")
Back to Journals » International Journal of General Medicine » Volume 14
Standardized Ultrasound Diagnosis of Nuchal Cord
Authors Xiao YJ, Chen YH, Zheng HY, Xu CM, Liu X, Yan SP
Received 3 June 2021
Accepted for publication 25 August 2021
Published 17 September 2021 Volume 2021:14 Pages 5825—5834
DOI https://doi.org/10.2147/IJGM.S322713
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Yan-ju Xiao,1,* Yan-hong Chen,1,* Hong-yu Zheng,1 Chun-mei Xu,1 Xiao Liu,2 Si-ping Yan2
1Department of Ultrasonography, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, 530021, People’s Republic of China; 2Department of Obstetrical, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, 530021, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan-hong Chen
Department of Ultrasonography, People’s Hospital of Guangxi Zhuang Autonomous Region, No. 6 of Taoyuan Street, Qingxiu District, Nanning, 530021, People’s Republic of China
Tel +86 771 2186593
Fax +86 771 2802018
Email [email protected]
Objective: This study aims to investigate the formation factors that affect the angle of nuchal cord and explore the types of nuchal cord that exist and the process of standardized ultrasound diagnosis of nuchal cord.
Methods: Ultrasonography was performed on 707 fetuses with nuchal cord, to observe the direction of the coil, determine the type of coil, and analyze the correlation between the fetal position, placental location, and the direction of the coil with the angle of the umbilical cord.
Results: Among the 707 fetuses, those with 1 loop accounted for 89.67%, fetuses with 2 loops accounted for 6.08%, fetuses with 3 loops accounted for 0.28%, and fetuses with partial draping of the umbilical cord accounted for 3.96%. Nuchal cord mostly occurred in fetuses where the placenta was attached to the anterior wall of the uterus, and the α-shaped and C-shaped types were in the majority. The C-shaped type accounted for 43.14%, the α-shaped type for 40.88%, the O-shaped type for 12.02%, and the L-shaped type for 3.96%.
Conclusion: The direction of the coil of the umbilical cord can be determined by blood flow vector observation. The fetal position, placental location, and the direction of the coil are the three factors affecting the coiling angle of the umbilical cord. Ultrasonic classification of nuchal cord can provide detailed information, which can be used by physicians when performing surgery on the fetus. The advances in the diagnosis procedure allow the diagnosis of nuchal cord to be carried out in an orderly manner, making it more accurate and standardized.
Keywords: nuchal cord, coiling direction, ultrasonic classification, diagnostic process, standardization
Introduction
Previous studies on the coiling of nuchal cord were limited to the number of loops and the incidence rate, and there were few reports on the diagnostic criteria.1–7 In the past ten years, a comprehensive and in-depth exploration of the direction of the coil, types of coil, guidelines for assessing coil direction and factors affecting the coiling angle has been made. There are now recognized to be 5 standard types and 11 subtypes of nuchal cord, while the guidelines for assessing coil direction and three main factors affecting the coiling angle have been determined.8,9 We propose a new ultrasonic diagnostic classification of nuchal cord. This diagnostic classification carries detailed ultrasonic diagnostic information, which can help clinicians accurately understand the status of nuchal cord and perceive the difference in the degree of fetal entanglement. Here, this paper summarizes the ultrasonic standardized diagnosis process of nuchal cord and forms a standardized process for practical application.
Data and Methods
Subjects
Between January 2, 2006 and December 31, 2019, 707 cases of mid and late singleton pregnancy diagnosed with nuchal cord were examined in our hospital. The pregnant women ranged in age from 17 to 46 years, with an average age of (29.6±3.9) years. The blood flow vector of the umbilical artery was observed using color Doppler ultrasonography to identify the direction and type of nuchal cord.
Study Methods
LOGIQ9, VOLUSON 730, VOLUSON E8 and VOLUSON E10 color Doppler ultrasound diagnostic apparatuses, with a probe frequency of 3.5–5.5 MHz, were used to observe various features of nuchal cord.
