")
Back to Journals » Clinical Interventions in Aging » Volume 17
Standard-Intensity Induction and Intermediate/High-Dose Cytarabine Consolidation Can Improve Survival for Elderly Patients with Newly Diagnosed Acute Myeloid Leukemia: A Retrospective Cohort Study
Authors Wang L, Zhao N, Zhou L , Tong J , Xue L, Zhang L, Han Y, Wang X, Geng L, Tang B, Liu H, Zhu W, Cai X, Liu X, Zhu X, Sun Z , Zheng C
Received 10 October 2021
Accepted for publication 28 December 2021
Published 20 January 2022 Volume 2022:17 Pages 55—64
DOI https://doi.org/10.2147/CIA.S343598
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Li Wang, Na Zhao, Li Zhou, Juan Tong, Lei Xue, Lei Zhang, Yongsheng Han, Xingbing Wang, Liangquan Geng, Baolin Tang, Huilan Liu, Weibo Zhu, Xiaoyan Cai, Xin Liu, Xiaoyu Zhu, Zimin Sun, Changcheng Zheng
Department of Hematology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei, People’s Republic of China
Correspondence: Changcheng Zheng
Department of Hematology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Lujiang Road No. 17, Hefei, 230001, People’s Republic of China
Tel/Fax +86-551-62284476
Email [email protected]
Background: There is great uncertainty in the treatment of elderly patients with acute myeloid leukemia (AML), which leads to great challenges in treatment decision. The aim of this study is to find more suitable induction therapy and consolidation therapy for elderly AML patients.
Methods: A total of 149 consecutive newly diagnosed elderly AML patients (aged ≥ 60 years) who received induction chemotherapy in our medical center from January 2015 to December 2019 were retrospectively analyzed.
Results: After the first induction treatment, the complete remission/or complete remission with incomplete hematologic recovery (CR/CRi) rates in the standard-intensity chemotherapy group was significantly higher than that in the low-intensity chemotherapy group (58.2% vs 32.9%, p = 0.003). Compared with the low-intensity chemotherapy, the incidence of severe infection in the standard-intensity chemotherapy was significantly increased (p < 0.001), but the early mortality was comparable. One hundred and seven patients received minimal residual disease (MRD) examination after the first induction treatment; and MRD was negative accounting for 51.9% in the standard-intensity chemotherapy group, while only 32.7% in the low-intensity group (p = 0.05). The 2-year-overall survival (OS) of patients in standard-intensity induction chemotherapy group (37.2%) was slightly higher than that in low-intensity induction chemotherapy group (23.4%) (p = 0.075). Eighty-one CR/CRi patients received intermediate or high dose cytarabine (n = 35) or sequential chemotherapy regimens (n = 46) as consolidation treatment. The 2-year OS and event-free survival (EFS) of patients in the intermediate or high-dose cytarabine group were significantly higher than those in the sequential chemotherapy regimens group (73.0% vs 38.5%, p = 0.002; 54.8% vs 35.0%, p = 0.035).
Conclusion: Our results showed that standard-intensity induction chemotherapy can significantly improve the CR rate for elderly AML patients, and does not increase the early mortality; consolidation therapy with intermediate or high-dose cytarabine can significantly improve EFS and OS for elderly AML patients achieved CR.
Keywords: acute myeloid leukemia, elderly patients, minimal residual disease, standard-intensity chemotherapy, intermediate or high dose cytarabine
Introduction
The incidence of acute myeloid leukemia increases with age;1 at least half of AML patients are over 60 years old.2 There is great uncertainty in the treatment of elderly patients with acute myeloid leukemia, which leads to great challenges in treatment decision. Treatment approach for elderly AML patients includes best supportive treatment, low-intensity chemotherapy and standard intensive chemotherapy, and previous clinical studies have shown that elderly AML patients receiving anti-leukemia treatment can still benefit compared with supportive treatment.3,4 Recently, the low-intensity regimen of BCL-2 inhibitor venetoclax plus hypomethylating agents (HMA) showed a relatively high complete remission (CR) rate and a tolerable safety profile in elderly AML patients unfit for intensive chemotherapy.5,6 However, based on the condition that venetoclax is not available, whether to use low-intensity chemotherapy or standard-intensity chemotherapy for the induction treatment of elderly AML is still unknown.
The CR rate of AML patients receiving intensive chemotherapy ranges from 39% to 65%;7–9 and patients who achieved CR do not receive consolidation treatment, the overall survival is relatively poor. However, little clear guidance is currently available on how to select a proper consolidation treatment approach for elderly AML patients who obtained CR.
