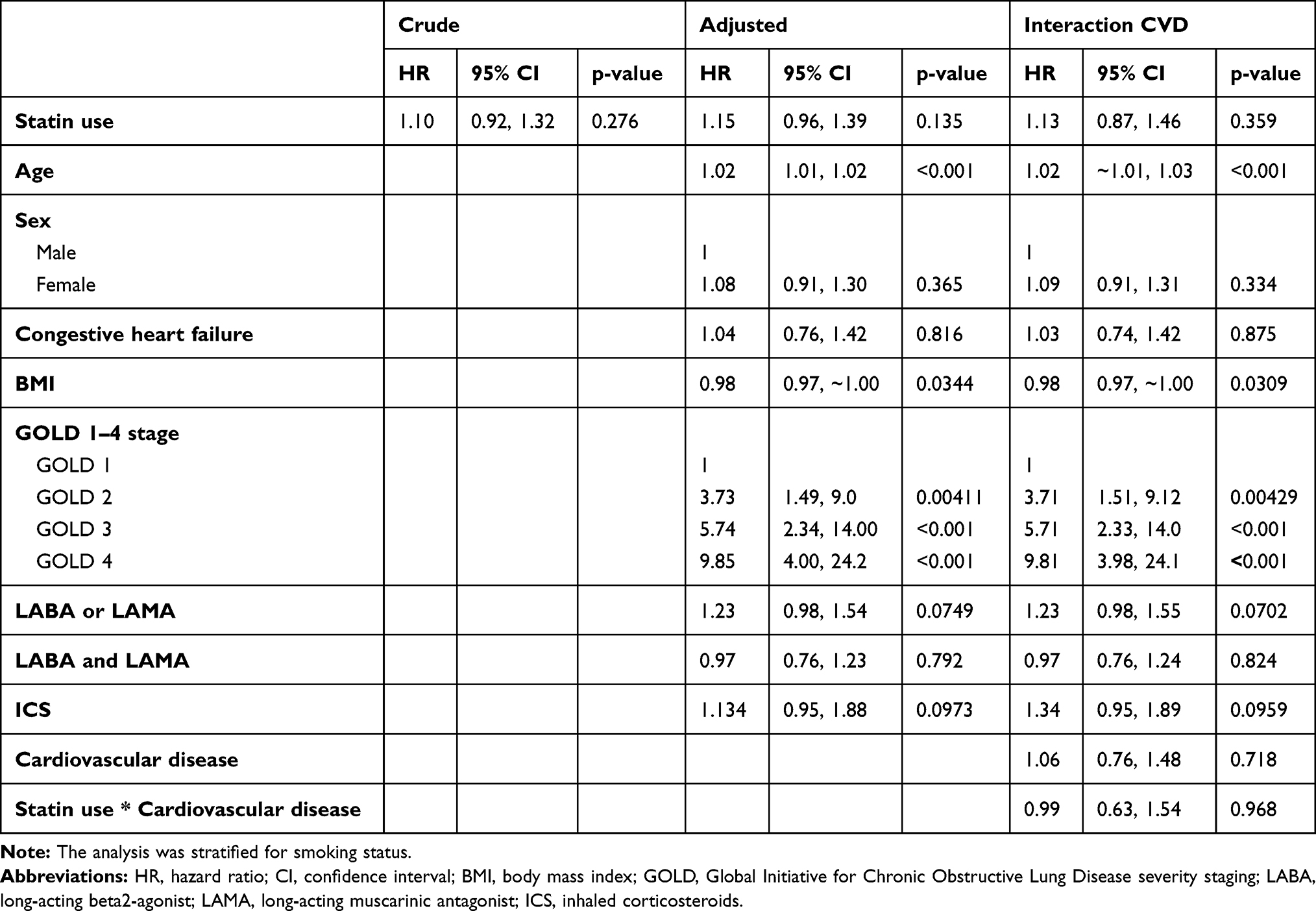 |
Table 2 A Time-Varying Covariate Cox Proportional Hazard Regression for Association of Statin Use and Hazard Ratio (HR) for Time to First Exacerbation in 950 COPD High-Risk Outpatients |
Patients were followed for a total of 3.5 years with median (IQR) of 2.82 years (2.63, 3.10), during which 2121 events were recorded for 600 patients. 373 and 344 patients experienced at least one moderate or severe exacerbation, respectively. For patients with exacerbations, mean yearly exacerbation rate was 0.80/person-year (1.29) and 0.80/person-year (1.36) for moderate and severe exacerbations, respectively. During follow-up, 220 patients died.