Determining the Direction of the Coil of the Umbilical Cord
The umbilical cord blood flow chart was obtained at the transverse section of the fetal neck, and according to the blood flow characteristics displayed on the screen, the following conclusions could be drawn: if there were two red and one blue continuous blood flow signals on the left half of the loop, and two blue and one red continuous blood flow signals on the right half of the loop, this indicated that the umbilical cord was coiling from left to right (anticlockwise coiling); if it was the other way round this meant the umbilical cord was coiling from right to left (clockwise coiling), as shown in Figure 1. Thus, after obtaining the umbilical cord blood flow chart at the transverse section of the fetal neck, it was possible to determine the direction of the coil of the umbilical cord.10
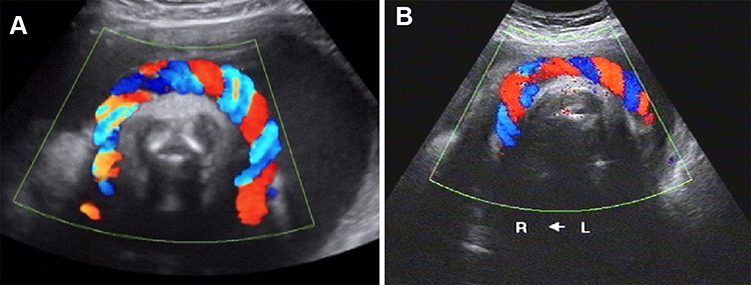 |
Figure 1 (A) Sonogram of nuchal cord clockwise coiling, the characteristic of blood flow: two red and one blue on the right half arc, and two blue and one red on the left half arc, it represents the umbilical cord coiling from right to left. (B) Sonogram of nuchal cord anticlockwise coiling, the characteristic of blood flow: two red and one blue on the left half arc, and two blue and one red on the right half arc, it represents the umbilical cord coiling from left to right. |
Determining the Fetal Position
Left occiput-anterior (LOA), breech or transverse presentations (for transverse presentation it should first be determined if the fetal head is in the left or right side of the uterine cavity) were recorded, and the left and right sides of the fetus were determined according to the fetal four-chamber view and the gastric vesicle view.11
Determining the Fetal Spine Orientation
The following were recorded: the left- and right-side aspects, the left and right anterior aspects, the left and right posterior aspects, and the front and back positions. When the fetal position was transverse, it was recorded whether the spine was facing the fundus of the uterus or the pubis.12
Determining the Placental Attachment Site
The following are the possible points where the placenta may be attached: the anterior wall, posterior wall, left wall, left anterior wall, left posterior wall, right wall, right anterior wall, right posterior wall, or the fundus of the uterus.13
Determining the Angle Between the Root and Pedicle of the Umbilical Cord
There are four types of nuchal cord, the α-shaped type, the O-shaped type, the C-shaped type, and the L-shaped type. The type depends on the angle formed by the root and the pedicle of the umbilical cord. Taking a fetus with a placenta attached to the posterior wall and a fetus attached at the LOA as examples, the standard types are as follows: the α-shaped type (360°< angle < 540°) is when the spine is located on the left side and the umbilical cord is wrapped round the neck more than once; the O-shaped type (the angle is approximately 360°) is when the spine is located on the front side and the umbilical cord is wrapped round the neck once; the C-shaped type (180° < angle < 360°) is when the spine is located on the right side and the umbilical cord is not completely wrapped round the neck; and it is the L-shaped type (angle ≤180), when the spine is located at the rear, the umbilical cord is about half a loop or less, and the cord runs to the placenta through the anterior chest and one side of the neck, as shown in Figure 2. When the umbilical cord is looped round more than twice, the part that does not form a complete loop can continue to be typed, so, for example, there is a two-looped α-shaped type and a three-looped C-shaped type. Ultrasonic images of α-shaped, O-shaped and L-shaped types of nuchal cord are shown in Figure 3.