This study retrospectively analyzed consecutive newly diagnosed elderly AML patients who received induction chemotherapy in our medical center, analyzed and compared treatment-related complications, early mortality during induction, the CR rate and survival between standard-intensity chemotherapy and low-intensity chemotherapy; for patients who achieved CR, consolidation with intermediate or high-dose cytarabine or sequential chemotherapy was also compared.
Methods
Patients
A total of 149 consecutive newly diagnosed elderly AML patients at the First Affiliated Hospital of University of Science and Technology of China from January 2015 to December 2019 were included in this retrospective analysis. All patients were aged 60 years or more. The diagnostic criteria of AML were based on the WHO classifications.10 All patients were diagnosed by bone marrow examination, including bone marrow cell morphology, immune phenotype, cytogenetic and molecular analyses, etc. Patient characteristics, blood cell counts, FAB-classification, molecular biology, European LeukemiaNet (ELN) risk assessment,11 induction chemotherapy, adverse events before or during induction, consolidation treatment, minimum residual disease (MRD) were collected. This research was approved and the written informed consent was waived by the Ethics Committee of the first affiliated hospital of university of science and technology of China (2021-RE-083).
Treatment
All elderly AML patients in this study received standard-intensity chemotherapy or low-intensity chemotherapy. Standard-intensity chemotherapy includes regimens of IA or DA (idarubicin, 8–12mg/m2/day, for 3 days or daunorubicin, 45–60mg/m2/day, for 3 days; and cytarabine,100 mg/m2/day, for 7 days), FLAG (fludarabine 30mg/m2/day, for 5 days; cytarabine 1g/m2/day, for 5 days; and granulocyte colony-stimulating factor (G-CSF) 5 ug/kg/day, for 5 days), or MA (mitoxantrone,10 mg/m2/day, for 3 days; cytarabine,100 mg/m2/day, for 7 days). Low-intensity chemotherapy included regimens of CAG (low-dose cytarabine 10 mg/m2, Q12h on days 1–14; aclarubicin 7 mg/m2/day on days 1–8, or 14 mg/m2/day on days 1–4; and G-CSF 5 ug/kg/day on days 1–14), HAG (homoharringtonine 1mg/m2/day on days 1–7; low-dose cytarabine 10 mg/m2, Q12h on days 1–14 and G-CSF 5ug/kg/day on days 1–14), IAG (idarubicin 5mg/m2/day on days 1–3; low-dose cytarabine 10mg/m2, Q12h on days 1–14 and G-CSF 5ug/kg/day on days 1–14), hypomethylating agents (HMA) (Azacitidine 75mg/m2/day, on days 1–7 or Decitabine 15–20mg/m2/day, on days 1–5), HMA +CAG, HMA+HAG, HMA+IAG, etc.
Patients who achieved CR/CRi entered consolidation treatment phase and were treated with intensive intermediate or high-dose cytarabine (1.5–2g/m2 q12h, for 3 days) or sequential chemotherapy regimens (such as IA, HA, MA, CAG, HAG, HMA +CAG, HMA+HAG, etc).
Definitions and Statistical Analysis
Bone marrow examination was used to judge whether the patient had CR or not. Morphological CR, molecular CR, CR with incomplete count recovery (CRi), partial response (PR), no response (NR), relapse, overall survival (OS) and event-free survival (EFS) were defined as reported elsewhere.11 Early death was defined as death within 30 days from the first diagnosis.
MRD was identified using the leukemia-associated immunophenotypes approach. Eight color flow cytometry was performed in all patients undergoing bone marrow examination as a routine clinical test. An MRD level <0.01% was considered negative in this study.
Categorical variables were assessed using the chi-square test or Fisher’s exact test, and continuous variables were assessed using the Mann–Whitney U-test between 2 groups. The probabilities of OS and EFS were estimated based on the Kaplan–Meier method. The probabilities of early death and relapse were estimated by the cumulative-incidence function method. Death from any reason other than leukemia progression or relapse represents a competing risk. The end point of OS was death from any cause, and the end point of EFS was relapse or death. Statistical analyses were conducted using R statistical software (R Foundation for Statistical Computing). Differences with p < 0.05 were considered significant.
Results
Clinical Characteristics
A total of 149 elderly AML patients (age ≥60 years) were enrolled in this study, 87 males and 62 females, with a median age of 66 years (range 60–83). Among them, 67 patients received standard-intensity chemotherapy and 82 patients received low-intensity chemotherapy. The median age was 65 years (60–76) in the standard-intensity chemotherapy group and 70 years (60–83) in the low-intensity chemotherapy group (p < 0.001). In standard-intensity chemotherapy group, 64 patients (64/67, 95.5%) were treated with IA regimen, 1 patient was treated with DA regimen, 1 patient was treated with FLAG regimen, 1 patient was treated with MA regimen. In low-intensity chemotherapy group, 35 patients (35/82, 42.7%) were treated with CAG or HAG or IAG regimens and 47 patients (47/82, 57.3%) were treated with hypomethylating agents plus low dose cytarabine or CAG or HAG or IAG regimens. The median white blood count at first diagnosis in standard-intensity chemotherapy group was higher than in low-intensity chemotherapy group (18.43×109/L vs 6.77 ×109/L) (p = 0.039). According to the 2017 ELN classification, the patients were divided into three risk groups, the high-risk patients receiving standard-intensity chemotherapy (28/67, 41.8%) were slightly higher than those receiving low-intensity chemotherapy (24/82, 29.3%) (p = 0.06). Detailed results are shown in Table 1.