The Effect of Statin-Use on Exacerbations
In the time-varying covariate, crude Cox regression model statin use was not found to be associated with reduced time to AECOPD (HR = 1.10; 95% CI 0.92 to 1.32; p = 0.276). Stratifying for smoking status and adjusting for age, sex, concomitant heart failure with reduced ejection fraction  40% (HFrEF), BMI, pulmonary medication use and GOLD 2020 classification did not influence the association between statin use and time to AECOPD (HR = 1.15; 95% CI 0.96 to 1.39; p = 0.135) although a slight increased HR in the statin group was observed (Table 2).
40% (HFrEF), BMI, pulmonary medication use and GOLD 2020 classification did not influence the association between statin use and time to AECOPD (HR = 1.15; 95% CI 0.96 to 1.39; p = 0.135) although a slight increased HR in the statin group was observed (Table 2).
When stratifying for moderate and severe exacerbations in a sub-analysis in the same model, statin use was not to reduced time to AECOPD for either severity (HR = 1.02 (95% CI 0.85 to 1.24; p = 0.811) and HR = 1.07 (95% CI 0.89 to 1.29; p = 0.492) respectively).
The Effect of Statin-Use on All-Cause Mortality
In the time-varying covariate, crude Cox regression model, a non-significant increase in mortality for statin users was observed in comparison to non-users, HR = 1.25 (95% CI 0.96 to 1.64, p = 0.10). Stratifying for age, sex and smoking status and adjusting for HFrEF, BMI and GOLD 2020 classification did not influence the association between statin use and mortality although the HR for mortality in the statin group was decreased to near 1, HR = 1.05 (95% CI, 0.75 to 1.47; p = 0.777) (Table 3).
 |
Table 3 A Time-Varying Covariate Cox Proportional Hazard Regression for Association of Statin Use and Hazard Ratio (HR) for All-Cause Mortality in 950 COPD High-Risk Outpatients |
Interaction Analyses
No interaction was observed between statin use and CVD in either model (p = 0.992) (Tables 2 and 3). It did however alter the association between statin use and mortality (HR = 0.81; 95% CI, 0.49 to 1.33; p = 0.402) in favor of statin use.
Likewise, no interaction was found between statin and ICS use in both models, but a borderline-significant decrease in HR was seen for time to first AECOPD, HR = 0.55 (95% CI, 0.29 to 1.06; p = 0.0778) and a non-significant decrease in HR was seen for mortality, HR= 0.69 (95% CI, 0.17 to 2.80; p = 0.604). And no interaction was found between ICS use and GOLD 1–4 severity (p = 0.221).
Discussion
In this cohort study consisting of 950 COPD outpatients followed for 3.5 years, we did not find any association between statin use and risk of AECOPD or all-cause mortality after adjusting for age, sex, BMI, GOLD 2020 classification, smoking status, HFrEF and concurrent CVD.