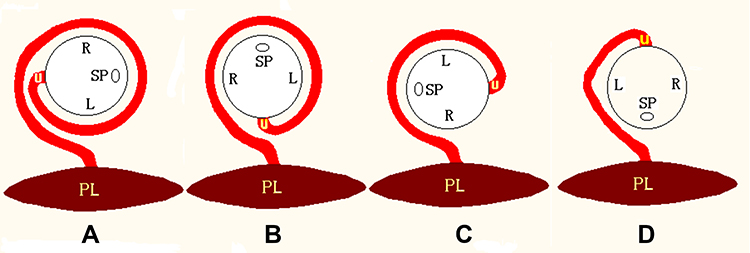 |
Figure 2 (A) α-shaped type: Left occipital transverse position, the spine is on the left side, the umbilical cord coils more than 1 cycle, 360° < angle < 540°; (B) O-shaped type: Anterior occipital position, the spine is in the front, the umbilical cord coils 1 cycle, the angle is 360°; (C) C-shaped type: Right occipital transverse position, the spine is on the right side, the umbilical cord coils less than 1 cycle, 180° < angle < 360°; (D) L-shaped type: Occipitoposterior position, the spine is at posterior site, the umbilical cord runs to the placenta through the anterior chest and one side of the neck, the coiling angle is ≤180°. Abbreviations: SP, spine; L, Left side; R, Right side; U, The root of the umbilical cord; PL, Placenta. |
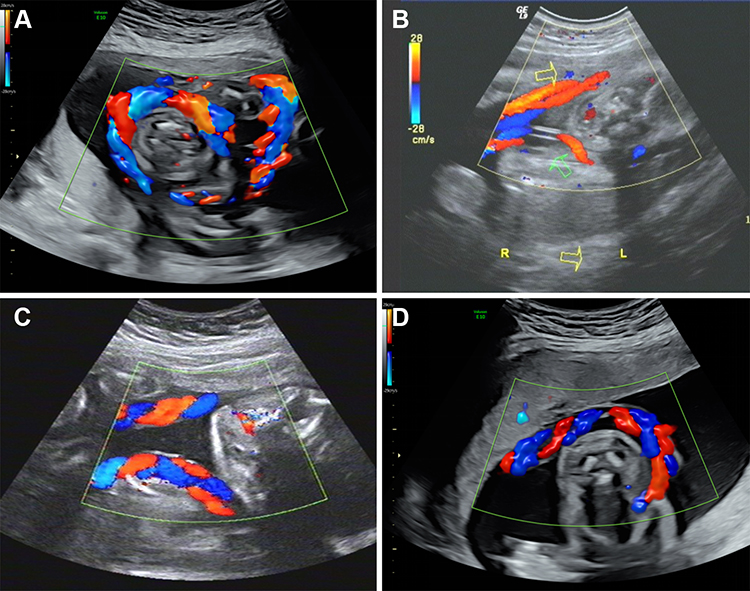 |
Figure 3 (A) α-shaped type: LOA position, right Figure shows the spine in the right front, the umbilical cord coils from left to right, left Figure shows the umbilical cord crossing the chest and entering the anterior wall of placenta, the coiling angle is >360°; (B) O-shaped type: The blood flow of the umbilical artery is in the direction of the arrow, the yellow arrow is the proximal end of the umbilical cord, and the green arrow is the distal end of the umbilical cord, the coiling angle is 360°; (C) C-shaped type: LOA position, the spine is on the left side, it can be seen that the umbilical cord coils from right to left, the distal end enters the posterior wall of placenta, the two ends of the umbilical cord are far away from each other and are hung in the neck like a scarf; (D) L-shaped type: LOA position, the spine is on the right side, the umbilical cord runs from the right anterior wall of the placenta through the left side of the fetal neck, the umbilical artery blood flow is blue, it represents the direction of the umbilical cord from the chest to the back. |
In summary, for each fetus with nuchal cord, the number of loops and the direction of the coil of the umbilical cord were determined by observing the umbilical cord indentation on the fetal neck skin. In addition, the angle between the root and pedicle of the umbilical cord was determined according to the fetal position, spinal position, and placental attachment position, and the type of nuchal cord was identified and all the data recorded.
Results
1. Of the 707 fetuses examined, fetuses with 1 loop accounted for 89.67%, fetuses with 2 loops accounted for 6.08%, fetuses with 3 loops accounted for 0.28%, and fetuses with partial draping of the umbilical cord accounted for 3.96%.
2. The fetuses whose umbilical cord was coiled from left to right accounted for 53.17%, those coiled from right to left accounted for 46.83%, but the fetuses with partial draping of the umbilical cord were not included the calculation of direction. Figure 4 shows the direction of the coil in three types of nuchal cord: the C-shaped type, O-shaped type and α-shaped type.
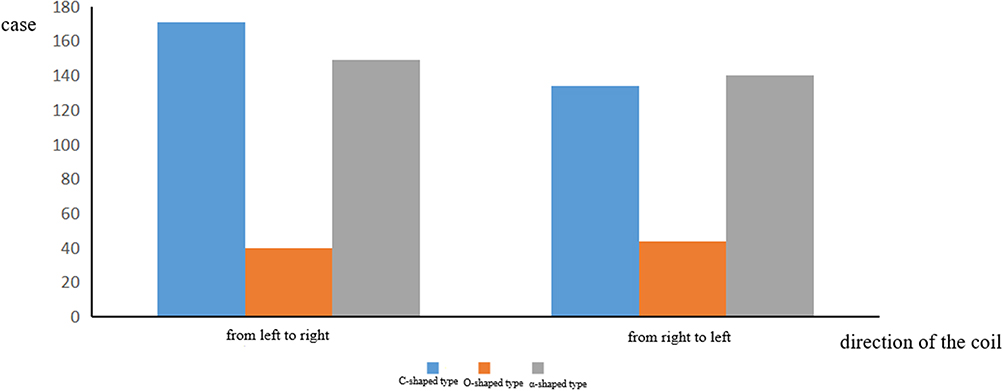 |
Figure 4 Type and direction of nuchal cord. |
3. Nuchal cord mostly occurred in fetuses with a placenta attached to the anterior wall of the uterus, and the α-shaped and C-shaped types were in the majority, the C-shaped type accounting for 43.14%, the α-shaped type accounting for 40.88%, the O-shaped type accounting for 12.02%, and the L-shaped type accounted for 3.96%. The correlation between the type of nuchal cord and placental position is shown in Figure 5.