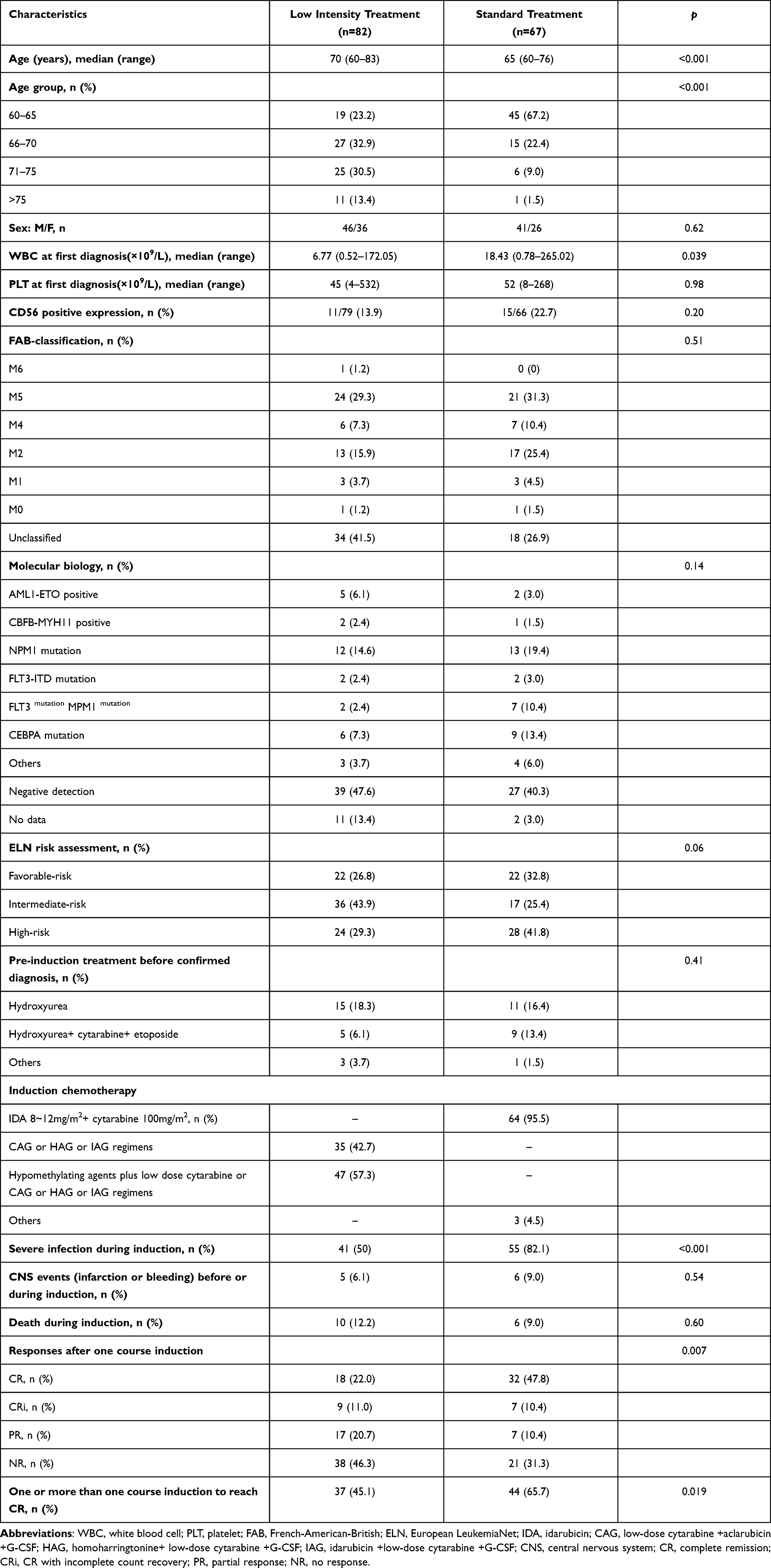 |
Table 1 Clinical Characteristics |
Response to Induction Chemotherapy
Of the 149 patients, 66 (44.3%) achieved CR/CRi after the first induction treatment. The CR/CRi rate was 58.2% (39/67) in the standard-intensity chemotherapy group and 32.9% (27/82) in the low-intensity group (p = 0.003) (Figure 1A). In 82 patients of low-intensity chemotherapy, 47 patients received HMA-based treatment during induction therapy and 35 patients were not; the CR/CRi rate in the HMA-based treatment group was 23.4% (11/47) and 45.7% (16/35) in the Non-HMA-based treatment group (p = 0.06) (Figure 1B).