Inflammation in COPD and CVD
Inflammation is a hallmark of COPD both locally and systemically20 and once established, the chronic inflammation in COPD is often persistent despite smoking cessation.21 An AECOPD is characterized by increased systemic inflammatory activity.22 Both endogenic and exogenic factors may be triggers, such as respiratory viral and bacterial infections, but mechanisms for flare-ups remain to be further elucidated to develop more efficient preventive initiatives.23 Anti-inflammatory agents such as ICS and macrolides are widely used in certain subsets of COPD patients with high morbidity and/or eosinophilic inflammation.17,24,25 While the anti-inflammatory effect of statins result in a significant reduction of IL-6 and CRP levels in COPD patients,9 the clinical significance remain unknown. A subset of COPD patients have a higher baseline inflammation level11 and therefore might benefit the most from a reduction in local and/or systemic inflammation. A baseline CRP level could potentially guide statin use in COPD patients as a treatable trait, on par with eosinophil-guided ICS-use.26 Systemic inflammation is furthermore a driver of atherosclerosis and heart failure in CVD,27 potentially explaining the high burden of CVD in COPD as well as the high IL-6-drive in COPD patients with manifest CVD compared to those without known CVD.10 As such, COPD patients with elevated systemic inflammatory drive have been hypothesized to benefit most from statin treatment, both in terms of COPD- and CVD-risk.
The Effect of Statin Use on Exacerbations
Our findings on exacerbations are in accordance with results from the RCT STATCOPE,28 where 40 mg daily of simvastatin had no effect on exacerbation rates in COPD patients without CVD-related comorbidities. Furthermore, in a well-characterized Dutch cohort study, COMIC,29 no association between statin use and AECOPD risk was found, supporting STATCOPE’s findings. In contrast to STATCOPE28 and COMIC,29 a Danish nested case–control study by Ingebrigtsen et al11 reported reduced odds of exacerbation in COPD patients with CVD receiving statin treatment. The increased HR observed in our statin group is likely due to chance or due to confounding by indication with a sicker statin group, because of unadjusted unmeasured bias.
The diverging results between these large, well-characterized studies could be attributed to different COPD populations being investigated. In the positive study by Ingebrigtsen et al,11 the study setting was primarily primary care, whereas the COMIC29 and STATUETTE cohorts were both conducted on moderate-to-high-risk COPD patients from a secondary care setting. Ingebrigtsen et al11 suggest that COPD patients with coexisting CVD as a potential target-population for statin treatment, but both the COMIC29 and STATUETTE cohorts contain a high burden of CVD comorbidity and as such cannot be the sole explanation for the diverging results. While CVD underdiagnosis could be more prevalent in a general COPD population than in specialized care, it is unlikely to drive the observed positive association. Two large Taiwanese retrospective cohort studies investigating the use of statins in high-risk populations with a history of previous AECOPD found a beneficial effect on risk of future exacerbations,30,31 with Lin et al30 reporting that the effect was primarily driven by older individuals with cardiovascular comorbidity. These findings are in accordance with Ingebrigtsen et al11 who used a study design that also matched on cardiovascular disease, in contrast to the present cohort which is designed without direct matching on cardiovascular disease status. As expected, this led to a higher comorbidity burden in intervention group due to confounding by indication, but even after adjusting for cardiovascular disease presence in multivariable analyses we are unable to identify a protective effect from statin treatment on exacerbations in the present study.
The Effect of Statin Use on Mortality
Our findings regarding statin use on all-cause mortality risk are in discordance with meta-analysis findings from previous observational studies reporting reduced risk of mortality.12 However, the COMIC29 findings on mortality risk are in accordance with the STATUETTE cohort. It should be noted that in some of the studies included in the meta-analysis by Lu et al,12 there was no adjustment for immortal time bias, whereas both the COMIC29 and STATUETTE cohorts were designed with this in mind. Depending on the degree of immortal time this bias can alter the results drastically due to the length of the follow-up period.18 Our results on exacerbations are still contrasted though by a recent retrospective cohort study by Raymakers et al32 using historical data records with COPD patients selected from a general population with a study design intended to minimize immortal time bias by study design. The study reported a reduced risk of mortality favoring statins, and differences in results could again be because of different COPD populations where Raymakers et al32 like Ingebrigtsen et al11 selected COPD patients from a general population. Other critical study design differences could also account for the contrasting findings, as Raymakers et al32 relied on prescription data to identify patients, whereas the present study had spirometry-verified patients and access to smoking status and lung function parameters, both important confounders for mortality.33,34 Another major retrospective cohort study from Sweden by Ekström et al,35 with a study design similar to the present study, found a trend towards statins reducing mortality. Ekström et al35 included COPD patients on long-term supplemental oxygen therapy and adjusted for cardiovascular disease in the multivariable model. When adjusting for cardiovascular disease in the STATUETTE cohort, similar, albeit non-significant, reductions in mortality are seen as those reported by Ekström et al,35 suggesting either a lack of power or a minute effect size in the included populations.