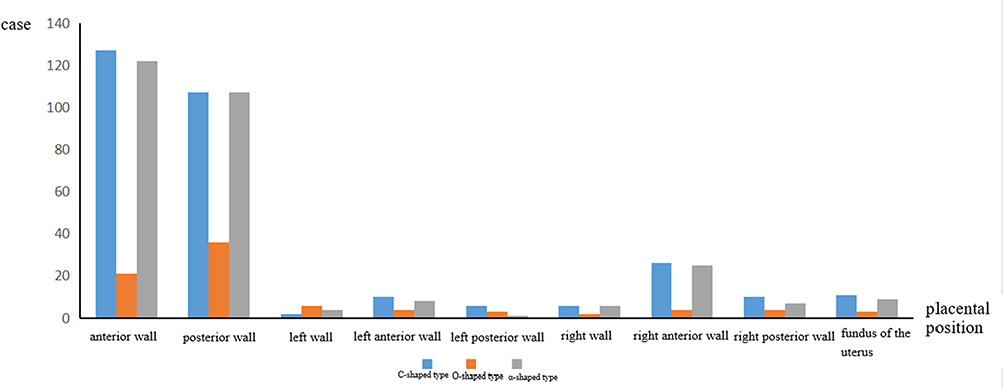 |
Figure 5 The relationship between the type of nuchal cord and placental position. |
4. The correlation between the type of nuchal cord and the spinal orientation is shown in Figure 6.
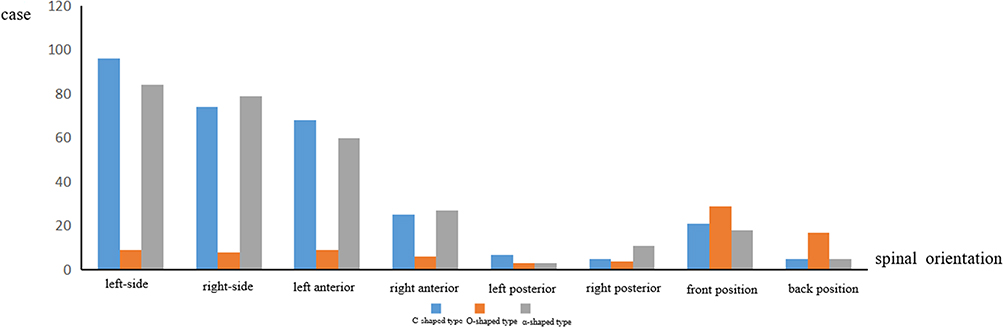 |
Figure 6 The relationship between the type of nuchal cord and spinal orientation. |
5. The correlation between the direction of the coil of the nuchal cord and the fetal position is shown in Figure 7.
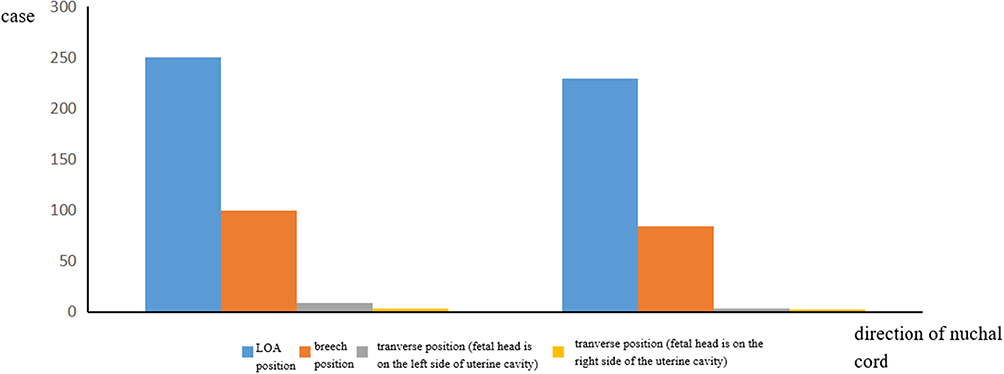 |
Figure 7 The relationship between coiling direction of nuchal cord and fetal position. |