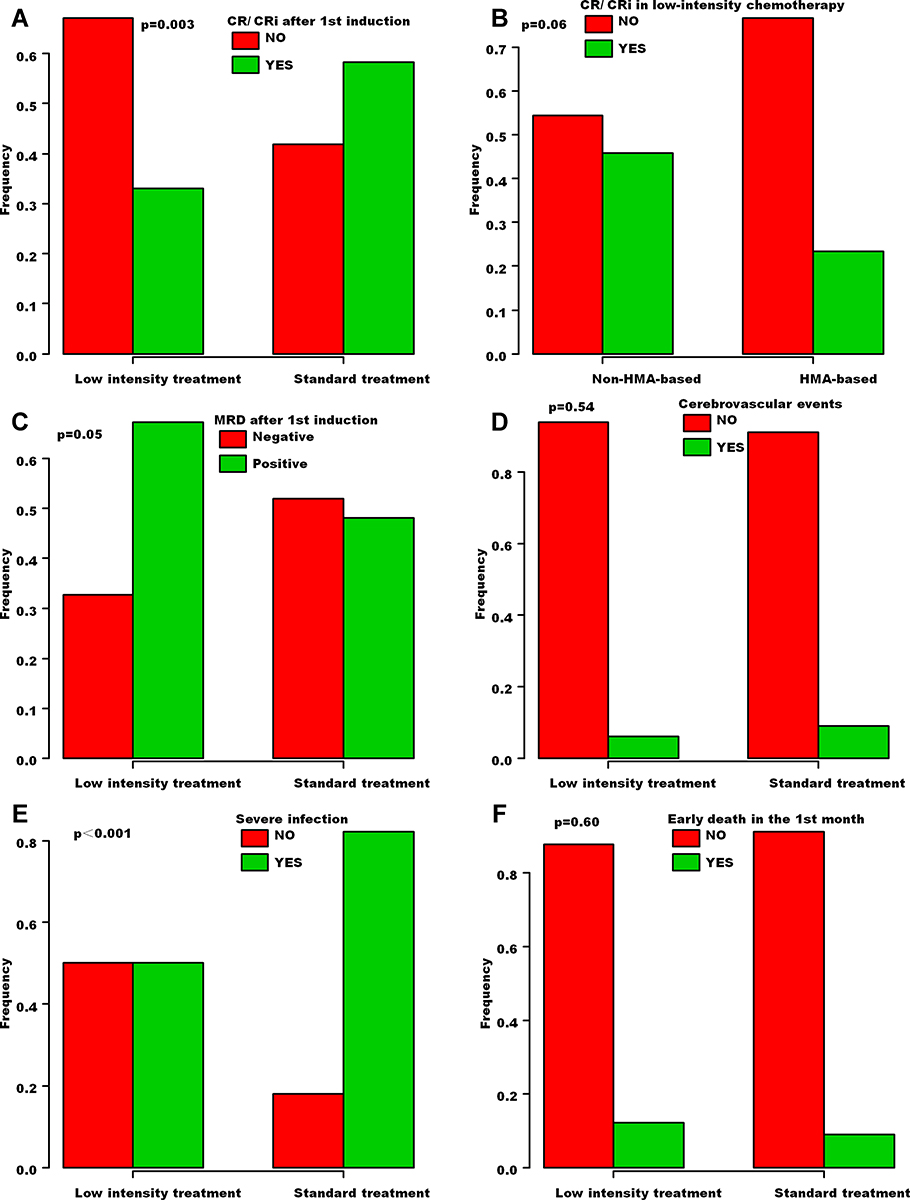 |
Figure 1 Efficacy and complications. The CR/CRi rate between the standard-intensity group and the low-intensity group (A). The effect of HMA on CR/CRi in low-intensity chemotherapy group (B). MRD after the first course of induction chemotherapy in the standard-intensity group and the low-intensity group (C). The occurrence of cerebrovascular events in the standard-intensity group and the low-intensity group (D). The incidence of severe infection between the standard-intensity group and the low-intensity group (E). Early death in the first month during induction chemotherapy between the standard-intensity group and the low-intensity group (F). Abbreviations: CR, complete remission; CRi, CR with incomplete count recovery; HMA, hypomethylating agents; MRD, minimal residual disease. |
Among 149 patients receiving induction chemotherapy, 107 patients received MRD examination after the first induction treatment. In 52 patients receiving standard-intensity chemotherapy, MRD was negative accounting for 51.9% (27/52); while in 55 patients receiving low-intensity chemotherapy, MRD was negative only accounting for 32.7% (18/55) (p = 0.05) (Figure 1C). Among 66 CR/CRi patients after the first induction treatment, 63 patients received MRD examination. MRD negativity was 71.1% (27/38) in the standard-intensity chemotherapy group and 72.0% (18/25) in the low-intensity group (p = 0.99).