There exists a considerable lack of evidence in terms of RCT studies exploring statin therapy and mortality in COPD, with current studies reporting negative results either due to sample size 36,37 or inappropriate exclusion of patients with concomitant cardiovascular disease.28 Nevertheless, the large amount of patients included and the sizeable mortality reduction observed in the meta-analysis by Chang et al12 as well as the discrepancy between observational and RCT studies, creates a large unmet need for large, high-quality RCTs with a study population as close to the real world as possible.
In terms of differential risk profiles within COPD, Ingebrigtsen et al11 and an observational study by Lahousse et al38 have reported an association between inflammation level and an increased risk of exacerbations and all-cause mortality respectively, suggesting that statins may work by altering the degree of systemic inflammation. Lahousse et al38 also reported a more beneficial statin-response in COPD patients with a high baseline hsCRP on mortality. The hypothesis that systemic inflammation drives a more beneficial statin response needs further testing and studies for this are warranted. Inflammation level could potentially help risk stratify and guide the treatment of COPD patients.
While the present study does not include baseline inflammatory markers, it did contain a high burden of CVD with 31% of included patients having one or more CVD comorbidities. Studies have shown that cardiac disease account for 12–60% of deaths in COPD patients, depending on study population.6 Thus, actively screening for and treating CVD when indicated in COPD patients should be of major concern for the clinician, especially as the suggested effects of statin treatment seemingly is found in COPD patients with concurrent CVD.11
Furthermore, we found that a significant proportion of COPD patients followed at a university hospital outpatient clinic never had cholesterol levels measured or received statin treatment despite significantly elevated cholesterol levels. Considering the significant overlap in risk factors and the increased mortality risk with concomitant CVD in COPD, clinicians should consider to routinely assess cardiovascular risk parameters such as cholesterol levels in COPD outpatient clinics.
Interestingly, ICS use in the interaction analysis altered the HR estimate between statin use and exacerbation and mortality in our regressions in favor of statins, suggesting that COPD patients who are eligible for ICS treatment might benefit even more from anti-inflammatory statin therapy. However, this analysis was likely underpowered but warrants further examination in future studies.
Limitations
The present study is limited by residual bias from the observational study design using historical data from medical journals and a national registry, however, the use of robust statistical measures reduces overall impact of known biases, such as immortal time bias. The single-center recruitment from a university hospital outpatient clinic limits the external validity, yet low amounts of missing data and loss to follow-up strengthens internal validity. As statin use-data is based on prescription redemption and not the prescriptions themselves, adherence to redeemed doses cannot be addressed, but is assumed to be within acceptable limits as the statin group had a significantly lower level of total cholesterol.
Conclusion
In this cohort study of 950 COPD outpatients, we did not find any association between statin use and risk of AECOPD or all-cause mortality. The result adds to the evidence that an approach with statin treatment upfront is not indicated per se in COPD but should be prescribed when indicated according to current guidelines on CVD, especially to reduce risk of mortality. Further studies examining whether a high systemic level of inflammation can guide statin treatment in COPD are warranted.
Data Sharing Statement
Data available from Mathias Damkjær upon reasonable requests, however, as per Danish law approval from the Danish Patient Safety Authority and the Greater Capital Region of Copenhagen’s Data Safety Board might be required.