6. Further classification of nuchal cord.
In addition to the typical α-shaped, O-shaped, C-shaped and L-shaped classifications, the following subtypes can be identified according to the direction of the coil of the proximal and distal parts of the umbilical cord (see Figure 8 for the model diagram of each type):
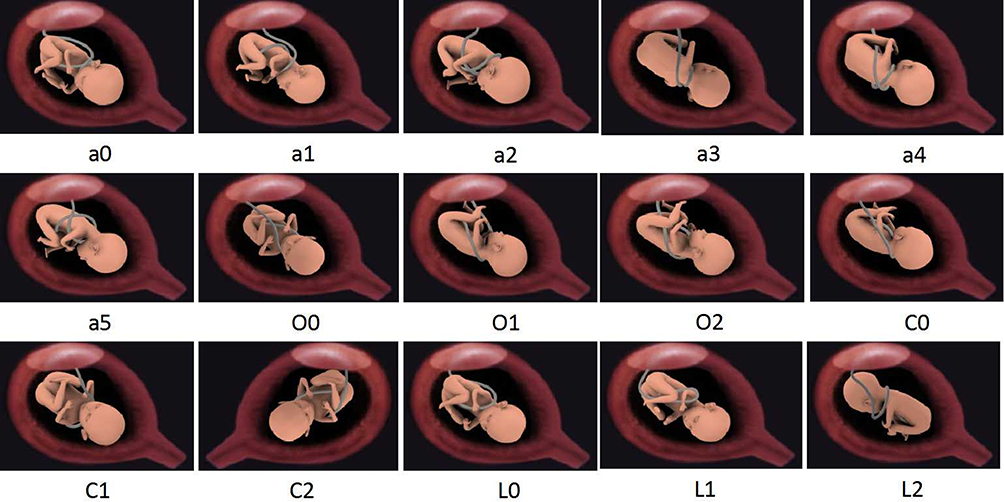 |
Figure 8 Model Figure of all types of nuchal cord. |
(1) The subtypes of the α-shaped type are as follows:α1, the proximal diagonal subtype, where the cord is coiled round the neck and then round the waist; α2, the distal-initiating side axillary diagonal subtype, where the cord goes to the opposite side, coils round the neck and goes through the ipsilateral armpit; α3, the distal opposite side axillary diagonal subtype, which is when the first loop coils around the neck, and the second runs diagonal to the contralateral armpit and then goes through; and the α4, the proximal diagonal–distal opposite axillary diagonal subtype, where the umbilical cord mainly coils across the front of the neck, and there is no umbilical cord indentation or blood flow signal on the dorsal side of the neck, which can sometimes lead to a missed diagnosis.
(2) The subtypes of the O-shaped type are as follows: O1, the proximal diagonal subtype, where the cord is wrapped around the fetus with the starting end at one side of the waist, extending to the opposite side of the neck, at an angle of up to 360°, and the O2, the distal diagonal subtype, where the distal end goes out from the armpit, at an angle of up to 360°.
(3) The subtypes of the C-shaped type are the C1, the proximal diagonal subtype, whose angle is <360° and the C2, the distal diagonal subtype, whose angle is <360°.
(4) There are two subtypes of the L-shaped type. The L1 is the back-to-front subtype, where the umbilical cord passes through the ipsilateral back to the ipsilateral neck from back to front, and the umbilical cord can easily slip off. The L2 is the turn-back subtype, where the umbilical cord does not run across the chest, but just runs from one side of the neck to the other, and there is a turn back at the distal end of the umbilical cord.
Discussion
The Need for Standardization of Diagnostic Criteria for Nuchal Cord
There had been no uniform diagnostic criteria for nuchal cord. At present, the diagnostic description of nuchal cord in ultrasound reports is very simple, and there was a lack of more specific and unified description method for the nuchal cord. Clinicians also could not accurately understand the status of the umbilical cord from the ultrasound report, and there was no specific classification diagnosis to help clinicians perceive the difference in the degree of umbilical cord. Therefore, it was necessary to carry out standardized management of diagnosis of nuchal cord.14
Feasibility of Standardization of Diagnostic Criteria for Nuchal Cord
The coiling direction, fetal position, placental position, proximal direction of umbilical cord and distal direction of umbilical cord are five necessary conditions for the standardization of diagnostic criteria. As long as the coiling direction, fetal position and placental position are mastered, and both ends of the umbilical cord are tracked and observed, the classification diagnosis of nuchal cord can be obtained. This method is simple and easy to implement, and the diagnostic information is comprehensive. Therefore, it is recommended that the standard diagnosis of umbilical cord around neck should include: fetal position, winding number of umbilical cord, and classification by coiling direction and coiling angle. For example, the diagnosis was “LOA position, fetuses with 1 loop of nuchal cord (coiling from left to right), C-shaped type” or “breech position, fetuses with 1 loop of nuchal cord (coiling from right to left), α4 subtype.”
Process of Standardized Diagnosis of Nuchal Cord
(1) To clear fetal position: Left occiput-anterior (LOA), breech or transverse presentations.
(2) To clear the winding number of the umbilical cord: “U” shaped imprint means the umbilical cord goes around the neck once, “W” shaped imprint means the umbilical cord goes around the neck twice, and “sawtooth” shaped imprint means the umbilical cord goes around the neck three times or more. The ultrasound probe was rotated 90 degrees to make a lateral scan of the neck to further observe the umbilical cord around the neck of the fetus.
(3) To clear the coiling direction:
The umbilical cord consists of two umbilical arteries and one umbilical vein. Blood in the umbilical arteries flows from the fetus to the placenta, and blood in the umbilical vein flows from the placenta to the fetus.15,16 This paper summarizes the ultrasound diagnostic techniques widely used in obstetrics in recent decades.17–19 Using blood flow vector observation, the direction of the coil can be determined accurately by applying the assessment guidelines for nuchal cord20 (see Figure 9).