During induction therapy, there was no significant difference in the occurrence of cerebrovascular events such as cerebral hemorrhage or cerebral infarction between two groups (6 patients in the standard-intensity chemotherapy group and 5 patients in the low-intensity group) (p = 0.54) (Figure 1D). The incidence of severe infection such as sepsis and severe pneumonia in the standard-intensity chemotherapy group (55/67, 82.1%) was significantly increased compared to the low-intensity chemotherapy group (41/82, 50%) (p < 0.001) (Figure 1E). Six patients (9.0%) in the standard-intensity chemotherapy group and 10 patients (12.2%) in the low-intensity group died during the first month of induction treatment (p = 0.60) (Figure 1F). There were no significant differences between the 2 groups in 1-month early mortality (p = 0.65) (Figure 2A).
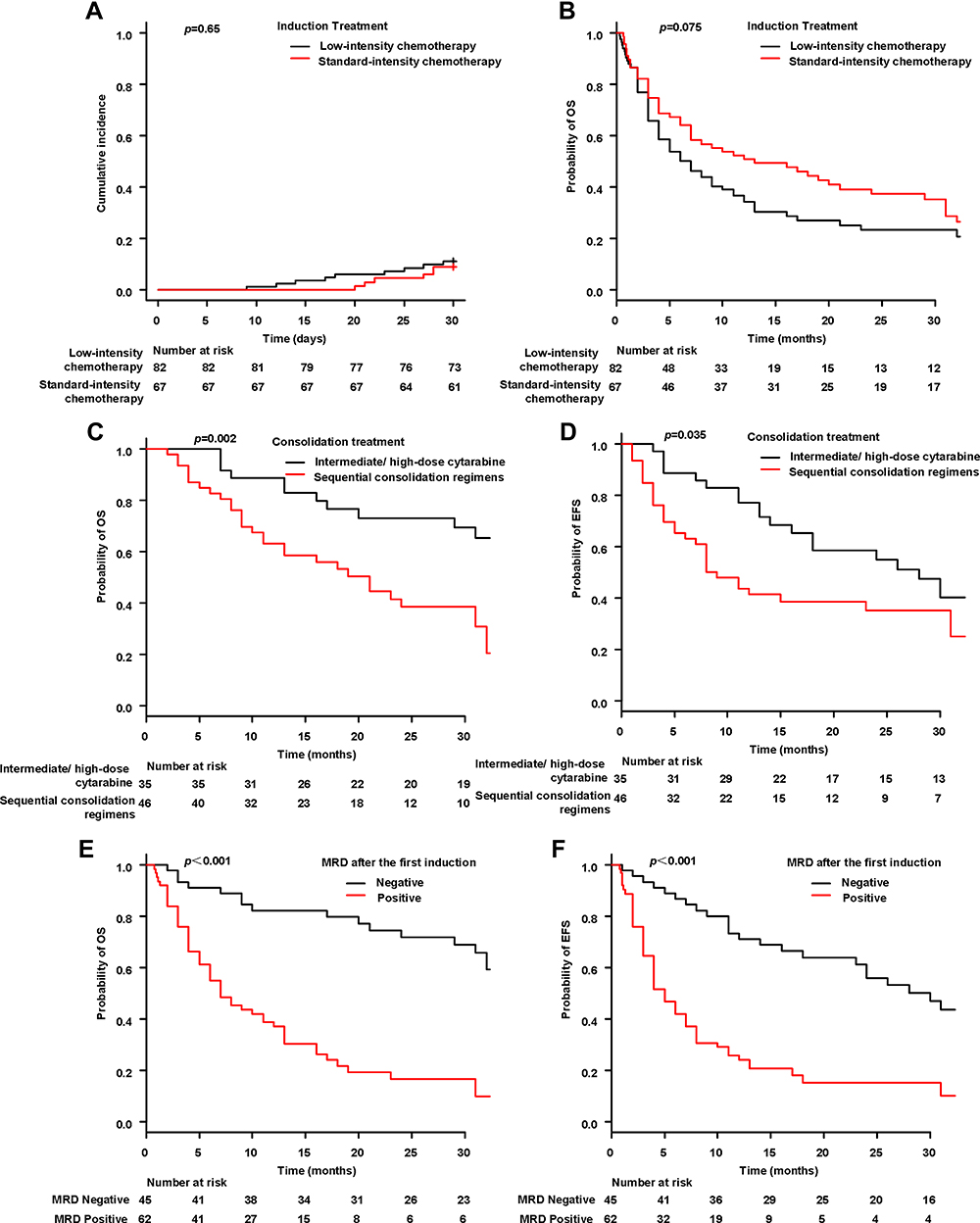 |
Figure 2 Survival. The 1-month early mortality between the standard-intensity group and the low- intensity group (A). The OS between the standard-intensity group and the low-intensity group (B). The OS and EFS between the intermediate/high-dose cytarabine group and the sequential chemotherapy consolidation group (C and D). OS and EFS stratified for MRD status in patients treated with standard-intensity chemotherapy or low-intensity chemotherapy (E and F). Abbreviations: OS, overall survival; EFS, event-free survival; MRD, minimal residual disease. |
Survival
The median follow-up time of 149 patients was 9 months (0.3–67). The 2-year OS of patients in standard-intensity induction chemotherapy group (37.2% with 95% CI, 25.5 to 49.0) was slightly longer than that in low-intensity induction chemotherapy group (23.4% with 95% CI, 14.4 to 33.6) (p = 0.075) (Figure 2B).