Guarantors
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
KH reports personal fees from TEVA, personal fees from AstraZeneca, personal fees from Chiesi, outside the submitted work; CSU reports personal fees from AstraZeneca, GSK, TEVA, Novartis, Chiesi, Boehringer-Ingelheim, SanofiGenzyme, ALK-Abello, MundiPharma, Orion Pharma and Actelion, outside the submitted work. NG reports personal fees from AstraZeneca, Boehringer-Ingelheim, Novartis and GSK, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. The Lancet - Global Burden of Disease. Available from: https://www.thelancet.com/gbd.
2. Maqsood U, Ho TN, Palmer K, et al. Once daily long-acting beta2-agonists and long-acting muscarinic antagonists in a combined inhaler versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;3. doi:10.1002/14651858.CD012930.pub2
3. Anthonisen NR, Connett JE, Murray RP. Smoking and lung function of Lung Health Study participants after 11 years. Am J Respir Crit Care Med. 2002;166(5):675–679. doi:10.1164/rccm.2112096
4. Mccarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2.
5. Vivodtzev I, Maltais F. Cardiovascular risk in COPD: searching for a culprit. Chest. 2020;157(4):753–754. doi:10.1016/j.chest.2020.01.008
6. Morgan AD, Zakeri R, Quint JK. Defining the relationship between COPD and CVD: what are the implications for clinical practice? Ther Adv Respir Dis. 2018;12:1–16. doi:10.1177/1753465817750524
7. Sin DD, Man SFP. Chronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortality.
8. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
9. Walsh A, Perrem L, Khashan AS, Henry MT, Ni Chroinin M. Statins versus placebo for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2019;7. doi:10.1002/14651858.CD011959.pub2
10. Miller J, Edwards LD, Agustí A, et al. Comorbidity, systemic inflammation and outcomes in the ECLIPSE cohort. Respir Med. 2013;107(9):1376–1384. doi:10.1016/j.rmed.2013.05.001
11. Ingebrigtsen TS, Marott JL, Nordestgaard BG, Lange P, Hallas J, Vestbo J. Statin use and exacerbations in individuals with chronic obstructive pulmonary disease. Thorax. 2015;70(1):33–40. doi:10.1136/thoraxjnl-2014-205795
12. Lu Y, Chang R, Yao J, Xu X, Teng Y, Cheng N. Effectiveness of long-term using statins in COPD - a network meta-analysis. Respir Res. 2019;20(1):1–14. doi:10.1186/s12931-019-0984-3
13. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22–25. doi:10.1177/1403494810387965
14. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data resource profile: the Danish national prescription registry. Int J Epidemiol. 2017;46(3):798. doi:10.1093/ije/dyw213
15. Ingebrigtsen TS, Marott JL, Lange P, Hallas J, Nordestgaard BG, Vestbo J. Medically treated exacerbations in COPD by GOLD 1–4: a valid, robust, and seemingly low-biased definition. Respir Med. 2015;109(12):1562–1568. doi:10.1016/j.rmed.2015.10.015
16. Reilev M, Pottegård A, Lykkegaard J, Søndergaard J, Ingebrigtsen TS, Hallas J. Increased risk of major adverse cardiac events following the onset of acute exacerbations of COPD. Respirology. 2019;24(12):1183–1190. doi:10.1111/resp.13620
17. GOLD guidelines. Availble from: https://goldcopd.org/gold-reports/.
18. Suissa S. Immortal time bias in pharmacoepidemiology. Am J Epidemiol. 2008;167(4):492–499. doi:10.1093/aje/kwm324
19. van Buuren S, Groothuis-Oudshoorn K. Mice: multivariate imputation by chained equations in R. J Stat Softw. 2011;45(3):1–67.