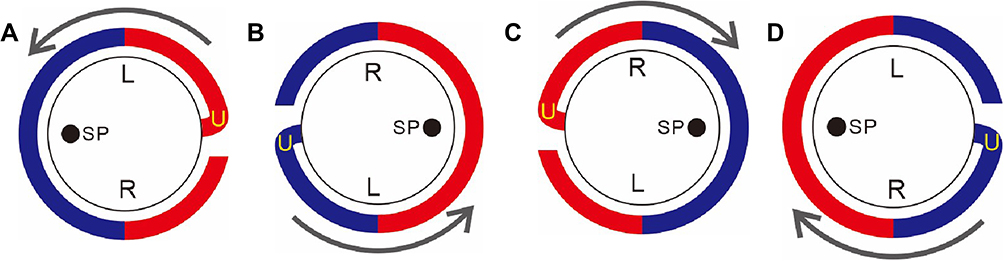 |
Figure 9 (A, B) If the direction of the blood flow is anti-clockwise, in case of LOA position, regardless of the spinal orientation, the umbilical cord coils from left to right; in case of breech presentation, regardless of the spinal orientation, the umbilical cord coils from right to left. (C, D) If the direction of the blood flow is clockwise, in case of LOA presentation, regardless of the spinal orientation, the umbilical cord coils from right to left; in case of in breech presentation, regardless of the spinal orientation, the umbilical cord coils from left to right. Abbreviations: SP, spine; U, Umbilical cord; L, Left side; R, Right side; Red, Blood flow towards the probe; Blue, Blood flow away from probe. |
When the fetus is in the LOA position, regardless of the orientation of the spine, if the blood flow direction is clockwise, it can be determined that the umbilical cord is coiling from right to left; if the blood flow direction is anti-clockwise, it can be determined that the umbilical cord is coiling from left to right.
When the fetus is in the breech position, regardless of the orientation of the spine, if the blood flow direction is clockwise, it can be determined that the umbilical cord is coiling from left to right; if the blood flow direction is anti-clockwise, it can be determined that the umbilical cord is coiling from right to left.
When the fetus is in the transverse position, and the fetal head is on the right side of the uterine cavity, the direction of the coil can be determined according to the assessment guidelines for the LOA position, and when the fetal head is on the left side of the uterine cavity, it can be determined according to those for the breech position.
(4) To clear the classification of nuchal cord.
Nuchal cord can be divided into four types, depending on the different angles of the coil and the body parts of the fetus around and across which the umbilical cord runs. These consist of the α-shaped type, the O-shaped type, the C-shaped type, and the L-shaped type, and these have corresponding subtypes. For example, the α-shaped type (360°< angle < 540°) is when the spine is located on the left side and the umbilical cord is wrapped round the neck more than once; the O-shaped type (the angle is approximately 360°) is when the spine is located on the front side and the umbilical cord is wrapped round the neck once; the C-shaped type (180° < angle < 360°) is when the spine is located on the right side and the umbilical cord is not completely wrapped round the neck; and it is the L-shaped type (angle ≤180), when the spine is located at the rear, the umbilical cord is about half a loop or less, and the cord runs to the placenta through the anterior chest and one side of the neck. When the umbilical cord is looped round more than twice, the part that does not form a complete loop can continue to be typed. The corresponding subtypes were diagnosed in Result 6. It is also worth noting that Subtype L2 should be distinguished from the 2-loop C-shaped type, since in subtype L2 it is possible to detect two opposite blood flow signals on the same side of the neck, which is due to the umbilical cord folding back on itself. When the umbilical cord blood flow signal is only detected on one side of the neck, in addition to potentially being the L-shaped type, it may also be the C1, C2, O1, O2 and α5 subtypes. Therefore, it is necessary to use the blood flow vector observation method to track and determine the course of the umbilical cord and make an accurate diagnosis of the type of coil to better assess its impact on the fetus.
(5) Pay attention to the association between the fetal position, placental location, and the direction of the coil with the type of coil.