Eighty-one patients achieved CR after one or more courses induction chemotherapy, 35 patients treated with intermediate or high-dose cytarabine, and 46 patients treated with sequential chemotherapy (clinical characteristics are shown in Supplement Table 1). During the consolidation phase, 44 of 81 experienced relapse. Eighteen patients (18/35, 51.4%) experienced relapse in the intermediate or high dose cytarabine group, and 26 patients (26/46, 56.5%) experienced relapse in the sequential chemotherapy group during follow-up. The 2-year OS was 73.0% (95% CI, 54.3 to 85.0) in the intermediate or high-dose cytarabine consolidation group, in comparison with 38.5% (95% CI, 23.5 to 53.3) in the sequential chemotherapy consolidation group (p = 0.002) (Figure 2C). The 2-year EFS was significantly higher after intermediate or high-dose cytarabine consolidation (54.8% with 95% CI, 36.3 to 70.0) in comparison with continuous sequential chemotherapy consolidation (35.0% with 95% CI, 21.1 to 49.4) (p = 0.035) (Figure 2D).
MRD Presence after the first induction was associated with poor prognosis. The 2-year OS was 71.8% (95% CI, 55.6 to 83.0) in the MRD negative group, which was significantly higher than that in the MRD positive group (16.5% with 95% CI, 7.75 to 28.2) (p < 0.001) (Figure 2E). A significant EFS advantage was also demonstrable, the 2-year EFS was 55.9% (95% CI, 39.7 to 69.3) in the MRD negative group and 15.1% (95% CI, 6.86 to 26.4) in the MRD positive group (p < 0.001) (Figure 2F). For patients who achieved CR/CRi after the first induction treatment, MRD negative group was also associated with higher 2-year OS and 2-year EFS rates when compared with MRD positive group (Supplement Figure 1).
Discussion
This study retrospectively analyzed all the elderly AML patients who received induction therapy in our medical center in the past five years. The median age was 66 years, which was consistent with the previously reported median age of 65–70 years.2,3,12 Elderly AML patients have a poor disease-free survival (DFS) and OS due to poor cytogenetic abnormalities, easily developing drug resistance, high incidence of cytopenia and low CR rate.13 There is no standard scoring system for the selection of induction therapy in elderly patients. Compared with supportive treatment, elderly AML patients receiving anti-leukemia treatment can still benefit, and low-intensity induction treatment are easily accepted and increasingly used. Recently, a multicenter retrospective (n = 1292) and prospective nonrandomized cohort study (n = 695) was conducted to investigate the survival and quality of life (QOL) benefits with intensive or less-intensive chemotherapy among elderly AML patients; and patients receiving intensive chemotherapy had superior OS compared with those receiving less-intensive options.14 At the same time, a multicentric European database which collected data of 3700 newly diagnosed acute myeloid leukemia patients ≥70 years, including 1199 patients receiving intensive chemotherapy and 1073 patients receiving hypomethylating agents; this study showed that intensive chemotherapy remains a valuable option associated with high remission rate and better long-term survival in older AML patients.15 In our data, 45% patients received standard-intensity induction chemotherapy, and the CR rate was 58.2%, which was consistent with the previous reports of 39–69%.3,7,9 Fifty-five percent of the patients received low-intensity chemotherapy and the CR rate was only 32.9%, which was consistent with previous reports of 27–35%.3,7
Previous studies had shown that standard-intensity chemotherapy increases the incidence of infection and treatment-related mortality (TRM).16,17 This study showed that although the incidence of severe infection was significantly increased during the period of standard-intensity induction, there was no increase in early mortality. The real cause of early death may be the disease itself rather than the TRM. The effective evaluation of AML patients after induction is generally reflected by the detection of bone marrow morphology and MRD. At present, assessment of MRD is more common in young AML patients receiving intensive chemotherapy, which has a certain value in the evaluation of disease recurrence and prognosis.18,19 The value of MRD in elderly AML patients based on different treatment regimens is still unclear. Our data showed MRD-negative patients in standard-intensity chemotherapy group accounted for 51.9% and only 32.7% in low intensity induction chemotherapy group, which was consistent with 62% receiving intensive chemotherapy and 30% receiving HMA in the study by Hilberink et al.20 Freeman et al21 showed that the OS of elderly AML patients with negative MRD was significantly better than that of patients with positive MRD, regardless of CR1 or CR2. Our results also showed that MRD negative patients had significantly improved OS and EFS compared with MRD positive patients.