20. Wouters EFM. Local and systemic inflammation in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2:26–33. doi:10.1513/pats.200408-039MS
21. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
22. Hurst JR, Donaldson GC, Perera WR, et al. Use of plasma biomarkers at exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2006;174(8):867–874. doi:10.1164/rccm.200604-506OC
23. White AJ, Gompertz S, Stockley RA. Chronic obstructive pulmonary disease • 6: the aetiology of exacerbations of chronic obstructive pulmonary disease. Thorax. 2003;58(1):73–80. doi:10.1136/thorax.58.1.73
24. Kunz LIZ, Ten Hacken N, Lapperre TS, et al. Airway inflammation in COPD after long-term withdrawal of inhaled corticosteroids. Eur Respir J. 2017;49(6):1700848. doi:10.1183/13993003.00848-2017
25. Kanoh S, Rubin BK. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin Microbiol Rev. 2010;23(3):590–615. doi:10.1128/CMR.00078-09
26. Cheng SL. Blood eosinophils and inhaled corticosteroids in patients with COPD: systematic review and meta-analysis. Int J COPD. 2018;13:2775–2784. doi:10.2147/COPD.S175017
27. Yndestad A, Damås JK, Øie E, Ueland T, Gullestad L, Aukrust P. Systemic inflammation in heart failure - the whys and wherefores. Heart Fail Rev. 2006;11(1):83–92. doi:10.1007/s10741-006-9196-2
28. Criner GJ, Connett JE, Aaron SD, et al. Simvastatin for the prevention of exacerbations in moderate-to-severe COPD. N Engl J Med. 2014;370(23):2201–2210. doi:10.1056/NEJMoa1403086
29. Citgez E, Van Der Palen J, Koehorst-Ter Huurne K, Movig K, Van Der Valk P, Brusse-Keizer M. Statins and morbidity and mortality in COPD in the COMIC study: a prospective COPD cohort study. BMJ Open Respir Res. 2016;3(1):1–7. doi:10.1136/bmjresp-2016-000142
30. Lin CM, Yang TM, Yang YH, et al. Statin use and the risk of subsequent hospitalized exacerbations in COPD patients with frequent exacerbations. Int J Chron Obstruct Pulmon Dis. 2020;15:289–299. doi:10.2147/COPD.S229047
31. Wang MT, Lo YW, Tsai CL, et al. Statin use and risk of COPD exacerbation requiring hospitalization. Am J Med. 2013;126(7):598–606.e2. doi:10.1016/j.amjmed.2013.01.036
32. Raymakers AJN, Sadatsafavi M, Sin DD, De Vera MA, Lynd LD. The impact of statin drug use on all-cause mortality in patients with COPD: a Population-Based Cohort Study. Chest. 2017;152(3):486–493. doi:10.1016/j.chest.2017.02.002
33. Godtfredsen NS, Lam TH, Hansel TT, et al. COPD-related morbidity and mortality after smoking cessation: status of the evidence. Eur Respir J. 2008;32(4):844–853. doi:10.1183/09031936.00160007
34. Ching SM, Chia YC, Lentjes MAH, Luben R, Wareham N, Khaw KT. FEV1 and total cardiovascular mortality and morbidity over an 18 years follow-up population-based prospective EPIC-NORFOLK Study. BMC Public Health. 2019;19(1):1–10. doi:10.1186/s12889-019-6818-x
35. Ekström M, Hermansson A, Ström K. Effects of cardiovascular drugs on mortality in severe chronic obstructive pulmonary disease: a time-dependent analysis. Am J Respir Crit Care Med. 2013;187:715–720. doi:10.1164/rccm.201208-1565OC
36. Bartziokas K, Papaioannou AI, Minas M, et al. Statins and outcome after hospitalization for COPD exacerbation: a prospective study. Pulm Pharmacol Ther. 2011;24(5):625–631. doi:10.1016/j.pupt.2011.06.003
37. Moosavi SA, Raji H, Faghankhani M, Yazdani R, Esmaeili M. Evaluation of the effects of atorvastatin on the treatment of secondary pulmonary hypertension due to chronic obstructive pulmonary diseases: a randomized controlled trial. Iran Red Crescent Med J. 2013;15(8):649–654. doi:10.5812/ircmj.8267
38. Lahousse L, Loth DW, Joos GF, et al. Statins, systemic inflammation and risk of death in COPD: the Rotterdam study. Pulm Pharmacol Ther. 2013;26(2):212–217. doi:10.1016/j.pupt.2012.10.008
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.