The direction of the coil (clockwise or anticlockwise) may be the same, but a different type of coil can form when the spinal orientation is different; similarly, when the spinal orientation is the same but the direction of the coil is different, different types can form. The type of coil can also differ when the direction of the coil and the spinal orientation are different, and when the direction and orientation are the same, if the placental position is different, the type of coil of the umbilical cord may be different (Figure 10). Therefore, the fetal position, placental location, and the direction of the coil of the umbilical cord are the three factors affecting the type of coil.21
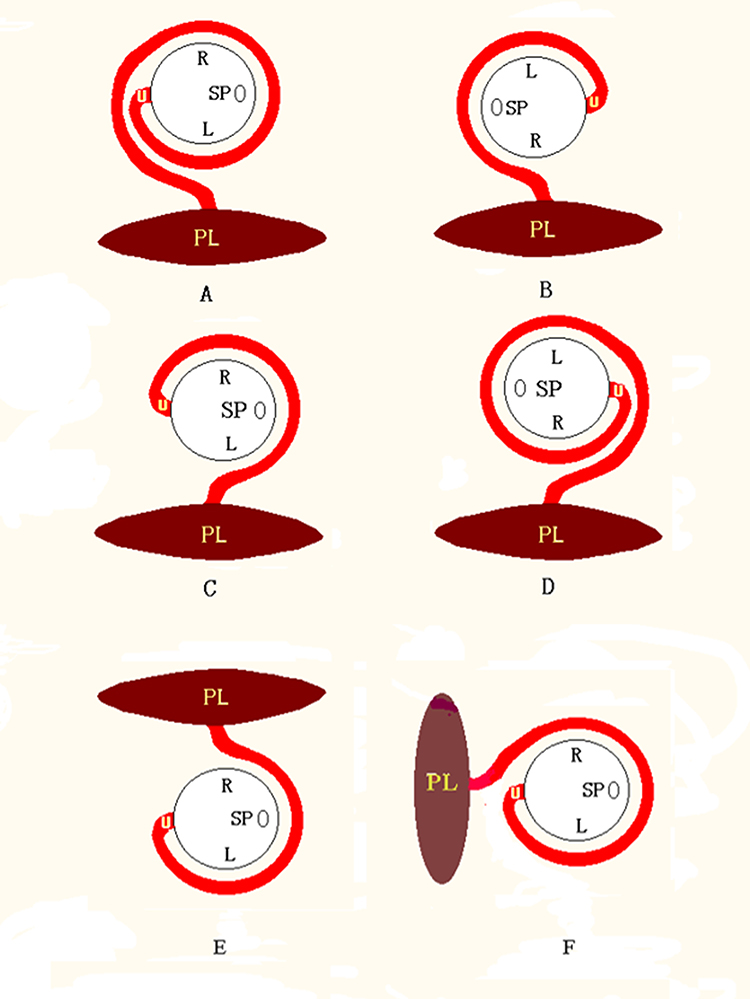 |
Figure 10 The relationship of the fetal position, placental location and the coiling direction of the umbilical cord with the coiling angle of the umbilical cord. When the coiling direction of the umbilical cord is the same (all from left to right or from right to left), but the spinal orientations are different, the coiling angles are different (A vs B and C vs D); when the coiling direction is different, and the spinal orientation is the same, the coiling angles are different (A vs C and B vs D); when the spinal orientations are different, and the coiling direction are different, the coiling angles are also the same (A vs D and B vs C); For population, even if the spinal orientations and the coiling directions are the same, but the placental locations are different, the coiling angles will also be different (E vs F). Therefore, the coiling angle of the umbilical cord is determined jointly by the placental location, the fetal position and the coiling direction of the umbilical cord. Abbreviations: L, Left; R, Right; SP, Spine; PL, Placenta; U, Umbilical cord. |
The Standardized Diagnosis Nuchal Cord Procedure
A procedure was formulated, as shown in Figure 11, to make the whole diagnosis process simpler and clearer and to standardize the diagnosis of nuchal cord.
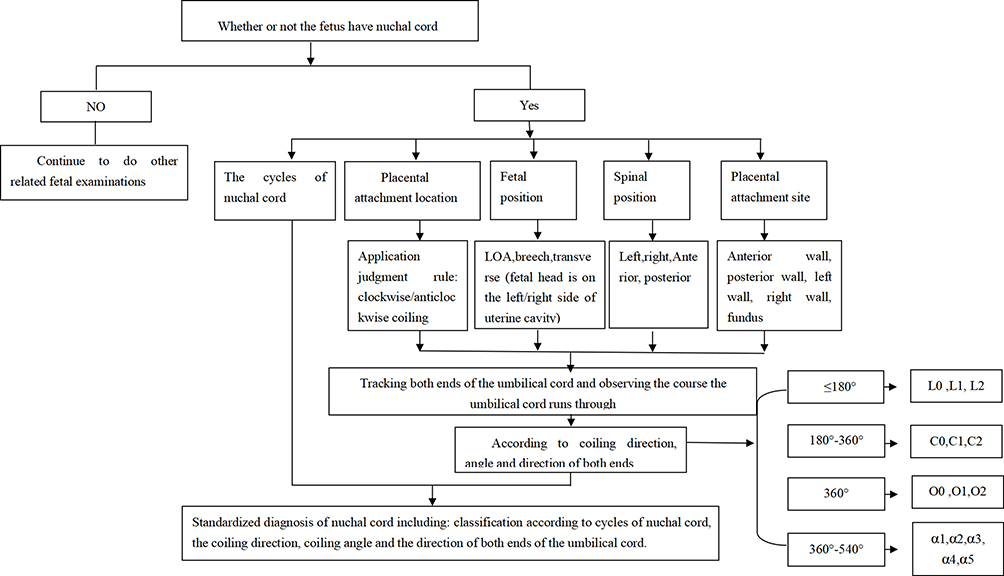 |
Figure 11 Standardized diagnosis process of nuchal cord. |
Conclusion
The direction of the coil of the umbilical cord can be determined by blood flow vector observation. The fetal position, placental location, and the direction of the coil of the umbilical cord are the three factors affecting the coiling angle of the umbilical cord. Ultrasonic classification of nuchal cord can provide detailed information, which can be used by physicians when performing surgery on the fetus. The advances in the diagnosis procedure allows for the standardized diagnosis of nuchal cord to be carried out in an efficient manner, making it more accurate and standardized, reducing the risk to the health of the unborn fetus and its mother.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of People’s Hospital of Guangxi Zhuang Autonomous Region (No. KY-LW-2019-2). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Consent for Publication
All patient guardians signed a document of informed consent.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Self-raised Fund of Guangxi Department of Health (Z2010257).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Birnholz JC. Ecologic physiology of the fetus: ultrasonography of supply-line deprivation syndromes. Radiol Clin North Am. 1990;28:179–188.