The consolidation treatment of young AML patients after remission is relatively clear, using high-dose cytarabine or allo-HSCT.22,23 However, due to the poor physical tolerance of elderly AML patients, there is currently no clear choice of follow-up consolidation therapy. Post-remission therapy is important to AML patients, and the mortality and recurrence rate without consolidation treatment are significantly increased. This study indicated that consolidation therapy with 3~ 4 courses intermediate or high-dose cytarabine significantly prolonged EFS and OS, and none of the patients terminated treatment due to severe neurotoxicity. Although not all elderly patients may receive intensive induction chemotherapy, those that do probably do better with intermediate or high dose cytarabine. Chemotherapy-related toxicity and patient tolerance are the main factors limiting the dose of cytarabine in elderly AML patients, and some studies have shown that 500 mg/m2 or 1 g/m2 cytarabine can also prolong DFS and OS.24,25
Conclusion
In conclusion, this study indicated that, treatment for elderly AML patients, standard-intensity induction chemotherapy can significantly improve the CR rate, and does not increase the early mortality; and consolidation therapy with intermediate or high-dose cytarabine can significantly improve EFS and OS. However, this is a retrospective clinical study with limited number of patients in each group; we will continue to expand the number of cases in a prospective study, try to find out which elderly AML patients can benefit from intensive chemotherapy. In addition, some clinical characteristics of patients receiving low intensity treatment differed from that of patients receiving standard treatment including age, WBC counts at first diagnosis and ELN risk assessment, etc. Furthermore, recent studies have indicated that the combination of venetoclax and HMA improves the remission rate and OS for elderly AML patients; we will also design and conduct a prospective study to reassess the efficacy differences between intensive chemotherapy and this new protocol.
Data Sharing Statement
The datasets used and/or analyzed in this study are available from the corresponding authors upon reasonable request.
Ethics Approval and Informed Consent
This study was approved and the written informed consent was waived by the ethics committee of the first affiliated hospital of university of science and technology of China (2021-RE-083) due to the retrospective nature of the review, and confirmed that the data was anonymized and maintained with confidentiality. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors thank the patients, their families, and all doctors who treated the patients.
Funding
This work was partly supported by Key research and development projects in Anhui Province (202004j07020025), the Fundamental Research Funds for the Central Universities of China (WK9110000003).
Disclosure
The authors report no conflicts of interest.
References
1. Estey E, Döhner H. Acute myeloid leukaemia. Lancet. 2006;368(9550):1894–1907. doi:10.1016/S0140-6736(06)69780-8
2. Nagel G, Weber D, Fromm E, et al. Epidemiological, genetic, and clinical characterization by age of newly diagnosed acute myeloid leukemia based on an academic population-based registry study (AMLSG BiO). Ann Hematol. 2017;96(12):1993–2003. doi:10.1007/s00277-017-3150-3
3. Hilberink J, Hazenberg C, van den Berg E, et al. Not type of induction therapy but consolidation with allogeneic hematopoietic cell transplantation determines outcome in older AML patients: a single center experience of 355 consecutive patients. Leuk Res. 2019;80:33–39. doi:10.1016/j.leukres.2019.03.004
4. Medeiros BC, Othus M, Fang M, Roulston D, Appelbaum FR. Prognostic impact of monosomal karyotype in young adult and elderly acute myeloid leukemia: the Southwest Oncology Group (SWOG) experience. Blood. 2010;116(13):2224–2228. doi:10.1182/blood-2010-02-270330
5. DiNardo CD, Pratz K, Pullarkat V, et al. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood. 2019;133(1):7–17. doi:10.1182/blood-2018-08-868752
6. DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and venetoclax in previously untreated acute myeloid leukemia. N Engl J Med. 2020;383(7):617–629. doi:10.1056/NEJMoa2012971
7. Vachhani P, Al Yacoub R, Miller A, et al. Intensive chemotherapy vs. hypomethylating agents in older adults with newly diagnosed high-risk acute myeloid leukemia: a single center experience. Leuk Res. 2018;75:29–35. doi:10.1016/j.leukres.2018.10.011
8. Löwenberg B, Suciu S, Archimbaud E, et al. Use of recombinant GM-CSF during and after remission induction chemotherapy in patients aged 61 years and older with acute myeloid leukemia: final report of AML-11, a Phase III randomized study of the Leukemia Cooperative Group of European Organisation for the research and treatment of cancer and the Dutch Belgian Hemato-Oncology Cooperative Group. Blood. 1997;90(8):2952–2961.