2. Sheiner E, Abramowicz JS, Levy A, Silberstein T, Mazor M, Hershkovitz R. Nuchal cord is not associated with adverse perinatal outcome. Arch Gynecol Obstet. 2006;274:81–83.
3. Clapp JF, Stepanachak W, Hashimoto K, Ehrenberg H, Lopez B. The natural history of antenatal nuchal cords. Am J Obstet Gynecol. 2003;189:488–493.
4. Crawford JS. Cord around the neck. Incidence and sequelae. Acta Paediatr. 1962;51:594–603.
5. Spellacy WN, Graven H, Fisch RO. The umbilical cord and complications of true knot, nuchal cords, and cords around the body. Am J Obstet Gynecol. 1966;94:1136–1142.
6. Chen YH, Qin GC. Clinical application of ultrasound in the detection of fetal umbilical cord. J Guangxi Med Univ. 2014;1(31):159–161.
7. Qin GC, Ning JL, Chen YH, et al. Dynamic monitoring of fetal nuchal cord. Chinese J Med Imag Technol. 2015;3(31):434–437.
8. Chen YH, Wan LK, Xu CM, Zhang BL, Wei LH, Shen GX. Application of cord blood flow vector in the diagnosis of fetal nuchal circular umbilical cord. Chinese J New Clin Med. 2010;3(10):937–940.
9. Chen YH, Xu CM, Wan LK, Zhang BL, Wei LH, Zheng HY. Classification of five types of fetal nuchal circular umbilical cord by ultrasound. Chinese J Ultrasound Med. 2011;27(3):270–273.
10. Chen YH, Xu CM, Yan SP, et al. Means of intrauterine intervention to fetal nuchal circular umbilical cord. Chinese J UltrasoundMed. 2009;25(7):694–696.
11. Eggebø TM, Hassan WA, Kå S, Torkildsen EA, Østborg TB, Lees CC. Prediction of delivery mode by ultrasound-assessed fetal position in nulliparous women with prolonged first stage of labor. Ultrasound Obstet Gynecol. 2015;46(5):606–610.
12. Masturzo B, Farina A, Attamante L, et al. Sonographic evaluation of the fetal spine position and success rate of manual rotation of the fetus in occiput posterior position: a randomized controlled trial. J Clin Ultrasound. 2017. doi:10.1002/jcu.22477
13. Zhang LH, Zhang RX, Wu SY. Effect of placental abruption on pregnant prognosis in different placental attachment sites. Hainan Med J. 2017;28(5):758–760.
14. Chen Y-H, Liu X, Xu C-M. Standardization of diagnosis for coiling of the umbilical cord around fetal neck by ultrasound. Int J Gynaecol Obstet. 2019;147(1):96–101.
15. Hellevik LR, Kiserud T, Irgens F, Stergiopulos N, Hanson M. Mechanical properties of the fetal ductus venosus and umbilical vein. Heart Vessels. 1998;13(4):175–180.
16. Saw SN, Dawn C, Biswas A, Mattar CN, Yap CH. Characterization of the in vivo wall shear stress environment of human fetus umbilical arteries and veins. Biomech Model Mechanobiol. 2017;16(1):197–211.
17. Sharma B, Bhardwaj N, Gupta S, Gupta PK, Verma A, Malviya K. Association of umbilical coiling index by colour Doppler ultrasonography at 18-22 weeks of gestation and perinatal outcome. J Obstet Gynaecol India. 2012;62(6):650–654.
18. Sun J, Wang L, Li Y. Clinical value of color doppler ultrasound in prenatal diagnosis of umbilical cord entry abnormity. Pak J Med Sci. 2016;32(6):1414–1418.
19. Bohîlțea RE, Turcan N, Cîrstoiu M. Prenatal ultrasound diagnosis and pregnancy outcome of umbilical cord knot - debate regarding ethical aspects of a series of cases. J Med Life. 2016;9(3):297–301.
20. Chen YH, Xu CM, Zheng HY, et al. Investigation on directions of fetal nuchal circular umbilical cord using color Doppler flow imaging. Chinese J Ultrasound Med. 2007;23(11):858–860.
21. Long FW, Chen YH, Chen HN, et al. Analysis of related factors of umbilical cord around neck. Chinese J Med Imag Technol. 2016;32(4):591–595.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.