9. Löwenberg B, Ossenkoppele GJ, van Putten W, et al. High-dose daunorubicin in older patients with acute myeloid leukemia. N Engl J Med. 2009;361(13):1235–1248. doi:10.1056/NEJMoa0901409
10. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. doi:10.1182/blood-2016-03-643544
11. Döhner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
12. Sharplin K, Wee LYA, Singhal D, et al. Outcomes and health care utilization of older patients with acute myeloid leukemia. J Geriatr Oncol. 2021;12(2):243–249. doi:10.1016/j.jgo.2020.07.002
13. Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloid leukemia. Blood. 2006;107(9):3481–3485. doi:10.1182/blood-2005-09-3724
14. Sorror ML, Storer BE, Fathi AT, et al. Multisite 11-year experience of less-intensive vs intensive therapies in acute myeloid leukemia. Blood. 2021;138(5):387–400. doi:10.1182/blood.2020008812
15. Récher C, Röllig C, Bérard E, et al. Long-term survival after intensive chemotherapy or hypomethylating agents in AML patients aged 70 years and older: a large patient data set study from European registries. Leukemia. 2021. PMID: 34775483. doi:10.1038/s41375-021-01425-9
16. Østgård LS, Nørgaard JM, Sengeløv H, et al. Comorbidity and performance status in acute myeloid leukemia patients: a nation-wide population-based cohort study. Leukemia. 2015;29(3):548–555. doi:10.1038/leu.2014.234
17. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med. 2009;7(4):357–363. doi:10.1370/afm.983
18. Terwijn M, van Putten WL, Kelder A, et al. High prognostic impact of flow cytometric minimal residual disease detection in acute myeloid leukemia: data from the HOVON/SAKK AML 42A study. J Clin Oncol. 2013;31(31):3889–3897. doi:10.1200/JCO.2012.45.9628
19. Araki D, Wood BL, Othus M, et al. Allogeneic hematopoietic cell transplantation for acute myeloid leukemia: time to move toward a minimal residual disease-based definition of complete remission? J Clin Oncol. 2016;34(4):329–336. doi:10.1200/JCO.2015.63.3826
20. Hilberink JR, Morsink LM, van der Velden WJFM, et al. Pretransplantation MRD in older patients with AML after treatment with decitabine or conventional chemotherapy. Transplant Cell Ther. 2021;27(3):246–252. doi:10.1016/j.jtct.2020.12.014
21. Freeman SD, Virgo P, Couzens S, et al. Prognostic relevance of treatment response measured by flow cytometric residual disease detection in older patients with acute myeloid leukemia. J Clin Oncol. 2013;31(32):4123–4131. doi:10.1200/JCO.2013.49.1753
22. Miyawaki S, Ohtake S, Fujisawa S, et al. A randomized comparison of 4 courses of standard-dose multiagent chemotherapy versus 3 courses of high-dose cytarabine alone in postremission therapy for acute myeloid leukemia in adults: the JALSG AML201 Study. Blood. 2011;117(8):2366–2372. doi:10.1182/blood-2010-07-295279
23. Koreth J, Schlenk R, Kopecky KJ, et al. Allogeneic stem cell transplantation for acute myeloid leukemia in first complete remission: systematic review and meta-analysis of prospective clinical trials. JAMA. 2009;301(22):2349–2361. doi:10.1001/jama.2009.813
24. Stone RM, Berg DT, George SL, et al. Postremission therapy in older patients with de novo acute myeloid leukemia: a randomized trial comparing mitoxantrone and intermediate-dose cytarabine with standard-dose cytarabine. Blood. 2001;98(3):548–553. doi:10.1182/blood.v98.3.548
25. Sperr WR, Piribauer M, Wimazal F, et al. A novel effective and safe consolidation for patients over 60 years with acute myeloid leukemia: intermediate dose cytarabine (2 x 1 g/m2 on days 1, 3, and 5). Clin Cancer Res. 2004;10(12 Pt 1):3965–3971. doi:10.1158/1078-0432.CCR-04-0185
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.